Back to Journals » Clinical Interventions in Aging » Volume 14
Use of transcutaneous electrical acupoint stimulation for prevention of postoperative delirium in geriatric patients with silent lacunar infarction
Authors Hou HJ ![]() , Xue FS
, Xue FS ![]() , Guo RJ
, Guo RJ ![]()
Received 12 December 2018
Accepted for publication 3 January 2019
Published 1 February 2019 Volume 2019:14 Pages 249—252
DOI https://doi.org/10.2147/CIA.S197922
Checked for plagiarism Yes
Editor who approved publication: Dr Zhi-Ying Wu
Hai-Jun Hou, Fu-Shan Xue, Rui-Juan Guo
Department of Anesthesiology, Beijing Friendship Hospital, Capital Medical University, Beijing, People’s Republic of China
In a preliminary study, Gao et al1 assessed the preventive effect of transcutaneous electrical acupoint stimulation (TEAS) on postoperative delirium (POD) in geriatric patients with silent lacunar infarction. They showed that TEAS could reduce the development of POD and might be related to attenuated neuroinflammation by reducing the permeability of the blood–brain barrier. Given that POD is a common postoperative complication associated with adverse events and outcomes including functional decline, and increased risks of morbidity and mortality in elderly surgical patients, their findings have the potential implications. To differentiate the real effect of one factor on primary endpoint in a randomized trial, however, all of other factors must be standardized for avoidance of potential bias. Other than the limitations described in the discussion, we noted several issues in this study that were not addressed well.
View original paper by Gao et al.
Dear editor
In a preliminary study, Gao et al1 assessed the preventive effect of transcutaneous electrical acupoint stimulation (TEAS) on postoperative delirium (POD) in geriatric patients with silent lacunar infarction. They showed that TEAS could reduce the development of POD and might be related to attenuated neuroinflammation by reducing the permeability of the blood–brain barrier. Given that POD is a common postoperative complication associated with adverse events and outcomes including functional decline, and increased risks of morbidity and mortality in elderly surgical patients, their findings have the potential implications. To differentiate the real effect of one factor on primary endpoint in a randomized trial, however, all of other factors must be standardized for avoidance of potential bias. Other than the limitations described in the discussion, we noted several issues in this study that were not addressed well.
First, study subjects were elderly patients undergoing spine surgery. The study did not provide the baseline education level and preoperative serum albumin concentration of patients. In available literature, both lower baseline education level and preoperative albumin concentration have been identified as significant risk factor of POD in elderly surgical patients.2,3 Regarding intraoperative factors, moreover, only providing anesthesia and operation durations were insufficient. It has been shown that intraoperative major blood loss and blood transfusion are significantly associated with an increased risk of POD after noncardiac surgery in elderly patients.4 In addition, the authors did not observe and compare the incidences of postoperative adverse events and complications between groups. In fact, prolonged hospital and intensive care unit stay, postoperative complications including urinary tract infection, pneumonia, and cognitive impairment can increase the risk of POD after noncardiac surgery.5 We are concerned that any imbalance in the above unknown factors would have biased their findings.
Second, this study excluded patients with an increased risk of POD, such as those with mini-mental state examination score of <24 or dementia, preoperative delirium, history of neurological or mental illness, current use of tranquilizers or antidepressants.5 Thus, an important question that remains unanswered in this study is whether TEAS is an effective treatment in elderly patients with an increased risk of POD. Furthermore, this study only assessed the incidence of POD, but not the severity and duration of POD due to a short observed time. The available evidence indicates that both more severe POD and longer in-hospital POD duration are significantly associated with worse postoperative outcomes.6 We believe that the results of this study would be more informative if the design had included these issues.
Finally, because of the small sample size, small intergroup mean differences and large standard deviations in this study, we questioned their results that serum levels of TNF-α and IL-6 were higher at T2–3 and serum levels of MMP-9 and S100β were higher at T3 in group C compared with group TEAS (P<0.05). Revalidation of these results with statistical software confirms our doubts.
Acknowledgment
All authors report no financial support.
Disclosure
The authors report no conflicts of interest in this communication.
References
Gao F, Zhang Q, Li Y, et al. Transcutaneous electrical acupoint stimulation for prevention of postoperative delirium in geriatric patients with silent lacunar infarction: a preliminary study. Clin Interv Aging. 2018;13:2127–2134. | ||
Sprung J, Roberts RO, Weingarten TN, et al. Postoperative delirium in elderly patients is associated with subsequent cognitive impairment. Br J Anaesth. 2017;119(2):316–323. | ||
Patti R, Saitta M, Cusumano G, Termine G, Di Vita G. Risk factors for postoperative delirium after colorectal surgery for carcinoma. Eur J Oncol Nurs. 2011;15(5):519–523. | ||
Marcantonio ER, Goldman L, Orav EJ, Cook EF, Lee TH. The association of intraoperative factors with the development of postoperative delirium. Am J Med. 1998;105:380–384. | ||
Smith TO, Cooper A, Peryer G, Griffiths R, Fox C, Cross J. Factors predicting incidence of post-operative delirium in older people following hip fracture surgery: a systematic review and meta-analysis. Int J Geriatr Psychiatry. 2017;32(4):386–396. | ||
Hughes CG, Patel MB, Jackson JC, et al.; MIND-ICU, BRAIN-ICU Investigators. Surgery and anesthesia exposure is not a risk factor for cognitive impairment after major noncardiac surgery and critical illness. Ann Surg. 2017;265(6):1126–1133. |
Authors’ reply
1Department of Anesthesiology, The Third Hospital of Hebei Medical University, Shijiazhuang City, Hebei, People’s Republic of China; 2Department of Anesthesiology, Children’s Hospital of Hebei Province, Shijiazhuang City, Hebei, People’s Republic of China; 3Department of Anesthesiology, Tianjin Third Central Hospital, Tianjin, People’s Republic of China
Correspondence: Qiujun Wang, Department of Anesthesiology, The Third Hospital of Hebei Medical University, No 139, Ziqiang Road, Shijiazhuang City, Hebei, People’s Republic of China, Tel/fax +86 311 8860 2072, Email [email protected]
Dear editor
We thank Hou et al for their interest in our paper entitled “Transcutaneous electrical acupoint stimulation for prevention of postoperative delirium in geriatric patients with silent lacunar infarction: a preliminary study” and their valuable comments. Here we respond to their concerns.
Hou et al found that baseline education level, intraoperative major blood loss and blood transfusion, and postoperative complications were identified as significant risk factors of postoperative delirium (POD) in elderly surgical patients in the literature. However, some other previous studies have had conflicting results that these factors were not related to POD.1–3 Further studies are needed to confirm these imparities.
For avoidance of potential bias, we set strict exclusion criteria. We would be pleased if our study provokes interest in further research into whether transcutaneous electrical acupoint stimulation (TEAS) is an effective treatment in elderly patients with an increased risk of POD. It will be useful to take into consideration the severity and duration of POD, but unfortunately we did not collect data on these variables due to the short observation time, and we have stated this in the discussion.
Our data were analyzed by SPSS, and the results are as follows.
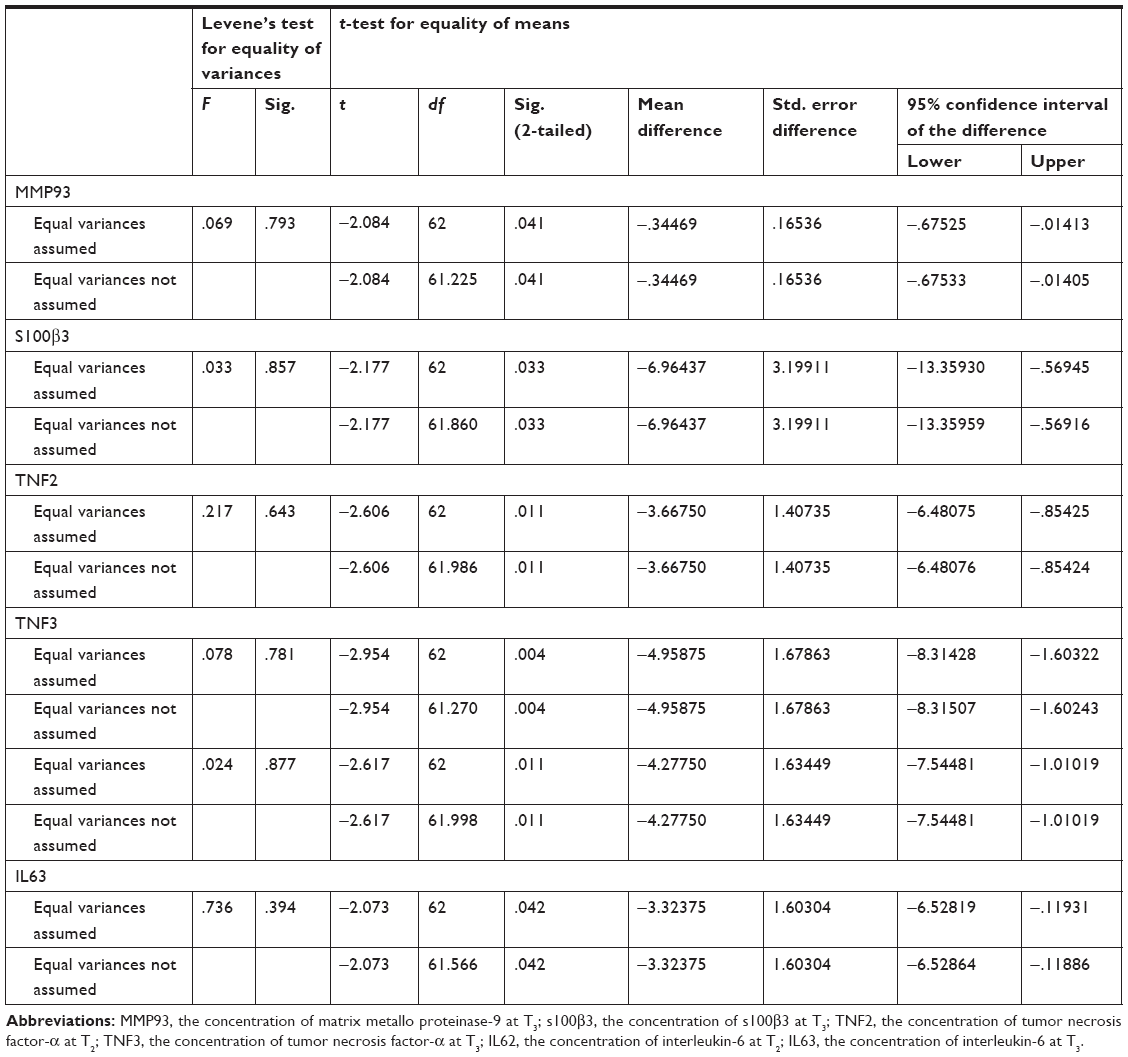 | Abbreviations: MMP93, the concentration of matrix metallo proteinase-9 at T3; s100β3, the concentration of s100β3 at T3; TNF2, the concentration of tumor necrosis factor-α at T2; TNF3, the concentration of tumor necrosis factor-α at T3; IL62, the concentration of interleukin-6 at T2; IL63, the concentration of interleukin-6 at T3. |
Disclosure
The authors report no conflicts of interest in this communication.
References
Kobayashi K, Imagama S, Ando K, et al. Risk Factors for delirium after spine surgery in extremely elderly patients aged 80 years or older and review of the literature: Japan Association of Spine Surgeons with Ambition Multicenter Study. Global Spine J. 2017;7(6):560–566. | ||
Brown CH 4th, LaFlam A, Max L, et al. Delirium after spine surgery in older adults: incidence, risk factors, and outcomes. J Am Geriatr Soc. 2016;64(10):2101–2108. | ||
Jiang X, Chen D, Lou Y, et al. Risk factors for postoperative delirium after spine surgery in middle- and old-aged patients. Aging Clin Exp Res. 2017;29(5):1039–1044. |
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.