Back to Journals » ClinicoEconomics and Outcomes Research » Volume 15
User Fee Exemption Policy Significantly Improved Adherence to Maternal Health Service Utilization in Bahir Dar City, Northwest Ethiopia: A Comparative Cross-Sectional Study
Authors Marye DM, Debalkie Atnafu D ![]() , Belayneh M
, Belayneh M ![]() , Takele Alemu A
, Takele Alemu A
Received 19 July 2023
Accepted for publication 6 December 2023
Published 11 December 2023 Volume 2023:15 Pages 775—785
DOI https://doi.org/10.2147/CEOR.S431488
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Samer Hamidi
Demlie Mekonnen Marye,1 Desta Debalkie Atnafu,1,2 Melesse Belayneh,1 Ayenew Takele Alemu3
1Department of Health System Management and Health Economics, School of Public Health, Bahir Dar University, Bahir Dar, Ethiopia; 2International Centre for Evidence in Disability, London School of Hygiene and Tropical Medicine, London, UK; 3Department of Public Health, College of Medicine and Health Sciences, Injibara University, Injibara, Ethiopia
Correspondence: Desta Debalkie Atnafu, Email [email protected]
Background: Increasing free and skilled delivery is a top priority in the global effort to reduce maternal and newborn mortality. Reducing user-fees through exemption policy has contributed to universal health coverage. However, there is scant evidence regarding the effect of exempted maternal services on adherence to utilization in Ethiopia. Thus, this study aimed to assess the effect of fee exemption policy on adherence to maternal health service utilization and its predictors.
Methods: A community-based comparative cross-sectional study was conducted in Bahir Dar City. A two-stage multistage sampling was employed; 497 women participated. Data were collected by face-to-face interview; entered and cleaned using Epi-Data 3.1. SPSS version 25 was used for further analysis. Bivariable and multivariable logistic regression models were computed to assess the association between explanatory and outcome variables. An adjusted odds ratio with a 95% confidence interval was used to interpret the degree of association. The effect of fee exemption policy on adherence to maternal health service utilization was measured by propensity score matching.
Results: The overall adherence to maternal service utilization was 54.2%. Factors associated with adherence to maternal health service utilization were pregnancy complications [AOR: 4.1, 95% CI (2.32, 7.28)], secondary and above education [AOR: 4.6, 95% CI (1.38, 15.08)], early ANC1 booking [AOR: 3.1, 95% CI (1.83, 5.16)], autonomous women [AOR: 2.1, 95% CI (1.02, 4.39)], user fee exemption [AOR: 2.3, 95% CI (1.20, 4.47)] and high parity [AOR: 0.39, 95% CI (0.2, 0.75)]. User fee exemption induced a 22.7% increment in adherence to maternal service utilization (ATET=0.227, t=2.13).
Conclusion: User fee exemption policy significantly improved adherence to maternal health service utilization. Promoting a fee exemption policy through third-party financing can enhance maternal health service utilization adherence in hard-to-reach settings of Ethiopia by targeting mothers with higher pregnancies, no complications, no autonomy, and less education.
Keywords: user fee exemption, maternal health services, Bahir Dar city, Ethiopia
Background
User fees for healthcare have been implemented in low- and middle-income countries since the 1980s as a strategy to enhance healthcare delivery by raising funds.1 However, studies indicated that user fees attributed to a decline in health services utilization, particularly in Sub-Saharan African (SSA) countries.2 It was evidenced that user fees were linked to reduced use of advanced treatment during pregnancy and childbirth.3 Hence, the exempted services that should be provided free of charge at public health facilities have been introduced by the essential health services package to address the prioritized health goals.4 A study has demonstrated that user fee exemption has a positive effect on adherence to maternal health service utilization; user fee removal has been shown to increase the use of maternal health services in many SSA countries.5
Globally, more than 600 women die every day from pregnancy and childbirth complications.6 Almost all maternal deaths (99%) occurred in developing countries of which 66% accounted for SSA countries.7 However, the Ethiopian Demographic Health Survey (EDHS) estimated a substantial reduction in the pregnancy-related mortality ratio from 871 deaths per 100,000 live births in (EDHS 2000) to 412 deaths per 100,000 live births in (EDHS 2016). Whereas the infant mortality rate was 48 deaths per 1, 000 live births as of (EDHS 2016).8
Despite the presence of exempted services in Zambia, 10% of households have been shown to suffer financial disasters as a result of out-of-pocket payments.9 In Malawi, the implementation of user fee exemption had no effect on the proportion of pregnant women who initiated their first ANC visit in the first trimester and those engaged in postpartum visits.5 World Health Organization recommended that 32% of women should have at least four antenatal care (ANC4) visits during their last pregnancy. However, 37% of women in Ethiopia had no ANC visits. Institutional delivery coverage is low in Ethiopia; home delivery, particularly in hard-to-reach areas is still popular. Five years before 2016 EDHS, 26% of live births were attended in health facilities. Institutional delivery was lower before the implementation of user fee exemption, from 5% in 2000 to 10% five years before 2011.8 In Ethiopia, the healthcare financing reform has been implemented since 2005. The reform incorporated health insurance initiation, fee waiver system, and exemption services in its components to make the services be provided free of charge to anyone at the point of departure.10
Before the introduction of healthcare financing reform in Ethiopia, the average costs for normal and cesarean delivery were 7.70 and 51.80 US $, respectively. The expected out-of-pocket per capita non-health expenditure was also high. The indirect cost which was higher for rural residents than urban residents was another paramount issue. All these induced catastrophic out-of-pocket expenditures for health.10
Adherence to maternal health services utilization (MHSU) from conception (ANC) to postnatal care (PNC) is attributed to multifaceted factors. Socio-demographic factors (eg age, ethnicity, religion, education status, and access to media), household characteristics (eg education attainment of household head, family size, and income), contextual factors (eg place of residence) and maternal factors (eg number of children ever born) were demonstrated as predictors of adherence to MHSU.11
Improving adherence to MHSU is essentially important for attaining sustainable development goals and reducing maternal and neonatal morbidity and mortality in low-income countries.12 Ethiopia has attempted to increase accessibility to maternal healthcare services through the rapid expansion of health facilities, quadrupling the number of qualified midwives, and introducing user fee-exempted services.10 Maternal deaths could also be substantially reduced by increasing the number of skilled birth attendants along with prompt access to secondary and tertiary care.13 Studies suggested that the implementation of the free delivery service policy in public health facilities significantly enhanced institutional delivery service.12 However, evidence is scant regarding the role of user fee exemption policy on adherence to MHSU. Therefore, this study aimed to assess the effect of user fee exemption on adherence to MHSU and to identify its predictors.
Methods and Materials
Study Design and Setting
A community-based comparative cross-sectional study was conducted from March 10, 2021, to April 21, 2021, in Bahir Dar City 560 kilo meters away from Addis Ababa, Ethiopia. The City administration report (2020/2021) estimated 389,177 population living in the city.14 Public health facilities in the city include two comprehensive specialized hospitals, one primary hospital, and ten health centers and the private hospitals and clinics are 4 and 40 in number respectively. Both facilities (public and private) are serving as alternative healthcare markets including maternal healthcare services (conception to post-natal care). Around seventy-nine percent (78.8%) of women gave birth to their current child in health institutions.15
Study Participants and Eligibility Criteria
The study incorporated mothers with a history of pre-post natal follow-up and giving birth at public facilities as intervention (fee exemption users) group and those at private facilities as reference group. Reproductive-age mothers in the selected kebeles who gave birth at health facilities in the last year were included to participate. However, we excluded reproductive-age mothers with acute illness and current pregnancy.
Sample Size Determination
The sample size was computed using Epi-Info 7 software based on the following assumption: 80% statistical power with a level of significance at 5%, odds ratio of 2.21, and an exemption service user to non-user ratio of 1:1. The estimated final sample size was 497 for both user and non-user groups using the double-proportions formula. The sample size was calculated for variables: means of transport to health facilities, maternal education (able to read and write), wealth index, and knowledge about danger signs of pregnancy. Hence, the largest sample size among the exposure variables was taken.
Sampling Procedure
A two-stage multistage sampling technique was employed. First, half of the sub-cities (3 out of 6) were selected randomly using a lottery method. All kebeles (lowest administrative level) in the selected sub-cities were included. A sampling frame (4707) was obtained from the community health information system (urban health extension program). The required sample in each kebele was allocated proportionally. Finally, the study participants fulfilling the inclusion criteria were selected using a simple random sampling technique.
Data Collection and Study Variables
Data were collected by trained midwifery professionals and urban health extension workers (4 in number each) using face-to-face interview technique and two senior BSc nurses were assigned as supervisors. Structured questionnaire tools were prepared in English and then translated into Amharic language and back into English to check their consistency. It was pre-tested using 5% of the sample outside of the study kebeles. Training for the data collectors and supervisors was provided. Supervisors and authors checked data for completeness and consistency on a daily basis. The adherence to MHSU was a dependent variable. The independent variables were age, educational status, religion, family size, gravidity, distance traveled, autonomous, wealth index, media exposure, and timing of first ANC visit, pregnancy complication, perceived quality of care, and healthcare costs.
Operational Definition
Exempted maternal health services refer to services that should be provided free of charge at public health facilities.16 We considered the MHSU as “good adherence” when a woman completely received at least four ANC visits and institutional delivery by skilled healthcare providers and post-natal maternal and neonatal care within 48 hours by either skilled healthcare providers or health extension workers. Women who missed at least one of the above-mentioned healthcare services of any level were considered to have “poor adherence” to MHSU.17 Women were considered autonomous when they could make decisions on healthcare spending alone or with their husbands. If the decision of healthcare spending was controlled by others (husbands only or other people), they were considered non-autonomous.18 Early initiation of ANC was considered if women were booked for ANC1 visits at the first trimester of pregnancy (within 16 weeks of gestation).19
Data Analysis
Data were entered and cleaned using Epi-Data version 3.1 and then exported to SPSS version 25 for further analysis. Descriptive statistics: Frequency, mean, standard deviations, and percentages were used to summarize the results. Bi-variable and multivariable logistic regression models were computed to assess the association between outcome variables and explanatory variables. Variables with a p-value <0.25 in bivariate logistic regression were candidates for multivariable logistic regression analysis. Adjusted odds ratio with a 95% CI at p-value <0.05 was used to interpret the strength of association. Model fitness was checked by the Hosmer and Lemeshow test (p=0.586)17. An independent sample t-test was computed to test the significant difference between exempted service users and non-users to the explanatory variables. A propensity score matching (PSM) was used to estimate the effect of user fee exemption on adherence to MHSU.20 Based on the closeness of the estimated propensity score of each individual from exempted service user and non-user groups, a matched sample was drawn.
Results
Socio-Demographic (Predisposing) Characteristics
A total of 454 women (227 exempted service users and 227 non-users) participated in the study giving a response rate of 91.34%. The mean age of respondents was 29±5.3 (SD) years. Independent sample t-test (χ2 for categorical variables) showed that exempted service users and non-users were significantly differentiated about husband’s education, religion, marital status, and family size factors (Table 1).
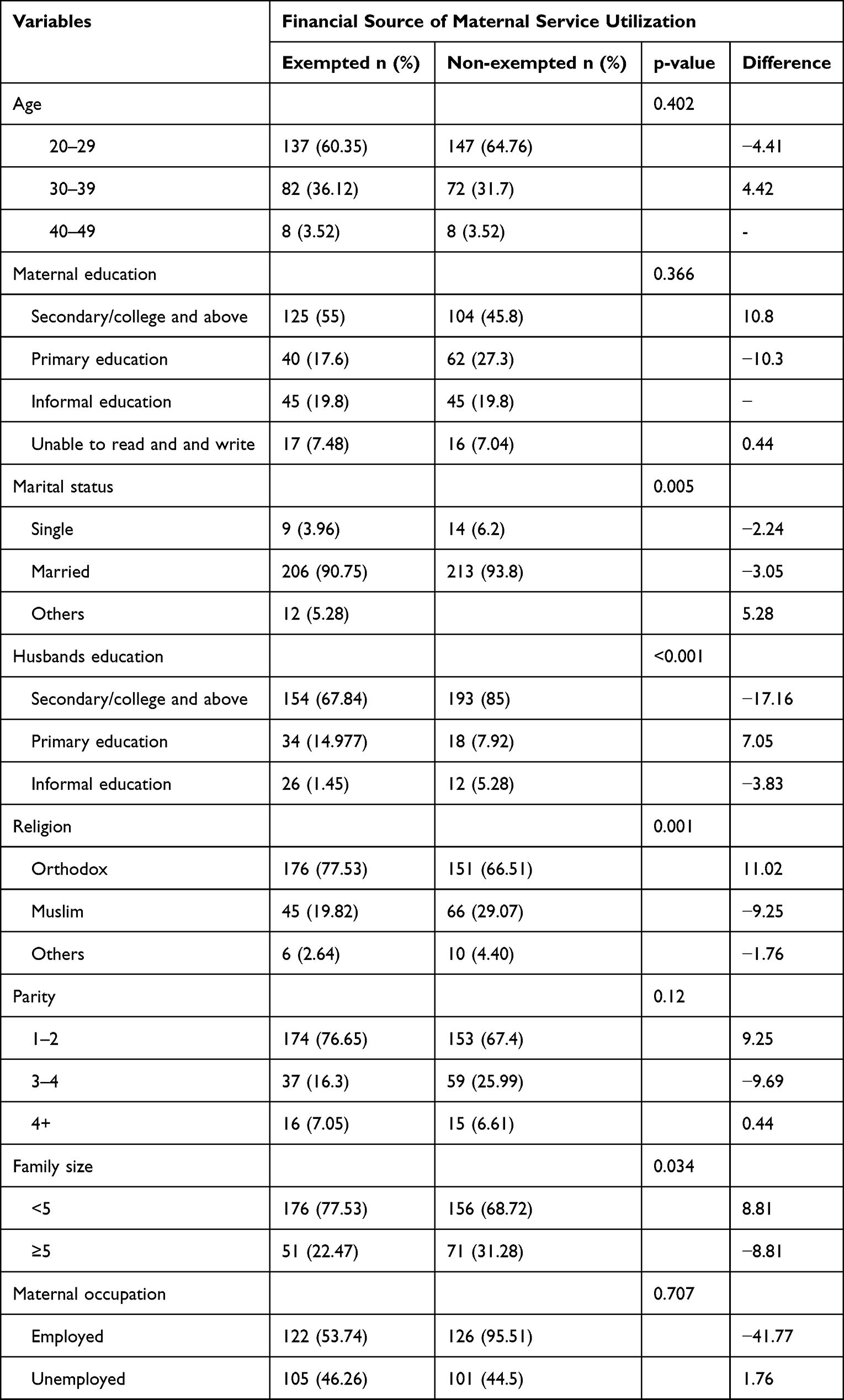 |
Table 1 Predisposing Characteristics of Women Who Gave Birth in Health Facilities in the Last Year Preceding the Survey Date, Bahir Dar City, 2021 (n = 454) |
Enabling Characteristics
A large segment of exempted service users (85.02%) traveled less than 5 kilo meters to get maternal health service from health facilities. Of those, 76.65% reached the service area within 30 minutes. However, 73.13% of non-exempted service users traveled greater than 5 kilometers to get maternity service from public health facilities. As a result, they prefer to use private health facilities. Generally, distance to public health facilities, travel time, means of transportation, women’s autonomy, and wealth index showed significant differences between exemption and non-exemption service users (Table 2).
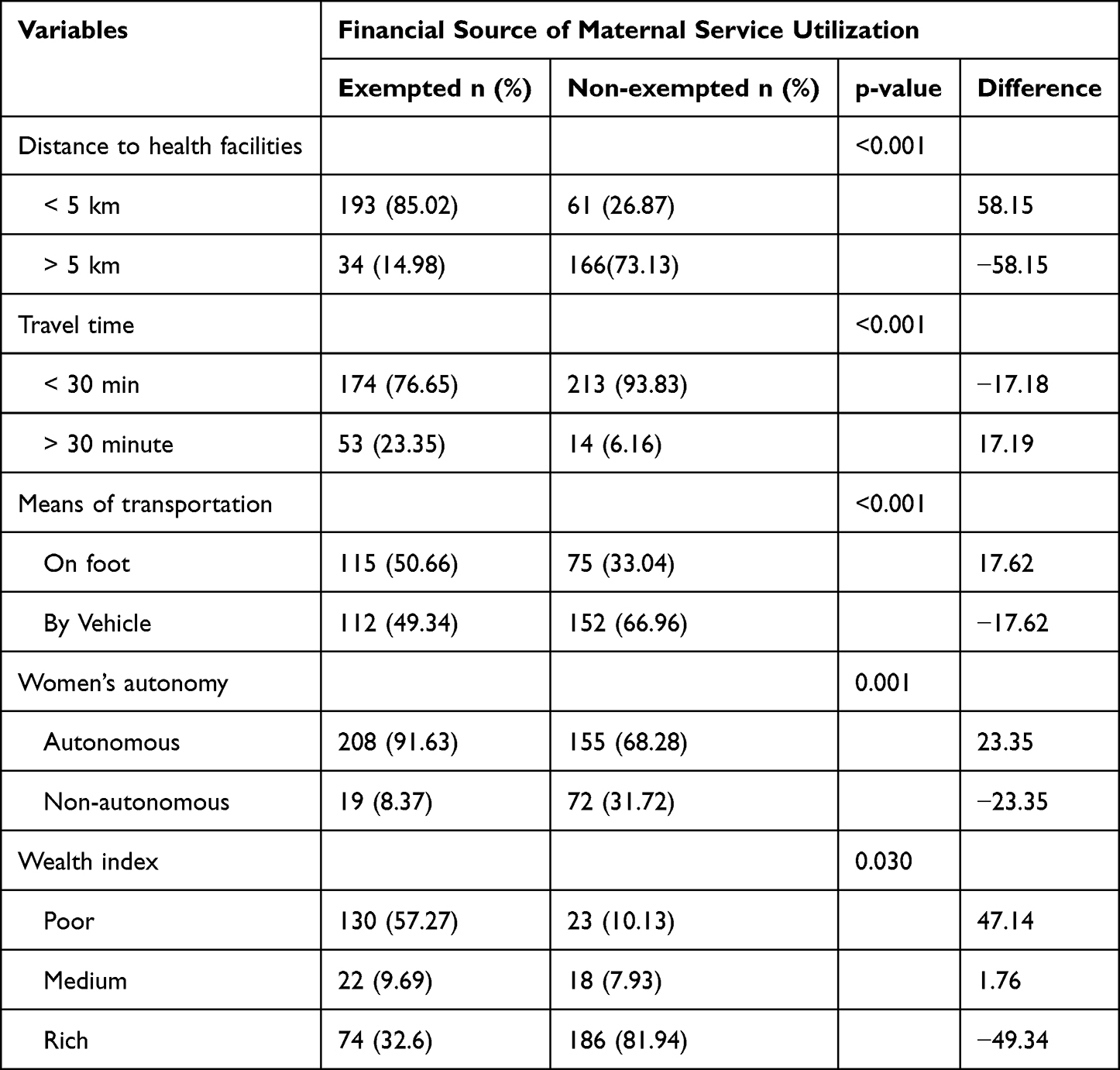 |
Table 2 Enabling Characteristics of Women Who Gave Birth in Health Facilities in the Last Year Preceding the Survey Date, Bahir Dar City, 2021 (N-454) |
Need-Based Characteristics
More than half of exempted service users (59.91%) had a history of early ANC initiation within the first trimester (before 16 weeks). However, 50.22% of non-exempted service users had a history of late first ANC initiation. About 90% of exempted service users and 97.8% of non-exempted service users had received a core set of services during prenatal visits (weight and BP measured (95% and 99.6%), urine and blood samples tested (96.8% and 100%), tetanus toxoid vaccination (95.9% and 99.6%), iron tablet supplementation (94.5% and 99.1%), counseling about danger sign of pregnancy (91.4% and 97.3%) and physical and ultra sound examination in privacy or ethical manner (91.8% and 98.2%) of exempted and non-exempted service users respectively. About 97.8% of user fee users and 15.4% of exempted service users incurred expenses during utilization of maternal service. From those, 97.8% of non-exempted service users and 19.3% of exempted service users incurred expenses for direct health care (ie for counseling, medication, and investigation). Variables like timing of ANC 1 booking, quality of care during ANC, complications related to pregnancy, history of family illness, and knowledge about danger signs of pregnancy showed significant differences between the two groups (Table 3).
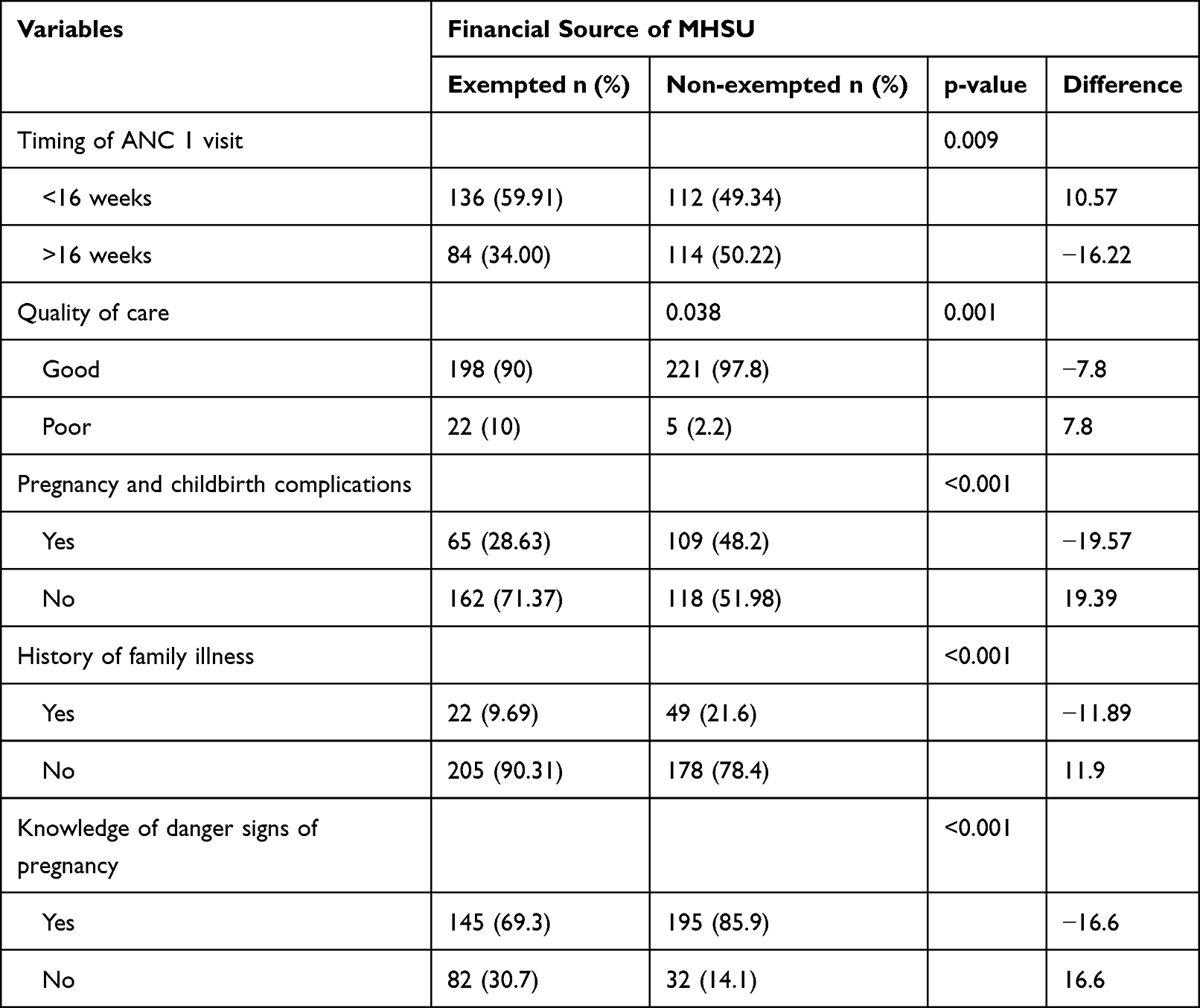 |
Table 3 Need-Based Characteristics of Women Who Gave Birth in Health Facilities in the Last Year Preceding the Survey Date, Bahir Dar City, 2021 (N=454) |
Adherence to Maternal Health Service Utilization
The overall adherence to MHSU was 54.2% (95% CI: 49.3–58.6). The proportion of good adherence to MHSU was 63.4% and 44.9% for exemption fee users and non-users respectively. Among exemption fee users 4+ ANC and postnatal care utilization was 69.5% and 85%, respectively. However, it was 60.2% and 69.8% for user fee exemption non-users. There is a statistically significant difference in adherence to MHSU between exemption fee users and non-users (p-value < 0.001, t = 4.07).
Factors Associated with Adherence to Maternal Health Services Utilization
The odds of adherence to MHSU was four times higher among respondents with pregnancy and childbirth complication than those without complication [AOR: 4.1, 95% CI (2.32, 7.28)]. Respondents with secondary and above education were 5 times more likely to adhere to MHSU than their counterparts [AOR: 4.6, 95% CI (1.38, 15.08)]. Furthermore, the odds of adherence to MHSU were about three times higher among women with primary education than those with informal education and below [AOR: 3.3, 95% CI (1.01, 11.03)]. The odds of adherence to MHSU were 2.1 times more likely among autonomous women than non-autonomous [AOR: 2.1, 95% CI (1.02, 4.39)]. Early booking for ANC1 (<16 weeks) was also attributed to adherence to MHSU more than late booking (>16 weeks) [AOR: 3.1, 95% CI (1.83, 5.16)]. It was significantly seen that exemption fee users were 2 folds more likely to adhere to MHSU when compared to non-users [AOR: 2.3, 95% CI (1.20, 4.47)]. However, women having parity 4+ were 61% less likely to comply with adherence to MHSU as compared to lower parity [AOR: 0.39, 95% CI (0.2, 0.75)] (Table 4).
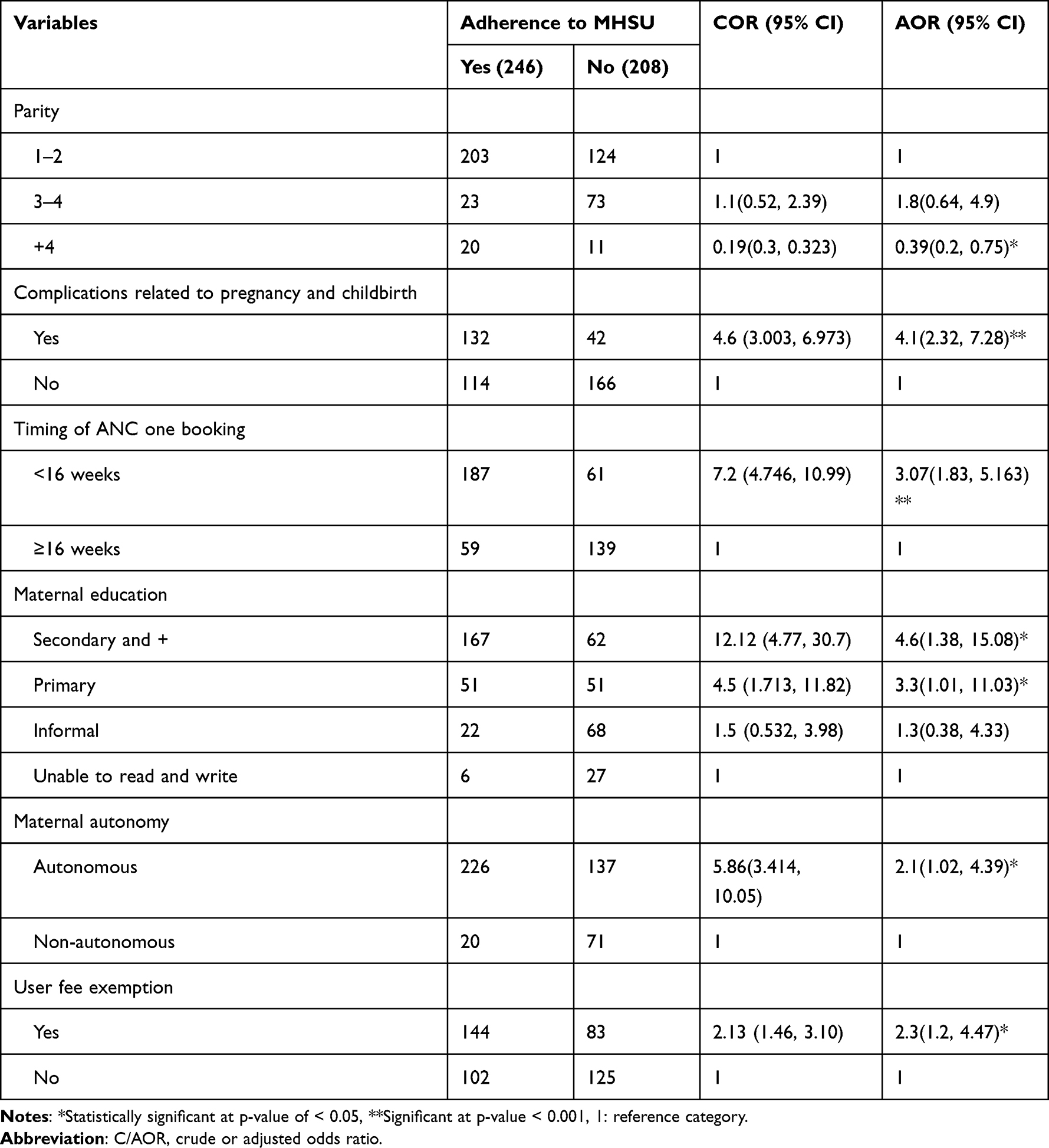 |
Table 4 Factors Associated with Adherence to Maternal Health Services Utilization in Bahir Dar City, March 2021 (N=454) |
Effect of User Fee Exemption Policy on Adherence to MHSU
The average treatment effect of user fee exemption on treated groups (users) was 0.227 (t=2.13, p-value=0.03). User fee exemption enrollment had induced a 22.7% increment in adherence to MHSU (Table 5).
 |
Table 5 The Average Treatment Effect of User Fee Exemption on Adherence to MHSU, Bahir Dar City, March 2021 (N=445) |
Discussion
Our study revealed that the overall adherence to MHSU was 54.2%. This was higher than other findings from West Gojjam, Ethiopia (12.1%),21 Nigeria (19%),22 Gambia (1.8%),23 Bangladesh (32.6%)24 and Afghanistan (17.8%).25 The reason for this discrepancy might be attributed to our inclusion of women only with institutional delivery and urban residents. Other studies included women with a history of institutional and home delivery modes and urban and rural residents.
This study identified multifaceted factors attributing to the adherence to MHSU. The odds of adherence to MHSU were higher among women with pregnancy-related complication than those without complications. This is in line with a finding from Lesotho which reported that pregnancy-related complications doubled the MHSU in higher hospitals.26 Women with identified and known complications related to their pregnancy might have good health-seeking behavior to mitigate risk. Similarly, the odds of adherence to MHSU were higher among women having primary/secondary and above educational background than their counterparts. This finding was supported by a study conducted in SSA which revealed that educated women benefited more from user fee abolition than non-educated women.27 It might be the fact that educated women have more information than non-educated about maternal health services consumption and its consequences. It was also revealed that autonomous women were 21% more likely to adhere to MHSU than non-autonomous women. A similar study from Bangladesh reported that autonomous women had a 20% higher probability of attending at least ANC4 visits and adhering to MHSU compared with non-autonomous women.24 This might be because autonomous women could have an opportunity to plan and decide alone or together with husbands concerning seeking and utilizing healthcare services.
Early booking to ANC1 was another statistically significant predictor of adherence to MHSU. Early-booked women to ANC1 were 3 times more likely to adhere to MHSU when compared to those lately booked. Other studies conducted in W/Gojjam and Arba Minch, Ethiopia reported similar findings.17,21 The findings are in congruence with the WHO recommendation of early booking to ANC1 enhancing the frequency and subsequent visits for maternal health services.28 The study also evidenced that exemption fee users were 2 times more likely to adhere to MHSU than non-users. It was in line with the findings from other studies.5,26,29–34 The possible explanation for this finding might be due to the removal of out-of-pocket payments encouraging women to seek and consume maternal health services. It implies implementing user fee exemption enhances MHSU. However, women having 4+ parity were 61% less likely to adhere to MHSU than those having lower parity. Other studies from Kenya35 and Ghana36 reported similar results.
Our study evidenced that user fee exemption significantly improved the adherence to MHSU over user fee exemption non-users. Adherence to MHSU was induced by 22.7% due to the presence of a user fee exemption policy. The finding was supported by another study.37 This implies that the implementation of a user fee exemption policy is imperative to improve maternal health services taking.
Limitations
The study was based on consumers’ perspectives only, the healthcare suppliers’ perspectives were not considered. The data might be prone to social desirability bias as the data were collected by health professionals working in the community. The recall bias might be considered as another limitation of this study. Factors do not establish a temporal relationship as a cross-sectional design was conducted.
Conclusions
Implementation of the user fee exemption policy to improve adherence to MHSU was effective. Pregnancy-related complications, maternal education, timing of ANC1 booking, women’s autonomy, user fee exemption, and high parity were significantly associated factors of adherence to MHSU. Advocating for early booking, maternal empowerment and education, and maternal engagement to user fee exemption should be emphasized to enhance adherence to MHSU at public health facilities.
Abbreviations
ANC, Antenatal Care; AOR, Adjusted Odds Ratio; CI, Confidence Interval; COR, Crude Odds Ratio; EDHS, Ethiopian Demographic Health Survey; MHSU, Maternal Health Service Utilization; PNC, Postnatal Care; SD, Standard Deviation; SPSS, Statistical Packages for Social Science; SSA, Sub Saharan Africa.
Data Sharing Statement
All data underlying the findings described in this manuscript were fully available without restriction.
Ethical Approval
Ethical clearance was received from the institutional review board (IRB) of the College of Medicine and health sciences, Bahir Dar University. Written informed consent was obtained from study participants. Anonymity and confidentiality were considered. The study adhered to tenets of the Declaration of Helsinki.
Acknowledgments
Authors gratefully acknowledge Bahir Dar University, data collectors, supervisors, and women who participated in the study.
Author Contributions
All authors made a significant contribution to the work reported: in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
We authors did not receive any financial support for the research (study design, data collection, and analysis), authorship, and publication of this manuscript.
Disclosure
The authors have declared that no competing interests exist.
References
1. Cotlear D, Rosemberg N. Going Universal in Africa: How 46 African Countries Reformed User Fees and Implemented Health Care Priorities. World Bank; 2018.
2. Borghi J, Storeng KT, Filippi V. Overview of the costs of obstetric care and the economic and social consequences for households. Reducing financial barriers to obstetric care in low-income countries; 2008.
3. Gabrysch S, Campbell OM. Still too far to walk: literature review of the determinants of delivery service use. BMC Pregnancy Childbirth. 2009;9(1):34. doi:10.1186/1471-2393-9-34
4. Alebachew A, Mitiku W, Mann C, Berman P. Exempted health services in Ethiopia: cost estimates and its financing challenges. Harvard T.H. Chan School of Public Health and Breakthrough International Consultancy PLC: Boston, Massachusetts and Addis Ababa, Ethiopia; 2018.
5. Manthalu G, Yi D, Farrar S, et al. The effect of user fee exemption on the utilization of maternal health care at mission health facilities in Malawi. Health Policy Plan. 2016;31(9):1184–1192. doi:10.1093/heapol/czw050
6. Naghavi M, Abajobir AA, Abbafati C, et al. Global, regional, and national age-sex specific mortality for 264 causes of death, 1980–2016: a systematic analysis for the global burden of disease study 2016. Lancet. 2017;390(10100):1151–1210.
7. Bongaarts J. WHO, UNICEF, UNFPA, World Bank Group, and United Nations Population Division Trends in Maternal Mortality: 1990 to 2015. Geneva: World Health Organization 2015, Wiley Online Library; 2016.
8. Csa, I., Central statistical agency (CSA)[Ethiopia] and ICF. Ethiopia demographic and health survey, Addis Ababa, Ethiopia and Calverton, Maryland, USA; 2016.
9. Masiye F, Kaonga O, Kirigia JM. Does user fee removal policy provide financial protection from catastrophic health care payments? Evidence from Zambia. PLoS One. 2016;11(1):e0146508. doi:10.1371/journal.pone.0146508
10. Pearson L, Gandhi M, Admasu K, et al. User fees and maternity services in Ethiopia. Int J Gynaecol Obstet. 2011;115(3):310–315. doi:10.1016/j.ijgo.2011.09.007
11. Chalise B, Chalise M, Bista B, et al. Correlates of continuum of maternal health services among Nepalese women: evidence from Nepal multiple indicator cluster survey. PLoS One. 2019;14(4):e0215613. doi:10.1371/journal.pone.0215613
12. Demissie A, Worku A, Berhane Y. Effect of implementing a free delivery service policy on women’s utilization of facility-based delivery in central Ethiopia: an interrupted time series analysis. J Pregnancy. 2020;2020:1–7. doi:10.1155/2020/8649598
13. Nguyen HT, Torbica A, Brenner S, et al. Economic evaluation of user-fee exemption policies for maternal healthcare in Burkina Faso: evidence from a cost-effectiveness analysis. Value Health. 2020;23(3):300–308. doi:10.1016/j.jval.2019.10.007
14. Central Statistical Agency. Population Projections for Ethiopia 2007-2037: Addis Ababa, July 2013.
15. Abeje G, Azage M, Setegn T. Factors associated with institutional delivery service utilization among mothers in Bahir Dar City administration, Amhara region: a community based cross sectional study. Reprod Health. 2014;11(1):22. doi:10.1186/1742-4755-11-22
16. Ministry of Health. Essential health services Package for Ethiopia; 2005.
17. Haile D, Kondale M, Andarge E, et al. Level of completion along continuum of care for maternal and newborn health services and factors associated with it among women in Arba Minch Zuria woreda, Gamo zone, Southern Ethiopia: a community based cross-sectional study. PLoS One. 2020;15(6):e0221670. doi:10.1371/journal.pone.0221670
18. Tarekegn SM, Lieberman LS, Giedraitis V. Determinants of maternal health service utilization in Ethiopia: analysis of the 2011 Ethiopian demographic and health survey. BMC Pregnancy Childbirth. 2014;14(1):161. doi:10.1186/1471-2393-14-161
19. Villar J, Bergsjo P. WHO Antenatal Care Randomized Trial: Manual for the Implementation of the New Model. World Health Organization; 2002:37.
20. Ahmed S, Sarker AR, Sultana M, et al. The impact of community-based health insurance on the utilization of medically trained healthcare providers among informal workers in Bangladesh. PLoS One. 2018;13(7):e0200265. doi:10.1371/journal.pone.0200265
21. Emiru AA, Alene GD, Debelew GT. Women’s retention on the continuum of maternal care pathway in west Gojjam Zone, Ethiopia: multilevel analysis. BMC Pregnancy Childbirth. 2020;20(1):1–14. doi:10.1186/s12884-020-02953-5
22. Akinyemi JO, Afolabi RF, Awolude OA. Patterns and determinants of dropout from maternity care continuum in Nigeria. BMC Pregnancy Childbirth. 2016;16(1):1–11. doi:10.1186/s12884-016-1083-9
23. Oh J, Moon J, Choi JW, et al. Factors associated with the continuum of care for maternal, newborn and child health in the Gambia: a cross-sectional study using demographic and health Survey 2013. BMJ Open. 2020;10(11):e036516. doi:10.1136/bmjopen-2019-036516
24. Ghose B, Feng D, Tang S, et al. Women’s decision-making autonomy and utilisation of maternal healthcare services: results from the Bangladesh demographic and health survey. BMJ Open. 2017;7(9):e017142. doi:10.1136/bmjopen-2017-017142
25. Mumtaz S, Bahk J, Khang Y-H. Current status and determinants of maternal healthcare utilization in Afghanistan: analysis from Afghanistan demographic and health survey 2015. PLoS One. 2019;14(6):e0217827. doi:10.1371/journal.pone.0217827
26. Steele SJ, Sugianto H, Baglione Q, et al. Removal of user fees and system strengthening improves access to maternity care, reducing neonatal mortality in a district hospital in Lesotho. Trop Med Int Health. 2019;24(1):2–10. doi:10.1111/tmi.13175
27. McKinnon B, Harper S, Kaufman JS. Who benefits from removing user fees for facility-based delivery services? Evidence on socioeconomic differences from Ghana, Senegal and Sierra Leone. Soc Sci Med. 2015;135:117–123. doi:10.1016/j.socscimed.2015.05.003
28. USAID, C. Maternal and Child Survival. Geneva: WHO Antenatal Care Guidelines: Malaria in Pregnancy Frequently Asked Questions (FAQ); 2016.
29. Edu BC, Agan TU, Monjok E, et al. Effect of free maternal health care program on health-seeking behaviour of women during pregnancy, intra-partum and postpartum periods in Cross River State of Nigeria: a mixed method study. Open Access Maced J Med Sci. 2017;5(3):370. doi:10.3889/oamjms.2017.075
30. Zeng W, Sun D, Mphwanthe H, et al. The impact and cost-effectiveness of user fee exemption by contracting out essential health package services in Malawi. BMJ Global Health. 2019;4(2):e001286. doi:10.1136/bmjgh-2018-001286
31. Nguyen HT, Zombré D, Ridde V, et al. The impact of reducing and eliminating user fees on facility-based delivery: a controlled interrupted time series in Burkina Faso. Health Policy Plan. 2018;33(8):948–956. doi:10.1093/heapol/czy077
32. Ravit M, Audibert M, Ridde V, et al. Removing user fees to improve access to caesarean delivery: a quasi-experimental evaluation in western Africa. BMJ Global Health. 2018;3(1):e000558. doi:10.1136/bmjgh-2017-000558
33. Garchitorena A, Miller AC, Cordier LF, et al. In Madagascar, use of health care services increased when fees were removed: lessons for universal health coverage. Health Affairs. 2017;36(8):1443–1451. doi:10.1377/hlthaff.2016.1419
34. Novignon J, Ofori B, Tabiri KG, et al. Socioeconomic inequalities in maternal health care utilization in Ghana. Int J Equity Health. 2019;18(1):141. doi:10.1186/s12939-019-1043-x
35. Dennis ML, Benova L, Abuya T, et al. Initiation and continuity of maternal healthcare: examining the role of vouchers and user-fee removal on maternal health service use in Kenya. Health Policy Plan. 2019;34(2):120–131. doi:10.1093/heapol/czz004
36. Ganle JK, Mahama MS, Maya E, et al. Understanding factors influencing home delivery in the context of user‐fee abolition in Northern Ghana: evidence from 2014 DHS. Int J Health Plann Manage. 2019;34(2):727–743. doi:10.1002/hpm.2731
37. Laurel E, Hatt MM, Supriya M, Claudia MConlon CM. Effects of user fee exemptions on the provision and use of maternal health services: a review of literature. J Health Popul Nutr. 2013;4:67–80.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.