Back to Journals » Clinical Ophthalmology » Volume 17
Using Light Meters to Investigate the Light-Myopia Association – A Literature Review of Devices and Research Methods
Authors Hönekopp A ![]() , Weigelt S
, Weigelt S
Received 24 May 2023
Accepted for publication 18 August 2023
Published 19 September 2023 Volume 2023:17 Pages 2737—2760
DOI https://doi.org/10.2147/OPTH.S420631
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Astrid Hönekopp, Sarah Weigelt
Department of Rehabilitation Sciences, Research Unit Vision, Visual Impairments & Blindness, TU Dortmund University, Dortmund, Germany
Correspondence: Astrid Hönekopp, TU Dortmund University, Department of Rehabilitation Sciences, Otto-Hahn-Straße 20, Dortmund, D-44227, Germany, Tel +49 231 755 8049, Fax +49 231 755 6219, Email [email protected]
Abstract: With the increasing prevalence of myopia, evaluating its relationship with objective light exposure as a potential adjustable environmental factor in myopia development has been an emerging research field in recent years. From a thorough literature search, we identify ten wearable light meters from human studies on light exposure and myopia and present an overview of their parameters, thereby demonstrating the wide between-device variability and discussing its implications. We further identify 20 publications, including two reanalyses, reporting investigations of light-myopia associations with data from human subjects wearing light meters. We thoroughly review the publications with respect to general characteristics, aspects of data collection, participant population, as well as data analysis and interpretation, and also assess potential patterns regarding the absence or presence of light-myopia associations in their results. In doing so, we highlight areas in which more research is needed as well as several aspects that warrant consideration in the study of light exposure and myopia.
Keywords: light exposure, outdoor exposure, myopia, wearables, lux
Introduction
The increasing prevalence of myopia worldwide is a cause for concern.1 Growing evidence suggests time outdoors2 and light exposure3 as adjustable environmental factors in myopia development. Hence, assessing the relationship between myopia and light exposure has been an emerging research field in the past years, regarding both animal4,5 and human6–8 studies. In human research, objective light measures are often also used to quantify time spent indoors vs outdoors. Thereby, myopia or associated metrics have repeatedly been associated with reduced light and/or outdoor exposure.6–9 Furthermore, intervention trials increasing children’s outdoor exposure found reduced myopia increase in the intervention groups.9–11 However, the current evidence is not unambiguous, as some investigations fail to detect associations between light exposure and myopia.12,13 Furthermore, many aspects are still unknown, eg, whether increased outdoor exposure affects both incidence and progression of myopia and which exact mechanisms underly the protective effect of outdoor exposure.14 While there is strong evidence for bright light as a key protective factor by inhibiting axial elongation through stimulation of retinal dopamine, there also are other hypotheses such as the involvement of vitamin D levels or the impact of different spatial frequencies or spectral composition of light indoors vs outdoors.14 Thus, further research on the association between myopia and light exposure is warranted.
Multiple studies on the association between objectively measured light exposure and myopia in humans have been conducted using various wearable light meters. These studies are subject to great variability, both regarding light meter specifications as well as research methods, and it is important to take this variability into account when assessing and comparing them. Apart from (1) general study characteristics like time of publication, considerations regarding research methods may concern (2) data acquisition, (3) parameters of the participant population, and (4) data analysis and interpretation. In the following, we will briefly review empirical findings on some aspects regarding (2)-(4).
(2) Regarding data acquisition, differences in light measurements from simultaneously worn, different light meters have been shown before.15–17 These differences are likely a combination of the devices’ specifications as well as how they were worn. The former claim is based on findings showing that deviations in light measurements between light meters and calibrated photometers vary between different types of light meters.15,18,19 This is not surprising since the light meters differ in several aspects, eg, spectral sensitivity or measurement range. With regard to device positioning, prior investigations revealed varying degrees of deviation between similar devices worn at different body positions.15,20,21
Furthermore, the light meters’ settings may affect the outcome. Ulaganathan et al (2017)22 systematically reduced the measurement duration and coarsened the sampling interval of instantaneous light measurements. They found a significant increase in the measurement variability of outdoor light exposure (daily time exposed to >1000 lux), but not group mean light exposure, when fewer measuring days or a coarser sampling interval were analyzed, and concluded that measuring for at least one week and at least every 2 minutes provided the most reliable outdoor light exposure measures.22 Geographical location and season of course also vary between investigations, and, eg, data acquisition during short daylengths, bad weather and low bright light availability may pose limited opportunities for investigations on associations between light/outdoor exposure and myopia.23 Any combination of these and other factors provides own challenges, eg, in choosing the optimal light meter.
(3) One relevant aspect of the participant population is participant age. Since myopia development differs across the lifespan, with school age as a critical period for development and onset of axial myopia,24 light exposure probably does not affect it in the same way across all ages. Another aspect is the overall light exposure. There has been speculation that a sample’s overall low (frequency of bright) light exposure may conceal associations between light exposure and, eg, refractive status.6,23 Also, Gordon-Shaag et al (2021)25 revealed greater myopia prevalence in ultra-Orthodox and religious than secular Israeli boys, but no group differences in outdoor (>1000 lux) exposure. They proposed a ceiling effect in the protective effect of outdoor exposure due to high light exposure across all participants, thus explaining the absent associations.25 Between-publication variability regarding refractive status assessment and refractive error classification might also be of relevance, as, eg, outcome differences between several methods to measure refraction have repeatedly been shown.26–28
(4) Finally, one major aspect regarding data analysis and interpretation is the calculation of time spent in indoor and outdoor environments. This is often done by quantifying the time spent in light intensities below and above a certain value, usually 1000 lux.6,8,12,13 This indoor-outdoor-cut-off (IO-cut-off) is also frequently used in other research involving personal light exposure.29–31 In myopia research, it has been applied in various circumstances – often without prior validation –, though there are indications that it may not always be the best estimator. For example, Mahroo et al (2013)32 suggested a higher IO-cut-off for a study by Dharani et al (2012)13 – who had initially used 1000 lux, but agreed that 1500 lux was indeed a better choice for their study.33 With regard to the light meters’ specifications, comparability of the IO-cut-off has, eg, been shown for two different, simultaneously worn devices (Actiwatch 2 and HOBO Temp/Light data logger).16 However, the previously mentioned findings of different devices’ light measurements differently deviating from calibrated photometers alone indicate a high probability of different ideal IO-cut-offs. For two devices, Howell et al (2021)19 empirically derived 533.15 lux (Actiwatch 2) and 850 lux (Clouclip) as corresponding to 1000 lux measured by a photometer. They further remarked that with a 1000 lux IO-cut-off, the photometer and Clouclip sometimes falsely classified indoors as outdoors, which was almost never the case for Actiwatch 2, due to its general underestimation of illumination.19
These and more aspects pose important challenges for comparing and integrating results of studies on the association between myopia and light/outdoor exposure. Thus, the purpose of this review is to give an overview of the parameters of the wearable light meters used in research on myopia and light/outdoor exposure and the publications investigating associations between them, as well as to reflect upon potential sources of variance between these studies. While there is also research on associations between dim light exposure and myopia,34 here, the term “light-myopia associations” (LMA) will be used to describe negative association between bright light and myopia – ie, more bright light exposure being associated with reduced myopia (metrics). Furthermore, while other factors may (also) underlie the protective effect of bright light/outdoor exposure on myopia,14 we focused on the measurement of (white) light intensity (lux). We hope that this work proves helpful in identifying relevant aspects when assessing or planning research on LMA.
Materials and Methods
Literature Search
In the literature search, all publications (journal articles, conference abstracts and posters, dissertations) using light measures with wearable light meters were included. If usage of a light meter, but no measurement or assessment of light was reported, and the device was already included, a publication was not included. The following steps were taken in the literature search: (a) 15 keyword searches were conducted in the PubMed database (see Supplementary Table 1), (b) the reference lists of the identified publications, and then again of the newly identified publications were searched, (c) publications from other sources like the own literature collection were included, and (d) a keyword search for (myopi*) AND (light) in Web of Science was conducted. For all N = 147 publications identified so far, (e) light meters that had been or may be used in research on light and myopia were extracted (see Supplementary Table 2). For each identified device, a keyword search for ([device name]) AND (myopi*) was conducted in PubMed and Web of Science. Furthermore, (f) a “cited references” search was conducted in Web of Science for all identified publications, in which wearable light meters had been used in combination with myopia research. Finally, (a) and (d) as well as (f) – for the N = 19 publications included in the analysis of research methods (see below) at that point – were repeated in January 2023 to include publications published up to and including 2022. In total, the literature search led to N = 169 publications. These were then assessed regarding their inclusion (see below). Figure 1 depicts a flowchart of the literature search, presenting the number of identified, in- and excluded publications.
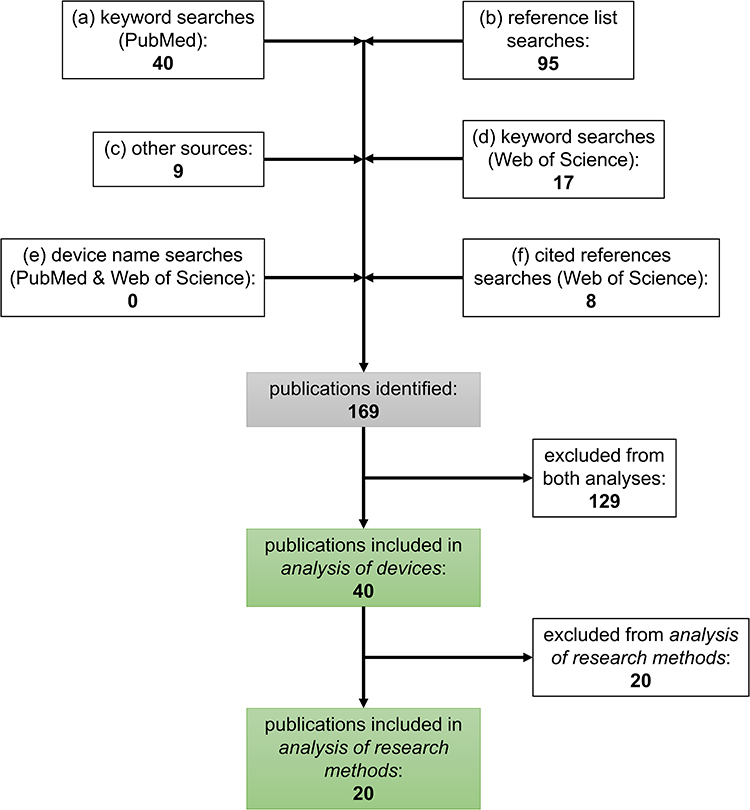 |
Figure 1 Flowchart of the literature search. The numbers indicate how many new publications were identified with the respective search strategies. |
Inclusion and Exclusion Criteria
Only English sources were considered. Inclusion criteria for the analysis of devices were as follows: (1) paper published in a scientific journal, dissertation, or conference poster – conference abstracts only if the device was not included via one of the former sources; (2) human participants wearing light meters; (3) myopia as a topic of the publication, including methodological investigations; (4) lux data collected, but not necessarily analyzed at all or in direct relation to myopia. If the same data was presented in a conference abstract and a paper, dissertation or conference poster, the conference abstract was excluded. For the analysis of research methods, the following inclusion criteria were applied: (1) paper published in a scientific journal, dissertation, or conference poster; (2) human participants wearing light meters; (3) myopia as a topic of the publication; (4a) lux data analyzed as a main outcome and in direct relation to refractive error/myopia/a proxy metric like axial length (AL) OR (4b) methodological investigation within the framework of wearable sensors in light exposure-myopia research, also reporting results on the association between (white) light intensity (lux) and refractive error/myopia (metrics). Due to criteria 4a and 4b, publications primarily concerned with other associations (eg, myopia – circadian rhythm), in which the relation between (white) light intensity and myopia was also analyzed, were not included because we assumed that their methodology would have been optimized for assessing their main objective rather than LMA. In one case, a study within a dissertation35 was later published in a paper,36 and both were identified in the literature search. Since methods, analyses and results on light exposure and refractive error appear to be similar in both publications, we only included the paper. Another publication did not fit criterion 4a perfectly as the analyses on LMA were not a main focus. However, as the investigation assessed an intervention to increase light exposure and time outdoors for myopia control and not other associations with light exposure and myopia, and analyses on LMA were conducted, it was included.37
Results
Analysis of Devices
We identified ten wearable light meters from human studies on light exposure and myopia based on 40 publications. As stated above, this review focuses on the association between myopia and light intensity measured in lux – the measurement unit of illuminance. Illuminance is defined as irradiance weighed by the photopic luminous efficiency function V(λ), which is based on the spectral sensitivity of human central vision, if not specified to follow another luminous efficiency function.15,38 However, in practice, the devices’ illuminance estimation is not always accurate, as, eg, their spectral sensitivity may deviate from V(λ).15,18 This should be kept in mind regarding the terminology used to describe the devices’ light measurement capacities.
In the following, all identified devices will be described briefly, together with a list of the associated publications. More detailed information is presented in Table 1. The information provided in the publications and by the manufacturers did not always contain all relevant details for our descriptions. Where possible, we asked authors and/or manufacturers for the respective details. If we could not receive the information, we consulted further sources, eg, other publications. If we could still not get the respective information, or it was conflicting between different sources, n/a is stated in the table. Also, while monetary aspects are certainly relevant for planning investigations, they are not included here. Furthermore, not all devices are commercially available (anymore), the reported specifications may change without notice, and devices used in cited publications might have had different specifications than reported here, eg, if an earlier version was used.
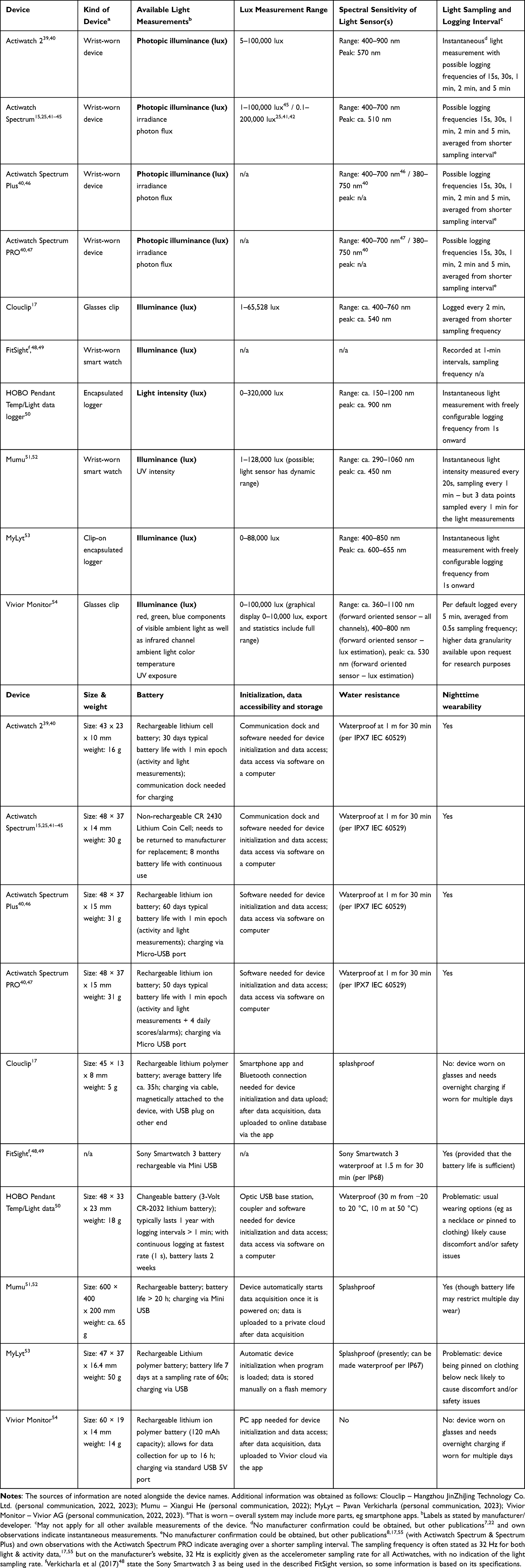 |
Table 1 Overview of the Identified Devices |
The Actiwatch 2 (Philips Respironics, Murrysville, PA, USA)6,7,16,23,34,56–60 is a wrist-worn actigraphy device. It includes a solid-state “piezo-electric” accelerometer sampling at 32 Hz and a silicone photodiode light sensor, and measures activity and photopic illuminance (lux). Events can be recorded via button press.39
The Actiwatch Spectrum (Philips Respironics, Murrysville, PA, USA)25,41,42,61–66 is a wrist-watch and activity monitor. It is also equipped with a solid-state “piezo-electric” accelerometer sampling at 32 Hz to record activity, and an event marker button. Light, however, is measured via three (red, green, blue) color-sensitive photodiodes, and available light measurement units are irradiance (µW/cm2), photon flux (photons/cm2/s), and photopic illuminance (lux). Furthermore, the device has an off-wrist detector.43 Following its production stop, the Actiwatch Spectrum Plus and PRO were its successor models.
The Actiwatch Spectrum Plus (Philips Respironics, Murrysville, PA, USA)8,17 is a wrist-watch and activity monitor with many features like off-wrist detection, an event marker button, and light measurements similar to the Actiwatch Spectrum. Activity is also sampled at 32 Hz, but via an MEMS type accelerometer.46
The Actiwatch Spectrum PRO (Philips Respironics, Murrysville, PA, USA)67 includes the same features as the Actiwatch Spectrum Plus and additionally provides the option to record two subjective scores (manually or on a programmed schedule) and alarms to remind participants to enter them.68
The Clouclip (Hangzhou JinZhiJing Technology Co. Ltd., Hangzhou, China)17,20,69–73 is a small device clipped to the right side of spectacles. It can measure viewing distance and duration via a laser ranging module, illuminance (lux) via an illuminance monitoring module, and viewing angle via a three-axis accelerometer.17,74 Two versions with partially different features are internationally available for personal use (Clouclip P2) and for business and research purposes (Clouclip M2),74 though similar sensors are used in both (Hangzhou JinZhiJing Technology Co. Ltd., personal communication, 2022). If no movement is detected for 40 seconds, Clouclip M2 goes into sleep mode until movement is detected again, but for at least 2 minutes.17 Clouclip P2 goes into sleep mode after 10–20 seconds without movement (Hangzhou JinZhiJing Technology Co. Ltd., personal communication, 2022).
The FitSight fitness tracker (patent WO2015152818A1)12,48,75 was developed by researchers48 to record, quantify, indicate, and motivate daytime outdoor activity. It includes a smart watch with a custom-made app and a smartphone app, and records ambient light illuminance (lux). The smart watch app also consists of an accelerometer function. Time outdoors is calculated by summarizing the time spent above an illumination threshold and via Bluetooth, this information is relayed to the smartphone app. A congratulatory message for reaching the daily outdoor time target and motivational messages if the target is not reached at specific times can be presented. One can also monitor physical activity in 30-minute epochs.48
The HOBO Pendant Temp/Light data logger (Onset Computer Corp., Bourne, MA, USA)9,13,16,36,37,76–78 is a small logger recording temperature and light intensity (lux) readings. Two versions have been used in the identified publications, the HOBO Pendant UA-002-64 and the HOBO Pendant UA-002-08, which only differ in their memory capacity (64 KB vs 8 KB).50
The Mumu,51,79,80 developed by researchers,51 is a smart watch containing a light sensor, a three axis-accelerometer, and a GPS receiver. It can sample illuminance (lux) and ultraviolet (UV) intensity, steps, and location data. Furthermore, weather and temperature can be synchronized in real time, and weather information is sampled as sunny/cloudy. Wearing status can be determined through light sensors in both front and back of the watch.51 Parents can manage the device via an app,79 and there is a website portal for teachers so that they, eg, can intervene if students wear the device improperly. A next generation, more lightweight device with longer battery life has also been developed and will eventually be put on the market (Xiangui He, personal communication, 2022).
The MyLyt53 is a prototype developed at the LV Prasad Eye Institute (Hyderabad, India) to track real-time light exposure. It records illumination (lux) against real time. A light-emitting diode can indicate data sampling (green) and low battery (red). Further improvements, eg, a smartphone connection for data transfer or reducing size and weight, are planned.53
The Vivior Monitor (Vivior AG, Zurich, Switzerland)81 is small device clipped to the right side of spectacles via an adapter. It encompasses two optical time-of-flight distance sensors directed forward and 30° downward, an ambient light sensor with separate red, green, blue and infrared channels directed forward, a combined UV and ambient light sensor directed upward, as well as motion and orientation sensors (accelerometer, gyroscope, magnetometer). Thus, the device can record various parameters, like viewing distance, head rotation, illuminance (lux), exposure to red, green, and blue light, and UV exposure. The illuminance measure is derived from the forward-oriented sensor as a mixture of the channels. Currently, the upwards-oriented light sensor is mainly used to quantify UV exposure.54 The device starts measuring when attached to the adapter, and stops when detached or when the spectacles are taken off.82 It can be used to create viewing profiles with recommendations for glasses and viewing behavior.
Additionally, we identified the Akeso eye care glasses (Beijing Akeso Technology Co., Ltd., Beijing, China),83 which have sensors installed in the right spectacle arm and contain a six-axis sensor, a UV light sensor, and a proximity sensor. Time of wearing, being outdoors, and near viewing can be recorded.83 Fan et al (2022)83 describe UV ≥ 1 or lux ≥ 1500 to be recognized as outdoors, and UV < 1 or lux < 1500 as indoors. We could not determine if the device can provide lux data, or if lux is only used to determine outdoor time. Thus, the device is not included in Table 1.
In summary, researching and developing devices to measure light exposure in the context of myopia is a rapidly developing field of research, and several other devices are being or have recently been developed, eg, the LUMINO-SD.84 Furthermore, there are a number of other light meters that could theoretically be used for such research. Hartmeyer et al (2022)85 present an overview of light dosimeters used in previous studies on non-visual effects of light.
Analysis of Research Methods
We identified 18 journal articles,6–9,12,13,16,34,36,37,41,42,60,71–73,76,80 one dissertation,59 and one conference poster.78 A detailed overview on their methodological aspects and findings regarding LMA can be found in Supplementary Table 3. For completeness, publications within a similar context but not fitting the inclusion criteria for this analysis23,62–64,81,83 are mentioned in Supplementary Information S1.
In the following, the publications will be assessed regarding selected methodological aspects to illustrate their methodological variety in (1) general characteristics, (2) data acquisition, (3) participant population, and (4) data analysis and interpretation. For the first three topics, we also looked for potential patterns regarding these aspects and the publications’ results supporting or not supporting LMA. Usually, no such patterns were observed. This is not surprising, given the large number of factors potentially influencing the results, the small number of publications and the usually large methodological variability. The absence of apparent patterns will thus not be discussed in detail for every aspect, but any interesting discoveries will. Furthermore, it was not attempted to assess such patterns for data analysis and interpretation aspects, since (almost) no grouping of publications in terms of these aspects was possible. Reanalyses16,34 are not generally included to not give a skewed impression of the data. If they are considered, it is explicitly stated. Lastly, there is a large overlap in the participants of two publications,6,7 but since one is cross-sectional and one primarily longitudinal, they will be considered separately.
General Characteristics
Time of Publication
To assess potential time trends regarding the publications or results on LMA, we assessed them regarding their time of publication. The oldest publication stems from 2011,78 the most recent one from 2022,37 the last year included in the review. The number of publications has grown more rapidly in more recent years, as six publications were published in the first,6,7,13,36,76,78 and twelve in the second half of said timeframe.8,9,12,37,41,42,59,60,71–73,80 Noticeably, the four oldest publications all report no LMA.13,36,76,78 The other four publications with no or only few such evidence were published later,12,41,42,59 in between publications supporting LMA. Importantly, the four oldest publications also share other features as will be discussed below. Thus, no clear-cut conclusion can be drawn based on time of publication alone.
Type of Study
Lingham et al (2020)86 state that longitudinal, but not cross-sectional studies using light meters found associations between higher average daily light exposure and slower eye growth. This is not reflected in our analysis, as LMA have been found both cross-sectionally and longitudinally. Of the ten cross-sectional publications, five show support for LMA,7,8,71–73 and five (almost) none.12,13,36,41,76 Of the eight longitudinal studies, the respective numbers are five7,9,37,60,80 and three,42,59,78 though one of the latter longitudinal studies only encompassed three months.78 Especially considering this, longitudinal publications tend to report LMA more often than cross-sectional ones. However, since one longitudinal publication reporting LMA60 and three cross-sectional ones not doing so36,41,76 have adult participants, this pattern does not exist when only considering publications with children.
Data Acquisition
Measurement Device
As various devices with different specifications (see Table 1) have been used to assess LMA, we considered potential associations between devices and wearing positions and results on LMA. The number of publications per device are: HOBO Pendant Temp/Light data logger – six,9,13,36,37,76,78 Actiwatch 2 – four,6,7,59,60 Clouclip – three,71–73 Actiwatch Spectrum – two,41,42 Actiwatch Spectrum Plus – one,8 FitSight – one,12 Mumu – one.80 No publication with Actiwatch Spectrum PRO, MyLyt or Vivior Monitor fit the inclusion criteria. Of the six HOBO Pendant Temp/Light data logger publications, only two support LMA.9,37 A somewhat reversed pattern emerges for the Actiwatch 2, where three of the four publications support LMA.6,7,60 The publication with the Actiwatch Spectrum Plus reports results in favor of LMA,8 while the two publications with the Actiwatch Spectrum either found no41 or only little42 support. The publication with Mumu shows strong support,80 the one with FitSight only minimal.12 Finally, all three publications with Clouclip strongly support LMA.71–73
The devices used entail differing wearing positions. While the HOBO Pendant Temp/Light data logger is usually worn forward-facing at the chest or collar, it has been mounted on a pedestal facing skyward in one case,36 and one publication does not report its wearing position.78 Clouclip can only be worn on the right side of spectacles, and all wrist-worn devices were worn as intended in the publications.
While there is no apparent pattern regarding the support of LMA, it is interesting that the HOBO Pendant Temp/Light data logger was used in the four earliest publications, in which no such support was found.13,36,76,78 Possibly, its technical specifications or ways of wearing may play a role here – though the two more recent publications with this device do report LMA.9,37 Furthermore, the publications with Clouclip71–73 are the only ones included that measured eye-level light exposure. All three of them supporting LMA may suggest that relevant differences in light exposure are indeed best uncovered in this manner. Overall, while such hints may suggest specific devices and their wearing location as better suited for identifying LMA, the small number of included publications makes this assessment speculative at this point.
Sampling and Logging Interval
As a measurement frequency (instantaneous sampling) of ≤ 2 minutes has been recommended for reliable ambient light and outdoor exposure measurements,22,36 we reviewed this aspect. Importantly, sampling and logging interval are not always the same – some devices log an averaged value of data sampled at finer intervals. The measurement frequency was consistent with the above recommendation in most publications, with logging intervals between 10 seconds36,37,78 and 2 minutes.71–73 The underlying sampling interval was sometimes even finer due to averaged logging. There are three publications with instantaneous sampling intervals coarser than 2 minutes – namely 5 minutes –, two of which did not find LMA,13,76 and one did.9 Furthermore, Read et al (2018)16 resampled data from Read et al (2014, 2015)6,7 at 5 minutes, and still found significantly lower outdoor light exposure in myopic than non-myopic children in these data. Generally, the absence of an apparent results pattern is not surprising since the recommended measurement frequency22,36 was almost always fulfilled.
Measurement Duration
Similarly, almost all publications report a measurement duration of seven days or longer, thus laying within the recommended timeframe of ≥ one week,22 so the absence of a results pattern is again unsurprising. In one of the two publications with a shorter duration, participants wore the device for three days, and no LMA were found.76 In the other one, participants wore the device for six days (three before, three after an intervention), and LMA were found.37 All other durations varied between seven days9,13,71–73 and one year.80
Geographic Location
The publications’ data was acquired in six countries: USA (five),8,36,41,42,73 Australia (four),6,7,60,76 New Zealand (one),78 China (four),37,71,72,80 Taiwan (one),9 Singapore (two),12,13 and the UK (one).59 We assumed two locations based on the authors’ affiliations.71,78 Thus, an important result of this analysis is the grave lack of data for many parts of the world. Notably, while there is a high myopia prevalence among school children in both East Asia and Singapore,87 all five publications from East Asia (China & Taiwan) report LMA,9,37,71,72,80 but either no13 or only few12 LMA were found in both Singaporean publications, all of which were conducted with school-aged children. No other pattern regarding results on LMA was detected.
Season
A relationship between season and myopia development has repeatedly been shown – for example, myopia progression and axial elongation in children is slower in summer than winter, which may be related to children spending more time outdoors during summer.88–90 Season therefore is an important factor that may influence the strength or even presence of LMA. Thus, we assessed the publications in this regard, though this is challenging for multiple reasons. For once, while there are highly distinct seasons at many locations in the world, this is not the case for others. And even for locations with distinct seasons, aspects like weather or daylength and their between-season differences are highly variable. We did not attempt to assess potential patterns between season and results on LMA, as season is not usually systematically controlled in the publications and many related aspects vary greatly between them: In four publications, no information is available on the season of data acquisition,12,71,72,76 and in another four, the analyzed data was acquired during one season (summer,8,59 winter,78 “mild, rainy season”13). Participants in He et al (2022)80 wore the device for one year, thus covering all seasons. In five further publications, different participants participated in different seasons,6,36,37,41,73 and in the remaining four, the same participants participated multiple times and across different seasons7,9,42,60 – in both cases, we sometimes presumed this based on measurement periods. While season was analyzed with regard to light exposure in six publications,7,36,41,42,59,60 it was investigated within LMA in only three: One reports seasonal differences on associations between refractive groups as well as AL and light exposure,60 one found season-independent light exposure differences between refractive groups,7 and one detected seasonal light exposure differences, but no effect of refractive groups upon them.42 Due to the relationship between season and myopia development, the large between-publication variation regarding season of data acquisition and whether it is systematically controlled or even reported should be considered as seasonal differences might influence LMA.
Measurement of refractive status and refractive group classification are also aspects of data acquisition, but they are closely related to aspects regarding the participant population as well, and will be considered in the next paragraph.
Participant Population
Number of Participants
The publications show large variability in the number of (analyzed) participants, ranging from twelve78 to 629580. There may be a tendency for publications with more participants to support LMA more often than not and vice versa: Of the nine publications analyzing more than 80 participants, seven report results in support of LMA,6,7,9,37,71,72,80 and only two show little to no support.12,13 Of the nine publications with fewer than 80 participants, only three present strong8,60,73 and six little to no support.36,41,42,59,76,78
Participant Age
Only four publications investigated adult participants,36,41,60,76 while 14 publications studied children. Of the publications targeting adults, only one60 supports LMA, while nine of the publications with child data do.6–9,37,71–73,80 As stated before, the only publication based on adults reporting LMA is longitudinal.60 Furthermore, as can be seen below, the three publications with adult data not reporting LMA are the ones with the highest percentage of myopic participants in the sample. LMA might thus be more readily seen in children, but more data is needed to confirm this potential pattern. In children, the investigated ages span 5–18 years, the age range – where reported – varying between one12 and nine years.73 As can also be seen in Figure 2, there was no apparent pattern regarding participant age and reporting LMA.
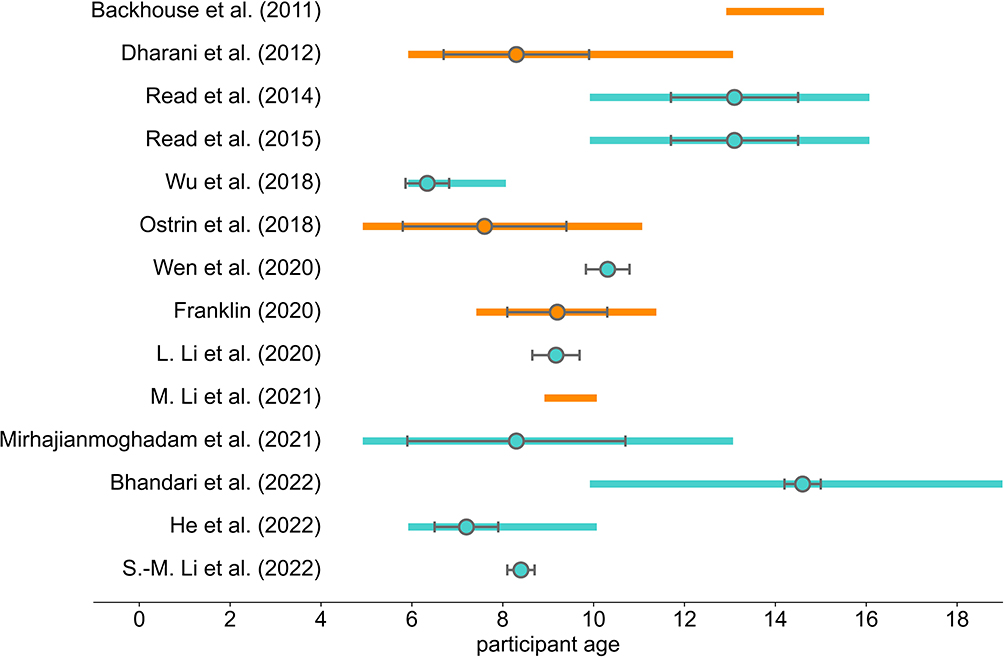 |
Figure 2 Participant age distribution in publications with children. The bars present age range of the sample, the circles and accompanying gray lines indicate mean and standard deviation. Since age range is usually stated in full years in the publications, we presented it as including the year given as the upper limit – eg, an age range of 13–14 years is presented as 13–14.99 years. Turquoise bars indicate that the publication (strongly) supports LMA, Orange bars indicate no or only minor support for LMA. If available, the information is presented for the analyzed sample – otherwise, it refers to the enrolled sample or the sample completing the trial (prior data exclusion for analysis). As no information on mean and standard deviation was available for the complete sample for Read et al (2015),7 said information was taken from Read et al (2014),6 with 101 of the 102 underlying participants being analyzed in Read et al (2015).7 |
General Time Spent in Bright Light Levels
Suggestions have been made that high or low bright light exposure of the entire sample may play a role in the results on LMA.6,23,25 Thus, we extracted information on the time the overall sample spent in >1000 lux, which was most commonly used to estimate time in outdoor light. For four publications, no such data exist.9,71,76,80 The overall time spent in >1000 lux varied largely – from 0.5 hours/day (mean all)73 to 1.67 hours/day (mean myopes) and 1.98 hours/day (mean emmetropes), respectively.72 Eleven publications include data on average lux exposure (mean or median).6–8,12,13,36,37,41,59,72,73 Here, the values varied between 164 lux (median)59 and 1669.46 lux (mean).41 There was no apparent relationship between time in >1000 lux or average light exposure and results on LMA. Importantly, measured time spent in >1000 lux and average light exposure may not only vary due to “real” exposure, but also due to factors like device specifications or wearing position. Yet, findings such as Clouclip having been used in the publications with the least73 as well as the most72 >1000 lux exposure show that such between-publication differences are not only determined by device specifications or wearing position. What may also potentially complicate comparisons is the fact that the times during which lux data was analyzed vary between publications. This will be discussed further in the data analysis and interpretation section, but regarding the light exposure aspects discussed here, no systematic variation was apparent with regard to analyzed times. Although we did not find a pattern regarding findings on LMA, the large variability in overall exposure time to >1000 lux as well as average lux exposure suggest that a sample’s general light exposure might indeed be a relevant factor to consider when assessing LMA, and there are many aspects that may complicate respective assessments.
Assessment of Refractive Status and Refractive Error Classifications
There are various ways to assess refractive status and to classify refractive error, and it can be assumed that the choice of method has an impact on the measured refractive status, as well as on which and how many participants will be classified into the respective refractive error groups. For example, non-cycloplegic autorefraction has repeatedly been shown to overestimate myopia compared to cycloplegic autorefraction, especially in younger children.26,27 Furthermore, cycloplegic autorefraction has been found to be more sensitive in measuring refractive error, and to measure a more myopic spherical equivalent refraction (SER) compared to non-cycloplegic subjective refraction, with the between-method difference decreasing with age.28
In 13 publications, participants were classified into refractive error groups, which were then used for analyses on light exposure. Classification was based on history and habitual correction in one publication,41 and on a questionnaire indirectly assessing refractive status in two.8,73 In the other ten publications, SER was used, whereby Dharani et al (2012)13 do not state its kind. Apart from that, either subjective, non-cycloplegic refraction6,7,60,76 or cycloplegic autorefraction9,12,42,72,80 was measured. In He et al (2022),80 the analysis regarding light exposure was not performed with the refractive groups per se, but with incident myopia. Schmid et al (2013)76 further split myopic participants into stable and progressing based on their history. In four additional publications, refractive error groups were not used for analyses on LMA, but were defined nonetheless based on autorefraction, either without36 or with37,59,71 cycloplegia. Lastly, Backhouse et al (2011)78 did not group participants via refractive status, but report cycloplegic autorefraction measurements. Thus, 15 publications include direct measurement of refraction: In one, the way of measurement is unspecified,13 four report non-cycloplegic subjective refraction,6,7,60,76 one non-cycloplegic autorefraction,36 and nine cycloplegic autorefraction.9,12,37,42,59,71,72,78,80
SER cut-offs for myopia, usually either applied on the eyes’ average or the right eye, were defined in 14 publications. The most liberal cut-off was < −0.25 D SER.42 The overwhelming majority of publications used the common ≤/< −0.50 D SER,6,7,9,12,13,37,59,71,72,76,80 though as described, this was based on different ways of refraction measurements: Subjective, non-cycloplegic refraction, cycloplegic autorefraction, or a non-specified refraction measurement are reported in the respective publications. Read et al (2014, 2015)6,7 additionally specified at least one eye needing to exhibit < −0.75 D SER apart from both eyes’ average being ≤ −0.50 D, and Franklin’s (2020)59 ≤ −0.50 D SER cut-off needed to be fulfilled for either eye. Both reanalyses16,34 used the ≤ −0.50 D SER cut-off, with Landis et al (2018)34 also applying the additional criteria as Read et al (2014, 2015).6,7 In two publications, having used either non-cycloplegic subjective refraction60 or non-cycloplegic autorefraction,36 more restrictive cut-offs of ≤ −0.75 D SER60 and ≤ −1.00 D SER36 were applied, respectively. There was no apparent pattern regarding LMA for both refractive status assessment and refractive error classification, but as both display some between-study methodological variability, these aspects should be kept in mind nonetheless.
Percentage of Myopic Participants
The within-sample distribution of refractive status may also be of interest when analyzing potential effects on refractive status. For example, possible differences between myopic and non-myopic participants or myopia-related associations with refractive status might be difficult to detect if there are only few myopic or non-myopic participants. Since amount and type of information on participants’ refractive status vary substantially between publications, we present the percentage of myopic participants in the sample to investigate this aspect. Of course, aspects like range, mean, standard deviation or skewedness of refractive status may also be relevant. Backhouse et al (2011)78 do not report a percentage of myopic participants, so we calculated it based on a ≤ −0.50 D SER myopia cut-off. A great variance in the proportion of myopic participants between publications is readily apparent, ranging from 4.4%59 to 85.2%.36 When only considering publications that specifically analyzed light exposure with regard to refractive groups, the percentage of myopic participants ranges from 13.3%42 to 67.3%.41
It is interesting to note that while the publication with the lowest percentage of myopia (4.4%)59 did not find LMA, the publications with the second and third lowest percentage (6.8%80 and 10.53%9) did. Both were intervention studies with many enrolled participants, namely 629580 and 930.9 The three publications with the highest proportion of myopic participants (62.9%,76 67.3%41 and 85.2%36) report no LMA, and their samples are all sized N = 55 or below. This might point to large sample sizes being necessary to assess LMA in case of rather unevenly distributed refractive error or status. However, assuming a pattern based on these few observations is highly speculative, and it should also be noted that the three publications with the highest proportion of myopic participants investigated adults,36,41,76 while those with the smallest proportion investigated children.9,59,80
Data Analysis and Interpretation
IO-Cut-off
As described above, the chosen IO-cut-off is worth considering, especially since 1000 lux is commonly applied, but may not always be the best estimator to distinguish indoor from outdoor light. In three publications, an IO-cut-off was either not needed,7,71 or not based on lux alone.80 The 1000 lux IO-cut-off was chosen in 14 publications.6,8,9,12,13,36,37,41,42,59,60,72,73,78 Thereby, Alvarez & Wildsoet (2013)36 had originally determined 882 lux as IO-cut-off based on own measurements, but as the results did not differ compared to 1000 lux, they used the latter for consistency. Schmid et al (2013)76 applied two IO-cut-offs, one potentially including some bright indoor light (500 lux) and one definitely only including outdoor light (10,000 lux). Thus, despite the use of varying devices with different specifications, the 1000 lux IO-cut-off was applied in almost all publications, including the reanalyses.16,34
Basis of IO-Cut-off
We examined the justification of the IO-cut-off within the 15 publications using one. Own pre-measurements for its determination are only reported in three publications, two36,76 of which used similar devices for these pre-measurements and data acquisition, and one9 used a luxmeter for the pre-measurements. In all other publications, usage of the chosen IO-cut-off is either not justified or other literature is cited for it.
In some publications, other additional measurements with the devices are reported: Correlations between devices and/or between the devices and a luxmeter were sometimes investigated,6,41,59,73 or lux values were measured in various indoor and outdoor conditions.13,41 Additionally, Ostrin (2017)41 tested the devices against a UV sensor and Franklin (2020)59 investigated how the devices’ rotational orientation may affect measurements. Lastly, for their reanalyses, Landis et al (2018)34 examined the devices’ sensitivity at dim illuminations, and Read et al (2018)16 determined the comparability between HOBO Temp/Light data logger and Actiwatch 2. In summary, while the IO cut-off of 1000 lux is generally accepted and used for various devices and settings, in the vast majority of cases its appropriateness for the given situation is not verified.
Analyzed Times for Light Data
Differences in analyzed times could complicate between-publication comparisons or a consideration of the overall picture. In fact, the publications differ greatly in the times during which light and/or outdoor data is analyzed. Read et al (2014, 2015)6,7 analyzed light data from 6:00h-18:00h, eg, for the calculation of daily light exposure in Read et al (2014),6 but 24 hours/day are considered for aspects like the daily light exposure pattern. Read et al (2015)7 state that the mean light exposure during the excluded times was uniformly low. Some publications used 7:00h-19:00h for analysis,12,13,59,80 including one reanalysis.16 Wen et al (2020)72 analyzed light data from 7:00h-20:00h, stating that a vast majority of light exposure lay within this timeframe. Alvarez & Wildsoet (2013)36 analyzed light data from sunrise to sunset, and Wu et al (2018)9 only analyzed device-measured light data during in-school times, as the wearing compliance was considerably lower out of school. Bhandari et al (2022)73 considered data from wake to bed time. Comparably, waking hours were considered in the second reanalysis.34
In the remaining publications, times included in the analyses are not explicitly stated,8,37,41,42,60,71,76,78 though a device wearing or recording time is specified in all but one.78 In five cases, 24 hours/day wearing or recording is reported.8,37,41,42,60 As a wrist-worn device was used in four of these publications, it is likely that this continuous data was also included in the analysis. In one publication, however, the device was pinned on clothing, so it may not have been worn continuously – though the analysis description indicates that data from 24 hours/day was in fact analyzed.37 Furthermore, daily recording time was specified as 7:00h-7:00h on the following day in this publication.37 In the last two publications without explicit mention of analyzed times, the device wearing time is reported as waking hours76 and throughout the day,71 respectively.
As (most of) daytime is included for analysis in all publications, the between-publication differences in analyzed times are probably not so problematic for comparisons regarding bright/outdoor light exposure – but for aspects like mean light exposure in the overall sample, between-publication comparisons are difficult if varying times are analyzed, and even more so if the analyzed times are not completely clear. Thus, present differences might indeed conceal potentially relevant associations that might be uncovered when considering more than one publication.
Exclusion and Replacement of Light Data
Like analyzed times, exclusion and replacement of data is important to consider, and again we found high between-publication variability. Thus, the procedures of light data exclusion and replacement will be reported in detail. While they are reported in most publications, the type and amount of information provided varies. Information on the respective details stated is presented in Supplementary Table 3. Here, we focus on (1) criteria for exclusion and/or replacement of specific invalid data, (2) criteria for exclusion of complete days and/or data sets, and (3) reported amount of in- and excluded data. The procedures applied in the two included reanalyses16,34 are considered here was well – though as Read et al (2018)16 refer to the publications describing the acquisition of their reanalyzed data for analysis procedures,6,7,13 this reanalysis will only be mentioned in case of additional information.
(1) Data was sometimes excluded as invalid in case of ≥15 minutes of complete inactivity and/or darkness during daytime (indicating covered light sensors and/or device removal)6,7,59,60 and replaced if certain criteria applied: In Read et al (2014, 2015),6,7 for any diary-documented “off-wrist” times, light levels were estimated as the average of 5 min before and after removal if consistent with the diary as indoors or outdoors (1000 lux IO-cut-off). In Read et al (2014),6 inconsistency only occurred for diary-recorded outdoor activities, in which case the mean outdoor light level over the same time averaged across all other days was used for estimation. Ulaganathan et al (2019)60 estimated light levels for excluded data as the average light level 5 min prior device removal, if consistent with the diary-reported activity. If not, the respective data was removed. Franklin (2020)59 substituted excluded data – on valid days only, see below – with the average for the same time period from valid days. Reanalyzing data from Read et al (2014, 2015),6,7 Landis et al (2018)34 describe that the activity diary was used to estimate illuminance for non-wear times.
(2) Often, criteria were defined for excluding days and/or data sets. Dharani et al (2012)13 excluded days with all light measures <100 lux, assuming non-wear of the device. Read et al (2014, 2015)6,7 only included days with ≥90% of valid data to determine average daily minutes in >1000 lux. Ostrin (2017)41 and Ostrin et al (2018)42 excluded days with device removal for >30 minutes or zero light exposure for ≥30 minutes during daylight, and nights if the device had been removed for any part of it. Wen et al (2020)72 only considered days with data from ≥80% of the required wearing time and data sets encompassing at least three weekdays and one weekend day (one week measurement period) as valid. Franklin (2020)59 only included days including 90% of valid data during daytime and data sets with at least five (out of nine) valid days. Data was excluded in M. Li et al (2021)12 if at least one weekday and one weekend day of device wear was missing from the 14-day measurement period, or if wear days had an average light intensity of ≤100 lux or entries of 0 lux for ≥60%. Bhandari et al (2022)73 considered days with ≥8 hours of data during wake time as valid, and required at least three valid weekdays and one valid weekend day (one week measurement period) for including the participant. S.-M. Li et al (2022)37 did not include measurements with fixed illumination values, assuming non-wear of the device. Finally, in their reanalyses, Landis et al (2018)34 eliminated days with device removal of >90%, and Read et al (2018)16 only included weekend data from children who had participated during school vacation in Dharani et al (2012)13 for comparability. As can be seen, there is substantial between-publication variability regarding exclusion practices.
(3) Information on the amount of in- and excluded data is given in most of the publications reporting respective procedures, and is presented in Table 2.
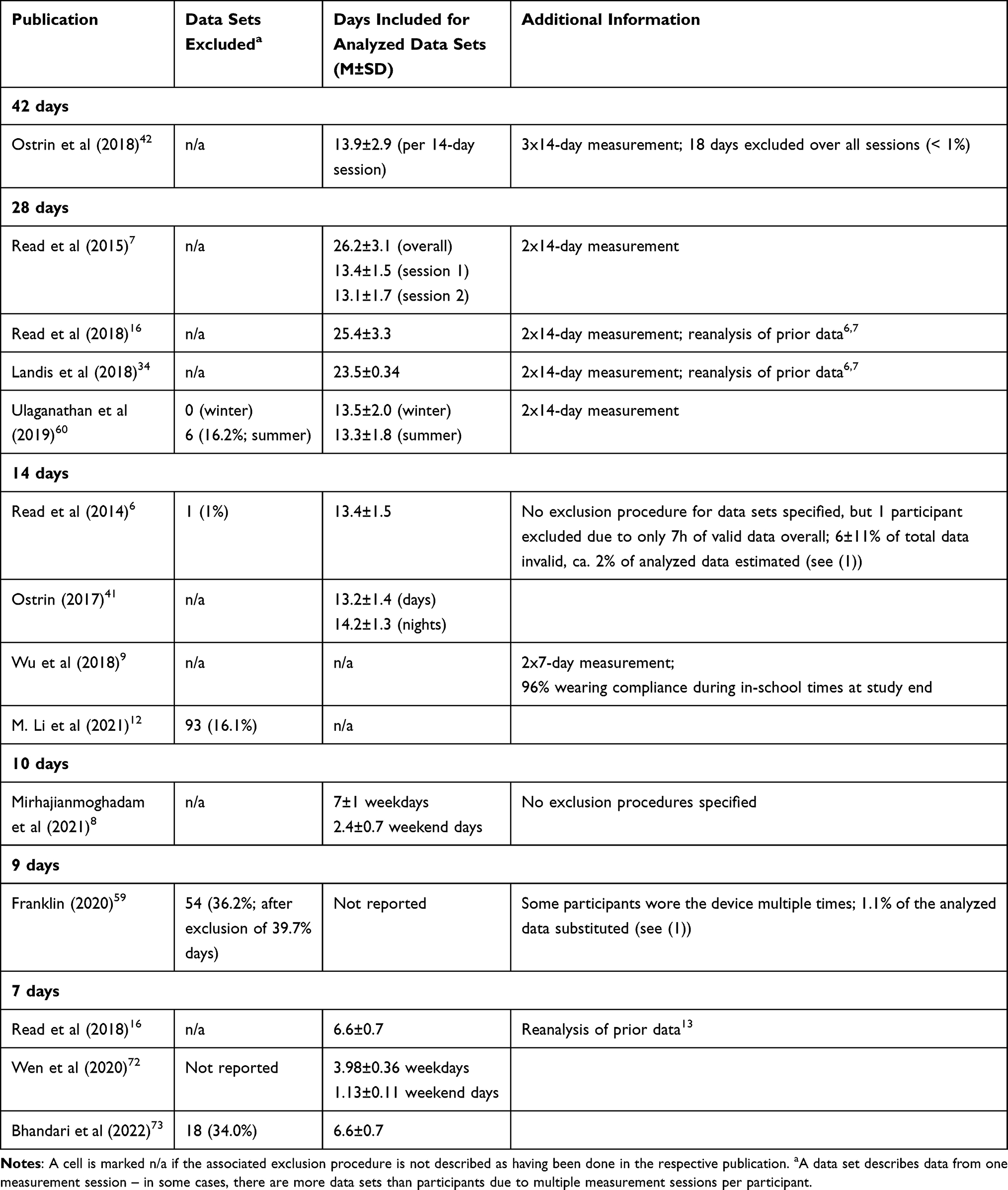 |
Table 2 Amount of Data in- and Excluded via the Publications’ Exclusion Criteria Described in (2) |
While for most publications, the mean days included in analysis – after potential exclusion of complete data sets – are at maximum one day fewer than the measurement period, there is some between-publication variation in the amount and proportion of included days. With regard to the exclusion of complete data sets, a varying percentage was excluded in the publications. Apart from aspects like participant age, devices or circumstances of data acquisition which may influence compliance and data quality, the varying in- and exclusion procedures are a potential factor underlying these differences. For example, in the publications where a criterion to exclude complete data sets had been applied, the percentage of excluded data sets is generally rather high (16.1–36.4%), while no such procedure had been applied in many other publications – in most of which it was indeed apparent from the data that no complete data sets were excluded. In general, given the various applied data in- and exclusion procedures, the apparent variation between publications with regard to the amount of excluded data is not surprising, though comparisons are inherently difficult due to the various approaches.
Discussion
We identified ten wearable light meters from studies on light exposure and myopia in humans, and included 20 publications in our analysis of research methods, two of which were reanalyses. The devices show large differences, for example in how they are worn, or their lux measurement range and spectral sensitivity. In the following, aspects related to the devices, as well as publications and research methods will be discussed and put into context. For the considerations mainly related to light meter characteristics, the devices will be grouped based on how they are usually worn. We will conclude by presenting a list of aspects that, in our opinion, should be considered when investigating LMA.
Light Meter Characteristics – Devices Attached Over Clothing
The HOBO Temp/Light data logger is generally worn over clothing, eg, attached with a pin, and was used in the earliest publications. Its spectral sensitivity strongly deviates from the photopic luminous efficiency function, with the manufacturer stating that the light sensor measures a much wider wavelength spectrum than is humanly visible.50 Importantly, most other devices’ light sensors also do not exactly fit the photopic luminous efficiency function, albeit they seem to deviate less strongly. Wearing the HOBO Temp/Light data logger may be more laborious compared to other light meters, and as it is usually worn forward-facing on clothing, it may easily be covered, eg, with a jacket. Also, the device can probably be worn during fewer activities than some other devices. For example, it is impractical to wear at night – though this is presumably not a large problem when investigating bright light – and even though it is waterproof, showering or swimming with it would be difficult due to its usual ways of wearing. Comparable considerations also apply to MyLyt, which, however, was not used in any of the publications included in the analysis of research methods. Aspects like these might have played a role in the four earliest publications not finding LMA – though the two most recent publications with the HOBO Temp/Light data logger did find LMA, both including a large number of participants.9,37 Furthermore, in both publications, teachers9 or teachers and parents37 were instructed to monitor device wear, and Wu et al (2018)9 only analyzed in-school times regarding objective light exposure. In general, there are some challenges regarding the wearability of devices attached over clothing, and for the HOBO Pendant Temp/Light data logger, one may also want to consider the spectral sensitivity function strongly deviating from the photopic luminous efficiency function.
Light Meter Characteristics – Devices Worn on Spectacles
Clouclip and Vivior Monitor are spectacle-worn and thus measure eye-level light intensity – on the other hand, their way of wearing as well as the fact that neither one is waterproof restrict potential activities. No publication with Vivior Monitor is included in the analysis of research methods, but interestingly, all three publications based on Clouclip data report LMA.71–73 Measuring of eye-level light intensity may thereby play a role, as light entering the eye is probably more relevant for myopia (development) than general ambient illumination. Another potential limitation of spectacle-worn devices is that myopic and non-myopic participants are subject to different alterations during data acquisition, since the former mostly do and the latter do not wear spectacles in real life. Indeed, in a study with fifth-graders wearing Clouclip, myopic participants reached the required wearing time more often than emmetropic participants.70 The authors discuss optimizing the device’s wearability, eg, by constructing it as an earphone.70 Something comparable has, for example, been implemented in the Daysimeter, a device designed to measure circadian light exposures: The photosensors of the Daysimeter-S are positioned at the plane of the cornea, but no spectacles are necessary for wearing.15 Overall, the possibility of measuring eye-level light intensity provided by spectacle-worn devices may be especially relevant when investigating LMA, while other aspects of these devices pose important challenges for field research.
Light Meter Characteristics – Devices Worn at Wrist
Wrist-worn devices, if waterproof, can be worn at almost all times. We identified six wrist-worn devices, five of them labelled waterproof per IPX7 (the Actiwatches) or IP68 (Sony Smartwatch 3 used for FitSight). Yet, Franklin (2020)59 found the Actiwatch 2 seals prone to leaking in 40°C water and thereafter advised participants not to shower, bath, or swim with the device, remarking that the water resistance recommendation is based on a cold water test.59 Wrist-worn devices may be covered by clothing, and how problematic this might be likely depends on circumstances like the weather. Light exposure at wrist has been shown to substantially deviate from that at eye-level – more strongly than light exposure measured at chest or at the collar.15,21 Thus, wrist-worn devices do not seem to measure eye-level light intensity, while measurements near the chest appear to match the latter more closely.85 Systematic variations have even been found, eg, wrist measurements tending to overestimate eye-level light exposure in indoor conditions and to underestimate it in outdoor conditions.85 All these aspects may influence light measurements, and confound comparisons between measurements with devices worn at different body locations. Thus, while the easy wearability and (in most cases) water resistance of wrist-worn devices post clear advantages for field studies, aspects like accidentally covering them or their measurements deviating from that of devices positioned closer to the eyes are potential challenges when measuring light exposure.
Time of Publication
The earliest publication included in the analysis of research methods stems from 2011,78 so this field of research is relatively young. Noticeably, the four oldest included publications do not support LMA.13,36,76,78 One may speculate whether aspects such as the lack of established procedures or experience regarding compliance enhancement or exclusion of data play a role. For example, as compared to most other publications, no or only few data pre-processing was conducted. However, said publications also share other criteria like the light meter, and no conclusion regarding LMA can be drawn based on time of publication alone.
Type of Study
The finding of longitudinal, but not cross-sectional, studies using light meters reporting associations between higher light exposure and slower eye growth86 is not reflected in our analysis, as results supporting LMA have been reported in both types of investigations. The fact that LMA have been found cross-sectionally may suggest that a person’s bright light exposure is somewhat stable over time – and may have played a role in whether or not myopia had developed earlier in their life. On the other hand, these cross-sectional results could also be explained by myopic participants being more likely to spend time indoors than emmetropic participants.
Sampling Interval and Measurement Duration
A sampling interval of ≤2 minutes22,36 and a measurement duration of ≥ one week22 have been proposed to ensure reliable (outdoor) light measurements. These settings should be considered when planning measurements, as, eg, Ulaganathan et al (2017)22 note that differences in these aspects may be one factor underlying between-study differences in findings regarding personal ambient light exposure – though since the recommendations are fulfilled in most publications included here, it is unsurprising that no pattern regarding results on LMA was apparent.
Geographic Location
Data on objectively measured light exposure with regard to myopia is missing for most parts of the world as the publications originate from only six countries. Interestingly, some LMA in school-aged children were discovered in all five East Asian,9,37,71,72,80 but not13 or only minimally12 in both Singaporean publications, despite the high myopia prevalence in school children in both regions.87 Here, one may consider the overall time spent in bright light. For example, Read et al (2014)6 speculate that Dharani et al (2012)13 may not have found a difference in time outdoors between myopic and emmetropic participants because some of the latter were already on their way to becoming myopic due to low overall light exposure. They also note the consistency of this with the high myopia prevalence in Singapore.6 In the Singaporean publications,12,13 overall mean light levels and time in ≥1000 lux were reduced compared to the one East Asian publication with this information available (for more than in-school times).72 As participants in the latter were on average older than in the Singaporean publications, one would rather expect a reverse pattern. Even though this is speculative and based on few data, it is worth to keep an eye on. Also, data from other parts of the world is needed for a more comprehensive picture of LMA.
Season
Due to the relationship between myopia development and season,88–90 the latter may potentially influence the measurement of LMA. Yet, seasons were not only very diverse between publications – data acquisition was also often not controlled in this respect, and only three publications investigated season with regard to LMA, yielding mixed results. It would be advisable to control and investigate season more thoroughly in research on LMA, a first step being to always specify the time and season of data acquisition. Also, one should control season with regard to participant groups, for example by matching participants from different groups to simultaneously wear the light meter as Read et al (2014)6 did. Importantly, season and geographic location are of course intertwined.
Participant Sample Size and Characteristics
There is large between-publication variability in sample size and participant age. Publications with a larger sample tended to support LMA more often than others. Age-wise, there were only four publications on adults and 14 on children – with one and nine of them supporting LMA, respectively. Due to the low number of publications with adult data, comparing adult and child publications regarding the proportion of publications (not) reporting LMA is not that informative. As axial myopia usually appears during childhood and youth,24 it does make sense that the focus lies primarily on these ages. Furthermore, with the large age (range) variance between publications with children, it is not surprising that no pattern emerged regarding age and results on LMA. However, age should be investigated further with respect to potential protective effects of light exposure: Since myopia development does not happen in the same way across all of childhood,24 more knowledge on relevant ages for the influence of light exposure may improve the development of preventive measures. With respect to sample characteristics, homogeneity regarding relevant behaviors may also be of interest. For example, Burfield et al (2019)63 speculate that due to similar schedules, their sample of emmetropic and myopic young adult university members may have been too homogeneous in light exposure and sleep-wake patterns to uncover associations – in this case, primarily regarding light exposure and diurnal rhythms. Of the four included publications investigating adults, three had a university student sample36,60,76 and one had a sample with unspecified occupations – but with a mean age of 37 years (range: 21–64), participants were probably not (exclusively) students.41 While this point is indeed interesting, four publications are not sufficient to analyze whether such homogeneity in adult participants may play a role in the results. However, it should be kept in mind, especially since lack of diversity in samples can be a large problem for analyzing, interpreting and generalizing results, as is well known in psychological research.91 In any case, while there is no clear picture as of yet, potential associations between participant age and LMA may become clearer with more data in the future, and aspects such as sample homogeneity in relevant characteristics should be considered.
General Time Spent in Bright Light Levels
The overall time participants in a sample spent in bright light has been suggested to affect LMA by concealing them due to an overall low exposure,6,23 or by the protective effect of light exposure on myopia reaching a ceiling effect in case of overall high exposure.25 We discovered large between-publication variability in “outdoor light” (>1000 lux) and average light levels. Importantly, it is difficult to determine how much of this is based on variability in actual light exposure versus on measurement differences, eg, due to device specifications or ways of wearing – though findings such as Clouclip having been used in both the publication with the least73 and the most reported >1000 lux exposure72 suggest that the device is not the only factor responsible for such variability. More research is warranted to detangle these aspects – also including between-publication differences in analyzed times and whether different devices are comparable regarding the measurement of time in >1000 lux – and assess the implications of a population’s overall (bright) light exposure.
Assessment of Refractive Status as Well as Classification and Proportion of Myopic Participants
Some between-publication variability was also discovered regarding the assessment of refractive status, and the classification and proportion of myopic participants. While in most publications, direct measures of refraction were used to assess refractive status, some applied indirect measures. For an SER-based myopia classification, the common −0.50 D SER cut-off was mostly used, and the underlying refractive status measurements were either non-cycloplegic subjective refraction, cycloplegic autorefraction or, in one case, unspecified. The percentage of myopic participants ranges from 4.4%59 to 85.2%36 between publications. Notably, of the three publications with the lowest9,59,80 and highest proportion of myopic participants,36,41,76 only those with a very large sample size strongly support LMA.9,80 However, whether this observation is meaningful cannot be determined with the few included publications. In any case, it is important to consider that measurement, definition and distribution of participant characteristics may influence analyses and results.
IO-Cut-off
One extremely relevant aspect when assessing light and outdoor exposure is the IO-cut-off. In all but one76 of the 15 publications using an IO-cut-off, it was set at 1000 lux. Own pre-measurements to determine said IO-cut-off were only mentioned in three publications.9,36,76 And although 1000 lux is widely accepted as IO-cut-off even beyond this specific research field, it is indeed questionable if it is always appropriate for the given circumstances. In fact, other IO-cut-offs have been applied before, eg, 800 lux with Clouclip92 or 200 lux with the Actiwatch Spectrum.93 Two aspects in particular are important, namely (1) whether 1000 lux is an accurate cut-off to distinguish indoors from outdoors, and (2) how comparable measurements of 1000 lux are between different light meters. Regarding (1), one study, eg, reported measurements of >1000 lux not only outdoors, but also indoors near a window even with a calibrated photometer.19 Although perfectly distinguishing indoors from outdoors via any one solely lux-based IO-cut-off is most likely impossible, such findings do call into question whether 1000 lux is in fact the ideal IO-cut-off in any given situation to classify environments as accurately as possible. For example, as lighting conditions are darker in winter than in summer, different IO-cut-offs may be useful in different seasons – with the same IO-cut-off, time outdoors may be overestimated in summer and underestimated in winter. Regarding (2), it has, eg, been found that despite a generally high correlation between lux measurements of Clouclip, Actiwatch 2 and a photometer, the lux values corresponding to 1000 lux as measured with the photometer were 533.15 lux for Actiwatch 2 and 850 lux for Clouclip.19 Importantly, these values represent the devices’ lux measurement best matching the photometer-measured 1000 lux and not their best IO-cut-off – but the finding does underline the notion that different devices’ lux measurements cannot necessarily be compared to one another. This is also represented in the fact that the Actiwatch 2 underestimates lux compared to a photometer, while the opposite is true for the Actiwatch Spectrum.15,19,94 Furthermore, our own research (Hönekopp & Weigelt, unpublished data) suggests that even when worn at exactly the same time, some light meters are better at correctly recognizing indoor than outdoor time and vice versa with the 1000 lux IO-cut-off. Furthermore, other IO-cut-offs, which varied between devices, were more accurate. These findings also suggest that (1) 1000 lux is not always an accurate IO-cut-off and (2) 1000 lux measurements are not necessarily comparable between devices. 1000 lux not always accurately separating indoor and outdoor locations may partly explain the often poor correlation between objective and subjective outdoor time estimations.32 In fact, other IO-cut-offs have sometimes been found to better correspond to subjective measures.20,33 What needs consideration here is if one actually aims to assess time spent outdoors vs indoors with this IO-cut-off, or if one rather wants to investigate time spent in brighter vs less bright light intensities, roughly resembling “outdoor-like” and “indoor-like” light levels, not being particularly interested in the environment participants were actually in. The former may, eg, be the case if one is (also) interested in influences other than higher light intensity that outdoor environments may have on myopia development.19 For example, different chromatic spectra of indoor and outdoor light may play a role, as the spectral composition of light has been found relevant with regard to emmetropization, ocular growth and myopia development in animal models.3,95
In the latter case, ie, if one primarily wishes to distinguish time spent in brighter vs less bright light intensities, (1) is less relevant – but it would still be problematic to compare data from different devices if 1000 lux measurements were not comparable between them as described in (2). If one actually wants to best distinguish indoors from outdoors, one could consider including other measurements. For example, Vivior Monitor can additionally measure UV exposure, which could be used instead of or together with lux data. The latter is described for the Akeso eye care glasses,83 and Ye et al (2019)51 used lux, UV and step data measured by Mumu in their model for indoor-outdoor discrimination. Generally, more methodological assessments are needed with regard to implications of the IO-cut-off, and it is advisable to consider and test which IO-cut-off is best for an investigation’s circumstances.
Analyzed Times for as Well as Exclusion and Replacement of Light Data
We detected large variability between publications regarding analyzed times of light exposure and other data exclusion and replacement procedures – this is especially relevant for comparing results of different publications. Usefulness and feasibility of potential procedures thereby depend on various factors like when the device can be worn, circumstances of data acquisition, or outcome measures. Thus, while unification of procedures would certainly be beneficial in some regards, it would presumably be difficult to achieve. Yet, it is important to at least thoroughly report procedures as well as rates of data exclusion and replacement, and to consider them when assessing or planning investigations. For the sake of comparability and consideration of the overall picture, it might also be useful to always report certain values (eg, mean lux during waking hours or between sunrise and sunset), which can then be compared between publications, even if the specific study focuses on other values.
Selected Relevant Aspects in the Study of Light-Myopia Associations
We will conclude with a list of aspects which we believe are relevant to the study of LMA with wearable light meters. Importantly, this list should not be considered exhaustive.
- Choose the light meter to suit the circumstances of data acquisition (eg, regarding battery life, water resistance, body position, wearability), thereby also considering whether any device specifications – or not knowing them – are problematic.
- Report the geographic location of data acquisition for comparability reasons. Furthermore, it would be desirable if investigations on LMA were conducted in more parts of the world than they are now.
- Likewise, report the season of data acquisition, and ideally consider it in study design and analysis because of its potential influence on LMA.
- Thoroughly report potentially relevant details of the participant sample, especially those that the international community might not be aware of (eg, school entry age), and keep in mind that sample homogeneity in relevant aspects might be problematic.
- Thoroughly report the assessment of refractive status as well as the classification of refractive error groups.
- Choose the IO-cut-off based on the circumstances of data acquisition (eg, device, weather) and what is to be achieved with it (eg, actual outdoor- and indoor-time vs “indoor-like” and “outdoor-like” lighting environments, comparison with other investigations). Ideally, conduct pre-measurements for its determination and explain your choice(s).
- Consider which times to include in the analyses of light data, and which pre-processing procedures to apply (eg, any data exclusion and/or replacement), and thoroughly report the procedures.
- In this context, also report the amount of excluded and replaced data.
Limitations
Naturally, this review is subject to limitations as we were not able to cover all interesting aspects with regard to the investigation of LMA – for example, the differentiation between autorefractor measurement methods (for the models used in each publication, see Supplementary Table 3), other visual assessments than that of refractive status and/or myopia classification, statistical procedures to assess LMA or to pre-process data like logarithmic transformation,85 or the variability in measurements of the same light meter type (for device calibration and additional lux measurements reported in each publication, see Supplementary Table 3).94
As per the dedicated focus of the review, we only investigated publications regarding white light exposure (lux). Aspects like the spectral composition of light were not considered, but – as pointed out earlier – are in fact very interesting regarding the protective effect of time outdoors on myopia,3,95 and some light meters can and have been used to measure the spectral composition of light.62,67
Conclusion
Various light meters have been used to assess the relationship between myopia and light/outdoor exposure. These differ in various technical specifications – not all of which are publicly available – and in aspects like wearability or how they are worn. We reviewed the literature on LMA with regard to general characteristics, data acquisition, participant population, as well as data analysis and interpretation of the publications, discussing several aspects that warrant critical consideration, for example the common use of the 1000 lux IO-cut-off. We found very high between-publication variability for many methodological aspects, and extremely limited for others. This makes it conceivable that some of these methodological aspects may contribute to between-publication variety in the results. The between-publication variability in methodological aspects often being very high or barely present may also impede the ability to find patterns between these aspects and results on the association between myopia and light exposure. The considered aspects were usually described thoroughly within the publications. Sometimes, information was missing, which would have been important to comprehensively assess and compare the respective publications. Missing information also occurred with regard to relevant light meter specifications like their spectral sensitivity, and in some cases, it was not possible for us to obtain them even after contacting manufacturers and/or authors.
In general, we demonstrate the wide variability between devices used for research on myopia and light exposure and discuss the implications thereof. We additionally identify and discuss relevant methodological aspects of the publications, highlighting areas where more research is needed and outlining factors that should be considered when planning similar investigations.
Acknowledgments
We acknowledge financial support by Deutsche Forschungsgemeinschaft and Technische Universität Dortmund/TU Dortmund Technical University within the funding program Open Access Publishing.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Holden BA, Fricke TR, Wilson DA, et al. Global prevalence of myopia and high myopia and temporal trends from 2000 through 2050. Ophthalmology. 2016;123(5):1036–1042. doi:10.1016/j.ophtha.2016.01.006
2. Karthikeyan SK, Ashwini DL, Priyanka M, Nayak A, Biswas S. Physical activity, time spent outdoors, and near work in relation to myopia prevalence, incidence, and progression: an overview of systematic reviews and meta-analyses. Indian J Ophthalmol. 2022;70(3):728–739. doi:10.4103/ijo.IJO_1564_21
3. Muralidharan AR, Lança C, Biswas S, et al. Light and myopia: from epidemiological studies to neurobiological mechanisms. Ther Adv Ophthalmol. 2021;13:25158414211059246. doi:10.1177/25158414211059246
4. Karouta C, Ashby RS. Correlation between light levels and the development of deprivation myopia. Invest Ophthalmol Vis Sci. 2014;56(1):299–309. doi:10.1167/iovs.14-15499
5. Biswas S, Muralidharan AR, Betzler BK, et al. A duration-dependent interaction between high-intensity light and unrestricted vision in the drive for myopia control. Invest Ophthalmol Vis Sci. 2023;64(3):31. doi:10.1167/iovs.64.3.31
6. Read SA, Collins MJ, Vincent SJ. Light exposure and physical activity in myopic and emmetropic children. Optom Vis Sci. 2014;91(3):330–341. doi:10.1097/OPX.0000000000000160
7. Read SA, Collins MJ, Vincent SJ. Light exposure and eye growth in childhood. Invest Ophthalmol Vis Sci. 2015;56(11):6779–6787. doi:10.1167/iovs.14-15978
8. Mirhajianmoghadam H, Piña A, Ostrin LA. Objective and subjective behavioral measures in myopic and non-myopic children during the COVID-19 pandemic. Trans Vis Sci Technol. 2021;10(11):4. doi:10.1167/tvst.10.11.4
9. Wu P-C, Chen C-T, Lin K-K, et al. Myopia prevention and outdoor light intensity in a school-based cluster randomized trial. Ophthalmology. 2018;125(8):1239–1250. doi:10.1016/j.ophtha.2017.12.011
10. He M, Xiang F, Zeng Y, et al. Effect of time spent outdoors at school on the development of myopia among children in China: a randomized clinical trial. JAMA. 2015;314(11):1142–1148. doi:10.1001/jama.2015.10803
11. Wu P-C, Tsai C-L, Wu H-L, Yang Y-H, Kuo H-K. Outdoor activity during class recess reduces myopia onset and progression in school children. Ophthalmology. 2013;120(5):1080–1085. doi:10.1016/j.ophtha.2012.11.009
12. Li M, Lanca C, Tan C-S, et al. Association of time outdoors and patterns of light exposure with myopia in children. Br J Ophthalmol Epub. 2021;107:133.
13. Dharani R, Lee C-F, Theng ZX, et al. Comparison of measurements of time outdoors and light levels as risk factors for myopia in young Singapore children. Eye. 2012;26(7):911–918. doi:10.1038/eye.2012.49
14. Morgan IG, P-C W, Ostrin LA, et al. IMI risk factors for myopia. Invest Ophthalmol Vis Sci. 2021;62(5):3. doi:10.1167/iovs.62.5.3
15. Figueiro MG, Hamner R, Bierman A, Rea MS. Comparisons of three practical field devices used to measure personal light exposures and activity levels. Light Res Technol. 2013;45(4):421–434. doi:10.1177/1477153512450453
16. Read SA, Vincent SJ, Tan C-S, Ngo C, Collins MJ, Saw S-M. Patterns of daily outdoor light exposure in Australian and Singaporean children. Trans Vis Sci Technol. 2018;7(3):8. doi:10.1167/tvst.7.3.8
17. Bhandari KR, Mirhajianmoghadam H, Ostrin LA. Wearable sensors for measurement of viewing behavior, light exposure, and sleep. Sensors. 2021;21(21):7096. doi:10.3390/s21217096
18. Joyce DS, Zele AJ, Feigl B, Adhikari P. The accuracy of artificial and natural light measurements by actigraphs. J Sleep Res. 2020;29(5):e12963. doi:10.1111/jsr.12963
19. Howell CM, McCullough SJ, Doyle L, Murphy MH, Saunders KJ. Reliability and validity of the Actiwatch and Clouclip for measuring illumination in real-world conditions. Ophthalmic Physiol Opt. 2021;41(5):1048–1059. doi:10.1111/opo.12860
20. Wen L, Cheng Q, Cao Y, et al. The Clouclip, a wearable device for measuring near-work and outdoor time: validation and comparison of objective measures with questionnaire estimates. Acta Ophthalmol. 2021;99(7):e1222–e1235. doi:10.1111/aos.14785
21. Aarts MP, van Duijnhoven J, Aries MB, Rosemann AL. Performance of personally worn dosimeters to study non-image forming effects of light: assessment methods. Build Environ. 2017;117:60–72. doi:10.1016/j.buildenv.2017.03.002
22. Ulaganathan S, Read SA, Collins MJ, Vincent SJ. Measurement duration and frequency impact objective light exposure measures. Optom Vis Sci. 2017;94(5):588–597. doi:10.1097/OPX.0000000000001041
23. Flanagan SC, Cobice D, Richardson P, Sittlington JJ, Saunders KJ. Elevated melatonin levels found in young myopic adults are not attributable to a shift in circadian phase. Invest Ophthalmol Vis. 2020;61(8):45. doi:10.1167/iovs.61.8.45
24. Morgan I, Rose K. How genetic is school myopia? Prog Retin Eye Res. 2005;24(1):1–38. doi:10.1016/j.preteyeres.2004.06.004
25. Gordon-Shaag A, Shneor E, Doron R, Levine J, Ostrin LA. Environmental and behavioral factors with refractive error in Israeli boys. Optom Vis Sci. 2021;98(8):959–970. doi:10.1097/OPX.0000000000001755
26. Grzybowski A, Kanclerz P, Tsubota K, Lanca C, Saw S-M. A review on the epidemiology of myopia in school children worldwide. BMC Ophthalmol. 2020;20(1):27. doi:10.1186/s12886-019-1220-0
27. Rudnicka AR, Kapetanakis VV, Wathern AK, et al. Global variations and time trends in the prevalence of childhood myopia, a systematic review and quantitative meta-analysis: implications for aetiology and early prevention. Br J Ophthalmol. 2016;100(7):882–890. doi:10.1136/bjophthalmol-2015-307724
28. Hashemi H, Khabazkhoob M, Asharlous A, et al. Cycloplegic autorefraction versus subjective refraction: the Tehran Eye Study. Br J Ophthalmol. 2016;100(8):1122–1127. doi:10.1136/bjophthalmol-2015-307871
29. Esaki Y, Kitajima T, Obayashi K, Saeki K, Fujita K, Iwata N. Daytime light exposure in daily life and depressive symptoms in bipolar disorder: a cross-sectional analysis in the APPLE cohort. J Psychiatr Res. 2019;116:151–156. doi:10.1016/j.jpsychires.2019.06.010
30. Scheuermaier K, Laffan AM, Duffy JF. Light exposure patterns in healthy older and young adults. J Biol Rhythms. 2010;25(2):113–122. doi:10.1177/0748730410361916
31. Liu L, Marler MR, Parker BA, et al. The relationship between fatigue and light exposure during chemotherapy. Support Care Cancer. 2005;13(12):1010–1017. doi:10.1007/s00520-005-0824-5
32. Mahroo OA, Gavin EA, Williams KM, de SE, Hammond CJ, Morrison DA. Potential effect of ‘cut-off intensity’ on correlation between light meter measurements and time outdoors. Eye (Lond). 2013;27(8):990–991. doi:10.1038/eye.2013.88
33. Dharani R, Lee C-F, Finkelstein EA, Saw S-M. Response to Mahroo et al. Eye (Lond). 2013;27(8):991. doi:10.1038/eye.2013.89
34. Landis EG, Yang V, Brown DM, Pardue MT, Read SA. Dim light exposure and myopia in children. Invest Ophthalmol Vis Sci. 2018;59(12):4804–4811. doi:10.1167/iovs.18-24415
35. Alvarez AA. Light, Nearwork, and Visual Environment Risk Factors in Myopia. Berkeley: University of California; 2012.
36. Alvarez AA, Wildsoet CF. Quantifying light exposure patterns in young adult students. J Mod Opt. 2013;60(14):1200–1208. doi:10.1080/09500340.2013.845700
37. Li S-M, Ran A-R, Kang M-T, et al. Effect of text messaging parents of school-aged children on outdoor time to control myopia: a randomized clinical trial. JAMA Pediatr. 2022;176(11):1077–1083. doi:10.1001/jamapediatrics.2022.3542
38. Ohno Y, Goodman T, Blattner P, et al. Principles governing photometry (2nd edition). Metrologia. 2020;57(2):20401. doi:10.1088/1681-7575/ab72f1
39. Koninklijke Philips N.V.. Actiwatch 2 - Activity Monitor; n.d. Available from: https://www.usa.philips.com/healthcare/product/HC1044809/actiwatch-2-activity-monitor.
40. Koninklijke Philips N.V. Actiwatch Specification Sheet; 2019.
41. Ostrin LA. Objectively measured light exposure in emmetropic and myopic adults. Optom Vis Sci. 2017;94(2):229–238. doi:10.1097/OPX.0000000000001013
42. Ostrin LA, Sajjadi A, Benoit JS. Objectively measured light exposure during school and summer in children. Optom Vis Sci. 2018;95(4):332–342. doi:10.1097/OPX.0000000000001208
43. Koninklijke Philips N.V.. Actiwatch Spectrum - Activity Monitor; n.d. Available from: https://www.usa.philips.com/healthcare/product/HC1046964/actiwatch-spectrum-activity-monitor.
44. Koninklijke Philips N.V. Characterization of Light Sensor Performance for Three Models of Actiwatch: Actiwatch-64, Actiwatch 2 and Actiwatch Spectrum; 2008.
45. Udovičić L, Janßen M, Nowack D, Price LLA Personenbezogene Lichtexpositionsmessungen in Feldstudien - Eine Handlungsanleitung zur Charakterisierung und Kalibrierung von Lichtexpositionsdetektoren [Light exposure measurements in field studies - A guide to action for the characterization and calibration of light exposure detectors]; 2016. German.
46. Koninklijke Philips N.V. Actiwatch Spectrum Plus - Get the Actiwatch advantage; n.d. Available from: https://www.usa.philips.com/healthcare/product/HCNOCTN445/actiwatch-spectrum-plus-get-The-actiwatch-advantage.
47. Koninklijke Philips N.V. Actiwatch Spectrum PRO: get the Actiwatch Advantage; n.d. Available from: https://www.usa.philips.com/healthcare/product/HCNOCTN446/actiwatch-spectrum-pro-get-The-actiwatch-advantage.
48. Verkicharla PK, Ramamurthy D, Nguyen QD, et al. Development of the FitSight fitness tracker to increase time outdoors to prevent myopia. Trans Vis Sci Technol. 2017;6(3):20. doi:10.1167/tvst.6.3.20
49. Sony Mobile Communications Inc. User Guide: SmartWatch 3 SWR50; 2014.
50. Onset Computer Corporation. HOBO® Pendant Temperature/Light Data Logger (Part # UA-002-XX); Doc # 9556-I, MAN-UA-002; 2012.
51. Ye B, Liu K, Cao S, et al. Discrimination of indoor versus outdoor environmental state with machine learning algorithms in myopia observational studies. J Transl Med. 2019;17(1):314. doi:10.1186/s12967-019-2057-2
52. Silicon Labs. Si1132: UV Index And Ambient Light Sensor IC With I2C Interface; 2014. Rev 1.2.
53. Dhakal R, Rudrapankte JR, Chittajallu HSNS, et al. Development and validation of a ‘MyLyt’ wearable light tracking device. Ophthalmic Physiol Opt. 2023;43(1):132–140. doi:10.1111/opo.13061
54. Vivior AG. Vivior Mark 3+: Technical Information; n.d.
55. Ostrin LA, Abbott KS, Queener HM. Attenuation of short wavelengths alters sleep and the ipRGC pupil response. Ophthalmic Physiol Opt. 2017;37(4):440–450. doi:10.1111/opo.12385
56. Ostrin LA, Read SA, Vincent SJ, Collins MJ. Sleep in myopic and non-myopic children. Trans Vis Sci Technol. 2020;9(9):22. doi:10.1167/tvst.9.9.22
57. Read SA, Pieterse EC, Alonso-Caneiro D, et al. Daily morning light therapy is associated with an increase in choroidal thickness in healthy young adults. Sci Rep. 2018;8(1):8200. doi:10.1038/s41598-018-26635-7
58. Ulaganathan S, Read SA, Collins MJ, Vincent SJ. Daily axial length and choroidal thickness variations in young adults: associations with light exposure and longitudinal axial length and choroid changes. Exp Eye Res. 2019;189:107850. doi:10.1016/j.exer.2019.107850
59. Franklin KJ The effects of environment and lifestyle on eye growth. Birmingham: Aston University; 2020.
60. Ulaganathan S, Read SA, Collins MJ, Vincent SJ. Influence of seasons upon personal light exposure and longitudinal axial length changes in young adults. Acta Ophthalmol. 2019;97(2):e256–e265. doi:10.1111/aos.13904
61. Williams R, Bakshi S, Ostrin EJ, Ostrin LA. Continuous objective assessment of near work. Sci Rep. 2019;9(1):6901. doi:10.1038/s41598-019-43408-y
62. Abbott KS, Queener HM, Ostrin LA. The ipRGC-driven pupil response with light exposure, refractive error, and sleep. Optom Vis Sci. 2018;95(4):323–331. doi:10.1097/OPX.0000000000001198
63. Burfield HJ, Carkeet A, Ostrin LA. Ocular and systemic diurnal rhythms in emmetropic and myopic adults. Invest Ophthalmol Vis Sci. 2019;60(6):2237–2247. doi:10.1167/iovs.19-26711
64. Ostrin LA. The ipRGC-driven pupil response with light exposure and refractive error in children. Ophthalm Physiol Opt. 2018;38(5):503–515. doi:10.1111/opo.12583
65. Ostrin LA, Jnawali A, Carkeet A, Patel NB. Twenty-four hour ocular and systemic diurnal rhythms in children. Ophthalm Physiol Opt. 2019;39(5):358–369. doi:10.1111/opo.12633
66. Shneor E, Doron R, Levine J, et al. Objective behavioral measures in children before, during, and after the COVID-19 lockdown in Israel. Int J Environ Res Public Health. 2021;18(16):8732. doi:10.3390/ijerph18168732
67. Harb EN, Chan M, Tran A, Wildsoet CF. Characteristics of indoor and outdoor light exposure differ with refractive status in young adults [conference abstract]. Invest Ophthalmol Vis Sci. 2016;57(12):2473.
68. Koninklijke Philips N.V. Professional sleep and activity monitoring solutions: Actiwatch monitoring systems; 2013.
69. Li L, Zhu H, Wen L, Lan W, Yang Z. An approach of combining convolution neural network and graph convolution network to predict the progression of myopia. Neural Process Lett. 2021.
70. Wen L, Cheng Q, Lan W, et al. An objective comparison of light intensity and near-visual tasks between rural and urban school children in china by a wearable device Clouclip. Trans Vis Sci Technol. 2019;8(6):15. doi:10.1167/tvst.8.6.15
71. Li L, Wen L, Lan W, Zhu H, Yang Z. A novel approach to quantify environmental risk factors of myopia: combination of wearable devices and big data science. Tran Vis Sci Technol. 2020;9(13):17. doi:10.1167/tvst.9.13.17
72. Wen L, Cao Y, Cheng Q, et al. Objectively measured near work, outdoor exposure and myopia in children. Br J Ophthalmol. 2020;104(11):1542–1547. doi:10.1136/bjophthalmol-2019-315258
73. Bhandari KR, Shukla D, Mirhajianmoghadam H, Ostrin LA. Objective measures of near viewing and light exposure in schoolchildren during COVID-19. Optom Vis Sci. 2022;99(3):241–252. doi:10.1097/OPX.0000000000001871
74. Hangzhou JinZhiJing Technology Co. Ltd. CLOUCLIP: Myopia Related Behavioral Control - Smart Device - Big Data; n.d.
75. Saw SM, Zhang X, Pu S-H, Inventors. Device to prevent a condition or disease associated with a lack of outdoor time. WO2015152818A1. October 8, 2015.
76. Schmid KL, Leyden K, Chiu Y, et al. Assessment of daily light and ultraviolet exposure in young adults. Optom Vis Sci. 2013;90(2):148–155. doi:10.1097/OPX.0b013e31827cda5b
77. Moafa MAM Quantifying Risk Factors for Myopia: Instrument Validation and Establishing Dosage for Light Intensity and Duration. Sydney: The University of Sydney; 2019.
78. Backhouse S, Ng H, Phillips J Light exposure patterns in children - a pilot study. In: Schaeffel F, Feldkaemper M, eds.
79. He X, Sankaridurg P, Xiong S, et al. Shanghai Time Outside to Reduce Myopia trial: design and baseline data. Clin Exp Ophthalmol. 2019;47(2):171–178. doi:10.1111/ceo.13391
80. He X, Sankaridurg P, Wang J, et al. Time outdoors in reducing myopia: a school-based cluster randomized trial with objective monitoring of outdoor time and light intensity. Ophthalmology. 2022;129(11):1245–1254. doi:10.1016/j.ophtha.2022.06.024
81. Tanrıverdi C, Tabakcı BN, Kılıç A, Mrochen MC Objective measurement of photopic illuminance rate in daily life of progressive myopic children.
82. Pajic B, Zakharov P, Pajic-Eggspuehler B, Cvejic Z. User friendliness of a wearable visual behavior monitor for cataract and refractive surgery. Appl Sci (Basel). 2020;10(6):2190. doi:10.3390/app10062190
83. Fan Y, Liao J, Liu S, et al. Effect of time outdoors and near-viewing time on myopia progression in 9- to 11-year-old children in Chongqing. Optom Vis Sci. 2022;99(6):489–495. doi:10.1097/OPX.0000000000001898
84. Nishanth S, Manoharan K, Srinivasan M, et al. Accurate measurement of outdoor activities in children with myopia: development of an affordable wearable device [conference abstract]. Invest Ophthalmol Vis Sci. 2022;63(7):2144–A0172.
85. Hartmeyer SL, Webler FS, Andersen M. Towards a framework for light-dosimetry studies: methodological considerations. Light Res Technol. 2022;147715352211032.
86. Lingham G, Mackey DA, Lucas R, Yazar S. How does spending time outdoors protect against myopia? A review. Br J Ophthalmol. 2020;104(5):593–599. doi:10.1136/bjophthalmol-2019-314675
87. Ding B-Y, Shih Y-F, Lin LLK, Hsiao CK, Wang I-J. Myopia among schoolchildren in East Asia and Singapore. Surv Ophthalmol. 2017;62(5):677–697. doi:10.1016/j.survophthal.2017.03.006
88. Gwiazda J, Deng L, Manny R, Norton TT. Seasonal variations in the progression of myopia in children enrolled in the correction of myopia evaluation trial. Invest Ophthalmol Vis Sci. 2014;55(2):752–758. doi:10.1167/iovs.13-13029
89. Cui D, Trier K, Munk Ribel-Madsen S. Effect of day length on eye growth, myopia progression, and change of corneal power in myopic children. Ophthalmology. 2013;120(5):1074–1079. doi:10.1016/j.ophtha.2012.10.022
90. Donovan L, Sankaridurg P, Ho A, et al. Myopia progression in Chinese children is slower in summer than in winter. Optom Vis Sci. 2012;89(8):1196–1202. doi:10.1097/OPX.0b013e3182640996
91. Henrich J, Heine SJ, Norenzayan A. The weirdest people in the world? Behav Brain Sci. 2010;33(2–3):61–135. doi:10.1017/S0140525X0999152X
92. Wen L, Cao Y, Huang Y, et al. Diverse visual behavior patterns in students in the same classroom [conference abstract]. Invest Ophthalmol Vis Sci. 2017;58(8):2403.
93. Refinetti R. Chronotype variability and patterns of light exposure of a large cohort of United States residents. Yale J Biol Med. 2019;92(2):179–186.
94. Markvart J, Hansen ÅM, Christoffersen J. Comparison and correction of the light sensor output from 48 wearable light exposure devices by using a side-by-side field calibration method. LEUKOS. 2015;11(3):155–171. doi:10.1080/15502724.2015.1020948
95. French AN, Ashby RS, Morgan IG, Rose KA. Time outdoors and the prevention of myopia. Exp Eye Res. 2013;114:58–68. doi:10.1016/j.exer.2013.04.018
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.