Back to Journals » Clinical Optometry » Volume 18
Using Lotilaner Ophthalmic Solution, 0.25% to Treat Demodex Blepharitis in Patients Who Were Initially Misdiagnosed: A Case Series
Authors Periman LM ![]() , Lindstrom R
, Lindstrom R ![]() , Karpecki P
, Karpecki P ![]() , Ayres B
, Ayres B ![]() , Donnenfeld E
, Donnenfeld E ![]() , Farid M, Gaddie IB
, Farid M, Gaddie IB ![]() , Gupta PK
, Gupta PK ![]() , McGee S, Nichols KK
, McGee S, Nichols KK ![]() , Pflugfelder S, Starr CE, Venkateswaran N, Yeu E
, Pflugfelder S, Starr CE, Venkateswaran N, Yeu E ![]() , Koetting C
, Koetting C ![]()
Received 4 February 2026
Accepted for publication 23 May 2026
Published 24 June 2026 Volume 2026:18 600893
DOI https://doi.org/10.2147/OPTO.S600893
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Prof. Dr. Chris Lievens
Laura M Periman,1 Richard Lindstrom,2 Paul Karpecki,3 Brandon Ayres,4 Eric Donnenfeld,5 Marjan Farid,6 Ian Benjamin Gaddie,7 Preeya K Gupta,8 Selina McGee,9 Kelly K Nichols,10 Stephen Pflugfelder,11 Christopher E Starr,12 Nandini Venkateswaran,13,14 Elizabeth Yeu,15 Cecelia Koetting16
1Periman Eye Institute, Seattle, WA, USA; 2Minnesota Eye Consultants, Bloomington, MN, USA; 3Kentucky Eye Institute, Lexington, KY, USA; 4Wills Eye Hospital, Philadelphia, PA, USA; 5Ophthalmic Consultants of Long Island, Long Island, NY, USA; 6Department of Ophthalmology, Gavin Herbert Eye Institute, UC-Irvine, Irvine, CA, USA; 7Gaddie Eye Centers, Louisville, KY, USA; 8Triangle Eye Consultants, Raleigh, NC, USA; 9BeSpoke Vision, Edmond, OK, USA; 10School of Optometry, University of Alabama at Birmingham, Birmingham, AL, USA; 11Department of Ophthalmology, Baylor College of Medicine, Houston, TX, USA; 12Department of Ophthalmology, Weill Cornell Medicine, New York, NY, USA; 13Department of Ophthalmology, Massachusetts Eye and Ear, Boston, MA, USA; 14Department of Ophthalmology, Harvard Medical School, Boston, MA, USA; 15Virginia Eye Consultants, Norfolk, VA, USA; 16Department of Ophthalmology, University of Colorado School of Medicine, Aurora, CO, USA
Correspondence: Cecelia Koetting, Department of Ophthalmology, University of Colorado School of Medicine, Aurora, CO, USA, Tel +1 720 848 2020, Email [email protected]
Introduction: Demodex blepharitis (DB) is a chronic ocular inflammation caused by Demodex mite infestation of the eyelid. DB is often misdiagnosed, as some of its clinical findings and patient-reported outcomes overlap with those of other ocular surface diseases. The Demodex Expert Panel on Treatment and Eyelid Health (DEPTH) has reached consensus on the symptomatology, diagnosis, and treatment of DB. Consensus findings from the DEPTH group include that collarettes are pathognomonic for DB and that lotilaner ophthalmic solution, 0.25%, the first and only FDA-approved treatment for DB, should be the first-line treatment for the disease. This case series highlights two instances of misdiagnosis that were subsequently re-evaluated using consensus findings from the DEPTH group, leading to a correct diagnosis and effective treatment with XDEMVY® (lotilaner ophthalmic solution) 0.25%.
Case Reports: Two cases of patients with DB are presented. In the first case, a 75-year-old female presented with collarettes, reduced meibomian gland secretions, and lid margin erythema. After an unsuccessful initial treatment for bacterial infection, the patient was diagnosed with DB and prescribed lotilaner ophthalmic solution, 0.25% twice daily for 6 weeks, which improved all clinical findings and patient-reported outcomes. In the second case, a 62-year-old male presented with ocular discomfort, dry eye, and burning and itching sensations. After an unsuccessful initial treatment for dry eye disease, collarettes were detected, and the patient was diagnosed with DB. Subsequent treatment with lotilaner ophthalmic solution, 0.25% reduced collarettes and resolved patient-reported symptoms.
Conclusion: These cases highlight patients with DB who were initially misdiagnosed and eventually treated with lotilaner ophthalmic solution, 0.25%. Each case exemplifies the utility of the DEPTH consensus findings in improving the diagnostic path for patients and eye care providers. Future case series from other groups will continue to shed light on the best practices for diagnosing and treating patients with DB.
Keywords: Demodex blepharitis, clinical management, misdiagnosis, dry eye disease, lotilaner, Staphylococcus blepharitis
Introduction
Blepharitis is a chronic ocular inflammatory disease characterized by pain, itching, and redness of the eyelid margins.1 If left untreated, complications due to blepharitis such as superficial keratopathy, corneal neovascularization, and ulcerations can cause persistent eyelid margin changes or vision loss.1
Demodicosis, overpopulation of Demodex mites within the eyelash follicle as well as the meibomian glands, leads to Demodex blepharitis (DB). In adults complaining of eye irritation, a strong correlation was noted between the number of Demodex mites and the severity of ocular discomfort, suggesting Demodex plays a pathogenic role.2 A comprehensive study of 1032 participants from seven geographically different clinical locations revealed that nearly 58% of adult eye care patients had DB, indicating a high prevalence of the disease.3 The daily life of patients with DB is negatively affected by patient-reported outcomes such as blurred vision, eye discomfort, and difficulty with routine activities such as hygienic routines and night driving.4,5 Moreover, people with DB experience an elevated risk of anxiety and depression.6
DB is often undiagnosed or misdiagnosed.7 In a prospective study with 524 patients with DB, approximately 68% experienced clinical findings or patient-reported outcomes related to the disease for more than 2 years. Despite consulting with their eye care providers (ECPs) on several occasions during that time span, 60% of patients did not receive a diagnosis of blepharitis or DB.5 These data indicate that diagnosis of DB remains a significant bottleneck along the patient journey, and achieving greater awareness of the disease is a persisting unmet need.
Generally, misdiagnosis is due to similarities with other ocular diseases such as dry eye disease (DED), Staphylococcus blepharitis, and meibomian gland dysfunction (MGD).1,8 DB and DED share symptoms of burning, irritation, photophobia, blurred vision, and red eyes.9 DED, characterized by ineffective tear production and/or instability of the tear film, can be caused by disrupted meibomian gland secretion of meibum.9 DB can cause lipid tear insufficiency by eliciting granulomatous reactions within the meibomian glands.10 Indeed, DB is highly prevalent in patients with DED.7 The close association between DB and DED causes diagnostic challenges for ECPs, who may diagnose their patients with DED without identifying DB as a root cause. Misdiagnosed patients may be prescribed artificial tears to restore tear volume5,9 or other treatments to increase tear production, such as TYRVAYA® (varenicline solution) nasal spray, TRYPTYR® (acoltremon ophthalmic solution) 0.003%, VEVYE® (cyclosporine ophthalmic solution) 0.1%, XIIDRA® (lifitegrast ophthalmic solution) 5%, or CEQUA® (cyclosporine ophthalmic solution) 0.09%.11–15 As these treatments do not resolve the root cause of DB, Demodex mite infestation, misdiagnosed patients continue to suffer from the disease.3
Another challenge ECPs face in diagnosing DB is differentiating it from other inflammatory conditions of the eyelid margin, particularly those associated with seborrheic dermatitis and Staphylococcus blepharitis.1 These conditions share many clinical features with DB, including burning, itching, redness, and foreign body sensation.1 Moreover, Demodex mites have been implicated in the carriage and transmission of bacteria, including Staphylococcus species, on the ocular surface, further complicating the clinical presentation and differential diagnosis.7 Misdiagnosis of Staphylococcus blepharitis can lead to treatment for bacterial infection with treatments containing antibiotics and steroids, such as neomycin–polymyxin B–dexamethasone (Neo-Poly-Dex) ointment.16 As with artificial tears, antibiotic treatment does not eradicate mites, so misdiagnosed patients continue to suffer from the clinical findings and patient-reported outcomes of DB.
Recognizing an unmet need to raise awareness of DB among ECPs and establish a well-delineated diagnostic path to accurately diagnose patients with DB, a group of US-based ophthalmologists and optometrists with expertise in ocular surface diseases such as DB established the Demodex Expert Panel on Treatment and Eyelid Health (DEPTH). To date, three iterations of the DEPTH group have used a modified Delphi method to establish consensus regarding clinical findings and patient-reported outcomes in DB, treatment goals, and the first-line treatment for the disease.8,17,18 The experts agreed that collarettes (cylindrical dandruff around the base of the eyelash) are the most common clinical finding in patients with DB and are pathognomonic for the disease.8 Collarette load is graded 0–4 based on the number of lashes per eyelid with collarettes (Table 1).19 The panelists also agreed that collarette reduction equates to eradication of Demodex mites, leading to an improvement in clinical findings and patient-reported outcomes, and should therefore be a goal of treatment.8
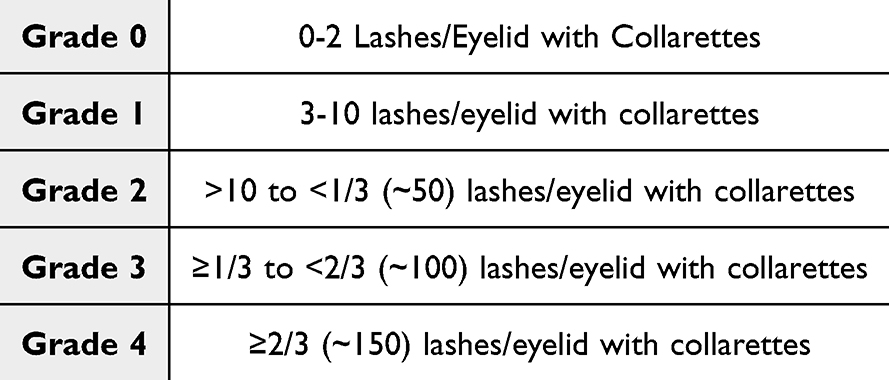 |
Table 1 Grading Scale Used to Classify Collarette Load. Grade 0–1 is Considered Clinically Meaningful.19 |
In the most recent iteration of the DEPTH study, panelists agreed that XDEMVY® (lotilaner ophthalmic solution) 0.25% (Tarsus Pharmaceuticals, Irvine, California; hereafter referred to as lotilaner 0.25%) should serve as the first-line treatment for patients with DB.18,20 Lotilaner 0.25%, the only FDA-approved drug for the treatment of DB, is a mite-selective GABA-gated chloride channel inhibitor that paralyzes mites, leading to their eradication.17 The safety and efficacy of lotilaner 0.25% have been established in several clinical trials.19,21–25
This case series presents two patient cases that highlight instances of misdiagnosis of patients with DB with either DED or Staphylococcus blepharitis. In both cases, patients were eventually diagnosed with DB and successfully treated with lotilaner 0.25%. These cases exemplify the utility of the DEPTH consensus findings in improving the diagnostic path for patients and ECPs.
Case Reports
Case 1
A 75-year-old female patient presented with grade 1 collarettes (3–10 lashes/eyelid with collarettes), multiple persistent chalazia along both eyelid margins, scalloped eyelid margins, a thin tear film, grade 2+ telangiectasia (moderate number of telangiectasias along the eyelid margin), and mild lid margin erythema in both eyes. Initial examination also indicated grade 2+ meibomian gland expression (moderate difficulty), with the Meibomian Glands Yielding Liquid Secretion (MGYLS) score of 10/15 in both eyes. Both eyes had grade 2+ conjunctivochalasis (two or more folds in the conjunctiva) and grade 1+ bulbar conjunctival injection (mild injection). The patient had trace inferior corneal superficial punctate keratitis and an 8-second tear break up time (TBUT) with sodium fluorescein in both eyes but showed no conjunctival staining with lissamine green in either eye. Her score on the Standard Patient Evaluation of Eye Dryness (SPEED) questionnaire was 22/28. Her best-corrected visual acuity (BCVA) was 20/25 in both eyes. Prior to this presentation, the patient had already been prescribed Neo-Poly-Dex ophthalmic solution to treat an apparent bacterial infection, preservative-free artificial tears, warm compresses, and OCuSOFT® Lid Scrub Original (eyelid cleanser).
The patient underwent incision and drainage of a single chalazion. Unfortunately, multiple new chalazia appeared afterward. At the postoperative appointment, the patient presented with continued presence of collarettes on the base of the eyelashes (Figure 1A) and was diagnosed with DB. The patient was then prescribed lotilaner 0.25% twice daily for 6 weeks in addition to the warm compresses once daily for 10 minutes, artificial tears as needed, re-esterified triglyceride form omega-3 supplements once daily, and ZocuFoam™, an okra-based foam lid cleanser and moisturizer, twice daily. She was to immediately stop treatment with the Neo-Poly-Dex solution. At the 2-month follow-up appointment, the patient presented with an absence of collarettes, indicating eradication of Demodex mites and complete resolution of DB (Figure 1B). Additionally, the patient exhibited improved lid margin appearance, grade 1+ MGD (mild) with improved meibum expressibility, grade 1+ telangiectasia (few, scattered telangiectatic vessels), a decrease in bulbar conjunctival injection, and no recurrence of chalazia. Her TBUT was maintained at 8 seconds in both eyes, and her score on the SPEED questionnaire had improved to 8/28. The patient’s post-treatment plan consisted of continued warm compresses with heat mask once daily for 10 minutes, TheraTears® preservative-free artificial tears 2–4x daily, omega-3 supplements, and eyelid cleansers once daily.
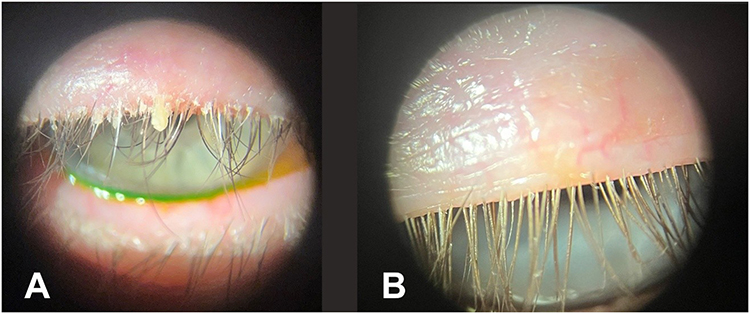 |
Figure 1 Slit lamp images taken of a patient with collarettes diagnosed with Demodex blepharitis. (A) Image taken of patient in Case 1 at initial visit. (B) Image taken of patient at the 2-month follow-up appointment after treatment with lotilaner 0.25%. |
Case 2
A 62-year-old male patient presented with ocular discomfort that worsened gradually throughout the day, eye dryness, burning, and itching sensation, both with and without scleral lens wear. Additional presentations included grade 1+ collarettes (3–10 lashes/eyelid with collarettes), eyelid margin erythema, eyelid thickening, grade 2+ telangiectasia (moderate number of telangiectasias along the eyelid margin), turbid meibomian gland secretions on expression, grade 2+ conjunctivochalasis (two or more parallel redundant folds of the nasal and temporal conjunctiva), grade 2+ conjunctival injection (moderate), mild punctate epitheliopathy with Fluorescein staining, and a reduced TBUT of 4 seconds in both eyes. The patient was initially prescribed varenicline solution 0.03% nasal spray and cyclosporine ophthalmic solution 0.09% for DED plus compounded topical ivermectin 1% cream for facial rosacea, but signs and symptoms persisted. Further examination revealed grade 2 collarettes (>10 to <1/3 [~50] lashes/eyelid with collarettes). The patient was diagnosed with DB and prescribed lotilaner 0.25% twice daily for 6 weeks. At the 20-day follow-up appointment, slit lamp examination indicated a reduction to grade 0 collarettes (0–2 lashes/eyelid with collarettes), improved meibomian gland expressibility and quality, and improved lid margin erythema. The patient also reported meaningful improvement in subjective ocular discomfort, eyelid redness, ocular redness, burning, and itching.
Discussion
Misdiagnosis of patients with DB remains a prevalent hurdle during the patient treatment journey.5,7 As such, achieving greater awareness of the signs and symptoms of DB and how they relate to other ocular surface diseases, allergies, and hypersensitivities remains an unmet need. Although this case series is limited to only two cases, it does contribute to resolving this unmet need. Future case series from other groups will continue to shed light on the best practices for diagnosing and treating patients with DB.
In this case series, both patients were older than 60 years of age and presented with clinical findings and patient-reported outcomes of DB. In both cases, the initial diagnosis was not DB, and the treatment regimen did not include lotilaner 0.25%. In Case 1, the patient was prescribed Neo-Poly-Dex ophthalmic solution to manage Staphylococcus blepharitis and serve as postoperative prophylaxis after the chalazion removal. Although the patient presented with collarettes, which are pathognomonic for DB, lotilaner 0.25% was not prescribed. Rather, she was instructed on eyelid hygiene methods to manage the clinical findings and patient-reported outcomes. Upon follow-up, the persistent collarettes and inflamed eyelid margins led her clinician to prescribe lotilaner 0.25% and discontinue the antibiotic/steroid ointment. In Case 2, the clinical findings and patient-reported symptoms commonly encountered in DB, such as collarettes, ocular discomfort, dry eye, burning, and itching, did not resolve despite treatment with varenicline solution 0.03% nasal spray and cyclosporine ophthalmic solution 0.09% for DED plus compounded topical ivermectin 1% cream for facial rosacea. The patient was then diagnosed with DB and was successfully treated with lotilaner 0.25% twice daily. In both cases, treatment with lotilaner 0.25% twice daily for 6 weeks improved both clinical findings and patient-reported outcomes, with no reported adverse events. Regarding case 1, the patient was also prescribed an okra-based foam lid cleanser and moisturizer. Okra-containing lid hygiene formulations have been reported to improve symptoms and reduce Demodex counts in small clinical studies, likely due to their cleansing and anti-inflammatory properties; however, robust evidence supporting direct acaricidal activity against Demodex mites remains limited.26
This case series underscores the clinical challenges ECPs face in diagnosing DB and highlights the potential consequences of misdiagnosis, including prolonged symptom duration, inappropriate treatment, and diminished patient quality of life. Both patients presented here had initially been misdiagnosed with other ocular surface disorders, DED and Staphylococcus blepharitis, without ruling out DB as a root cause. Consequentially, the patients were treated with pharmacological agents intended to initiate production of the tear film or combat bacterial infection, respectively. The result of these misdiagnoses and inappropriate treatments was prolongation of clinical findings and patient-reported outcomes because the initial treatment plans did not address the root cause: Demodex mite infestation of the eyelid.
Collarettes at the base of the eyelashes remains the pathognomonic sign for DB. The best method for assessing collarette load is to have the patient look downward during a slit lamp examination.8 The DEPTH group agrees that every patient undergoing a routine slit lamp examination should be instructed to look downward so that the ECP could check for Demodex mites in the form of collarettes.8 Adherence to this guidance from the DEPTH group could minimize instances of overlooking collarettes that lead to misdiagnoses of patients with DB.
The DEPTH group previously agreed that the presence of grade 2+ collarettes (>10 lashes/eyelid with collarettes) is sufficient to diagnose DB, even in the absence of other clinical findings and patient-reported outcomes (Figure 2).8,18 DEPTH experts also aligned on the diagnosis and treatment of patients who present with a less severe grade of collarettes (ie, < grade 2) According to DEPTH experts, patients who present with grade 1 collarettes should be treated with lotilaner 0.25% if they also present with ≥1 additional sign of DB (Figure 2). Both patients in these case series presented with grade 1 collarettes and at least 1 additional sign of DB, such as lid margin erythema. Adherence to this guidance from the DEPTH group could help treat patients with DB early in the diagnostic pathway, potentially minimizing patient suffering.
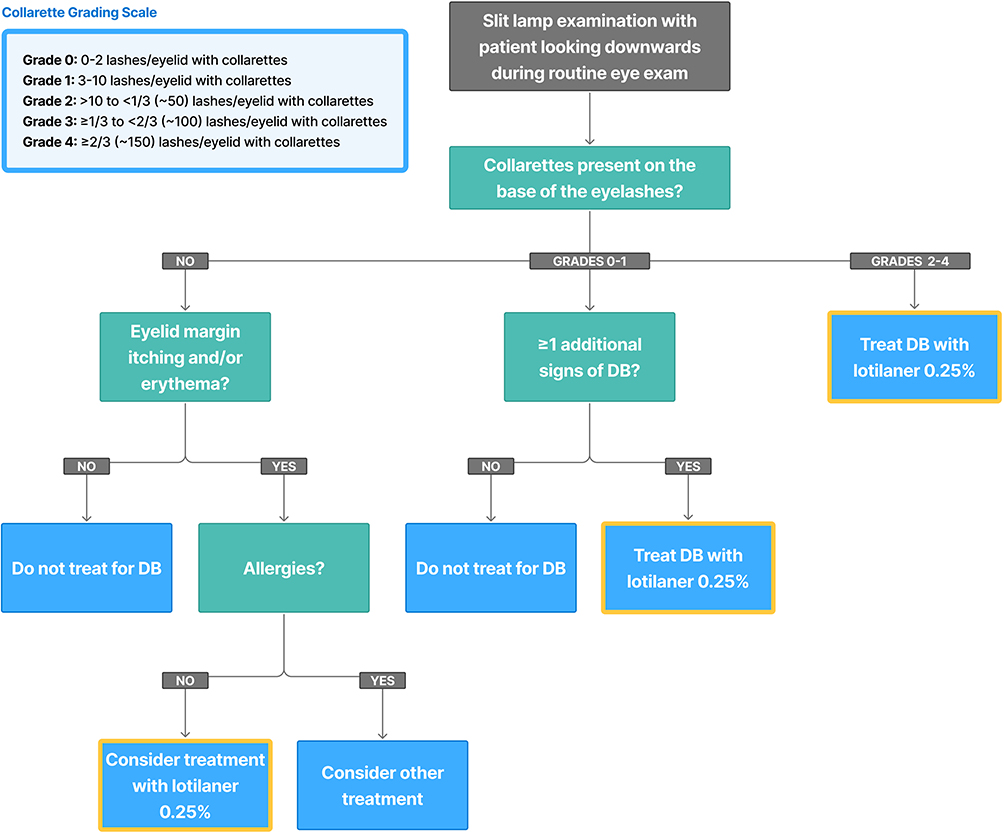 |
Figure 2 Diagnostic path for patients with clinical findings and patient-reported outcomes associated with DB in accordance with consensus agreements from the DEPTH group. Grade 0–1 (0–10 lashes/eyelid with collarettes) requires ≥1 additional signs of DB to prompt treatment with lotilaner 0.25%, while grade 2 (>10 lashes/eyelid with collarettes) is sufficient to prompt diagnosis of DB and treatment with lotilaner 0.25%. Common signs of DB include eyelid margin erythema and telangiectasia, and lash anomalies such as trichiasis and madarosis. In cases where eyelid margin itching and/or erythema are presented, ECPs should consider treatment with lotilaner 0.25% after diagnostically ruled out allergies as a root cause. Yellow boxes indicate decisions to treat with lotilaner 0.25% or to consider treatment. Abbreviations: DB, Demodex blepharitis; DEPTH, Demodex Expert Panel on Treatment and Eyelid Health. |
Additionally, the DEPTH experts agreed that patients who present with eyelid margin itching and/or erythema and without collarettes should be considered for treatment with lotilaner 0.25% once ECPs have diagnostically ruled out allergies as a root cause (Figure 2).18 Thus, when diagnosing a patient without collarettes, ECPs should first conduct an appropriate differential assessment and consider alternative or coexisting causes of symptoms such as allergic conjunctivitis, contact or medication-related dermatitis, DED, MGD, staphylococcal blepharitis, seborrheic blepharitis, and ocular rosacea. Allergies and hypersensitivities that should be ruled out are detailed in Table 2.
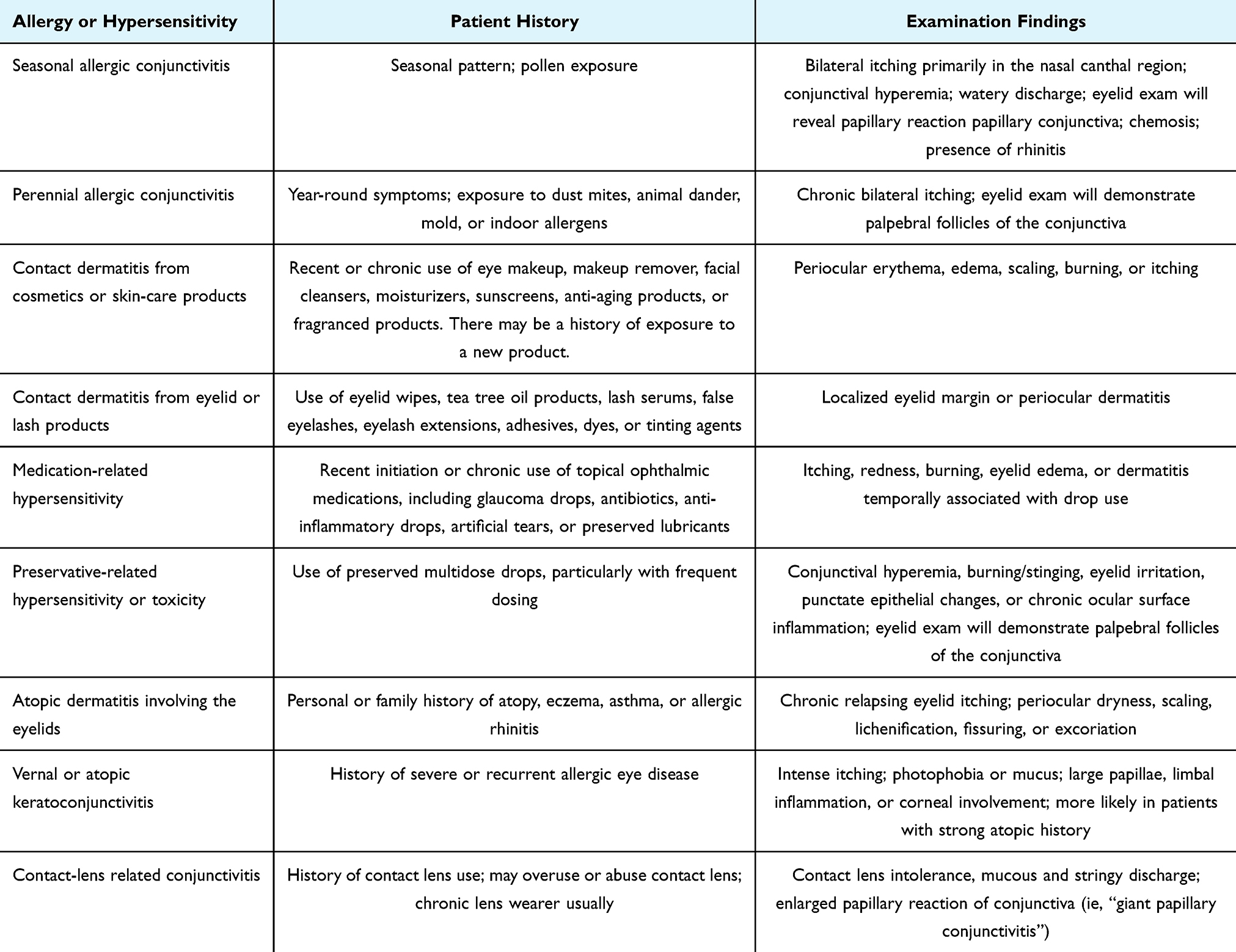 |
Table 2 Allergies and Hypersensitivity Conditions That Should Be Considered and Ruled Out When Evaluating Patients with Symptoms Suggestive of Demodex Blepharitis (eg, Itching, Tearing Redness), with or without Collarettes. Symptoms May Be Attributable to Demodex Blepharitis Alone, an Allergic or Hypersensitivity Condition as Defined Below, or Co-Existing Disease |
Currently, lotilaner 025% is only approved in the United States. Inaccessibility to lotilaner 0.25% in Europe limits ECPs to treat disease symptoms rather than its root cause. That said, European regulatory approval of lotilaner 0.25% is expected in 2027.27 Interestingly, a Delphi study conducted in the United Kingdom established consensus on best practice for the diagnosis and treatment of DB that was in alignment with the findings from the two DEPTH studies that were conducted prior to the FDA approval of lotilaner 0.25%.8,17,28 These data suggest that the results from these Delphi studies may be generally applicable.
Conclusion
The misdiagnosis of the patients in these cases indicates a need to increase awareness of DB throughout the eye care community and establish a diagnostic path for ECPs. Consensus from the DEPTH experts has provided an important foundation for establishing this diagnostic path. This, coupled with the FDA approval of lotilaner 0.25%, represents a regimen that could help mitigate the prevalence of misdiagnosis and prolonged patient burden.
Abbreviations
BCVA, best corrected visual acuity; DB, Demodex blepharitis; DED, dry eye disease; DEPTH, Demodex Expert Panel on Treatment and Eyelid Health; ECP, eye care provider; MGD, meibomian gland dysfunction; Neo-Poly-Dex, neomycin–polymyxin B–dexamethasone; SPEED, Standard Patient Evaluation of Eye Dryness; TBUT, tear break up time.
Ethics Approval and Informed Consent
Both patients included in this case series provided informed consent for the use of their clinical details. Consent forms will be provided during the submission process. Institutional approval was not required to publish the case details.
Consent for Publication
Both patients included in this case series consented to the use of their clinical details in this publication. Consent forms will be provided during the submission process.
Acknowledgments
The authors would like to thank Ivan J. Santiago, PhD, employee of i2Vision, for providing medical writing support for this publication. The authors would also like to thank Tarsus Pharmaceuticals, Inc. for funding this endeavor.
Funding
The DEPTH Panel Consensus project was funded by Tarsus Pharmaceuticals, Inc. Medical writing support for this manuscript was provided by i2Vision and funded by Tarsus Pharmaceuticals, Inc. Tarsus involvement in this project was limited to an accuracy review.
Disclosure
L. M. Periman is a consultant to Alcon, Aldeyra, Allergan/Abbvie, Amgen, Azura, B&L, Harrow, Kala, Lumenis, Myze, Nordic Pharma, Nusight Medical, Nusight Medical, Science Based Health, Scope, Sun, Tarsus; a speaker for Alcon, Allergan/Abbvie, Bausch, Lumenis, Mallinckrodt, Nordic Pharma, Science Based Health, Scope, and Sun; has served on advisory boards for Alcon, Aldeyra, Allergan/Abbvie, Amgen, Azura, Bausch, Dompe, Eyedetec, Harrow, Kala, Mallinckrodt, MD Elite, Myze, Nusight Medical, NuVissa, Science Based Health, Scope, Sun, Tarsus; has conducted clinical research for Bausch, Kala, Lumenis, and Tarsus; a shareholder for Eyedetec, Harrow, Myze, Nusight Medical, and Quench Method. R. Lindstrom is a consultant to and has stock or stock options in Tarsus. P. Karpecki is a consultant to Abbvie, Alcon, Aldeyra, Aramis, Atlas, Azura, Bausch & Lomb, BioTissue, Bruder, Bruno Vision Care, Dompe, Essilor, Eyedetec, Harrow, Healthe, Nordic Pharma, Oasis Medical, Oculis, Ocuphire, Oculus, OcuSoft, Orasis, RxSight, Science Based Health, Scope, Sentiss, Sight Sciences, Silk Tears, Sun Pharmaceuticals, Surface, Sydnexis, Tarsus, Thea, Topcon, Viatris, Vital Tears, and Zeiss; has received honoraria from Bausch & Lomb, Dompe, Mallinckrodt, and Tarsus; and has stock or stock options in AdOM, AI Optics, Azura, Barti, Danelli Ocular Creations, Eyedaptec, Eyedetec, Eyesafe, Hui.AI, iOR Holdings, Iveena, LacriSciences, LeGrande, LenTechs, Lubris, Mati Therapeutics, New Sight Reality, Ocular Science, OcuMedic, Omega Ophthalmics, Omera Medical, Ophthalmic Resources, Orasis, Percept Health, Cambium, Olympic Ophthalmics, RegenerEyes, Silk Technologies, Stuart Therapeutics, TearClear, TearSolutions, TecLens, Visant Medical, and Vision Path. B. Ayres is a consultant to and has received honoraria from Tarsus. E. Donnenfeld is a consultant to Aeon, Allegro, Allergan, Alcon, Aurion, Avellino Labs, Bausch & Lomb, CorneaGen, Covalent, CRST, Crystilex, BVI, Blephex, Dompe, ELT Sight, EyePoint Pharma, Foresight, Glaukos, Horizon Surgical Systems, Inversa, Ivantis, Johnson & Johnson, Kala, Katena, Lacripen, LayerBio, LensGen, Mati Pharmaceuticals, Melt Pharmaceuticals, MDBackline, Merck, Mimetogen, MOA, Nanowafer, Nordic Pharma, Novabay, Novartis, Novaliq, Ocular Innovations, Oculis, Odyssey, Omega Ophthalmics, Pfizer, Ocuhub, Omeros, PRN, Rayner, ReTear, RPS, Shire, Strathspey Crown, SUN, Surface, Tarsus, Tearscience, Thea, Trukera, Veracity, Versant Ventures, Visionary Venture, Visus, and Zeiss; has held leadership or committee positions at MOA, Oculis, and Ten Point; and has stock or stock options in Aeon, Aurion, Avedro, CorneaGen, Covalent, Crystilex, ELT Sight, EyePoint Pharma Glaukos, Horizon Surgical Systems, Inversa, Ivantis, Lacripen, LayerBio, LensGen, Mati Pharmaceuticals, Melt Pharmaceuticals, MDBackline, Mimetogen, MOA, Novabay, Ocuhub, Ocular Innovations Oculis, Rayner, ReTear, RPS, Strathspey Crown, Surface, Tarsus, TenPoint, Veracity, Versant Ventures, and Visionary Ventures. M. Farid is a consultant to Abbvie, Alcon, Bausch & Lomb, Biotissue, CorneaGen, Glaukos, Harrow, Johnson and Johnson Vision, Tarsus, Viatris, and Zeiss. I. B. Gaddie is a consultant to Alcon, Bausch & Lomb, Harrow, and Tarsus; has received honoraria from Bausch & Lomb, Harrow, and Tarsus; and has stock or stock options in Harrow and Tarsus. P. K. Gupta is a consultant to Azura, Alcon, Aldeyra, Abbvie, Bausch + Lomb, Dompe, Expert Opinion, HanAll Biopharma, J&J Vision, Kala, Mazado, Inc, Nordic Pharma, Ocular Science, Oculis, Orasis, Sight Sciences, Science Based Health, Spyglass, Surface Ophthalmics, Tarsus, Tear Clear, Thea, Tissue Tech, Inc, Trukera, Viatris, Visionology, Vital Tears, and Zeiss, and has stock or stock options in Azura, Expert Opinion, Orasis, Tarsus, Tear Clear, Surface, Spyglass, and Visionology. S. McGee is a consultant to Aldeyra, Abbvie, Alcon, Avellino, Lumenis, Bausch & Lomb, Bruder, Cynosure, Horizon, Optovue, Novartis, Sun, Versant, Kala, Dompe, RVL, Tarsus, Science Based Health, Thea, Oyster Point, Topcon, and Zeiss. K. K. Nichols discloses grants or contacts paid to her institution by Aramis, Kowa, Science Based Health, Sylentis, and TearScience; and is a consultant to Abbvie, Alcon, Alderya, Azura, Bausch & Lomb, Bruder, Cavalry, Cloudbreak, Dompe, Glaukos, Kendrion Biopharma, HanAll Bio, Visus/Tenpoint, Science Based Health, Harrow, Novartis, Novaliq, Oyster Point Pharma/Viatris, Santec, Sight Sciences, Sydnexis, Tarsus, TearSolutions, Thea, Topcon, and Trukera. S. Pflugfelder discloses grants or contracts paid to his institution by Alcon; is a consultant to Alcon, Dompe, Kala, Kowa, and Tarsus; and was an advisor for AstraZeneca. C. E. Starr is a consultant to Aesculus, Alcon, Aldeyra, Allgenesis, Allergan/Abbvie, Amgen, Azura, Bausch & Lomb, BlephEx, Bruder, CSI Dry Eye, Dompe, Eyebiotech Limited, Eye Care International, Glaukos, Johnson & Johnson Vision, Kala, Novaliq, Novartis, Nuvissa, Oculis, Olivio & Co., Ocubio, Oyster Point, Quidel, Sight Sciences, Sofia Biologics, Sun Pharma, Tarsus, Trukera, Versea, and Visionology; and has stock or stock options in CSI Dry Eye, Essiri LLC, Nuvissa, Sofia Biologics, and Visionology. N. Venkateswaran is a consultant to Abbvie, Alcon, Bausch & Lomb, Glaukos, Johnson and Johnson, Ocular Therapeutix, Sight Sciences, Tarsus, and Thea. E. Yeu was an employee of Virginia Eye Consultants and a board member, consultant, and stockholder of Tarsus Pharmaceuticals, Inc. (“Tarsus”) at the time of the study. She was also a consultant for Abbvie, AcuFocus, Adaptilens, Advanced Vision Group, Alcon, Aldeyra, Aurion, Avellino, Bausch & Lomb, BioTissue, BVI, Blephex, Bruder, Centricity, Dompe, Elios, Expert Opinion, Eyenovia, Foresight, Glaukos, Guidepoint, Iveric, Johnson & Johnson Vision, Kala, LayerBio, LensAR, Melt, New World Medical, OSRX, Oculis, Ocusoft, Samsara, Science Based Health, Sight Sciences, STAAR, Surface, Thea, Tarsus, Visus, and Zeiss. Dr. Yeu is now an employee of Tarsus Pharmaceuticals, Inc. C. Koetting is a consultant to Abbvie, Alcon, Bausch & Lomb, Dompe, and Tarsus; and has received honoraria from Alcon, Bausch & Lomb, Dompe, and Tarsus. The authors report no other conflicts of interest in this work.
References
1. Eberhardt M, Zeppieri M, Rammohan G. Blepharitis. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025. Available from: https://www.ncbi.nlm.nih.gov/books/NBK459305.
2. Lee SH, Chun YS, Kim JH, et al. The relationship between Demodex and ocular discomfort. Invest Ophthalmol Vis Sci. 2010;51:2906–9. doi:10.1167/iovs.09-4850
3. Trattler W, Karpecki P, Rapoport Y, et al. The prevalence of Demodex blepharitis in US eye care clinic patients as determined by collarettes: a pathognomonic sign. Clin Ophthalmol. 2022;16:1153–1164. doi:10.2147/OPTH.S354692
4. O’Dell L, Dierker DS, Devries DK, et al. Psychosocial impact of Demodex blepharitis. Clin Ophthalmol. 2022;16:2979–2987. doi:10.2147/OPTH.S374530
5. Barnett M, Simmons B, Vollmer P, et al. The impact of Demodex blepharitis on patient symptoms and daily life. Optom Vis Sci. 2024;101:151–156. doi:10.1097/OPX.0000000000002111
6. Chiang -C-C, Lin C-L, Tsai -Y-Y, et al. Patients with blepharitis are at elevated risk of anxiety and depression. PLoS One. 2013;8:e83335. doi:10.1371/journal.pone.0083335
7. Rhee MK, Yeu E, Barnett M, et al. Demodex blepharitis: a comprehensive review of the disease, current management, and emerging therapies. Eye Contact Lens. 2023;49:311–318. doi:10.1097/ICL.0000000000001003
8. Farid M, Ayres BD, Donnenfeld E, et al. Delphi panel consensus regarding current clinical practice management options for Demodex blepharitis. Clin Ophthalmol. 2023;17:667–679. doi:10.2147/OPTH.S399989
9. Aragona P, Barabino S, Di Zazzo A, et al. Dry eye disease: from causes to patient care and clinical collaboration-a narrative review. Ophthalmol Ther. 2025;14(7):1411–1428. doi:10.1007/s40123-025-01161-8
10. Cheng AMS, Galor A. Blepharitis and Demodex: insights into the pathophysiology and management of these conditions. Cat Ref Surg Today. 2025;1:34–37.
11. TYRVAVA® (varenicline solution) [prescribing information]. Oyster Point Pharma, Inc. a Viatris Company; 2006. Available from: https://www.tyrvaya-pro.com/files/prescribing-information.pdf.
12. TRYPTYR® (acoltremon ophthalmic solution) 0.003% [prescribing information]. Alcon Laboratories, Inc; 2025. Available from: https://alcon.widen.net/s/vmnmcnwkfq/tryptyr-pi.
13. VEVYE® (cyclosporine ophthalmic solution) 0.1% [prescribing information]. Harrow, Inc; 1983. Available from: https://vevye.nyc3.cdn.digitaloceanspaces.com/files/VEVYE-Prescribing-Information.pdf.
14. XIIDRA® (lifitegrast ophthalmic solution) 5% [prescribing information]. Bausch & Lomb, Inc. Available from: https://pi.bausch.com/globalassets/pdf/packageinserts/pharma/xiidra-prescribing-information.pdf.
15. CEQUA® (cyclosporine ophthalmic solution) 0.09% [prescribing information]. Sun Pharmaceutical Industries, Inc; 1983. Available from: https://cequapro.com/CequaPI.pdf.
16. McLeod A, Nau A. Anterior blepharitis: the front line of OSD. Review of Optometry. 2021. Available from: https://www.reviewofoptometry.com/article/anterior-blepharitis-the-front-line-of-osd.
17. Ayres BD, Donnenfeld E, Farid M, et al. Clinical diagnosis and management of Demodex blepharitis: the Demodex Expert Panel on Treatment and Eyelid Health (DEPTH). Eye. 2023;37:3249–3255. doi:10.1038/s41433-023-02500-4
18. Donnenfeld E, Nichols KK, Ayres BD, et al. The Demodex Expert Panel on Treatment and Eyelid Health (DEPTH) consensus regarding the preferred treatment for Demodex blepharitis. Clin Ophthalmol. 2025;19:1893–1904. doi:10.2147/OPTH.S525681
19. Yeu E, Wirta DL, Karpecki P, et al; Saturn Study Group. Lotilaner ophthalmic solution, 0.25%, for the treatment of Demodex blepharitis: results of a prospective, randomized, vehicle-controlled, double-masked, pivotal trial (Saturn-1). Cornea. 42;2023:435–443. doi:10.1097/ICO.0000000000003097
20. XDEMVY® (lotilaner ophthalmic solution) 0.25% [prescribing information]. Tarsus Pharmaceuticals, Inc; 2023. Available from: https://tarsusrx.com/wp-content/uploads/XDEMVY-Prescribing-Information-24JUL23.pdf.
21. Gonzalez-Salinas R, Yeu E, Holdbrook M, et al. Safety and efficacy of topical lotilaner ophthalmic solution, 0.25% for the treatment of Demodex blepharitis: a pilot study. J Ophthalmol. 2021;2021:3862684. doi:10.1155/2021/3862684
22. Gonzalez-Salinas R, Karpecki P, Yeu E, et al. Safety and efficacy of lotilaner ophthalmic solution, 0.25% for the treatment of blepharitis due to Demodex infestation: a randomized, controlled, double-masked clinical trial. Cont Lens Anterior Eye. 2022;45:101492. doi:10.1016/j.clae.2021.101492
23. Gonzalez-Salinas R, Yeu E, Holdbrook M, et al. Collarette elimination and Demodex mite eradication with topical lotilaner ophthalmic solution, 0.25%. J Ocul Pharmacol Ther. 2021;37:479–484. doi:10.1089/jop.2021.0011
24. Gonzalez-Salinas R, Yeu E, Quiroz-Mercado H, et al. Safety and efficacy of lotilaner ophthalmic solution 0.25% for the treatment of Demodex blepharitis: the Europa Study. Invest Ophthalmol Vis Sci. 2021;62:1332.
25. Gaddie IB, Donnenfeld ED, Karpecki P, et al. Lotilaner ophthalmic solution 0.25% for Demodex blepharitis: randomized, vehicle-controlled, multicenter, Phase 3 trial (Saturn-2). Ophthalmology. 2023;130:1015–1023. doi:10.1016/j.ophtha.2023.05.030
26. Liu W, Gong L. Anti-demodectic effects of okra eyelid patch in Demodex blepharitis compared with tea tree oil. Exp Ther Med. 2021;21(4):338. doi:10.3892/etm.2021.9769
27. Czępińska-Myszura A, Kozioł MM, Rymgayłło-Jankowska B. Pharmacotherapy of Demodex-associated blepharitis: current trends and future perspectives. Pharmacy. 2025;13(5):148. doi:10.3390/pharmacy13050148
28. Sharma N, Martin E, Pearce EI, et al. A Delphi approach to establishing consensus on best practice for the diagnosis and treatment of Demodex blepharitis. Cont Lens Anterior Eye. 2024;47(1):102080. doi:10.1016/j.clae.2023.102080
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.