Back to Journals » Research and Reports in Urology » Volume 18
Vacuum-Assisted Mini-PCNL is Associated with Lower Postoperative SIRS: A Real-World Cohort Study
Authors Piyawannarat S ![]() , Sirisopana K, Choonu N, Phengsalae Y, Sangkum P, Ketsuwan C, Kongchareonsombat W
, Sirisopana K, Choonu N, Phengsalae Y, Sangkum P, Ketsuwan C, Kongchareonsombat W ![]()
Received 25 April 2026
Accepted for publication 6 June 2026
Published 15 June 2026 Volume 2026:18 618289
DOI https://doi.org/10.2147/RRU.S618289
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Panagiotis J Vlachostergios
Surawach Piyawannarat, Kun Sirisopana, Nipapan Choonu, Yada Phengsalae, Premsant Sangkum, Chinnakhet Ketsuwan, Wisoot Kongchareonsombat
Division of Urology, Department of Surgery, Faculty of Medicine Ramathibodi Hospital, Mahidol University, Bangkok, Thailand
Correspondence: Wisoot Kongchareonsombat, Fax +66-2-2794704, Email [email protected]
Background: Postoperative systemic inflammatory response syndrome (SIRS) remains a key complication after mini-percutaneous nephrolithotomy (mini-PCNL) and is often related to elevated intrarenal pressure and bacterial translocation. Vacuum-assisted mini-PCNL (VmPCNL) has been developed to mitigate this risk through active pressure control.
Objective: To evaluate the association between VmPCNL and postoperative SIRS and to identify the independent predictors of SIRS in a real-world cohort.
Materials and Methods: A retrospective cohort study was conducted of patients undergoing mini-PCNL at a tertiary referral center between January 2021 and May 2025. Patients were stratified into standard mini-PCNL (SmPCNL) and VmPCNL groups. The primary endpoint was SIRS within 48 hours post-surgery. Secondary outcomes included operative time, stone-free rate (SFR), and length of hospital stay (LOS). Multivariable logistic regression was used to identify independent predictors of SIRS.
Results: A total of 136 patients were included in the study (SmPCNL, n = 78; VmPCNL, n = 58). The incidence of postoperative SIRS was significantly lower in the VmPCNL group (8.6% vs 21.8%, p = 0.036). VmPCNL was also associated with shorter operative time (median 90 minutes vs 115 minutes, p = 0.038) and reduced LOS (p = 0.012). Stone-free rates were comparable between the groups, indicating no compromise in procedural efficacy. In the multivariable analysis, VmPCNL was independently associated with a lower risk of SIRS (adjusted OR [aOR] 0.44, 95% CI 0.19– 0.98, p = 0.041), while a positive preoperative urine culture was an independent risk factor (aOR 2.60, 95% CI 1.01– 6.60, p = 0.045).
Conclusion: In this real-world cohort, VmPCNL was associated with a lower SIRS incidence and improved perioperative efficiency without compromising stone-free outcomes. The mechanism may involve improved intraoperative outflow dynamics through active suction, although direct measurement of intrarenal pressure is needed to confirm this hypothesis.
Keywords: mini-PCNL, vacuum-assisted, intrarenal pressure, systemic inflammatory response syndrome, kidney stones
Introduction
Percutaneous nephrolithotomy (PCNL) remains the gold standard for managing renal calculi larger than 2 cm.1,2 While conventional PCNL achieves high stone-free rates (SFR), it is associated with significant morbidity, including hemorrhage and infectious complications.3–5 Postoperative fever occurs in 21–37% of cases, while systemic inflammatory response syndrome (SIRS) and sepsis are reported in up to 35% and 9.3% of patients, respectively.6–8
A key modifiable intraoperative factor influencing these outcomes is intrarenal pressure (IRP).9,10 Elevated intrarenal pressure may promote pyelovenous and pyelolymphatic backflow, facilitating bacterial and endotoxin translocation into the systemic circulation and potentially contributing to postoperative SIRS and sepsis.11–13
Mini-percutaneous nephrolithotomy (mini-PCNL) was developed to mitigate surgical morbidity by utilizing smaller tract sizes (14–20 Fr).14,15 Although it provides comparable SFR with reduced blood loss and shorter recovery, the narrower tract creates a dynamic imbalance between irrigation inflow and outflow, potentially resulting in increased IRP and a higher risk of infectious complications compared to standard large-tract PCNL.
Vacuum-assisted mini-PCNL (VmPCNL) has been developed to address this limitation. By applying regulated negative pressure through a suction-enabled access sheath, this technique aims to maintain a stable, low-pressure environment during stone fragmentation and evacuation. Although preliminary studies have suggested potential perioperative advantages of vacuum-assisted systems, direct real-world comparative evidence between VmPCNL and standard mini-PCNL (SmPCNL), particularly regarding postoperative inflammatory outcomes, remains limited.16 Therefore, this study aimed to compare the incidence of postoperative SIRS between VmPCNL and SmPCNL and to identify the independent predictors of postoperative SIRS in a real-world clinical cohort.
Materials and Methods
Study Design and Ethical Considerations
This retrospective cohort study was conducted at a tertiary referral center (Ramathibodi Hospital) and approved by the Human Research Ethics Committee, Faculty of Medicine Ramathibodi Hospital, Mahidol University (COA No. MURA2025/804). The requirement for informed consent was waived by the ethics committee due to the retrospective nature of the study and the use of de-identified data. The study was performed in accordance with the principles of the Declaration of Helsinki, and all patient data were encrypted to ensure confidentiality.
Patient Selection and Data Collection
We identified all consecutive adult patients (≥ 18 years) who underwent mini-PCNL for renal calculi between January 2021 and May 2025. Patients with congenital renal anomalies (eg., horseshoe kidney or medullary sponge kidney), kidney transplant recipients, and those undergoing concurrent surgical procedures were excluded. Additional exclusion criteria included general contraindications to surgery, pregnancy, skeletal deformities precluding proper positioning, uncorrectable coagulopathy, pyonephrosis, and uncontrolled upper urinary tract infection.
All patients underwent standardized preoperative evaluation, including a complete blood count, serum biochemistry, urinalysis, and urine culture. Perioperative antibiotic prophylaxis was administered according to institutional protocol. Patients with positive preoperative urine cultures received culture-directed antibiotics before surgery until no evidence of active urinary tract infection remained. Radiologic assessment included kidneys, ureters, and bladder (KUB) radiography and non-contrast computed tomography of the kidneys, ureters, and bladder (CT KUB) to characterize stone burden and renal anatomy.
Collected variables included age, sex, body mass index (BMI), American Society of Anesthesiologists (ASA) classification, stone laterality, history of urinary tract infection (UTI), preoperative urine culture results, preoperative stenting or nephrostomy, stone size, stone multiplicity, Guy’s stone score (GSS), Hounsfield units (HU), presence of hydronephrosis, and number of access tracts. Perioperative and postoperative variables collected included operative time, estimated blood loss, transfusion requirement, postoperative SIRS, quick Sequential Organ Failure Assessment (qSOFA) positivity, sepsis, SFR, and length of hospital stay (LOS).
Outcome Definitions
The primary outcome was the incidence of postoperative SIRS within 48 hours. SIRS was defined as the presence of at least two of the following: body temperature < 36°C or > 38°C, heart rate > 90 beats/min, respiratory rate > 20 breaths/min, or abnormal white blood cell count (> 12,000/mm3, < 4,000/mm3, or > 10% bands). The SIRS criteria were selected as an early and sensitive marker of postoperative inflammatory response.
Secondary outcomes included qSOFA positivity (score ≥ 2), defined by altered mental status, systolic blood pressure ≤ 100 mmHg, or respiratory rate ≥ 22 breaths/min, and sepsis, defined according to the Sepsis-3 criteria.
Operative outcomes included operative time, estimated blood loss, transfusion rate, SFR, and LOS. Stone size was defined as the maximum diameter; for multiple stones, the sum of the maximum diameters was used. SFR was defined as no residual fragments or clinically insignificant residual fragments < 4 mm, assessed at 12 weeks using non-contrast CT KUB.
Surgical Technique
All procedures were performed by a single experienced surgeon using a standardized operative protocol. The patients were positioned in the Galdakao-modified supine Valdivia position. Percutaneous renal access was obtained under fluoroscopic guidance following ureteric catheter placement. Tract dilation was performed using a single-step technique. After predilation to 12 Fr with fascial dilators, the access sheath was advanced directly into the collecting system in one pass. The patients were then managed using one of two techniques:
SmPCNL group: A 15/16-Fr metallic sheath (Karl Storz, Germany) was used to allow passive irrigation outflow.
VmPCNL group: A 14/16-Fr ClearPetra disposable nephrostomic sheath (Well Lead Medical Co., China) was connected to standard hospital wall vacuum suction via a closed suction canister system with an inline adjustable vacuum regulator. The negative pressure was not quantitatively recorded during the procedure; instead, the suction level was titrated qualitatively by the operating surgeon according to endoscopic visibility, irrigation outflow, and fragment clearance, reflecting routine clinical practice.
Irrigation was delivered using a pressure-controlled double-roller pump system (UROMAT E.A.S.I., Karl Storz, Germany) to maintain adequate visualization while minimizing intrarenal pressure. Laser lithotripsy was performed using a 120-W holmium laser with a 550-μm fiber for stone fragmentation and dusting.
Stone fragments were primarily evacuated using continuous suction, and auxiliary devices, such as baskets, were not routinely required. At the end of the procedure, a 6-Fr double-J ureteral stent was routinely placed.
Statistical Analysis
Statistical analysis was performed using STATA version 18 (StataCorp, College Station, TX, USA). A two-sided p-value < 0.05 was considered statistically significant.
Continuous variables were assessed for normality using the Shapiro–Wilk test and compared using Student’s t-test or the Mann–Whitney U-test, as appropriate. Categorical variables were compared using the chi-square test or Fisher’s exact test.
The primary outcome was postoperative SIRS within 48 hours. Multivariable logistic regression was performed to identify the independent predictors of postoperative SIRS. Clinically relevant covariates were selected a priori, including treatment group, preoperative urine culture status, and operative time. Adjusted odds ratios (aORs) with 95% confidence intervals (CIs) were reported.
To account for non-randomized treatment allocation, inverse probability of treatment weighting (IPTW) based on the propensity score was performed as a sensitivity analysis. The propensity score model included age, sex, BMI, ASA classification, diabetes mellitus, hypertension, dyslipidemia, history of urinary tract infection, positive preoperative urine culture, previous stone surgery, GSS, stone volume, stone density, stone multiplicity, hydronephrosis, and preoperative estimated glomerular filtration rate (eGFR), as presented in Supplementary Table S1. Covariate balance before and after weighting was assessed using standardized mean differences (SMD), with an SMD < 0.1 considered indicative of adequate balance. Weighted logistic regression was then used to estimate the association between the treatment group and postoperative SIRS.
Missing data were minimal and were handled using complete-case analysis.
Results
A total of 136 patients were included in the analysis, comprising 78 patients in the SmPCNL group and 58 patients in the VmPCNL group.
Baseline characteristics were generally comparable between the groups (Table 1); there were no significant differences in age, sex, BMI, or ASA classification. Stone-related parameters, including stone size, GSS, stone density, and the presence of hydronephrosis, were also similar between the groups. Although not statistically significant, the SmPCNL group had a higher proportion of patients with a history of urinary tract infection and a positive preoperative urine culture.
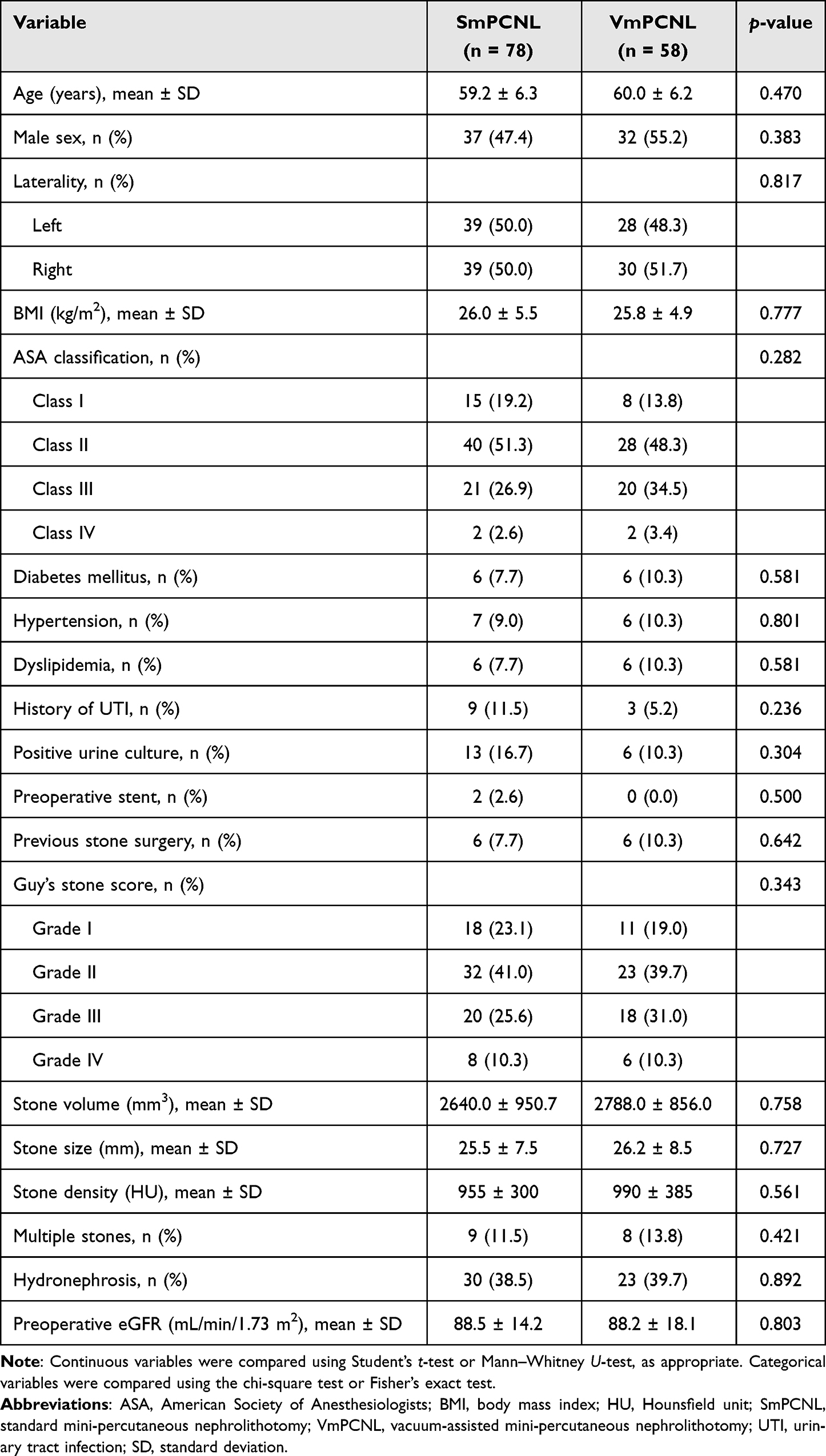 |
Table 1 Baseline Characteristics of the Study Population |
Perioperative Outcomes
The VmPCNL group demonstrated significantly shorter operative times compared with the SmPCNL group (median 90 minutes [IQR 65–125] vs 115 minutes [IQR 90–140], p = 0.038). Estimated blood loss and transfusion rates were comparable between the groups. Stone-free rates were similar (86.2% vs 82.1%, p = 0.384), indicating no compromise in procedural efficacy. The length of hospital stay was significantly shorter in the VmPCNL group (p = 0.012) (Table 2).
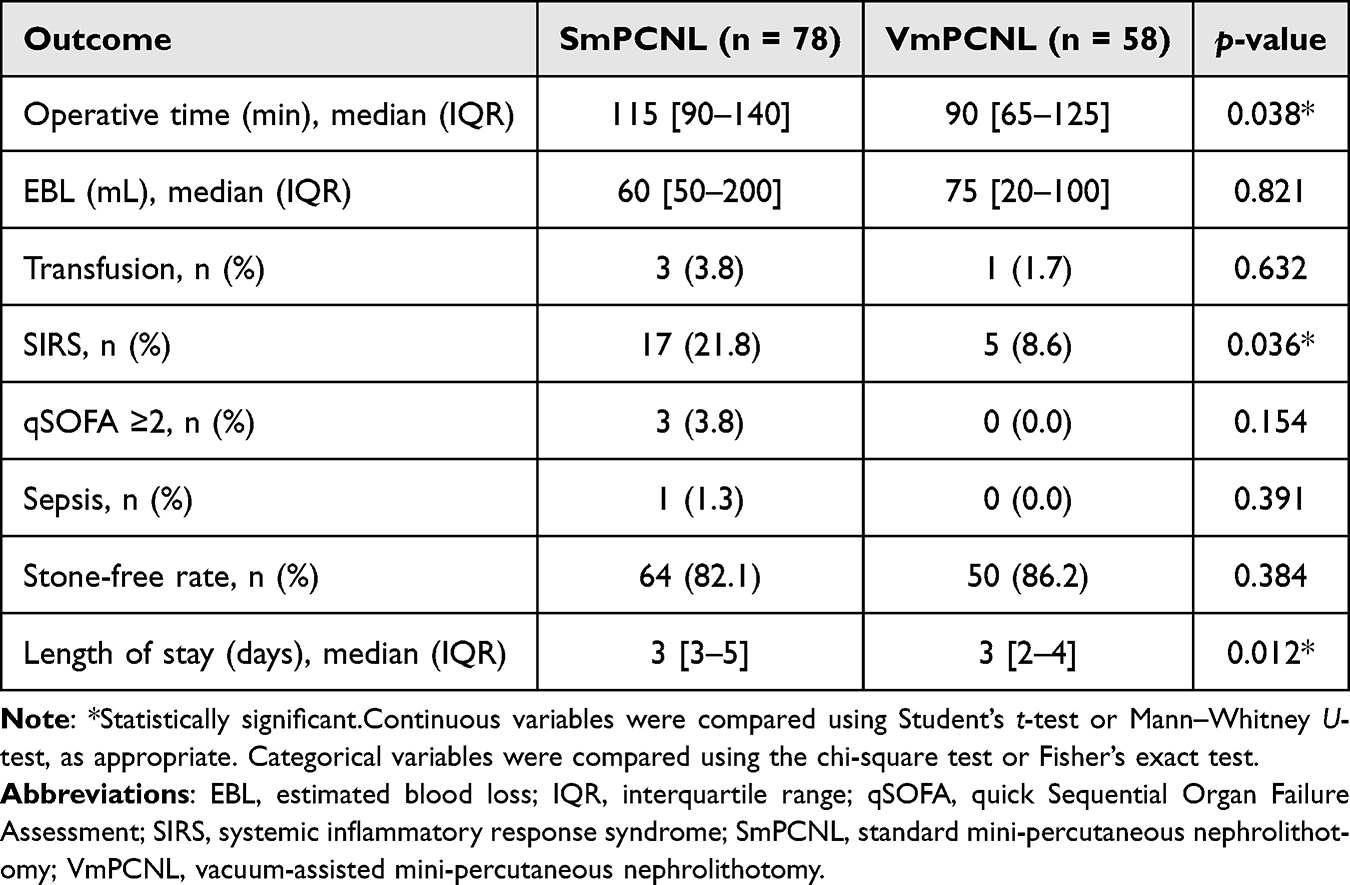 |
Table 2 Perioperative and Postoperative Outcomes |
Infection Outcomes
The incidence of postoperative SIRS was significantly lower in the VmPCNL group compared with the SmPCNL group (8.6% vs 21.8%, p = 0.036). Severe infectious complications were uncommon. qSOFA positivity occurred in 3.8% of patients in the SmPCNL group and in none of the VmPCNL group (p = 0.154). Only one patient (1.3%) in the SmPCNL group developed sepsis, with no cases observed in the VmPCNL group (p = 0.391) (Table 2).
Predictors of Postoperative SIRS
In the multivariable logistic regression analysis, VmPCNL was independently associated with a lower risk of postoperative SIRS (adjusted odds ratio [aOR] 0.44, 95% confidence interval [CI] 0.19–0.98, p = 0.041). A positive preoperative urine culture was also identified as an independent predictor of SIRS (aOR 2.60, 95% CI 1.01–6.60, p = 0.045). Operative time was not significantly associated with SIRS in the adjusted model (Table 3).
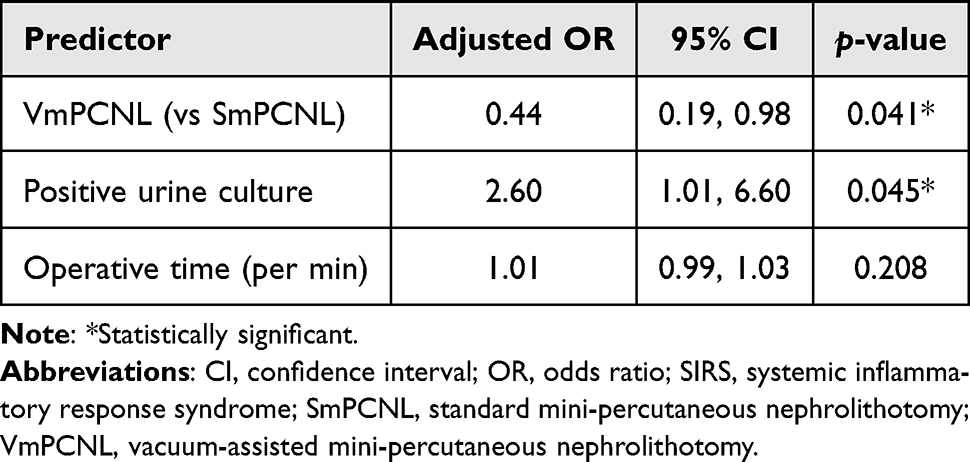 |
Table 3 Multivariable Logistic Regression Analysis for Postoperative SIRS |
Sensitivity Analysis
In the IPTW-adjusted analysis, baseline covariates were well balanced between the groups, with standardized mean differences < 0.1 for all variables (Supplementary Table S1 and Supplementary Figure S1). The weighted analysis confirmed the primary findings, with VmPCNL remaining associated with a lower risk of postoperative SIRS (weighted OR 0.46, 95% CI 0.22–0.96, p = 0.039). The direction and magnitude of the effect were consistent with the primary multivariable model.
Discussion
In this real-world cohort study, VmPCNL was associated with a significantly lower incidence of postoperative SIRS compared to SmPCNL, while maintaining comparable SFR. In addition, VmPCNL demonstrated superior perioperative efficiency, as reflected by shorter operative times and reduced LOS. Collectively, these findings suggest that the incorporation of active suction into the mini-PCNL workflow may offer meaningful clinical advantages in both the safety and efficiency domains.
The observed reduction in SIRS (8.6% vs 21.8%) is clinically meaningful and consistent with the growing body of literature highlighting the importance of IRP in the pathogenesis of infectious complications following endourological procedures. Previous studies have reported SIRS rates ranging from 15% to 35% after conventional PCNL, placing the outcomes of the SmPCNL group within the expected range, while the substantially lower rate observed in the VmPCNL group suggests a potential protective effect.17–20
Elevated IRP has been shown to promote pyelovenous and pyelolymphatic backflow, facilitating the systemic dissemination of bacteria and endotoxins.21,22 In standard mini-PCNL, the relatively small tract size may predispose to impaired outflow and transient IRP elevation. In contrast, the active suction mechanism in VmPCNL enables the continuous evacuation of irrigation fluid and stone debris and may contribute to maintaining a lower and more stable intrarenal pressure environment.23 Although IRP was not directly measured in this study, our findings are consistent with prior reports suggesting that improved outflow dynamics may reduce inflammatory morbidity.16
Despite the reduction in SIRS, the incidence of severe infectious complications, such as sepsis, remained low and comparable between the groups. This is consistent with prior reports demonstrating sepsis rates of approximately 0.3% to 4.7% following PCNL.5,24 The lack of statistical difference in this outcome is likely attributable to the relatively low event rate and limited statistical power inherent in single-center cohort studies. Nevertheless, SIRS remains a clinically relevant endpoint, as it represents an early stage in the inflammatory cascade that may progress to more severe complications and is associated with increased morbidity and healthcare utilization.25
The identification of a positive preoperative urine culture as an independent predictor of postoperative SIRS is in agreement with established evidence, which consistently highlights the role of preexisting urinary tract infection in increasing the risk of postoperative infectious complications.26,27 Importantly, VmPCNL remained independently associated with a lower risk of SIRS even after adjusting for baseline differences, suggesting that the optimization of intraoperative factors—particularly fluid outflow and pressure dynamics—may reduce procedural risk beyond standard preoperative measures. Patients with positive preoperative urine cultures may harbor occult bacterial colonization within the collecting system or stone matrix despite appropriate antimicrobial treatment, thereby predisposing them to postoperative inflammatory complications. This finding reinforces the importance of careful preoperative infection control and risk stratification in patients undergoing mini-PCNL.
In addition to its impact on infectious outcomes, VmPCNL demonstrated improved operative efficiency. The shorter operative time observed in the VmPCNL group is likely attributable to enhanced fragment clearance and improved endoscopic visualization facilitated by active suction. The suction-assisted access sheath may help mitigate the “snowstorm effect” caused by stone dust during high-power laser lithotripsy, thereby maintaining a clearer operative field.28–30 Furthermore, these findings may reflect a functional synergy between suction-assisted outflow and modern laser lithotripsy techniques, which together may improve procedural efficiency.31,32
From a clinical perspective, the reduction in SIRS and shorter LOS observed in the VmPCNL group may have important implications for patient outcomes and healthcare resource utilization. Although vacuum-assisted access sheaths are associated with additional device costs, these may be offset by reductions in postoperative complications and LOS and the need for intensive monitoring. In high-volume centers, strategies that enhance both procedural safety and efficiency are particularly valuable.
Several limitations of this study should be acknowledged. First, the retrospective single-center design introduced the potential for selection bias, although this was partially mitigated through multivariable adjustment and IPTW analysis. Second, all procedures were performed by a single experienced surgeon, which may limit the generalizability to other settings with different levels of expertise. In addition, because vacuum-assisted procedures were introduced later in the study period, a temporal or learning-curve effect could not be completely excluded. Third, the sample size and number of SIRS events were relatively limited, and the statistical power should therefore be interpreted cautiously. Fourth, intrarenal pressure was not directly measured; therefore, the proposed mechanism underlying the reduction in SIRS remains inferential. Finally, residual confounding from unmeasured variables could not be entirely excluded.
Notwithstanding these limitations, this study has several notable strengths. It reflects real-world clinical practice, includes a well-characterized cohort with comprehensive perioperative data, and demonstrates consistent findings across multiple clinically relevant outcomes. The integration of both clinical and mechanistic perspectives further enhances the robustness and interpretability of the results.
Future prospective studies incorporating real-time intrarenal pressure monitoring and randomized study designs are warranted to validate these findings and to further elucidate the physiological mechanisms underlying the benefits of vacuum-assisted techniques.
Conclusion
In this real-world cohort, VmPCNL was associated with a lower incidence of postoperative SIRS and improved perioperative efficiency compared with standard mini-PCNL, while maintaining comparable stone-free rates. These findings suggest that active suction may improve intraoperative outflow dynamics and reduce postoperative inflammatory morbidity. However, given that intrarenal pressure was not directly measured, prospective studies incorporating real-time pressure monitoring are warranted to confirm the proposed mechanism.
Acknowledgments
We would like to thank everyone involved in this study, including the Department of Clinical Epidemiology and Biostatistics, Faculty of Medicine, Ramathibodi Hospital, for their support in the statistical analysis.
Disclosure
The authors declare that they have no competing interests in this work.
References
1. Pearle MS, Matlaga BR, Antonelli JA, et al. Surgical management of kidney and ureteral stones: aua guideline. part ii: evaluation and treatment of patients with kidney and/or ureteral stones. J Urol. 2026;215(2):124–8. doi:10.1097/JU.0000000000004843
2. Pietropaolo A, Keller EX, Sener TE, et al. Economic burden of imaging and interventions in endourology: a worldwide cost analysis from european association of urology young academic urology endourology and urolithiasis working party. J Endourol. 2025;39(4):389–398. doi:10.1089/end.2024.0673
3. Ketsuwan C, Pimpanit N, Phengsalae Y, Leenanupunth C, Kongchareonsombat W, Sangkum P. Peri-operative factors affecting blood transfusion requirements during pcnl: a retrospective non-randomized study. Res Rep Urol. 12:279–285. 10.2147/RRU.S261888
4. Ketsuwan C, Phengsalae Y, Kijvikai K, et al. Endoscopic combined intrakidney surgery to remove a large renal calculus in a transplanted kidney: a case report. Transplant Proc. 2022;54(10):2705–2708. doi:10.1016/j.transproceed.2022.10.031
5. Korets R, Graversen JA, Kates M, Mues AC, Gupta M. Post-percutaneous nephrolithotomy systemic inflammatory response: a prospective analysis of preoperative urine, renal pelvic urine and stone cultures. J Urol. 2011;186(5):1899–1903. doi:10.1016/j.juro.2011.06.064
6. Seitz C, Desai M, Häcker A, et al. Incidence, prevention, and management of complications following percutaneous nephrolitholapaxy. Eur Urol. 2012;61(1):146–158. doi:10.1016/j.eururo.2011.09.016
7. Yu J, Guo B, Yu J, et al. Antibiotic prophylaxis in perioperative period of percutaneous nephrolithotomy: a systematic review and meta-analysis of comparative studies. World J Urol. 2020;38(7):1685–1700. doi:10.1007/s00345-019-02967-5
8. Hanessian K, Albaghli A, Crew R, et al. The effect of negative, single and multi-organism positive cultures on outcomes following PCNL. BJUI Compass. 2026;7(1):e70150. doi:10.1002/bco2.70150
9. Gauhar V, Castellani D, Kalathia J, et al. Prospective multicenter real-world outcomes of Suction Technology Utility in Mini-PCNL Study (STUMPS) in modern-day practice: formulation of the global STUMPS registry on behalf of the endourology section of the European Association of Urology and the suction mini-PCNL collaborative study group. World J Urol. 43(1):298.
10. Gauhar V, Yuen SK, Zawadzki M, et al. Utility of the Guy’s Stone Score on real world outcomes of suction mini-PCNL in 1527 adult patients with normal collecting system anatomy. A prospective multicenter study from the EAU section of endourology and asian urological society of endoluminal surgery and technology collaboration. Minerva Urol Nephrol.
11. Kayano S, Yanagisawa T, Shibata K, et al. Intrarenal pressure during the flexible and navigable suction ureteral access sheath-assisted retrograde intrarenal surgery: a two-center study. Int Urol Nephrol. 2025:1–7.
12. Tokas T, Herrmann TRW, Skolarikos A, Nagele U. Training and Research in Urological Surgery and Technology (T.R.U.S.T.)-Group. Pressure matters: intrarenal pressures during normal and pathological conditions, and impact of increased values to renal physiology. World J Urol. 2019;37(1):125–131. doi:10.1007/s00345-018-2378-4
13. Kritsing S, Udomsombatmeechai K, Prohsoontorn O, Sangnoppatham N, Ketsuwan C. Application of the direct in-scope suction technique in antegrade flexible ureteroscopic lithotripsy for the removal of a large ureteric calculus in a kidney transplant recipient: a case report. Urol Case Rep. 2024;53:102663. doi:10.1016/j.eucr.2024.102663
14. Jackman SV, Hedican SP, Peters CA, Docimo SG. Percutaneous nephrolithotomy in infants and preschool age children: experience with a new technique. Urology. 1998;52(4):697–701. doi:10.1016/S0090-4295(98)00315-X
15. Thampravit T, Phengsalae Y, Ketsuwan C. Tubeless mini-percutaneous nephrolithotomy to remove a staghorn stone concurrent with proximal ureteral calculus in an elderly patient: a case report. Urol Case Rep. 2023;47:102332. doi:10.1016/j.eucr.2023.102332
16. Lievore E, Boeri L, Zanetti SP, et al. Clinical comparison of mini-percutaneous nephrolithotomy with vacuum cleaner effect or with a vacuum-assisted access sheath: a single-center experience. J Endourol. 2021;35(5):601–608. doi:10.1089/end.2020.0555
17. Mariappan P, Smith G, Bariol SV, Moussa SA, Tolley DA. Stone and pelvic urine culture and sensitivity are better than bladder urine as predictors of urosepsis following percutaneous nephrolithotomy: a prospective clinical study. J Urol. 2005;173(5):1610–1614. doi:10.1097/01.ju.0000154350.78826.96
18. Zhu L, Wang Z, Zhou Y, Gou L, Huang Y, Zheng X. Comparison of vacuum-assisted sheaths and normal sheaths in minimally invasive percutaneous nephrolithotomy: a systematic review and meta-analysis. BMC Urol, 21 1 158 doi: 10.1186/s12894-021-00925-1.
19. Chen L, Xu QQ, Li JX, Xiong LL, Wang XF, Huang XB. Systemic inflammatory response syndrome after percutaneous nephrolithotomy: an assessment of risk factors. Int J Urol. 2008;15(12):1025–1028. doi:10.1111/j.1442-2042.2008.02170.x
20. Yuen SKK, Pek GXW, Herrmann T, et al. Propensity Score-Matched Analysis of 30-Day Outcomes of Suction Versus Nonsuction Mini Percutaneous Nephrolithotomy From a Real-World Multicenter Prospective Study: Collaboration Between the European Association of Urology Endourology Section and the Asian Urological Society of Endoluminal Surgery and Technology. Eur Urol Focus. 2025;19:S2405–4569.
21. Hong A, du Plessis J, Browne C, Jack G, Bolton D. Mechanism of urosepsis: relationship between intrarenal pressures and pyelovenous backflow. BJU Int. 2023;132(5):512–519. doi:10.1111/bju.16095
22. Srithongsongsaeng P, Sirisopana K, Piyawannarat S, et al. Vacuum-assisted mini-ECIRS for calyceal diverticular stones in a recipient of a kidney transplant: a case report. Urol Case Rep. 2025;61:103079. doi:10.1016/j.eucr.2025.103079
23. Qin P, Zhang D, Huang T, Fang L, Cheng Y. Comparison of mini percutaneous nephrolithotomy and standard percutaneous nephrolithotomy for renal stones >2cm: a systematic review and meta-analysis. Int Braz J Urol. 2022;48(4):637–648. doi:10.1590/s1677-5538.ibju.2021.0347
24. Mariappan P, Smith G, Moussa SA, Tolley DA. One week of ciprofloxacin before percutaneous nephrolithotomy significantly reduces upper tract infection and urosepsis: a prospective controlled study. BJU Int. 2006;98(5):1075–1079. doi:10.1111/j.1464-410X.2006.06450.x
25. Balk RA. Systemic inflammatory response syndrome (SIRS): where did it come from and is it still relevant today? Virulence. 2014;5(1):20–26. doi:10.4161/viru.27135
26. Osther PJS, Osther SS, Hesselholt MP, et al. Understanding intrarenal backflow: intrarenal pressure during ureteroscopy and beyond. Asian J Urol. 2024;11(2):139–142. doi:10.1016/j.ajur.2024.01.008
27. Margel D, Ehrlich Y, Brown N, Lask D, Livne PM, Lifshitz DA. Clinical implication of routine stone culture in percutaneous nephrolithotomy--a prospective study. Urology. 2006;67(1):26–29. doi:10.1016/j.urology.2005.08.008
28. Lai D, Chen M, Sheng M, et al. Use of a novel vacuum-assisted access sheath in minimally invasive percutaneous nephrolithotomy: a feasibility study. J Endourol. 2020;34(3):339–344. doi:10.1089/end.2019.0652
29. Mager R, Balzereit C, Gust K, et al. The hydrodynamic basis of the vacuum cleaner effect in continuous-flow PCNL instruments: an empiric approach and mathematical model. World J Urol. 2016;34(5):717–724. doi:10.1007/s00345-015-1682-5
30. Setthawong T, Namwongsa T, Ketsuwan C. Retrograde vacuum-assisted MiniPCNL system for large distal ureteric calculus removal: a case report. Urol Case Rep. 2023;51:102622. doi:10.1016/j.eucr.2023.102622
31. Traxer O, Corrales M. Managing urolithiasis with thulium fiber laser: updated real-life results-a systematic review. J Clin Med. 2021;10(15):3390. doi:10.3390/jcm10153390
32. Gauhar V, Traxer O, Fong KY, et al. Comparing thulium fiber versus high-power holmium laser lithotripsy combined with the flexible and navigable suction access sheath in flexible ureteroscopy for kidney stone disease: a propensity score matched analysis by the global fans collaborative group. J Endourol. 2025;39(1):42–49. doi:10.1089/end.2024.0653
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.