")
Back to Journals » International Journal of Women's Health » Volume 14
Use of Galactagogues in a Multi-Ethnic Community in Southeast Asia: A Descriptive Study
Authors Tan ML , Foong SC , Foong WC, Ho JJ
Received 21 March 2022
Accepted for publication 15 August 2022
Published 22 September 2022 Volume 2022:14 Pages 1395—1404
DOI https://doi.org/10.2147/IJWH.S366288
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Everett Magann
May Loong Tan, Siew Cheng Foong, Wai Cheng Foong, Jacqueline J Ho
Department of Pediatrics, RCSI & UCD Malaysia Campus, George Town, Penang, Malaysia
Correspondence: May Loong Tan, Department of Pediatrics, RCSI & UCD Malaysia Campus, George Town, Penang, Malaysia, Tel +60 42171948, Fax +60 42284285, Email [email protected]
Purpose: Galactagogues are substances that increase breast-milk production. They can be medication, herbs or food. Use of galactagogues may be different among the major ethnic groups in Malaysia. The primary objective of this cross-sectional study is to determine the prevalence of galactagogues use among breastfeeding mothers in a multi-ethnic community.
Patients and Methods: Self-administered questionnaires were distributed between November 2016 and January 2017 to mothers attending the health clinics and private hospital paediatric clinics in Penang, Malaysia, whose infants were below 6 months of age. The questionnaire enquired about use of galactagogues, types of galactagogue used, perceived effectiveness and sources of information. It also asked mothers about what they would do to increase milk supply.
Results: We analyzed 322 out of 530 questionnaires distributed where 76% of mothers reported use of galactagogues; most of which were food-based: dates (66%), oats (58%) and soya bean (56%). Each major ethnic group had a different preference for galactagogues: Malays (dates), Chinese (soya bean) and Indians (oats). Only one mother used pharmacological galactagogues alone. Galactagogues were perceived to be effective by 65% of mothers who used them. Multivariate analysis showed that use of galactagogues was not related to ethnicity, education, work, perception of milk supply or use of formula milk. The most common source of information on galactagogues came from family and friends.
Conclusion: Use of galactagogues is common in our population, especially food-based ones, and the choice of galactagogues differs by ethnicity. Future studies on efficacy and safety galactagogues should be focused these commonly used ones. There is also a need for qualitative studies to improve our understanding of why they are widely used in this region.
Keywords: breastfeeding, lactation, milk-booster, multi-ethnic
Introduction
It is well recognized that breastfeeding provides many immediate and also long-term benefits to the infant and mother, and breast milk remains the best nutrition for the infants’ early months.1 The World Health Organization (WHO) recommends exclusive breastfeeding for the first six months of life.2 Exclusive breastfeeding means that the infant is only given breast milk with no additional fluids such as formula milk or solids.3 Inadequate milk supply has been the commonest reason given by mothers for formula milk supplementation and early cessation of breastfeeding.4,5 Failure to exclusively breastfeed an infant because of inadequate milk production can be distressing for the mother and increase the risk of illness to the infant.6
Galactagogues are substances that increase breast milk production, although for many of these, their effectiveness has not been determined.7 They can be broadly categorized as pharmacological or non-pharmacological. The pharmacological galactagogues include dopamine receptor antagonists such as metoclopramide and domperidone but other medications like sulpiride and metformin have also been used as galactagogues.8–11 Non-pharmacological galactagogues, on the other hand, are a diverse group of substances ranging from herbal preparations to teas and food. For most of them, the mechanism of action is not known but have been used traditionally to help increase breast milk production. Examples of non-pharmacological galactagogues include fenugreek (Trigonella foenum-graecum), fennel (Foeniculum vulgare), blessed thistle (Cnicus benedictus), shatavari (Asparagus racemosus), anise or aniseed (Pimpinella anisum), milk thistle (Silybum marianum), barley (Hordeum vulgare), malunggay (Moringa oleifera) and goat’s rue (Galega officinalis).12,13 In addition, common food items like ginger has also been used as galactagogue.14
The use of galactagogues, especially non-pharmacological ones, is in many ways influenced by culture. Post-partum women are offered special food or drink to ensure an adequate supply of milk for the newborn. In Indonesia, Bataknese women routinely consume torbangun leaves for a month after delivery, and in the Philippines and in parts of Africa and India, dishes featuring malunggay (moringa) are given to new mothers both as a prevention of and treatment for low milk production.15,16 On the other hand, mothers in Europe are more likely to use galactagogue decoctions and tea brew infusions only when they are faced with low milk production.17
The practice of consuming galactagogues is also common among breastfeeding mothers in Malaysia.18 There are currently two reports in Malaysia, both conducted in the East Coast states of Malaysia, which are relatively mono-cultural and less urbanized.18,19 From these studies, herbal galactagogues and food are the more likely choice. There is little information if this practice is similar in communities that are more culturally diverse. It is important to know the actual prevalence of use of any type of galactagogue so that issues surrounding use of galactagogues such as efficacy and safety can be addressed. Penang, a state located at the northern peninsula of Malaysia is multi-ethnic and has a good mix of urban and rural communities. In the year of the survey, the main ethnic groups in Penang were Malays (41%) Chinese (40%) and Indians (10%).20 The remaining 9% were people who did not consider themselves to belong to one of the aforementioned ethnic groups.
We conducted this study to understand galactagogue usage among a multi-ethnic population which we hope will inform future research seeking to test the safety and effectiveness of commonly used galactagogues. Our primary objective is to determine the prevalence of galactagogue use among breastfeeding mothers in a multi-ethnic community such as Penang, and their source of information. In addition, we also wanted to determine what mothers would do to increase their breast milk supply.
Materials and Methods
This was a cross-sectional study conducted between November 2016 and January 2017 in Penang. The study was conducted at all 31 government community health clinics and 7 private pediatric clinics. Mothers aged above 21 years old with infants less than 6 months old attending the clinics for any reason were invited to participate by the attending doctor or nurse. If consented, they would complete an anonymous self-administered questionnaire. No reimbursements or incentives were offered to the participating mothers.
We specifically designed a questionnaire using an iterative process for this study, which was then translated into Malay and Chinese. The questionnaire collected basic demographic data including age of mother, age of baby, her ethnicity and nationality, employment status and any medical conditions that may interfere with breastmilk production. The questionnaire also asked whether she was still breastfeeding and if not, age of baby when breastfeeding was stopped and reasons for it. This was followed by a list of common galactagogues and for each of the galactagogue listed, the mother was asked if she has ever “heard of it as milk boosters”, “used it as milk boosters” or “never heard of and never used as milk boosters”. The list categorized the galactagogues to pharmacological, herbal and food galactagogues. We defined the categories as follows: a) pharmacological galactagogues: medications or drugs that increases milk supply; b) food galactagogues: substances normally taken as food (meat, vegetables, fruits) used in larger amounts to increase milk supply; and c) herbal galactagogues: plant materials such as leaves, flowers, seed, bark, rhizomes or other plant parts used to increase milk supply. The galactagogues in the list were chosen by the author team either because they were known to be used locally or obtained from literature review. The team has experience in other breastfeeding research as well as providing training on breastfeeding and thus, gained insight into the use of galactagogues locally (See Supplementary Table 1 for the complete list). In addition, the mothers were asked what would be the first step they would take to increase milk supply. They were asked to select one of the following answers: “I do not know”, “Increase the number of times of breastfeeding”, “Use breast pumps”, “Take milk booster(s) such as herbs/food/medicine” or “Others”. Mothers who had used any type of galactagogue were asked about sources of information about galactagogues, whether galactagogues in general were perceived to be effective and which specific galactagogue was effective. The questionnaire was piloted on a small group of mothers and minor adjustments made before it was used in the study.
Sample Size Calculation
Sample size was determined by single proportion formula, normally used for prevalence studies, calculated based on a presumption that 50% of mothers would have used a galactagogue with a 95% confidence interval and 5% confidence level.21 The calculated sample size was 384.
Statistical Analysis
We tabulated the responses and presented numbers and proportions. Free text responses were compiled verbatim and categorized into themes. Questionnaires with more than 50% unanswered questions were excluded. Univariate and multivariate logistic regression were conducted to determine the factors associated with use of galactagogues and presented as odds ratio (OR) with 95% confidence interval (CI). The dependent variables for the univariate and multivariate regression were galactagogue users while the independent variables were ethnicity, education level, employment status, perception of milk supply and use of additional formula milk. All statistical analysis was done using Stata version 13.22 A p-value of <0.05 was taken as the level of significance.
Results
We distributed a total of 530 questionnaires during the study period and collected back 370 questionnaires (response rate of 70%). We analyzed 322 completed questionnaires after excluding 5 incomplete questionnaires and 43 that did not meet our inclusion criteria of the age of babies or mother. The mean age of the mothers was 31.6 (SD 4.7) years and their babies was 3.4 (SD 1.7) months. The mothers were mainly Malaysians (94%), of Malay ethnicity (56%), had at least high school education (96%) and working (61%). Six mothers had twins. Majority of the mothers had no medical illness during pregnancy (84%) and were still breastfeeding at the time of survey (82%). Participants who indicated they had medical illnesses during pregnancy reported one or more of the following: diabetes (n=3), gestational diabetes (n=19), thyroid disease (n=8), hypertension (n=15), kidney related conditions (n=2), anaemia (n=2), asthma (n=2) and schizophrenia (n=1). There were no differences in the demographic details of mothers who used galactagogues and those who did not use them. There were also no differences in the mothers’ satisfaction of milk supply or their need to give additional formula milk between the two groups. See Table 1.
 |
Table 1 Baseline Data: Overall, Galactagogue Users and Non-Galactagogue Users |
Use of galactagogues was common, with 76% (95% confidence interval 71–81%) of the mothers reporting the use of at least one type of galactagogue. Among mothers who used galactagogues, 51% used a combination of food and herbal galactagogues, while 39% used only food galactagogues. The use of pharmacological galactagogues were uncommon (7.5%), and they were mainly used in combination with other groups of galactagogues. Only one reported taking a pharmacological galactagogue (domperidone) on its own.
The most used galactagogues were dates (palm and Chinese dates) (66%), oats (58%), soya bean (56%) and spinach (46%), ginger (46%), garlic (45%) and fenugreek (35%). The least known galactagogues were blessed thistle (92%), milk thistle (89%), nettle (89%), moringa (81%), asparagus (50%), carrot (42%) and shark (42%). A high proportion of mothers did not know that metoclopramide (72%) and domperidone (70%) are medication used to increase milk supply. Lecithin, a food supplement was reportedly used by two mothers. See Tables 2 and 3.
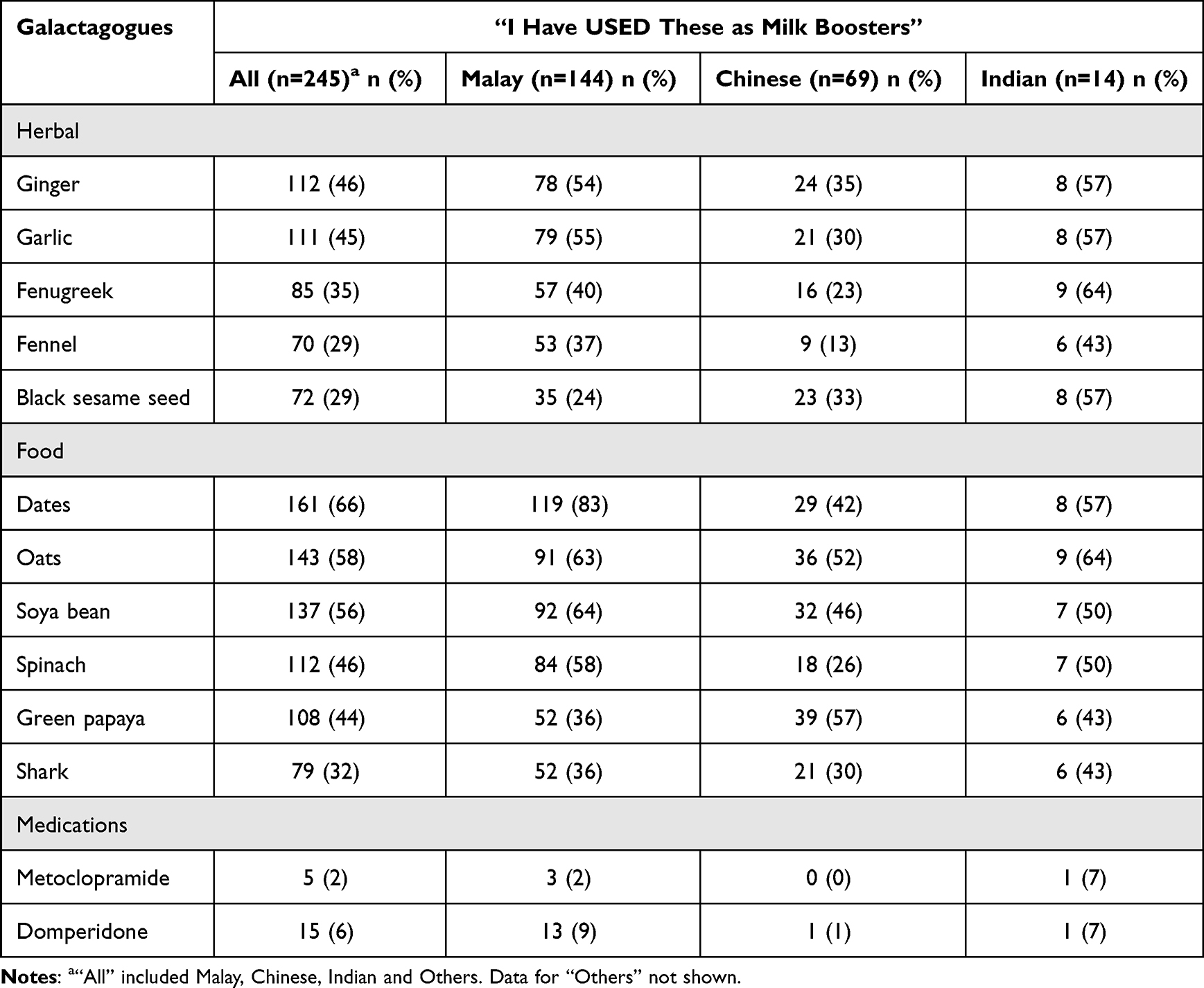 |
Table 2 Most Commonly Used Galactagogues by All Participants and Major Ethnic Groups |
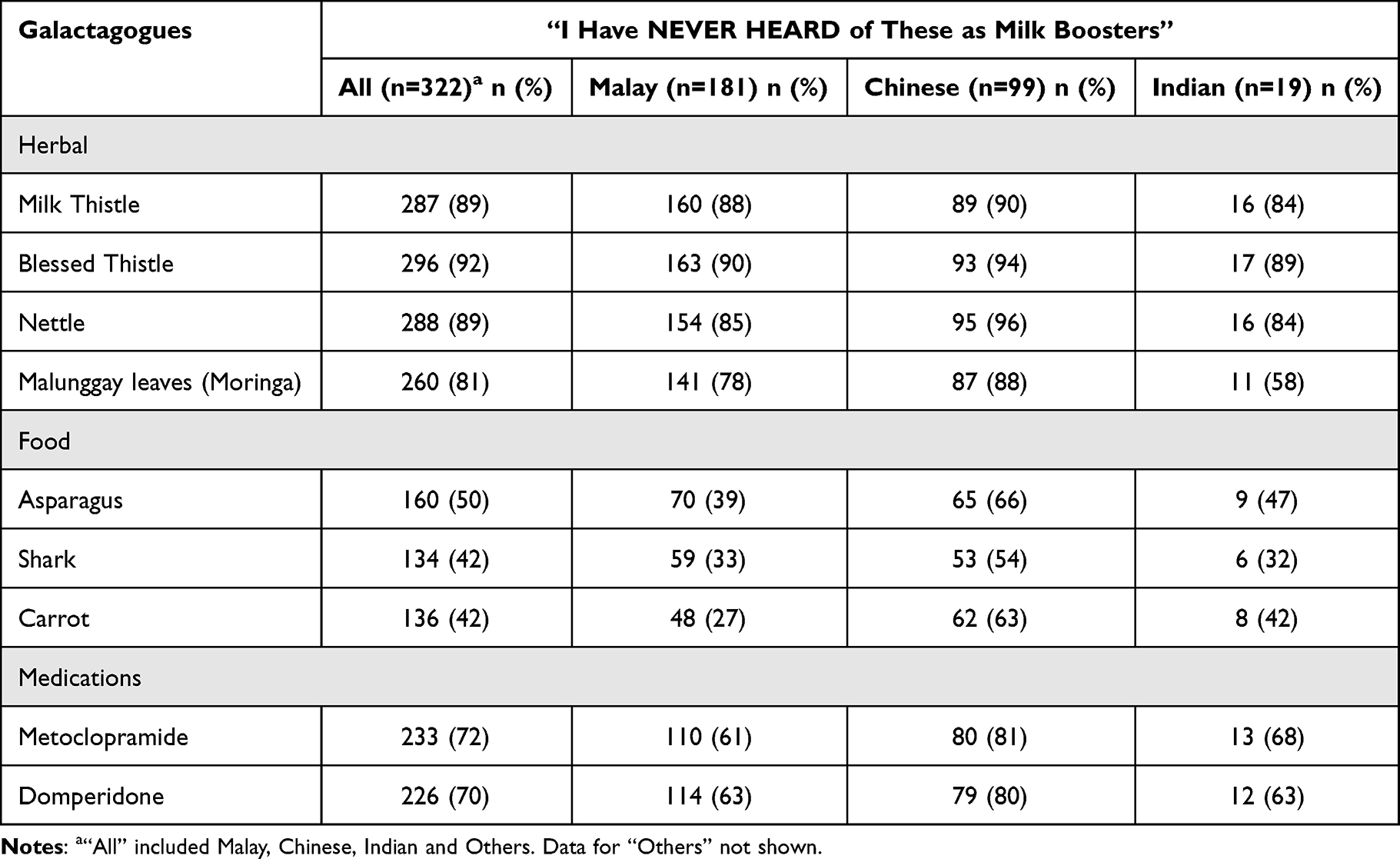 |
Table 3 Least Known Galactagogues by All Participants and Major Ethnic Groups |
The different ethnic groups had different choices of galactagogues. The top three most-frequently used galactagogues among Malay mothers were palm dates, soya bean and oats while among the Chinese mothers were soya bean, green papaya and oats. Among the Indian mothers, oats and fenugreek were the most frequently used choices, followed by black sesame seeds, dates, ginger and garlic. See Figure 1.
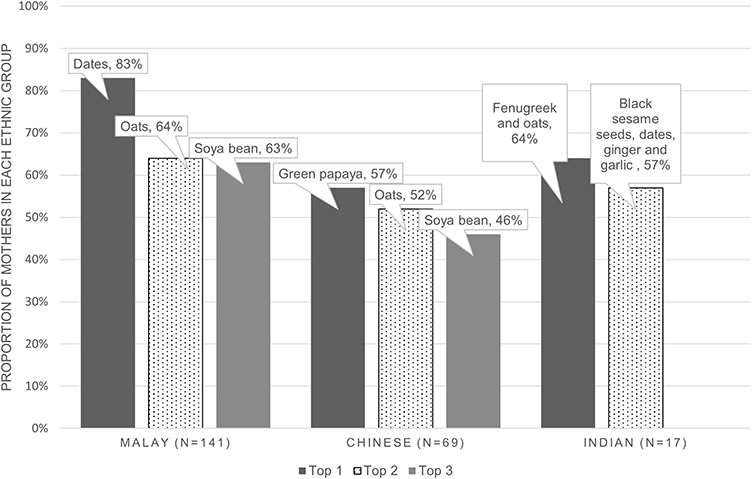 |
Figure 1 Most commonly used galactagogues by ethnicity. Notes: Some mothers used more than one galactagogue. Equal number of Indian mothers reported use of fenugreek and oat, as well as for black sesame seeds, ginger, and garlic. |
Univariate analysis was performed to explore if ethnicity, education level, employment status, satisfaction with milk supply and the need to add formula milk might affect the use of galactagogues. The results showed that apart from a higher use in more educated women (p =0.03), none of these were related to the use of galactagogues. However, with multivariate analysis, none of the factors, including education level had any association with the use of galactagogues. See Table 4.
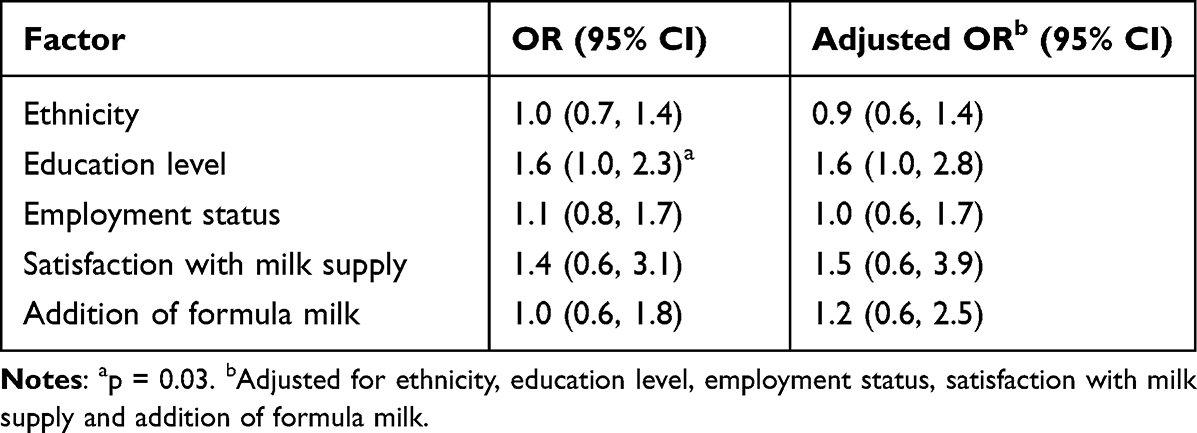 |
Table 4 Demographic and Breastfeeding Factors Affecting Use of Galactagogues |
Of the mothers who used galactagogues, 65% (n =159) perceived them to be effective, 21% (n =52) were unsure if they were effective, and the remaining did not answer the question. The galactagogue most commonly reported as effective was dates (n=41), followed by oats (n=22) and soya bean (n=22). When asked what their first action would be to increase milk supply, 44% of mothers chose increasing the frequency of breastfeeding. The next most common response was to consume galactagogues (15%), followed by use of breast pumps (8%). About 25% of the mothers chose more than one response and a small proportion (5%) responded that they do not know what to do. The combination answers were mainly one of these two combinations: increase frequency of breastfeeding and consume galactagogues (n=37, 45%) and increase frequency of breastfeeding, use a breast pump and consume galactagogues (n=33, 40%). See Figure 2. Out of the 82 combination answers, 75 included consumptions of galactagogues.
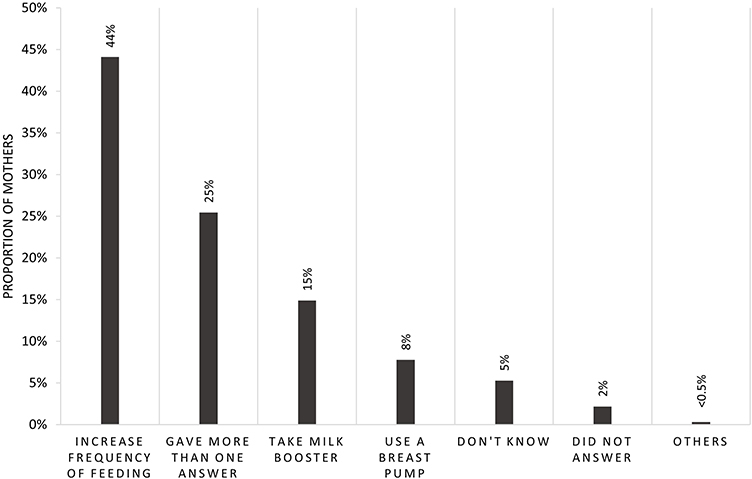 |
Figure 2 Responses to “What would be your first action to increase milk supply?” (n = 322). Notes: Other method was “drink more water” (n=1). Of the 82 (25%) mothers who gave more than one answer, 45% chose to “increase frequency of feeding” and “take a milk booster”, 40% chose to “increase frequency of feeding”, “take a milk booster” and “use a breast pump” and 5% chose to either “increase frequency of feeding” and “use a breast pump” or “take a milk booster” and “use a breast pump”. |
Most mothers reported more than one source of information about galactagogue. Family and friends were the most common source of information (50%), followed by health-care providers (44%), social media (40%) and the internet (33%).
Discussion
This is the first study describing galactagogue use in a multi-ethnic community in South East Asia (SEA) among mothers with an infant below 6 months old. The use of galactagogues was common in our study population with three-quarters of mothers reporting the use of it. As the mothers were largely recruited from health clinics where majority of infants go for their immunization, they were generally representative of mothers with infants of similar age in Penang. From our study, the mothers preferred to use galactagogues originating from food or herbal sources, while pharmacological galactagogues were quite unheard of.
Published data on the use of galactagogues among breastfeeding women is generally scanty and actual prevalence is not known. One study conducted in another state in Malaysia only reported that use of galactagogues was “highly prevalent”.19 Elsewhere around the world, the prevalence of galactagogue use is dependent on the type of galactagogue. In Australia, one study reported the prevalence of herbal galactagogue use to be 60% while another study in United States reported the prevalence of pharmacological galactagogue use to be 6% and herbal galactagogue up to 45%.23,24 Pharmacological galactagogues would require prescription and their use may be determined by drug regulatory bodies specific to each country.25,26 Food or herbal galactagogues do not require any prescriptions and are thus more widely available.
Our study found that differences that exist among ethnic groups in their choice of galactagogues, and this is not found in literature from this region. Palm dates are very popular among the Malay ethnic group in general as it is considered a staple during the annual fasting month of Ramadhan. However, their use as a galactagogue was also common among the other ethnic groups in Malaysia, probably as a result of information sharing on social media and the internet. Cross-cultural influence on general food choices is a documented phenomenon.27
Qualitative studies of women in Australia exploring reasons for use of herbal galactagogues found the driving factors to be related to determination to breastfeed, over-coming low milk supply and feelings of empowerment.28,29 Our data does not suggest these reasons were operating in our cohort. In our univariate analysis, we found that the use of galactagogues here was not related to the mothers’ perceptions of milk supply or addition of infant formula. This suggests that the mothers in our population were not using galactagogues because they had low milk supply. We postulate that reason for galactagogue use among SEA women could be because these herbs and food are part of their traditional post-partum care. It is possible that many may have been consuming them without knowing they were galactagogues. Belief in the health properties of food is one of the driving forces of food choices in SEA.27 Studies on cultural beliefs about health have shown that such beliefs are still very common among the general population in the SEA30 and also around perinatal practices in this region.31 An example of a cultural belief is where certain foods are thought to impact on the well-being of the mother. “Heaty” food such as ginger should be taken during the postnatal period because the mother is considered to have lost “heat” during childbirth. Qualitative studies of women in regions where traditional practices are held strongly are needed to find out the reasons for using galactagogues.
Our study is important because it supports the general perception that galactagogues are frequently used, despite the limited evidence about their safety and effectiveness. A high proportion of mothers who used galactagogues perceived them to be effective, even if they did not have concerns about their milk supply. These mothers may also be sharing this information with their friends and family. Perpetuation of the perceived effectiveness of galactagogues through these anecdotal reports may also be a reason why they are very commonly used. Even though almost all women were using foods and herbs as galactagogues, there may still be safety considerations as most of these galactagogues are not adequately studied. Indeed, a Cochrane review found that there is not enough evidence from RCTs to determine if galactagogues are effective in increasing milk production.32 In this review, the authors also found that adverse effects were poorly reported by studies and thus, there is very limited evidence on them. Women may be unknowingly taking excessive amounts of them without realizing the potential harms. Studies should be done to determine how much on top of normal daily use is needed for these foods to exert their lactogenic effect. Food used beyond usual consumption may have detrimental nutritional effects and mothers using these as galactagogues should be aware of what might happen if they are taken in large amounts.33 Even though the adverse effects of a food-based galactagogue might be small on its own, the effect could be large if multiplied across a large population. In addition, it may have an effect on the infant as well. Newer studies on effects of food and herbal galactagogues have been more intentional in looking for adverse effects.34,35 This is a welcomed step, and we continue to reiterate the call for high-quality studies that clearly state dosages and preparation as well as adequately document adverse effects.
In addition, potential adverse effects of commonly used galactagogues could be identified through adverse drug reporting systems. For example, women who need to see a doctor for any reason during lactation should be encouraged to tell their doctors that they are using a galactagogue. It is possible that the condition that the woman or the baby presents with is potentially an adverse effect of the galactagogue. The doctors should also be encouraged to report these potential adverse effects to the relevant authorities. Researchers can then include these reported adverse effects when conducting their studies.
Although galactagogues are desirable for increasing milk supply, optimizing effective breastfeeding practices should be the priority in managing low breastmilk production.36 It is only when these measures fail that galactagogues could be an option. It was reassuring to know that most mothers in our cohort knew they had to increase the frequency of breastfeeding to increase milk supply. However, there were more than half who picked the wrong answer, thought they had to do more than one thing or did not know the answer. This meant a gap in knowledge on how to self-manage this problem still exists. A study looking at post-partum women’s perception of antenatal breastfeeding education (ANBE) in Penang found that mothers perceived that methods to increase milk supply was not adequately covered during their ANBE.37 It should be emphasized to mothers during their antenatal and postnatal breastfeeding education that taking galactagogues alone without increasing frequency of feeding or milk expression would not solve their problem.
There are several limitations to this study. This is a purely descriptive study therefore no association can be made between the use of galactagogues and breastfeeding outcomes. Many of the food galactagogues we listed are also common food items. Although we specifically instructed the participants that they should only select one of them if they had ever used it with the intention of increasing milk supply, there may have been those who did not follow this instruction, thus over-estimating the frequency of use of these items as a galactagogue. We also did not ask mothers the duration of galactagogue use and if they had experienced any adverse effects from taking them. Our overall sample did not reach our calculated sample size, but the confidence interval of the prevalence of use of galactagogue was relatively narrow. Thus, we consider the effect of not obtaining the calculated sample size was likely to be unimportant. However, the number of Indian mothers were small, thus the results related to this ethnic group need to be read with caution. There may also be a potential selection bias of participants who are better educated because the study utilizes a self-completed questionnaire. However, the demographics of the study population is similar to the general population of Penang, Malaysia.
Conclusion
Use of galactagogues is common across all ethnic groups in our population, especially food-based ones, and the choice of galactagogues differs by ethnicity. Future studies on efficacy and safety galactagogues should be focused on these commonly used ones. Information about use of galactagogues mainly came from family and friends. While most mothers knew that they should increase frequency of breastfeeding to improve milk supply, a significant number would also take a galactagogue as the first step or in combination with increasing frequency of feeds. In addition, galactagogues were commonly used even when there was no expressed concern about milk supply. Therefore, there is also a need for qualitative studies to improve our understanding of why they are widely used in this region.
Abbreviations
WHO, World Health Organization; SEA, South East Asia; ANBE, Antenatal breastfeeding education.
Data Sharing Statement
Data for this study is not publicly available but can be obtained from the corresponding author upon reasonable request.
Ethics Approval and Consent to Participate
This study complies with the Declaration of Helsinki and received ethical approval from the Medical Research Ethics Committee, Ministry of Health Malaysia (NMRR No 16-1512-31886). All participants gave written informed consent.
Acknowledgments
Drs Yew Lyn Lim and Chern Yang Jason Khaw helped develop and conducted the study during their Junior Research Fellowships. We thank the Penang State Health Department and participating Pediatricians in private practice for their support and help; Fairuz Fadzilah Rahim for additional statistical support; as well as Yee Ping Cheah and Bee Hong Ang for data management.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by Penang Medical College Research Grant (Grant Number PMC-RC-10).
Disclosure
All authors report no conflicts of interest in this work
References
1. Victora CG, Bahl R, Barros AJD, et al. Breastfeeding in the 21st century: epidemiology, mechanisms, and lifelong effect. Lancet. 2016;387(10017):475–490. doi:10.1016/S0140-6736(15)01024-7
2. World Health Organization, Unicef. Global strategy for infant and young child feeding; 2003. Available from: whqlibdoc.who.int/publications/2003/9241562218.pdf.
3. World Health Organization. Protecting, Promoting and Supporting Breastfeeding in Facilities Providing Maternity and Newborn Services. Geneva: World Health Organization; 2017.
4. Li R, Fein SB, Chen J, Grummer-Strawn LM. Why mothers stop breastfeeding: mothers’ self-reported reasons for stopping during the first year. Pediatrics. 2008;122(Suppl 2):S69–76. doi:10.1542/peds.2008-1315i
5. Hauck Y, Fenwick J, Dhaliwal S, Butt J. A western Australian survey of breastfeeding initiation, prevalence and early cessation patterns. Matern Child Health. 2011;15(2):260–268. doi:10.1007/s10995-009-0554-2
6. Williams N. Supporting the mother coming to terms with persistent insufficient milk supply: the role of the lactation consultant. J Hum Lact. 2002;18(3):262–263.
7. Zuppa A, Sindico P, Orchi C, et al. Safety and efficacy of galactagogues: substances that induce, maintain and increase breast milk production. J Pharm Pharmaceut Sci. 2010;13(2):162–174. doi:10.18433/J3DS3R
8. Forinash A, Yancey A, Barnes K, Myles T. The use of galactogogues in the breastfeeding mother. Ann Pharmacother. 2012;46(10):1392–1404. doi:10.1345/aph.1R167
9. Aono T, Aki T, Koike K, Kurachi K. Effect of sulpiride on poor puerperal lactation. Am J Obstet Gynecol. 1982;143(8):927–932. doi:10.1016/0002-9378(82)90476-8
10. Barguno JM, Del Pozo E, Cruz M, Figueras J. Failure of maintained hyperprolactinemia to improve lactational performance in late puerperium. J Clin Endocrinol Metabol. 1988;66(4):876–879. doi:10.1210/jcem-66-4-876
11. Nommsen-Rivers LA, Riddle SW, Ward LP, Wagner EA, Thompson AA. Metformin to augment low milk supply: a protocol summary. FASEB J. 2016;30(1Suppl):1150–1158.
12. Zapantis A, Steinberg JG, Schilit L. Use of herbals as galactagogues. J Pharm Pract. 2012;25:13.
13. West D, Marasco L. The breastfeeding mother’s guide to making more milk. Available from: http://www.alhadapedia.com/hospen/Edu/PDFbks/BreastfeedingMoth.pdf2014.
14. Paritakul P, Ruangrongmorakot K, Laosooksathit W, Suksamarnwong M, Puapornpong P. The effect of ginger on breast milk volume in the early postpartum period: a randomized, double-blind controlled trial. Breastfeed Med. 2016;11(7):361–365. doi:10.1089/bfm.2016.0073
15. Damanik R. Torbangun (Coleus amboinicus Lour): a Bataknese traditional cuisine perceived as lactagogue by Bataknese lactating women in Simalungun, North Sumatera, Indonesia. J Hum Lact. 2009;25(1):64–72. doi:10.1177/0890334408326086
16. Rajith NP, Navas M, Thaha AM, et al. A study on traditional mother care plants of rural communities of South Kerala. Indian J Tradit Knowl. 2010;9(1):203–208.
17. Bruckner C A survey on herbal galactogogues used in Europe.
18. Othman N, Lamin RAC, Othman CN. Exploring behavior on the herbal galactagogue usage among Malay lactating mothers in Malaysia. Procedia Soc Behav Sci. 2014;153(SupplementC):199–208. doi:10.1016/j.sbspro.2014.10.054
19. Mahasan AS, Tengku Azhar TN, Abdul Rahim N, Abdul Ghani R. Knowledge and practice of galactogogues consumption among breastfeeding mothers in Pahang. IJCWED. 2019;7:38–44.
20. Institute P. Penang Statistics Quarter 4. Penang, Malaysia: Penang Institute; 2016.
21. Daniel W. Biostatistics: A Foundation for Analysis in the Health Sciences.
22. StataCorp. Stata Statistical Software: Release 13. College Station, TX: StataCorp LP [computer program]; 2013.
23. Sim TF, Sherriff J, Hattingh HL, Parsons R, Tee LB. The use of herbal medicines during breastfeeding: a population-based survey in Western Australia. BMC Complement Altern Med. 2013;13(1):1–10. doi:10.1186/1472-6882-13-317
24. Bazzano AN, Cenac L, Brandt AJ, Barnett J, Thibeau S, Theall KP. Maternal experiences with and sources of information on galactagogues to support lactation: a cross-sectional study. Int J Womens Health. 2017;9:105–113. doi:10.2147/IJWH.S128517
25. Moriello C, Paterson JM, Reynier P, et al. Off-label postpartum use of domperidone in Canada: a multidatabase cohort study. CMAJ Open. 2021;9(2):E500–E509. doi:10.9778/cmajo.20200084
26. Mehrabadi A, Reynier P, Platt RW, Filion KB. Domperidone for insufficient lactation in England 2002–2015: a drug utilization study with interrupted time series analysis. Pharmacoepidemiol Drug Saf. 2018;27(12):1316–1324. doi:10.1002/pds.4621
27. Reddy G, van Dam RM. Food, culture, and identity in multicultural societies: insights from Singapore. Appetite. 2020;149:104633. doi:10.1016/j.appet.2020.104633
28. Sim TF, Hattingh HL, Sherriff J, Tee LBG. Perspectives and attitudes of breastfeeding women using herbal galactagogues during breastfeeding: a qualitative study. BMC Complement Altern Med. 2014;14(1):216. doi:10.1186/1472-6882-14-216
29. Zizzo G, Amir LH, Moore V, Grzeskowiak LE, Rumbold AR. The risk-risk trade-offs: understanding factors that influence women’s decision to use substances to boost breast milk supply. PLoS One. 2021;16(5):e0249599. doi:10.1371/journal.pone.0249599
30. Chew KS, Tan TW, Ooi YT. Influence of Chinese cultural health beliefs among Malaysian Chinese in a suburban population: a survey. Singapore Med J. 2011;52(4):252–256.
31. Withers M, Kharazmi N, Lim E. Traditional beliefs and practices in pregnancy, childbirth and postpartum: a review of the evidence from Asian countries. Midwifery. 2018;56:158–170. doi:10.1016/j.midw.2017.10.019
32. Foong SC, Tan ML, Foong WC, Marasco LA, Ho JJ, Ong JH. Oral galactagogues (natural therapies or drugs) for increasing breast milk production in mothers of non‐hospitalised term infants. Cochrane Database Syst Rev. 2020;5(5). doi:10.1002/14651858.CD011505.pub2
33. Anderson PO. Potentially toxic foods while breastfeeding: garlic, caffeine, mushrooms, and more. Breastfeed Med. 2018;13(10):642–644. doi:10.1089/bfm.2018.0192
34. Saejueng K, Nopsopon T, Wuttikonsammakit P, Khumbun W, Pongpirul K. Efficacy of Wang Nam Yen herbal tea on human milk production: a randomized controlled trial. PLoS One. 2022;17(1):e0247637. doi:10.1371/journal.pone.0247637
35. Fungtammasan S, Phupong V. The effect of Moringa oleifera capsule in increasing breastmilk volume in early postpartum patients: a double-blind, randomized controlled trial. PLoS One. 2021;16(4):e0248950. doi:10.1371/journal.pone.0248950
36. The Academy of Breastfeeding Medicine Protocol Committee. ABM Clinical Protocol #9: use of galactogogues in initiating or augmenting the rate of maternal milk secretion (First Revision January 2011). Breastfeed Med. 2011;6(1):41–49. doi:10.1089/bfm.2011.9998
37. Tan ML, Foong SC, Ho JJ, Foong WC, Mohd R, Harun Z. Postpartum women’s perception of antenatal breastfeeding education: a descriptive survey. Int Breastfeed J. 2020;15(1):85. doi:10.1186/s13006-020-00328-2
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.