")
Back to Journals » Clinical, Cosmetic and Investigational Dermatology » Volume 14
Use of Methotrexate in the Treatment of Moderate to Severe Plaque Psoriasis in France: A Practice Survey
Authors Fougerousse AC , Mery-Bossard L, Parier J, Taieb C , Bertolotti A , Maccari F
Received 16 March 2021
Accepted for publication 15 April 2021
Published 23 April 2021 Volume 2021:14 Pages 389—393
DOI https://doi.org/10.2147/CCID.S311269
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jeffrey Weinberg
Anne-Claire Fougerousse,1 Laure Mery-Bossard,2 Josiane Parier,3 Charles Taieb,4 Antoine Bertolotti,5,6 Francois Maccari3 On behalf of GEM ResoPso
1Dermatology Department, Hôpital d’Instruction des Armées Bégin, Saint Mandé, 94160, France; 2Dermatology Department, Centre Hospitalier Intercommunal Poissy Sant Germain en Laye, Saint-Germain-en-Laye, 78100, France; 3Private Practice, La Varenne Saint Hilaire, Saint-Maur-des-Fossés, 94210, France; 4European Market Maintenance Assessment, Patients Priority Department, Fontenay sous-Bois, France; 5Infectious Diseases and Dermatology Department, Centre Hospitalier Universitaire de la Réunion, Saint Pierre, La Réunion, France; 6Inserm CIC1410, Centre Hospitalier Universitaire de la Réunion, Saint Pierre, La Réunion, France
Correspondence: Anne-Claire Fougerousse
Dermatology Department, Hôpital d’Instruction des Armées Bégin, 69 Avenue de Paris, Saint Mandé, 94160, France
Tel + 331 43 98 50 00
Fax + 331 43 98 49 15
Email [email protected]
Purpose: To evaluate the modalities of methotrexate prescription for moderate to severe psoriasis by dermatologists in France.
Patients and Methods: We performed a national online practice survey between October and December 2020.
Results: A total of 254 dermatologists responded, 237 reported prescribing methotrexate for moderate to severe psoriasis in adults, of which 57% as a first line systemic treatment. Nineteen percent reported performing a test dose at the initiation of treatment. Methotrexate was prescribed orally in 54.7% of cases, subcutaneously in 44.8% of cases and intramuscularly in 0.4% of cases. The initial weekly dose of methotrexate was < 15 mg for 30% of the dermatologists and ≥ 15 mg for 70% of them. Two hundred and three dermatologists had already change the route of administration for methotrexate from the oral to injectable form due to poor tolerance (48.3%), lack of efficacy (35%) or lack of compliance (16.7%). Two hundred thirty-four dermatologists (98.7%) reported prescribing folic acid with methotrexate, and 79.3% reported prescribing tests evaluating the risk of hepatic fibrosis. Forty-three percent of dermatologists have not initiated or have reduced their prescriptions since the beginning of the pandemic of COVID-19. Prescribing patterns were different according to the type of practice (private practice versus hospital/mixed practice).
Conclusion: Methotrexate is used by the majority of dermatologists interviewed for moderate to severe psoriasis in adults, with heterogeneity of practices.
Keywords: psoriasis, methotrexate, practice survey, dermatologists
Adult psoriasis is a frequently occurring chronic inflammatory dermatosis, the prevalence of which is estimated to be 4.4% in France.1 Moderate to severe forms, defined by a Psoriasis Activity and Severity Index (PASI) score >10, an affected skin surface >10, a Dermatology Life Quality Index (DLQI) score >10, or the involvement of particular locations (palms and soles, scalp, face, genital area, nails, etc.) justify prescription of a systemic treatment.2 Methotrexate is the first-line systemic treatment recommended in France.3 Surveys of international practice have highlighted heterogeneity in the prescription of methotrexate for this indication.4,5 Herein, we evaluate the modalities of methotrexate prescription for moderate to severe psoriasis by dermatologists in France.
Patients and Methods
We conducted a practice survey of Reso member dermatologists. Reso gathers more than 700 French dermatologists [ie nearly one French dermatologist out of 4]. These dermatologists work exclusively in hospitals, exclusively in private practice or in a mixed practice. They were asked by email to answer a digital questionnaire between October and December 2020. In the invitation email to participate in the project, each doctor had to confirm his or her agreement to participate in order to access the online questionnaire.They were under no obligation to respond and were not paid for it.
Questionnaire
The questionnaire was developed by dermatologists and a physician specialist in public health. It collected the age of the dermatologist, the length of the practice, the mode of practice (hospital, private or mixed), whether consultation dedicated to psoriasis is offered, and the prescription of methotrexate for adult psoriasis. It collected information on the methods of prescribing methotrexate, including the method of administration, dose, concomitant prescription of folic acid, monitoring methods, as well as the impact of the COVID-19 pandemic on prescriptions. The reasons for not prescribing methotrexate were collected for dermatologists who stated that they did not prescribe methotrexate for this indication.
For this type of study, French regulations do not require submission to an ethics committee as this study does not enter the field of the deliberation n°2018-154 of the 3rd of May 2018 (JORF n°0160 of the 13th of July 2018).
Statistics
Quantitative data are expressed as the average ± standard deviation (SD), and qualitative data are expressed as percentages (%). Means were compared using Student’s t-test, and frequencies were compared using Chi-square test. A value of p < 0.05 was considered statistically significant. Statistical analyses were performed using R software version 3.5.1.
Results
Characteristics of Dermatologists
Two hundred fifty-four dermatologists answered the questionnaire, representing 7.6% of French dermatologists [source JO Sénat du 11/12/2014 - page 2726]. The average length of practice was 18.9 years; 74 (29.1%) worked in hospitals, 93 (36.6%) in private practice and 87 (34.2%) in a mixed practice; and 71 (27.9%) offered consultation dedicated to psoriasis.
Prescription of Methotrexate
Two hundred thirty-seven dermatologists (93.3%) reported prescribing methotrexate for moderate to severe psoriasis in adults. This proportion was 100% for dermatologists with hospital activity and 90% for those in private or mixed practices.
Seventeen dermatologists declared themselves to be non-prescribers. Among these physicians, 9 were in private practice, and 8 were in a mixed practice. Reasons given for non-prescription included fear of side effects (n=8), lack of experience (n=7), and dearth of eligible patients (n=2).
Prescription Modalities
Among prescribers, 57% stated that they prescribed methotrexate as a first line systemic treatment for adult psoriasis, 29% as a second line treatment and 14% as a third line treatment or less frequently. Dermatologists estimated the percentage of their moderate to severe psoriatic patients treated with methotrexate to be 36.2%.
Forty-six dermatologists (19%) reported that they perform a test dose at the initiation of treatment. Methotrexate was prescribed orally in 54.7% of cases, subcutaneously in 44.8% (pen, 36.1%; syringe, 8.7%), and intramuscularly in 0.4% of cases. The proportion of patients judged to be autonomous in carrying out the injections was 65.4%. The initial weekly dose of methotrexate was less than 15 mg for 30% of the dermatologists (7.5 mg: 7.6%; 10 mg: 16%; and 12.5 mg: 6.7%) and ≥15 mg for 70% (15 mg: 51.9%; 17.5 mg: 7.1%; 20 mg: 9.7%; 22.5 mg: 0.4%; and 25 mg: 0.4%). The time elapsing between dermatologists prescribing and evaluating the efficacy of methotrexate was less than 6 weeks for 9% (2 weeks: 0.4%; 4 weeks: 8.4%), from 6 to 8 weeks for 13% (6 weeks: 4.6%; 8 weeks: 8%) and greater than or equal to 10 weeks for 78% (10 weeks: 1.3%; 12 weeks: 30.4%; and 16 weeks: 46.8%). Two hundred and three dermatologists (86%) stated that they had already changed the route of administration for methotrexate (from the oral to injectable form) due to poor tolerance (48.3%), lack of efficacy (35%) or lack of compliance (16.7%).
In the event of a therapeutic response being deemed insufficient, 40 dermatologists (16.9%) declared changing to subcutaneous administration, 20 (8.4%) changing treatment and 177 dermatologists (74.7%) to increasing the dose of methotrexate. Of these changes, the adjustment steps were 2.5 mg/week in 54.9% of cases, 5 mg/week in 41.8% of cases, and other in 3.4% of cases. In the case of digestive side effects, 172 dermatologists (72.6%) reported switching to subcutaneous administration, 29 (12.2%) to decreasing the dosage of methotrexate, and 36 (15.2%) to changing treatment. In cases of asthenia, 122 dermatologists (51.5%) reported reducing the dose of methotrexate, 87 (36.7%) changing treatment, and 28 (11.8%) switching to subcutaneous administration.
Two hundred thirty-four dermatologists (98.7%) reported prescribing folic acid with methotrexate. The dose was 5 mg/week for 59 dermatologists (24.9%), 10 mg/week for 134 (56.5%) and more than 10 mg/week for 44 (18.6%). The recommended day of use was the day after taking methotrexate for 24 dermatologists (10.1%), 48 hours after taking methotrexate for 204 dermatologists (86.1%), and every day except for the day of methotrexate use for 9 dermatologists (3.8%).
One hundred eighty-eight dermatologists (79.3%) stated that they prescribed tests evaluating the risk of hepatic fibrosis, including Fibrotest® for 25 (13.3%), pro-collagen III assay for 110 (58.5%) and Fibroscan for 132 (70.2%).
Since the start of the COVID-19 pandemic, 128 dermatologists (54%) reported that their methotrexate prescriptions for psoriasis had remained stable, 71 (30%) that they had decreased, and 3 (1.3%) that they had increased. Twenty-eight (11.8%) reported that they had not initiated methotrexate since the beginning of the pandemic.
Prescribing patterns by type of practice are shown in Table 1.
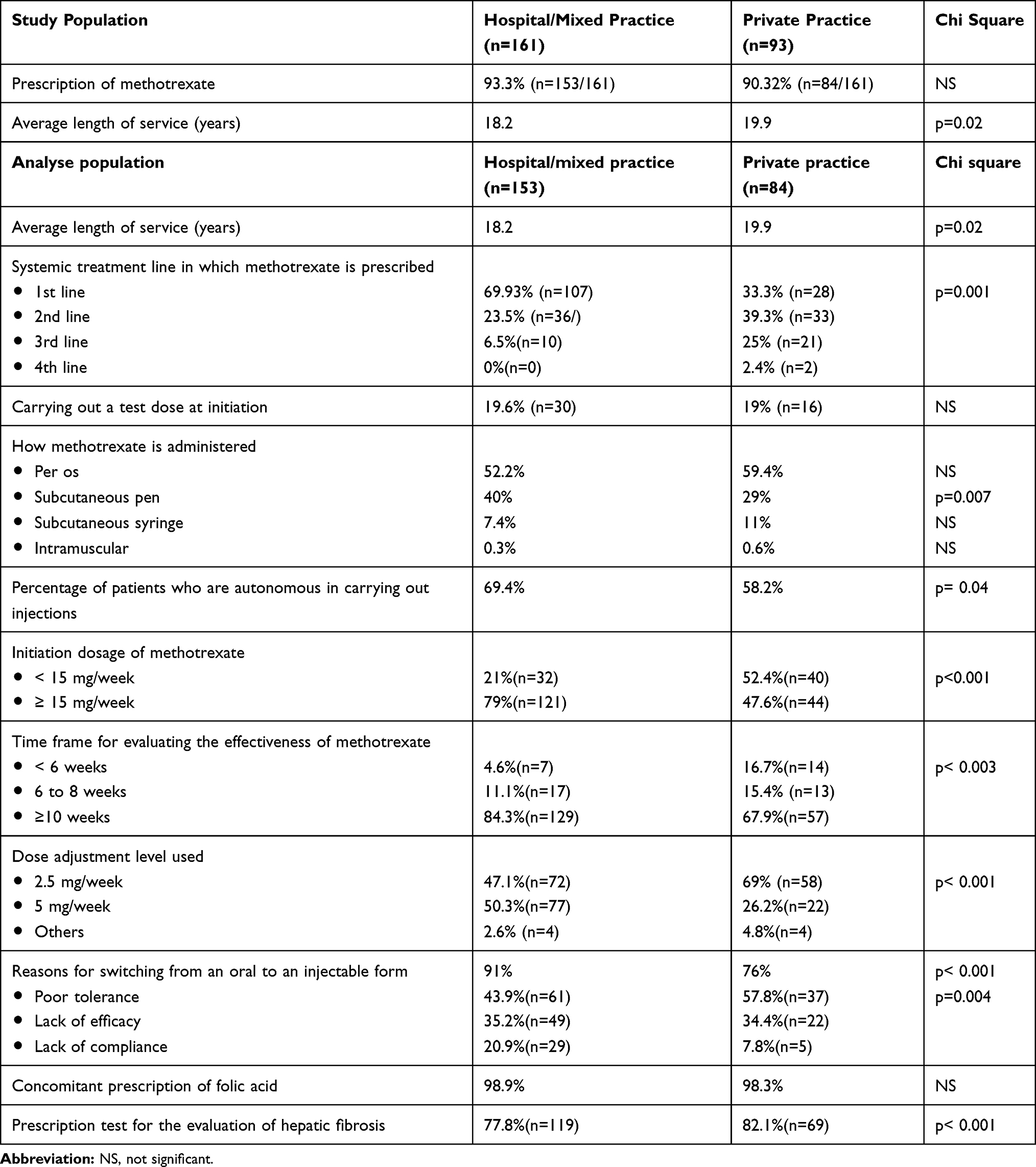 |
Table 1 Results by Mode of Practice (Hospital and Mixed Practice/Private Practice) |
Discussion
The results of this survey underline the heterogeneity of practices in the prescription of methotrexate in moderate to severe psoriasis in adult patients in France. In fact, even though almost all dermatologists questioned used methotrexate for moderate to severe psoriasis in adults, the methods of prescription vary, apart from to the association with folic acid supplementation, which is almost systematic.
Only slightly more than one-half of dermatologists questioned indicated that they prescribe methotrexate as a first-line systemic treatment for moderate to severe psoriasis, whereas it is the first-line systemic treatment recommended in France.3 A fifth of dermatologists questioned stated that they perform a test dose, which is currently no longer compulsory3 but may be useful in fragile patients.6,7 Almost two-thirds of dermatologists questioned start at a dose between 7.5 and 15 mg/week, in accordance with French recommendations.3 However, a high cumulative dose during the first month of treatment (between 60 and 75 mg) was associated with improved efficacy in one study,8 while an initial dose of 15 mg/week was proposed in some recommendations.7,9 The oral route of administration is preferred, although recent data have shown better efficacy and tolerance with a subcutaneous route of administration in a cohort of German patients.9 Even though the different recommendations agree on the need for folic acid supplementation,3,7,10 prescription modalities differ: while there are currently no British recommendations,10 a daily supplementation, except if methotrexate is administered concomitantly is suggested by American recommendations7 and a 5mg supplementation, 24h after the intake of methotrexate, is suggested by French recommendation.3 The time taken to evaluate the efficacy of treatment is more than 10 weeks for 78% of dermatologists, consistent with the kinetics of the molecule.3,7 The vast majority of dermatologists interviewed stated that they monitor the risk of hepatic fibrosis upon methotrexate use by dedicated testing. This risk remains debated since meta-analyses have yielded contradictory results; the cumulative dose of methotrexate has not been systematically identified as a risk factor, in contrast to diabetes, alcoholism and obesity.11,12 The COVID-19 pandemic has impacted the prescription of methotrexate among the dermatologists questioned, since 43% of them have not initiated or have reduced their prescriptions since the beginning of the pandemic. However, data have highlighted the absence of a seriously increased risk of COVID-19 in those undergoing systemic treatment for psoriasis, whether in the initiation or maintenance phase of treatment.13 It might be useful to vaccinate against COVID-19 before initiating methotrexate treatment, particularly in patients at risk of severe COVID-19, as there is a lower vaccine response in patients on this treatment.14
For the analysis, we grouped dermatologists in mixed and hospital-based practices together, as practising in a hospital environment in France allows access to the primary prescription of certain psoriasis treatments (cyclosporine and biotherapy). This study highlights differences in practice according to prescribing patterns. Dermatologists in hospital and mixed practice more frequently prescribe methotrexate as a first line systemic treatment at a higher initial dosage, more often in the form of subcutaneous pens, and evaluate their patients later. This may reflect a greater habit of methotrexate use. Their patients are more autonomous in performing subcutaneous injections, likely because they benefit from therapeutic education by paramedical staff. Dermatologists in private practice, on the other hand, carry out more tests to monitor risk to the liver. We have assessed whether the date of graduation has an impact, it does not for the prescription of methotrexate, test dose or fibrosis test, only the initiation dose is different.
The limitations of this study are the declarative nature of the data and the method of recruitment of the dermatologists questioned as they all participate in a network dedicated to chronic inflammatory dermatoses.
Conclusion
The results of our study show that methotrexate is used by the majority of dermatologists interviewed for moderate to severe psoriasis in adults. We highlighted heterogeneity in prescription modalities depending on the mode of practice (hospital based or private) but not the years of experience.
Disclosure
Funding source: Nordic Pharma laboratory. Dr Anne-Claire Fougerousse report grants from NORDIC Pharma, during the conduct of the study; Dr Josiane Parier reports personal fees from Medac, personal fees from Janssen, personal fees from Novartis, personal fees from Amgen, personal fees from Leo Pharma, outside the submitted work.
The authors report no other conflicts of interest in this work.
References
1. Richard MA, Corgibet F, Beylot-Barry M, et al. Sex- and age-ajusted prevalence estimates of five chronic inflammatory skin diseases in France: results of the OBJECTIFS PEAU study. J Eur Acad Dermatol Venereol. 2018;32:1967–1971. doi:10.1111/jdv.14959
2. Mrowietz U, Kragballe K, Reich K, et al. Definition of treatment goals for moderate to severe psoriasis: a European consensus. Arch Dermatol Res. 2011;303(1):1–10. doi:10.1007/s00403-010-1080-1
3. Amatore F, Villani AP, Tauber M, Viguier M, Guillot B; Psoriasis Research Group of the French Society of Dermatology (Groupe de Recherche sur le Psoriasis de la Société Française de Dermatologie). French guidelines on the use of systemic treatments for moderate-to-severe psoriasis in adults. J Eur Acad Dermatol Venereol. 2019;33(3):464–483. doi:10.1111/jdv.15340
4. Gyulai R, Bagot M, Griffiths CEM, et al. Current practice of méthotrexate use for psoriasis: results of a worldwide survey among dermatologists. J Eur Acad Dermatol Venereol. 2015;29(2):224–231. doi:10.1111/jdv.12495
5. Mazzuoccolo LD, Luna PC, Marciano S, et al. Real world prescription trends of méthotrexate for psoriasis in Argentina: results of a national survey. J Dermatolog Treat. 2017;28(7):631–634. doi:10.1080/09546634.2017.1329503
6. Menting SP, Dekker PM, Limpens J, Hooft L, Spuls PI. Methotrexate dosing regimen for plaque-type psoriasis: a systematic review of the use of test-dose, start-dose, dosing scheme, dose adjustments, maximum dose and folic acid supplementation. Acta Derm Venereol. 2016;96(1):23–28. doi:10.2340/00015555-2081
7. Menter A, Gelfand JM, Connor C, et al. Joint American Academy of Dermatology-National Psoriasis Foundation guidelines of care for the management of psoriasis with systemic nonbiologic therapies. J Am Acad Dermatol. 2020;82(6):1445–1486. doi:10.1016/j.jaad.2020.02.044
8. Tournier A, Khemis A, Maccari F, et al. Methotrexate efficacy and tolerance in plaque psoriasis. A prospective real-life multicentre study in France. Ann Dermatol Venereol. 2019;146(2):106–114. doi:10.1016/j.annder.2018.11.011
9. Reich K, Sorbe C, Griese L, Reich JLK, Augustin M. The value of subcutaneous vs. oral méthotrexate: real-world data from the German psoriasis registry PsoBest. Br J Dermatol. 2020. doi:10.1111/bjd.19690.
10. Warren RB, Weatherhead SC, Smith CH, et al. British Association of Dermatologists’ guidelines for the safe and effective prescribing of methotrexate for skin disease 2016. Br J Dermatol. 2016;175(1):23–44. doi:10.1111/bjd.14816
11. Montaudié H, Sbidian E, Paul C, et al. Methotrexate in psoriasis: a systematic review of treatment modalities, incidence, risk factors and monitoring of liver toxicity. J Eur Acad Dermatol Venereol. 2011;25(Suppl 2):12–18. doi:10.1111/j.1468-3083.2011.03991.x
12. Maybury CM, Jabbar-Lopez ZK, Wong T, Dhillon AP, Barker JN, Smith CH. Methotrexate and liver fibrosis in people with psoriasis: a systematic review of observational studies. Br J Dermatol. 2014;171(1):17–29. doi:10.1111/bjd.12941
13. Fougerousse AC, Perrussel M, Bécherel PA, et al. Systemic or biologic treatment in psoriasis patients does not increase the risk of a severe form of COVID-19. J Eur Acad Dermatol Venereol. 2020;34(11):e676–e679. doi:10.1111/jdv.16761
14. Chiricozzi A, Gisondi P, Bellinato F, Girolomoni G. Immune response to vaccination in patients with psoriasis treated with systemic therapies. Vaccines (Basel). 2020;8(4):769. doi:10.3390/vaccines8040769
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.