Back to Journals » Journal of Pain Research » Volume 19
Utility of Peripheral Nerve Block in Lower Extremity Amputation
Authors Onyewu SC, Yanez D, Nnamdi J ![]() , Onyewu MC, Effraim PR
, Onyewu MC, Effraim PR
Received 16 December 2025
Accepted for publication 23 March 2026
Published 27 March 2026 Volume 2026:19 588924
DOI https://doi.org/10.2147/JPR.S588924
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jinlei Li
Samuel C Onyewu,1 David Yanez,2 Jude Nnamdi,3 Miriam C Onyewu,4 Philip R Effraim5
1Department of Anesthesiology and Critical Care Medicine, George Washington University/George Washington University Hospital, Washington, DC, USA; 2Department of Biostatistics & Bioinformatics, Duke University School of Medicine, Duke Clinical Research Institute, Durham, NC, USA; 3First Cardiology Consultants, Lagos, Nigeria; 4Department of Global and Community Health, George Mason University, Fairfax, VA, USA; 5Department of Anesthesiology, Yale School of Medicine/Yale New Haven Hospital, New Haven, CT, USA
Correspondence: Samuel C Onyewu, Department of Anesthesiology and Critical Care Medicine, George Washington University/George Washington University Hospital, Washington, DC, USA, Tel +12024360060, Email [email protected]
Background: Approximately 200,000 limb amputations (LA) occur annually in the United States, with almost two million people living with limb loss. Phantom limb pain (PLP) is a common sequela of LA, and accounts for $12 billion in health care expenditure. The optimal anesthetic modality to reduce PLP and improve perioperative outcomes remains unclear. This study evaluated whether peripheral nerve block (PNB), used as a primary anesthetic modality, improves perioperative outcomes compared with general anesthesia (GA) in lower extremity amputation (LEA).
Methods: A single-institution retrospective review was conducted of adult patients undergoing first-time LEA between January 2019 and June 2020. Patients were stratified by anesthetic techniques: GA, PNB, neuraxial anesthesia, or GA combined with PNB. Outcomes included incidence of PLP, length of hospital stay, opioid requirements within the first 72 hours, and operative/anesthetic time. Statistical analyses included ANOVA, chi-square testing, and multivariable regression with robust standard errors.
Results: 193 records were reviewed; 179 met inclusion criteria. GA was used in 54% of cases, GA+PNB in 44%, and PNB or neuraxial anesthesia in 2%. Patients receiving PNB alone were older and had higher BMI, with a greater proportion undergoing below-knee amputation. PLP incidence was lower in GA compared with GA+PNB (8% vs 14%), though not statistically significant. Notably, no cases of PLP occurred in patients receiving PNB alone. PNB use was associated with lower opioid requirements and a significant reduction in operative time, while hospital length of stay was similar across groups. Phantom limb pain did not differ significantly between groups (GA+PNB vs GA), OR = 1.94, 95% CI [0.71, 5.28], p =0.196.
Conclusion: Overall, PNB demonstrated potential benefits in reducing opioid use and operative time, with promising findings regarding PLP prevention. These results support further prospective, randomized trial of PNB as a primary anesthetic strategy for LEA.
Keywords: phantom limb pain, lower extremity amputation, peripheral nerve block, primary anesthetic
Introduction
Lower extremity amputation (LEA), which includes above knee amputation (AKA) and below knee amputation (BKA), accounts for approximately 200 thousand cases annually in the United States (US), with approximately 2 million amputees residing in the US.1 The leading causes for LEA are failed attempts at revascularization, extensive tissue death resulting in gangrene or unabated wound infection in patients with peripheral vascular disease and diabetes. In addition, patients undergoing LEA have multiple comorbidities besides those mentioned earlier, such as hypertension, hypertensive heart disease, end-stage renal disease, coronary, cerebral, and renal vascular diseases.2 These conditions adversely impact the perioperative risk of these patients, thus influencing the anesthetic modality employed for good outcomes.
Phantom limb pain (PLP), a possible sequela of limb amputation, has an economic burden of approximately $12 billion,3 with a prevalence as high as 85% following LEA.4 The exact pathophysiology is unknown, however the postulates include: peripheral nerve injury and resultant hyperexcitability; spinal cord sensitization due to increased nociceptive signals and diminished function of the descending inhibitory pathway; cortical reorganization of the somatosensory cortex receiving projections from amputated region and surrounding areas; the sympathetic nervous system, and psychogenic mechanisms triggered by stress and anxiety.4–7 Also, adequate management of PLP has been elusive, hence, a major focus on prevention is strongly encouraged.4,5
We hypothesize that peripheral nerve block with sedation is a superior anesthetic modality in the management of lower extremity amputation (LEA) during the perioperative period when compared to general anesthesia in preventing phantom limb pain (PLP). Regional anesthesia, which includes neuraxial anesthesia and peripheral nerve block, have a few studies that have shown it is more beneficial in reducing perioperative pain when compared to general anesthesia,8,9 however, there are still conflicting data on its impact to help address the menace of PLP. Neuraxial anesthesia is fraught with multiple limitations: coagulopathy, multiple systemic effects, and impact similar to general anesthesia.10,11 Hence, we believe that peripheral nerve block (PNB), as a primary anesthetic for LEA, will lead to better perioperative outcomes, and its effectiveness in preventing PLP as a primary anesthetic is yet to be elucidated. Our premise is that PNB will prevent peripheral nerve hyperexcitability and spinal cord sensitization by precluding transmission of nociceptive signals. These are major postulates in the pathophysiology of PLP.
Our objective in this study is to elicit the utility of PNB when used as the primary anesthetic modality for LEA, on its impact to prevent/reduce the incidence of PLP, provide better perioperative pain control, address stump pain, decrease anesthetic time and cost by decreasing total intraoperative time.
Materials and Methods
Study Population
We performed a single-institutional retrospective study from January 2019 to June 2020. An Institutional Review Board (IRB) protocol was approved with protocol number 2000029598 from the Yale New Haven Hospital/Yale University. Patient informed consent was waived because this is a retrospective study, with no more than minimal risk, data was de-identified and maintained in compliance with the World Medical Association Declaration of Helsinki. Our inclusion criteria were for patients 18 years and older undergoing LEA for the first time; the patients were stratified based on the anesthetic type received. LEA was categorized as above knee amputation (AKA) and below knee amputation (BKA). Anesthetic type was stratified between general anesthesia (GA), peripheral nerve block (PNB), neuraxial anesthesia (NA), and a combination of GA+PNB. Our exclusion criteria were LEA due to trauma, amputation revision, or multiple surgeries.
Study Objectives
Our primary outcome is the incidence of phantom limb pain (PLP); secondary outcomes were length of hospital stay, opioid requirement in the first 72 hours, and intraoperative/anesthetic length of procedure.
Study Demographics and Perioperative Variables
Standard demographic data, including age, sex, and body mass index, were obtained for all patients. The type of surgery (ie, amputation level), length of stay at the hospital, and operating time were all recorded for every patient.
Statistical Analysis
We summarized patient characteristics using means and standard deviations (SD) by surgery type for quantitative characteristics and frequencies, with percentages for categorical characteristics. We performed unadjusted comparisons of quantitative characteristics for the four anesthetic types using ANOVA and chi-square tests of homogeneity for categorical characteristics and anesthetic types. We used logistic regression analysis with robust (sandwich) standard errors for the analysis of phantom limb pain, adjusting for baseline morphine milligram equivalent (MME). We used linear regression with robust standard errors for the secondary outcomes. All hypothesis tests, p-values, and confidence intervals are two-sided. All analyses were conducted using the Stata (version 16.0) statistical package.
Results
We reviewed 193 records, and 179 met our criteria. Figure 1 shows a pictorial representation of the different anesthetic types received by these patients. GA was performed in 54% of cases, while GA+PNB was performed in 44% of cases, and the remaining 2% were PNB and NA. Patients who had GA only were older, with a mean age of 65 years vs. 62 years when compared to patients with GA+PNB; they also had more AKA, 46% vs. 33%, when compared to GA+PNB patients, although these differences were not statistically significant (Table 1). Patients who received PNB only were the oldest, with a mean age of 71 years, had the highest BMI (31.7), and had more BKAs (67%) when compared to patients with GA and GA+PNB. In addition, patients who underwent GA had lower BMI (25.1 vs. 28) than those with GA+PNB (Table 1).
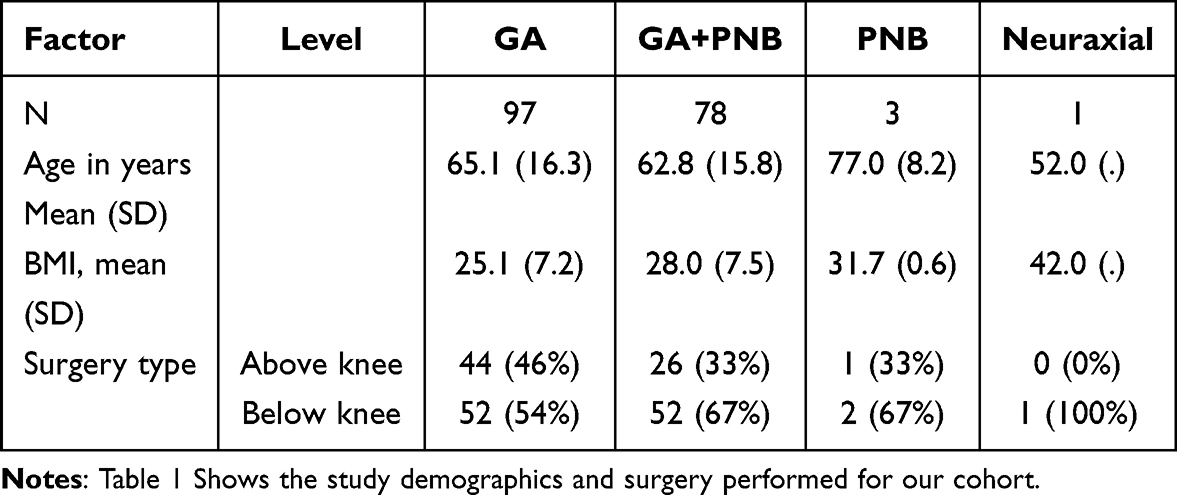 |
Table 1 Study Demographics |
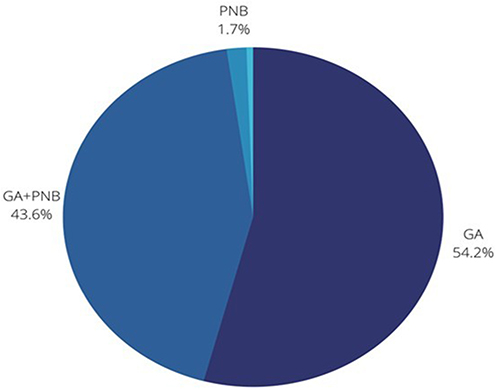 |
Figure 1 Pie Chart showing the frequency of anesthetic type in percentages. Abbreviations: PNB+, Peripheral nerve block; GA, General Anesthesia; GA+PNB, General Anesthesia + Peripheral Nerve Block. |
The incidence of phantom limb pain was 6% less likely to occur when patients received GA compared to GA+PNB (incidence of 8% and 14%, respectively), while perioperative opioid consumption was higher in GA patients when compared to GA+PNB patients, although these data were not statistically significant (Table 2). Patients with PNB had no incidence of phantom limb pain, required fewer intraoperative opioids, and had a similar length of hospital stay as patients with GA, ie., 10 days (Table 3). In addition, patients who underwent GA spent approximately 1 day less in the hospital (10 vs. 10.9 days) when compared to patients with GA+PNB. Also, this data was not statistically significant (Table 2). Finally, operative time was 24 minutes less for GA patients (123 minutes vs. 147 minutes) when compared to GA+PNB patients; this data was statistically significant (Table 2). Patients who received general anesthesia plus peripheral nerve block had 1.94 times the odds of developing phantom limb pain compared to those who received general anesthesia alone, but this difference was not statistically significant, p =0.196, 95% CI [0.71, 5.28] (Table 4). In addition, length of stay did not differ significantly between groups. Patients receiving general anesthesia plus nerve block stayed 0.93 days longer on average, but this was not statistically significant, p =0.615, 95% CI [–2.71, 4.57] (Table 4). In contrast, operation time was significantly longer in the general anesthesia plus nerve block group, with procedures taking 22.9 minutes more on average, p =0.007, 95% CI [6.36, 39.5] (Table 4).
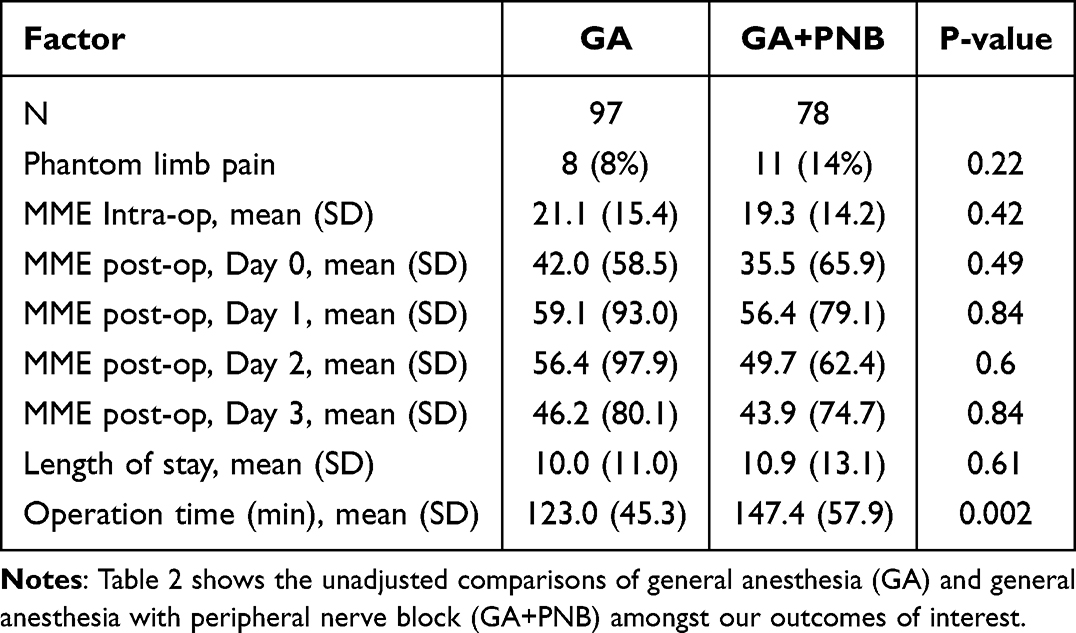 |
Table 2 PLP and MME Comparison Between General Anesthesia and General Anesthesia + PNB |
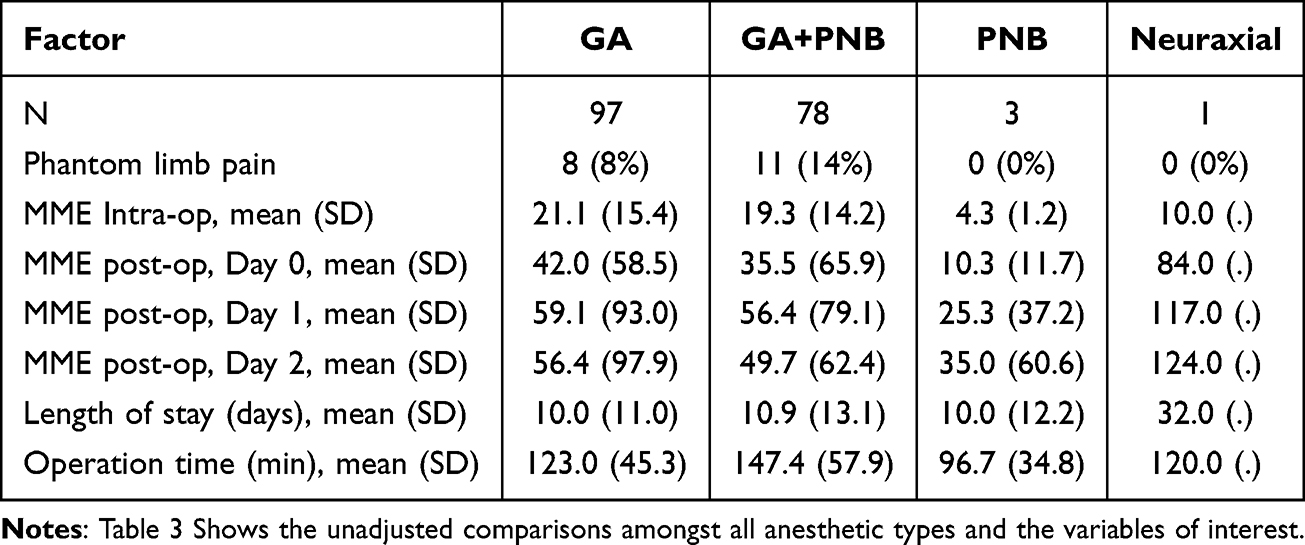 |
Table 3 PLP and MME Comparison Between All Anesthetic Groups |
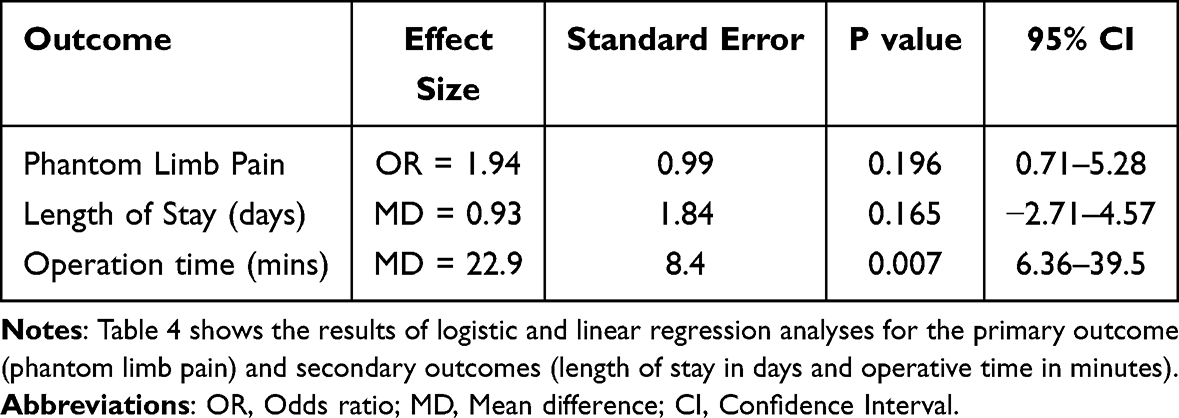 |
Table 4 Regression Analysis for the Primary and Secondary Outcomes |
Discussion
In our present analysis, our study showed that patients who received PNB only trended towards requiring lower amounts of intraoperative and postoperative opioids, and no diagnosis of PLP, although the data were not statistically significant. This data was obtained following a chart review of up to 18 months post-surgery looking for an ICD 10 diagnosis code for these patients. Prior studies have also shown that the use of a perineural infusion catheter effectively reduced postamputation opioid analgesic consumption while also providing adequate postoperative pain control.12–15 Reducing postamputation opioid use while also maintaining adequate postoperative pain control, especially amongst elderly patients, helps mitigate the multiple adverse side effects of opioid analgesics. These include respiratory depression, immune suppression, tolerance and risk of addiction.14,15 There was also a statistically significant reduction in operative time when PNB only was employed; a similar observational study also showed a statistically significant reduction in operation and anesthesia time.16 Taken together, this would suggest that there are benefits to the utilization of PNBs in LEA.
For the other anesthetic types, GA showed a trend towards a lower likelihood of PLP when compared to the GA+PNB group. Following adjusted analysis, GA+PNB patients had about twice the likelihood of developing PLP when compared to GA only patients. This finding, is surprising and in contrast with a population-based retrospective cohort study which showed PNB to be most effective in reducing the incidence of PLP, when compared to patients who underwent general anesthesia and neuraxial anesthesia respectively.17 Sahin et al18 showed a similar finding, where there was a significant reduction of PLP in patients who underwent epidural anesthesia or PNB just in the first week postoperatively; however, beyond 14 to 17 months post-surgical procedure, the anesthetic technique had no effect on PLP and other associated phantom limb syndromes.18 Another systematic review showed conflicting results that peripheral nerve catheters (PNC) revealed no significant effect on the incidence of PLP.13 Given the benefits of opioid reduction and the low incidence of PLP overall in our study, we believe that further study is warranted. We intend to embark on a randomized prospective study to compare LEA patients who receive GA only vs. PNB with sedation only. We believe this study will be better powered to determine whether PNB has an impact in preventing the development of PLP.
The length of hospital stay between GA and GA+PNB was not statistically significant, which is similar to previous studies, which revealed that the median length of stay between patients who underwent general and regional anesthesia were similar.10,11 However, this is in contrast to some studies that showed a statistically significant reduced length of hospital stay in patients who underwent regional anesthesia.19
This study has some limitations; it is a retrospective study from a single institution with the inherent limitation of the validity, generalization, and power of the findings of the study. Also, the PNB cohort was too small to draw a strong correlation from its findings. In addition, the incidence of PLP was deduced from the ICD-10 code and may not be an accurate representation of the incidence of the disease. A few patients may not have reported their symptoms at presentation to their office visits. Despite these limitations, we believe that with better stratification of the patient cohort and adequate power, we will be able to elicit the utility of PNB as a sole anesthetic technique to combat the burden of PLP. Lastly, some of the clinical factors that could influence the anesthetic technique were not assessed, such as bleeding disorders, the presence of surgical site infection, and patient preference.
Conclusion
Our findings suggest that the use of PNB in lower extremity amputations may help improve perioperative pain management and operative time. Phantom limb pain incidence did not differ significantly between GA+PNB and GA only. In addition, length of stay also showed no significant difference between both groups. However, operative time in contrast was significantly longer in the GA+PNB group. Hence, further research is imperative to address the impact of PLP on the populace.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Owings MF, Kozak LJ. Ambulatory and inpatient procedures in the United States, 1996. Vital Health Stat. 1998;139:1–6.
2. Aulivola B, Hile CN, Hamdan AD, et al. Major lower extremity amputation: outcome of a modern series. Arch Surg. 2004;139(4):395–9;discussion399. doi:10.1001/archsurg.139.4.395
3. Healthcare Cost and Utilization Project (HCUP). Agency for healthcare research and quality; 2025. Available from: https://www.ahrq.gov/data/hcup/index.html.
4. Ephraim PL, Wegener ST, MacKenzie EJ, Dillingham TR, Pezzin LE. Phantom pain, residual limb pain, and back pain in amputees: results of a national survey. Arch Phys Med Rehabil. 2005;86(10):1910–1919. doi:10.1016/j.apmr.2005.03.031
5. Hsu E, Cohen SP. Postamputation pain: epidemiology, mechanisms, and treatment. J Pain Res. 2013;6:121–136. doi:10.2147/JPR.S32299
6. Subedi B, Grossberg GT. Phantom limb pain: mechanisms and treatment approaches. Pain Res Treat. 2011;2011:864605. doi:10.1155/2011/864605
7. Anwar F. Phantom limb pain: review of literature. Khyber Med Univ J. 2013;5(4):213–218.
8. Madabhushi L, Reuben SS, Steinberg RB, Adesioye J. The efficacy of postoperative perineural infusion of bupivacaine and clonidine after lower extremity amputation in preventing phantom limb and stump pain. J Clin Anesth. 2007;19(3):226–229. doi:10.1016/j.jclinane.2006.07.008
9. Byun SH, Lee J, Kim JH. Ultrasound-guided bilateral combined inguinal femoral and subgluteal sciatic nerve blocks for simultaneous bilateral below-knee amputations due to bilateral diabetic foot gangrene unresponsive to peripheral arterial angioplasty and bypass surgery in a coagulopathic patient on antiplatelet therapy with a history of percutaneous coronary intervention for ischemic heart disease: a case report. Medicine. 2016;95(29):e4324. doi:10.1097/MD.0000000000004324
10. Moreira CC, Farber A, Kalish JA, et al. The effect of anesthesia type on major lower extremity amputation in functionally impaired elderly patients. J Vasc Surg. 2016;63(3):696–701. doi:10.1016/j.jvs.2015.09.050
11. Pisansky AJB, Brovman EY, Kuo C, Kaye AD, Urman RD. Perioperative outcomes after regional versus general anesthesia for above the knee amputations. Ann Vasc Surg. 2018;48:53–66. doi:10.1016/j.avsg.2017.10.014
12. Ayling OG, Montbriand J, Jiang J, et al. Continuous regional anaesthesia provides effective pain management and reduces opioid requirement following major lower limb amputation. Eur J Vasc Endovasc Surg. 2014;48(5):559–564. doi:10.1016/j.ejvs.2014.07.002
13. Bosanquet DC, Glasbey JC, Stimpson A, Williams IM, Twine CP. Systematic review and meta-analysis of the efficacy of perineural local anaesthetic catheters after major lower limb amputation. Eur J Vasc Endovasc Surg. 2015;50(2):241–249. doi:10.1016/j.ejvs.2015.04.030
14. Grant AJ, Wood C. The effect of intra-neural local anaesthetic infusion on pain following major lower limb amputation. Scott Med J. 2008;53(1):4–6. doi:10.1258/RSMSMJ.53.1.4
15. Fisher A, Meller Y. Continuous postoperative regional analgesia by nerve sheath block for amputation surgery--a pilot study. Anesth Analg. 1991;72(3):300–303. doi:10.1213/00000539-199103000-00004
16. Kim SJ, Kim N, Kim EH, et al. Use of regional anesthesia for lower extremity amputation may reduce the need for perioperative vasopressors: a propensity score-matched observational study. Ther Clin Risk Manag. 2019;15:1163–1171. doi:10.2147/TCRM.S213443
17. Cho HS, Kim S, Kim CS, Kim YJ, Lee JH, Leem JG. Effects of different anesthetic techniques on the incidence of phantom limb pain after limb amputation: a population-based retrospective cohort study. Korean J Pain. 2020;33(3):267–274. doi:10.3344/kjp.2020.33.3.267
18. Sahin SH, Colak A, Arar C, et al. A retrospective trial comparing the effects of different anesthetic techniques on phantom pain after lower limb amputation. Curr Ther Res Clin Exp. 2011;72(3):127–137. doi:10.1016/j.curtheres.2011.06.001
19. Chery J, Semaan E, Darji S, Briggs WT, Yarmush J, D’Ayala M. Impact of regional versus general anesthesia on the clinical outcomes of patients undergoing major lower extremity amputation. Ann Vasc Surg. 2014;28(5):1149–1156. doi:10.1016/j.avsg.2013.07.033
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.