Back to Journals » Advances in Medical Education and Practice » Volume 14
Using a Smartphone Application as a Tool for English Learning Among Medical Staff and Students in Japan
Authors Iwata Y ![]() , Iwata Y, Iida H, Inamori M, Maeda S
, Iwata Y, Iida H, Inamori M, Maeda S
Received 24 October 2022
Accepted for publication 17 February 2023
Published 28 February 2023 Volume 2023:14 Pages 167—182
DOI https://doi.org/10.2147/AMEP.S394625
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Md Anwarul Azim Majumder
Yuri Iwata,1 Yumiko Iwata,2 Hiroshi Iida,1 Masahiko Inamori,1 Shin Maeda3
1Department of Medical Education, Yokohama City University, Yokohama, Japan; 2Department of English Language, Communication and Cultures, University of the Sacred Heart, Tokyo, Japan; 3Department of Gastroenterology, Yokohama City University, Yokohama, Japan
Correspondence: Yuri Iwata, Department of Medical Education, Yokohama City University, School of Medicine, 3-9 Fukuura, Kanazawa-ku, Yokohama, Kanagawa, 236-0004, Japan, Tel +81-45-787-2626, Fax +81-45-787-2620, Email [email protected]
Aim: To report on the effects of a smartphone application, among the medical staff and medical students, for learning English as a foreign language.
Methods: We conducted an exploratory quasi-experimental study among eight medical staff and 10 medical students in Japan. The participants used an application called ABC Talking (created by ABC Talking Laboratories Inc, currently unavailable due to application renewal), loaded onto their smartphones, to talk with native English speakers from overseas. The participants used the application for five minutes twice a day over five consecutive days as per their convenience. The study collected quantitative and qualitative data using assessments on the participants’ listening and speaking skills and questionnaire. The assessment scores of the first five sessions were compared to those of the last five. Average self-assessment scores and teacher assessment scores were compared using a t-test. A paired t-test was performed on quantitative data of the questionnaire, and content analysis was performed on qualitative data.
Results: More than 80% of the calls were made from home and 70% occurred between 9PM and 1AM. The participants’ self-assessment scores on their listening and speaking skills increased significantly from the first five sessions to the last five sessions (14.8– 26.1%). However, there was no significant change in the assessments by the teachers (− 4.5– 2.1%). The self-assessment scores of those with low English proficiency were lower than the teachers’ assessment scores. Improvement of communicative self-confidence and communicative competence, two factors that affect willingness to communicate, were seen from the questionnaire.
Conclusion: Using smartphone applications allows on-demand English training, which may be especially useful to medical staff and students who have unpredictable work schedules. Teachers should be aware that learners tend to assess themselves lower than their actual ability so that they can give appropriate feedback to the learners.
Keywords: limited English proficiency, communication, medical training, professional competence, language barrier
Introduction
English Education in Japan
According to the 2022 results of the Education First’s English Proficiency index, Japan is classified as a country of low English proficiency, ranking in eightieth out of 111 countries and regions.1 In order to improve the English skills of students, the English educational system in Japan has been under constant refinement. For example, the national syllabus for English was revised to place emphasis on developing oral communication skills. However, many Japanese grad students still cannot speak English even after having studied English for ten years from high school to university.2 This is partly due to the English requirements of the university entrance examinations. Students who plan on advancing to universities tend to focus on grammar and memorize vocabulary in English, not really for authentic usage, but for entrance examinations.3 All medical universities have an English language section as part of their entrance examination, but none of them tests the speaking skills. As a result, students tend to have little conversational practice.
Despite having enough English knowledge to pass the competitive medical university entrance examinations, it is often said that the English ability of medical students peak at matriculation and declines thereafter. Although many medical universities teach English to some extent for one to two years, the English education curriculum is yet to be standardized.4 No two medical schools have the same program. Course objectives, material, topics, and teaching methods depend on the teacher. Even within a single year in a single medical school, the materials taught to students in different classes may differ.
It has been reported that many medical staff and students feel that the English education at their universities have failed in improving their English communication skills.5 They lack confidence and feel uncomfortable in using English in unscripted situations.6 The general emphasis on grammatical accuracy over oral fluency throughout English education, and the tendency for Japanese medical staff and students to be perfectionists, leads to their fear of making mistakes in public.
The Needs and Challenges of Learning English in the Medical Field
As a result of globalization, there is an increasing need for proficiency in English, especially communication skills, in medical staff. For a long time, English was not essential for clinical practice in Japan because the national health insurance system in Japan demanded that all medical terms in the chart to be written in Japanese.7 English was primarily used to access or share the latest knowledge in medicine, as international journals and conferences mainly use English as the common universal language. However, with the increasing number of foreign visitors and residents, there is more demand for the use of English in clinical practice nowadays. Furthermore, many of the English-speaking patients are not native English speakers and so sufficient skills to manage general English is required as well as medical English.6
Although both medical staff and students are aware of the need to improve their English communication skills, it is not easy for them to find time and opportunity to do so. According to Ishikawa, who reported the outcomes of medical English conversation classes held at a hospital, there were three factors that led to the decrease in the number of attendees: irregular work shifts, poor motivation, and an insufficient level of English needed for medical English communication.8 Medical staff often have irregular work shifts and may have to work overnight. Even after leaving the hospital, some may need to respond to emergency calls. Setting time aside and motivating themselves to learn English outside their studies or work, is not easy.
Problems Related to Willingness to Communicate and Communicative Competence Among Japanese Medical Staff and Students
In order to improve English communication skills of medical staff and students in Japan, it is essential to investigate their willingness to communicate. Willingness to communicate, a concept in applied linguistics, is defined as the intention to speak or to remain silent, given free choice.9 There are various factors that enhance willingness to communicate. Assessing these factors will give us a better understanding of why learners do or do not engage in second language communication (Figure 1).10 State of communicative self-confidence, which is low among medical staff and students, directly affects willingness to communicate, and consequently the use of English.
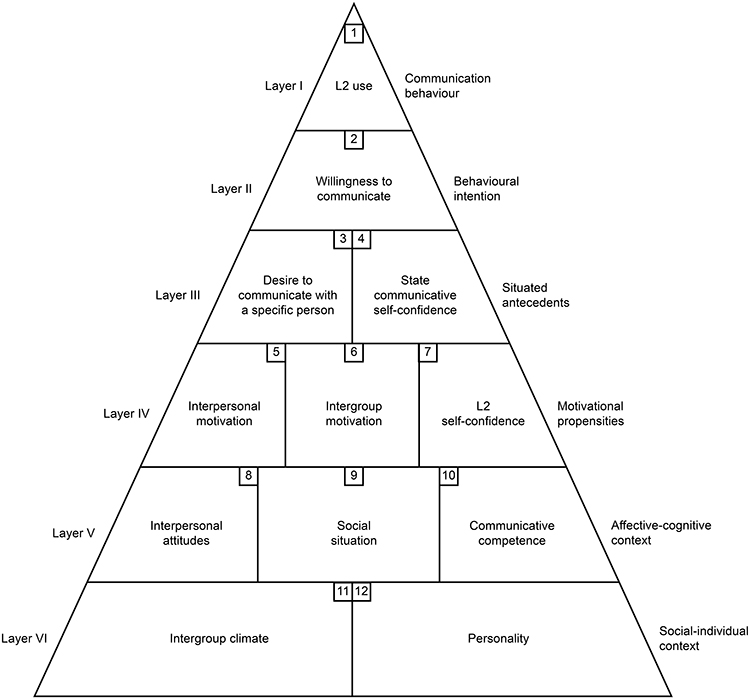 |
Figure 1 Heuristic model of variables influencing willingness to communicate. (Reproduced from The Modern Language Journal with permission from John Wiley & Sons, Inc). |
Among the factors that influence communicative self-confidence, the lack of communicative competence in Japanese learners is frequently mentioned.2,11,12 Communicative competence, another concept in applied linguistics, is the ability to control the knowledge of a language in actual communication. Learners need to develop communicative competence in order to communicate successfully. Among the subcomponents of communicative competence, grammatical competence (ability to use sounds, grammar, and words correctly) is emphasized throughout English education in Japan. Lack of conversational practice means that learners do not experience the necessity of sociolinguistic competence (ability to use the language in a socially and culturally appropriate manner), discourse competence (ability to connect sentences logically one after the other) and strategic competence (ability to come up with strategies to compensate for breakdowns in communication).
Furthermore, due to the Japanese culture where silence is considered a virtue, many feel uneasy in situations where they must speak to strangers. Willingness to communicate remains a challenge, even in the native language.3
To summarize, willingness to communicate is the key to fostering English communication skills. In order to enhance willingness to communicate among medical staff and students, communicative self-confidence is required. Among the various factors that build communicative self-confidence, Japanese learners need to work especially on their communicative competence through conversational practice.
Learning English Online: Computers versus Smartphones
Computer-mediated online videoconferencing is one of the popular methods in learning English communication skills. Communication software such as Skype create a comfortable, spontaneous, and less threatening environment for second language learners to interact with native speakers.13 Studies using Skype have suggested that it could increase confidence in English communication, develop oral communicative competence and intercultural awareness.14–18 These Skype based studies used computers but nowadays, many smartphone functions mimic computer functions.19 Currently, over 95% of Japan’s population in the 20–39 age group own a smartphone. Half of them spend two to four hours a day on their smartphones.20 Screen size and costs, which used to be the barriers to learning through smartphones, are becoming less of a problem. So, smartphones may be effective tools in young learners of English.
Most of the previous studies on language learning through smartphones focused on receptive language skills (listening and reading) rather than productive language skills (speaking and writing).21–24 Due to the lack of studies on smartphone-mediated conversation practice despite the rising need for English communication skills among medical staff and students, the present study set out to investigate the effects of a smartphone application for learning English as a foreign language.
Materials and Methods
This is an exploratory quasi-experimental study and is based on the TREND Statement. The two research questions addressed in this study are: 1) What are the effects of a smartphone application on medical staff and students in learning English as a foreign language? 2) What are the strengths and weaknesses of smartphone applications in learning English communication skills? To answer these questions, two methods were used to collect data: assessments of the participants’ listening and speaking skills and questionnaire. t-tests were performed on quantitative data of the assessments and questionnaire. Content analysis was performed on qualitative data of the questionnaire.
Participants and Recruitment
As this is an exploratory study, the number of participants was based on the number of credited accounts arranged for the study. The participants were recruited via open recruitment at Yokohama City University or by invitation. Medical staff and students who owned a smartphone with access to Wi-Fi were eligible for the study. Many medical students at Yokohama City University feel the need for English communication skills as half of the students take the opportunity to study abroad during their time at the University. The medical staff in the study were those who occasionally required English communication skills, for example when they had English speaking patients or when they attended international conferences. Their working environment varied from primary care settings to public tertiary hospitals. This study was approved by the Ethics Committee of Yokohama City University. All participants provided informed consent in writing.
The online teachers were native English speakers, mostly residents of the Philippines, selected by the provider of the application, ABC Talking Laboratories Inc. They were not English teachers per se, and possessed other jobs, such as nursing. This meant that the teachers did not necessarily have a teacher’s license, but they were all specifically recruited and interviewed online for an hour to see if they were native speakers fit to teach through this application. The interviewer focused on the interviewee’s character, the quality of their English-speaking skills, their ability to use smartphones and their access to Wi-Fi. All teachers were orientated on the aim of the application, how to use the application, how to evaluate students and give feedback.
Intervention
When we investigated services that provided online English conversation lessons to Japanese learners, the average lesson duration was 25 minutes. Most of them were Skype based videoconferences. Among these services, a smartphone application called “ABC Talking” (currently unavailable due to application renewal) was selected for this study. This application was chosen for its three distinct features. First, as far as we could find, it was the only service in Japan that provides five-minute lessons. The application was designed to provide an opportunity for users to engage in brief but frequent chats. Second, the application did not require appointments. This allowed the medical staff and students to practice English whenever they find time, whether at home, school, or work. Third, the application used voice-based communication and does not have a camera function. The participants engaged in a normal audio call, either with the smartphone pressed to one ear or using a headset. In a face-to-face or video-based communication, second language learners can resort to a wide range of paralinguistic cues such as body language and gestures to get their points across.25 However, in a voice-based communication, learners must convey their thoughts only through speaking. Additionally, as some studies have noted, to be thrust into a live conversation with a stranger can be awkward. In a study using Skype videoconferencing, students felt the need to look their best before the sessions began.18 Thus, the aim of the application was to lower the hurdles of English conversation by promoting short, frequent chats and by not including a camera function. These features were expected to allow medical staff and students to engage in English conversation within their unpredictable work or study schedules. They also would not need to worry about others overhearing them which may reduce their fear of making mistakes in public.
The participants installed the application on their smartphones. This application allowed them to converse with native English speakers living abroad. The participants were given credited accounts, as each call cost JPY 250 (Japanese yen) on an average. The participants of the study used the application to call twice a day over five consecutive days. They simply logged in and looked for an available online teacher. A participant could start the study any day as long as the five days included a weekend; thus, some started on a weekend, and some ended on a weekend.
The teachers of the application were orientated to let users raise conversation topics and to suggest some topics if the users were unable to do so. Having no set topic of conversation could be an advantage as well as a disadvantage. Giving learners the opportunity to raise conversation topics allow them to choose and prepare topics that they are comfortable talking about. Furthermore, selecting appropriate topics of conversation in certain situations will enhance their communicative competence. However, beginners with low willingness to communicate may find this challenging. Another disadvantage of this application is that the users must keep themselves motivated. Making appointments for future lessons motivates users to continue language learning. As this application does not require prior appointments, the users are responsible for finding a time and place during their day to make the calls and continue to do so.
Data Collecting Strategies
Two sets of data were collected: assessment and questionnaire (Figure 2). From the first group, which consisted of 6 participants, only assessment data were collected. From the second group, which consisted of 12 different participants, data from assessment and questionnaire were collected.
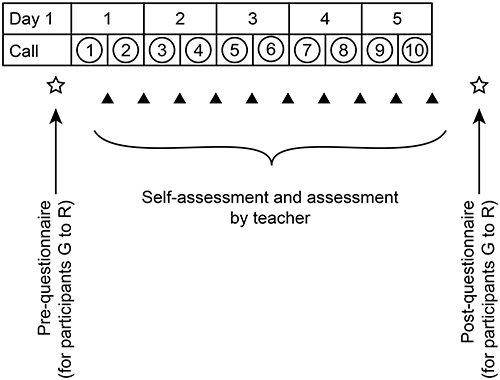 |
Figure 2 Study schedule. |
In the assessments, the participants self-rated their listening and speaking skills after each call. The assessment was on a scale of 1–5, with 1 representing “very poor” and 5 representing “very good”. The online teachers assessed them the same way.
The questionnaire was requested to the second group to allow further analysis (Figure 3). The questionnaire in the study was based on the questionnaire used in Mita’s study, which was originally created by Kobayakawa.16,17 Kobayakawa created the questionnaire to see the change in learners’ views on their English skills and on learning English. Out of the previous studies of Skype based computer-mediated language learning in Japan, only Mita and Kobayakawa used the same questionnaire. Since the aim of the questionnaire was similar to the current study, and because it was the only questionnaire that was used in two separate studies, this questionnaire was selected and adapted to the current study. The validity and reliability of the questionnaire are yet to be assessed.
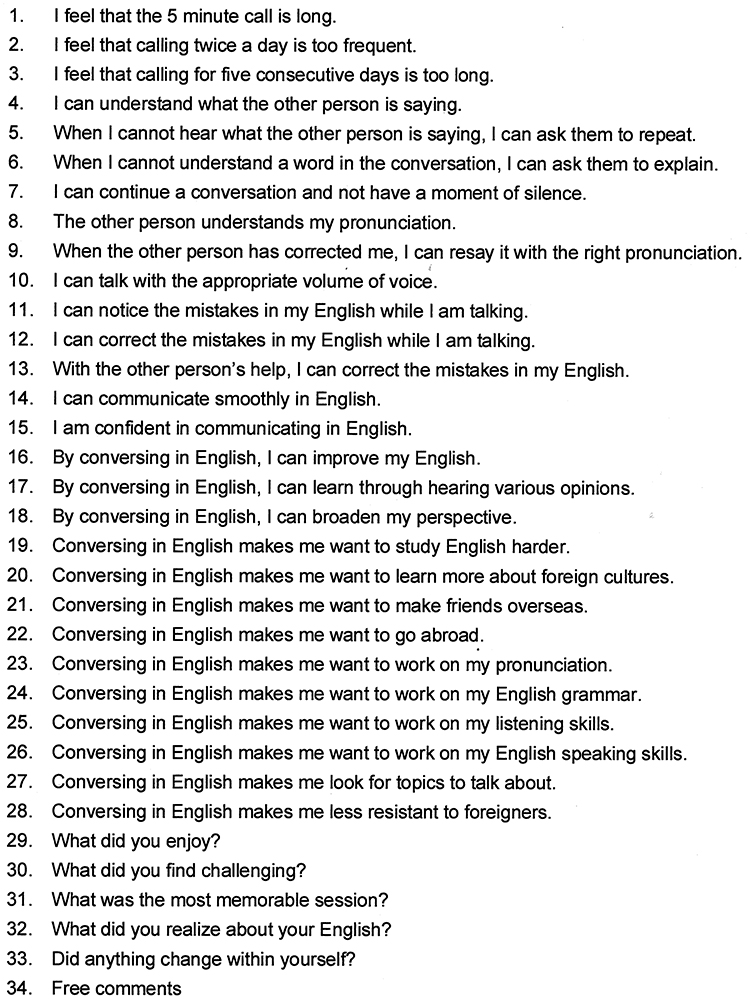 |
Figure 3 Questionnaire administered in the second group of the study. |
Questions 1 to 3 were added to Mita’s questionnaire to investigate the participants’ views on the application. Questions 4 to 15 aimed to investigate the participants’ views on their English communication skills. Questions 16 to 28 aimed to investigate the participants’ views on learning English. Questions 29 to 34 were open ended questions. The questionnaire used a seven-point Likert scale. The responses were coded 1–7, with 1 representing “strongly disagree” and 7 representing “strongly agree”.
Data Analysis and Reporting
Data were extracted from hard-copies (self-assessments and questionnaire) and web-based forms (teachers’ assessments) and integrated in Microsoft Excel software. Percentage change was used to compare the assessment scores of the first five sessions to those of the last five. Average self-assessment scores and teacher assessment scores were compared using a t-test. The statistical significance level was set at p-value < 0.05 and was considered statistically significant. A paired t-test was performed on quantitative data of the questionnaire, and content analysis was performed on qualitative data.
Results
18 participants completed the five-day session. There were 13 male and five female participants, aged 20–35. Table 1 shows the level of English proficiency of the participants in the second group (this information was requested in the questionnaire that was added in the second group). As the participants had experience with different English proficiency tests, such as the International English Language Testing System, Test of English for International Communication, Test of English as a Foreign Language and Jitsugyo Eigo Gino Kentei (EIKEN, a test of practical English proficiency done in Japan), the scores were converted and standardized to EIKEN scores for comparison. For EIKEN, grade 5 is the lowest and grade 1 is the highest.
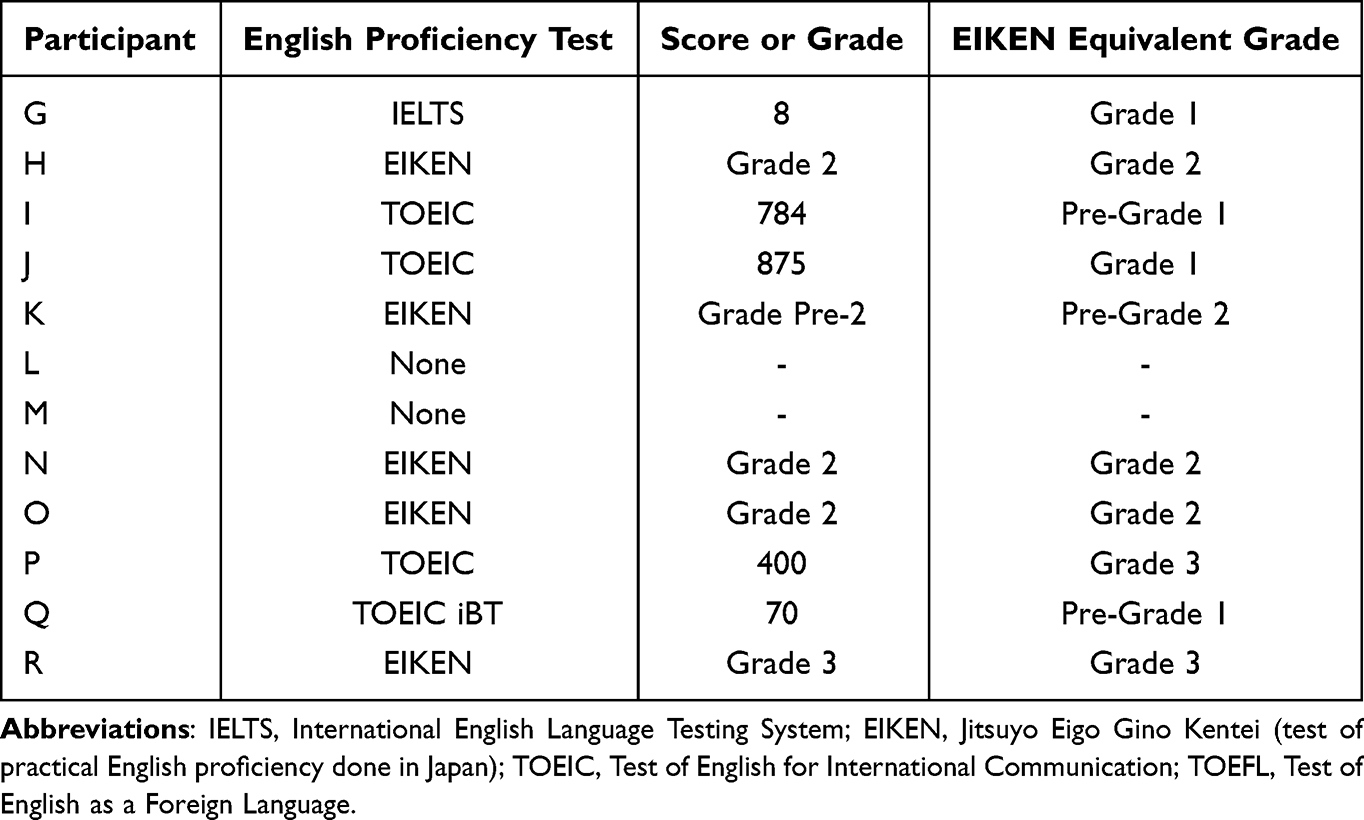 |
Table 1 English Proficiency of Participants in the Second Cycle of the Study |
Assessment After Each Session (Scale of 1–5)
The participants and online teachers assessed the participants’ listening and speaking skills after each session. When the scores of the first five sessions were compared to those of the last five, the self-assessment scores increased in all items (Figure 4). Although the participants’ self-assessment scores increased, the teachers’ assessment scores showed little change. Table 2 shows the percentage change of self-assessment and teacher’s assessment between the first five sessions and the last five sessions. For example, participant A’s self-assessment in catching words through listening increased by 10.7%. The average self-assessment percentage change increased by 14.8–26.1%, while the teacher’s assessment percentage change varied between −4.5–2.1%. This implies that although there was no objective improvement of the listening and speaking skills, the participants’ self-perceptions improved.
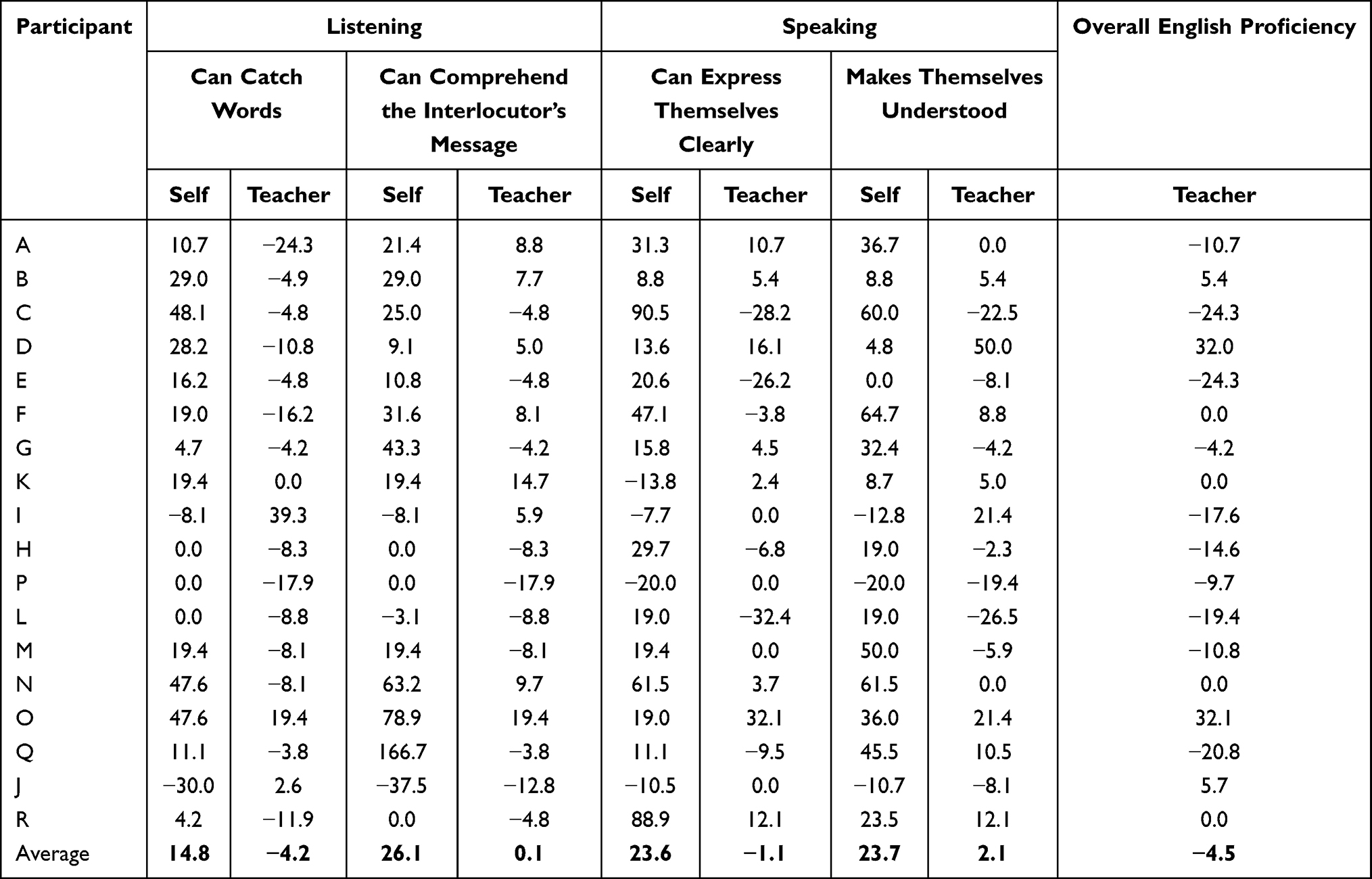 |
Table 2 Percentage Change of Self-Assessment and Teacher’s Assessment Between the First Five Sessions and the Last Five Sessions |
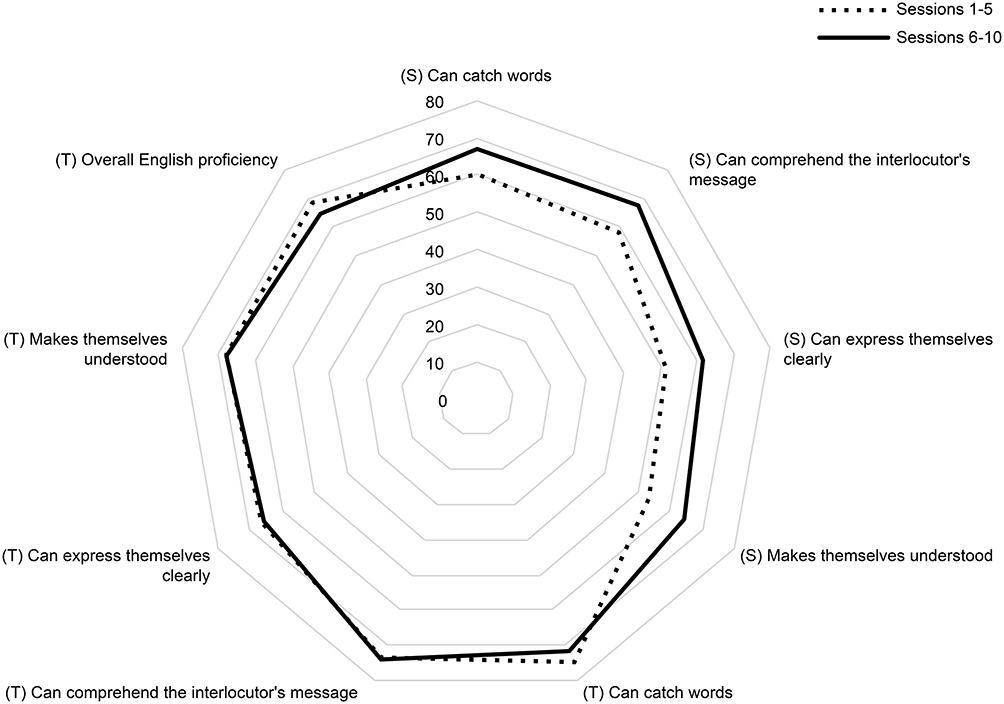 |
Figure 4 Self-assessment and teacher assessment results. |
Changes in self-assessment between the first five sessions and the last five sessions did not depend on the participants’ English proficiency levels (Table 3). Table 4 compares self and teacher assessment scores of all ten sessions. For example, participant G’s self-assessment scores were lower than the teacher assessment scores in all items. With the exception of participant I, whose self-assessment was higher than the teacher’s assessment in all items, the self-assessment scores were generally lower than the teacher’s assessment scores. A t-test was performed on these data. The statistical significance level was set at p-value < 0.05 and was considered statistically significant. The results showed that participants with lower English proficiency levels tend to evaluate themselves lower than the teachers’ evaluations.
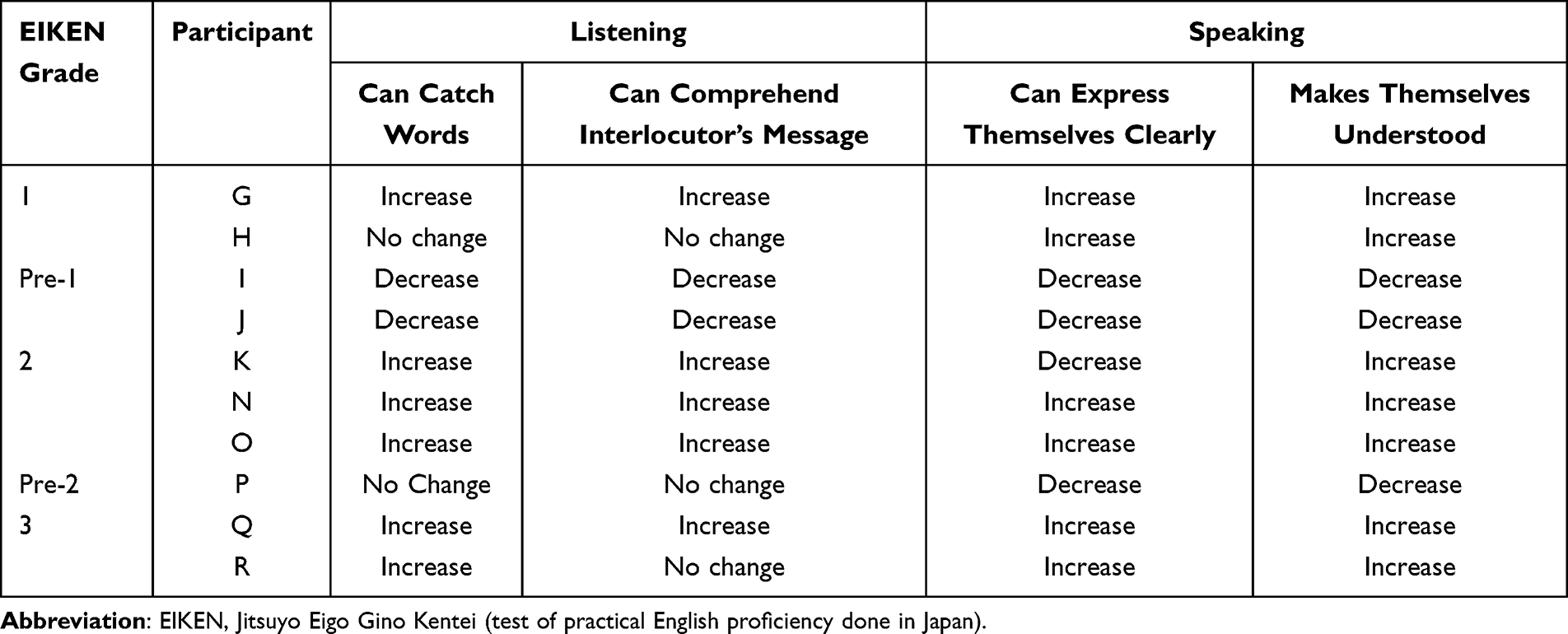 |
Table 3 How Self-Assessment from the First Five Sessions Changed in the Last Five Sessions |
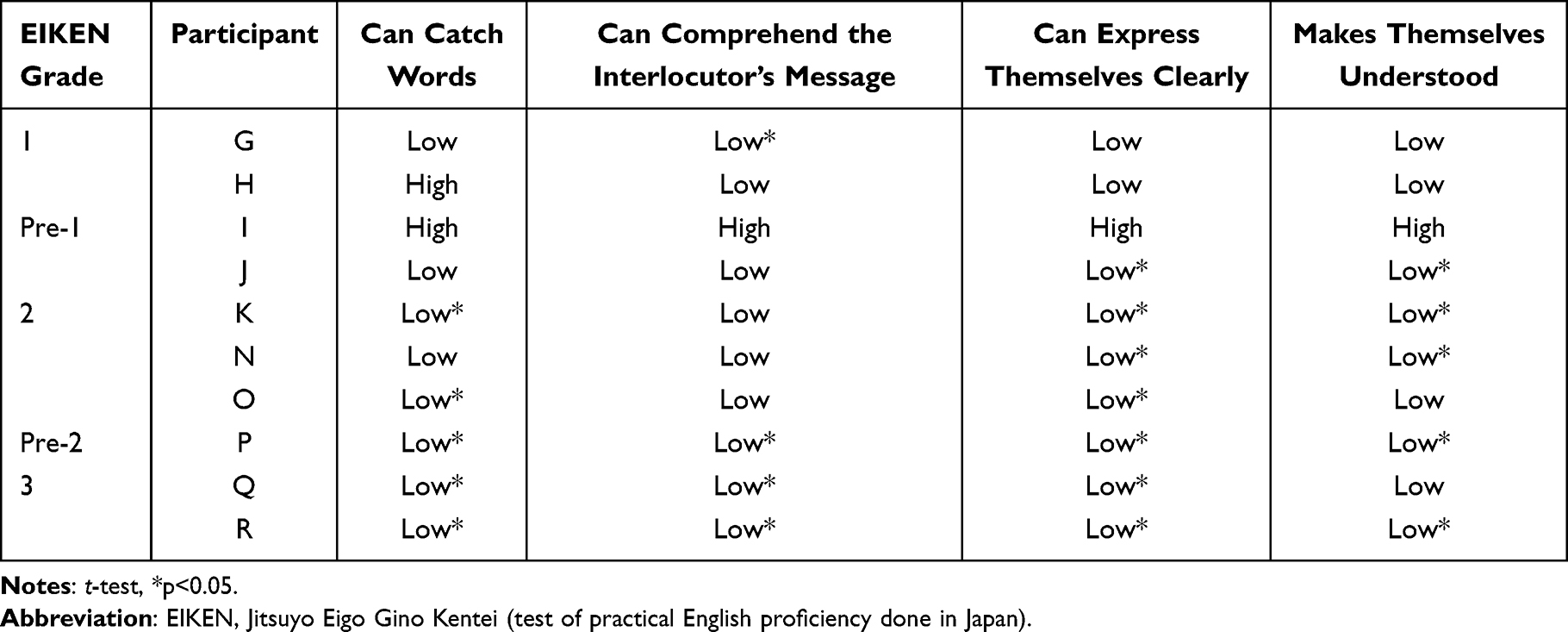 |
Table 4 Comparison of Average Self-Assessment Scores to Teacher Assessment Scores |
The Questionnaire (Seven-Point Likert Scale)
Participants’ Impression of the Application
Figures 5–7 show the participants’ impression of the application at the end of the study. Making a five-minute call twice a day was generally accepted by the participants.
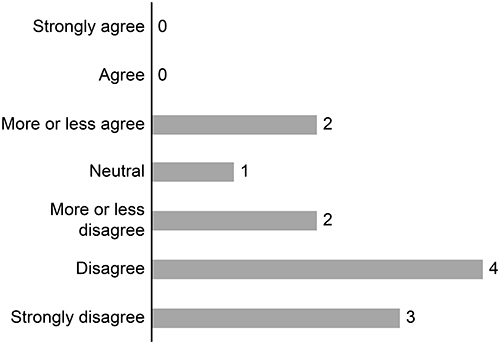 |
Figure 5 Participants’ impression of the length of each conversation (“I feel that the 5-minute call is long”). |
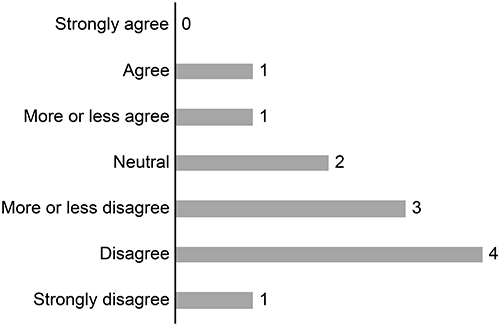 |
Figure 6 Participants’ impression of the frequency of conversations (“I feel that calling twice a day is too frequent”). |
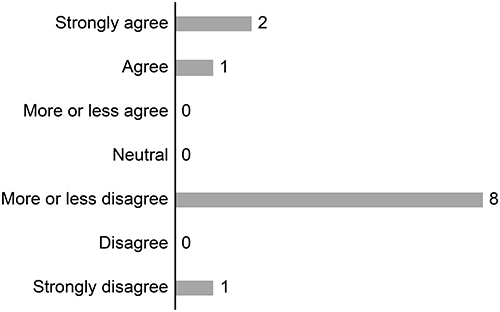 |
Figure 7 Participants’ impression of the length of the study (“I feel that calling for five consecutive days is too long”). |
Participants’ Views on Their English Skills and on Learning English
Questions 4 to 28 focused on the participants’ views on their English skills and on learning English. The results of the questionnaire done before the five-day period are available as Supplementary Figures 1 and 2, and those from after the five-day period are available as Supplementary Figures 3 and 4.
A paired t-test was performed on these data (Table 5). An increase in the average scores for question 4 and 8: “I can understand what the other person is saying”; and “the other person understands my pronunciation (p=0.026, 0.046 respectively, p<0.05) was observed. These items represent skills in listening comprehension and speaking respectively. The average score for question 6 “When I cannot understand a word in the conversation, I can ask them to explain” also increased (p=0.012, p<0.05). This represents improvement of strategic competence, one of the subcomponents of communicative competence. Increase in the average scores imply enhancement of self-confidence, an important component of willingness to communicate. There was no significant change in the participants’ views on learning English.
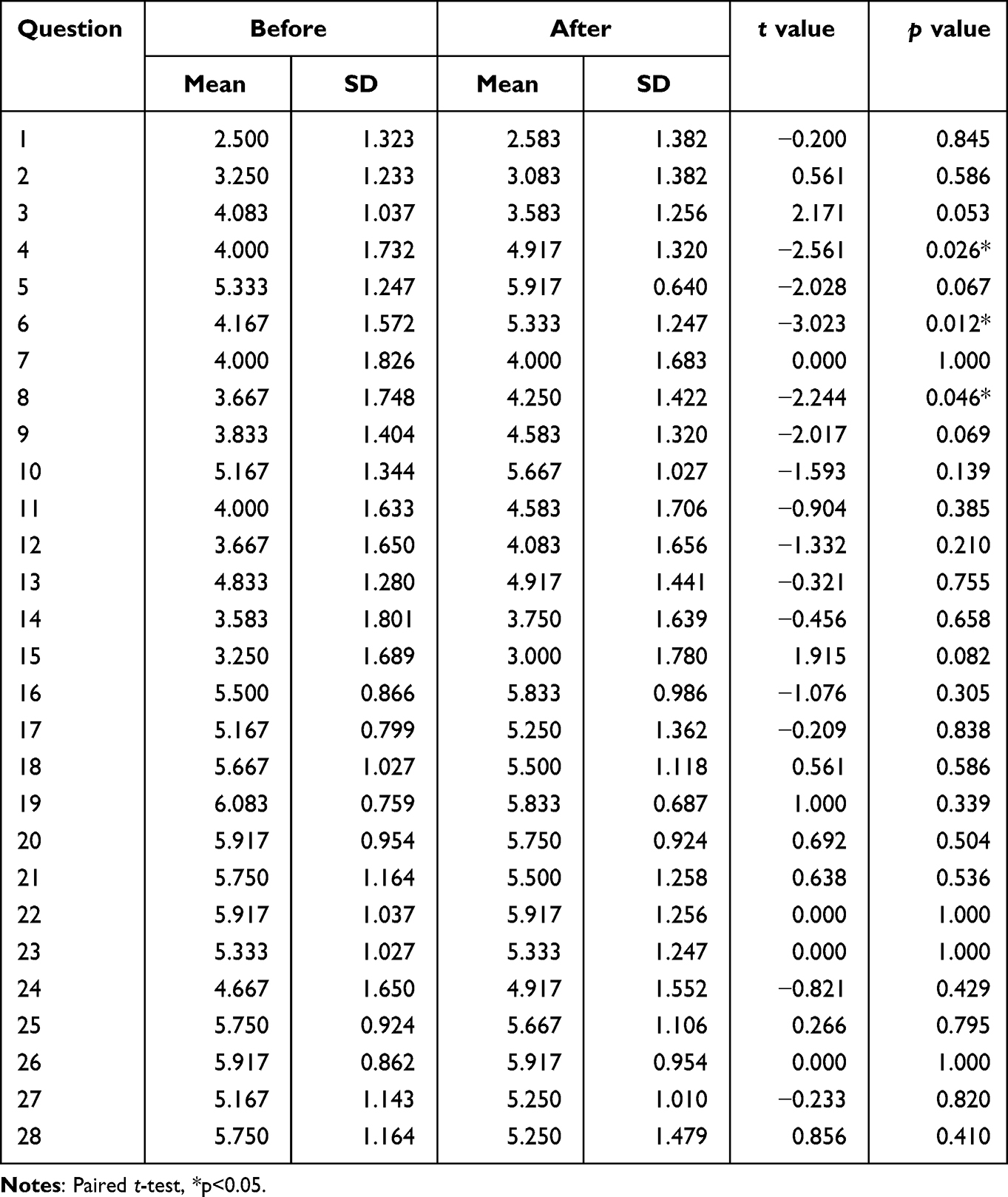 |
Table 5 Comparison of Questionnaires Done Before and After the Five-Day Period |
Responses to Open Ended Questions
When asked what they enjoyed, nine out of ten participants that responded gave examples of successful experiences such as “when I understood what the teacher said”, “when the teacher understood what I said”, and “when I succeeded in telling the second teacher what I had failed to communicate to the first teacher” (Table 6). On the other hand, when asked what they found challenging, all the participants referred to having poor English communication skills, such as “The silence. When I couldn’t say what I wanted to say”, “when I couldn’t decide what to talk about”, and “when I can’t correct myself even though I know that I am wrong”. A few also experienced unavailability of teachers or problems with Wi-Fi connection. When asked if there were any changes within themselves, six out of eight responses mentioned that their motivation to learn English was reignited. The two other responses were about enhanced sociolinguistic competence, which refers to the ability to select appropriate topics of conversation in a specific setting.
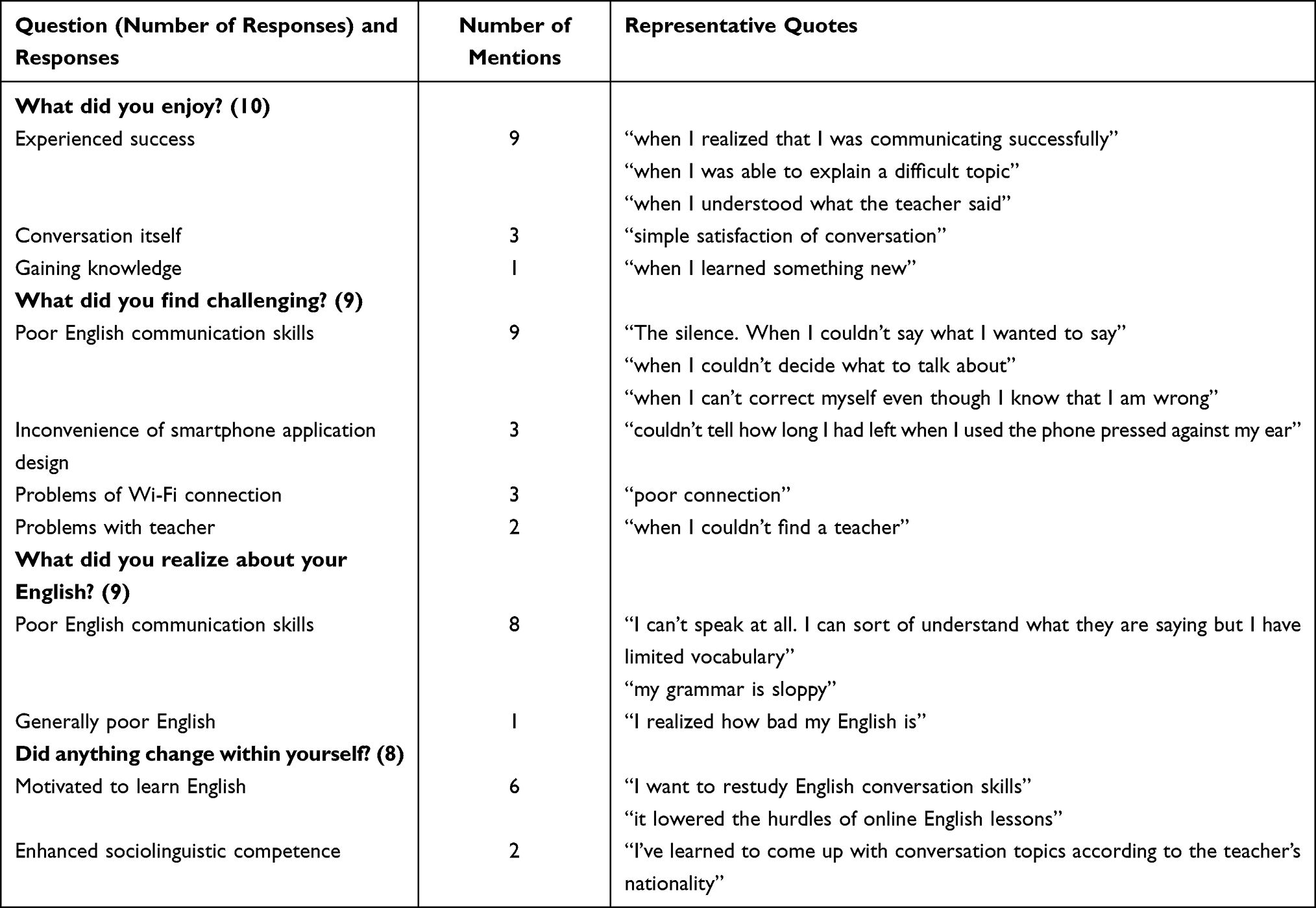 |
Table 6 Responses to Open-Ended Questions |
Time and Location of Application Usage
More than 80% of the calls were made from home and 70% occurred in the evening (Figures 8 and 9). It may be difficult for learners to find an appropriate place to engage in a phone call, especially because speaking on mobile phones in enclosed public spaces such as public transportation and cafes is considered rude in Japan. They also need a quiet (so that the learner can hear the teacher) and safe (so that the learner can focus on the call) environment. In addition, free public Wi-Fi in Japan is scarce compared to many other countries. These factors may have led to the participants’ decision to use the application in the evening when they are at home, despite having the option to use the application at any time and at any place.
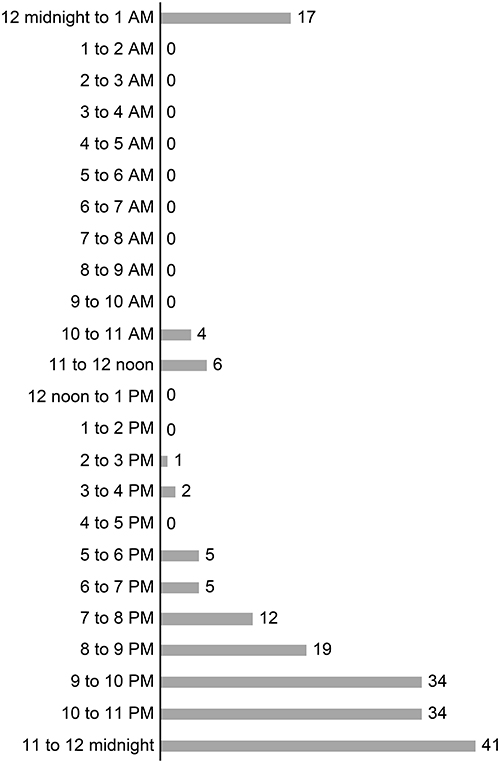 |
Figure 8 Timing of application usage (all participants, 10 calls each). |
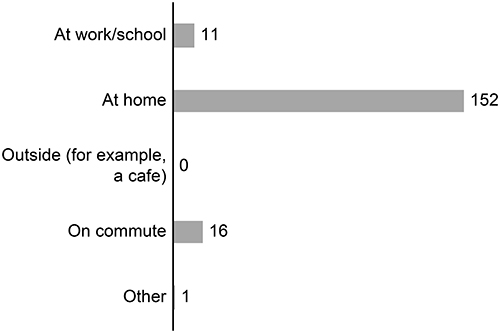 |
Figure 9 Location of application usage (all participants, 10 calls each). |
Discussion
The results of the study can be summarized as follows. First, the self-assessment and questionnaire both showed increases in “state of communicative self-confidence”. Second, the self-assessment scores improved although the teacher-assessment scores showed little changes. Third, participants with low English proficiency had low self-perception of English communication skills when compared to the teachers’ perception. Fourth, the participants used the application at home in the evening, despite the flexibility of the smartphone application. Finally, participants’ motivation to learn English was reignited.
Effects of a Smartphone Application on the Medical Staff and Students in Learning English as a Foreign Language
As there are no reports of smartphone-based studies focusing on oral communication skills, the results of the present study were compared with computer-based studies using Skype in Japan (Table 7). Kobayakawa reported an increase in confidence in English communication.17 Mita reported similarly.16 Ryobe reported that Skype was effective for improving communicative competence in spoken English and developing intercultural awareness.14,15 The current study also showed increase in communicative self-confidence. Some participants also experienced improvement of communicative competence, such as sociolinguistic competence (“I learned to come up with conversation topics according to the teacher’s nationality”) and strategic competence (“I was able to explain a difficult topic”).
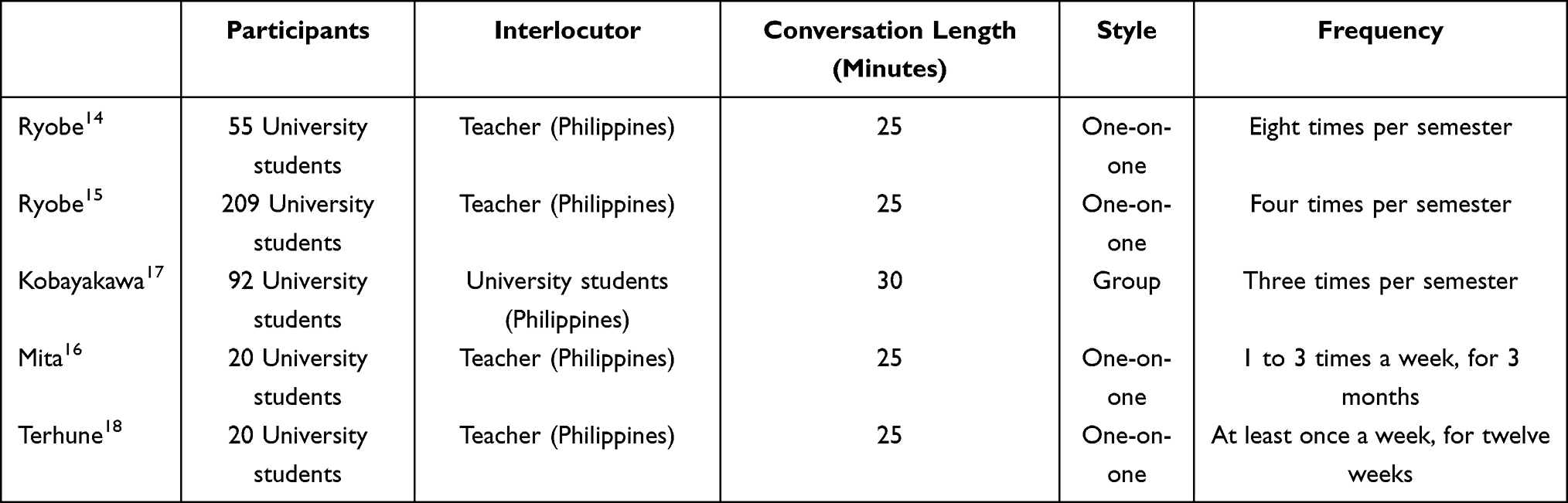 |
Table 7 Previous Studies on Foreign Language Education Using Computer-Mediated Skype Based Communication |
It should be noted that while the participants of the previous studies engaged in 25-minute conversations over a period of three to six months, the participants of the current study engaged in five-minute conversations, twice a day, over five days. Thus, our study shows that communicative self-confidence could be enhanced in several days. Although there was no measure of objective improvements of the participants’ English communication skills during the course of the study, communicative self-confidence was enhanced through the use of a smartphone application. Furthermore, communicative competence also improved and the participants were further motivated to learn English communication skills.
Strengths and Weaknesses of Smartphone Applications
The strengths of smartphone applications are their flexibility and portability. These traits allow learners to engage in short, frequent conversations. In order to improve English communication skills among medical staff and students, communicative self-confidence needs to be enhanced through conversational practice. However, setting aside blocks of time within their unpredictable work or study schedules is difficult. In the past, computer-mediated online English training required commitment, as the learner had to be in a certain place at a certain time. The application used in the current study provided on-demand English conversational practice and required only five minutes. The results showed that engaging in five-minute conversations twice a day can improve communicative self-confidence and enhance communicative competence. The first step in improving English communication skills among medical staff and students is to lower the hurdles of online English learning, so that they would take these opportunities to learn and engage in conversation. The flexibility and portability of smartphones make this possible.
Three weaknesses of smartphone applications were observed in this study. First, smartphones cannot use wired LAN and requires Wi-Fi. Previous Skype-based studies required a facility with adequate capacity and transmission speed for an entire class to use Skype, as Skype video chats involve two-way audio-video communication.15 Theoretically, the current study did not require the same capacity or transmission speed, as the application was audio-based, and because the participants used the application individually. However, the internet connection in the Philippines was unstable due to the monsoon season. Some calls were terminated (these calls were excluded), and some learners could not hear the teacher due to poor reception. This problem could occur in any smartphone application as the stability of Wi-Fi may vary depending on the environment. Second, free public Wi-Fi in Japan is not as common as other countries. This may be one of the reasons why most participants in the study did not make use of the flexibility of smartphones and used the application at home. Third, applications that provide on demand English lessons have a possibility of teachers being unavailable. Without prior appointments, it is difficult to estimate the number of teachers required. In the current study, some participants reported that they were unable to find available online teachers. Improvements in connection and providing the appropriate number of teachers may further promote the use of smartphone applications.
Study Limitations
There are various limitations associated with this study. First, this is an exploratory study consisting of a small sample with a short turnaround time. A study with a larger sample observed over a longer period is required to assess the long-term effects of the smartphone application for English communication skills training in medical staff and students. The second limitation of this study is that the participants chose to take part in the study, and thus were motivated to use the application to begin with. Whether or not less motivated learners will use smartphone applications and how they respond is yet to be studied. Third, the validity and reliability of the assessments and questionnaire are yet to be assessed. Finally, a more qualitative approach, such as interviews, may have been favorable for data collection.
Practice and Pedagogical Implications
This study shows that short daily conversations in English using a smartphone application could enhance communicative self-confidence. While other methods of conversational practice, such as computer-mediated videoconferencing or face-to-face lessons, could also enhance communicative self-confidence, these lessons take more time. The first challenge for learners is to take part in conversational practice. As smartphone applications allow medical staff and students to engage in conversation at their convenience, it should be considered as a tool to improve the English communication skills. Within the application, teachers should be aware that learners tend to assess themselves lower than their actual ability, so that they can give appropriate feedback to the learners.
Future Research
There is a plan to follow-up on the participants to see whether they have continued to learn English in any form, for example by using smartphone applications or by attending face-to-face English lessons. Further work should be done for a longer period to investigate if their motivation is maintained and if improvement in communication skills is achieved. Utilizing larger sample sizes, for example by making smartphone-mediated online English learning a part of English education at medical universities, could clarify whether smartphone applications are useful in less motivated learners. Another good recommendation would be to compare this application with other applications, or to compare smartphone and computer applications of the same service (for example, using Skype on a smartphone or a computer).
Conclusion
This study provides insights into the effects and drawbacks of using a smartphone application to improve the English communication skills of medical staff and students in Japan. The results suggested improvements in communicative self-confidence, which may lead to enhanced willingness to communicate. Participants also experienced improved communicative competence. Making a five-minute call twice a day on their smartphones to practice English conversation was generally accepted by the participants. Using a smartphone application allows on-demand English training, which may be especially useful to medical staff and students with unpredictable schedules. Teachers should be aware that learners tend to assess themselves lower than their actual ability, so that they can give appropriate feedback to the learners.
Abbreviations
EIKEN, Jitsuyo Eigo Gino Kentei (Test for Practical English Proficiency); JPY, Japanese yen.
Ethics Approval and Consent
This study was approved by the Ethics Committee of Yokohama City University (Approval number A170400004). All participants provided informed consent in writing to participate and for publication.
Consent for Publication
Consent for publication was taken and agreed to publish.
Acknowledgments
The kind offer by ABC Talking Laboratories Inc to provide free accounts for our participants to use their application made this research possible. The authors received no compensation from ABC Talking Laboratories Inc. We would like to thank Editage for English language editing.
Funding
Manuscript preparation and open access funding was provided by the basic research fund of Yokohama City University.
Disclosure
The authors declare that they have no competing interests in this work.
References
1. English First. EF English proficiency index 2022; 2022. Available from: https://www.ef.com/wwen/epi/.
2. Yamaoka K. The current situation and future prospects of Japanese English teaching. Ritsumeikan Univ Lang Cult Stud. 2010;22(1):59–66.
3. Torikai K. English Language Education in Japan: past, present and future. Lang Teach. 2000;24(7):4.
4. Barron P, Breugelmans R, Ashida R. A fundamental approach to radically improve English education in Japanese Medical Schools. Igaku Kyoiku. 2009;40(2):113–115. doi:10.11307/MEDEDJAPAN.40.113
5. Hasegawa M, Ozaki C. A Survey on Medical Students’ attitudes towards learning English language. Kawasaki Ikaishi Arts Sci. 2016;41:41–48. doi:10.11482/KMJ-LAS41)41
6. Willey I, Tanimoto K, McCrohan G, Nishiya K. An English needs analysis of medical doctors in Western Japan. JALT J. 2020;42(2):143. doi:10.37546/JALTJJ42.2-3
7. Uemura K. Medical English education in Japan: past, present & future. JMEE. 2009;8(1):7–11.
8. Miho I, Hiroki W. Medical English conversation classes for nurses and doctors at Shikoku Central Hospital. JMEE. 2018;17(3):112–116.
9. Macintyre PD. Willingness to communicate in the second language: understanding the decision to speak as a volitional process. Mod Lang J. 2007;91(4):564–576. doi:10.1111/j.1540-4781.2007.00623.x
10. MacIntyre PD, Clement R, Dornyei Z, Noels KA. Conceptualizing willingness to communicate in a L2: a situational model of L2 confidence and affiliation. Mod Lang J. 1998;82(4):545–562. doi:10.1111/j.1540-4781.1998.tb05543.x
11. Haugh S. Examining the challenges concerning communicative competence within Japan. Human Welfare. 2019;11(1):173–179.
12. Chambers G. English Education in Japan: (Re)Considering the continuous challenges in communicative competence. Bull Faculty Sociol. 2015;53(1):127–137.
13. Xiao M. An empirical study of using internet-based desktop videoconferencing in an EFL setting; 2007. Available from: https://etd.ohiolink.edu/!etd.send_file?accession=ohiou1194703859&disposition=attachment.
14. Ryobe I. The effects of skype-based video chats with volunteer Filipino English teachers (II). In:
15. Ryobe I. Using skype and moodle at the university level for supplementary oral communication practice. In:
16. Mita K. Using Skype to enhance junior college students’ oral English proficiency. Bull Jissen Women’s Junior Coll. 2014;35:19–43.
17. Kobayakawa S, Fukuda A. English education through communication with overseas university students using Skype. Studies in Improving Education through ICT (ICT利用による教育改善研究発表会); 2012:42–43. Available from: http://www.juce.jp/archives/houhou_2012/b-08.pdf.
18. Terhune NM. Language learning going global: linking teachers and learners via commercial Skype-based CMC. Comput Assist Lang Learn. 2016;29(6):1071–1089. doi:10.1080/09588221.2015.1061020
19. Chinnery GM. Going to the MALL: Mobile Assisted Language Learning. LLT. 2006;10(1):9–16.
20. Information and Communications in Japan. Ministry of internal affairs and communications; 2018. Available from: soumu.go.jp/johotsusintokei/whitepaper/eng/WP2018/2018-index.html.
21. Kukulska-Hulme A, Shield L. An overview of mobile assisted language learning: from content delivery to supported collaboration and interaction. ReCALL. 2008;20(3):271–289. doi:10.1017/S0958344008000335
22. Yang B, Zhou S, Ju W. Learning English speaking through mobile-based role-plays: the exploration of a mobile English language learning app called engage. EuroCALL Rev. 2013;21(2):38. doi:10.4995/eurocall.2013.9788
23. Duman G, Orhon G, Gedik N. Research trends in mobile assisted language learning from 2000 to 2012. ReCALL. 2014;27(2):197–216. doi:10.1017/S0958344014000287
24. Darmi R, Albion P. A review of integrating mobile phones for language learning. In:
25. Payne JS, Whitney PJ. Developing L2 oral proficiency through synchronous CMC: output, working memory, and interlanguage development. CALICO J. 2003;20(1):7–32. doi:10.1558/cj.v20i1.7-32
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.