Back to Journals » Risk Management and Healthcare Policy » Volume 15
Vaccinated Healthcare Workers’ Adherence to COVID-19 Prevention Measures and Associated Factors in Northwest Ethiopia: A Facility-Based Cross-Sectional Study
Authors Gubae K, Agegnew Wondm S ![]() , Birhane W, Fetene A
, Birhane W, Fetene A ![]() , Arega Moges T
, Arega Moges T ![]() , Kiflu M
, Kiflu M ![]()
Received 4 September 2022
Accepted for publication 13 December 2022
Published 16 December 2022 Volume 2022:15 Pages 2389—2398
DOI https://doi.org/10.2147/RMHP.S388668
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jongwha Chang
Kale Gubae,1 Samuel Agegnew Wondm,1 Worku Birhane,1 Akalu Fetene,1 Tilaye Arega Moges,2 Mekdes Kiflu1
1Department of Pharmacy, College of Health Sciences, Debre Markos University, Debre Markos, Ethiopia; 2Department of Pharmacy, College of Health Sciences, Debre Tabor University, Debre Tabor, Ethiopia
Correspondence: Kale Gubae, Email [email protected]
Background: The initial response to coronavirus disease 2019 (COVID-19) was non-pharmaceutical interventions (NPIs). Long-term protection against severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection does not appear to be possible by either infection or vaccination. Thus, traditional herd immunity seems impossible. In addition to increasing vaccination rates, NPIs may be needed.
Methods: A facility-based cross-sectional study was conducted among vaccinated healthcare workers. The study took place from July 15 to August 15, 2022. A self-administered questionnaire was used for data collection. In a multivariable logistic regression model, a p-value of less than 0.05 was considered statistically significant.
Results: Four hundred eleven healthcare workers were included in the study. Sixty percent of participants were fully vaccinated. After vaccination, 10.2% of respondents reported infection with SARS-CoV-2. The study showed that 49.4% of participants had a good knowledge of the efficacy and safety of vaccines against SARS-CoV-2. In this study, 36% of individuals adhered well to the COVID-19 prevention strategies. Good knowledge of the efficacy and safety of SARS-CoV-2 vaccines (AOR = 1.69, 95% CI: 1.03– 2.78) increased the odds of implementing preventive measures. Healthcare workers who perceived a low and medium risk of SARS-CoV-2 infection after vaccination and who were knowledgeable about SARS-CoV-2 breakthrough infections were less likely to follow preventive measures.
Conclusion: The knowledge of healthcare workers regarding the efficacy and safety of vaccines against SARS-CoV-2 was comparable. However, a large proportion of healthcare workers poorly adhered to prevention practices. Therefore, to reduce the risk of SARS-CoV-2 infection among healthcare professionals, prevention strategies must be continuously evaluated and awareness of the need for preventive measures must be raised even after vaccination.
Keywords: prevention practices, vaccine, knowledge, Ethiopia
Introduction
In the absence of vaccines, non-pharmaceutical interventions (NPIs) were used to contain the 2019 coronavirus disease pandemic (COVID-19) in 2020. The combined implementation of NPIs was temporally linked to COVID-19 control.1 NPIs were also estimated to prevent nearly 3 million deaths from COVID-19 in 11 European countries.2
Currently, vaccines are the world’s leading COVID-19 mitigation method. They have shifted the pandemic’s direction. However, as infection does not appear to confer sustained protection against reinfection with severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), vaccination has not been successful either.3 Vaccine efficacy is also compromised by variants of SARS-CoV-2.4 Variants of SARS-CoV-2 can escape antibody binding and reduce vaccine efficacy.5 Thus, despite the clear public health benefits of COVID-19 vaccines, a vaccinated person is still at risk for infection or reinfection with SARS-CoV-2 and even the possibility of transmission of the infection.6 Such breakthrough infections are evidence of the real possibility of post-vaccination infections, the ineffectiveness of vaccines against circulating COVID-19 variants, and the need for continued protective measures after vaccination.
Therefore, a reconsideration of relying solely on immunization as the main strategy to mitigate COVID-19 and its adverse consequences has been proposed.7 Direct protection of individuals only through vaccination may not be sufficient. In this sense, NPIs may need to be introduced in addition to increasing vaccination rates. Such course corrections are critical to reducing the burden of COVID-19.3,8,9
Healthcare workers (HCWs) are the group most at risk for SARS-CoV-2 infection;10 therefore, their adherence to preventive measures requires evaluation for early intervention. The perception of being fully protected after vaccination could lead HCWs to be less cautious about SARS-CoV-2 transmission, which would further exacerbate the crisis.11 However, to our knowledge, behavioral changes in the use of COVID-19 prevention methods after vaccination have not been studied. In Ethiopia, adherence of HCWs to COVID-19 prevention methods before vaccination was low.12,13 To our knowledge, adherence of vaccinated HCWs to COVID-19 prevention interventions has not been studied in Ethiopia. Therefore, this study will serve as a baseline for further studies. The study will provide information on intervention areas that should be explored by policy makers. The aim of the study was to determine how well healthcare workers adhere to COVID-19 prevention interventions after vaccination.
Methods and Materials
Study Design and Duration
We conducted a health facility-based cross-sectional study among vaccinated healthcare workers. The study took place from July 15 to August 15, 2022.
Study Setting
We conducted the study in five specialized hospitals in Northwestern Ethiopia. The comprehensive specialized hospitals in Northwestern Ethiopia were University of Gondar Comprehensive Specialized Hospital (UoGCSH), Debre Markos Comprehensive Specialized Hospital (DMCSH), Debre Tabor Comprehensive Specialized Hospital (DTCSH), Tibebe Gion Comprehensive Specialized Hospital (TGCSH), and Felege Hiwot Comprehensive Specialized Hospital (FHCSH).
Population
All healthcare workers living in Northwestern Ethiopia during the data collection period were the source population. The study population included all participants who had been vaccinated (at least once), were over 18 years of age, and had completed and submitted the questionnaire.
Sample Size and Sampling Technique
The following statistical assumptions were used to determine the sample size using a single population proportion formula. A confidence level (CI) of 95%, a standard error (d) of 5%, and a proportion (p) of 50% were assumed. Assuming a non-response rate of 10%, the final sample size was 424.
Study Variables
Dependent Variable
Adherence to COVID-19 prevention methods after vaccination.
Independent Variables
The independent variables were socio-demographic characteristics, health status, COVID-19 experience-related items, and COVID-19 vaccine efficacy and safety-related items.
Data Collection Procedure
A self-administered questionnaire was used for data collection. The questionnaire was written in English. The introductory part of the questionnaire included: the purpose of the study, the voluntary nature of participation, informed consent with a statement of anonymity, and the response procedure. We adapted the instrument we used to measure adherence, health status, COVID-19 experience, and perceived risk from the previous studies.13–16 COVID-19 vaccine efficacy and safety-related items were based on current evidence.3,8,17–25 The instrument included the following categories: socio-demographic characteristics, health status, and COVID-19 experience-related items, COVID-19 vaccine efficacy and safety-related items, and adherence to COVID-19 preventive measures. Adherence to 10 prevention measures was measured. If an individual answered “yes” to the median and one higher value of the composite variable, adherence to the COVID-19 prevention measures was considered good. We determined vaccination status based on the healthcare workers’ responses to the type and number of vaccine doses administered. They were considered fully vaccinated if they had received two doses of AstraZeneca vaccine, two doses of Pfizer-BioNTech vaccine, or a single dose of Johnson and Johnson (J & J) vaccine; otherwise, they were considered partially vaccinated. To determine the timing of infection, participants were also asked about the type and number of vaccine doses received. In this way, it was possible to determine whether infection occurred after full or partial vaccination. Knowledge of vaccine efficacy and safety was measured by three responses: agree, disagree, and not sure. In the analysis, disagreement and uncertainty were coded as “no”, whereas agreement was coded as “yes”. Participants who responded with intermediate and higher scores were classified as good knowledge, and otherwise poor knowledge.
Data Analysis
We analyzed data using SPSS version 26. Descriptive analysis was used to estimate different variables, such as frequency, percentage, and mean. A binary logistic regression model was used for the identification of factors associated with adherence to COVID-19 prevention measures. In bivariate analyses, all variables with a P-value of < 0.05 were included in the final multivariate analysis. The odds ratio and 95% CI were used to verify the presence and strength of the relationship between independent variables and the result variable. In the multivariable analysis, variables having a P-value of < 0.05 were declared to have a statistically significant correlation with adherence to COVID-19 preventive measures.
Ethical Approval
We obtained ethical approval with reference number (Ref. No 708/15) from Debre Tabor University, College of Medicine and Health Science ethical review board. This study was conducted in accordance with the Declaration of Helsinki. Privacy and confidentiality were maintained during data collection. To ensure privacy and confidentiality, the information collected was not directly linked to the respective participants; participants’ names were not used. Codes were used as identifiers. Participants were informed of the purpose of the study and had the option to withdraw from participation at any time. Written informed consent was obtained from all participants.
Result
Socio-Demographic Characteristics of Participants
Four hundred eleven participants were included in the study, with a response rate of 97%. The mean age of the study participants was 29 years ± (range 21–52). Most participants (52.6%) were in the 25–29 years age group. More than half (56.4%) of the participants were female. Most of the respondents (61.3%) were single. The socio-demographic details of the study participants are shown in Table 1.
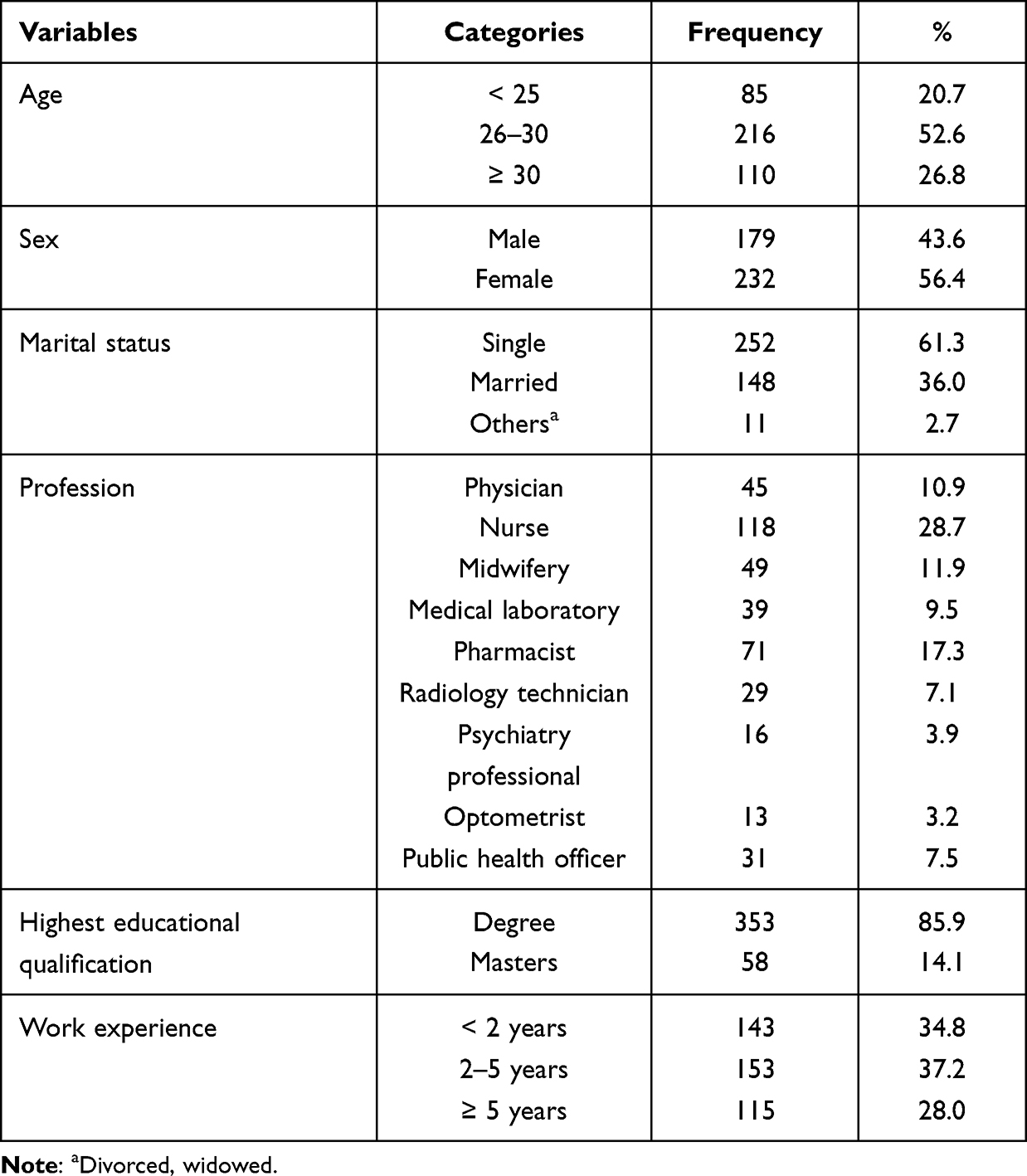 |
Table 1 Socio-Demographic Characteristics of the Study Participants, 2022 (n=411) |
Health Status and COVID-19 Experience of Healthcare Workers
A small number (12.7%) of HCWs had a history of chronic disease. Half of the participants reported a medium level of risk of infection with SARS-CoV-2 after vaccination. Most of the HCWs (60%) were fully vaccinated. Ten percent of HCWs reported infection with SARS-CoV-2 after receiving any of the COVID-19 vaccines. Of these, 24 (57.1%) occurred after partial vaccination, while 18 (42.9%) occurred after full vaccination. Details are presented in Table 2.
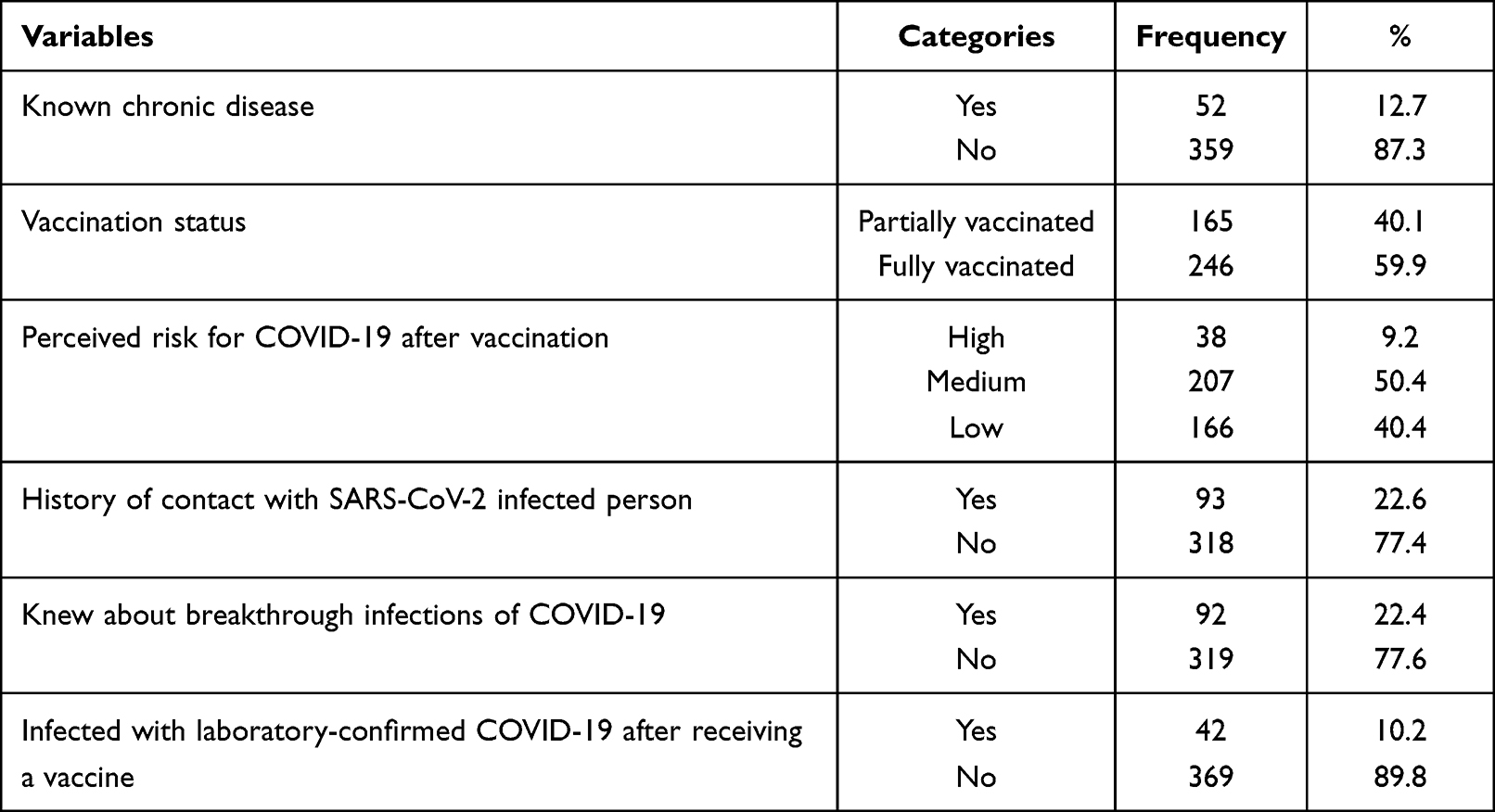 |
Table 2 Health Status, Vaccination Status, and COVID-19 Experience of the Study Participants, 2022 (n=411) |
Knowledge of Healthcare Workers About Vaccine Efficacy, Safety, and Source of Information
The study showed that 49.4% of health professionals had a good knowledge of the efficacy and safety of vaccines against SARS-CoV-2 (Table 3). More than one-third of the study participants (34.5%) reported the Ethiopian Ministry of Health/Ethiopian Public Health Institute (EPHI) as their main source of information. Table 4 provides specifics.
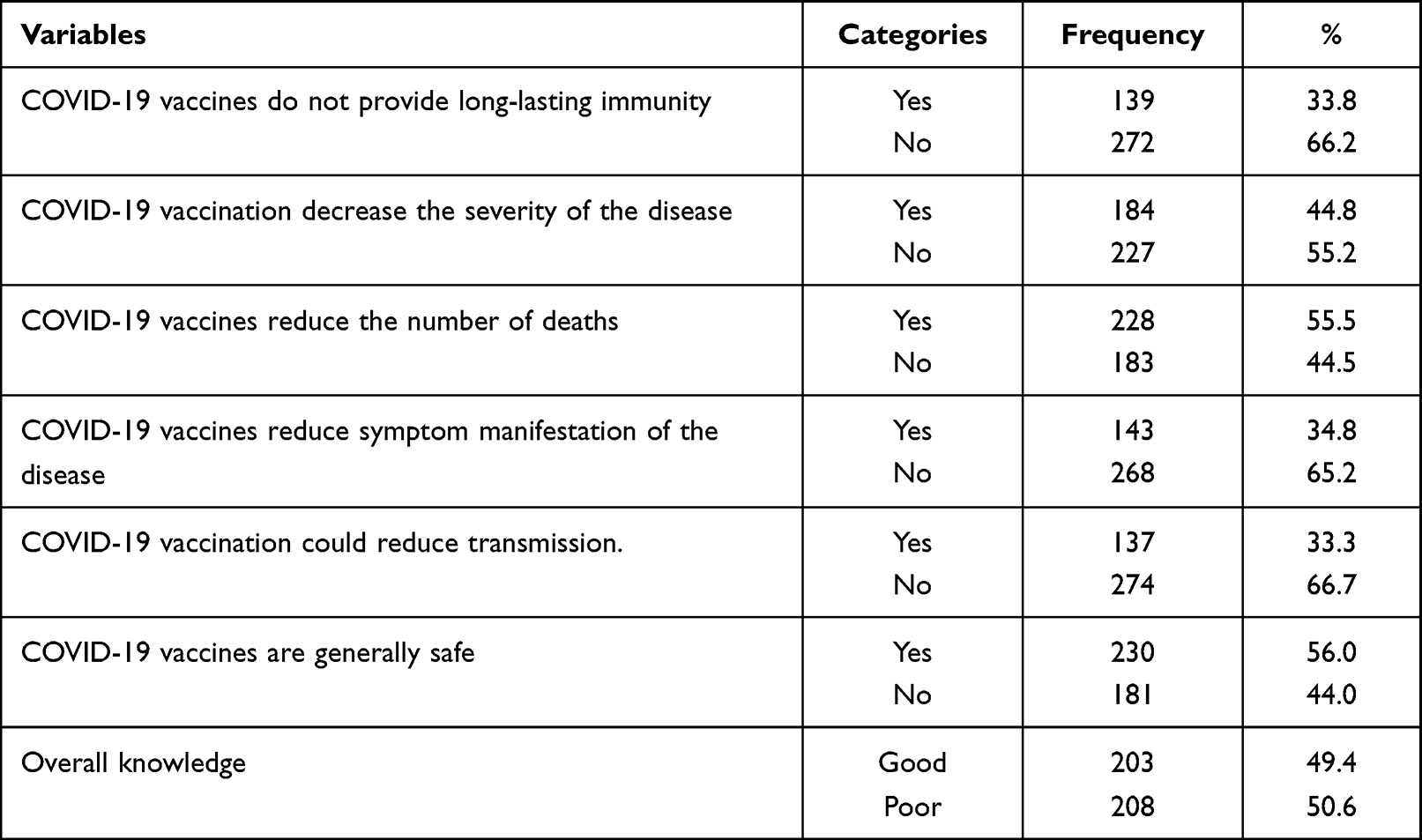 |
Table 3 Knowledge of the Respondents About Vaccine Efficacy and Safety, 2022 (n=411) |
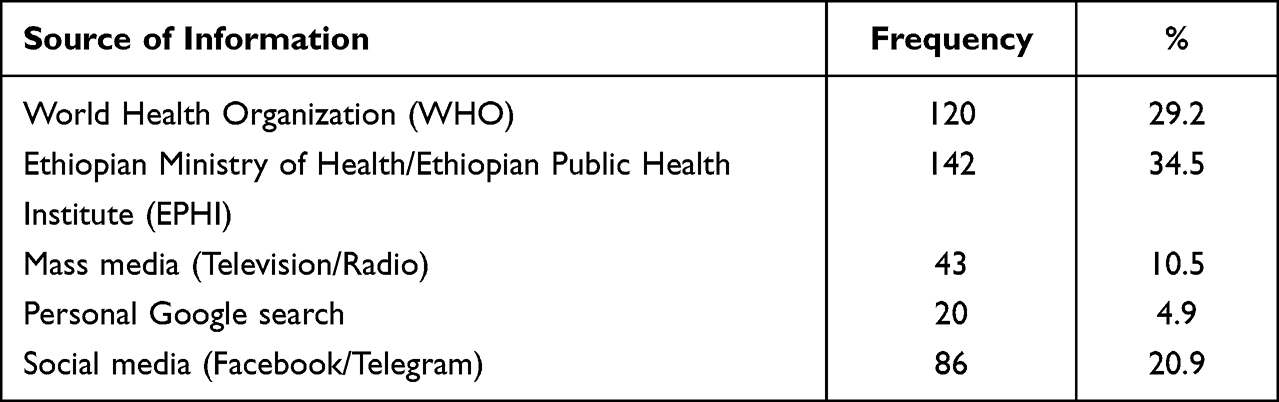 |
Table 4 Sources of Information on Preventive Practices and COVID-19 Vaccines of Participants, 2022 (n=411) |
Adherence of HCWs to COVID-19 Prevention Measures
We found that 36% of individuals adhered well to the COVID-19 prevention strategies. Healthcare workers were most likely to use alcohol-based hand sanitizers (65.7%) and wear masks (62.5%) as preventive measures. In contrast, maintaining a minimum distance of 2 meters (33.8%), regularly cleaning and disinfecting frequently touched objects (33%), and avoiding large crowds (37.7%) were least practiced (Table 5).
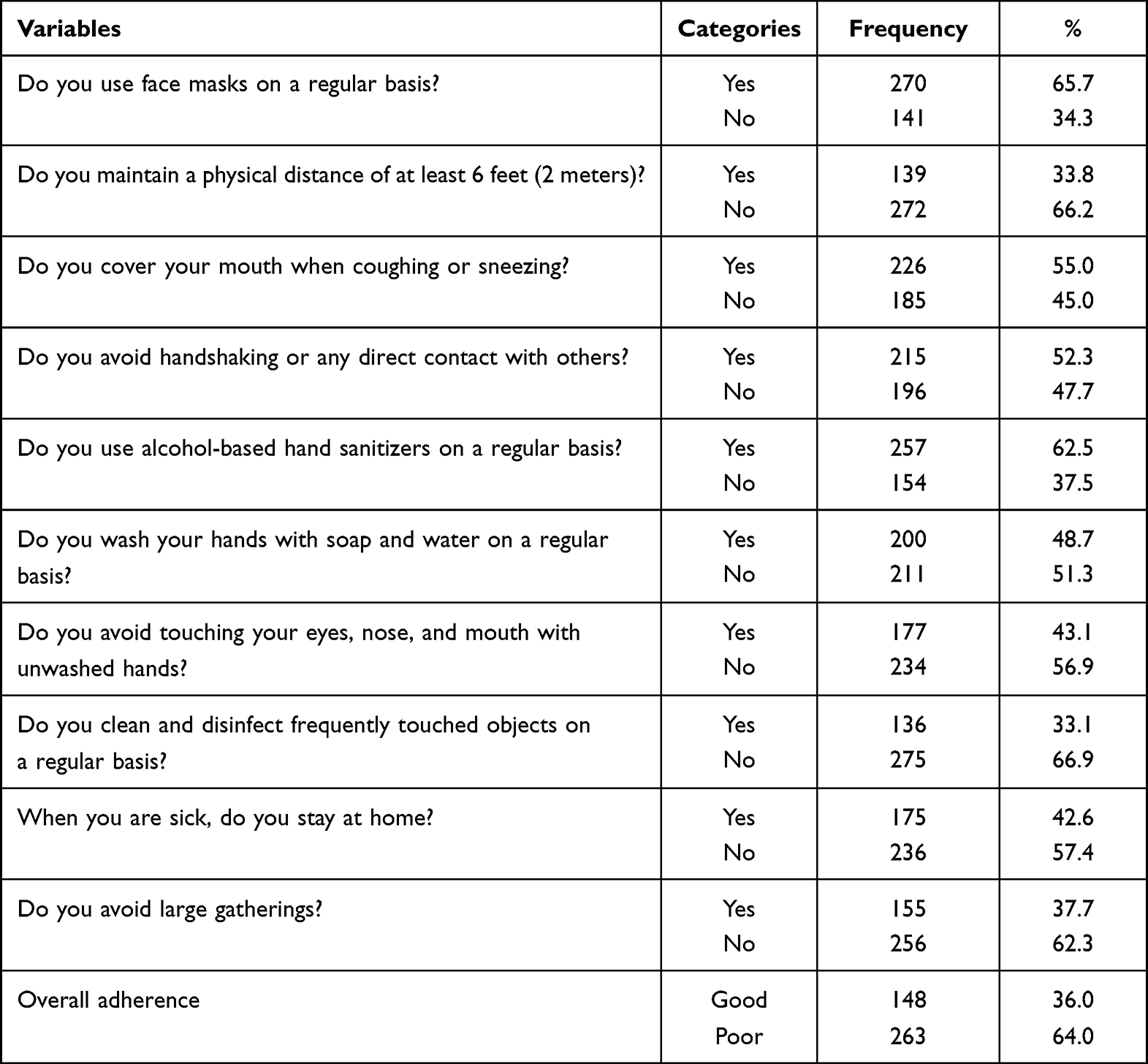 |
Table 5 Adherence of Study Participants to COVID-19 Prevention Measures, 2022 (n=411) |
Factors Associated with Adherence to COVID-19 Prevention Measures
Binary logistic regression was used to assess the relationship between the independent variables and adherence to the COVID-19 preventive measures. In bivariate analysis, age, work experience, known chronic disease, perceived risk for COVID-19 after vaccination, knowledge of breakthrough infections of COVID-19, history of contact with SARS-CoV-2 infected persons, infection with laboratory-confirmed COVID-19 after vaccination, and knowledge of vaccine efficacy and safety were candidates for multivariate analysis. Given the independent variables, the full model explained between 22% (Cox and Snell R Square) and 30% (Nagelkerke R Square) of the variation in the dependent variable and correctly classified 64% of the cases. The model has statistically significant predictive power (X2 (11, N = 411) = 101.9, p < 0.001). The model also has a good fit, as Hosmer and Lemeshow’s goodness-of-fit test yielded a p value of 0.702.
Perceived risk for COVID-19 after vaccination, knowledge of COVID-19 breakthrough infections, and knowledge of vaccine efficacy and safety were the statistically significant independent variables associated with adherence to COVID-19 preventive measures in multivariate analysis. Respondents who perceived a low risk of infection with SARS-CoV-2 after vaccination were 93% less likely (AOR = 0.07, 95% CI: 0.02–0.20) to have good adherence, whereas respondents with a perceived medium level of infection risk were 86% less likely (AOR = 0.14, 95% CI: 0.05–0.38) to have good adherence to COVID-19 preventive measures than respondents with a perceived high risk of infection.
The odds of good adherence to COVID-19 prevention measures in participants who knew about SARS-CoV-2 breakthrough infections were reduced by 52% (AOR = 0.48, 95% CI: 0.26–0.86) compared to those who did not know about SARS-CoV-2 breakthrough infections.
Healthcare workers who had good knowledge regarding the efficacy and safety of vaccines against SARS-CoV-2 were 1.69 times (AOR = 1.69, 95% CI: 1.03–2.78) more likely to have good adherence to COVID-19 prevention practices than those who had poor knowledge (Table 6).
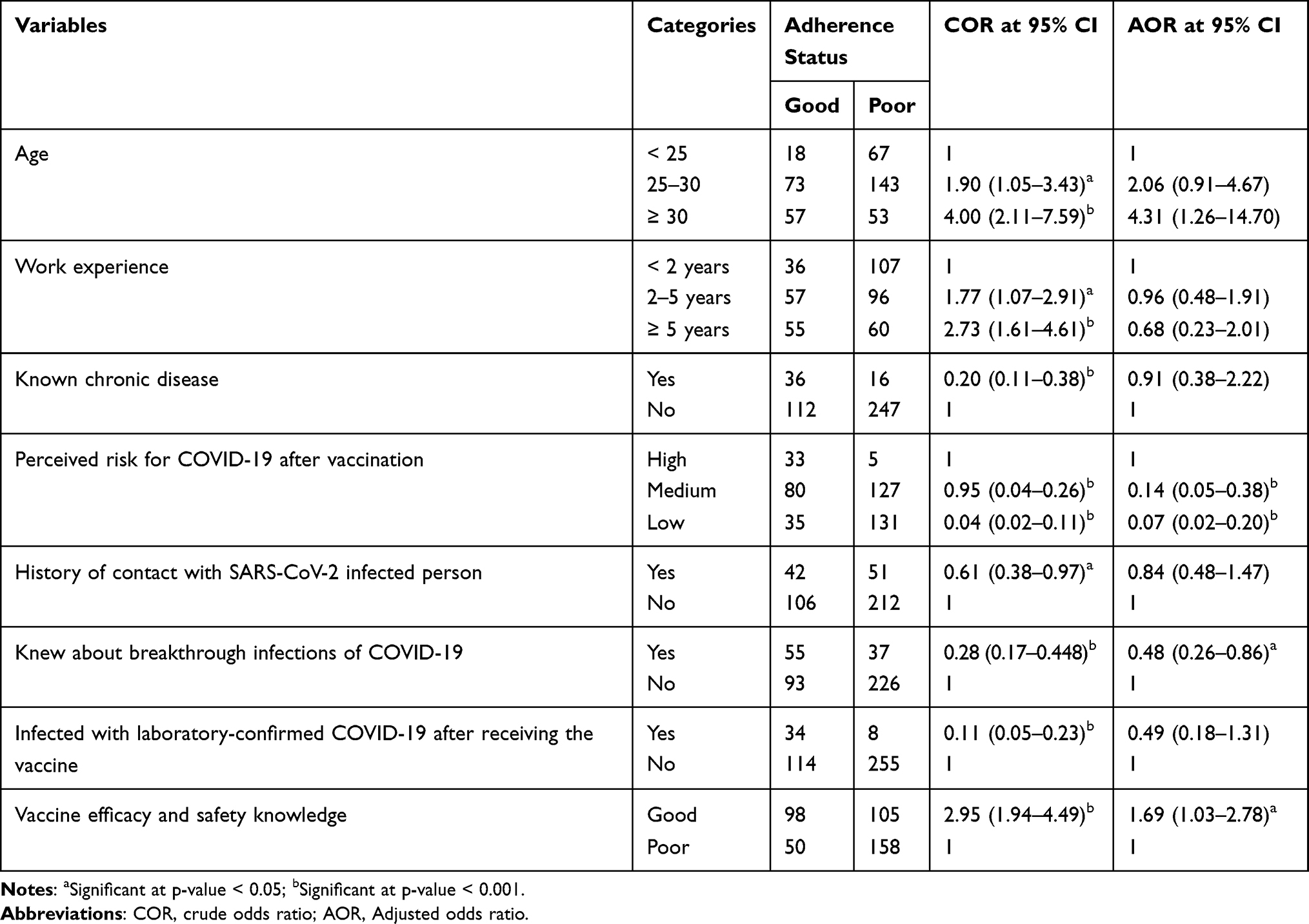 |
Table 6 Factors Associated with Adherence to COVID-19 Prevention Measures, 2022 (n=411) |
Discussion
This study examined medical personnel’s adherence to COVID-19 preventive measures after vaccination. Results showed that most health professionals had poor adherence to COVID-19 preventive measures.
This low level of adherence could be explained by vaccination and the decrease in new COVID-19 cases. Indeed, these two ideas led the Ethiopian government to issue a directive on March 13, 2022, to relax public prevention practices.26 Nevertheless, prevention measures should continue to be used in public and private organizations by both staff and clients. Similar poor results in adherence to prevention measures were found in other studies in Ethiopia12,13 before the introduction of vaccination on March 13, 2021, and in Nigeria.27 This indicates that other factors besides vaccination and the decrease in new cases COVID-19 play a role in health workers’ adherence to prevention strategies. On the contrary, high levels of good adherence have been observed in other studies.14,15,28
Differences can be attributed to, among other factors, the educational background of the participants,15 the timing of the studies, as evidenced by the sharp decline in prevention practices from 89.7% to 38% within six months,12 professional experience,28 health professionals’ knowledge of COVID-19,29 and differences in sample size and study population.
However, in studies in which overall adherence was either poor or good, the most commonly practiced items were similar. Except in one study where face mask use was the least practiced,29 hand washing, the use of alcohol-based sanitizers, and the use of face masks were the most frequently practiced elements. This is consistent with our finding that face masks and alcohol-based hand sanitizers were the most commonly used precautions. The most commonly used precautions appear to be similar before and after vaccination.
Clinical trials and real-world data demonstrate the efficacy and acceptable safety of vaccines against SARS-CoV-2. Vaccination reduces hospitalizations and deaths after infection;19,21,24 the manifestation of symptoms;18,21 and the severity of illness.19,23,25 Vaccination also reduces the risk of infectiousness.8,17,20 Indeed, increasing the number of vaccinated individuals reduces the risk of significant community-wide transmission. This reduces the risk of emergence of new variants that could bypass the immunity induced by vaccination.30 However, they do not provide long-lasting immunity. This has led to infections after full vaccination.3,22
In our study, HCWs’ overall knowledge of the above COVID-19 vaccine efficacy and safety-related evidence was comparable, with good knowledge being positively associated with adherence to prevention practices after vaccination. However, most healthcare workers indicated that COVID-19 vaccines confer long-term immunity. This may have led healthcare workers to believe they were fully protected. This is supported by the finding that almost all participants perceived low or moderate levels of infection after vaccination. This is also supported by the negative association of awareness of COVID-19 breakthrough infections with good adherence, which may be due to awareness of the rarity of breakthrough infections.25,31,32
Currently, the main strategy against SARS-CoV-2 is vaccination. However, the fight against COVID-19 is complicated by the nature of the virus, the SARS-CoV-2 variants, the effectiveness of vaccines against the different variants, the effectiveness of vaccines in providing long-term immunity or preventing breakthrough infections, and the public’s reluctance to vaccinate and take preventive measures. In addition, people who have been vaccinated may change their behavior and be less concerned about SARS-CoV-2 transmission because they believe they are fully protected.11 This is supported by the low adherence of most HCWs in this study. However, it is important to consider the possibility that medical personnel are at higher risk of contracting SARS-CoV-2 even after vaccination. Therefore, there is still a need for more effective behavior change methods to encourage professionals to adhere to important health measures.
Conclusion
Adherence to prevention practices for COVID-19 by healthcare workers was poor. Statistically significant poor prevention practices were found among participants with low vaccine knowledge, low or moderate perceived risk of post-vaccination SARS-CoV-2 infection, and knowledge of COVID-19 breakthrough infections. Behavioral changes in healthcare workers due to vaccination may pose a risk in the fight against COVID-19. Therefore, ongoing evaluation of prevention practices is needed to reduce the risk of infection to healthcare workers and the general public.
Limitations of the Study
The results presented in this study are self-reported and depend in part on the honesty of the participants and may be biased by recall. Only health workers working in government health facilities were included in the study. This may limit the external validity of the research findings. The study also has the limitations of a cross-sectional study in establishing cause-effect relationships. However, the study is the first to assess adherence to COVID-19 prevention strategies by vaccinated healthcare workers. The study also used reliable measurement methods, and included a sufficient number of individuals in the sample.
Data Sharing Statement
The raw data supporting the conclusions of this article will be made available by the corresponding author to any qualified researcher without undue reservation.
Acknowledgments
The authors acknowledge Debre Tabor University and the study participants.
Disclosure
The authors declare no conflicts of interest.
References
1. Pan A, Liu L, Wang C, et al. Association of public health interventions with the epidemiology of the COVID-19 outbreak in Wuhan, China. JAMA. 2020;323(19):1915–1923. doi:10.1001/jama.2020.6130
2. Flaxman S, Mishra S, Gandy A, et al. Estimating the effects of non-pharmaceutical interventions on COVID-19 in Europe. Nature. 2020;584(7820):257–261. doi:10.1038/s41586-020-2405-7
3. Morens DM, Folkers GK, Fauci AS. The Concept of Classical Herd Immunity May Not Apply to COVID-19. J Infect Dis. 2022;226(2):195–198. doi:10.1093/infdis/jiac109
4. Lopez Bernal J, Andrews N, Gower C, et al. Effectiveness of Covid-19 vaccines against the B.1.617.2 (Delta) variant. N Engl J Med. 2021;385(7):585–594. doi:10.1056/nejmoa2108891
5. Madhi SA, Baillie V, Cutland CL, et al. Efficacy of the ChAdOx1 nCoV-19 Covid-19 vaccine against the B.1.351 variant. N Engl J Med. 2021;384(20):1885–1898. doi:10.1056/nejmoa2102214
6. Hacisuleyman E, Hale C, Saito Y, et al. Vaccine Breakthrough Infections with SARS-CoV-2 Variants. N Engl J Med. 2021;384(23):2212–2218. doi:10.1056/nejmoa2105000
7. Subramanian SV, Kumar A. Increases in COVID-19 are unrelated to levels of vaccination across 68 countries and 2947 counties in the United States. Eur J Epidemiol. 2021;36(12):1237–1240. doi:10.1007/s10654-021-00808-7
8. Singanayagam A, Hakki S, Dunning J, et al. Community transmission and viral load kinetics of the SARS-CoV-2 delta (B.1.617.2) variant in vaccinated and unvaccinated individuals in the UK: a prospective, longitudinal, cohort study. Lancet Infect Dis. 2022;22(2):183–195. doi:10.1016/S1473-3099(21)00648-4
9. Moore S, Hill EM, Tildesley MJ, Dyson L, Keeling MJ. Vaccination and non-pharmaceutical interventions for COVID-19: a mathematical modelling study. Lancet Infect Dis. 2021;21(6):793–802. doi:10.1016/S1473-3099(21)00143-2
10. Martischang R, Iten A, Arm I, et al. Severe acute respiratory coronavirus virus 2 (SARS-CoV-2) seroconversion and occupational exposure of employees at a Swiss University Hospital: a large longitudinal cohort study. Infect Control Hosp Epidemiol. 2022;43(3):326–333. doi:10.1017/ice.2021.117
11. Vilches TN, Sah P, Abdollahi E, Moghadas SM, Galvani AP. Importance of non-pharmaceutical interventions in the COVID-19 vaccination era: a case study of the Seychelles. J Glob Health. 2021;11:03104. doi:10.7189/jogh.11.03104
12. Gebremedhin T, Abebe H, Wondimu W, Gizaw AT. COVID-19 prevention practices and associated factors among frontline community health workers in Jimma zone, Southwest Ethiopia. J Multidiscip Healthc. 2021;14:2239–2247. doi:10.2147/JMDH.S327293
13. Kassie BA, Adane A, Kassahun EA, Ayele AS, Belew AK. Poor COVID-19 preventive practice among healthcare workers in Northwest Ethiopia, 2020. Adv Public Heal. 2020;2020. doi:10.1155/2020/7526037
14. Gebremeskel TG, Kiros K, Gesesew HA, Ward PR. Assessment of knowledge and practices toward COVID-19 prevention among healthcare workers in Tigray, North Ethiopia. Front Public Heal. 2021;9:1–9. doi:10.3389/fpubh.2021.614321
15. Asemahagn MA. Factors determining the knowledge and prevention practice of healthcare workers towards COVID-19 in Amhara region, Ethiopia: a cross-sectional survey. Trop Med Health. 2020;48(1). doi:10.1186/s41182-020-00254-3
16. Ahmed MH, Siraj SS, Klein J, Ali FY, Kanfe SG. Knowledge and attitude towards second covid-19 vaccine dose among health professionals working at public health facilities in a low income country. Infect Drug Resist. 2021;14:3125–3134. doi:10.2147/IDR.S327954
17. Shah ASV, Gribben C, Bishop J, et al. Effect of vaccination on transmission of SARS-CoV-2. N Engl J Med. 2021;385(18):1718–1720. doi:10.1056/nejmc2106757
18. Khoury J, Najjar-Debbiny R, Hanna A, et al. COVID-19 vaccine – long term immune decline and breakthrough infections. Vaccine. 2021;39(48):6984–6989. doi:10.1016/j.vaccine.2021.10.038
19. Bernal JL, Andrews N, Gower C, et al. Effectiveness of the Pfizer-BioNTech and Oxford-AstraZeneca vaccines on covid-19 related symptoms, hospital admissions, and mortality in older adults in England: test negative case-control study. BMJ. 2021:373. doi:10.1136/bmj.n1088
20. Lyngse F, Mølbak K, Franck KT, et al. Association between SARS-CoV-2 transmissibility, viral load, and age in households. medRxiv. 2021. doi:10.1101/2021.02.28.21252608
21. Antonelli M, Penfold RS, Merino J, et al. Risk factors and disease profile of post-vaccination SARS-CoV-2 infection in UK users of the COVID Symptom Study app: a prospective, community-based, nested, case-control study. Lancet Infect Dis. 2022;22(1):43–55. doi:10.1016/S1473-3099(21)00460-6
22. Bergwerk M, Gonen T, Lustig Y, et al. Covid-19 breakthrough infections in vaccinated health care workers. N Engl J Med. 2021;385(16):1474–1484. doi:10.1056/nejmoa2109072
23. Bernal JL, Andrews N, Gower C, et al. Early effectiveness of COVID-19 vaccination with BNT162b2 mRNA vaccine and ChAdOx1 adenovirus vector vaccine on symptomatic disease, hospitalisations and mortality in older adults in England. medRxiv. 2021. doi:10.1101/2021.03.01.21252652
24. Christie A, Henley SJ, Mattocks L, et al. Decreases in COVID-19 cases, emergency department visits, hospital admissions, and deaths among older adults following the introduction of COVID-19 vaccine — United States, September 6, 2020-May 1, 2021. MMWR Recomm Rep. 2021;70(23):858–864. doi:10.15585/mmwr.mm7023e2
25. Polack FP, Thomas SJ, Kitchin N, et al. Safety and Efficacy of the BNT162b2 mRNA Covid-19 Vaccine. N Engl J Med. 2020;383(27):2603–2615. doi:10.1056/nejmoa2034577
26. Ethiopian Public Health Institution. Revised directive to provide for the prevention and control of the COVID-19 pandemic; 2022.
27. Iyal H, Ishaku S, Zakari A, et al. Knowledge and practice of Kaduna State Health Care providers on infection prevention and control during COVID-19 pandemic. Jmbsr. 2021;1(1):27–41. doi:10.46912/jmbsr.xx
28. Birihane BM, Bayih WA, Alemu AY, Belay DM. Perceived barriers and preventive measures of COVID-19 among healthcare providers in debretabor, north central Ethiopia, 2020. Risk Manag Healthc Policy. 2020;13:2699–2706. doi:10.2147/RMHP.S287772
29. Girma S, Alenko A, Agenagnew L. Knowledge and precautionary behavioral practice toward covid-19 among health professionals working in public university hospitals in Ethiopia: a web-based survey. Risk Manag Healthc Policy. 2020;13:1327–1334. doi:10.2147/RMHP.S267261
30. Christie A, Brooks JT, Hicks LA, Sauber-Schatz EK, Yoder JS, Honein MA. Guidance for implementing COVID-19 prevention strategies in the context of varying community transmission levels and vaccination coverage. MMWR Recomm Rep. 2021;70(30):1044–1047. doi:10.15585/mmwr.mm7030e2
31. Keehner J, Horton LE, Pfeffer MA, et al. SARS-CoV-2 Infection after vaccination in health care workers in California. N Engl J Med. 2021;384(18):1774–1775. doi:10.1056/nejmc2101927
32. Haas EJ, Angulo FJ, McLaughlin JM, et al. Impact and effectiveness of mRNA BNT162b2 vaccine against SARS-CoV-2 infections and COVID-19 cases, hospitalisations, and deaths following a nationwide vaccination campaign in Israel: an observational study using national surveillance data. Lancet. 2021;397(10287):1819–1829. doi:10.1016/S0140-6736(21)00947-8
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Willingness to receive the COVID-19 vaccine and associated factors among residents of Southwestern Ethiopia: A cross-sectional study
Jabessa D, Bekele F
Patient Preference and Adherence 2022, 16:1177-1185
Published Date: 3 May 2022
Health-care Workers’ Willingness to Pay for COVID-19 Vaccines in Eastern Ethiopia: Using Contingent Valuation Method
Merga BT, Ayana GM, Negash B, Alemu A, Abdurke M, Abdu A, Balis B, Bekana M, Fekadu G, Raru TB
ClinicoEconomics and Outcomes Research 2022, 14:395-404
Published Date: 19 May 2022
Prevalence and Determinants of COVID-19 Vaccine Hesitancy Among the Ethiopian Population: A Systematic Review
Yehualashet DE, Seboka BT, Tesfa GA, Mamo TT, Yawo MN, Hailegebreal S
Risk Management and Healthcare Policy 2022, 15:1433-1445
Published Date: 29 July 2022
COVID-19 Vaccine Acceptance and Associated Factors Among College Students in Dessie City, Northeastern Ethiopia
Berihun G, Walle Z, Teshome D, Berhanu L, Derso M
Journal of Multidisciplinary Healthcare 2022, 15:1735-1746
Published Date: 13 August 2022
Assessing the Knowledge, Attitudes, and Vaccination Practices Towards COVID-19 Vaccination Among Mainland Chinese Nursing Students and Interns: A Multicenter Cross-Sectional Study

Qin Z, Ye X, Liu H, Tao Y, Zheng X, Zhong Y, Chen D, Ye W, Zhan C
Infection and Drug Resistance 2023, 16:4717-4728
Published Date: 20 July 2023