Back to Journals » Patient Preference and Adherence » Volume 16
Utilization of Rehabilitation Services and Associated Factors Among Adults with Cancer Diagnoses at Hawassa Comprehensive Specialized Hospital, Ethiopia
Authors Bunare A ![]() , Weldegebreal F
, Weldegebreal F ![]() , Habte S
, Habte S ![]() , Ketema I
, Ketema I ![]() , Worku T
, Worku T
Received 15 April 2022
Accepted for publication 18 June 2022
Published 29 June 2022 Volume 2022:16 Pages 1571—1580
DOI https://doi.org/10.2147/PPA.S370923
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Arata Bunare,1 Fitsum Weldegebreal,2 Sisay Habte,3 Indeshaw Ketema,4 Teshager Worku3
1Department of Nursing, Hawassa Health Science College, Hawassa, Ethiopia; 2School of Medical Laboratory Sciences, Haramaya University, Harar, Ethiopia; 3School of Nursing and Midwifery, Haramaya University, Harar, Ethiopia; 4Department of Emergency and Critical Care Nursing, Haramaya University, Harar, Ethiopia
Correspondence: Sisay Habte, School of Nursing and Midwifery, Haramaya University, Harar, Ethiopia, Tel: +251 911807998, Email [email protected]
Background: Rehabilitation is a type of treatment that focuses on improving a person’s physical, social, cognitive, and emotional functioning. Currently, there is a significant unmet need for rehabilitation. Despite the expansion of rehabilitation services in Ethiopia, little is known about its utilization and associated factors.
Objective: This study aimed to assess the utilization of rehabilitation services and associated factors among adults with cancer diagnoses at Hawassa Comprehensive Specialized Hospital, Ethiopia.
Methods: An institutional-based cross-sectional study was employed among 325 participants selected using a systematic sampling technique. Data were collected using a pre-tested, interviewer-administered questionnaire and a review of medical records. Participants were considered as utilized if they attended at least one cancer rehabilitation service at the hospital in the last 1 year. The data were entered into EpiData version 4.6 and exported to Statistical Package for Social Science Version 23 for analysis. Binary logistic regression analysis was used to identify factors associated with the utilization of rehabilitation services. Variables with a P-value of < 0.05 were considered statistically significant.
Results: Utilization of rehabilitation service among adults with cancer diagnoses in the last 1 year were found to be 33.2% (95% CI; 27.93– 41.25). Being male (AOR=5.76; 95% CI: 2.60, 12.75), urban residence (AOR=2.56; 95% CI: 1.04, 6.26), ability to perform the activity of daily living independently (AOR=2.68; 95% CI: 1.20, 6.00), receiving education on cancer rehabilitation services (AOR=2.44; 95% CI: 1.21, having strong social support (AOR=2.10; 95% CI: 1.02, 4.87), 4.91) and satisfaction with cancer care (AOR=3.21; 95% CI: 1.42, 5.76) were factors associated with the utilization of rehabilitation services.
Conclusion: Only 33.2% of adults with cancer diagnoses at Hawassa Comprehensive Specialized Hospital utilized rehabilitation services. To improve the utilization of rehabilitation services, patients should receive adequate education on the benefits of rehabilitation.
Keywords: cancer care, hospice care, oncology, palliative care, supportive care
Introduction
Cancer has become a common disease with high morbidity and mortality worldwide.1 Globally, about 19.3 million new cancer cases and almost 10 million cancer deaths occurred in 2020.2 It is estimated that about 26 million new cancer cases and 17 million cancer deaths would occur by 2030.3 Cancer is quickly becoming a major public health issue in Africa.4 According to the GLOBOCAN report, cancer incidence was 1.1 million in Africa in 2020, with 711,000 deaths.5 By 2030, Africa is expected to have 1.28 million new cancer cases and 970,000 cancer deaths.6 In Ethiopia, cancer is expected to account for around 5.8% of total national mortality. The yearly cancer incidence is projected to be over 60,960 cases, with a fatality rate of over 44,000.1 Breast cancer is the most commonly diagnosed malignancy among Ethiopian adults.7 In Ethiopia, about 80% of cancer cases are diagnosed at an advanced stage.8
Survival rates for cancer patients are improving, and the number of survivors is expected to rise.9 Cancer survivors may experience physical, mental, and social challenges that negatively impact their quality of life.10,11 Cancer-related functional impairments are expected to worsen during the next few decades among cancer survivors.12 Cancer survivors experience a variety of functional limitations both during and after treatment.13 Individuals’ employment status is greatly impacted by functional limitations, which result in a significant financial burden and loss of productivity.14 These cancer-related impairments necessitated individualized and targeted rehabilitation services.15
Rehabilitation is defined as “a collection of therapies aimed at optimizing functioning and minimizing impairment in individuals with health concerns“.16 Rehabilitation involves various exercises, nutritional support, cognitive and psychosocial support, treatment of side effects, and pain management.16,17 Rehabilitation service is known to have a great benefit for a patient diagnosed with cancer.18 Patients at all phases of their cancer diagnosis benefit from cancer rehabilitation.19 Cancer rehabilitation programs can help cancer survivors regain function, reduce discomfort, and enhance their overall well-being. Previous research has shown that cancer rehabilitation can improve a person’s mobility, safety, and quality of life both during and after treatment.20,21 Moreover, cancer rehabilitation can have a great benefit for patients with both physical and mental health problems.17
Despite the fact that cancer rehabilitation is very important for patients who have been diagnosed with cancer, the need for rehabilitation is now largely unmet.16,22 More than half of the people in several the low- and middle-income nations do not obtain the rehabilitation services they require.16 The previous study conducted in Ethiopia showed that only 26% of patients with cancer diagnoses utilized rehabilitation services.23 In fact, the study was conducted almost eight years ago (April 2014) in Ethiopia’s capital city, where people traveled from all over the country to receive cancer treatment at Tikur Anbessa (Black Lion) specialized hospital, the country’s only center for cancer treatment at the time.24 Furthermore, the study was carried out before the cancer treatment center was expanded to other parts of Ethiopia.
Cancer was included in the Ethiopian Federal Ministry of Health’s efforts to combat non-communicable diseases.24 The Ministry of Health built six specialized cancer treatment centers in Gondar, Hawassa, Jimma, Mekele, St. Paul’s Hospital, and Haramaya as part of an effort to expand cancer treatment centers in Ethiopia.25 Cancer treatment and care are among the services covered by Ethiopia’s health insurance scheme.26 However, only little is known about the rate of utilization of cancer rehabilitation services and the factors that influence it. Therefore, this study aimed to assess the utilization of rehabilitation services and associated factors among adults with cancer diagnoses at Hawassa Comprehensive Specialized Hospital, Ethiopia.
Methods and Materials
Study Area and Period
The study was conducted at Hawassa Comprehensive Specialized Hospital (HCSH) from June 01- to July 30, 2021. Hawassa Comprehensive Specialized Hospital is located in Hawassa which is 275 kilometers south of Addis Ababa. Hawassa Comprehensive Specialized Hospital is a teaching and referral hospital affiliated with Hawassa University that provides cancer treatment. The hospital was founded in 1998 and has approximately 480 beds. The hospital opened a cancer center in 2013. The hospital serves more than 18 million people in Ethiopia’s Sidama, southern nations and nationalities, and some Oromia regions with cancer treatment and care.27 Nearly 2700 cases were registered in HCSH’s cancer center during the 2020/21 fiscal year. The HCSH’s cancer center is providing provided chemotherapy, radiation therapy, surgery and cancer rehabilitation care since its establishment. The majority of cancer rehabilitation service costs in this hospital are covered by patients or their family members, similar to other health care services; however, cancer treatment is one of the services covered by health insurance.26,28
Study Design and Population
An institutional-based cross-sectional study was conducted. All adults aged 18 years or older diagnosed with any type of cancer and who visited HCSH’s cancer center during the data collection period were included in this study. Adults with any type of cancer who were critically sick and unable to provide written informed consent due to cognitive impairment were excluded from the study.
Sample Size Determination
The sample size was determined using single population proportion formula with the assumptions: 95% confidence level with a 5% margin of error and 26% proportion of utilization of rehabilitation services from previous study.,23 Hence, the final sample size including 10% non-response rate was 325.
Sampling Procedure
A systematic sampling technique was used to select study participants. The total number of cancer patients who visited the hospital during the data collection period (741) was divided by the calculated total sample size (325) to get the fixed periodic interval (K value). Then study participants were selected at every two interval. The first study participant was selected by lottery method.
Data Collection Methods
The data were collected through a review of patient records and a face-to-face interview using questionnaires adapted from available literature in Ethiopia23 and tailored to the study’s objective. The questionnaires were prepared in English and translated into the local language (Amharic, Afan Oromo and Sidama language) by experts. The questionnaires were pretested on 5% of the study participants who were not enrolled in the study. The questionnaires included sociodemographic information, clinical information, cancer diagnosis types, satisfaction with cancer care received, social support, cancer rehabilitation utilization, and cancer rehabilitation service types. The interview was conducted at the HCSH cancer center by four trained nurses with a BSc degree.
Variables in the Study
Participants’ sociodemographic variables collected were: sex, age, educational status, marital status, residency, and monthly income. The basic activities of daily living (ADL) include bathing, dressing, toileting, maintaining continence, grooming, feeding, and transferring. The ability to perform ADL by study participants was assessed using the Katz Index of Independence in Activities of Daily Living. The total score ranges from 0 to 6. Scores less than 6 were classified as dependent, while scores greater than 6 were classified as independent.29 Participants’ satisfaction with cancer care was measured with the six-item Short Assessment of Patient Satisfaction (SAPS) scale. The total score ranges from 0 to 28, with 0 to 10 indicating “very dissatisfied”, 11 to 18 indicating “dissatisfied”, 19 to 26 indicating “satisfied”, and 27 to 28 indicating “very satisfied”.30 The categories, however, were merged into two for this study. Very satisfied and satisfied were combined to form “satisfied,” while very dissatisfied and dissatisfied were combined to form “dissatisfied.”
The Oslo social support scale (OSSS-3) was used to measure the level of social support. The OSSS-3 consists of three items with an overall score ranging from 3 to 14. The scores represent 3–8 poor social support, 9–11 moderate social support, and 12–14 strong social support.31 The type of cancer diagnosis, the stage of cancer, and the presence of comorbidity were captured from patients’ medical records.
The participants were assessed for the utilization and type of rehabilitation services, that individuals with cancer could receive, within the past 1 year. The rehabilitation services included physical therapy (PT), self-care education and training, energy conservation, nutritional support program, cognitive rehabilitation, psychosocial support program, emotional rehabilitation, relaxation training, treatment of the medication side effects, pain management, cancer survivorship education, and others. Participants were considered as utilized if they attended at least one cancer rehabilitation service at the hospital in the last 1 year.23
Data Processing and Analysis
The data were entered into Epi-data version 4.6 and exported to SPSS version 23 for analysis. Both bivariate and multivariable binary logistic regression analyses were performed to identify factors associated with the utilization of the rehabilitation service. Variables with a P-value <0.25 in the bivariate logistic regression analysis were retained for further analysis in multivariable binary logistic regression analysis. Adjusted Odds Ratio (AOR) along with a 95% confidence interval was estimated to assess the strength of the association. Variables with a p-value < 0.05 in the multivariable binary logistic regression analysis were considered statistically significant. Frequencies and percentages were used to summarize data and the descriptive statistics were presented using text and tables.
Results
Socio-Demographic Characteristics
A total of 325 adults with cancer diagnoses took part in the study. The mean age (SD) of study participants was 49 (±8). More than half, 177 (55.5%), of the study participants were females. Most of the study participants, 269 (82.8%) were rural residents. The majority of them,254 (78%), were literate (Table 1).
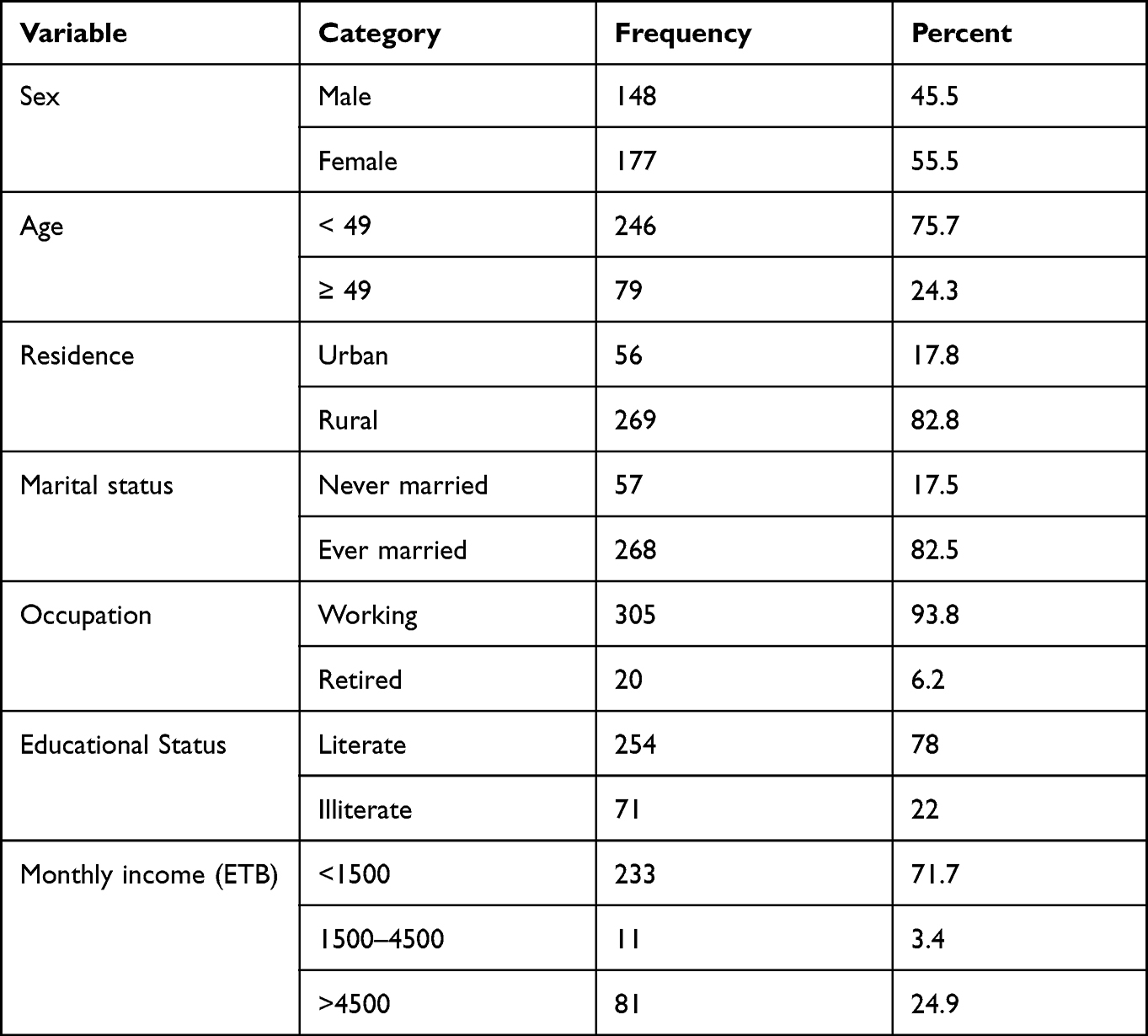 |
Table 1 Socio-Demographic Characteristics of Adults with Cancer Diagnoses at Hawassa Comprehensive Specialized Hospital, Ethiopia, 2021 (n = 325) |
Clinical Characteristics
The majority of the study participants were able to perform the activity of daily living (ADL) independently, 250 (76.9%). About 83.1% of them were without any comorbidities and 55.7% of them had localized cancer (Table 2).
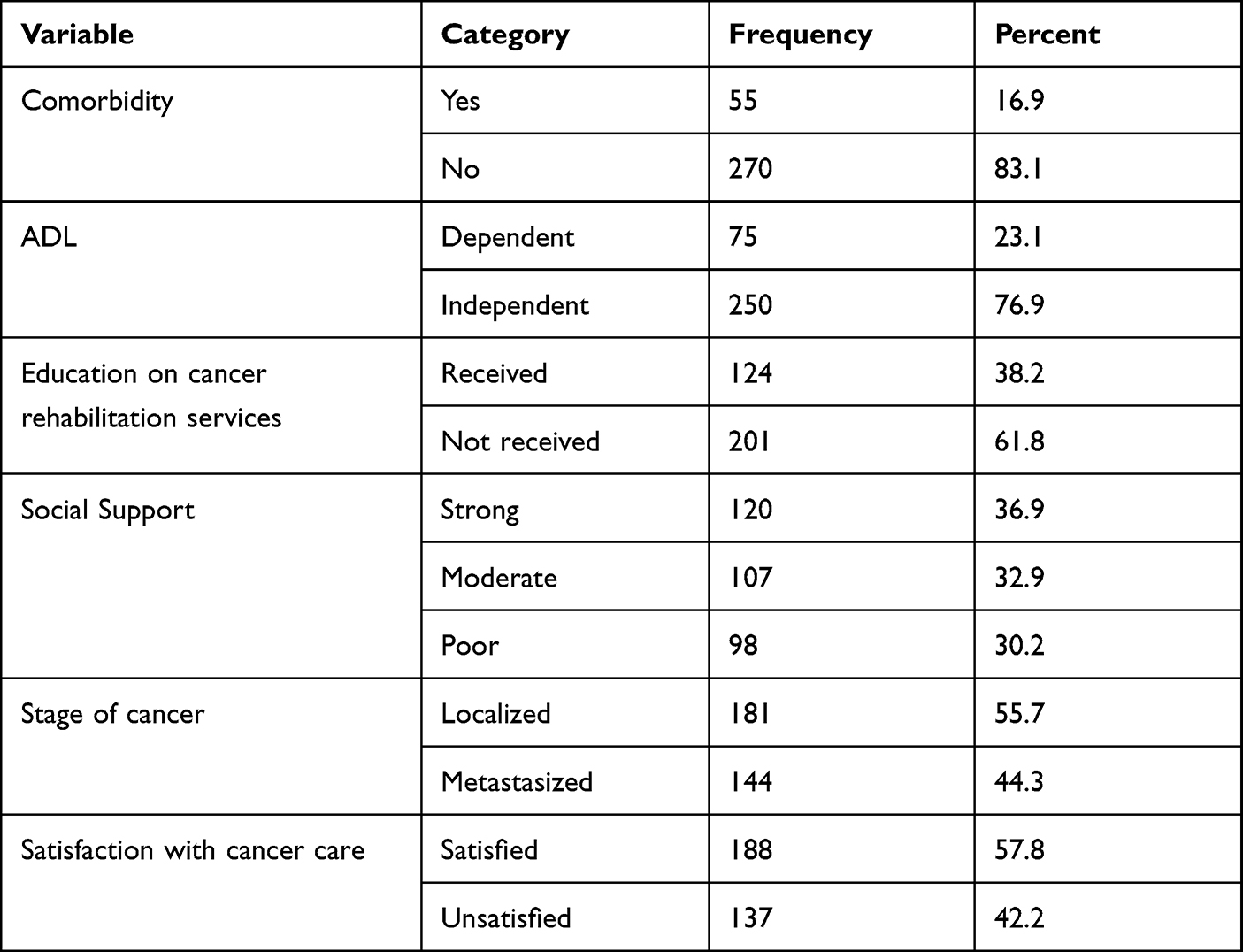 |
Table 2 Clinical Characteristics of Adults with Cancer Diagnoses at Hawassa Comprehensive Specialized Hospital, Ethiopia, 2021 (n = 325) |
Types of Cancer Diagnosis
Among the total study participants 29.8%, 14.8 and, 14.2% had breast, prostate, and gynecological cancer, respectively (Table 3).
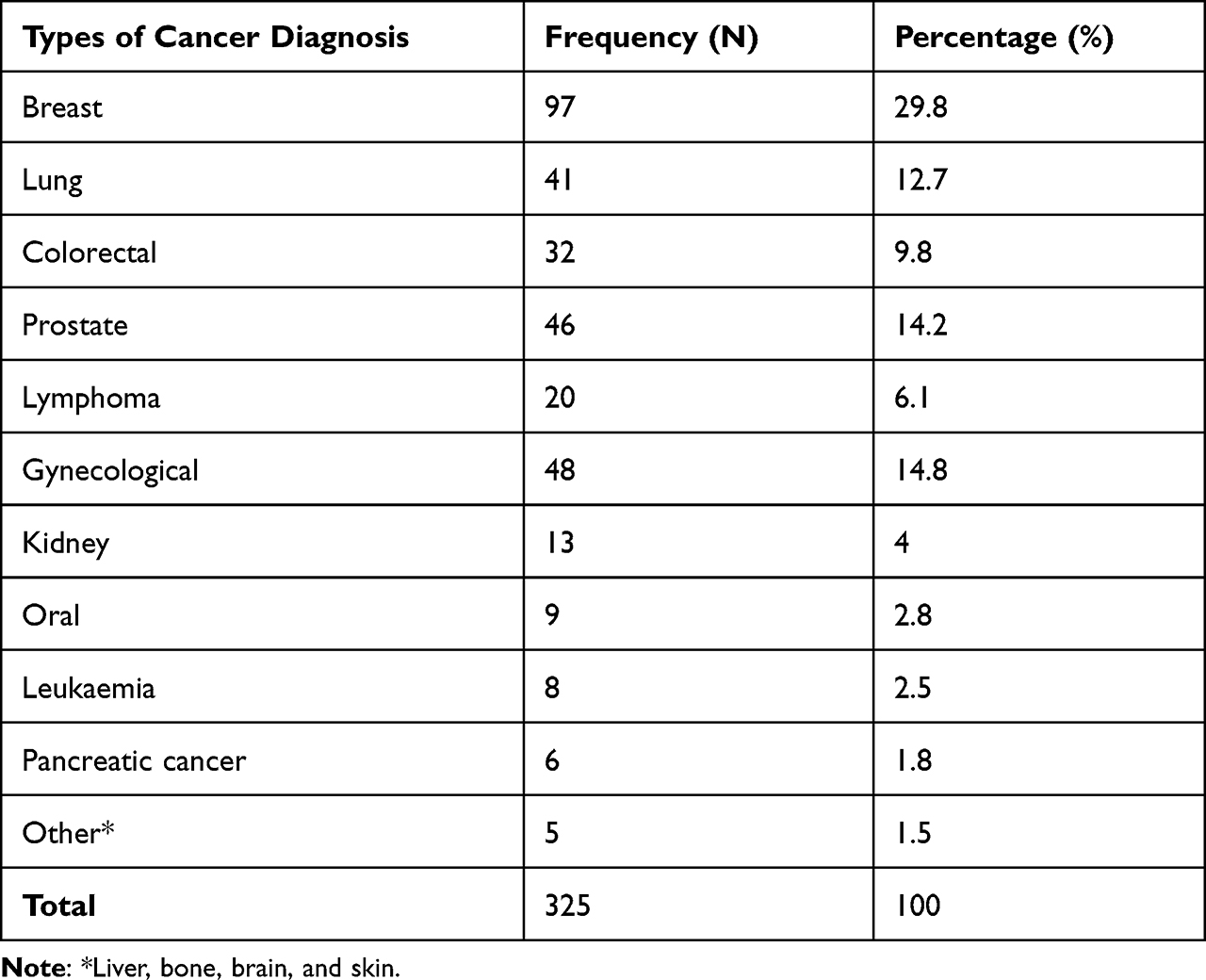 |
Table 3 Types of Cancer Diagnosis Among Adults with Cancer Diagnoses at Hawassa Comprehensive Specialized Hospital, Ethiopia, 2021 (n = 325) |
Utilization of Rehabilitation Services and Types of Rehabilitation Services Obtained
The overall utilization of rehabilitation services was found to be 33.2% (95% CI; 25.93–41.25). The most common types of rehabilitation services obtained were pain management (93.5%), treatment of side effects (69.4%), and, physical therapy (PT) (68.5%) (Table 4).
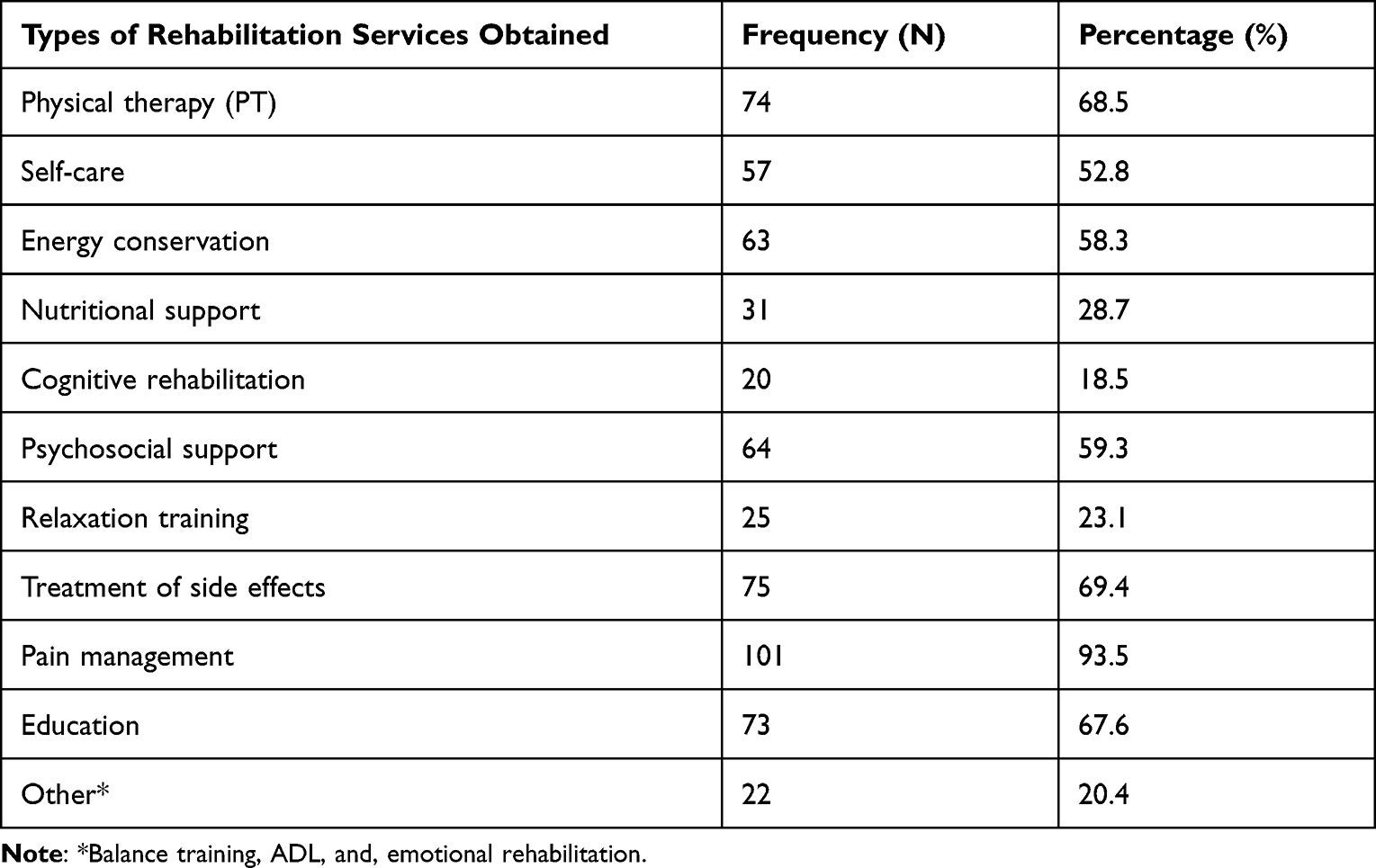 |
Table 4 Types of Rehabilitation Services Obtained by Adults with Cancer Diagnoses at Hawassa Comprehensive Specialized Hospital, Ethiopia, 2021 (n = 108) |
Factors Associated with Utilization of Rehabilitation Services
Multivariable logistic regression analysis demonstrated that sex, residence, ability to perform the activity of daily living, education on rehabilitation services, social support, and satisfaction with cancer care were significantly associated with utilization of rehabilitation services. Male participants were almost six [AOR = 5.76 (95% CI: 2.60, 12.75)] times more likely to utilize rehabilitation services when compared with females. Participants living in urban were 2.56 [AOR = 2.56 (95% CI: 1.04, 6.26)] times more likely to utilize rehabilitation services when compared with their counterparts. The odds of the utilization of rehabilitation services were 2.68 [AOR = 2.68 (95% CI: 1.20, 6.00)] times higher among participants who could perform the activities of daily living independently compared with their counterparts. Participants who received education on cancer rehabilitation services were 2.44 [AOR = 2.44 (95% CI: 1.21, 4.91)] times more likely to utilize rehabilitation services when compared with participants who have not received an education. The odds of the utilization of rehabilitation services were 3.21[AOR = 3.21 (95% CI: 1.42, 5.76)] times higher among participants who were satisfied with the cancer care received when compared with those unsatisfied. Moreover, participants having strong social support were twice 2.10 [AOR = 2.10 (95% CI: 1.02, 4.87)] more likely to utilize rehabilitation services when compared with those having poor social support (Table 5).
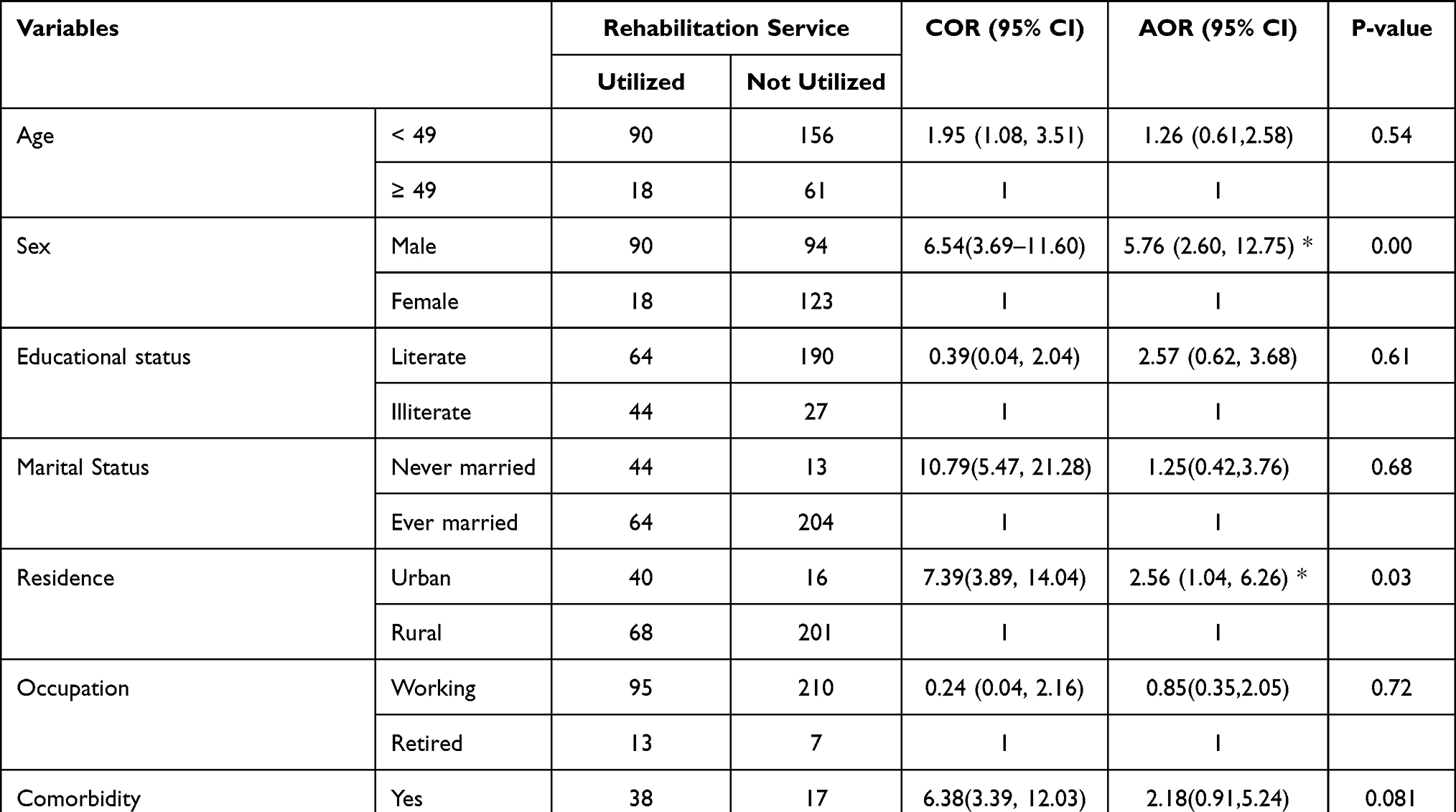 |
Table 5 Factors Associated with Utilization of Rehabilitation Services Among Adults with Cancer Diagnoses at Hawassa Comprehensive Specialized Hospital, Ethiopia, 2021 (n = 325) |
Discussion
This study was conducted to assess the utilization of rehabilitation services and associated factors among adults with a cancer diagnosis at Hawassa Comprehensive Specialized Hospital, Ethiopia. According to this study, the overall utilization of rehabilitation services among cancer patients was 33.2%. Sex, residence, ability to perform the activity of daily living, education on rehabilitation services, social support, and satisfaction with cancer care were significantly associated with the utilization of rehabilitation services.
In the current study, the overall utilization of rehabilitation services among adults with a cancer diagnosis was 33.2% (95% CI; 25.93–41.25). This finding is almost consistent with the previous study conducted at Black Lion hospital, Addis Ababa, Ethiopia (26%).23 Ethiopia has built six specialized cancer treatment centers, including the Hawassa Comprehensive Specialized Hospital Cancer Center, which offers comprehensive cancer care as well as cancer rehabilitation. Cancer rehabilitation services, on the other hand, are still underutilized. The finding of this study is, however, lower than those of studies conducted in developed countries like Norway (63%)32 and Sweden (57%).33 The possible explanation for the discrepancies might be because there are enormous differences in the socio-demographic status, health policy and health care delivery system, infrastructure, and accessibility of the rehabilitative services.
In this study, there is a significant association between sex and the utilization of rehabilitation services. Males were more likely to utilize rehabilitation services when compared with females. However, previous studies in Ethiopia on the utilization of modern healthcare services revealed that females use healthcare services at a higher rate than males.34,35 The majority of our study participants were from rural areas, thus females may not be able to travel alone to seek rehabilitation services, which is one possible explanation. Moreover, studies revealed women in low- and middle-income nations do not have equal access to healthcare as males.36,37
The finding of this study revealed that urban residents were more likely to utilize rehabilitation services. Previous research has shown that the location of one’s residence has a significant impact on healthcare utilization.38 Access to health care determines its use, and rehabilitation services are mostly found in cities. The six newly built cancer centers in Ethiopia, including the Hawassa Comprehensive Specialized Hospital Cancer Center, are all in cities (Adis Abeba, Gondor, Jima, Hawassa, Mekele, and Harar). Moreover, most of our study participants were rural dwellers.
The ability to perform the activities of daily livings (ADLs) independently was significantly associated with the utilization of rehabilitation services. This finding is supported by the study conducted in Ethiopia.23 The possible reason might be because ADLs are necessary and routine tasks that healthy people can perform independently and mainly involve mobility and those without mobility may find it difficult to access healthcare services.
Receiving education on cancer rehabilitation services was significantly associated with the utilization of rehabilitation services. This finding is supported by a study conducted in Taiwan which revealed that lack of awareness was a factor in the underutilization of rehabilitative services.18 This might be because people may not fully and effectively utilize a service if they are unaware of its availability, type, costs, and benefits. Lack of awareness of the service’s availability can be a barrier to utilization, resulting in people’s rehabilitation needs not being met.17
In this study, social support was positively associated with the utilization of rehabilitation services. This finding is supported by studies conducted in Germany11 and UK.17 The possible explanation for this finding is that social support has a direct and modifying effect on healthcare service utilization as indicated in previous literature.39,40 Furthermore, this study showed that satisfaction with cancer care is significantly associated with the utilization of rehabilitation services. This might be because patient satisfaction is one of the desired outcomes of health care and is directly correlated to the use of healthcare services. Patient satisfaction has been shown in previous studies to lead to increased utilization of healthcare services.41
Finally, this study has some limitations. Since this was a cross-sectional study, a causal relationship between the study’s dependent and independent variables could not be established. The study also assessed findings on a single point in time therefore, factors associated with the utilization of rehabilitation services outside of the study period could not be studied. The questionnaire was prone to social desirability bias.
Conclusion and Recommendation
Only 33.2% of adults with cancer diagnoses utilized rehabilitation services. Males, urban residents, those able to perform activities of daily living, those who received rehabilitation education, those with strong social support, and those satisfied with cancer care were all more likely to utilize the rehabilitation service. To improve the utilization of rehabilitation services, patients should receive adequate education on the benefits of rehabilitation, and there should be routine screening for rehabilitation needs to facilitate referral. Special attention should be given to patients coming from rural areas and female patients. Furthermore, future research should focus on how patients perceive and value cancer rehabilitation, as well as access and cost-related barriers.
Abbreviations
ADL, Activity of Daily Living; AOR, Adjusted Odds Ratio; CI, Confidence Interval; SD, Standard deviation; SPSS, Statistical Package for the Social Sciences; UK, United Kingdom.
Ethical Approval and Consent to Participate
The study was carried out in accordance with the Helsinki Declaration, and ethical approval was obtained from Haramaya University College of Health and Medical Sciences Institutional Health Research Ethics Review Committee (IHRERC). Written informed voluntary consent was obtained from study participants. The confidentiality of the information was ensured throughout the data collection period.
Acknowledgments
Firstly, we would like to forward our kindest regards to our study participants. We extend our thanks to all data collectors and supervisors they are the backbone to finalize the report. In conclusion, the authors would forward great thanks to Haramaya University for minimal financial support.
Author Contributions
All authors contributed significantly to the work reported, whether in the conception, study design, execution, data acquisition, analysis, and interpretation; participated in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article was submitted; and agreed to accept responsibility and accountability for all aspects of the work.
Funding
Haramaya University has provided financial support for this study. The authors declared that the funding body had no role in designing the study, data collection, data analysis, and writing the manuscript.
Disclosure
The authors declared no conflicts of interest in relation to this work.
References
1. Solomon S, Mulugeta W. Diagnosis and risk factors of advanced cancers in Ethiopia. J Cancer Prevent. 2019;24(3):163. doi:10.15430/JCP.2019.24.3.163
2. Sung H, Ferlay J, Siegel RL, et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2021;71(3):209–249. doi:10.3322/caac.21660
3. Levin P. World cancer report. World Health Organization; 2008.
4. Duncan K, Cira MK, Barango P, Trimble EL. Challenges and opportunities in the creation and implementation of cancer-control plans in Africa. Ecancermedicalscience. 2019;13:938. doi:10.3332/ecancer.2019.938
5. Sharma R, Aashima NM, Fronterre C, et al. Mapping cancer in Africa: a comprehensive and comparable characterization of 34 cancer types using estimates from GLOBOCAN 2020. Front Public Health. 2022;10. doi:10.3389/fpubh.2022.839835
6. Ferlay J, Shin H, Bray F, Forman D, Mathers C, Parkin D. GLOBOCAN 2008, Cancer incidence and mortality worldwide: IARC CancerBase No. 10. Lyon, France. International Agency for Research on Cancer; 2008.
7. Memirie ST, Habtemariam MK, Asefa M, et al. Estimates of cancer incidence in Ethiopia in 2015 using population-based registry data. J Glob Oncol. 2018;4(4):1–11. doi:10.1200/JGO.17.00175
8. Jemal A, Bray F, Forman D, et al. Cancer burden in Africa and opportunities for prevention. Cancer. 2012;118(18):4372–4384. doi:10.1002/cncr.27410
9. de Boer AG. The European cancer and work network: CANWON. J Occup Rehabil. 2014;24(3):393–398. doi:10.1007/s10926-013-9474-5
10. Naughton MJ, Weaver KE. Physical and mental health among cancer survivors: considerations for long-term care and quality of life. N C Med J. 2014;75(4):283–286. doi:10.18043/ncm.75.4.283
11. Aziz NM. Cancer survivorship research: state of knowledge, challenges and opportunities. Acta Oncol. 2007;46(4):417–432. doi:10.1080/02841860701367878
12. Cheville AL. Cancer rehabilitation. Semin Oncol. 2005;32(2):219–224. doi:10.1053/j.seminoncol.2004.11.009
13. Von Ah D, Storey S, Crouch A. Relationship between self-reported cognitive function and work-related outcomes in breast cancer survivors. J Cancer Surviv. 2018;12(2):246–255. doi:10.1007/s11764-017-0664-6
14. Zheng Z, Yabroff KR, Guy GP, et al. Annual medical expenditure and productivity loss among colorectal, female breast, and prostate cancer survivors in the United States. J Natl Cancer Inst. 2016;108(5):5. doi:10.1093/jnci/djv382
15. Miller KD, Nogueira L, Mariotto AB, et al. Cancer treatment and survivorship statistics, 2019. CA Cancer J Clin. 2019;69(5):363–385. doi:10.3322/caac.21565
16. World Health Organization. Rehabilitation; 2021. Available from: https://www.who.int/news-room/fact-sheets/detail/rehabilitation.
17. Csontos JK, Fitzsimmons D, Jones M, et al. Realist evaluation of cancer rehabilitation services in South Wales (REEACaRS): a mixed methods study protocol. BMJ open. 2019;9(4):e025953–e025953. doi:10.1136/bmjopen-2018-025953
18. Lin H-F, Wu Y-T, Tsauo J-Y. Utilization of rehabilitation services for inpatient with cancer in Taiwan: a descriptive analysis from national health insurance database. BMC Health Serv Res. 2012;12(1):255. doi:10.1186/1472-6963-12-255
19. Stubblefield MD. Cancer Rehabilitation. Semin Oncol. 2011;38(3):386–393. doi:10.1053/j.seminoncol.2011.03.008
20. Raj VS, Silver JK, Pugh TM, Fu JB. Palliative care and physiatry in the oncology care spectrum: an opportunity for distinct and collaborative approaches. Phys Med Rehabil Clin. 2017;28(1):35–47. doi:10.1016/j.pmr.2016.08.006
21. Stout NL, Alfano CM, Belter CW, et al. A bibliometric analysis of the landscape of cancer rehabilitation research (1992–2016). J Natl Cancer Inst. 2018;110(8):815–824. doi:10.1093/jnci/djy108
22. Kamenov K, Mills J-A, Chatterji S, Cieza A. Needs and unmet needs for rehabilitation services: a scoping review. Disabil Rehabil. 2019;41(10):1227–1237. doi:10.1080/09638288.2017.1422036
23. Worku T, Mengistu Z, Semahegn A, Tesfaye G. Rehabilitation for cancer patients at Black Lion hospital, Addis Ababa, Ethiopia: a cross-sectional study. BMC Palliat Care. 2017;16(1):1–7. doi:10.1186/s12904-017-0235-7
24. Woldeamanuel YW, Girma B, Teklu AM. Cancer in Ethiopia. Lancet Oncol. 2013;14(4):289–290. doi:10.1016/S1470-2045(12)70399-6
25. Deressa BT, Cihoric N, Badra EV, Tsikkinis A, Rauch D. Breast cancer care in northern Ethiopia – cross-sectional analysis. BMC Cancer. 2019;19(1):393. doi:10.1186/s12885-019-5612-6
26. Feleke S, Mitiku W, Zelelew H, Ashagari T. Ethiopia’s community-based health insurance: a step on the road to universal health coverage. Washington: World Bank Group; 2015.
27. Deribe B, Ayalew M, Geleta D, et al. Perceived quality of nursing care among cancer patients attending Hawassa University comprehensive specialized hospital cancer treatment center; Hawassa Southern Ethiopia: cross-sectional study. Cancer Manag Res. 2021;13:1225–1231. doi:10.2147/CMAR.S275729
28. Bona LG, Geleta D, Dulla D, et al. Economic burden of cancer on cancer patients treated at Hawassa university comprehensive specialized hospital. Cancer Control. 2021;28:10732748211009252. doi:10.1177/10732748211009252
29. Shelkey M, Wallace M. Katz index of Independence in activities of daily living (ADL). Int J Older People Nurs. 2012;2(3):204–212.
30. Hawthorne G, Sansoni J, Hayes L, Marosszeky N, Sansoni E. Measuring patient satisfaction with health care treatment using the short assessment of patient satisfaction measure delivered superior and robust satisfaction estimates. J Clin Epidemiol. 2014;67(5):527–537. doi:10.1016/j.jclinepi.2013.12.010
31. Kocalevent R-D, Berg L, Beutel ME, et al. Social support in the general population: standardization of the Oslo social support scale (OSSS-3). BMC Psychol. 2018;6(1):31. doi:10.1186/s40359-018-0249-9
32. Thorsen L, Gjerset GM, Loge JH, et al. Cancer patients’ needs for rehabilitation services. Acta Oncol. 2011;50(2):212–222. doi:10.3109/0284186X.2010.531050
33. Garmy P, Jakobsson L. Experiences of cancer rehabilitation: a cross‐sectional study. J Clin Nurs. 2018;27(9–10):2014–2021. doi:10.1111/jocn.14321
34. Bazie GW, Adimassie MT. Modern health services utilization and associated factors in North East Ethiopia. PLoS One. 2017;12(9):e0185381. doi:10.1371/journal.pone.0185381
35. Girma F, Jira C, Girma B. Health services utilization and associated factors in jimma zone, South west Ethiopia. Ethiop J Health Sci. 2011;21(Suppl 1):85–94.
36. Panezai S, Ahmad MM, Saqib SE. Factors affecting access to primary health care services in Pakistan: a gender-based analysis. Dev Pract. 2017;27(6):813–827. doi:10.1080/09614524.2017.1344188
37. Azad AD, Charles AG, Ding Q, Trickey AW, Wren SM. The gender gap and healthcare: associations between gender roles and factors affecting healthcare access in Central Malawi, June–August 2017. Arch Public Health. 2020;78(1):119. doi:10.1186/s13690-020-00497-w
38. National Academies of Sciences E, Medicine. Health-care utilization as a proxy in disability determination; 2018.
39. Lasebikan VO, Owoaje ET, Asuzu MC. Social network as a determinant of pathway to mental health service utilization among psychotic patients in a Nigerian hospital. Ann Afr Med. 2012;11(1):1. doi:10.4103/1596-3519.91010
40. Maulik PK, Eaton WW, Bradshaw CP. The role of social network and support in mental health service use: findings from the Baltimore ECA study. Psychiatr serv. 2009;60(9):1222–1229. doi:10.1176/ps.2009.60.9.1222
41. Fenny AP, Enemark U, Asante FA, Hansen KS. Patient satisfaction with primary health care–a comparison between the insured and non-insured under the National Health Insurance Policy in Ghana. Glob J Health Sci. 2014;6(4):9. doi:10.5539/gjhs.v6n4p9
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Patients’ and Relatives’ Preferences for Outpatient and Day Care Services Within End-of-Life Care in Germany – A Discrete Choice Experiment
Apolinarski B, de Jong L, Herbst FA, Huperz C, Röwer HAA, Schneider N, Damm K, Stiel S
Patient Preference and Adherence 2024, 18:519-529
Published Date: 29 February 2024
Multidimensional Sleep Health and Sleep Environment Factors in Individuals with Cancer Undergoing Outpatient Chemotherapy: An Exploratory Cross-Sectional Analysis
Adams S, Clay TD, Hasani A, Turner M, Cruickshank T
Nature and Science of Sleep 2026, 18:572577
Published Date: 17 April 2026