Back to Journals » International Journal of General Medicine » Volume 17
Using XGBoost for Predicting In-Stent Restenosis Post-DES Implantation: Role of Lymphocyte-to-Monocyte Ratio and Residual Cholesterol
Authors Hou L, Su K, He T, Zhao J, Li Y
Received 5 July 2024
Accepted for publication 2 August 2024
Published 9 August 2024 Volume 2024:17 Pages 3443—3452
DOI https://doi.org/10.2147/IJGM.S477053
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Prof. Dr. Yuriy Sirenko
Ling Hou,1,* Ke Su,2,* Ting He,1 Jinbo Zhao,2 Yuanhong Li2
1Central Hospital of Tujia and Miao Autonomous Prefecture, Hubei University of Medicine, Shiyan, Hubei Province, People’s Republic of China; 2Cardiovascular Disease Center, Central Hospital of Tujia and Miao Autonomous Prefecture, Hubei University of Medicine, Enshi, Hubei Province, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Yuanhong Li, Email [email protected]
Objective: This study aims to investigate their correlation and predictive utility for in-stent restenosis (ISR) in patients with acute coronary syndrome (ACS) following percutaneous coronary intervention (PCI).
Methods: We collected medical records of 668 patients who underwent PCI treatment from January 2022 to December 2022. Based on follow-up results (ISR defined as luminal narrowing ≥ 50% on angiography), all participants were divided into ISR and non-ISR groups. The XGBoost machine learning (ML) model was employed to identify the optimal predictive variables from a set of 31 variables. Discriminatory ability was evaluated using the area under the receiver operating characteristic (ROC) curve (AUC), while calibration and performance of the prediction models were assessed using the Hosmer-Lemeshow (HL) test and calibration plots. Clinical utility of each model was evaluated using decision curve analysis (DCA).
Results: In the XGBoost importance ranking of predictive factors, LMR and RC ranked first and fourth, respectively. The AUC of the entire XGBoost ML model was 0.8098, whereas the model using traditional stepwise backward regression, comprising five predictive factors, had an AUC of 0.706. The XGBoost model showed superior predictive performance with a higher AUC, indicating better discrimination and predictive accuracy for ISR compared to traditional methods.
Conclusion: LMR and RC are identified as cost-effective and reliable biomarkers for predicting ISR risk in ACS patients following drug-eluting stent (DES) implantation. LMR and RC represent cost-effective and reliable biomarkers for predicting ISR risk in ACS patients following drug-eluting stent implantation. Enhances the accuracy and clinical utility of ISR prediction models, offering clinicians a robust tool for risk stratification and personalized patient management.
Keywords: Lymphocyte-to-monocyte ratio, residual cholesterol, XGBoost, machine learning, in-stent restenosis, drug-eluting stent
Background
Coronary artery disease (CAD) affects around 200 million individuals worldwide, standing as a prominent contributor to chronic disease-related mortality.1 Percutaneous coronary intervention (PCI) with drug-eluting stent (DES) implantation has become the cornerstone for CAD treatment, particularly in acute coronary syndrome (ACS) cases.2 Technological advancements have substantially reduced ISR rates, transitioning from 20–30% during the bare-metal stent (BMS) era to the current 3% with second-generation DES.3 Despite these advancements, ISR remains a significant challenge, necessitating better predictive tools to identify patients at high risk. In the context of over a million annual PCIs in China, deciphering the interplay of inflammation, lipid disturbances, and residual cholesterol becomes crucial.4
Recent studies have highlighted the need for refined biomarkers and models to improve risk prediction and management of ISR. Even in the DES era, inflammation and lipid imbalances continue to underpin PCI failures.5–7 Systemic chronic inflammation, characterized by low-grade, non-infectious homeostatic imbalance, is intricately linked to alterations in lipid metabolism.8 During acute inflammatory phases, elevated triglyceride (TG) levels and decreased high-density lipoprotein (HDL) levels are observed.9–11 Lymphocyte-to-monocyte ratio (LMR) emerges as a novel inflammation biomarker,12 while triglycerides and high-density lipoprotein cholesterol serve as indicators of cardiovascular mortality risk.13
Residual cholesterol (RC), the cholesterol content in triglyceride-rich lipoproteins, plays a pivotal role. Calculating residual cholesterol involves subtracting total cholesterol (TC) minus HDL minus low-density lipoprotein (LDL).14 Prior studies have underscored inflammation’s formidable predictive role in cardiovascular disease occurrence and mortality.15 For instance, recent research has shown that residual cholesterol and inflammatory markers are significant predictors of cardiovascular outcomes, which aligns with our study’s focus on ISR. This study aims to address gaps in current ISR prediction models by incorporating novel biomarkers such as LMR and RC, which have shown promise in recent literature. In recent years, heightened attention has shifted towards the lipid profile as a critical cardiovascular risk factor and predictor.16
This study aims to address gaps in current ISR prediction models by incorporating novel biomarkers such as LMR and RC, which have shown promise in recent literature. RC, encompassing non-fasting VLDL, IDL (Intermediate-Density Lipoprotein), chylomicron remnants, fasting VLDL, and IDL, emerges as a key player.17 Elevated RC levels significantly contribute to atherosclerosis, instigating cardiac metabolic abnormalities.18 Furthermore, a compelling body of research has established a noteworthy correlation between RC and adverse cardiovascular events.19 This prompts the belief that both inflammation and lipid profiles intricately intertwine with the severity and prognosis of cardiovascular diseases, including ISR. The motivation behind this research is to enhance the predictive accuracy of ISR by integrating machine learning techniques and novel biomarkers. By incorporating LMR and RC into prediction models, our study aims to improve risk stratification and patient management in ACS cases.
Methods
According to the Declaration of Helsinki, this study received approval from the Ethics Committee of Enshi Tujia and Miao Autonomous Prefecture Central Hospital. The ethical approval number is 2023-070-001. The committee does not require patient consent for the review of medical records, thus patient informed consent was not necessary for this retrospective study. Nevertheless, to ensure ethical compliance, we have provided the editor with the approval certificate issued by the ethics committee. Firstly, this study solely collects clinical case data, ensuring no adverse effects or harm to patients. Secondly, the patient data utilized in this study is anonymized, with anonymization conducted prior to data access and analysis. Consequently, it is permissible to review patient medical records without prior consent. A total of 699 patients who underwent PCI surgery at Enshi Tujia and Miao Autonomous Prefecture Central Hospital between December 2021 and January 2023 were retrospectively selected for this study. The primary exclusion criteria included a history of coronary artery bypass grafting, heart failure, acute infections, inflammatory diseases, structural heart diseases, and renal or hepatic dysfunction, as well as patients with incomplete follow-up within 6–12 months (Figure 1). ISR defined as ≥ 50% luminal narrowing on vascular imaging during follow-up.
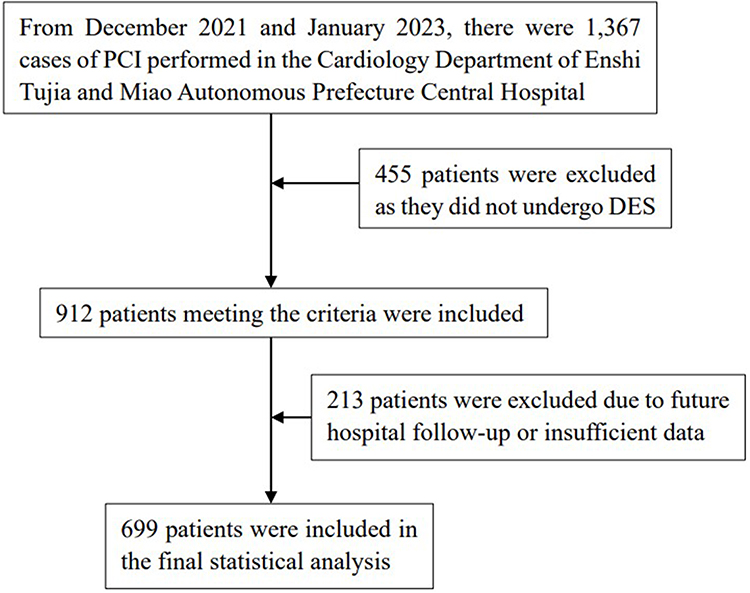 |
Figure 1 The selective procession of the participants. |
All baseline demographic, clinical, biochemical, and angiographic details of the patients were collected. Demographic and clinical data included age, gender, diabetes status, history of stroke, smoking habits, and postoperative medication (such as ACE inhibitors, beta-blockers, etc). Biochemical indicators comprised platelet distribution width (PDW), mean platelet volume (MPV), hemoglobin (Hb), alanine aminotransferase (ALT), creatinine (Cr), among others. Angiographic information recorded details about the number of stents and characteristics of the diseased vessels. All patients underwent DES implantation at the Enshi Autonomous Prefecture Central Hospital. Patients were categorized into ISR and non-ISR groups based on follow-up results from angiography. The LMR was calculated as lymphocyte count divided by monocyte count.
Student’s t-test was used to compare normally distributed continuous variables, while chi-square test or Fisher’s exact test was utilized for categorical variables. For skewed distributions, data were represented using the interquartile range (IQR), and the Mann–Whitney U-test was employed for assessment. The data were divided into training and validation sets in a 3:7 ratio, with the former used for model training and the latter for validation. KNN imputation method was employed to handle missing data to avoid selection bias. All variables from univariate analysis were included in logistic regression (stepwise regression). XGBoost, a gradient boosting algorithm, was used to incorporate all variables from univariate analysis into the model. The GDM model trained on the training set was validated on the test set using 10-fold cross-validation with the best hyperparameters. Finally, the discriminatory ability of the models was evaluated using receiver operating characteristic (ROC) curves and the area under the ROC curve (AUC). Calibration was evaluated for each model using calibration plots and the Hosmer-Lemeshow (HL) test. Decision curve analysis (DCA) was introduced to assess the clinical utility of the models. Statistical analysis was performed using R version 4.3.2.
Results
Baseline Characteristics
Table 1 shows that the baseline characteristics of this study included 549 participants with in-stent restenosis (ISR) and 119 participants without ISR. In the ISR group, the proportion of males was 69.4%, while in the non-ISR group it was 81.5%, indicating a significant difference in gender distribution (P = 0.008). There were no significant differences observed in the distribution of lesion sites, including the left main, left anterior descending, left circumflex, and right coronary arteries. Among clinical parameters, there were no significant differences between the two groups in terms of stroke history, multivessel disease, diabetes, hypertension, or the use of β-blockers and ACEI/ARB medications. The median age and Gensini score were similar between the ISR and non-ISR groups, with no significant differences observed. However, a significant difference was noted in smoking status between the two groups (P = 0.043), with a higher proportion of smokers in the non-ISR group. Laboratory parameters revealed significant differences only in RC and ALT levels between the two groups. Regarding blood parameters, there were no significant differences observed in platelet distribution width, mean platelet volume, red cell distribution width, platelet count, hemoglobin, neutrophil count, or white blood cell count between the two groups. Patients with ISR exhibited higher LMR and RC levels. Furthermore, smoking was associated with a higher incidence of ISR. Male gender and abnormal ALT levels were also identified as risk factors for ISR (P < 0.05).
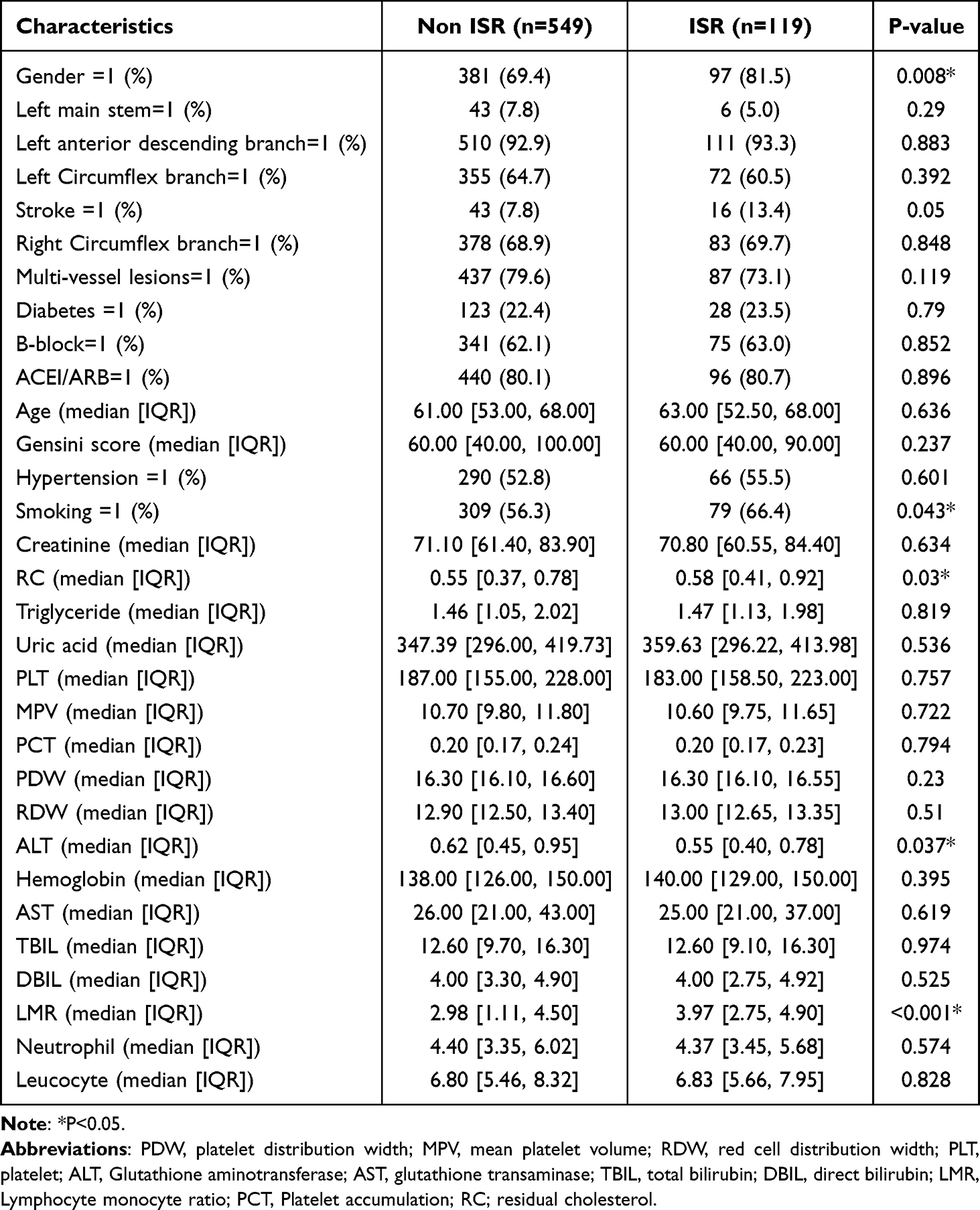 |
Table 1 The Baseline Characteristics of the Subjects Between ISR Group and Non-ISR Group |
Model Development
The prediction model constructed using logistic regression (LR) utilized five predictive factors, namely gender, PDW, multivessel disease, LMR, RC, and PDW (Table 2). Eventually, ten predictive factors were included in the XGBoost machine learning (ML) model. Figure 2 illustrates the relative importance of these ten variables in the GDM prediction model using XGBoost ML. For data from the training set, the AUC of the ISR prediction model using stepwise backward LR was 0.706 (Figure 3), while the AUC using the XGBoost ML model was 0.877 (Figure 4). The specificity of the model using XGBoost ML was higher than that of the model using traditional LR. Consequently, the sensitivity of the model using XGBoost ML was lower than that of the model using traditional LR. The calibration curves and decision curve analysis plots demonstrate the consistency between predicted values and true outcomes, as depicted in Figures 5–8. In the LR model, the p-value of the HL test for the training set was 0.337, while for the XGBoost ML model, it was 0.06. The DCA plot indicates a favorable net benefit in the XGBoost ML model.
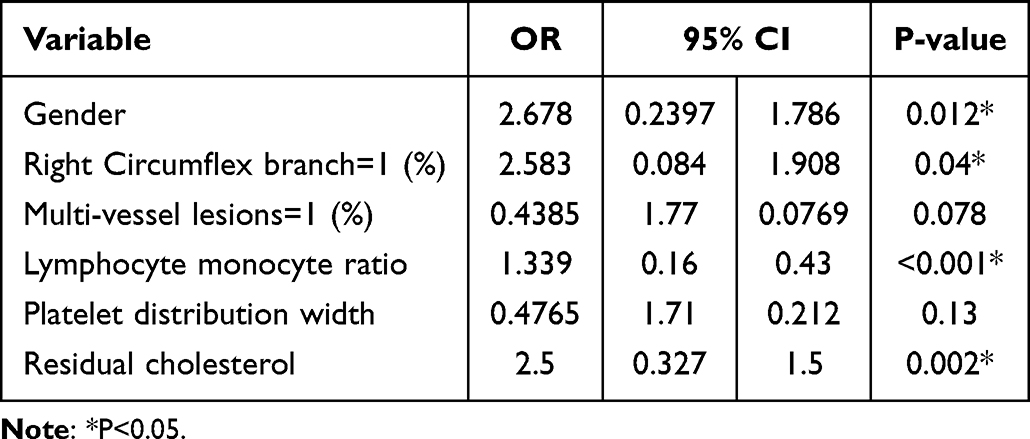 |
Table 2 Five Predictors are Included in the Model Using Stepwise LR in the Training Set |
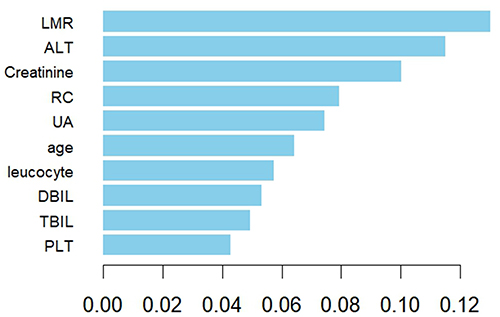 |
Figure 2 Relative Importance of the Top 10 Variables Included in the XG Boost ML Model for In-Stent Restenosis in the Training Set. |
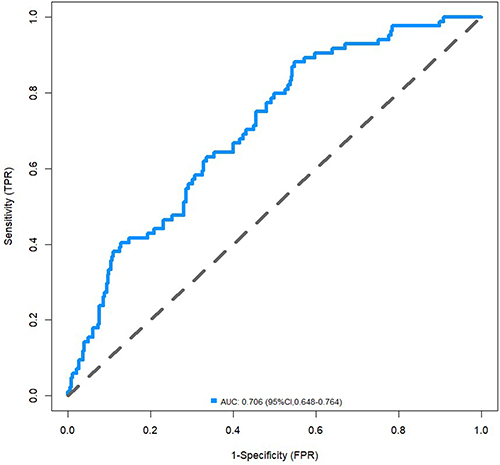 |
Figure 3 The AUC of the prediction model for ISR by stepwise LR. |
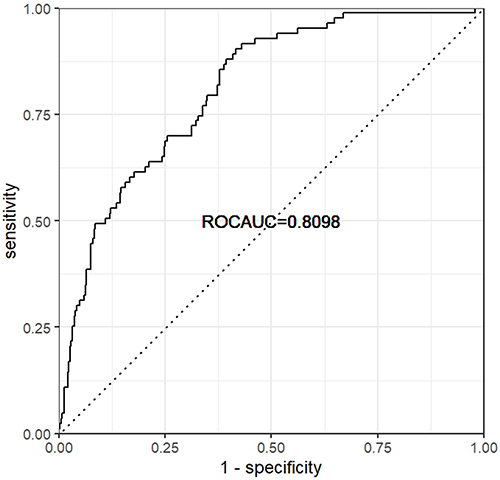 |
Figure 4 The AUC of the prediction model for ISR by XG Boost ML. |
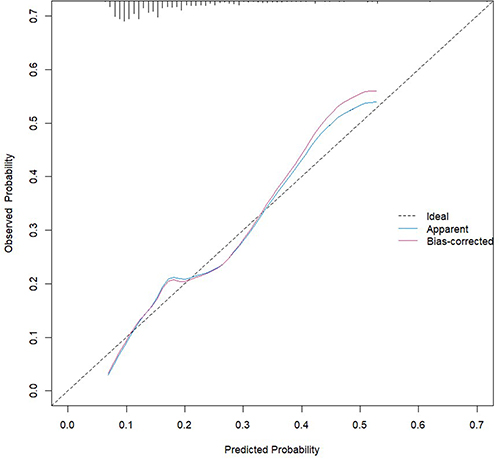 |
Figure 5 The calibration plots of the training set by LR. |
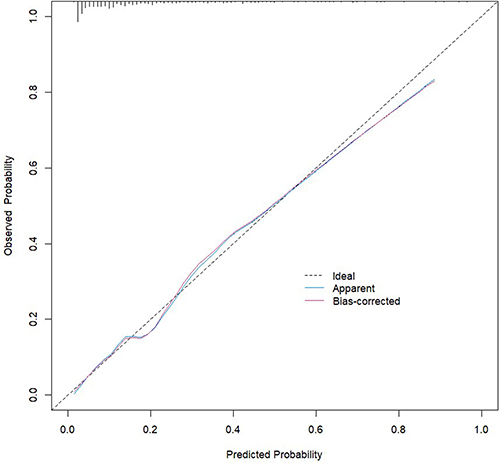 |
Figure 6 The calibration plots of the training set by XG Boost ML. |
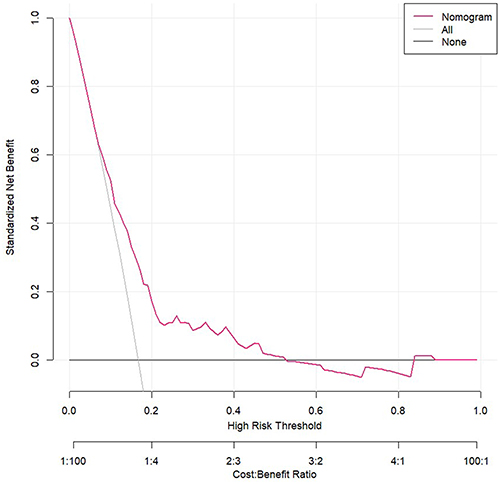 |
Figure 7 The DCA of the model using LR. |
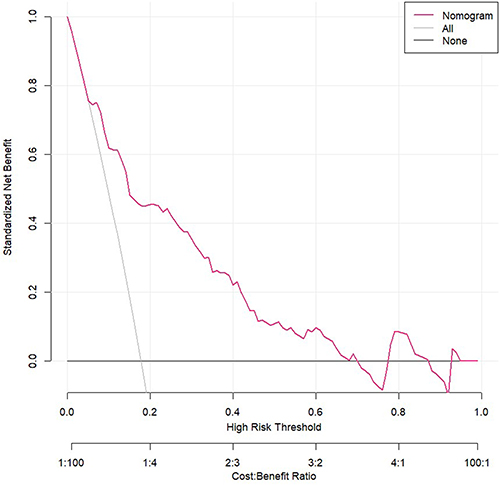 |
Figure 8 The DCA of the model using XG Boost ML. |
Discussion
Our model development process involved constructing prediction models using LR and XGBoost ML. LR model utilized five predictive factors, while XGBoost ML model incorporated ten predictive factors, including LMR and RC. Notably, XGBoost ML model demonstrated superior discrimination ability, as evidenced by its higher AUC compared to the LR model. Additionally, the specificity of the XGBoost ML model was higher, although its sensitivity was lower than that of the LR model. Calibration curves and decision curve analysis further validated the predictive performance of both models, with the XGBoost ML model exhibiting a favorable net benefit. The validation procedures for the XGBoost model included rigorous cross-validation techniques, which enhanced the reliability of the model’s performance estimates. The findings of our study highlight the potential utility of LMR and RC as biomarkers for predicting ISR risk in patients with ACS. These biomarkers provide valuable insights into the inflammatory and cholesterol-related pathways underlying ISR development. Furthermore, the application of machine learning techniques, such as XGBoost ML, enhances the predictive accuracy of ISR risk models, offering clinicians a robust tool for risk stratification and patient management.
This study explores the significant roles of dyslipidemia and inflammatory responses in cardiovascular disease progression. It specifically investigates the correlation between LMR and RC with ISR, a complex process involving inflammation and lipid accumulation.20 Chronic inflammation is crucial in cardiovascular diseases, while lipid protein accumulation promotes atherosclerotic plaque formation.21 The key finding is that LMR and RC independently act as risk factors for ISR after DES implantation.
From a clinical perspective, integrating LMR and RC into routine risk assessments could help identify patients at higher risk for ISR, leading to more personalized treatment strategies. LMR, a novel circulatory inflammatory biomarker, is crucial in predicting adverse outcomes in cardiovascular patients.22 New composite inflammatory ratios outperform traditional markers, with inflammation promoting plaque development. T-lymphocytes, macrophages, and interleukins within plaques play essential roles in cardiovascular diseases.23 Prolonged inflammation leads to smooth muscle cell proliferation and neointimal hyperplasia, causing ISR.24 While LMR predicts survival in malignancies,25–27 its role in coronary artery diseases is less explored compared to NLR.28,29 Our study addresses this gap, emphasizing LMR’s predictive value in coronary artery disease. RC represents cholesterol in triglyceride-rich lipoproteins, contributing to atherosclerosis similar to LDL.30 Elevated RC can infiltrate arterial intima, leading to localized cholesterol accumulation, atherosclerosis, neointimal formation, and ISR.31 Growing evidence highlights RC as a significant risk factor for atherosclerosis and ISR.32–34
The biological mechanisms underlying the association between LMR, RC, and ISR involve complex interactions between inflammatory and lipid pathways. While most clinical studies on in-stent restenosis (ISR) focus on lipid profiles, limited attention is given to the combined impact of lipids and inflammation.17,35,36 Research confirms that residual cholesterol infiltrates arterial walls, sparking an inflammatory response.37 Triglycerides in arterial walls induce local or systemic low-grade inflammation.38 Elevated TC in the cardiovascular system contributes to systemic inflammation. As lipid metabolism abnormalities progress, increased residual cholesterol concentration leads to extensive arterial wall infiltration, promoting foam cell formation and triggering systemic inflammation. This cascade culminates in adverse cardiovascular events, including in-stent restenosis.
In recent years, various models for predicting ISR have emerged, but our study pioneers an ISR prediction model based on LMR and RC. The constructed model exhibits excellent sensitivity and accuracy, providing a convenient tool for assessing ISR risk post DES implantation using readily available parameters. Our findings guide targeted populations for coronary angiography follow-up, potentially preventing adverse cardiovascular events and improving long-term patient prognosis. Additionally, prioritized follow-up for patients with elevated LMR or RC levels may reduce economic and clinical burdens associated with regular check-ups.
However, our study has limitations. It is single-center, introducing potential selection bias, and the voluntary nature of patient follow-up may limit generalizability. The relatively small sample size and nonsignificant differences in some clinical variables underscore the need for larger, more comprehensive studies. Future research should focus on multi-center studies to confirm our findings and evaluate the impact of potential biases. Despite these limitations, the study remains clinically significant, identifying LMR and RC predictive value for ISR.
Conclusion
LMR and RC are independent risk factors and potential predictive factors for ISR. Utilizing these inexpensive and readily available clinical markers to predict ISR incidence can enhance the long-term prognosis of CAD patients and improve their quality of life. Further studies should aim to validate these findings in diverse populations and explore the mechanistic pathways linking these biomarkers to ISR.
Funding
This work was funded by Technology Support Project of Enshi Prefecture Science and Technology Bureau (D20200018).
Disclosure
The authors have no conflicts of interest to declare in this work.
References
1. Tsao CW, Aday AW, Almarzooq ZI, et al. Heart disease and stroke statistics-2022 update: a report from the American Heart Association. Circulation. 2022;145(8):e153–e639. doi:10.1161/cir.0000000000001052
2. Head SJ, Milojevic M, Daemen J, et al. Mortality after coronary artery bypass grafting versus percutaneous coronary intervention with stenting for coronary artery disease: a pooled analysis of individual patient data. Lancet. 2018;391(10124):939–948. doi:10.1016/s0140-6736(18)30423-9
3. Giustino G, Colombo A, Camaj A, et al. Coronary in-stent restenosis: JACC State-of-the-Art review. J Am Coll Cardiol. 2022;80(4):348–372. doi:10.1016/j.jacc.2022.05.017
4. Farhan S, Redfors B, Maehara A, et al. Relationship between insulin resistance, coronary plaque, and clinical outcomes in patients with acute coronary syndromes: an analysis from the PROSPECT study. Cardiovasc Diabetol. 2021;20(1):10. doi:10.1186/s12933-020-01207-0
5. Alfonso F, Coughlan JJ, Giacoppo D, Kastrati A, Byrne RA. Management of in-stent restenosis. EuroIntervention. 2022;18(2):e103–e123. doi:10.4244/eij-d-21-01034
6. Lahmann AL, Joner M. In-stent restenosis: chasing our tails in search of a solution. JACC Basic Transl Sci. 2020;5(1):12–14. doi:10.1016/j.jacbts.2019.12.002
7. Kastrati A, Cassese S. In-Stent Restenosis in the United States: time to Enrich its Treatment Armamentarium. J Am Coll Cardiol. 2020;76(13):1532–1535. doi:10.1016/j.jacc.2020.08.035
8. Rasmussen LJH, Petersen JEV, Eugen-Olsen J. Soluble Urokinase Plasminogen Activator Receptor (suPAR) as a biomarker of systemic chronic inflammation. Front Immunol. 2021;12:780641. doi:10.3389/fimmu.2021.780641
9. Lan Y, Chen G, Wu D, et al. Temporal relationship between atherogenic dyslipidemia and inflammation and their joint cumulative effect on type 2 diabetes onset: a longitudinal cohort study. BMC Med. 2023;21(1):31. doi:10.1186/s12916-023-02729-6
10. André S, Conde B, Fragoso E, Boléo-Tomé JP, Areias V, Cardoso J. COPD and Cardiovascular Disease. Pulmonology. 2019;25(3):168–176. doi:10.1016/j.pulmoe.2018.09.006
11. Liberale L, Badimon L, Montecucco F, Lüscher TF, Libby P, Camici GG. Inflammation, aging, and cardiovascular disease: JACC review topic of the week. J Am Coll Cardiol. 2022;79(8):837–847. doi:10.1016/j.jacc.2021.12.017
12. Wu XB, Huang LX, Huang ZR, et al. The lymphocyte-to-monocyte ratio predicts intracranial atherosclerotic stenosis plaque instability. Front Immunol. 2022;13:915126. doi:10.3389/fimmu.2022.915126
13. Khan SS, Fonarow GC. Very elevated high-density lipoprotein cholesterol and mortality-the good gone bad? JAMA Cardiol. 2022;7(7):681. doi:10.1001/jamacardio.2022.0924
14. Fu L, Tai S, Sun J, et al. Remnant cholesterol and its visit-to-visit variability predict cardiovascular outcomes in patients with type 2 diabetes: findings from the ACCORD cohort. Diabetes Care. 2022;45(9):2136–2143. doi:10.2337/dc21-2511
15. Silvestre-Roig C, Braster Q, Ortega-Gomez A, Soehnlein O. Neutrophils as regulators of cardiovascular inflammation. Nat Rev Cardiol. 2020;17(6):327–340. doi:10.1038/s41569-019-0326-7
16. Vesa CM, Bungau SG. Novel molecules in diabetes mellitus, dyslipidemia and cardiovascular disease. Int J Mol Sci. 2023;24(4). doi:10.3390/ijms24044029
17. Qian S, You S, Sun Y, et al. Remnant cholesterol and common carotid artery intima-media thickness in patients with ischemic stroke. Circ Cardiovasc Imaging. 2021;14(4):e010953. doi:10.1161/circimaging.120.010953
18. Hao QY, Gao JW, Yuan ZM, et al. Remnant cholesterol and the risk of coronary artery calcium progression: insights from the CARDIA and Mesa Study. Circ Cardiovasc Imaging. 2022;15(7):e014116. doi:10.1161/circimaging.122.014116
19. Baratta F, Cocomello N, Coronati M, et al. Cholesterol remnants, triglyceride-rich lipoproteins and cardiovascular risk. Int J Mol Sci. 2023;24(5). doi:10.3390/ijms24054268
20. Alfonso F, Byrne RA, Rivero F, Kastrati A. Current treatment of in-stent restenosis. J Am Coll Cardiol. 2014;63(24):2659–2673. doi:10.1016/j.jacc.2014.02.545
21. Michos ED, McEvoy JW, Blumenthal RS. Lipid management for the prevention of atherosclerotic cardiovascular disease. N Engl J Med. 2019;381(16):1557–1567. doi:10.1056/NEJMra1806939
22. Tudurachi BS, Anghel L, Tudurachi A, Sascău RA, Stătescu C. Assessment of Inflammatory Hematological Ratios (NLR, PLR, MLR, LMR and Monocyte/HDL-Cholesterol Ratio) in acute myocardial infarction and particularities in young patients. Int J Mol Sci. 2023;24(18). doi:10.3390/ijms241814378
23. Panigrahy D, Gilligan MM, Serhan CN, Kashfi K. Resolution of inflammation: an organizing principle in biology and medicine. Pharmacol Ther. 2021;227:107879. doi:10.1016/j.pharmthera.2021.107879
24. Drachman DE, Simon DI. Inflammation as a mechanism and therapeutic target for in-stent restenosis. Curr Atheroscler Rep. 2005;7(1):44–49. doi:10.1007/s11883-005-0074-5
25. Mandaliya H, Jones M, Oldmeadow C, Nordman II. Prognostic biomarkers in stage IV non-small cell lung cancer (NSCLC): neutrophil to lymphocyte ratio (NLR), lymphocyte to monocyte ratio (LMR), platelet to lymphocyte ratio (PLR) and advanced lung cancer inflammation index (ALI). Transl Lung Cancer Res. 2019;8(6):886–894. doi:10.21037/tlcr.2019.11.16
26. Miyahara Y, Takashi S, Shimizu Y, Ohtsuka M. The prognostic impact of neutrophil-to-lymphocyte ratio (NLR) and lymphocyte-to-monocyte ratio (LMR) in patients with distal bile duct cancer. World J Surg Oncol. 2020;18(1):78. doi:10.1186/s12957-020-01847-2
27. Trinh H, Dzul SP, Hyder J, et al. Prognostic value of changes in neutrophil-to-lymphocyte ratio (NLR), platelet-to-lymphocyte ratio (PLR) and lymphocyte-to-monocyte ratio (LMR) for patients with cervical cancer undergoing definitive chemoradiotherapy (dCRT). Clin Chim Acta. 2020;510:711–716. doi:10.1016/j.cca.2020.09.008
28. Afari ME, Bhat T. Neutrophil to lymphocyte ratio (NLR) and cardiovascular diseases: an update. Expert Rev Cardiovasc Ther. 2016;14(5):573–577. doi:10.1586/14779072.2016.1154788
29. Balta S, Celik T, Mikhailidis DP, et al. The relation between atherosclerosis and the neutrophil-lymphocyte ratio. Clin Appl Thromb Hemost. 2016;22(5):405–411. doi:10.1177/1076029615569568
30. Varbo A, Benn M, Tybjærg-Hansen A, Jørgensen AB, Frikke-Schmidt R, Nordestgaard BG. Remnant cholesterol as a causal risk factor for ischemic heart disease. J Am Coll Cardiol. 2013;61(4):427–436. doi:10.1016/j.jacc.2012.08.1026
31. Doi T, Langsted A, Nordestgaard BG. Elevated remnant cholesterol reclassifies risk of ischemic heart disease and myocardial infarction. J Am Coll Cardiol. 2022;79(24):2383–2397. doi:10.1016/j.jacc.2022.03.384
32. Çınar T, Şaylık F, Akbulut T, et al. Evaluation of intermountain risk score for short- and long-term mortality in ST elevation myocardial infarction patients. Angiology. 2022;74(4):357–364. doi:10.1177/00033197221105753
33. Quispe R, Martin SS, Michos ED, et al. Remnant cholesterol predicts cardiovascular disease beyond LDL and ApoB: a primary prevention study. Eur Heart J. 2021;42(42):4324–4332. doi:10.1093/eurheartj/ehab432
34. Li W, Huang Z, Fang W, et al. Remnant cholesterol variability and incident ischemic stroke in the general population. Stroke. 2022;53(6):1934–1941. doi:10.1161/strokeaha.121.037756
35. Kazemian MR, Solouk A, Tan A, Seifalian AM. Preventing in-stent restenosis using lipoprotein (a), lipid and cholesterol adsorbent materials. Med Hypotheses. 2015;85(6):986–988. doi:10.1016/j.mehy.2015.08.023
36. Nakamura D, Dohi T, Ishihara T, et al. Predictors and outcomes of neoatherosclerosis in patients with in-stent restenosis. EuroIntervention. 2021;17(6):489–496. doi:10.4244/eij-d-20-00539
37. Wu BJ, Li Y, Ong KL, et al. Reduction of in-stent restenosis by cholesteryl ester transfer protein inhibition. Arterioscler Thromb Vasc Biol. 2017;37(12):2333–2341. doi:10.1161/atvbaha.117.310051
38. Leuti A, Fazio D, Fava M, Piccoli A, Oddi S, Maccarrone M. Bioactive lipids, inflammation and chronic diseases. Adv Drug Deliv Rev. 2020;159:133–169. doi:10.1016/j.addr.2020.06.028
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.