Back to Journals » Pediatric Health, Medicine and Therapeutics » Volume 15
Utilizing T-Lymphocyte Activation-Related Cytokines to Predict Non-Responsiveness to Treatment in Pediatric Kawasaki Disease
Received 19 September 2024
Accepted for publication 11 December 2024
Published 17 December 2024 Volume 2024:15 Pages 375—383
DOI https://doi.org/10.2147/PHMT.S489512
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Roosy Aulakh
Bei Ye,1 Jiying Xiao,2 Caiyun Zhang3
1Department of Pediatrics, Hangzhou Children’s Hospital, Hangzhou, Zhejiang, People’s Republic of China; 2Department of Respiratory Medicine, Hangzhou Children’s Hospital, Hangzhou, Zhejiang, People’s Republic of China; 3Department of Pediatric Intensive Care Unit, Hangzhou Children’s Hospital, Hangzhou, Zhejiang, People’s Republic of China
Correspondence: Caiyun Zhang, Department of Pediatric Intensive Care Unit, Hangzhou Children’s Hospital, Hangzhou, Zhejiang, People’s Republic of China, Email [email protected]
Objective: To investigate the predictive value of T-lymphocyte activation-related cytokines in non-responsive Kawasaki disease.
Methods: Eighty-two children with Kawasaki disease, hospitalized from June 2022 to December 2023, were divided into two groups based on treatment response: the sensitive Kawasaki disease group (n=71) and the non-responsive Kawasaki disease group (n=11). Serum levels of T-lymph activation-related cytokines, including interleukin-2, 6, 7, 12, 15, 17, and tumor necrosis factor alpha, were measured before and after IVIG treatment in both groups. The differences in cytokine levels between the two groups were compared pre- and post-treatment. The ability of these cytokines to discriminate non-responsive Kawasaki disease was evaluated using ROC curves to determine the cut-off value.
Results: Before initial treatment, IL-2, IL-6, IL-7, IL-12, IL-15, IL-17, and tumor necrosis factor-α values were significantly higher in the non-responsive Kawasaki disease group compared to the sensitive Kawasaki disease group. Comparisons before and after initial treatment showed significant decreases in IL-6 and 17 in the sensitive Kawasaki disease group and significant decreases in IL-6 and 7 in the non-responsive Kawasaki disease group. IL-6 and 17 significantly increased in the sensitive group compared to the non-responsive group after initial treatment. The ROC curves indicated that IL-6 predicted the area under the curve (AUC) for non-responsive Kawasaki disease to be 0.859 before treatment and 0.920 after treatment. Similarly, IL-17 had AUC values of 0.699 before treatment and 0.884 after treatment.
Conclusion: Reassessing IL-6 and IL-17 following the initial treatment for Kawasaki disease may improve early warning signals for unresponsive Kawasaki disease.
Keywords: Kawasaki disease, unresponsive Kawasaki disease, cytokines, T-lymphocyte activation, immunoglobulin
Graphical Abstract:

Introduction
Kawasaki disease (KD) is an acute systemic vasculitis that presents in early childhood. Its most significant complication is coronary artery aneurysm (CAA), which can cause myocardial ischemia or acute coronary syndromes. KD has become the leading cause of acquired heart disease in most developed countries and regions.1,2 The standard treatment for KD is a single injection of intravenous immunoglobulin (IVIG) 2 g/kg and aspirin. However, approximately 10%~20% of children do not respond to IVIG and require additional IVIG therapy and/or other treatments. These patients are categorized as having immunoglobulin-unresponsive KD. Immunoglobulin-unresponsive KD is a high-risk factor for CAA.3–6 The lack of response to IVIG may indicate severe underlying inflammation.7 Additionally, more severe complications of the hyperinflammatory state, such as KD shock syndrome (KDSS) or KD combined with macrophage activation syndrome (MAS), may occur,8–10 endangering children’s lives. Non-responsive KD (also known as refractory KD) is a challenging problem for clinicians. It requires secondary treatment after standard therapy, and early recognition is crucial for initiating IVIG and additional treatments. Predicting IVIG resistance is key to enhancing initial therapy and preventing cardiac complications.11 Existing national scoring systems for predicting IVIG resistance vary among different ethnicities.12 Since 2006, approximately 17 predictive models have been published globally, including those by Kobayashi (2006), Tang, Y. (2016), and Piram-M (2020). Most models are from Asia (China, Japan, Taiwan, and Israel), and two are from the West (France and the United States).13 All studies are single-center studies. For example, the earliest Kobayashi score (2006) has some value in predicting treatment failure in unresponsive KD in the Japanese population but may have limited applicability in the UK, USA, and other regions.14 There is a lack of objective and reliable experimental markers to predict drug resistance. Several studies have shown an association between T-cell activation and anti-IVIG KD. T-cell activation requires multiple co-stimulatory signals and cytokines.15,16 Measurement of cytokines is commonly used in clinical practice. Therefore, cytokines associated with T-cell activation (IL-2, IL-7, IL-12, IL-15, and IL-17) and cytokines currently studied internationally (IL-6, TNF-α) were selected. In this study, we compared IL-2, IL-6, IL-7, IL-12, IL-15, IL-17, and tumor necrosis factor-alpha (TNF-α) in sensitive versus non-responsive KD patients. We investigated whether these cytokines can provide valid clues for non-responsive KD and enhance existing scoring mechanisms.
Materials and Methods
Study Population
This study was conducted from June 2022 to December 2023 at a specialized children’s hospital in Zhejiang Province, China. Children aged 1–14 years diagnosed with KD in the inpatient ward were included in the study. The study was approved by the Ethics Committee of the Institutional Review Board at Hangzhou Children’s Hospital [Ethical Review Approval No.: (2020) Ethical Approval (Research) No. 10], Informed consent was obtained from the parents or guardians of the minor participants. Inclusion criteria: 1) compliance with the 2017 American Heart Association (AHA) guidelines for the diagnosis of KD;17 2) age range of 1–14 years, both sexes; 3) complete inpatient data. Exclusion criteria: 1) comorbidities with other immune or immunodeficiency disorders, such as systemic juvenile idiopathic arthritis and leukemia; 2) recent treatment with immunoglobulin; 3) incomplete inpatient data.
Grouping criteria: All patients received intravenous immunoglobulin (IVIG) at a dose of 2 g/kg and aspirin at a dose of 30–50 mg/kg within 10 days of diagnosis. Unresponsive KD18 was defined as fever that did not subside (T > 38 °C) after 36 hours of IVIG treatment or reappearance of fever 2–7 days after resolution, accompanied by at least one main clinical feature of KD. Criteria for coronary artery anomalies (CAL):19 (1) Noninvasive: Z-value < 2; (2) Abnormal: Z-value ≥ 2 or initial Z-value < 2, with a decrease in Z-value by ≥ 1 during follow-up.
Diagnostic criteria for KD comorbidity: (1) Hepatic insufficiency: Elevated ALT, serum ALT > 50 U/L. (2) Myocardial damage: CK-MB > 50 U/L or ultrasensitive troponin (hs-cTn) > 0.05 ng/mL. (3) Hypoproteinemia: Total protein < 60 g/L or albumin < 25 g/L. (4) Cholestasis: Direct bilirubin > 17 μmol/L.
T-Lymphocyte-Activated Cytokines Detection
The T lymphocyte activation-related cytokines test is performed using a yellow procoagulation blood collection tube to collect a 2mL blood sample from the child’s peripheral vein. The sample is kept at room temperature for 15–30 minutes, then centrifuged at 2000g for 10 minutes at 4°C. After coagulation, the supernatant is collected and stored at −20°C or lower for later use. Serum samples will be sent to Hangzhou Dacheng Biotechnology Co. for analysis. The levels of IL-2, IL-6, IL-7, IL-12, IL-15, IL-17, and TNF-α will be measured according to the instructions of the ELISA kit (ELK Biotechnology).
Data Acquisition and Analysis
Clinical data collected included sex, age, clinical characteristics of the subjects, and clinical treatment received. Clinical characteristics primarily referred to complications meeting the diagnostic criteria for KD. Laboratory data were collected 24 hours before IVIG treatment and 3 days after the temperature returned to normal post-IVIG treatment.
Statistical Analysis
SPSS 25.0 statistical software was used to analyze the data. The raw data were first tested for normality. If they conformed to a normal distribution, a two independent samples t-test was used; if they did not, a two-sample rank sum test was used. Numerical data were expressed as numbers and percentages (%) and compared using the chi-square test. One-way analysis of variance (ANOVA) was performed using GraphPad Prism 9, and graphs were plotted to test for equality of variance. If the variances are equal, ordinary ANOVA should be used; if they are not, Boutefossess and Welch ANOVA methods should be used. MedCalc statistical software was used to plot ROC curves. In all statistical analyses, P < 0.05 was considered statistically significant.
Results
General Information
Eighty-two children with KD were included in this study. Among them, 48 were males and 34 were females, with a male-to-female ratio of 1.44:1. There were 19 cases in the 1–12 months age group, 24 cases in the 13–24 months age group, 21 cases in the 25–60 months age group, and 18 cases in the >60 months age group. According to whether the fever did not subside (T > 38°C) after 36 hours of initial IVIG (2g/kg/day) treatment or reappeared 2–7 days after subsiding, along with at least one main clinical feature of KD, the cases were divided into 71 in the sensitive KD group and 11 in the non-responsive KD group. The 11 cases of non-responsive KD were treated with a second full dose of IVIG (2g/kg/day, total dose 4g/kg) in combination with corticosteroids(1–2mg/kg each time, twice a day for 3–5 days, tapered off within 15 days after temperature stabilization and C-reactive protein reduction). In one case, after the second round of IVIG combined with hormone therapy, fever reappeared when the hormone dose was reduced. Infliximab (IFX) (5 mg/kg) was administered once, and the fever did not recur.
There was a significant increase in the proportion of unresponsive KD cases combined with hepatic insufficiency (p=0.004). There was no statistically significant difference when comparing other comorbidities (Table 1).
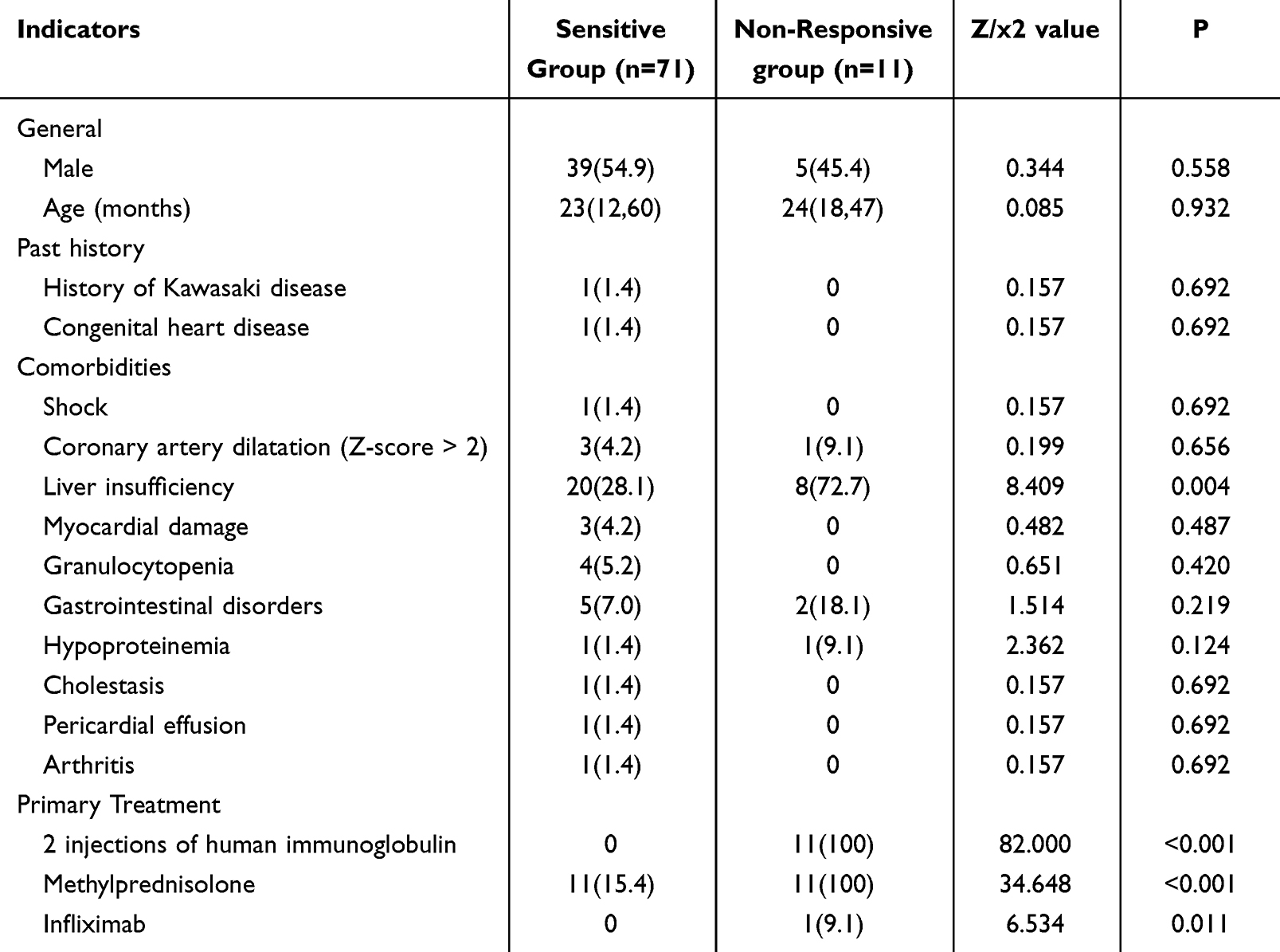 |
Table 1 Presents the Essential Clinical Data [Cases (%) and Represented by X2, M (P25, P75)] |
T-Lymphocyte Activation-Related Cytokine Levels
Differences in changes in T-lymphocyte-activating cytokines IL-2, IL-6, IL-7, IL-12, IL-15, IL-17, and TNF-α before and after treatment were compared between the sensitive and non-responder groups (see Figure 1). Before initial treatment, IL-2, IL-6, IL-7, IL-12, IL-15, IL-17, and tumor necrosis factor-α values were significantly higher in the non-responsive KD group compared to the sensitive KD group. Comparisons before and after initial treatment showed significant decreases in IL-6 and 17 in the sensitive KD group and significant decreases in IL-6 and 7 in the non-responsive KD group. IL-6 and 17 significantly increased in the sensitive group compared to the non-responsive group after initial treatment.
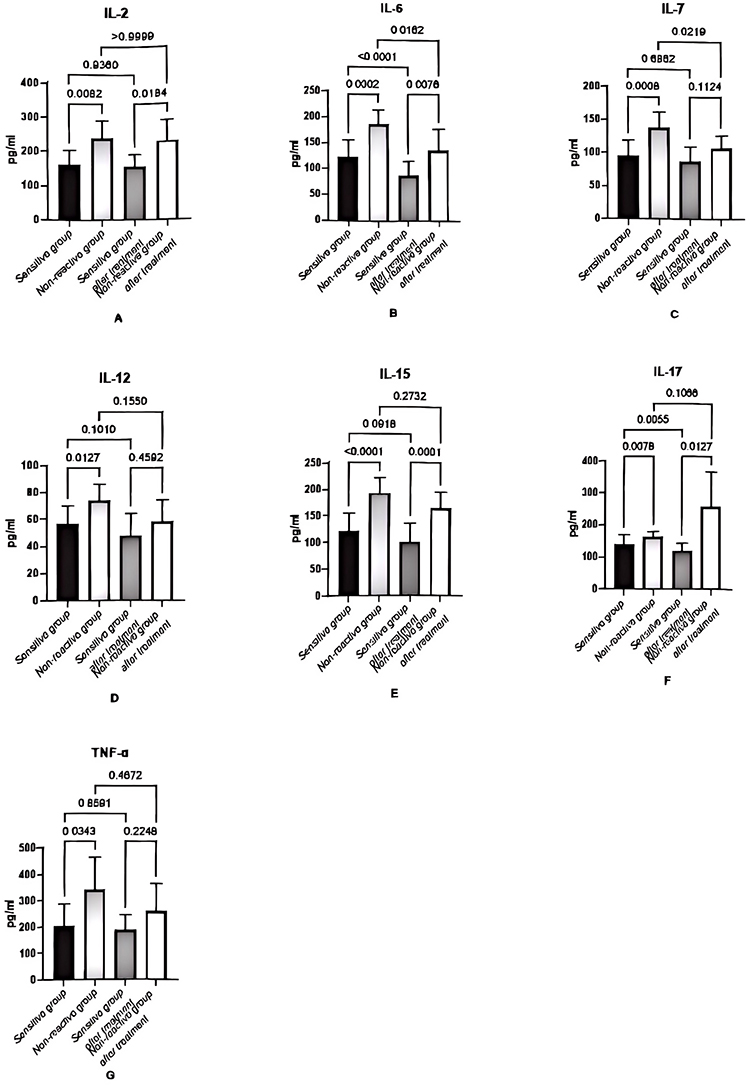 |
Figure 1 The study assessed the variations in cytokine levels associated with T lymphocyte activation (IL-2, 6, 7, 12, 15, 17, and TNF-α) across different groups. (A) Significant differences in IL-2 levels were noted between the sensitive and non-responsive groups, both before and after treatment (P < 0.05). (B) Statistically significant differences in IL-6 levels were observed in the sensitive group compared to the non-reactive group before and after treatment, as well as within each group over the treatment period (P < 0.05). (C) Statistically significant differences were observed pre-treatment between the sensitive and non-responsive groups, and within the non-responsive group before and after treatment (P < 0.05). (D) There was a significant difference in IL-12 levels between the sensitive and non-responsive groups before treatment (P < 0.05). (E) Statistically significant differences were noted between the IL-15-sensitive and non-responsive groups before and after treatment (P < 0.05). (F) Significant variations in IL-17 levels were noted between the sensitive and non-responsive groups before and after treatment, including changes within the sensitive group itself (P < 0.05). (G) A significant difference in TNF-α levels was found between the sensitive and non-responsive groups before treatment (P < 0.05). |
Predictive Efficacy of IL-6 and IL-17 for Non-Responsive KD
ROC curve analysis revealed that the AUCs for predicting non-responsive KD were 0.859 and 0.920 before and after IL-6 treatment, and 0.699 and 0.884 before and after IL-17 treatment, respectively (Table 2 and Figure 2).
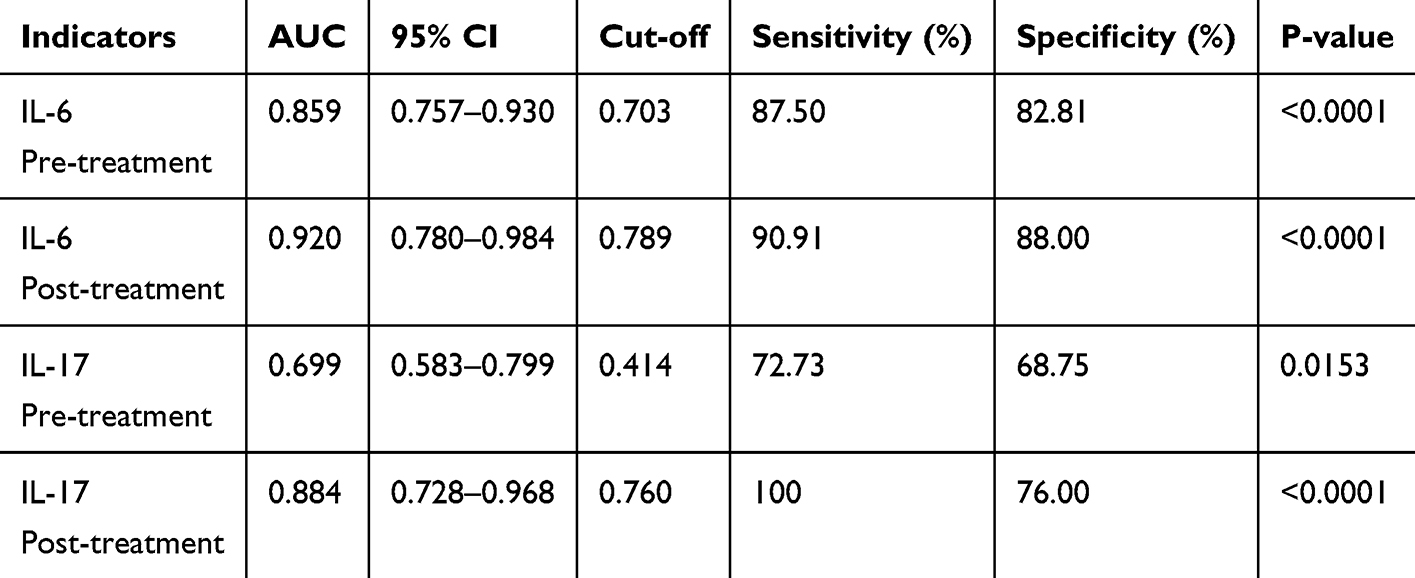 |
Table 2 Pre- and Post-Treatment Efficacy of IL-6 and IL-17 Alone |
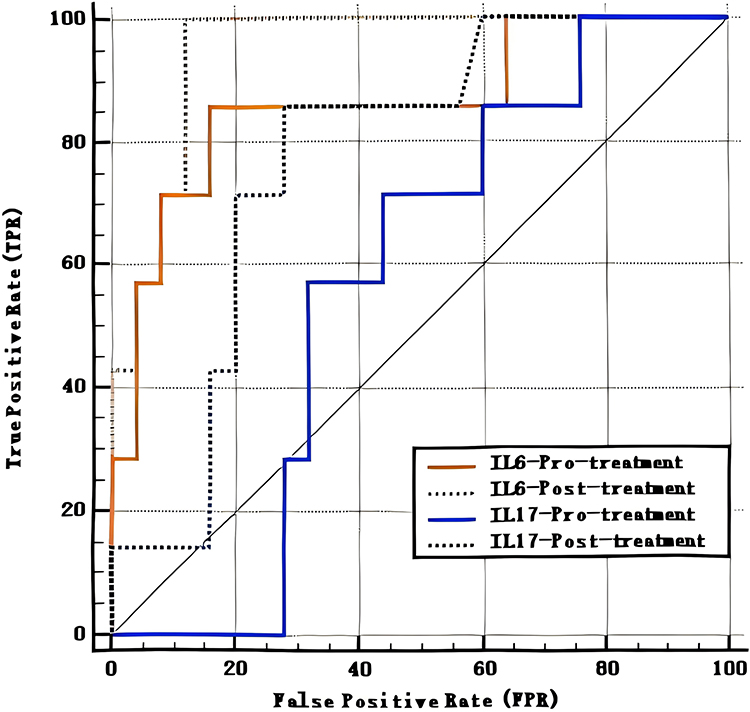 |
Figure 2 The ROC curves illustrate the pre- and post-treatment area under the curve for IL-6 and IL-17 in predicting nonresponsive Kawasaki disease. |
Discussion
Vascular complications and IVIG response in KD are closely linked to inflammation. The exact pathogenesis of KD remains unknown20 and is likely multifactorial,21 potentially involving immune activation triggered by infections in genetically susceptible children, leading to an inflammatory cascade.22 IVIG-unresponsive KD is less understood and may involve factors like insufficient IVIG dosage, hypermetabolism, neutrophil overactivation, elevated cytokine levels, and immature Fc receptor expression.23 A large multi-ethnic cohort study identified a polymorphism in the FCGR2A gene, with upregulated FcγRIIA mRNA levels associated with IVIG resistance. FcγRIIA interacts with IgG antibodies to activate antigen-presenting cells, prompting T-cell activation.24
Research on immune cell profiles during KD, particularly IVIG-unresponsive cases, is limited.25 Abnormal lymphocyte activation, such as heightened CD8+ T cell activity, may contribute to IVIG resistance.15,16,26 T cell activation requires antigen stimulation, co-stimulation, and cytokines, enabling differentiation into effector cells that produce immune mediators. Effector Th cells are classified into Th1, Th2, and Th17 subpopulations, regulated by specific cytokines: Th1 (IL-12): Produces IFN-γ for cellular immunity. Th2 (IL-25/33): Produces IL-4, IL-5, and IL-13 for parasitic and allergic immunity. Th17 (IL-6): Produces IL-17, IL-21, and IL-22 for tissue inflammatory responses.27 The γ-chain cytokine family (IL-2, IL-4, IL-7, IL-9, IL-15, IL-21) plays a critical role in T cell differentiation, proliferation, and homeostasis.28 Based on this, we analyzed IL-2, IL-6, IL-7, IL-12, IL-15, IL-17, and TNF-α for comparison.
In this paper, abnormal liver function was identified as statistically significant. Numerous studies have also highlighted it as a potential risk factor for unresponsive Kawasaki disease. The study further demonstrated significantly elevated levels of IL-2, IL-6, IL-7, IL-12, IL-15, IL-17, and TNF-α in the non-responder group, with IL-6 and IL-17 showing particular significance both before and after treatment. In non-responsive KD, T cell imbalances are observed, with reduced regulatory T cells (Treg) and increased inflammatory Th17 cells. T cell activation involves a complex system,27,29 with cytokine release playing a critical role: Antigen recognition: T-cell receptors (TCRs) recognize antigens presented by Antigen-Presenting Cells (APCs) via Major Histocompatibility Complex (MHC) molecules. Co-stimulatory signaling: APC-expressed CD80/CD86 interact with CD28 on T cells, delivering essential secondary signals. T cell activation: T cells proliferate and differentiate into effector cells, such as CD8+ cytotoxic T cells and CD4+ T cells (eg, Th1, Th2, Th17). Cytokine release: Activated T cells release cytokines like IL-6 and IL-17 to regulate immune responses. In IVIG-unresponsive KD, hypercytokinemia with elevated TNF-α and IL-6 is a hallmark.30,31 Studies show significantly higher plasma TNF-α levels in IVIG-unresponsive patients compared to responsive ones, strongly correlating with IVIG resistance.32,33 Cytokines like IL-2,34 IL-7, IL-12, IL-15, and IL-17, closely tied to T-cell activation, are also implicated in unresponsive KD. Additionally, IL-6 and TNF-α can be produced by neutrophils, monocytes, and macrophages, confirming that while T-cell activation is central to unresponsive KD, it is not the sole factor in its pathogenesis.
In this study, pairwise comparisons within each group identified IL-6 and IL-17 as significant factors. IL-6 showed statistically significant changes before and after treatment, both between and within the sensitive and non-responsive groups. The IL-17-sensitive group also demonstrated significant differences compared to the non-responsive group before and after treatment, as well as within the group itself. It was found that IL-6 and IL-17 were significantly elevated in the acute phase of non-responsive KD and remained high after initial IVIG treatment. Specifically, IL-6 showed statistical significance both between and within groups before and after treatment. Numerous studies confirm IL-6 predicts IVIG non-responsive KD.23,35,36 IL-6 promotes lymphocyte proliferation, macrophage activation, and interaction between immune cells, further activating other immune and inflammatory cells. Thus, IL-6 plays a critical role in immune response, inflammation, and antibody production. As a pleiotropic proinflammatory factor, IL-6 activates various signaling mechanisms involved in CD4+ T cell regulation and vascular growth, contributing to complex disease pathophysiology. It is suggested that IL-6 is highly sensitive but not very specific for unresponsive KD.37 IL-17, produced mainly by CD4+ T cells, activates Th17 cells and plays a crucial role in inflammation and tissue damage. Th17 cells produce IL-17 and are associated with autoimmunity and tissue damage. IL-17 induces additional pro-inflammatory cytokines, including IL-6, TNF-α, and IL-8,38 and the IL-17 family, especially IL-17A, signals to non-hematopoietic cells to initiate immune defense mechanisms. High blood levels of IL-17A correlate with KD severity. IL-17A levels are higher in IVIG-resistant KD patients39 and in CAL-positive sensitized groups compared to CAL-negative ones.40 IVIG inhibits Th17 differentiation and IL-17A/F production,41 and IL-17 may serve as a diagnostic marker for KD and a risk factor for coronary artery aneurysms.42 Overexpression of IL-17 is hypothesized to inhibit IVIG’s anti-inflammatory effects. Both IL-6 and IL-17, mainly derived from CD4+ T cells, are involved in non-responsive KD.43 ROC curve analysis showed IL-6 predicted non-responsive KD with an AUC of 0.859 before and 0.920 after treatment, while IL-17’s AUC was 0.699 and 0.884, respectively, indicating higher predictive value after IVIG treatment. Thus, re-testing IL-6 and IL-17 within 36 hours post-IVIG treatment is recommended. If IL-6 shows minimal decrease and/or IL-17 continues to rise, non-responsive KD is strongly suggested. Combined with clinical manifestations, this approach could enhance the predictive value and supplement existing scoring systems.
This study has several limitations. First, the sample size is relatively small, and only a limited range of T-cell activation-related cytokines was analyzed. Moreover, as a single-center study, its findings may lack generalizability, necessitating future large-scale, multi-center studies for more robust and reliable results. Second, IL-17 was not further subtyped, with future studies expected to focus specifically on IL-17A. Third, the optimal method for assessing T-cell activation, such as T-cell flow cytometry, was not utilized in this study due to the constraints of experimental time and blood sample storage during specimen collection.
Conclusion
The involvement of cytokines related to T-cell activation, particularly through retesting IL-6 and IL-17 after initial treatment, enhances the predictability of unresponsive KD. This indicates that T-cell-activated cytokines are implicated in the pathogenesis of refractory Kawasaki disease, highlighting the need for further investigation. Unresponsive KD remains a clinical diagnosis, and the findings of this study aim to aid clinicians in initiating early treatment to minimize the severe consequences of unresponsive KD.
Ethical Approval
This study was in compliance with the Declaration of Helsinki, and approved by the Ethical Committees of Hangzhou children’s Hospital.
Acknowledgments
The author expresses profound appreciation to Laboratory Physician Renxi Zhou and Nurse Wenjun Shi for them role in procuring comprehensive data and blood specimens from the participants involved in the ongoing research.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the 2020 hangzhou Science and Technology Program under the Class A category, with project number A20200778.
Disclosure
The authors declare that the research was conducted without any commercial or financial relationships that might be interpreted as potential conflicts of interest.
References
1. Piram M, Darce Bello M, Tellier S, et al. Defining the risk of first intravenous immunoglobulin unresponsiveness in non-Asian patients with Kawasaki disease. Sci Rep. 2020;10(1):3125. doi:10.1038/s41598-020-59972-7
2. Chen J, Liao J, Xiang L, et al. Current knowledge of TNF-α monoclonal antibody infliximab in treating Kawasaki disease: a comprehensive review. Front Immunol. 2023;14:1237670. doi:10.3389/fimmu.2023.1237670
3. Han SB, Lee SY. Macrophage activation syndrome in children with Kawasaki disease: diagnostic and therapeutic approaches. World J Pediatr. 2020;16(6):566–574. doi:10.1007/s12519-020-00360-6
4. Friedman KG, Jone PN. Update on the management of Kawasaki disease. Pediatr Clin North Am. 2020;67(5):811–819. doi:10.1016/j.pcl.2020.06.002
5. Takekoshi N, Kitano N, Takeuchi T, et al. Analysis of age, sex, lack of response to intravenous immunoglobulin, and development of coronary artery abnormalities in children with Kawasaki disease in Japan. JAMA Netw Open. 2022;5(6):e2216642. doi:10.1001/jamanetworkopen.2022.16642
6. Inoue T, Murakami S, Matsumoto K, et al. Functional benefits of corticosteroid and IVIG combination therapy in a coronary artery endothelial cell model of Kawasaki disease. Pediatr Rheumatol Online J. 2020;18(1):76. doi:10.1186/s12969-020-00461-6
7. Marchesi A, Tarissi de Jacobis I, Rigante D, et al. Kawasaki disease: guidelines of Italian Society of Pediatrics, part II - treatment of resistant forms and cardiovascular complications, follow-up, lifestyle and prevention of cardiovascular risks. Ital J Pediatr. 2018;44(1):103. doi:10.1186/s13052-018-0529-2
8. Kuo HC. Diagnosis, progress, and treatment update of Kawasaki disease. Int J Mol Sci. 2023;24(18):13948. doi:10.3390/ijms241813948
9. Zhang RL, Lo HH, Lei C, et al. Current pharmacological intervention and development of targeting IVIG resistance in Kawasaki disease. Curr Opin Pharmacol. 2020;54:72–81. doi:10.1016/j.coph.2020.08.008
10. Bordea MA, Costache C, Grama A, et al. Cytokine cascade in Kawasaki disease versus Kawasaki-like syndrome. Physiol Res. 2022;71(1):17–27. doi:10.33549/physiolres.934672
11. Sudo D, Makino N, Nakamura Y. Recurrent Kawasaki disease and cardiac complications: nationwide surveys in Japan. Arch Dis Child. 2020;105(9):848–852. doi:10.1136/archdischild-2019-317238
12. Conte C, Sogni F, Rigante D, et al. An update on reports of atypical presentations of Kawasaki disease and the recognition of IVIG non-responder children. Diagnostics. 2023;13(8):1441. doi:10.3390/diagnostics13081441
13. Wang S, Huang H, Hou M, et al. Risk-prediction models for intravenous immunoglobulin resistance in Kawasaki disease: risk-of-bias assessment using PROBAST. Pediatr Res. 2023;94(3):1125–1135. doi:10.1038/s41390-023-02558-6
14. Kainth R, Shah P. Kawasaki disease: origins and evolution. Arch Dis Child. 2021;106(4):413–414. doi:10.1136/archdischild-2019-317070
15. Ye Q, Gong FQ, Shang SQ, et al. Intravenous immunoglobulin treatment responsiveness depends on the degree of CD8+ T cell activation in Kawasaki disease. Clin Immunol. 2016;171:25–31. doi:10.1016/j.clim.2016.08.012
16. Matsuguma C, Wakiguchi H, Suzuki Y, et al. Dynamics of immunocyte activation during intravenous immunoglobulin treatment in Kawasaki disease. Scand J Rheumatol. 2019;48(6):491–496. doi:10.1080/03009742.2019.1604992
17. McCrindle BW, Rowley AH, Newburger JW, et al. Diagnosis, treatment, and long-term management of Kawasaki disease: a scientific statement for health professionals from the American Heart Association. Circulation. 2017;135(17):e927–e999. doi:10.1161/CIR.0000000000000484
18. Burns JC, Roberts SC, Tremoulet AH, et al. Infliximab versus second intravenous immunoglobulin for treatment of resistant Kawasaki disease in the USA (KIDCARE): a randomised, multicentre comparative effectiveness trial. Lancet Child Adolesc Health. 2021;5(12):852–861. Correction published in Lancet Child Adolesc Health. 2022;6(2):e5. doi:10.1016/S2352-4642(21)00270-4
19. Center for Diagnosis and Treatment of Kawasaki Disease/Children’s Hospital of Shaanxi Provincial People’s Hospital, National Children’s Medical Center/Beijing Children’s Hospital, Capital Medical University, et al. Evidence-based guidelines for the diagnosis and treatment of Kawasaki disease in children in China (2023). Zhongguo Dang Dai Er Ke Za Zhi. 2023;25(12):1198–1210. Chinese. doi:10.7499/j.issn.1008-8830.2309038
20. Burns JC. The etiologies of Kawasaki disease. J Clin Invest. 2024;134(5):e176938. doi:10.1172/JCI176938
21. Aggarwal R, Pilania RK, Sharma S, et al. Kawasaki disease and the environment: an enigmatic interplay. Front Immunol. 2023;14:1259094. doi:10.3389/fimmu.2023.1259094
22. Broderick C, Kobayashi S, Suto M, Ito S, Kobayashi T. Intravenous immunoglobulin for the treatment of Kawasaki disease. Cochrane Database Syst Rev. 2023;
23. Wang Y, Qian SY, Yuan Y, et al. Do cytokines correlate with refractory Kawasaki disease in children? Clin Chim Acta. 2020;506:222–227. doi:10.1016/j.cca.2020.03.014
24. Nadig PL, Joshi V, Pilania RK, et al. Intravenous immunoglobulin in Kawasaki disease-evolution and pathogenic mechanisms. Diagnostics. 2023;13(14):2338. doi:10.3390/diagnostics13142338
25. Choi IS, Lee MJ, Choi SA, et al. Circulating immune cell profile and changes in intravenous immunoglobulin responsiveness over the disease course in children with Kawasaki disease. Front Pediatr. 2022;9:792870. doi:10.3389/fped.2021.792870
26. Xie Z, Huang Y, Li X, et al. Atlas of circulating immune cells in Kawasaki disease. Int Immunopharmacol. 2022;102:108396. doi:10.1016/j.intimp.2022.108396
27. Dong C. Cytokine Regulation and Function in T Cells. Annu Rev Immunol. 2021;39:51–76. doi:10.1146/annurev-immunol-061020-053702
28. Bell M, Gottschalk S. Engineered cytokine signaling to improve CAR T cell effector function. Front Immunol. 2021;12:684642. doi:10.3389/fimmu.2021.684642
29. Wik JA, Skålhegg BS. T cell metabolism in infection. Front Immunol. 2022;13:840610. doi:10.3389/fimmu.2022.840610
30. Hu P, Jiang GM, Wu Y, et al. TNF-α is superior to conventional inflammatory mediators in forecasting IVIG nonresponse and coronary arteritis in Chinese children with Kawasaki disease. Clin Chim Acta. 2017;471:76–80. doi:10.1016/j.cca.2017.05.019
31. Chang L, Yang HW, Lin TY, et al. Perspective of immunopathogenesis and immunotherapies for Kawasaki disease. Front Pediatr. 2021;9:697632. doi:10.3389/fped.2021.697632
32. Yamaji N, da Silva Lopes K, Shoda T, et al. TNF-α blockers for the treatment of Kawasaki disease in children. Cochrane. Database Syst Rev. 2019;8(8):CD012448. doi:10.1002/14651858.CD012448
33. Lo MS. A framework for understanding Kawasaki disease pathogenesis. Clin Immunol. 2020;214:108385. doi:10.1016/j.clim.2020.108385
34. Teraura H, Kotani K, Minami T, et al. The serum concentration of soluble interleukin-2 receptor in patients with Kawasaki disease. Ann Clin Biochem. 2017;54(2):209–213. doi:10.1177/0004563216677583
35. Zhang H, Song HB, Wang DX, et al. Correlation between the level of inflammatory cytokines and prognosis in children with IVIG-sensitive Kawasaki disease and IVIG-resistant Kawasaki disease. Pak J Med Sci. 2022;38(5):1165–1169. doi:10.12669/pjms.38.5.5408
36. Wu Y, Liu FF, Xu Y, et al. Interleukin-6 is prone to be a candidate biomarker for predicting incomplete and IVIG nonresponsive Kawasaki disease rather than coronary artery aneurysm. Clin Exp Med. 2019;19(2):173–181. doi:10.1007/s10238-018-00544-5
37. Kessel C, Koné-Paut I, Tellier S, et al. An immunological axis involving interleukin 1β and leucine-rich-α2-glycoprotein reflects therapeutic response of children with Kawasaki disease: implications from the KAWAKINRA trial. J Clin Immunol. 2022;42(6):1330–1341. doi:10.1007/s10875-022-01301-w
38. Koizumi K, Hoshiai M, Moriguchi T, et al. Plasma exchange downregulates activated monocytes and restores regulatory T cells in Kawasaki disease. Ther Apher Dial. 2019;23(1):92–98. doi:10.1111/1744-9987.12754
39. Li SY, Ding Y. Expression of interleukin-17A in serum of children with intravenous immunoglobulin-resistant Kawasaki disease and its clinical significance. Zhongguo Dang Dai Er Ke Za Zhi. 2023;25(3):244–249. doi:10.7499/j.issn.1008-8830.2210151
40. Inoue T, Miyashita M, Murakami S, et al. IL-1β and IL-17A are involved in IVIG resistance through activation of C/EBPβ and δ in a coronary artery model of Kawasaki disease. Allergy. 2020;75(8):2102–2105. doi:10.1111/all.14281
41. Wang N, Chen Z, Zhang F, et al. Intravenous immunoglobulin therapy restores the quantity and phenotype of circulating dendritic cells and CD4+ T cells in children with acute Kawasaki disease. Front Immunol. 2022;13:802690. doi:10.3389/fimmu.2022.802690
42. Brodeur KE, Liu M, Ibanez D, et al. Elevation of IL-17 cytokines distinguishes Kawasaki disease from other pediatric inflammatory disorders. Arthritis Rheumatol. 2024;76(2):285–292. doi:10.1002/art.42680
43. Xue Y, Yin J, Xu L, et al. Predictive value of peripheral blood lymphocyte subsets for children with intravenous immunoglobulin-resistant Kawasaki disease. Zhongguo Dang Dai Er Ke Za Zhi. 2023;25(12):1211–1218. doi:10.7499/j.issn.1008-8830.2305067
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.