Back to Journals » Therapeutics and Clinical Risk Management » Volume 15
Using Patient Profiles To Guide The Choice Of Antihistamines In The Primary Care Setting In Malaysia: Expert Consensus And Recommendations
Authors Baharudin A ![]() , Abdul Latiff AH
, Abdul Latiff AH ![]() , Woo K, Yap FBB, Tang IP, Leong KF, Chin WS
, Woo K, Yap FBB, Tang IP, Leong KF, Chin WS ![]() , Wang DY
, Wang DY ![]()
Received 5 July 2019
Accepted for publication 14 September 2019
Published 31 October 2019 Volume 2019:15 Pages 1267—1275
DOI https://doi.org/10.2147/TCRM.S221059
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Garry Walsh
Abdullah Baharudin,1 Amir Hamzah Abdul Latiff,2 Kent Woo,3 Felix Boon-Bin Yap,4 Ing Ping Tang,5 Kin Fon Leong,6 Wai Seong Chin,7 De Yun Wang8
1Department of Otorhinolaryngology – Head and Neck Surgery, School of Medical Sciences, Universiti Sains Malaysia, Kubang Kerian, Kelantan, Malaysia; 2Allergy & Immunology Centre, Pantai Hospital Kuala Lumpur, Kuala Lumpur, Malaysia; 3Allergy and Immunology Clinic, Gleneagles Hospital Kuala Lumpur, Kuala Lumpur, Malaysia; 4Department of Dermatology, Sunway Medical Centre, Bandar Sunway, Selangor, Malaysia; 5Department of Otorhinolaryngology – Head and Neck Surgery, Faculty of Medicine & Health Sciences, University Malaysia Sarawak, Kuching, Sarawak, Malaysia; 6Department of Dermatology, Pediatric Institute, Hospital Kuala Lumpur, Kuala Lumpur, Malaysia; 7Pediatric Clinic, Dr Chin’s Child Specialist Clinic, Kuala Lumpur, Malaysia; 8Department of Otolaryngology, Yong Loo Lin School of Medicine, National University of Singapore, Singapore, Singapore
Correspondence: Abdullah Baharudin
Department of Otorhinolaryngology – Head and Neck Surgery, School of Medical Sciences, Universiti Sains Malaysia, Kubang Kerian, Kelantan 16150, Malaysia
Email [email protected]
Abstract: H1-antihistamines are recognized to be effective for conditions such as allergic rhinitis and chronic spontaneous urticaria. However, management of such conditions in the real-world primary care setting may be challenging due to diverse patient-specific considerations, the wide range of antihistamines available, choice of other treatment modalities, and the complexity of interpreting specialist treatment algorithms. Despite regular updates to international guidelines, regional/national surveys of healthcare professionals show a clear gap between guidelines and real-world practice, particularly at the primary care level. This article thus presents the consensus opinion of experts from relevant specialties in Malaysia – allergology, pediatrics, otorhinolaryngology, and dermtology – on harmonizing the use and choice of antihistamines in primary care. Patient profiling is recommended as a tool to guide primary care practitioners in prescribing the appropriate antihistamine for each patient. Patient profiling is a three-step approach that involves 1) identifying the individual’s needs; 2) reviewing patient-specific considerations; and 3) monitoring treatment response and referral to specialists in more severe or difficult-to-treat cases. Concurrently, guidelct 3ines should be reviewed and updated periodically to include recommendations that are easily actionable for primary care practitioners.
Keywords: antihistamines, primary care, patient profiling, Malaysia
Introduction
H1-antihistamines are mostly indicated for the treatment of allergic rhinitis (AR) and chronic spontaneous urticaria (CSU).1,2 H1-antihistamines downregulate H1-receptor activity by binding to and stabilizing the inactive form of the H1-receptor. They also induce anti-allergic and anti-inflammatory properties, independent of H1-receptor activity.3 First-generation antihistamines (such as diphenhydramine and chlorpheniramine), whilst efficacious, lack receptor selectivity and cross the blood-brain barrier, leading to undesirable anticholinergic effects such as sedation and dizziness.3 Second-generation antihistamines (such as loratadine, desloratadine, cetirizine, levocetirizine, fexofenadine, and bilastine) are selective for peripheral H1-receptors and do not readily cross the blood-brain barrier.4 In the primary care setting, oral antihistamines are the initial treatment of choice for AR and CSU.5 In a recent survey of over 500 Malaysian ear, nose, and throat (ENT) specialists, pharmacists, and general practitioners, antihistamines were identified as the preferred treatment for mild AR.5 This study also identified major unmet needs in local Malaysian practice, notably complaints of drowsiness associated with non-sedating antihistamines.
In primary care, general practitioners and community pharmacists frequently find themselves on the front-line of AR and CSU management, where they face the challenge of identifying and managing the conditions, with varied presentation and symptoms, in a diverse population of patients.6–10 The challenge of appropriate prescribing for diverse patients in primary care is compounded by the wide range of antihistamines available, choice of other treatment modalities, as well as the complexity of interpreting specialist treatment algorithms (treatment duration, dose increase, supportive medication, specialist referral).5,11 Moreover, there is evidence of poor concordance between patient and physician perceptions of disease severity, with patients perceiving their condition to be more severe than their physicians’ assessments suggest.12
Despite active development and regular updates to international guidelines for allergy, regional/national surveys of healthcare professionals show a clear gap between guidelines and real-world practice, particularly at primary care level.11,13 This motivates efforts to devise pragmatic guidelines to meet the challenges of primary care and real-life practice. In March 2019, an Advisory Board Meeting, sponsored by Bayer, was conducted in Kuala Lumpur, Malaysia. The meeting was attended by a group of experts from relevant specialties in Malaysia – allergology, pediatrics, otorhinolaryngology, and dermatology. This review article summarizes the consensus opinion of experts on the use of patient profiles to guide the use and choice of antihistamines in primary care to improve current management of AR and CSU.
Interpretation Of Guidelines
In the treatment of AR and CSU, H1-antihistamines are recommended in key international guidelines such as the Allergic Rhinitis and its Impact on Asthma (ARIA) guidelines14 and the European Academy of Allergology and Clinical Immunology/Global Allergy and Asthma European Network/European Dermatology Forum/World Allergy Organization (EAACI/GA(2)LEN/EDF/WAO)15 guidelines. Both guidelines advocate the use of second-generation antihistamines over first-generation14,15 due to the more favorable tolerability profile (minimal anticholinergic and sedating effects). The ARIA guidelines stratify AR by duration, symptom chronicity, and symptom severity.14 Guidance on the specifics of antihistamine choice, duration of treatment, increase or decrease in dose, and steps after a rebound in symptoms, may not be adequate for non-specialists.14 The EAACI/GA(2)LEN/EDF/WAO guidelines provide recommendations with respect to up-dosing second-generation antihistamines (up to fourfold) if symptom control of urticaria is inadequate.15 In addition, persistence of symptoms may necessitate add-on therapy to antihistamines (first with omalizumab, followed by cyclosporine), performed under the supervision of a specialist.15 Both omalizumab and cyclosporine are not commonly available in primary care. Across AR and CSU guidelines, the choice of treatment is also highly dependent on patient responses,14,15 which in turn requires accurate patient diagnosis and profiling.
Awareness of and adherence to guidelines is high among specialists, but notably lower in primary care, in Asia and elsewhere.1,5,11 Non-adherence to guidelines is reported particularly in general practitioners, many of whom still prescribe first-generation antihistamines.13 Notably, a higher proportion of pharmacists (42%) than general practitioners (11%) in Malaysia were dissatisfied with the ARIA guidelines.5 The root cause identified by the authors is that current guidelines do not provide sufficient step-wise guidance that is relevant for primary care. Examples of common questions from primary care practitioners include i) what is the maximum duration of antihistamine use; ii) what to do in the event of symptoms rebound post-treatment, iii) which antihistamines should be given to pediatric patients, busy working adults, pregnant/breastfeeding women, or elderly patients?
Given the gaps identified above in guidance for primary care, the authors recommend that primary care providers utilize patient profiling as a tool to guide the recommendation of antihistamines in the management of AR and CSU. Figure 1 describes a practical algorithm for primary care practitioners. This starts with clearly identifying the individual’s needs through patient profiling, followed by specific considerations for each type of patient, and lastly monitoring treatment response and referral to specialists when escalation in management is required.
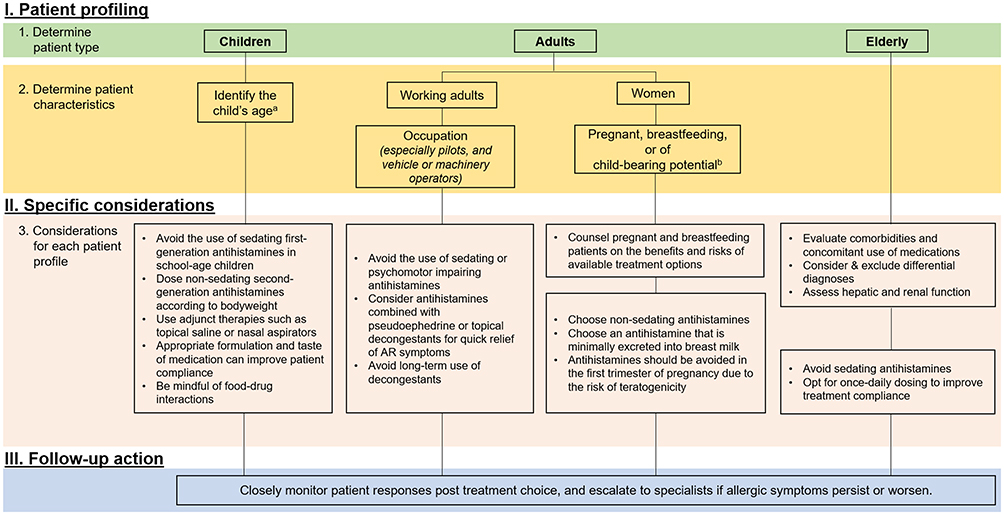 |
Figure 1 Recommended algorithm for primary care practitioners in the selection of antihistamines. aUp to 18 years old. Refer to Table 1 for licensing age and children’s doses of commonly prescribed antihistamines. b5-49 years old. |
Patient Profiles
Children
- Avoid the use of first-generation antihistamines in children due to their sedating effects.
- Dose non-sedating second-generation antihistamines according to bodyweight rather than age.
- Use adjunct therapies such as topical saline or nasal aspirators.
- Appropriate formulation and taste of medications can improve patient compliance.
- Be mindful of food–drug interactions.
- Refer to a specialist when allergic symptoms persist or worsen.
Management of AR and CSU in children is challenging due to inadequate clinical data in children.16 This is further compounded by the varying licensing age indications amongst available antihistamines (Table 117–25) and the wide array of formats, formulations and tastes.6 Currently, a proportion of physicians reportedly prescribes first-generation antihistamines in pediatric patients.13,16,26 One cited reason for this is that second-generation antihistamines are not approved for use in infants under 6 months old. However, it should be noted that first-generation antihistamines were licensed at a time when the requirements for registration of pharmaceuticals were less stringent.27 As such, first-generation antihistamines were licensed for use in the absence of clinical pharmacology and pharmacokinetic and pharmacodynamic data in children, infants, the elderly, and other special patient populations.27 In today’s context, first-generation antihistamines have little place in managing AR and CSU.28
 |
Table 1 Licensing Age And Children’s Doses Of Commonly Prescribed Antihistamines |
In school-age children, the impact of sedation on learning ability is of great concern.6,29 Uncontrolled AR impairs children’s learning ability and affects their behavioral and psychosocial development.30 Use of sedating antihistamines further affects cognitive and psychomotor performance,31 rapid eye movement sleep,32 and may also cause a paradoxical effect where children become hyperactive instead due to sleep deprivation.3 As such, the authors recommend the use of second-generation antihistamines for school-age children suffering from AR and/or CSU. For example, loratadine is a non-sedating second-generation antihistamine that has demonstrated effectiveness in managing AR in children.29,33 In a 3-week, double-blind, placebo-controlled, randomized trial involving children aged 3–12 years with AR, loratadine significantly reduced sneezing, rhinorrhea and nasal itching.33 Loratadine further minimizes allergy-induced learning impairments when compared with diphenhydramine.29 In addition, the authors recommend dosing second-generation antihistamines according to each child’s bodyweight. Adjunct therapies such as topical saline and nasal aspirators will also be useful for the symptomatic relief of AR in children.34
Medication acceptability affects treatment compliance and, in turn, treatment outcomes.35,36 The authors are in agreement that the format and taste of antihistamines is critical in pediatric care. Taste-masking of bitter drugs in liquid formulations significantly improves treatment compliance and outcome in children.33 Since it is common for parents to mix the medication with food or beverages35 to improve palatability, it is beneficial to understand the compatibility of different medicine formats with food and beverages. Food–drug interactions are also important to consider, since certain antihistamines such as fexofenadine37 and bilastine38 interact with grapefruit juice or any acidic fruit juice,39 and this decreases drug bioavailability.
Primary care practitioners should refer their pediatric patients to a specialist if symptoms persist or are not controlled with the indicated antihistamine dose.
Working Adults
- Avoid the use of sedating or psychomotor-impairing antihistamines in working adults, especially in pilots and individuals who operate vehicles or machinery.
- In the treatment of AR, enhanced relief of symptoms can be achieved with a combination of antihistamines and decongestants; however, long-term use of decongestants is discouraged because of the risk of rebound congestion.
- Primary care providers are recommended to refer patients to a specialist if symptoms cannot be controlled by indicated doses.
The symptoms of AR and CSU significantly impair quality of life both directly and indirectly, and contribute to absenteeism, presenteeism, and loss of work productivity.40,41 Incorrect choice of antihistamines can lead to poor symptom control and unwanted side effects; these in turn may impair cognitive performance and work productivity,27,32,42,43 and worsen overall quality of life.
The sedating effects of first-generation antihistamines are well documented,27,32,44 but their other adverse effects also warrant attention. Sedating antihistamines can affect rapid eye movement sleep,32 and impair cognitive and psychomotor performance,42 with potentially serious consequences in safety-critical occupations (eg, pilots, commercial vehicle drivers, or machine operators).8 Importantly, the US Federal Aviation Administration has advised pilots to use only non-sedating antihistamines such as loratadine, desloratadine, and fexofenadine.45
Due to these effects, the common but non-evidence-based practice of prescribing night-time sedating antihistamines to aid sleep should be avoided. Staevska et al showed that night-time dosing of a sedating antihistamine alongside a morning dose of non-sedating antihistamine increased daytime somnolence, but did not provide superior relief of CSU symptoms compared with non-sedating antihistamine monotherapy.46 Such findings reinforce the lack of justification for prescribing night-time sedating antihistamines to “enhance” sleep, since the effects may persist into the next day and affect performance and safety.
At the same time, it should be noted that some second-generation antihistamines such as cetirizine and levocetirizine may still induce sedation-like effects, despite being selective for peripheral H1-receptors.44,47–49 Subjective or self-reported somnolence or drowsiness has been reported with certain second-generation antihistamines, notably cetirizine.27,44,48,49 In patients with AR symptoms, cetirizine increased subjective drowsiness and significantly impaired driving performance even at a normal therapeutic dose of 10 mg, whereas loratadine (another second-generation antihistamine) did not affect performance.50 Compared with loratadine, cetirizine also significantly increased somnolence and reduced motivation during the work-day.49 Notably, drowsiness associated with “non-sedating” antihistamines was recently highlighted as an unmet need in a survey of healthcare providers in Malaysia, and may be an issue that warrants attention. Taken together, the authors advise against the use of antihistamines with sedating or psychomotor-impairing effects in working adults, especially in pilots and individuals who operate vehicles or dangerous machinery.
In the treatment of AR, antihistamines may be combined with decongestants such as pseudoephedrine (oral format) or oxymetazoline (topical format) for symptomatic relief.51,52 Specifically, loratadine combined with pseudoephedrine demonstrated enhanced and faster relief of nasal symptoms, as rapidly as 30 mins post-dosing.51 It is important to note that, although both systemic and topical decongestants can be used for short-term symptom relief, they should not be taken long-term (usually not more than 14 days due to the risk of rhinitis medicamentosa).53,54 Continued decongestant use may have other unwanted side-effects such as headache, palpitations, nervousness, insomnia,55 and dry mouth and nose.56 Based on the real-world practice of the authors and marketing authorization, the use of decongestant particularly topical decongestant should not exceed 1 week. Even though damage to nasal mucosa has only been demonstrated when used for more than 14 days, caution and restraint are advised when it is used more than 1 week as the harmful effects of decongestant are not well documented in inflamed mucosa. Therefore, the authors recommend first understanding the needs of patients in seeking treatment (eg, the urgent need for quick symptom relief), and consider recommending a combination of antihistamines with decongestants for enhanced symptom relief. However, if treatment with the standard duration fails, the primary care practitioner may need to reassess disease severity, along with the possibility of stepping up treatment as per ARIA guidelines.14 Specialist referral may also be considered.
In the treatment of CSU, the visibility of symptoms is another key consideration for patients, especially working adults.57,58 In contrast to AR, alternative medications and treatment modalities for CSU are limited in the primary care setting.15 Even so, the EAACI/GA(2)LEN/EDF/WAO guidelines recommend treatment for 2–4 weeks before considering an increase in dose of antihistamines (up to fourfold), or earlier if symptoms are intolerable.15 It should be noted that such up-dosing of antihistamines departs from the licensed indication of once-daily dosing, reflecting a gap between guideline recommendations and licensed indications. As such, the authors advocate that primary care practitioners may adjust the dose according to international guidelines and escalate cases to a specialist when the symptoms are not controlled by the indicated dose of antihistamines.
Women
- Choose non-sedating antihistamines for pregnant or breastfeeding women.
- Choose an antihistamine that is minimally excreted into breast milk.
- Choose antihistamines according to their safety profile during pregnancy.
- Counsel pregnant and breastfeeding patients on the benefits and risks of available treatment options.
- Antihistamines should be avoided in the first trimester of pregnancy due to the risk of teratogenicity.
- Refer to a specialist when in doubt or if symptoms persist or worsen.
Women of child-bearing age (15–49 years old59) represent a distinct patient profile. In this phase of life, women may be preparing for conception, pregnancy or breastfeeding. Choice of medication during pregnancy or lactation is challenging due to the lack of clinical data from well-controlled human studies (similar to the pediatric prescribing situation). The potential benefits must outweigh risks (such as potential teratogenicity) to warrant use.7,60 The authors strongly advocate for primary care practitioners to first spend time counselling pregnant or breastfeeding patients on the benefits versus risks of treatment options. Non-pharmacological management of allergic conditions during pregnancy or lactation should be prioritized.7 Where pharmacological management of symptoms of AR is required in pregnant or breastfeeding women, the authors recommend non-sedating options such as second-generation antihistamines and/or non-systemic options such as intranasal sprays. The authors’ recommendation for use of a non-sedating antihistamine during pregnancy and breastfeeding is in line with that recommended by the ARIA14 and EAACI/GA(2)LEN/EDF/WAO.15
Since high-quality clinical studies in pregnant or lactating women are lacking, the safety of existing OTC antihistamines for use during pregnancy has not been established. Antihistamines such as loratadine and cetirizine have shown no evidence of risk in animal studies (where human studies are unavailable), but updated trials are necessary to establish their safety for use during pregnancy and lactation.7,61 Of note, like other medications, antihistamines should be avoided in the first trimester of pregnancy due to the risk of teratogenicity.7 Caution should also be exercised when recommending second-generation antihistamines that affect psychomotor function, such as cetirizine.50 On breastfeeding, it should be noted that although all H1-antihistamines are excreted in breast milk in low concentrations,15 certain antihistamines, such as loratadine and fexofenadine show minimal excretion into breast milk.4
Given the potential complexities of managing AR and/or CSU in this special patient population, primary care practitioners should refer the patient to a specialist if in doubt, or if symptoms persist or worsen.
Elderly
- Prior to prescribing an antihistamine, evaluate elderly patients for comorbidities, concomitant use of medications, differential diagnoses, and assess hepatic and renal function.
- Avoid the use of sedating antihistamines in elderly patients.
- Opt for once daily dosing to improve treatment compliance.
Refer to a specialist when in doubt, or if symptoms persist or worsen.
Among the elderly in Asia, AR and CSU are more prevalent and may have greater impact than previously assumed.62–64 This may be a growing concern in Malaysia, which has a rapidly aging population. Primary care practitioners are often not the sole provider of treatment to elderly patients. As comorbidities tend to increase with age,65 elderly patients are likely to have one or more chronic comorbid conditions requiring specialist or multidisciplinary care. Polypharmacy is another important issue associated with multimorbidity.66,67 Management of elderly patients is thus challenging, especially in countries without centralized medical records.68 In patients with multiple comorbidities, management of more serious conditions such as cardiovascular disease frequently receives more attention than allergic conditions. Even though allergies may be deemed less life-threatening than cardiovascular disease or other major medical conditions, allergy symptoms such as nasal blockage and skin discomfort significantly compromise quality of life. Because the symptoms of AR and CSU can overlap with other conditions,69 the authors recommend considering differential diagnoses and excluding alternative causes prior to start of treatment. It is also important to evaluate the elderly patient’s hepatic and renal function,67 which may influence metabolism and excretion of specific drugs. Notably, loratadine, desloratadine, cetirizine, levocetirizine and fexofenadine are subject to hepatic metabolism and are excreted via the kidneys.4 Decreased hepatic or renal function may thus impair the metabolism and excretion of these drugs, and lead to adverse effects or toxicity. Dose adjustments may be necessary for patients with hepatic or renal insufficiency.67 For elderly patients, with emphasis on those with dementia, the use of sedating antihistamines should be avoided to reduce the risk of agitation and delirium.70 Patients with dementia will also benefit from once-daily dosing, which provides convenience and improves treatment compliance.9 The authors recommend prescribing only non-sedating antihistamines to elderly patients to prevent the risk of falls.
It is also important to consider cardiovascular effects when recommending antihistamines for elderly patients. Adverse cardiovascular effects have been reported with astemizole and terfenadine, which have both been withdrawn from the market and discontinued.71 Such cardiovascular adverse effects are not a class effect of H1-antagonists, but arise from overdose or interaction with drugs that are cytochrome P450 inhibitors.4,10 Good cardiovascular safety has been reported for currently available second-generation antihistamines (eg, loratadine, cetirizine) in elderly patients.72 The authors recommend that primary care practitioners should refer elderly patients to a specialist when in doubt or if symptoms persist or worsen.
Long-Term Use Of Antihistamines
- Review patient response on a regular basis to determine the appropriate duration of antihistamine use.
- Advise patients on the importance of treatment compliance for improving outcomes.
- Refer to a specialist for difficult-to-treat cases.
AR and CSU are chronic conditions, meaning that treatments such as antihistamines may have to be used on a long-term basis. Current evidence-based guidelines do not provide specific recommendations for duration of treatment and step-down/discontinuation of antihistamines. Rather, the guidelines recommend a “treat and review” approach to determine treatment duration based on patient response. This may demand specialist experience and advanced clinical judgement in some cases, and thus represents a potential gap in primary care.14,15 The ARIA guidelines provide recommendations for treatment duration (2–4 weeks) in patients with mild or moderate-to-severe persistent AR symptoms or moderate to severe intermittent AR symptoms but not for mild intermittent AR symptoms.14 The EAACI/GA(2)LEN/EDF/WAO guidelines recommend a treatment period of 2–4 weeks for CSU with indicated antihistamine doses before considering up-dosing or referral to a specialist for further evaluation.15 The authors recommend to review patient responses at 2–4 weeks according to the guidelines to decide on the appropriate duration of antihistamine use, and to consider specialist referral if in doubt.
Treatment adherence improves outcomes, but at the same time, physicians need to proactively manage potential side-effects of long-term antihistamine treatment. Safety data for the second-generation antihistamines (eg, cetirizine, desloratadine, fexofenadine, levocetirizine, and loratadine) from randomized controlled trials are only available up to 18 months.3 Longer-term safety data will be required to make better recommendations on use of antihistamines beyond 18 months. Of note, in reviewing the available treatment modalities for AR and CSU in primary care, the authors observed more options for AR and fewer for CSU in the primary care setting. For example, in moderate-severe AR, oral antihistamine treatment can be used together with an intranasal steroid spray to resolve underlying nasal inflammation while providing symptom relief. However, for CSU, the step-up alternative to antihistamines may be biologics and cyclosporine, both of which are not commonly available in primary care and should only be administered under the care of specialists.15 Alternative treatment options such as ranitidine (H2-antihistamine)15 may be considered in place of cyclosporine or omalizumab for difficult-to-treat CSU.
Conclusion
Patient profiling is an important and useful tool that will aid primary care practitioners in prescribing the appropriate antihistamine for each patient. Common patient profiles include children, working adults, women, and the elderly. Patient profiling entails a three-step approach: 1) identifying the individual’s needs; 2) considering specific considerations for each patient type; finally, 3) monitoring treatment response and referral to specialists when escalation in management is required. Specialist referral in more severe or difficult-to-treat cases is recommended by current guidelines for managing AR and CSU.
Primary care practitioners are encouraged to practice in accordance with guideline recommendations such as ARIA and EAACI/GA(2)LEN/EDF/WAO. Yet, these guidelines lack information that are pertinent to primary care practitioners (ie, stepwise guidance on the maximum duration of antihistamine use, and prescribing of antihistamines for different patient profiles). Therefore, it may be necessary for guidelines committees to review current recommendations and consider more specific and readily actionable guidance for primary care practitioners.
Acknowledgments
This manuscript was developed by Tech Observer Asia Pacific Pte Ltd., following an advisory board meeting supported by Bayer Co. (Malaysia) Sdn. Bhd. in March 2019. Bayer Co. (Malaysia) Sdn. Bhd. provided support in respect of publication costs but had no influence on the content of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Koberlein J, Vent J, Mosges R. On the sustainability of guideline implementation. World Allergy Organ J. 2010;3:258–261. doi:10.1097/WOX.0b013e3181fdfc7a
2. Kulthanan K, Chusakul S, Recto MT, et al. Economic burden of the inadequate management of allergic rhinitis and urticaria in Asian countries based on the GA(2)LEN model. Allergy Asthma Immunol Res. 2018;10:370–378. doi:10.4168/aair.2018.10.4.370
3. Simons FE, Simons KJ. Histamine and H1-antihistamines: celebrating a century of progress. J Allergy Clin Immunol. 2011;128:1139–50 e4. doi:10.1016/j.jaci.2011.09.005
4. Davila I, Del Cuvillo A, Mullol J, et al. Use of second generation H1 antihistamines in special situations. J Investig Allergol Clin Immunol. 2013;23(Suppl 1):1–16.
5. Prepageran N, Wang de Y, Nair G, Maurer M. The status quo and unmet needs in the management of allergic rhinitis and chronic rhinosinusitis: a Malaysian perspective. Asia Pac Allergy. 2014;4:142–148. doi:10.5415/apallergy.2014.4.3.142
6. Fitzsimons R, van der Poel LA, Thornhill W, du Toit G, Shah N, Brough HA. Antihistamine use in children. Arch Dis Child Educ Pract Ed. 2015;100:122–131. doi:10.1136/archdischild-2013-304446
7. Kar S, Krishnan A, Preetha K, Mohankar A. A review of antihistamines used during pregnancy. J Pharmacol Pharmacother. 2012;3:105–108. doi:10.4103/0976-500X.95503
8. Kay GG, Quig ME. Impact of sedating antihistamines on safety and productivity. Allergy Asthma Proc. 2001;22:281–283.
9. Kuna P, Jurkiewicz D, Czarnecka-Operacz MM, et al. The role and choice criteria of antihistamines in allergy management – expert opinion. Postepy Dermatol Alergol. 2016;33:397–410. doi:10.5114/pdia.2016.63942
10. McCue JD. Safety of antihistamines in the treatment of allergic rhinitis in elderly patients. Arch Fam Med. 1996;5:464–468.
11. Yang HJ, Kim YH, Lee B, et al. Unmet primary physicians’ needs for allergic rhinitis care in Korea. Allergy Asthma Immunol Res. 2017;9:265–271. doi:10.4168/aair.2017.9.3.265
12. Scadding GK, Williams A. The burden of allergic rhinitis as reported by UK patients compared with their doctors. Rhinology. 2008;46:99–106.
13. Recto MT, Gabriel MT, Kulthanan K, et al. Selecting optimal second-generation antihistamines for allergic rhinitis and urticaria in Asia. Clin Mol Allergy. 2017;15:19. doi:10.1186/s12948-017-0074-3
14. Bousquet J, Khaltaev N, Cruz AA, et al. Allergic rhinitis and its impact on asthma (ARIA) 2008 update (in collaboration with the World Health Organization, GA(2)LEN and AllerGen). Allergy. 2008;63(Suppl 86):8–160. doi:10.1111/j.1398-9995.2007.01620.x
15. Zuberbier T, Aberer W, Asero R, et al. The EAACI/GA(2)LEN/EDF/WAO guideline for the definition, classification, diagnosis and management of urticaria. Allergy. 2018;73:1393–1414. doi:10.1111/all.13397
16. Del Cuvillo A, Sastre J, Montoro J, et al. Use of antihistamines in pediatrics. J Investig Allergol Clin Immunol. 2007;17(Suppl 2):28–40.
17. Bayer Healthcare. Clarityne® Tablet & Syrup. 2015.
18. GlaxoSmithKline Pharmaceutical Sdn Bhd. ZYRTEC FILM-COATED TABLET/ORAL SOLUTION/ORAL DROPS. Cetirizine dihydrochloride (10mg, 1mg/mL, 10mg/mL). 2018.
19. HOE Pharmaceuticals Sdn. Bhd. ZORALIX 5 SF ELIXIR 5MG/5ML. 2014.
20. Kotra Pharma (M) Sdn. Bhd. AXCEL® CHLORPHENIRAMINE SYRUP.
21. Merck Sharp & Dohme (Malaysia) Sdn.Bhd. AERIUS® SYRUP. Desloratadine 0.5 mg/mL. 2018.
22. Sanofi-aventis (Malaysia) Sdn. Bhd. TELFAST® ORAL SUSPENSION. Fexofenadine hydrochloride (30mg/5ml). 2017.
23. Sunward Pharmaceutical Sdn. Bhd. POLARAX TABLET/SYRUP [AMENDED DRAFT PACKAGE INSERT]. 2019.
24. Upha Pharmaceutical Mfg. (M) Sdn. Bhd. CHLORAMINE SYRUP. 2016.
25. Xepa-Soul Pattinson (Malaysia) Sdn Bhd. Antamin™ Syrup. 2017.
26. Chainani E, Godse K, Agarwal S, Patil S. Knowledge and attitude of medical resident doctors toward antihistamines. Indian J Dermatol. 2015;60:635. doi:10.4103/0019-5154.169141
27. Simons FE, Simons KJ. H1 antihistamines: current status and future directions. World Allergy Organ J. 2008;1:145–155. doi:10.1186/s40413-018-0188-1
28. Randall KL, Hawkins CA. Antihistamines and allergy. Aust Prescr. 2018;41:41–45. doi:10.18773/austprescr.2018.013
29. Vuurman EF, van Veggel LM, Uiterwijk MM, Leutner D, O’Hanlon JF. Seasonal allergic rhinitis and antihistamine effects on children’s learning. Ann Allergy. 1993;71:121–126.
30. Blaiss MS and Allergic Rhinitis in Schoolchildren Consensus G. Allergic rhinitis and impairment issues in schoolchildren: a consensus report. Curr Med Res Opin. 2004;20:1937–1952. doi:10.1185/030079904x13266
31. Kay GG. The effects of antihistamines on cognition and performance. J Allergy Clin Immunol. 2000;105:S622–S627. doi:10.1067/mai.2000.106153
32. Church MK, Maurer M, Simons FE, et al. Risk of first-generation H(1)-antihistamines: a GA(2)LEN position paper. Allergy. 2010;65:459–466. doi:10.1111/j.1398-9995.2009.02325.x
33. Yang YH, Lin YT, Lu MY, Tsai MJ, Chiang BL. A double-blind, placebo-controlled, and randomized study of loratadine (Clarityne) syrup for the treatment of allergic rhinitis in children aged 3 to 12 years. Asian Pac J Allergy Immunol. 2001;19:171–175.
34. Garavello W, Romagnoli M, Sordo L, Gaini RM, Di Berardino C, Angrisano A. Hypersaline nasal irrigation in children with symptomatic seasonal allergic rhinitis: a randomized study. Pediatr Allergy Immunol. 2003;14:140–143.
35. Batchelor HK, Marriott JF. Formulations for children: problems and solutions. Br J Clin Pharmacol. 2015;79:405–418. doi:10.1111/bcp.12268
36. Nunn T, Williams J. Formulation of medicines for children. Br J Clin Pharmacol. 2005;59:674–676. doi:10.1111/j.1365-2125.2005.02410.x
37. Banfield C, Gupta S, Marino M, Lim J, Affrime M. Grapefruit juice reduces the oral bioavailability of fexofenadine but not desloratadine. Clin Pharmacokinet. 2002;41:311–318. doi:10.2165/00003088-200241040-00004
38. Sadaba B, Azanza JR, Gomez-Guiu A, Rodil R. Critical appraisal of bilastine for the treatment of allergic rhinoconjunctivitis and urticaria. Ther Clin Risk Manag. 2013;9:197–205. doi:10.2147/TCRM.S16079
39. Bailey DG. Fruit juice inhibition of uptake transport: a new type of food-drug interaction. Br J Clin Pharmacol. 2010;70:645–655. doi:10.1111/j.1365-2125.2010.03722.x
40. Meltzer EO, Blaiss MS, Naclerio RM, et al. Burden of allergic rhinitis: allergies in America, Latin America, and Asia-Pacific adult surveys. Allergy Asthma Proc. 2012;33(Suppl 1):S113–S141. doi:10.2500/aap.2012.33.3603
41. Yun J, Katelaris CH, Weerasinghe A, Adikari DB, Ratnayake C. Impact of chronic urticaria on the quality of life in Australian and Sri Lankan populations. Asia Pac Allergy. 2011;1:25–29. doi:10.5415/apallergy.2011.1.1.25
42. Kay GG, Berman B, Mockoviak SH, et al. Initial and steady-state effects of diphenhydramine and loratadine on sedation, cognition, mood, and psychomotor performance. Arch Intern Med. 1997;157:2350–2356.
43. Wilken JA, Berkowitz R, Kane R. Decrements in vigilance and cognitive functioning associated with ragweed-induced allergic rhinitis. Ann Allergy Asthma Immunol. 2002;89:372–380. doi:10.1016/S1081-1206(10)62038-8
44. Simons FE, Fraser TG, Reggin JD, Simons KJ. Comparison of the central nervous system effects produced by six H1-receptor antagonists. Clin Exp Allergy. 1996;26:1092–1097.
45. Guide for Aviation Medical Examiners: pharmaceuticals (Therapeutic Medications) do not Issue – do not Fly. Available from: https://www.faa.gov/about/office_org/headquarters_offices/avs/offices/aam/ame/guide/pharm/dni_dnf/.
46. Staevska M, Gugutkova M, Lazarova C, et al. Night-time sedating H1-antihistamine increases daytime somnolence but not treatment efficacy in chronic spontaneous urticaria: a randomized controlled trial. Br J Dermatol. 2014;171:148–154. doi:10.1111/bjd.12846
47. Herman D, Arnaud A, Dry J, et al. [Clinical effectiveness and tolerance of loratadine versus cetirizine in the treatment of seasonal allergic rhinitis]. Allerg Immunol (Paris). 1992;24:270–274.
48. Mann RD, Pearce GL, Dunn N, Shakir S. Sedation with “non-sedating” antihistamines: four prescription-event monitoring studies in general practice. BMJ. 2000;320:1184–1186. doi:10.1136/bmj.320.7243.1184
49. Salmun LM, Gates D, Scharf M, Greiding L, Ramon F, Heithoff K. Loratadine versus cetirizine: assessment of somnolence and motivation during the workday. Clin Ther. 2000;22:573–582. doi:10.1016/S0149-2918(00)80045-4
50. Ramaekers JG, Uiterwijk MM, O’Hanlon JF. Effects of loratadine and cetirizine on actual driving and psychometric test performance, and EEG during driving. Eur J Clin Pharmacol. 1992;42:363–369. doi:10.1007/bf00280119
51. Georgitis JW, Meltzer EO, Kaliner M, Weiler J, Berkowitz R. Onset-of-action for antihistamine and decongestant combinations during an outdoor challenge. Ann Allergy Asthma Immunol. 2000;84:451–459. doi:10.1016/S1081-1206(10)62280-6
52. Kaiser HB, Banov CH, Berkowitz RR, et al. Comparative efficacy and safety of once-daily versus twice-daily loratadine-pseudoephedrine combinations versus placebo in seasonal allergic rhinitis. Am J Ther. 1998;5:245–251.
53. Lockey RF. Rhinitis medicamentosa and the stuffy nose. J Allergy Clin Immunol. 2006;118:1017–1018. doi:10.1016/j.jaci.2006.06.018
54. Mortuaire G, de Gabory L, Francois M, et al. Rebound congestion and rhinitis medicamentosa: nasal decongestants in clinical practice. Critical review of the literature by a medical panel. Eur Ann Otorhinolaryngol Head Neck Dis. 2013;130:137–144. doi:10.1016/j.anorl.2012.09.005
55. Aaronson DW. Side effects of rhinitis medications. J Allergy Clin Immunol. 1998;101:S379–S382. doi:10.1016/s0091-6749(98)70225-8
56. Deckx L, De Sutter AI, Guo L, Mir NA, van Driel ML. Nasal decongestants in monotherapy for the common cold. Cochrane Database Syst Rev. 2016;10:CD009612.
57. Thomas J, Pandhi RK, Oberoi C, et al. A multicentric trial of loratadine and cetirizine in urticaria. Indian J Dermatol Venereol Leprol. 1998;64:12–16.
58. Zuberbier T, Munzberger C, Haustein U, et al. Double-blind crossover study of high-dose cetirizine in cholinergic urticaria. Dermatology. 1996;193:324–327. doi:10.1159/000246281
59. World Health Organization. Reproductive Health and Research. Reproductive Health Indicators: Guidelines for Their Generation, Interpretation and Analysis for Global Monitoring. Geneva: World Health Organization; 2006.
60. Mehta N, Chen K, Powrie RO. Prescribing for the pregnant patient. Cleve Clin J Med. 2014;81:367–372. doi:10.3949/ccjm.81a.13124
61. Gonzalez-Estrada A, Geraci SA. Allergy medications during pregnancy. Am J Med Sci. 2016;352:326–331. doi:10.1016/j.amjms.2016.05.030
62. Ban GY, Kim MY, Yoo HS, et al. Clinical features of elderly chronic urticaria. Korean J Intern Med. 2014;29:800–806. doi:10.3904/kjim.2014.29.6.800
63. Chuamanochan M, Kulthanan K, Tuchinda P, Chularojanamontri L, Nuchkull P. Clinical features of chronic urticaria in aging population. Asian Pac J Allergy Immunol. 2016;34:201–205. doi:10.12932/AP0708
64. Song WJ, Chang YS. Respiratory allergies in the elderly: findings from the Korean Longitudinal Study on Health and Aging phase I study (2005–2006). Asia Pac Allergy. 2017;7:185–192. doi:10.5415/apallergy.2017.7.4.185
65. Divo MJ, Martinez CH, Mannino DM. Ageing and the epidemiology of multimorbidity. Eur Respir J. 2014;44:1055–1068. doi:10.1183/09031936.00059814
66. Pinto JM, Jeswani S. Rhinitis in the geriatric population. Allergy Asthma Clin Immunol. 2010;6:10. doi:10.1186/1710-1492-6-10
67. Slavin RG. Treating rhinitis in the older population: special considerations. Allergy Asthma Clin Immunol. 2009;5:9. doi:10.1186/1710-1492-5-9
68. Bowden T, Coiera E. The role and benefits of accessing primary care patient records during unscheduled care: a systematic review. BMC Med Inform Decis Mak. 2017;17:138. doi:10.1186/s12911-017-0523-4
69. Nyenhuis SM, Mathur SK. Rhinitis in older adults. Curr Allergy Asthma Rep. 2013;13:171–177. doi:10.1007/s11882-013-0342-3
70. Maeda T, Babazono A, Nishi T. Surveillance of first-generation H1-antihistamine use for older patients with dementia in Japan: a retrospective cohort study. Curr Gerontol Geriatr Res. 2018;2018:3406210. doi:10.1155/2018/3406210
71. Olasinska-Wisniewska A, Olasinski J, Grajek S. Cardiovascular safety of antihistamines. Postepy Dermatol Alergol. 2014;31:182–186. doi:10.5114/pdia.2014.43191
72. Philpot EE. Safety of second generation antihistamines. Allergy Asthma Proc. 2000;21:15–20. doi:10.2500/108854100778249033
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.