Back to Journals » Risk Management and Healthcare Policy » Volume 15
Using Multilevel Structural Equation Modeling (MSEM) to Identify the Predictors and Influencing Mechanism of Technology Use Among Chinese Physicians: An Example from Des-Gamma-Carboxy Prothrombin (DCP)
Received 18 October 2021
Accepted for publication 12 January 2022
Published 18 January 2022 Volume 2022:15 Pages 59—70
DOI https://doi.org/10.2147/RMHP.S344923
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jongwha Chang
Qingwen Deng,1,2 Yueqin Wang,1 Wenbin Liu1
1Department of Health Management, School of Public Health, Fujian Medical University, Fuzhou, 350122, People’s Republic of China; 2School of Public Health, Fudan University, Shanghai, 200032, People’s Republic of China
Correspondence: Wenbin Liu, Department of Health Management, School of Public Health, Fujian Medical University, Fuzhou, 350122, People’s Republic of China, Tel +86 13799983766, Email [email protected]
Background: Since expanding the use of appropriate and effective health technologies will greatly benefit the diagnosis and treatment of some major diseases at an early stage, understanding the mechanism of technology use is crucial for its successful implementation. Few previous studies focused on the healthcare providers and involved multi-facets factors at individual, technical, organizational, and environmental levels.
Purpose: To examine the influencing mechanism of technology use among Chinese physicians by integrating multilevel factors, Des-gamma-Carboxy Prothrombin (DCP) was taken as an example.
Methods: Through multistage random sampling, a cross-sectional questionnaire survey was conducted among physicians in charge of direct use of DCP of sampled secondary and tertiary hospitals. Since the sample data comprised two hierarchical levels (physicians and hospitals), multilevel structural equation modeling was used to link five aspects of factors with physicians’ technology use and estimate the effects.
Results: Totally, 229 physicians completed the investigation. The use of DCP appears to be at a relatively low level. Intra-class coefficients of the null model (unadjusted baseline model) suggested that physicians’ DCP use has a significant variation between hospitals. The final model identified that value cognition (B = 0.447, P < 0.01), experienced organizational practice (B = 0.203, P < 0.05), and perceived organizational atmosphere (B = –0.237, P < 0.01) contributed directly to physicians’ DCP use. Additionally, technical assessment, perceived organizational atmosphere, and perceived environmental pressure had indirect impacts on physicians’ DCP use that were mediated by value cognition and experienced organizational practice (P < 0.05).
Conclusion: This study incorporated and determined the significant direct or indirect role of value cognition, technical assessment, experienced organizational practice, perceived organizational atmosphere, and perceived environmental pressure. This influencing mechanism with integrated multilevel factors could serve as a theoretical basis for tailoring interventions to promote technology use among Chinese physicians.
Keywords: technology use, physician, multilevel structural equation modeling, China
Introduction
It is well known that expanding the use of appropriate and effective health technologies would greatly benefit the early diagnosis and treatment of some major diseases, which would subsequently reduce the heavy burden of the corresponding diseases on individuals, families and society. For example, as one of the major diseases worldwide, liver cancer ranks the second leading cause of cancer-related deaths.1 Especially in China, the number of new cases and deaths from liver cancer increases dramatically every year, accounting for more than half of the world’s cases.2 Clinical practice shows that many patients with liver cancer are detected only after the onset of abdominal pain. By then, most cases are already in advanced stages, with extremely high treatment costs and low survival rates. Under the critical situation of liver cancer prevention and treatment, promoting the use of early diagnosis and treatment techniques for related diseases will be beneficial to improve the patients’ survival rate and quality of life, and enhance the service delivery capacity of the health system. In order to design targeted interventions that effectively promote the use of corresponding technologies, it is of great theoretical and practical significance to identify the determinants and elucidate their interactions and overall impact mechanisms.
Many theories and models have been used to explain the rationale mechanism for individual involvement in health behavior decisions about technology use and have showed great explanatory power in interpreting behaviors of healthcare professionals, such as the Theory of Planned Behavior (TPB), Innovation Diffusion Theory (IDT), Organizational Readiness for Change (ORC), and Technology-Organization-Environment framework (TOE). TPB was developed by Ajzen to understand the relationship between attitudes, subjective norms, perceived behavioral control, intentions, and behaviors.3 IDT summarizes five attributes of how an innovative product is introduced at the technological level, with compatibility and complexity frequently reported in studies of technology use.4 According to ORC, the changes of medical practitioners’ behavior should start from the organizational level, including atmosphere (eg, organizational culture) and practices (eg, systems and implementation activities).5 In addition to technical and organizational factors, TOE places particular emphasis on the effect of the external environment, such as industry pressure.6
To date, based on the above theories, a number of studies have identified and highlighted the importance of influencing factors influencing technology use from one or two of the five aspects: individual, technology, organizational atmosphere, organizational practice, and industry environment.7–10 For instance, a study by Saigí-Rubió F remarked technology characteristics and environmental pressure as determinants of healthcare professionals’ intentions to use digital clinical consultations tools.7 Liu’s study focused on predictors that shape primary care physicians’ antibiotic prescribing behavior at the individual level.8 Besides, Randall CL and Knerr reported the significance of organizational factors to the successful implementation of certain health technologies.9,10 And the association of these factors in different aspects has been sporadically documented in the previous literature. Specifically, several studies have revealed that certain technology characteristics influence physicians’ beliefs on cloud health information systems,11 the introduction of electronic health records in medical centers,12 and the industry environment of cloud computing.13 Beyond these associations, organizational practice has been found to be predicted by organizational atmosphere and industry environment, such as a study conducted in Canadian hospitals pointed out that culture served a role in program implementation14 and a cohort study confirmed that hospitals’ decisions to use surgical robots were related to regional competition.15 However, few have integrated these different perspectives and comprehensively explored the potential interactions between them. Additionally, most previous studies have focused on patients,16–18 with less attention to healthcare providers (eg, physicians).
With regard to analytic strategies, consideration of predictors has recently expanded from individual-level factors to multilevel factors;19 in particular, structural factors of the organization or life context of the research subject are continuously being valued. The hospital is one of the most important arenas in the life of a physician. Physicians’ technology use may be influenced by structural characteristics among hospitals. Evidence demonstrates that the practice behavior of health care professionals is mediated to some extent by the context in which they work.20 Failure to address interorganizational heterogeneity may cause biased results due to aggregation effects.21 To solve this issue while determining the relationship between the proposed factors, multilevel structural equation modeling (MSEM) is the best choice.22 Currently, MSEM has been used in the fields of public health policy23–25 and adolescent health,26,27 but rarely in health technology use.
Given that understanding of the mechanisms for the use of technology at multiple levels is still relatively limited, this study aims to examine the mechanisms linking the predictors and technology use in five aspects among physicians through the MSEM approach. Figure 1 displays the predictions we made in this study. To make the study more pertinent, we investigated the use of Des-gamma-Carboxy Prothrombin (DCP), a technology proven to be effective and suitable for early screening of liver cancer. The findings are promising for bridging the research gap about the mechanism of technology use among physicians.
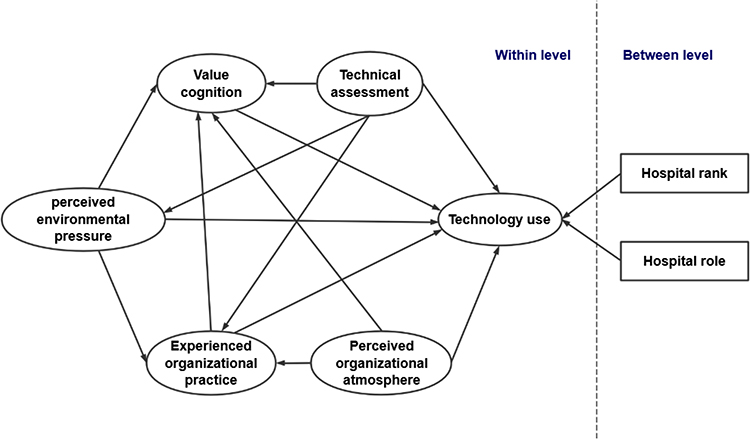 |
Figure 1 The research model of the mechanism of physicians’ technology use. |
Materials and Methods
Study Setting and Population
Since almost all health institutions at all levels are part of a set of regional medical consortiums (RMC, a model of integration of health services in China, where technical cooperation and assistance is one of its most prominent features28), and most primary health institutions do not currently have the capacity to deploy DCP, this study was implemented in secondary and tertiary hospitals that have the capacity to deploy DCP. Physicians in charge of the direct use of DCP in the aforementioned hospitals were taken as the target population and were eligible to participate.
Sampling Strategy
From February to August 2019, a cross-sectional survey was conducted using a multistage random sampling. The concrete steps included: firstly, Fujian and Jiangxi provinces were selected from provinces with high and low incidence of liver cancer, respectively; Secondly, two RMCs were selected from each province, and hospitals with the ability to deploy DCP in the two selected RMCs in each province were included at a rate of 50%; Thirdly, physicians who have knowledge of DCP and work in liver disease-related departments (including hepatology, oncology, infection, gastroenterology, interventional medicine, radiotherapy, etc.) were invited to participate. It is expected to investigate 10~20 physicians per hospital and 5~8 hospitals per RMC. Totally, at least 200 physicians were approached, which meets the sample size requirement of at least five times the survey questions.29
Study Variables
Dependent Variables
The dependent variable of this study is technology use, which derived from its related notions as follows. As described by Beyer and Estabrooks, there are three types of technology use: symbolic use (SU), conceptual use (CU) and instrumental use (IU).30,31 SU indicates increased awareness through existing research findings; CU evinces general enlightenment through research findings; IU involves the use of research findings in a specific and direct manner.
Based on the above understanding, this study assessed SU by asking physicians about their initiatives and knowledge of DCP use. CU was captured by asking them about their actions in introducing DCP to patients, colleagues and department heads. IU was also asked regarding their use of DCP in clinical practice. More details on dependent variable are available in the Supplementary File. A six-point Likert scale was used for all items, with “never”, “rarely”, “less”, “general”, “more” and “a lot” recorded as 0, 1, 2, 3, 4 and 5, respectively. And the score for each type of technology use was measured by the mean score of all items under a certain technology use.
Physician Level Variables
Five aspects are included at the physician level. Value cognition (VC) is the perception and predisposition to DCP use. According to the TPB scale, this aspect is examined by three dimensions: attitudes, subjective norms and perceived behavioral control.3 Attitudes are defined as positive or negative evaluations of DCP use; subjective norms are perceived pressure to engage or not to engage in behavior from the influential people; perceived behavioral control reflects the physicians’ beliefs that DCP use is under his or her control.
The second aspect is technical assessment (TA). In the opinion of IDT, perceived ease of use and compatibility are the two most important factors in technology use.4 In this study, ease of use refers to the degree to which DCP can be easily used; compatibility refers to the consistency between the use of DCP in physicians and their previous experience, habits and existing practical processes.
ORC theory deems physicians’ perceptions of organizational factors are important prerequisites for changing their medical behaviors.5 Due to the different focal points, the organizational factors perceived by the physicians were divided into practice-related and atmosphere-related. Experienced organizational practice (EOP) refers to a series of practical actions that promote the DCP use, including mechanism establishment, staff allocation and post-implementation communication. It consists of two dimensions: perceived support mechanism and internal diffusion. As for perceived organizational atmosphere (POA), it is the preparedness and norms of the DCP use that are collectively shared by all members within the hospital, and it includes two dimensions of perceived organizational culture and technology sharing willingness.
Originating from the TOE framework,6 the last aspect of the perceived external environment (PEP) was developed. For hospitals, the external environment that affects their technology use is mainly manifested in the industry pressure. Such pressure may come from competition with other hospitals, from the preferences of business partners, or from compliance with industry standards.
All items within physician-level variables have the following response categories: (1) “Strongly disagree”, (2) “Disagree”, (3) “Neutral”, (4) “Agree”, and (5) “Strongly agree”. The score for each dimension was obtained by calculating the mean score of all the items in it.
Hospital Level Variables
Hospital-level variables refer to the structural characteristics of the hospital in the study, including hospital rank and hospital role. Hospital rank was classified into two groups: (1) “tertiary” and (2) “secondary”. Hospital role was defined according to the function of the hospital in the RMC. Four of the hospitals were categorized as “leading hospitals”, which are responsible for the overall organization of the RMC and coordinating the participation of other institutions in the various efforts. The other hospitals were classified as non-leading hospitals.
Statistical Analysis
After data checking, incomplete questionnaires were eliminated. Frequencies and percentages were used to present the participants’ demographic characteristics. Means, standard deviations and medians were used for demonstrating continuous characteristics of the variable scores.
Data collected for health services research regularly involve nested (or hierarchical) structures,32 such as physicians being nested within hospitals or patients being nested within wards. The characteristics of contextual factors may influence individual outcomes. Given that the data structure of this study was hierarchical, an MSEM was performed for outcome measures and mechanistic exploration, with physicians as level 1 and hospitals as level 2. The MSEM analysis consisted of three steps. Firstly, a null model (Model 1) was established without including any independent variables. Secondly, only physician-level variables were added in Model 2. Thirdly, both physician-level and hospital-level variables were contained in Model 3. We report the intraclass correlation (ICC) for each model to estimate the variance attributable to the hospital level. The ICC was considered high if it was greater than 0.20, moderate if 0.10 < ICC ≤ 0.20, and low if ≤0.10.33,34 The following criteria assessed the model fit: the RMSEA (root mean square error of approximation) and SRMR (standardized root mean square residual) < 0.08, CFI (comparative fit index) and TLI (Tucker-Lewis index) > 0.90.35 The AIC (Akaike information criterion) and BIC (Bayesian information criterion) were decreased compared to the previous models. Data analyses were conducted using Mplus Version 8.3. All tests were two-tailed with α = 0.05.
Results
Sample Demographics
The 229 participants were aged from 24 to 56 years old (Mean = 36.79; SD = 7.27), 66.4% (n = 152) were male, 91.7% (n = 210) had a bachelor’s degree or above, 79.9% (n = 183) had no administration position, 29.7% (n = 68) had 5~10 years in practice, 60.7% (n = 139) worked in tertiary hospitals, and 59.0% (n = 135) were affiliated with non-leading hospitals. The characteristics of the participants are described in Table 1.
 |
Table 1 Characteristics of the Sample |
Measurement of Outcomes
The scores of technology use were relatively low. SU, CU and IU scored 2.31 ± 1.21, 1.51 ± 1.61 and 1.61 ± 1.61, respectively. The proportions of scores above their mean scores was 52.40%, 41.00% and 41.50% for SU, CU and IU, respectively. The scores of the dimension were closer to the ones for the dimensions within the same aspect. Overall, the dimension score was in descending order: VC > TA > POA > PEP > EOP. Table 2 provides the outcomes of all measures.
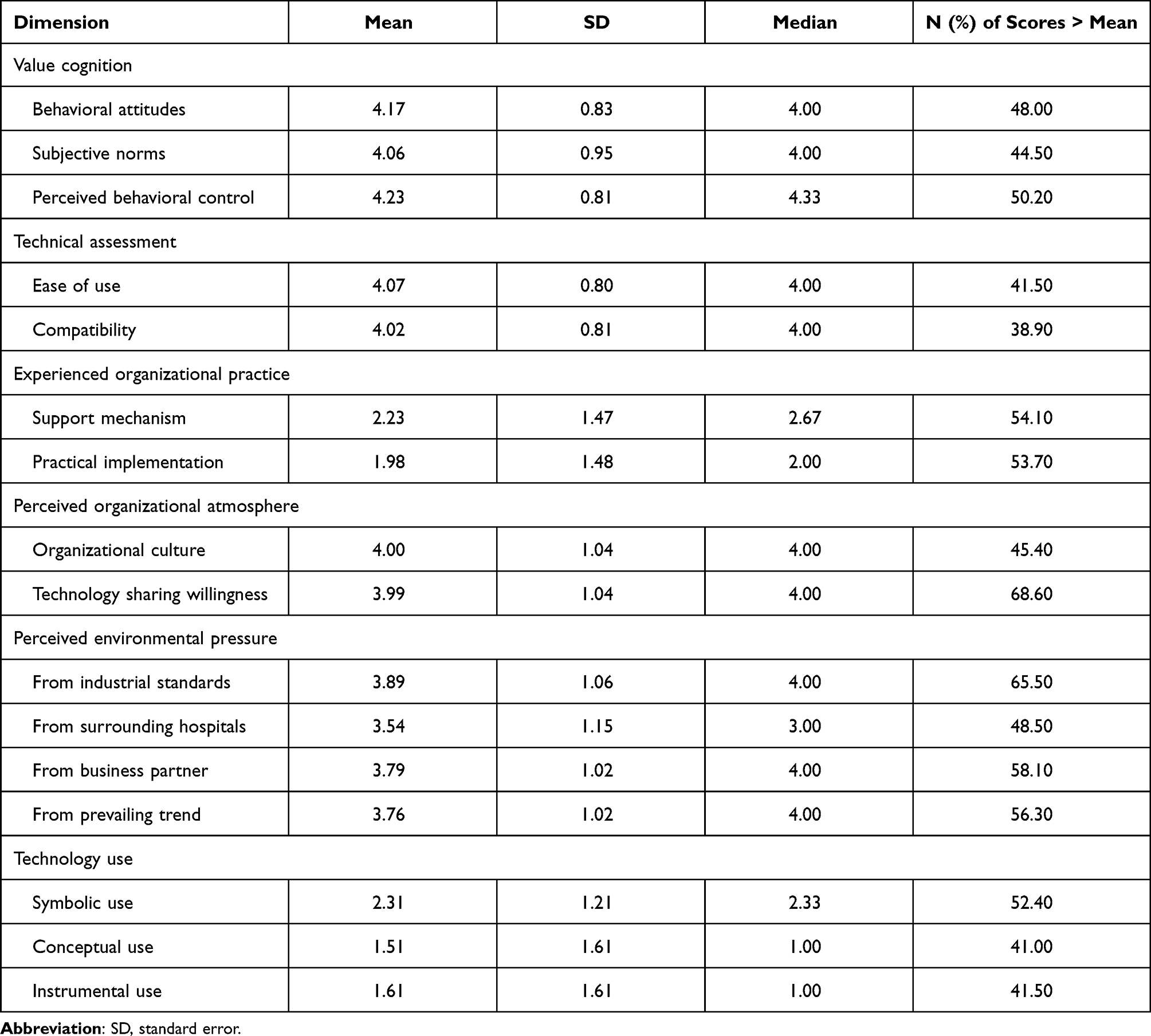 |
Table 2 Measurement Scores of the Participants |
Influencing Factors of Technology Use
The results from the MSEM analyses are presented in Table 3. Model 1 showed substantial variation at the hospital level, as the ICC values for SU, CU and IU were 0.111, 0.233 and 0.289, respectively. These suggested that the DCP use of physicians was clustered within the same hospital; the two-level hierarchical data structure was suitable for multilevel analysis. When adjusting for physician-level factors, VC and EOP had a positive influence on physicians’ DCP use (P < 0.05), POA had an inverse relationship with physicians’ DCP use (P < 0.001), and the effect of TA and PEP was insignificant. The addition of hospital-level factors did not alter test results. Model fit statistics indicated a reasonable fit of the final model: RMSEA = 0.077 < 0.08, CFI = 0.943 > 0.90, TLI = 0.922 > 0.90, SRMR for within = 0.046 < 0.08, SRMR for between = 0.037 < 0.08, and AIC and BIC were decreased by 91.75 and 64.28, respectively.
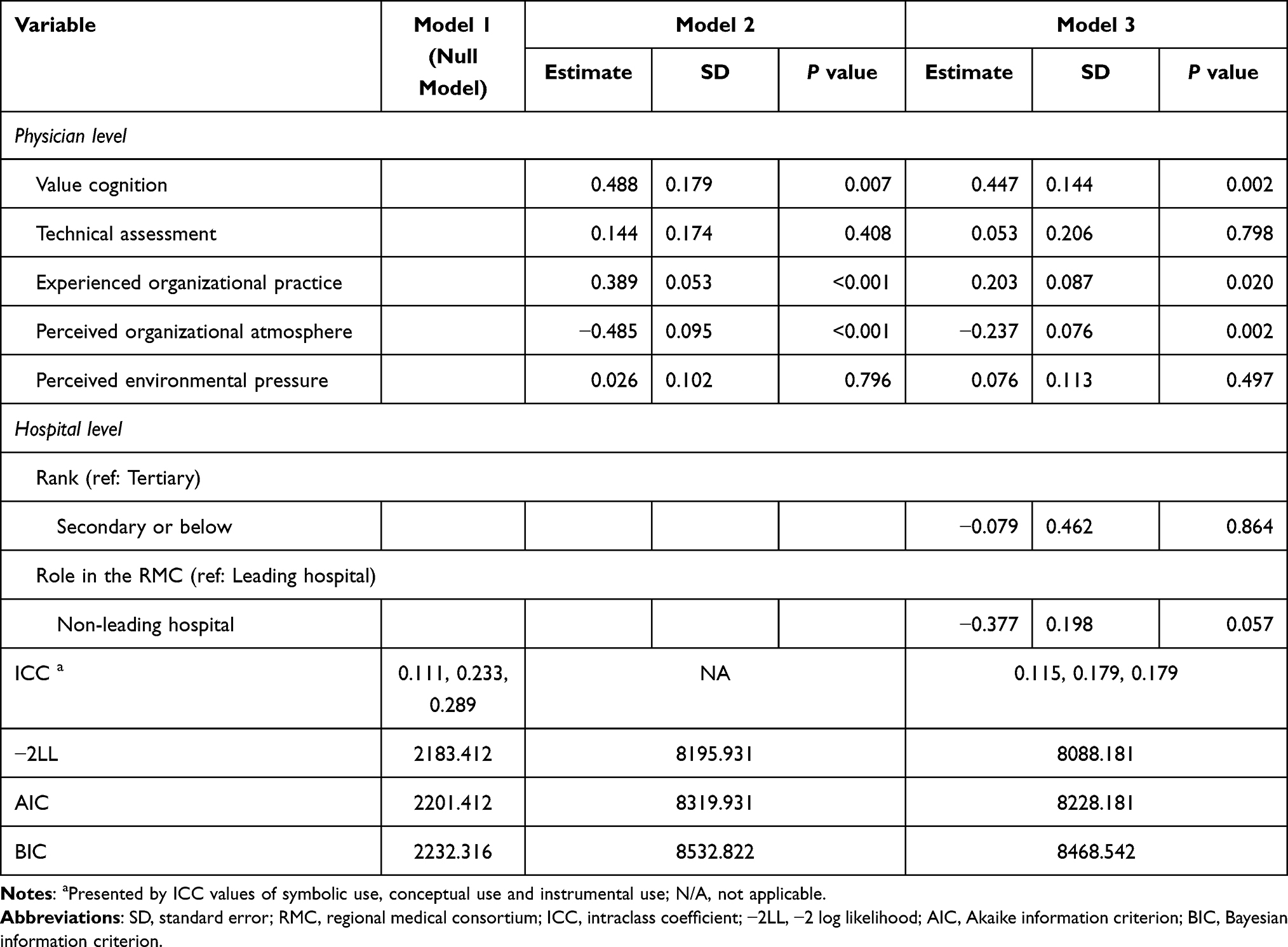 |
Table 3 Multilevel Structural Equation Modeling for the Technology Use of Physicians |
Mediation Effects of Within-Level Factors
As further indicated by our MSEM analysis, VC had no indirect effect on physicians’ DCP use; its total effect was 0.447 (P < 0.01). The relationship between TA and physicians’ DCP use was mainly mediated by VC (Indirect effect = 0.311, P < 0.01). There was a significant positive relationship between TA and PEP. Besides, TA indirectly influenced EOP through PEP (Indirect effect = 0.309, P < 0.01). EOP was positively associated with physicians’ DCP use (B = 0.203, P < 0.05), but its impact on VC was not significant (B = −0.042, P > 0.05). POA has a negative direct effect on technology use (B = −0.237, P < 0.01). In addition, VC and EOP moderated the relation between POA and physicians’ DCP use (P < 0.05). POA has a significant influence on VC (B = 0.148, P < 0.01) and EOP (B = 0.410, P < 0.001). EOP was significantly influenced by PEP (B = 0.392, P < 0.001), and the relationship between PEP and physicians’ DCP use was mediated by EOP (B = 0.079, P < 0.05). Table 4 shows the details of the direct, mediated, and total effects estimated at the physician level.
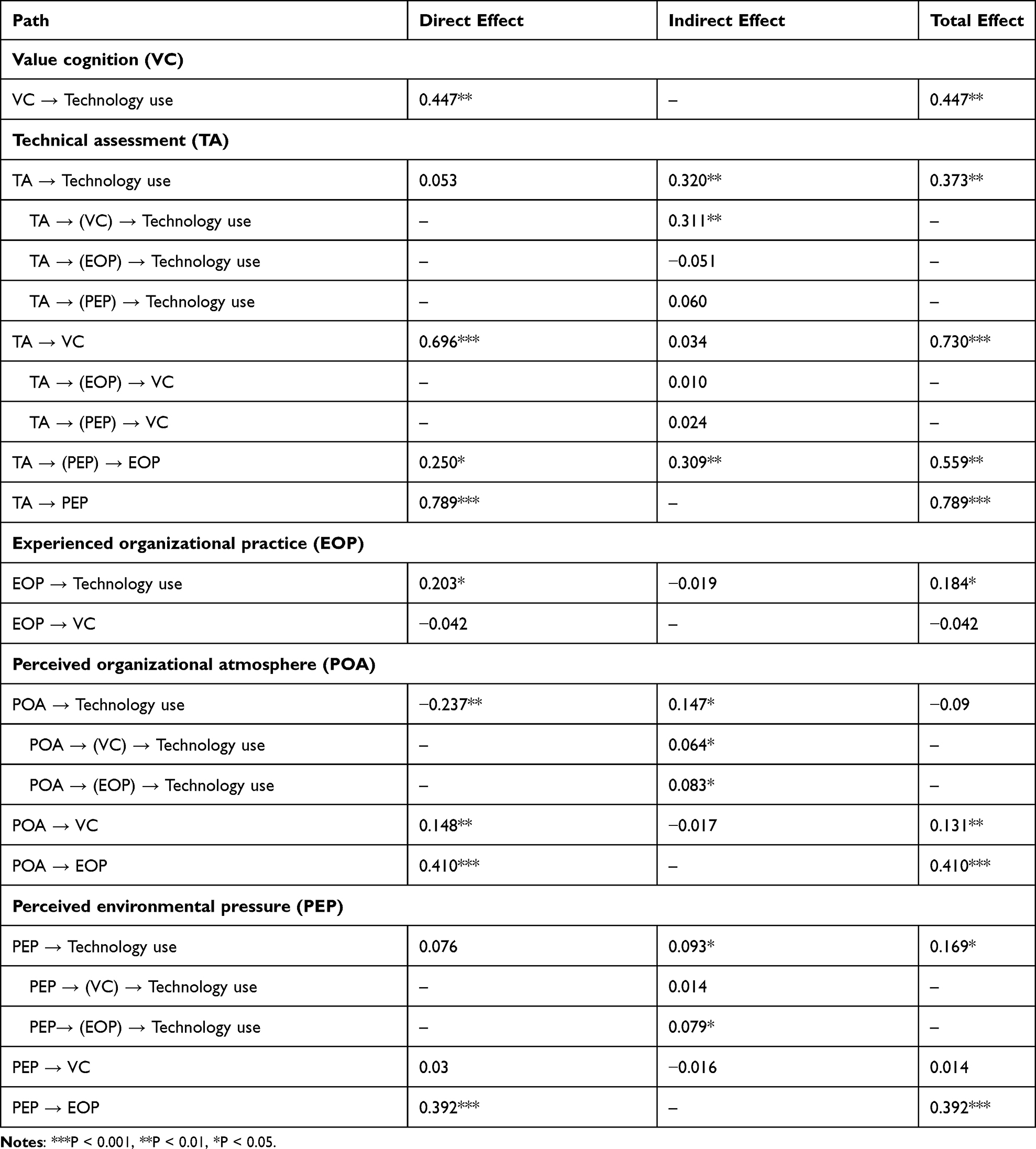 |
Table 4 Direct, Indirect and Total Effect of Predictors on Technology Use |
Discussion
Sufficient understanding of the mechanism contributes to a large extent to the effective implementation of technologies. To increase the corresponding knowledge, we developed the research model by integrating TPB, IDT, ORC and TOE using DCP as an example. The findings determined the factors associated with physicians’ technology use behavior from five aspects: VC, TA, EOP, POA and PEP. This study may provide insight into orientation strategies for advancing technology use in healthcare professionals.
The scores of DCP use in this study were low and were significantly lower than their attitudinal levels, suggested that although physicians hold positive attitudes and perceptions towards DCP use, problems such as lack of relevant knowledge and limited practical implementation still exist. This result was consistent with previous studies.36–38 For instance, in Xu Y’s study, health care professionals had positive attitudes towards graduated compression stockings, while the application rate was low because a considerable part of them did not understand the essential knowledge, such as clinical implications and contraindications.37
In this study, the significant direct impact of VC on DCP use by physicians revealed the combined function of attitudes, subjective norms and perceived behavioral control, which have been reported as important predictors of technology use in prior research.39–41 Physicians will be more apt to adopt and use a technology in their clinical practice if they rate it highly and deem it can be implemented successfully. In addition, the direct influence of EOP on physicians’ DCP use was confirmed by both support mechanism and practical implementation. When hospitals provide financial, personnel, and information guarantees for technology use,42 as well as placing emphasis on pre-training, mid-term communication and post-term feedback,43,44 it will facilitate effective interventions in physicians’ technology decision-making behavior.
Contrary to our expectations, POA had a negative effect on technology use. The plausible reason is that an outcome-oriented organizational culture has a significant negative impact on the behaviors of its members.45 Hospital supervisors attach more importance to the achievement of performance goals than to the actual developmental needs of physicians. As Quinn once pointed out, overemphasis on a certain culture may divert members’ behavior from organizational objectives.46 Also, POA indirectly affected physicians’ technology use through VC and EOP. On the one hand, most people adjust their behavior to align with the organization in general cases.47 The “invisible norms” formed by the hospital’s long-term readiness to adopt new technologies can unknowingly affect physicians’ perceptions and even actual technology use behavior.48 On the other hand, the implementation of technology use promotion often occurs when hospitals advocate self-innovation.
Notably, although no direct effects of TA and PEP on technology use were found, their mediation effects were observed through VC and EOP, respectively. The insignificance of TA reflected the limited influence of perceived ease of use and compatibility on physicians’ DCP use. A possible explanation was that such technical characteristics often have no significant effect in the early stages of technology use,49 which was in line with previous findings.50,51 To some extent, the perceived industry environment determines the macro-levels such as market orientation, and its influence on individual physicians needs to be realized through their organizations as “executive agencies”.
For nested data processing, MSEM is an effective approach to avoid clustered bias.22 Although the results showed the role of the hospitals in the RMC was insignificant (p-value of 0.057, very close to the significance level), their influence on physicians’ technology use cannot be completely ignored, which can be supported by the ICC estimates of the null model and final model. Obviously, there was a two-level structure in the study. That is, physicians’ technology use was aggregated across hospitals with different roles. Thus, the role of the hospital did contribute to the usage behavior of the physicians. As reported in Waddell JP’s study, some advanced medical devices and tests are only performed by specifically trained practitioners in certain hospitals.52 In China, the leading hospitals for the RMCs are generally local or inter-regional medical treatment centers with a strong medical services capacity,29 where advanced technologies are first deployed. Logically and practically, DCP is first applied in the leading hospitals of RMCs since it is an innovative health technology. Physicians in leading hospitals have greater access to DCP and other new technologies, both physically available and as a result of patient demand.
Based on the above understandings, several strategies can be highlighted for improving the use of health technologies among health professionals. On the one hand, for the authorities, while urging leading hospitals to assume responsibility for technical support within the RMC, external incentives such as subsidies need to provided on an ongoing basis to enable them to sustain their role. On the other hand, hospital managers can advance the promotion of technology use by providing organizational management support. Firstly, provide physicians with high-quality and adequate training about technology use.53 Secondly, mobilize authoritative physicians and managers to gradually adjust other physicians’ compliance with technology use.54 Thirdly, cultivate organizational readiness for technology use through long-term implementation of bulletin boards and typical event learning. Finally, designate staff push timely industry information so that physicians can make more accurate technology decisions.55
This study was strengthened by some features. Firstly, the integration of the TPB, IDT, OCR and TOE systematically expands the interpretations of the research basis from five aspects and also benefits a comprehensive identification of the influencing mechanism of technology use. Secondly, the subjects of this study were medical service providers (physicians, specifically), who have rarely been investigated in previous studies of technology use. Thirdly, the application of MSEM allows simultaneous analysis of physician-level and hospital-level factors, which makes the estimation of the model more accurate and comprehensive. Nevertheless, the study also has some limitations. First, the sample size was small due to funding constraints, and the accuracy and the generalizability of the findings could be improved by enrolling more participants in future research. Besides, the self-reported data might lead to social desirability bias that participants tend to give more positive responses. Finally, this study only uses DCP as an example, and the predictive power of the model needs to be tested by focusing on other technologies.
Conclusion
This study enriches the knowledge about physicians’ technology use and its associated influencing mechanism by indicating the combined impact of VC, TA, EOP, POA and PEP on technology use among physicians. The findings highlight the importance of taking some of the following pertinent measures. It is recommended that policy makers fully elaborate the driving effect of leading hospitals in RMCs on other hospitals. Additionally, several tailored interventions allow hospital managers to look at different ways to promote technology use, such as mobilizing core members, cultivating organizational readiness, implementing workable practice and providing relevant technology information.
Abbreviations
TPB, Theory of Planned Behavior; IDT, Innovation Diffusion Theory; ORC, Organizational Readiness for Change; TOE, Technology-Organization-Environment framework; MSEM, Multilevel structural equation modeling; DCP, Des-gamma-Carboxy Prothrombin; ICC, Intraclass correlation; RMSEA, Root mean square error of approximation; SRMR, Standardized root mean square residual; CFI, Comparative fit index; TLI, Tucker-Lewis index; AIC, Akaike information criterion; BIC, Bayesian information criterion.
Ethical Statement
Ethical permission was granted for this study from the Ethics Committee of Fujian Medical University (No. 2017-17). This study was conducted under the Declaration of Helsinki. A formal letter of cooperation was written to the directors of each selected medical institution and permission was obtained. All participants were informed about the study purpose, participation in the study was voluntary, and all responses were anonymous. If the participants completed and returned the questionnaire, it was considered informed consent.
Consent for Publication
All participants provided written informed consent to publish this study.
Acknowledgments
We acknowledge the support of each hospital for their involvement in this study, as well as all facilitators who contributed to coordination in the site. We also like to thank all physicians who agreed to participate.
Funding
This research was supported by the National Natural Science Foundation of China (Grant Number: 71704026) and the Distinguished Young Scientific Research Talents Plan in Universities of Fujian Province (Grant number: 2018B030). And the funders had no involvement in study design, data collection, statistical analysis, and manuscript writing.
Disclosure
The authors declare that they have no competing interests in this work.
References
1. Ma C, Kesarwala AH, Eggert T, et al. NAFLD causes selective CD4(+) T lymphocyte loss and promotes hepatocarcinogenesis. Nature. 2016;531(7593):253–257. doi:10.1038/nature16969
2. Chen W, Zheng R, Baade PD, et al. Cancer statistics in China, 2015. CA Cancer J Clin. 2016;66(2):115–132. doi:10.3322/caac.21338
3. Ajzen I. The theory of planned behavior. Organ Behav Hum Decis Process. 1991;50(2):179–211. doi:10.1016/0749-5978(91)90020-T
4. Rogers EM. Diffusion of preventive innovations. Addict Behav. 2002;27(6):989–993. doi:10.1016/S0306-4603(02)00300-3
5. Weiner BJ. A theory of organizational readiness for change. Implement Sci. 2009;4(1):67. doi:10.1186/1748-5908-4-67
6. Tornatzky LG, Fleischer M, Chakrabarti AK. Processes of Technological Innovation. Washington: Lexington books; 1990.
7. Saigí-Rubió F, Vidal-Alaball J, Torrent-Sellens J, et al. Determinants of Catalan public primary care professionals’ intention to use digital clinical consultations (eConsulta) in the post-COVID-19 context: optical illusion or permanent transformation? J Med Internet Res. 2021;23(6):e28944. doi:10.2196/28944
8. Liu C, Liu C, Wang D, Deng Z, Tang Y, Zhang X. Determinants of antibiotic prescribing behaviors of primary care physicians in Hubei of China: a structural equation model based on the theory of planned behavior. Antimicrob Resist Infect Control. 2019;8(1):23. doi:10.1186/s13756-019-0478-6
9. Randall CL, Hort K, Huebner CE, et al. Organizational readiness to implement system changes in an Alaskan Tribal Dental Care Organization. JDR Clin and Trans Res. 2020;5(2):156–165.
10. Knerr S, West KM, Angelo FA. Organizational readiness to implement population-based screening and genetic service delivery for hereditary cancer prevention and control. J Genet Couns. 2020;29(5):867–876. doi:10.1002/jgc4.1216
11. Meri A, Hasan MK, Danaee M, et al. Modelling the utilization of cloud health information systems in the Iraqi public healthcare sector. Telemat Inform. 2019;36:132–146. doi:10.1016/j.tele.2018.12.001
12. Chang IC, Hwang HG, Yen DC, Lian JW. Critical factors for adopting PACS in Taiwan: views of radiology department directors. Decis Support Syst. 2006;42(2):1042–1053. doi:10.1016/j.dss.2005.08.007
13. Lian JW, Yen DC, Wang YT. An exploratory study to understand the critical factors affecting the decision to adopt cloud computing in Taiwan hospital. Int J Inf Manag. 2014;34(1):28–36. doi:10.1016/j.ijinfomgt.2013.09.004
14. Tyagi RK, Cook L, Olson J, Belohlav J. Healthcare technologies, quality improvement programs and hospital organizational culture in Canadian hospitals. BMC Health Serv Res. 2013;13(1):413. doi:10.1186/1472-6963-13-413
15. Wright JD, Tergas AI, Hou JY, et al. Effect of regional hospital competition and hospital financial status on the use of robotic-assisted surgery. JAMA Surg. 2016;151(7):612–620. doi:10.1001/jamasurg.2015.5508
16. Ebu NI, Ogah JK. Predictors of cervical cancer screening intention of HIV-positive women in the central region of Ghana. BMC Womens Health. 2018;18(1):43. doi:10.1186/s12905-018-0534-z
17. Lee FH. Intention to receive breast cancer screening and related factors of influence among Vietnamese women in transnational marriages. J Nurs Res. 2018;26(2):112–122. doi:10.1097/jnr.0000000000000210
18. Besharati F, Karimi-Shahanjarini A, Hazavehie SMM, Bashirian S, Faradmal J. Predictors of colorectal cancer screening intention among Iranian adults: an application of the preventive health model. J Prev Med Hyg. 2018;59:E159–E166.
19. Jiang H, Chen X, Li J, Tan Z, Cheng W, Yang Y. Predictors of condom use behavior among men who have sex with men in China using a modified information-motivation-behavioral skills (IMB) model. BMC Public Health. 2019;19(1):261. doi:10.1186/s12889-019-6593-8
20. Disch J. Clinical microsystems: the building blocks of patient safety. Creat Nurs. 2006;12(3):13–14. doi:10.1891/1078-4535.12.3.13
21. Estabrooks CA, Squires JE, Hutchinson AM, et al. Assessment of variation in the Alberta Context Tool: the contribution of unit level contextual factors and specialty in Canadian pediatric acute care settings. BMC Health Serv Res. 2011;11(1):251. doi:10.1186/1472-6963-11-251
22. Rabe-Hesketh S, Skrondal A, Pickles A. Generalized multilevel structural equation modeling. Psychometrika. 2004;69(2):167–190. doi:10.1007/BF02295939
23. Van Hootegem A, Meuleman B, Abts K. Attitudes toward asylum policy in a divided Europe: diverging contexts, diverging attitudes? Front Sociol. 2020;5:35. doi:10.3389/fsoc.2020.00035
24. Gu Y, Li L, Zhou C, Yang T, Dong H. Factors influencing voluntary premarital medical examination in Zhejiang province, China: a culturally-tailored health behavioral model analysis. BMC Public Health. 2014;14(1):659. doi:10.1186/1471-2458-14-659
25. Huh J, Yu S, Galimov A, et al. Hypothetical flavour ban and intention to vape among vape shop customers: the role of flavour preference and e-cigarette dependence. Tob Control. 2021. doi:10.1136/tobaccocontrol-2020-056321
26. Hosseinkhani Z, Hassanabadi HR, Parsaeian M, Karimi M, Nedjat S. Academic stress and adolescents mental health: a Multilevel Structural Equation Modeling (MSEM) study in Northwest of Iran. J Res Health Sci. 2020;20(4):e00496. doi:10.34172/jrhs.2020.30
27. Låftman SB, Modin B, Olsson G, Sundqvist K, Svensson J, Wennberg P. School ethos and adolescent gambling: a multilevel study of upper secondary schools in Stockholm, Sweden. BMC Public Health. 2020;20(1):130. doi:10.1186/s12889-020-8230-y
28. Cai M, Liu E, Tao H, et al. Does A medical consortium influence health outcomes of hospitalized cancer patients? An integrated care model in Shanxi, China. Int J Integr Care. 2018;18(2):7. doi:10.5334/ijic.3588
29. Nunnally JC. Psychometric Theory.
30. Beyer JM. Research utilization: bridging the gap between communities. J Manag Inq. 1997;6(1):17–22. doi:10.1177/105649269761004
31. Estabrooks CA. The conceptual structure of research utilization. Res Nurs Health. 1999;22(3):203–216. doi:10.1002/(SICI)1098-240X(199906)22:3<203::AID-NUR3>3.0.CO;2-9
32. Husum TL, Bjørngaard JH, Finset A, Ruud T. A cross-sectional prospective study of seclusion, restraint and involuntary medication in acute psychiatric wards: patient, staff and ward characteristics. BMC Health Serv Res. 2010;10:89.
33. JWR Twisk. Applied Multilevel Analysis. New York: Cambridge University Press; 2006.
34. Schellart AJ, Mulders H, Steenbeek R, Anema JR, Kroneman H, Besseling J. Inter-doctor variations in the assessment of functional incapacities by insurance physicians. BMC Public Health. 2011;11(1):864. doi:10.1186/1471-2458-11-864
35. Arpaci I, Baloğlu M. The impact of cultural collectivism on knowledge sharing among information technology majoring undergraduates. Comput Human Behav. 2016;56:65–71. doi:10.1016/j.chb.2015.11.031
36. Di Gennaro F, Marotta C, Amicone M, et al. Italian young doctors’ knowledge, attitudes and practices on antibiotic use and resistance: a national cross-sectional survey. J Glob Antimicrob Resist. 2020;23:167–173. doi:10.1016/j.jgar.2020.08.022
37. Xu Y, Wang W, Zhao J, et al. Knowledge, attitude, and practice of healthcare professionals toward clinically applying graduated compression stockings: results of a Chinese web-based survey. J Thromb Thrombolysis. 2019;47(1):102–108. doi:10.1007/s11239-018-1749-4
38. Bhattarai S. Knowledge, attitude and practice of hepatitis b vaccination among health care workers at Manipal Teaching Hospital. Kathmandu Univ Med J. 2020;18(72):256–259.
39. Kermel Schiffman I, Werner P. Willingness of family caregivers of people with dementia to undertake advance care planning: examining an extended model of the theory of planned behavior. Dementia. 2021;20(3):1044–1057. doi:10.1177/1471301220922761
40. Rich A, Medisauskaite A, Potts HWW, Griffin A. A theory-based study of doctors’ intentions to engage in professional behaviours. BMC Med Educ. 2020;20(1):44. doi:10.1186/s12909-020-1961-8
41. Archambault P, Turcotte S, Smith PY, et al. Wiki-based knowledge tool investigators. intention to use wiki-based knowledge tools: survey of Quebec Emergency Health Professionals. JMIR Med Inform. 2021;9(6):e24649. doi:10.2196/24649
42. Kummer TF, Recker J, Bick M. Technology-induced anxiety: manifestations, cultural influences, and its effect on the adoption of sensor-based technology in German and Australian hospitals. Inf Manag. 2017;54(1):73–89. doi:10.1016/j.im.2016.04.002
43. Helfrich CD, Li YF, Sharp ND, et al. Organizational readiness to change assessment (ORCA): development of an instrument based on the Promoting Action on Research in Health Services (PARIHS) framework. Implement Sci. 2009;4(1):1–13. doi:10.1186/1748-5908-4-38
44. Mccormack B, Mccarthy G, Wright J, et al. Development and testing of the Context Assessment Index (CAI). Worldviews Evid Based Nurs. 2009;6(1):27–35. doi:10.1111/j.1741-6787.2008.00130.x
45. Zhang W, Liu YP. Study on the influence of different oriented organizational cultures on staff’s career growth: based on multi-group structural modeling method. Stat Inf Forum. 2015;8:106–112. Chinese.
46. Quinn RE. Beyond Rational Management. San Francisco: Jossey-Bass; 1988.
47. Li Y, Yan X. How Could Peers in Online Health Community Help Improve Health Behavior. Int J Environ Res Public Health. 2020;17(9):2995. doi:10.3390/ijerph17092995
48. Deng Q, Zeng Z, Zheng Y, Lu J, Liu W. Predictors of physicians’ intentions to use clinical practice guidelines on antimicrobial in tertiary general hospitals of China: a structural equation modeling approach. Antimicrob Resist Infect Control. 2021;10(1):97. doi:10.1186/s13756-021-00966-z
49. Venkatesh V, Bala H. Technology acceptance model 3 and a research agenda on interventions. Decis Sci. 2008;39(2):273–315. doi:10.1111/j.1540-5915.2008.00192.x
50. Bhattacherjee A, Hikmet N. Physicians’ resistance toward healthcare information technology: a theoretical model and empirical test. EurJ Inform Syst. 2007;16(6):725–737. doi:10.1057/palgrave.ejis.3000717
51. Chismar WG, Wiley-Patton S. Test of the technology acceptance model for the internet in pediatrics.
52. Waddell JP. The introduction of new technology. Can J Surg. 2004;47(4):246–248.
53. Vaishnavi V, Suresh M, Dutta P. A study on the influence of factors associated with organizational readiness for change in healthcare organizations using TISM. Benchmarking. 2019;26(4):1290–1313. doi:10.1108/BIJ-06-2018-0161
54. Deng Q, Zheng Y, Lu J, Zeng Z, Liu W. What factors predict physicians’ utilization behavior of contrast-enhanced ultrasound? Evidence from the integration of the theory of planned behavior and technology acceptance model using a structural equation modeling approach. BMC Med Inform Decis Mak. 2021;21(1):173. doi:10.1186/s12911-021-01540-8
55. Young HP. The evolution of social norms. Annu Rev Economics. 2015;7(1):359–387. doi:10.1146/annurev-economics-080614-115322
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.