Back to Journals » Risk Management and Healthcare Policy » Volume 14
Utilization of Routine Health Information from Health Management Information System and Associated Factors Among Health Workers at Health Centers in Oromia Special Zone, Ethiopia: A Multilevel Analysis
Authors Seid MA, Bayou NB, Ayele FY ![]() , Zerga AA
, Zerga AA ![]()
Received 7 October 2020
Accepted for publication 10 March 2021
Published 18 March 2021 Volume 2021:14 Pages 1189—1198
DOI https://doi.org/10.2147/RMHP.S285604
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Kent Rondeau
Mohammed Ahmed Seid,1 Negalign Berhanu Bayou,2 Fanos Yeshanew Ayele,3 Aregash Abebayehu Zerga3
1Zone Health Office, Oromia Specialized Zone, Kemisse, Amhara Region, Ethiopia; 2Department of Health Service Management School of Public Health, College of Medicine and Health Science, Jimma University, Jimma, Ethiopia; 3Department of Nutrition, School of Public Health, College of Medicine and Health Science, Wollo University, Dessie, Ethiopia
Correspondence: Fanos Yeshanew Ayele Tel +251921202298
Email [email protected]
Introduction: Health management information system is a building block for the health system. Even if using health facility data at all levels is critical, it is poorly practiced in developing countries. There is limited evidence about the utilization of routine health information from the health management information system in the study area. This study aimed to assess the utilization of routine health information from health management information system and associated factors among health professionals at health centers in Oromia special zone, Amhara region, Ethiopia.
Methods: A facility-based cross-sectional study was conducted from February to March 2019. A total of 369 health professionals who were the focal person for each service delivery point were taken from the selected health centers. The data analysis was done using STATA version 14. A multilevel mixed-effect logistic regression model was carried out to identify factors associated with utilization of routine health information from the health management information system. Adjusted odds ratio with 95% CI was reported to show the strength of association. A P-value of < 0.05 was used to declare statistical significance.
Results: The magnitude of good routine health information utilization among health care professionals was 52.8%. Training (AOR=2.40, 95% CI=1.35, 4.26), availability of standard indicator definition (AOR=2.01, 95% CI=1.13, 3.57), data analysis skills (AOR=2.59, 95% CI=1.45, 4.62), regular feedback (AOR=2.29, 95% CI=1.29, 4.05), performance evaluation (AOR=2.60, 95% CI=1.19, 5.68) and timely reporting (AOR=2.89, 95% CI=1.54, 5.42) were significantly associated with routine health information utilization.
Conclusion: The overall utilization of routine health information from the health management information system was low. Therefore, the Zone health department and woreda health offices need to give training on HMIS data use, and avail standard indicator definition for all health care workers at all service delivery points.
Keywords: routine health information utilization, health care professionals, health centers
Introduction
Health information system (HIS) is a system that integrates data collection, processing, analyze, use, and dissemination of health-related information to improve health-care outcomes.1 Health management information system (HMIS) is an integrated effort to collect, analyze, report and use health information to support planning, management, and decision-making in health facilities and organizations.2,3 Routine health information system (RHIS) from HMIS has been a main source of information for continuous monitoring of health service. It is used for decision-making, resource allocation and strategy development.4,5 All functions of the health system rely on the availability of timely, accurate and reliable information for better clinical and health management decision-making.6
Although HMIS is a backbone for strong health systems, most decisions were made without the utilization of routine data.1,7 In developing countries, the health system managers tend to miss the role of routine data instead it sat in reports, shelves, cabinets, databases.6 Findings from Africa indicated that the routine health information utilization varied from 27% to 69.6%.8–12 Local studies conducted in Jimma, Dire Dawa, Hadiya, and Gondar, Ethiopia stated that the overall utilization of routine health information was 32.9%, 53.1%, 69.3%, and 78.5%, respectively.13–16
Routine health information utilization was affected by organizational and individual characteristics of health care professionals.15–19 Analysis skill, lack of a culture of information use, lack of supervision and regular feedback, organizational infrastructure, availability of skilled human resources, the inconsistency of data, completeness of data and HMIS training affect utilization of routine health information.13,14,18,20
Even if efforts are made to improve HMIS use, the quality of data and utilization remains unsatisfactory at peripheral health systems.11,13,17,21 There were also poorly harmonized processes.16,17 As a result, most administrative decisions were made without evidence.13,16 There is limited evidence about the utilization of routine health information from HMIS by multilevel analysis. Hence, this study was designed to assess the utilization of routine health information from HMIS among health care professionals and its associated factors in Oromia special zone, Amhara region, Ethiopia.
Materials and Methods
Study Design and Setting
A facility-based cross-sectional study was conducted among health care professionals from February 1–30, 2019 in Oromia special zone, Amhara region, Ethiopia. Its capital city is Kemisse which is located at 325 kilometer north of Addis Ababa.22 According to the 2018 Zonal health department data, the total population was 57,677. There is one general hospital, one primary hospital, twenty-seven health centers, and one hundred five health posts in the zone. Around 940 health care professionals are working at the health centers.
Study Population, Sampling Size and Sampling Procedure
The source populations were all health professionals working at health centers in Oromia special zone. The study populations were all health professionals in selected health centers of Oromia special zone. All health professionals in the selected health centers who were representative (focal person) for service delivery points were included in the study.
The sample size was calculated by single population proportion formula, assuming 38.4% prevalence of utilization of RHIS in West Gojam health facilities in 2017,18 95% level of confidence, and marginal of error (d) of 5%. This yields a sample size of 363.4. By considering 5% non-response rate the final sample size was 382.
In Oromia special zone 27 health centers implement the HMIS, from these 21 health centers were selected by lottery method. From each selected health centers, eighteen study participants (leader of the health center, HMIS focal person and focal person of each service delivery points) were taken.
Data Collection and Data Quality Control
The questionnaire was adapted from the Performance of Routine Information System Management (PRISM) framework assessment tool.19,23 The PRISM framework consists of tools to assess HIS performance and to identify technical, behavioral, and organizational factors.7,23
Data were collected by a pretested, structured, and interviewer-administered questionnaire. Ten diploma health information technicians (HIT) who had training on HMIS were assigned for data collection. Two BSc health professionals who had experience in HMIS monitoring and evaluation were assigned for supervision. Training was given for data collectors and supervisors on the overall data collection procedure. A pre-test was conducted on 8% of the sample size in Kombolcha health centers. Daily supervision was held at all health facilities by the supervisors and the investigators. The collected data were rechecked before data entry by the investigators.
Study Variables
Dependent Variables
Utilization of routine health information from HMIS data (Poor, Good).
Independent Variable
- Socio-demographic variables: Age, sex, education level, professional category, and experience
- Technical characteristics: Computer skills, regular report preparation indicators definition, training, data management, standard reporting, supportive supervision, and regular feedback
- Behavioral characteristics: Problem-solving for HIS tasks, competence in HIS tasks, confidence levels for HIS tasks, and motivation.
Performance evaluation plan, finance, data storage devices access, computer access, standard guideline availability, data quality check, presence of HIT, operational plan, regular supervision and management support.
Operational Definitions
Routine health information system utilization was measured by the PRISM assessment tool.23 It is defined as the use of health information in decision-making, such as for planning, monitoring, evaluation, treating patients/services, disease prioritization, budget allocation, supervision, writing feedback, showing trends and quality data reporting. Health information utilization scores of health professionals’ were computed from these 10 criteria. Then, respondents were grouped as having good routine health information utilization, when their mean score was greater than or equals to 65%, otherwise they were grouped as having poor routine health information utilization.23
Statistical Analysis
Data were entered into Epi data version 3.1 and exported to STATA version 14 for analysis. Descriptive statistics were computed to summarize the data. Due to the hierarchical nature of the data (individual-level variables were nested within organization-level variables), multilevel mixed-effect logistic regression was considered. To check eligibility of the data for multilevel analysis, Intra-cluster Correlation (ICC) was calculated and it was eligible with ICC greater than 10%. The log of the probability of utilization of routine health information from HMIS was modelled as follows:24

where:
- i and j are individual-level and organization-level units, respectively.
- X and Z refer to individual and organization-level variables, respectively.
- πij is the probability of utilization of routine health information from HMIS for the ith health professional in the jth health centers.
- β’s indicates the fixed coefficients.
- (Β0) is the intercept, μj showed the random effect and eij showed random errors.
The analysis was done in four models. Model I (Empty model) was fitted without explanatory variables to test random variability in the intercept and to estimate the intra-class correlation (ICC). Model II examined the effects of individual-level characteristics. Model III examined the effect of organizational-level variables, and Model IV examined the effects of both individual and organizational level characteristics simultaneously. Bi-variable multilevel logistic regression was fitted. Then, variables with a p-value <0.2 at model II and model III were entered into the multivariable multilevel logistic regression analysis (final model).
The likelihood of utilization of routine health information from HMIS among health professionals and different explanatory factors were measured by Adjusted Odds Ratio (AOR) with respective 95% confidence interval (CI). Variables with a p-value less than 0.05 at model-IV were considered as significantly associated.
The random-effects were measured by using ICC, Median Odds Ratio (MOR) and Proportional Change in Variance (PCV). ICC shows the variation in utilization of routine health information from HMIS among health professionals due to organization characteristics. It can be calculated as: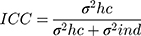 , where
, where  = variance between health centers, and
= variance between health centers, and  = variance within individual health professionals.
= variance within individual health professionals.
MOR is the median value of the odds ratio between the health centers at good utilization and the poorest utilization when randomly picking out two health centers. And it was calculated as MOR = Exp . PCV measures the total variation attributed to individual-level variables and organizational-level variables in the final model.25 Multicollinearity among explanatory variables was checked by using standard error at cut-off point ±2 and there was no multicollinearity. The log-likelihood test was used to estimate the goodness of fit of the adjusted final model in comparison to the preceding models.
. PCV measures the total variation attributed to individual-level variables and organizational-level variables in the final model.25 Multicollinearity among explanatory variables was checked by using standard error at cut-off point ±2 and there was no multicollinearity. The log-likelihood test was used to estimate the goodness of fit of the adjusted final model in comparison to the preceding models.
Results
Socio-Demographic Characteristics
A total of 369 health professionals were included in the study, with a response rate of 96.5%. Around two-third (62.6%) of the respondents was male. The majority (84%) of the respondents were belonged to the age group of <30 years, with a mean age of 26.28 years ± 3.75 SD. More than half (55.8%) of the respondents were diploma graduates. One hundred fifty-two (41.2%) of the respondents were nurses and 232 (62.9%) of the respondents had ≤3 years’ work experience (Table 1).
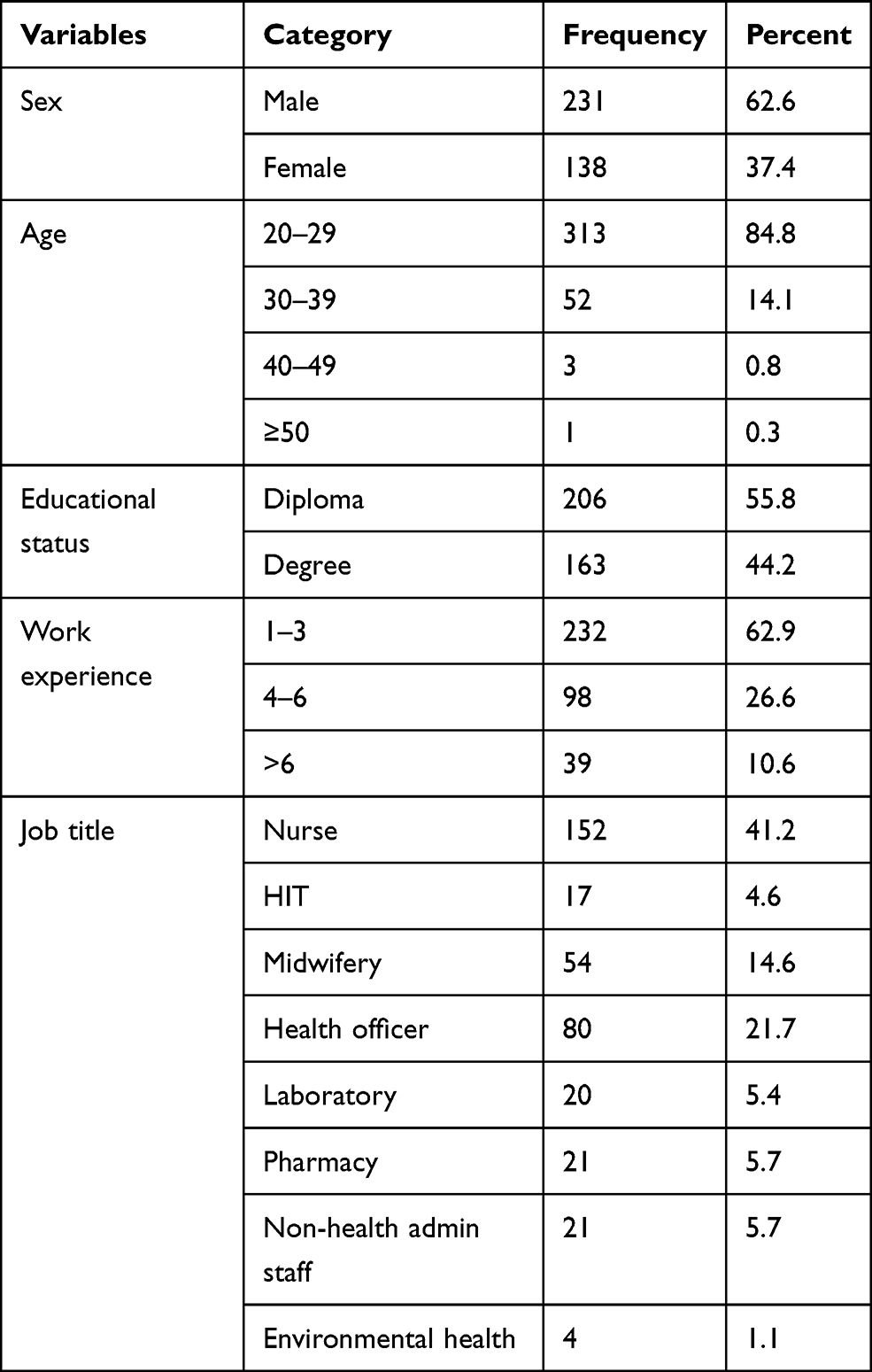 |
Table 1 Socio-Demographic Characteristics of Health Professionals from Health Centers in Oromia Special Zone, Amhara Region, Ethiopia, 2019 (n=369) |
Routine Health Information Utilization from HMIS Data
In this study, the majority 293 (79.4%) of the respondents used routine health data for treating patients 286 (77.5%) for monitoring day to day health service activities, 277 (75.1%) for planning, 233 (63.3%) for disease prioritization, 222 (60.2%) for performance evaluation, 226 (61.2%) for observing trends of services, 224 (60.7%) for checking data quality, 217 (58.8%) for showing a key performance by the chart, 198 (53.7%) for taking action and 187 (50.7%) for information dissemination (Table 2). The overall magnitude of good routine health information utilization of health professionals was 52.8% with 95% CI (47.7%, 57.7%) (Figure 1).
 |
Table 2 Routine Health Information System Utilization of Health Professionals Working at Health Centers in Oromia Special Zone, Amhara Region, Ethiopia, 2019 (n=369) |
 |
Figure 1 HMIS routine data utilization among health workers working at health centers in Oromia special zone, Ethiopia, 2019. |
Technical and Organizational Characteristics
Two hundred six (55.8%) of the participants received training about HMIS. More than half 212 (57.5%) and 213 (57.7%) of the health professionals had awareness about data presentation and data analysis skills, respectively. The majority (325, 88.1%) of the study participants had a standardized reporting period (Figure 2).
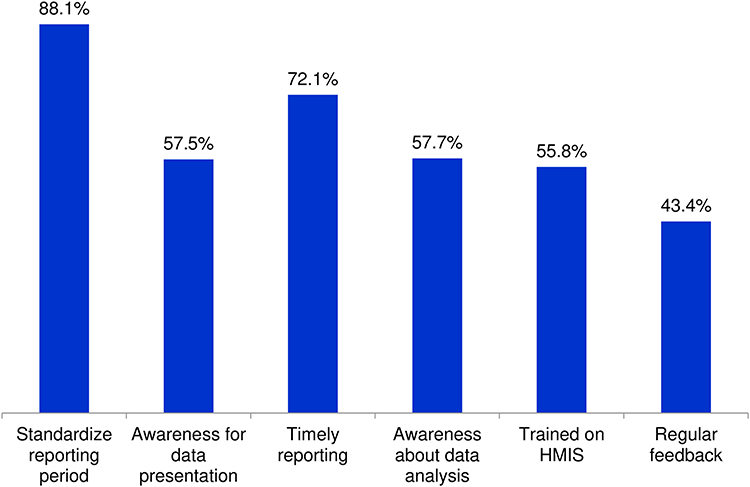 |
Figure 2 Technical characteristics of health workers working at health centers in Oromia special zone, Amhara Region, Ethiopia, 2019. |
More than half of the health centers (61.9%) give regular supervision and had adequate recording and reporting tools. And 13 (62.6%) of the health centers had a standard guideline for routine health information utilization. Seventeen (80.9%) and 18 (85.7%) of the health centers had no computer access and data storage devices, respectively (Table 3).
 |
Table 3 Organizational Characteristics of the Health Centers in Oromia Special Zone, Amhara Region, Ethiopia, 2019 (n=21) |
Behavioural Characteristics of Health Professionals
More than half 211 (57.2%) of the participants had a competence for routine health information utilization. Three-fourth (69%) of the health professionals had favourable motivation about routine health information (Table 4).
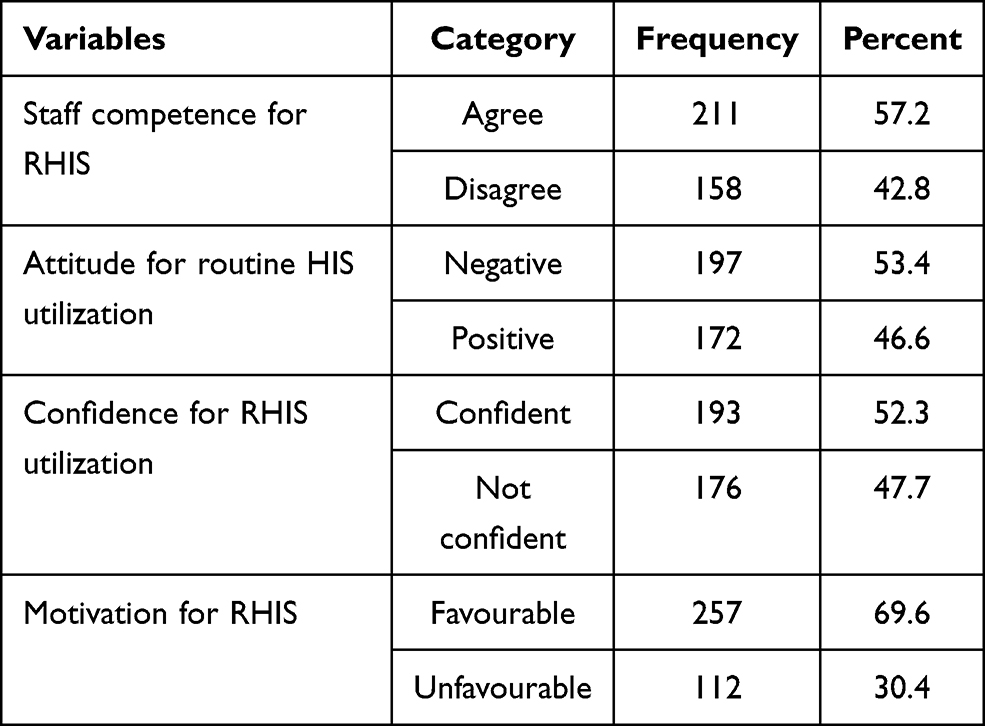 |
Table 4 Behavioural Characteristics of Health Workers in Health Centers of Oromia Special Zone, Ethiopia, 2019 (n=369) |
Cross-Organizational/Health Center/Variations Analysis
The estimates of cluster health center random effects show significant variations in routine data utilization among health workers across health centers. Estimates of intra-class correlations show that about 37.5% of the total variation in routine data utilization factors among health workers is attributable to health center cluster-level differences. Estimates of intra-class correlation suggest that 31% of the total variation in the routine health information utilization is attributable to unobserved health center level factors. When resource allocation and data quality check factors were controlled, the intra-class correlation coefficient was reduced to 6.38%. This means 6.38% of the total variability in HMIS data utilization by health workers was attributable to the health center level. The remaining 93.62% of the variation was attributable to the individual level difference (Table 5).
 |
Table 5 Estimation of Random Effect of Health Centers Factors Associated with Routine Health Information Utilization, in Oromia Special Zone, Amhara Region, Ethiopia, 2019 |
Factors Associated with Routine Health Information Utilization
In the bivariable analysis; work plan, training, standard indicator definition, financial allocation, data storage device, timely reporting, data presentation skill, data analysis skills, regular feedback, performance evaluation, information culture and timely reporting had an association with good RHIS utilization at a p-value of <0.2. In the multivariable multilevel mixed-effect logistic regression analysis; HMIS training, standard indicator definition, data analysis skills, regular feedback, performance evaluation and timely reporting were significantly associated with good routine HMIS.
Health care providers who had training were 2.4 times (AOR= 2.40, 95% CI=1.35, 4.26) more likely to utilize RHIS compared to those who had no training. Similarly, the health workers who got regular feedback were 2.9 times (AOR=2.29, 95% CI =1.29, 4.05) more likely to utilize RHIS from HMIS than those who did not get regular feedback. The odds of RHIS utilization by health care workers who regularly monitor their performance were 2.60 times (AOR=2.60, 95% CI=1.19, 5.68) higher compared to those who did not monitor their performance. Health care providers who had awareness about standard HMIS indicator definition were two times more likely to utilize HMIS routine data (AOR= 2.01. 95% CI=1.13, 3.57) compared to those who do not have awareness. Besides, the odds of HMIS data utilization were 2.59 times (AOR=2.59, 95% CI =1.45, 4.62) higher among health workers who perform data analysis than those who did not perform data analysis (Table 6).
 |
Table 6 Individual and Health Center Level Factors Associated with Routine Health Information Utilization from HMIS in Oromia Special Zone, Amhara Region, Ethiopia, 2019 |
Discussion
This study aimed to assess the utilization of routine health information from HMIS data and associated factors among health professionals working at health centers. In this study, the proportion of routine health information utilization of health care professional was 52.8% (47.7%, 57.7%). This finding was parallel to a study conducted in Wollega (57.6%) and Dire Dewa (53.1%).16,26 While it was higher than a study conducted in Kenya (27%), Coˆ te d’Ivoire (38%), Jimma (32.9%), East Gojam (45.8%) and West Amhara (38%).8,9,13,17,18 This inconsistency might be due to the difference in the study period and setting. Recently different training opportunities were prepared for health professionals that may contribute to the better utilization of RHIS in the current study. However, the result of this study was lower than studies from Benin (58.9%), South Africa (65%), North Gondar (78.5%) and Hadiya (69.3%).10,11,14,15 The discrepancy might be due to the difference in the study period and efforts exerted. When the study participants have a higher opportunity to participate in different training, the training helps them to established behavior of routine data utilization.
In this study, training had a positive association with RHIS utilization in which health workers who had training were more likely to utilize the HMIS data. This finding was comparable with studies conducted in West Amhara,18 Jimma13 and South Africa.11 This might be since health professionals who took training on HMIS had the skill to compile and analyse data, and utilize information generated in the routine day-to-day activities.27
The finding of this study showed that health workers regular supervision have a positive association with RHIS utilization. This is consistent with studies done in Wollega26 and Jimma.13 This might be because health professionals’ decisions based on superiors’ directives and regular performance monitoring increase the utilization of HMIS data. Supportive supervision is important to encourage health workers, to identify the gaps and improve health workers’ performance.
Health workers who receive regular feedback were almost two times more likely to utilize routine health information data. This finding was comparable to study conducted in East Gojam,17 West Amhara18 and Dire Dewa.16 This might be because providing feedback both the strength and weakness to health professionals may encourage them to increase the utilization of data.
The other significant variable is that health workers who had data analyzing skills were 2.6 times more likely to utilize routine health information. This finding was similar to studies conducted in North Gondar,15 East Gojjam17 and West Amhara.18 This might be because data analysis skills are one of the inputs for utilizing routine health information and the skills of health workers to transform routine data into meaningful information.28 Without changing data into information, it is difficult to utilize routine health information for evidence-based decision-making.
In this study, the health workers who gave reports timely were more likely to utilize routine health information than those who delayed for reporting. This finding was aligned with studies conducted in North Gondar,15 Dire Dewa16 and Hadiya Zone.14 This might be due to the reason that data reported on time can be used for decision-making.
Finally, this study found that health care professionals who had standard indicator definitions in their service delivery point were two times more likely utilized routine health information. This finding was consistence with studies done in Hadiya zone,14 North Gondar,15 and Jimma zone.13 This might be due to the presence of standard indicator which provides utilization of information for evidence-based decision-making20 and also important to perform HIS activities with a standardized and appropriate way.
The strength of this study is using multilevel mixed-effect logistic regression model which is a powerful statistical tool to remove the cluster effect for the association between dependent and independent variables at different levels of cluster data. The findings of this study shall be interpreted with the following limitations. The nature of cross-sectional study design; some findings might reflect reverse causality and it might also difficult to establish a cause–effect relationship.
Conclusion
The findings of this study concluded that the overall health workers' routine health information utilization from HMIS was low compared to the national expectation. HMIS training, standard indicator definition, data analysis skills, regular feedback, performance evaluation and timely reporting had a significant association with routine health information utilization.
Therefore, the Zone health department and woreda health offices need to give training on HMIS data use, and avail standard indicator definition for all health care workers at all service delivery points. Program planners and officers should conduct regular supervision with periodical feedback for health care providers to improve the skill of routine information utilization.
Abbreviations
AOR, Adjusted odds ratio; CI, Confidence interval; HIS, Health Information System; HIT, Health Information Technician; HMIS, Health Management Information System; ICC, Intra-class Correlation; PRISM, Performance of Routine Information System Management; RHIS, Routine Health Information System.
Ethics Approval and Informed Consent
Ethical clearance was obtained from Wollo University, College of Medicine and Health Sciences ethical review committee. A supporting letter was taken from Oromia special zone Health Department. After a clear explanation of the study objectives, data collection procedures, data confidentiality and their rights to withdraw, informed consent was secured from health center administrators and study participants.
Acknowledgments
We would like to acknowledge Wollo University for the approval of the ethical clearance. We were also highly indebted to Oromia special zone health department for its valuable cooperation and support. Our gratitude also forwards to the study participants, data collectors and supervisors for their cooperation.
Author Contributions
MA: Participated in conceptualization, data curation, formal analysis, funding acquisition, investigation, methodology, project administration, resources, software, supervision, validation, visualization, writing the original draft, writing, review, and editing. NB: Participated in data curation, formal analysis, investigation, methodology, project administration, validation, visualization, writing, review, and editing. FY: Participated in data curation, formal analysis, investigation, methodology, project administration, validation, visualization, writing, review, and editing. AA: Participated in formal analysis, investigation, methodology, validation, visualization, writing, review, and editing.
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Lippeveld T, Sauerborn R, Bodart C; World Health Organization. Design and Implementation of Health Information Systems. World Health Organization; 2000.
2. Ross JE. Management by Information System. Englewood Cliffs^ eNew Jersey New Jersey: Prentice-Hall; 1970.
3. World Health Organization. Analysing Disrupted Health Systems in Countries in Crises Analysing Disrupted Health Sectors. Geneva: World Health Organization; 2008.
4. AbouZahr C, Boerma T. Health information systems: the foundations of public health. Bull World Health Organ. 2005;83:578–583
5. Network H. Framework and Standards for Country Health Information Systems. Geneva, Switzerland: World Health Organization; 2008.
6. Team HR. Health Management Information System (HMIS)/Monitoring and Evaluation (M&E): Strategic Plan for Ethiopian Health Sector. 2008. FMOH, editor.
7. Karijo E. Determinants of Utilization of Routine Data for Decision Making in Heal the Facilities in Kitui County. Kenya: Kenyatta University; 2013.
8. Wekesa RN. Utilization of the health information management system by community health workers in the AMREF facility in Kibera, Nairobi County, Kenya. Unpublished Masters Degree in Public Health, Monitoring and Evaluation Project, Kenyatta University, Nairobi, Kenya; 2014.
9. Nutley T, Gnassou L, Traore M, Bosso AE, Mullen S. Moving data off the shelf and into action: an intervention to improve data-informed decision making in Côte d’Ivoire. Glob Health Action. 2014;7(1):25035. doi:10.3402/gha.v7.25035
10. Ahanhanzo YG, Ouedraogo LT, Kpozèhouen A, Coppieters Y, Makoutodé M, Wilmet-Dramaix M. Factors associated with data quality in the routine health information system of Benin. Arch Public Health. 2014;72(1):25. doi:10.1186/2049-3258-72-25
11. Garrib A, Stoops N, McKenzie A, et al. An evaluation of the district health information system in rural South Africa. S Afri Med J. 2008;98(7):549–552.
12. Nzomo G. Use of routine health information for decision making among health workers at Coast General Hospital. Mombasa County, Kenya, Kenyatta University, Kenya; 2017.
13. Abajebel S, Jira C, Beyene W. Utilization of health information system at district level in Jimma zone Oromia regional state, South West Ethiopia. Ethiop J Health Sci. 2011;21:65–76.
14. Abera E, Daniel K, Letta T, Tsegaw D. Utilization of health management information system and associated factors in Hadiya zone health centers, Southern Ethiopia. Res Health Sci. 2016;1(2):e98. doi:10.22158/rhs.v1n2p98
15. Dagnew E, Woreta SA, Shiferaw AM. Routine health information utilization and associated factors among health care professionals working at public health institution in North Gondar, Northwest Ethiopia. BMC Health Serv Res. 2018;18(1):685. doi:10.1186/s12913-018-3498-7
16. Teklegiorgis K, Tadesse K, Mirutse G, Terefe W. Factors associated with low level of health information utilization in resources limited setting, eastern Ethiopia. Inf Syst. 2014;3(6):69–75.
17. Shiferaw AM, Zegeye DT, Assefa S, Yenit MK. Routine health information system utilization and factors associated thereof among health workers at government health institutions in East Gojjam Zone, Northwest Ethiopia. BMC Med Inform Decis Mak. 2017;17(1):116. doi:10.1186/s12911-017-0509-2
18. Asemahagn MA. Determinants of routine health information utilization at primary healthcare facilities in Western Amhara, Ethiopia. Cogent Med. 2017;4(1):1387971. doi:10.1080/2331205X.2017.1387971
19. Aqil A, Lippeveld T, Hozumi D. PRISM framework: a paradigm shift for designing, strengthening and evaluating routine health information systems. Health Policy Plan. 2009;24(3):217–228. doi:10.1093/heapol/czp010
20. Silas N. Factors influencing performance of routine health information system: the case of Garissa Subcounty, Kenya. 2017.
21. Tadesse K, Gebeyoh E, Tadesse G. Assessment of health management information system implementation in Ayder referral hospital, Mekelle, Ethiopia. Int J Intell Inf Syst. 2014;3(4):34.
22. Mengesha Y, Manaye B, Moges G. Assessment of public awareness, attitude, and practice regarding antibiotic resistance in Kemissie Town, Northeast Ethiopia: community-Based Cross-Sectional Study. Infect Drug Resist. 2020;13:3783. doi:10.2147/IDR.S280036
23. Hotchkiss DR, Aqil A, Lippeveld T, Mukooyo E. Evaluation of the performance of routine information system management (PRISM) framework: evidence from Uganda. BMC Health Serv Res. 2010;10(1):188. doi:10.1186/1472-6963-10-188
24. Christ O, Hewstone M, Schmid K, et al. Advanced multilevel modeling for a science of groups: a short primer on multilevel structural equation modeling. Group Dyn Theory Res Pract. 2017;21(3):121. doi:10.1037/gdn0000065
25. Brault MA, Ngure K, Haley CA, et al. The introduction of new policies and strategies to reduce inequities and improve child health in Kenya: a country case study on progress in child survival, 2000–2013. PLoS One. 2017;12(8):e0181777. doi:10.1371/journal.pone.0181777
26. Yarinbab TE, Assefa MK. Utilization of HMIS data and its determinants at health facilities in east Wollega zone, Oromia regional state, Ethiopia: a health facility based cross-sectional study. Med Health Sci. 2018;7(1).
27. Nutley T, Reynolds H. Improving the use of health data for health system strengthening. Glob Health Action. 2013;6(1):20001. doi:10.3402/gha.v6i0.20001
28. Press S. Stata Multilevel Mixed-Effects Reference Manual Release 13. StataCorp LP: Texas; 2013.
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.