")
Back to Journals » Clinical Interventions in Aging » Volume 18
Use of Electronic Medical Records (EMR) in Gerontology: Benefits, Considerations and a Promising Future
Authors Bednorz A , Mak JKL , Jylhävä J, Religa D
Received 29 June 2023
Accepted for publication 5 November 2023
Published 23 December 2023 Volume 2023:18 Pages 2171—2183
DOI https://doi.org/10.2147/CIA.S400887
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Prof. Dr. Nandu Goswami
Adam Bednorz,1,2 Jonathan KL Mak,3 Juulia Jylhävä,3,4 Dorota Religa5,6
1John Paul II Geriatric Hospital, Katowice, Poland; 2Institute of Psychology, Humanitas Academy, Sosnowiec, Poland; 3Department of Medical Epidemiology and Biostatistics, Karolinska Institutet, Stockholm, Sweden; 4Faculty of Social Sciences (Health Sciences) and Gerontology Research Center (GEREC), University of Tampere, Tampere, Finland; 5Division of Clinical Geriatrics, Department of Neurobiology, Care sciences and Society, Karolinska Institutet, Stockholm, Sweden; 6Theme Inflammation and Aging, Karolinska University Hospital, Huddinge, Sweden
Correspondence: Dorota Religa, Department of Neurobiology, Care Sciences and Society (NVS), Karolinska Institutet, H1 Neurobiologi, vårdvetenskap och samhälle, H1 Klinisk geriatrik Religa, Stockholm, 171 77, Sweden, Tel +46 724698503, Fax +46 08-31 11 01, Email [email protected]
Abstract: Electronic medical records (EMRs) have many benefits in clinical research in gerontology, enabling data analysis, development of prognostic tools and disease risk prediction. EMRs also offer a range of advantages in clinical practice, such as comprehensive medical records, streamlined communication with healthcare providers, remote data access, and rapid retrieval of test results, ultimately leading to increased efficiency, enhanced patient safety, and improved quality of care in gerontology, which includes benefits like reduced medication use and better patient history taking and physical examination assessments. The use of artificial intelligence (AI) and machine learning (ML) approaches on EMRs can further improve disease diagnosis, symptom classification, and support clinical decision-making. However, there are also challenges related to data quality, data entry errors, as well as the ethics and safety of using AI in healthcare. This article discusses the future of EMRs in gerontology and the application of AI and ML in clinical research. Ethical and legal issues surrounding data sharing and the need for healthcare professionals to critically evaluate and integrate these technologies are also emphasized. The article concludes by discussing the challenges related to the use of EMRs in research as well as in their primary intended use, the daily clinical practice.
Keywords: electronic medical records, gerontology, artificial intelligence, geriatrics, aging
Introduction
Older adults have a higher incidence of chronic conditions, and they are also at a higher risk of experiencing adverse health events, such as falls and infections.1 Health information technology has the potential to improve care for older patients by enabling appropriate diagnosis, disease risk monitoring, and prevention, with the transition to computer-based patient records seen as essential for modern healthcare.2,3 A previous systematic review revealed various types of technological solutions that have been the focus of research in gerontology, including telecare (which is the most common), electronic medical record (EMR), decision support systems, web-based packages for patients and their families, and assistive information technology.2 EMRs are digital versions of patient’s medical records, which contain dynamic information about their medical history, diagnoses, treatment, and health care data.2 EMRs are more than a simple representation of paper documentation because of their multi-domain characteristics. EMRs are designed to facilitate efficient storage, retrieval, and sharing of patient information between providers. The terms EMR and electronic health record (EHR) are often used interchangeably; EMR refers to a digital patient record within a healthcare provider’s office, containing human and machine-generated data, offering instant access and efficient tracking, while EHR encompasses information from multiple medical investigators, enabling sharing among clinicians and researchers across hospitals to enhance disease understanding and study underlying causes.4
The purpose of this article was to review the EMRs literature with a focus on the advantages, weaknesses and issues related to their use in the future with the aid of technological advancements. It is a narrative type of review. Due to the diversity of the literature in this area, each section is presented from the perspective of scientific research and clinical practice. Based on an analysis of the literature on EMRs, we concluded that machine learning (ML) and artificial intelligence (AI) are increasingly being applied in this area. For this reason, we decided to include it in our review. It is hoped that this expanded coverage of the topic of EMRs will show important subject areas, be useful in designing future research in the field of gerontology and guidelines to improve care of older patients. Review can be useful for many healthcare and IT professionals who plan to conduct research using EMRs, intend to create/implement new EMRs systems or plan to evaluate existing ones. A chronology of selected events relevant to the two perspectives is presented in Figure 1.3,5–14 The recipient of EMR, ie, the older patients, is also considered.
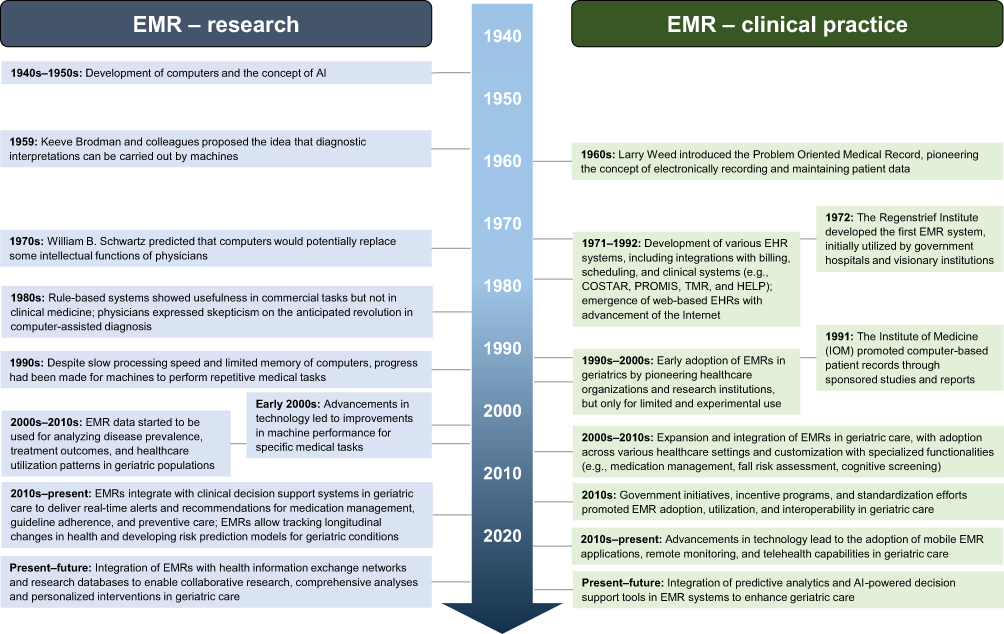 |
Figure 1 Evolution of electronic medical records in research and clinical practice.3,5–14 |
Benefits – Research
Applications of EMRs in Research
EMRs data generated during patient care can be used to support research in several ways (Figure 2).9,15 Studies using EMRs have analyzed various somatic conditions of older patients including frailty syndrome,16–18 type 2 diabetes,19 dementia,20,21 and falls.22 Table 1 lists the selected articles that demonstrate the use of EMRs in different areas, including diagnosis of specific diseases, pharmacology, and clinical decision support.17,23–29 Notable in the literature review is the large number of retrospective studies using the already collected EMR datasets.24,28,30,31 There are also numerous pilot studies most often aimed at improving EMR-based diagnostics.16,29,32
 |
Figure 2 Summary of benefits and limitations of using electronic medical records.2,3,5–14,16,33 |
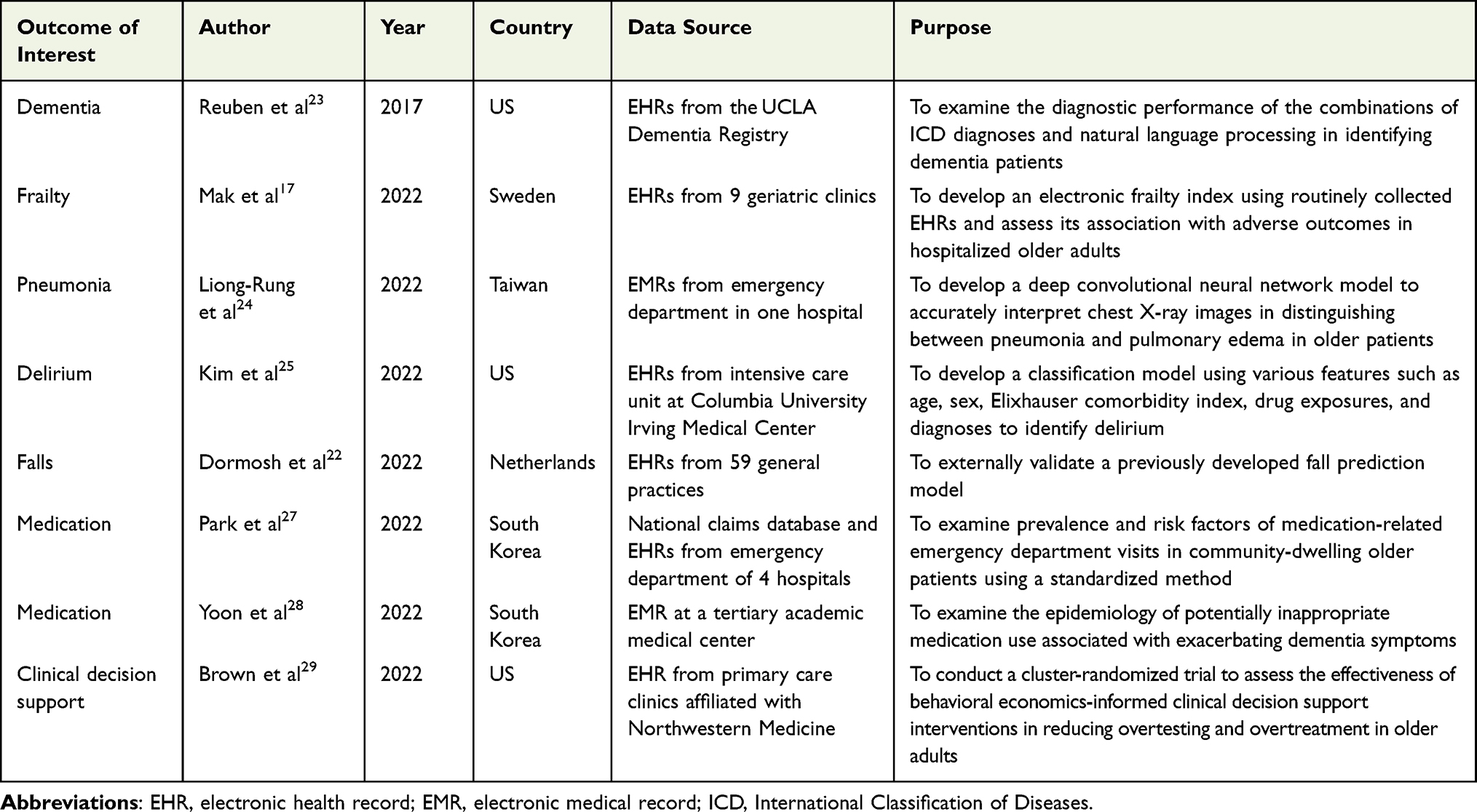 |
Table 1 Selected Studies Using EMRs Along with a Brief Overview |
EMRs offer rich resources and opportunities to improve research (and clinical care), especially for undiagnosed dementia. Structured EMR data (eg, diagnostic and procedural codes and laboratory values) have been used in population-based research, which can be used in identifying specific patient characteristics, conducting surveillance, and estimating dementia risk.34 Many research consortia, including the Electronic Medical Records and Genomics Network (eMERGE), have used EMRs to construct and identify dementia phenotypes.35 In older population, both dementia and depression are common, and identifying these conditions still remains a challenge. These sources are made available in many countries, and information is collected for research purposes and for epidemiological studies.12,33 EMRs contain rich data on health and sociodemographic variables, making them promising sources for generating simpler scores such as the electronic frailty index (eFI).36 In the field of gerontology, new insights from old data may prove valuable in identifying risk factors for conditions and in improving diagnostics and treatment. Analysis of routine data can be used to develop prognostic tools to identify future risk of events.12 For example, the Hospital Frailty Risk Score offers a cost-effective and systematic approach to screen for frailty, enabling the identification of high-risk patients who may benefit from a frailty-focused approach.16 Validation study have demonstrated that patients with higher frailty risk, as determined by the Hospital Frailty Risk Score, have increased 30-day mortality, longer hospital stays and higher readmission rates, although the score’s ability to differentiate outcomes at the individual level is limited.16 This initial identification, however, can be useful in making decisions about follow-up care. Updating clinical data also allows for regular validation of prognostic models with current health status and population demographics (an example is the Q-Ris version of the cardiovascular risk calculator).37 EMRs generate new and additional information.
To address clinical uncertainties and answer research questions, different approaches in clinical decision-making across diseases can be explored.7,12 This can be achieved through evaluation design, cohort trials or cluster randomization, in which general practices contributing to routine datasets are randomly assigned to intervention or control groups. Additionally, assessing critical health indicators associated with aging, such as frailty or dementia, during the recruitment phase and comparing them to population-level data can enhance the applicability of study findings.12 Moreover, by combining surveys with EMR data, less burdensome monitoring of study endpoints becomes possible, allowing for longer and more meaningful follow-up periods for decision-making.38 People aged over 85, with frailty syndrome or dementia, from ethnic minorities or living in poor areas are often underrepresented in studies. Many older patients may drop out of the study for a variety of reasons (eg, poor health, high number of visits to specialists that limit their ability to participate in other research projects, social factors). The aforementioned variables can affect the results of ongoing studies and limited options in recruiting participants can lead to errors in analyses.12 The utilization of routine data with consent at the general practice level can significantly mitigate this type of selection bias. Older patient at any stage should be able to change decision to share data for research purposes.12
The cost of routine data collection is also lower; in addition, routine data offer precise records of prescriptions over a lifetime (there is still a demand to obtain reliable data on the benefits and effects of drugs in the older patients, where multimorbidity, polypharmacy and frailty syndrome are common).12
Machine Learning Algorithms in EMRs Data
The use of AI for EMR analysis is increasing.39,40 AI tools, which include ML, are technologies for analyzing data, catching hidden information, identifying risk factors and giving suggestions for diagnosis.8 In ML, input data are provided along with expected results (supervised learning - one of the types of ML). The algorithm learns the relationship between the input data and the corresponding output variables (eg, disease identification); after the learning process, the algorithm can give a classification or prediction after new input data.41,42 The number of citations referencing ML in PubMed significantly grew from 358 in 2008 to 3543 in 2017, and surpassed 3700 within the first three quarters of 2018.15 ML algorithms are used for classification or prediction, which translates into clinical applications related to diagnosis and prognosis.43 ML has been used in dementia research, including neuroimaging studies and biomarkers (which are not routinely available in EMRs).33,44 Although most studies are currently limited to diagnosing dementia, analyses related to identifying other geriatric syndromes or behavioral symptom patterns in dementia are emerging. Approaches using ML require further research in diagnosing mental health problems in older adults.33 In addition to validated tools that assess a patient’s cognitive function, a model that uses retrospective EMRs data to identify delirium (where age, sex, Elixhauser comorbidity index, drug exposure and diagnoses were used as features) may be useful.25 One study developed a keyword scale for semi-automated detection of delirium using natural language processing (NLP) of clinical notes from EMRs, which presented a new diagnostic instrument.32
The use of ML and deep learning (a more advanced form of ML) can also contribute to better symptom detection and disease classification, which has the potential to improve the diagnostic and decision-making process and reduce the cost of medical care.10,45 Deep learning has been used for clinical decision support in the diagnosis of various diseases,8 due to the fact that it effectively handles unstructured and ambiguous data,46 including diabetic retinopathy,47 skin cancer,48 and dyspnea in older patients.24 ML has also been used to predict future oxygen demand in patients with Covid-19 infection using inputs of vital signs, laboratory data and chest X-rays.49 It has also found application in identifying abuse.50 In addition to systems focused on collecting and codifying data, new forms of technology can use data that is both human-generated and machine-generated.8
EMRs contain diverse information categorized as structured (eg, diagnoses, prescriptions) and unstructured free text (eg, medical status). NLP techniques are commonly used to analyze and extract information from the unstructured data, enabling the development of classification and prediction models for conditions like dementia. Combining structured and unstructured EMR data using ML approaches has shown promise in gerontology research, including mortality prediction and diagnosing geriatric syndromes such as delirium.32,33,44
Benefits – Clinical Practice
EMRs offer numerous advantages, including comprehensive medical records, improved communication with healthcare providers, remote data access, and quick retrieval of test results and personal records (Figure 2). This leads to increased efficiency, enhanced patient safety, improved adherence to guidelines, reduced medication errors, and improved quality of care in gerontology, with benefits such as decreased medication use, better patient history taking and physical examination assessments and improved documentation of the patient’s condition.5,51–53
Family physicians can be more effective in managing dementia treatment by having care guidelines that are integrated within EMRs and they can thus also better meet the needs of the caregiver and patient.20 Hospital EMRs can be useful in evaluating outpatient prescriptions54 and facilitate the care of dementia patients with pain complaints.55 The introduction of EMRs in nursing homes has improved communication between providers, consultants, the hospital and nursing home staff.56 The use of EMRs can also be useful when it comes to monitoring trends including estimates of diagnosis rates (underdiagnosis vs overdiagnosis), prescribing and hospital admissions.57 Routine data can provide valuable insights into the performance of clinical services compared to benchmarks, informing quality improvement projects at the regional level and guiding service design and policy changes at the national level.12,58
The use of EMRs can be beneficial in areas such as documentation, care co-ordination, patient engagement, automation, checklists, next-step guidance, avoidance of redundancy, and expanded differential diagnoses.12,59 Research data indicate that the use of EMRs improves performance on various quality indicators compared to practices that use paper documentation. However, it is important to emphasize that post-improvement quality requires more than just an electronic record.60 EMRs can be useful in improving the measurement and analysis of clinical performance metrics, assuming the system is properly configured, data fields are accurately populated, and the software application is sophisticated enough to support the measurement and reporting process.9 Computerized systems integrated with EMRs, such as those for identifying drug interactions and providing clinical decision support, hold promise for improving patient care and safety.61
Considerations and Challenges – Research
The use of EMRs allows for the analysis of large amounts of healthcare data, which can be valuable for epidemiological research, such as studying hospitalization trends at population level.62 However, evaluations of these data may cause problems (Figure 2). Typical medical research methodology often involves redundant data entry into EMRs in healthcare and research. The appropriate data transcription that this methodology requires increases the burden on clinical researchers and practitioners.19
AI and ML have shown promise in interpreting medical images for radiographs, CT scans, skin and retinal images.8,63 However, insufficient evidence exists for successful implementation of ML and deep learning in clinical care, raising concerns about safety, data quality and ethical considerations.8,64–66 ML methods require a large amount of data to train; data preprocessing is another challenge, as dealing with missing values and improving quality (eg, improving image quality is very labor-intensive).4 It is also important to consider the potential errors that may arise when using ML algorithms.8 Although a human EMR user can manually exclude erroneous values when checking trends, most automated analyses cannot do so, which can distort averages or undermine the validity of records of specific parameters (eg, body weight).67 Important information (eg, the dose of a particular drug) may be missed from the collected data due to lack of routine recording. Some conditions may not be routinely recorded in clinical care (eg, physical disabilities) or may be recorded insufficiently (eg, dementia); omission or insufficient counting of such information in studies may lead to incorrect conclusions. In addition, routinely collected data may contain information relevant to clinical or administrative but not research purpose.12 Concerns about AI are greater than before, which is related to the colloquial expression “garbage in, garbage out” which is used to refer to the poor performance of ML models when the data they learn from is low quality.14,68 Recent analyses show that the tools used to construct algorithms may tend to exclude the interests and values of older people and contribute to reinforcing ageism.69 A recent World Health Organization (WHO) paper titled “Ageism in artificial intelligence for health” examines the use of AI in medicine and public health in relation to older people, including conditions under which AI may exacerbate or introduce new forms of ageism.70 The MIT AGELAB report found that despite an optimistic outlook on the capabilities of AI systems, experts interviewed about the benefits of AI for the aging population were least confident in AI’s ability to provide more equitable access to health care. They pointed out that any system that replaces humans with an algorithm has the potential to make erroneous decisions that could jeopardize human health. It is increasingly indicated that AI in medicine is viewed too optimistically about the technology’s potential to prevent or treat disease.14 There are only a few certified and even fewer clinically validated tools available in clinical settings. Hence, many experts suggest caution in estimating the real effects of this technology on the future of health care for older adults.14
In the field of geriatrics, few studies have compared ML approaches with previously used statistical methods.33 A study by Park et al found that the predictive performance of ML techniques (random forest and support vector machines) was superior to logistic regression in predicting Alzheimer’s dementia.71 A study by Ford et al observed similar performance of ML techniques (random forest, naive Bayes classifier and logistic regression) in dementia classification.72 ML demonstrates superior accuracy compared to statistical methods in predicting various adverse outcomes in older adults, such as acute kidney injury,73 functional fall risk,74 delirium,75 and overall risk of emergency admission.76 These ML algorithms hold the potential to provide a more comprehensive and precise assessment of aging effects, physical illnesses, and fall risk in older populations, enabling earlier intervention for those at the highest risk. This area, however, requires further empirical verification.10,14
Considerations – Clinical Practice
The widespread adoption of EMRs in the late 20th century faced challenges such as high costs, data entry errors, and initial resistance from physicians (Figure 1). During transitional periods of EMRs implementation, discrepancies between paper and electronic documentation can arise, potentially affecting patient care quality and necessitating audits.77
While the introduction of EMRs aimed to improve clinical practice, simplify quality assurance, and enhance data collection, some goals have not been fully met. Issues like data duplication, difficulty in extracting relevant information, and delayed entry of notes into EMRs have been reported (and many clinicians do not believe that EMRs save time).7,61,78 Despite positive impacts on clinical processes, such as improved assistance and health parameter monitoring, there are mixed findings regarding EMRs’ association with healthcare quality improvement and physician satisfaction.2
EMRs and Medical Staff
Although a review of studies on the use of EMRs in geriatrics indicates that the use of EMRs had a positive impact on clinical processes (including improved assistance, fall detection, and monitoring of health parameters), it should be noted that other indicators were less frequently evaluated. Results were generally positive, except for physician satisfaction.2 A systematic review showed that in most studies (3/4; 75%), EMRs were not consistent with current values, professional practices, and the needs of patients and clinicians.2 EMRs were found to be easy to use in only half of the studies (3/6; 50%). In terms of implementation, half of the studies negatively evaluated the ability to try/test them (3/6; 50%).2
Previous research has overlooked the variation in effects of different implementation sequences of EMRs on medical personnel behavior, data recording timing, and import process complexity. Additionally, there is inconsistent evidence on the association between EMRs implementation and healthcare quality improvements, especially across different hospital levels.79 Effective collaboration in modern, team-based healthcare requires designing and implementing EMRs systems that consider the capabilities and limitations of all team members.3
The expansion of time spent with EMRs has correlated with a dramatic decrease in clinicians’ time spent at the bedside, an increase in computer-assisted work, and rising rates of burnout.80 In the case of EMRs, some of the words in the description are duplicated from previous documentation.81 Card review, electronic distractions like clinical decision support alerts, and messages from other staff members can further exacerbate clinicians’ fatigue, increasing errors in patient care and causing professional burnout.82 Data showed that physicians spend about two-thirds of their work time interacting with EMRs in their offices.83 The imposition of technology onto clinical workflows has created challenges for healthcare professionals, who perceive a lack of meaningful impact on patient care despite the effort invested in data entry.3 For this reason, more and more facilities are hiring medical assistants to help navigate the EMRs. Assigning EMR-related work to other team members can allow physicians to focus more on diagnosis, treatment, and building relationships with patients.11 The Covid-19 pandemic has only exacerbated the digital work of clinicians, including increased use of telemedicine, increasing patient messaging.84
In the context of EMRs, it is important to tailor them to the user and educate the user on how to use EMRs.85,86 It is necessary to find a balance between a state of information overload and appropriate (and helpful) information.87 Reports considering the use of EMRs increasingly specify recommended strategies to help transform technology from a tool that captures information to one that generates knowledge useful in guiding and supporting patient care. Such coordination requires that health professionals receive training in the use of information technology.88 Physicians are often optimistic about the future benefits of EMRs but are frustrated by unintuitive and multiclickable interfaces and cumbersome data retrieval in existing EMRs.89 The procedure for extracting specific information from large amounts of data is still tedious and time-consuming.4 While physician satisfaction with EMR technology is generally positive, the transition to electronic records has had a negative impact on clinician wellness. In the absence of physicians during EMRs implementation meetings, the burden of regulatory requirements was shifted back to them, exacerbating the already burdensome “click” workload.2,3 This highlights the need for better alignment between technology and clinical workflow to alleviate physician burden and improve efficiency. Other studies indicate that EMRs implementation may lead to reduced communication between medical staff (eg, physician - nurse), potentially negatively affecting patient care and increasing the likelihood of incomplete documentation.61
The findings confirm that there is no one-size-fits-all solution. Clinicians and healthcare managers need to carefully select the type of EMRs that will be most appropriate based on the needs of their organization and clients.90 While choosing the right software seems essential, it is also important to fit it into the overall organizational system.91 If EMRs are difficult to use (eg, too many reminders or excessive information complexity), they can create barriers to their use.11
Ethical Concerns
The use of EMR raises the risk of potential breaches in patient confidentiality, highlighting ethical concerns related to data control, ownership, accountability, informed consent, and security in EMRs implementation.7,12,92 These concerns may be greater if the patient has cognitive impairment. European Union regulations emphasize the need for unambiguous consent, clear information about withdrawal of consent, and pseudonymization of routine data to ensure secure separation from additional identifying information.93 Institutions must also review datasets to mitigate the risk of disclosure, while researchers involved in data analysis are increasingly required to undergo accredited training in appropriate data storage practices.12
The need for standardized EMRs data is being recognized, encompassing areas, such as population data, decision support, and data exchange.7 The lack of interoperability protocols among different EMRs systems hampers information exchange among healthcare professionals, while the presence of diverse EMRs systems and mixed electronic-paper environments limits the full potential of EMRs for collaboration and care coordination. National and regional regulations are necessary to establish EMRs interoperability standards.9 Efforts are underway to interconnect shared healthcare records and standardize terminology and representation across data systems.12
The Older Patients as the EMRs Recipients
The widespread use of EMRs by hospitals is creating opportunities for patients to access clinical data and actively participate in their care through the EMRs.12 The increase in the implementation of patient portals is due in part to some preliminary evidence that they can improve patient engagement and health outcomes (including medication adherence).6 Patient-accessible electronic health records (PAEHRs) are being implemented around the world.6,94 Although the older patients may feel resistance to digital technology, they benefit from the services of the system, which is based on EMRs.95 With the increasing aging and digitization of societies, the needs of the older adult population in terms of using health-related information systems are being taken into account.96,97 Among the solutions used, an online health record available to the patient and family has been introduced (it has been suggested that such a solution could become a useful tool for sharing health information), and patients have been monitored for the long-term impact of PAEHRs on their communication with health care professionals and engagement in the care process.98 Nurgalieva et al analyzed patients’ views on sharing their health data through PAEHRs and found that older patients and patients with lower levels of education were more likely to share their data.99 Eriksson-Backa et al evaluated older adults’ experiences of using the PAEHR portal and other electronic health services and found that improvements in security, usability, and additional information and features could increase effective use.100 Another study found that patient-provider collaboration promotes the use of apps dedicated to older adults and empowers them to lead healthy lifestyles.101
Future – Research
Technological advancements in geriatrics, necessitate the involvement of biomedical informatics specialists to leverage clinical data for improved patient care. The integration of electronic healthcare data, including genetic data and wearable technology, offers opportunities for personalized healthcare, but challenges, such as data complexity and ethical considerations must be addressed.8,12,49,102 Careful consideration of data representativeness and potential biases is crucial when utilizing EMR databases for research purposes.21,103,104 Research questions on already diagnosed diseases (retrospective EMRs data) remain relatively new and involve significant methodological challenges. Developing research questions that can be answered with routine EMRs data should be done in a dialogic format and with an interdisciplinary team (data analysts, clinicians and social care professionals). An example is the Ageing Data Research Collaborative (@geridata),12 which was created for mutual collaboration among researchers to develop pre-analytic protocols, code lists for conditions relevant to geriatric medicine and gerontology, data coding and analysis.105
AI and ML have the potential to simplify and accelerate clinical trials through more efficient recruitment and matching of study participants and more comprehensive data analysis.8 In addition, it is possible to create synthetic control groups by matching historical data to target criteria for a given study. It seems possible that AI could generate “synthetic patients” to simulate diagnostic or therapeutic outcomes. AI and ML could also be used to better predict and understand possible adverse events.8,106,107 The demand for continuous monitoring and timely diagnosis in geriatric care drives the adoption of technological solutions for efficient, personalized, and cost-effective healthcare. The ability to share and utilize data for generating knowledge has the potential to significantly improve healthcare in the geriatric field. The integration of AI and ML algorithms as clinical tools could aid in accurate diagnosis by analyzing vast amounts of clinical, genomic, metabolic, and environmental data, potentially serving as a physician’s personal scribe and optimizing time spent with patients.8,12 However, healthcare professionals should critically evaluate the proposals offered, integrate ML into multidisciplinary meetings, and additionally learn new skills in statistics and programming to help develop clinical algorithms and evaluate them in routine clinical practice.10 Currently, international efforts are being made to regulate AI, guidelines are being developed, and policy recommendations are being made on aspects of fairness, accountability, transparency to meet the reliability criteria for AI systems (eg, the European Artificial Intelligence Act). The outcome and implementation of these regulations, especially in the healthcare sector, will present additional challenges yet to come.14
Future – Clinical Practice
EMR safety concerns about both the technology and its use are likely to persist into the future.7 Infrastructure will need to be continually adapted to monitor and learn from adverse events and errors.108 Reducing documentation burden can improve clinical workflow. Adopting a digital minimalism framework can inspire critical analysis of the need for compliance and reimbursement documentation that makes the difference. Digital minimalism can be effective when used as a framework to guide the health system’s relationship with technology.11 The current approach focused on accepting each additional form of technology without considering the cumulative impact. While there is acknowledgment of the importance of incorporating social and behavioral determinants of health data into the EMRs, there is concern about the additional documentation burden it may impose on an already overwhelmed healthcare workforce.3 Change will never lead to a sustainable relationship with digital technology if the basic philosophy of technology use remains maximalist.11 EMR use is influenced by both physical (computers) and logical (ie, ease of use) accessibility. IT professionals should become part of healthcare teams, and new technologies should be tested through realistic and simulated environments for improvement before implementation into daily clinical practice.109,110 Research data indicate that in order to maximize success in the area of EMRs implementation, it is necessary to identify the best methods for integrating EMRs into clinicians’ routine workflows. Proper implementation of an electronic system requires education. It is important to provide timely support to staff, document problems with the system, and provide prompt feedback.2,7
It is also necessary to define the role of AI as a tool to assist rather than replace medical personnel.8 Adequate training and skill development are key to ensuring that medical personnel are able to effectively use advanced technologies to improve the quality of care. Advancements in AI offer our healthcare system a choice: utilizing AI-based care to increase hourly revenue or leveraging AI-based care to free up time and empower physicians to provide more accurate and thoughtful patient care.111
As technology is integrated into healthcare practice, it is important to understand how technology shapes communication to identify changes in practice that may be warranted to ensure safe and effective patient care.61 Future research on communication should analyze not only how it is used, but also how it is optimized to achieve better outcomes for patients (effectiveness of various communication functions - information sharing, decision making, emotional support).9,112 The implementation of EMRs and AI in geriatric care offers benefits in managing patient information and facilitating communication, but it is crucial to ensure that the human factor and empathy in patient interactions are not compromised. Physicians should have sufficient time to spend with patients, providing personalized care, understanding and empathy. The human element in healthcare remains indispensable and should be considered alongside the integration of new technologies.8,11
Limitations
There is a notable imbalance in the literature, with more studies focusing on the diagnostic use of EMRs data and fewer examining the daily workflow and interdisciplinary teamwork in geriatric departments. However, this is our subjective impression and would need to be verified by a systematic review. Besides, it should be noted that the field of EMRs is very broad, and for future review articles, it would be beneficial to focus more on the specific thematic sections, such as diseases (ie, only dementia), ML algorithms, or technological issues related to the implementation and use of EMRs in daily clinical practice. Typically, publications that showed positive results dominated over those that showed negative results, and thus, some caution should also be exercised in evaluating studies on EMRs.
Conclusion
EMRs data generated during care of older patients can be used to support clinical research and quality improvement. The literature provides evidence for the use of EMRs in research and describes their impact on everyday clinical practice. In both areas, the use of EMRs presents opportunities as well as limitations that need to be addressed and further empirical verification. In answering the question of whether the advantages from the use of EMRs outweigh the limitations (Figure 2), it is important to keep in mind the individual perspective of the person who uses them (researcher, physician at the hospital, etc.). In this context, the scales may tilt in different directions. However, it seems important to look at EMRs from the perspective of a process (Figure 1) – a process that is still ongoing and that creates new opportunities.
An analysis of the literature has shown that this area lies at the intersection of medicine and informatics. Therefore, both in the area of improving daily clinical practice and in the implementation of scientific research, interdisciplinary teams are necessary.12 Utilizing the experience of various professionals in using EMRs will be key to the successful implementation of appropriately designed medical information management technology. In the context of today’s healthcare, which relies on multiple professionals working as a team, the design and implementation of EMRs management systems must take into account the needs and opinions of all team members, rather than focusing solely on one professional group.3
EMRs are becoming more common around the world, fostering greater interoperability and facilitating the exchange of patient information between medical facilities, in line with the growing global trend toward integrated digital health systems. It should be noted, however, that access to EMRs can be hampered by varying regulations at the state and international levels, as well as differences in national laws. Medical institutions and government agencies are recognizing EMRs in shaping better healthcare models, however, there are still serious concerns about the privacy and security of this data. As EMRs become more widespread, procedural, social, ethical and compliance issues and data security have begun to be addressed in addition to purely technical aspects.7
Our goal was to assess the capabilities as well as the limitations of EMRs. Despite detailing the area of clinical research and daily clinical practice for the purpose of clarity in the article, EMRs bridge the gap between these areas. In the future, it may be useful to develop the development of core outcome sets that are relevant to older adults, as well as patient self-reported outcomes, in a way that can be implemented into daily routine clinical practice. Such initiatives would aim to incorporate the results of big data research into common medical practice, improve the quality of the data collected, and raise awareness of the potential of big data research in the design of health services. In addition, policy maker engagement is key to increasing public awareness of the utility and uses of data to improve the quality of health care. This, in turn, is a key part of the contract of trust between the public and those who control access to health data.7,12
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
Juulia Jylhävä was supported by the Swedish Research Council (grant no. 2018–02077), the Academy of Finland (grant no. 349335), the Sigrid Jusélius Foundation and the Instrumentarium Science Foundation.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Age UK. Briefing: Health and Care of Older People in England 2017; 2017.
2. Vedel I, Akhlaghpour S, Vaghefi I, Bergman H, Lapointe L. Health information technologies in geriatrics and gerontology: a mixed systematic review. J Am Med Informatics Assoc. 2013;20(6):1109–1119. doi:10.1136/amiajnl-2013-001705
3. Johnson KB, Neuss MJ, Detmer DE. Electronic health records and clinician burnout: a story of three eras. J Am Med Informatics Assoc. 2021;28(5):967–973. doi:10.1093/jamia/ocaa274
4. Latif J, Xiao C, Tu S, Rehman SU, Imran A, Bilal A. Implementation and Use of Disease Diagnosis Systems for Electronic Medical Records Based on Machine Learning: a Complete Review. IEEE Access. 2020;8:150489–150513. doi:10.1109/access.2020.3016782
5. Campanella P, Lovato E, Marone C, et al. The impact of electronic health records on healthcare quality: a systematic review and meta-analysis. Eur J Public Health. 2015;26(1):60–64. doi:10.1093/eurpub/ckv122
6. Dendere R, Slade C, Burton-Jones A, Sullivan C, Staib A, Janda M. Patient Portals Facilitating Engagement With Inpatient Electronic Medical Records: a Systematic Review. J Med Internet Res. 2019;21(4):e12779–e12779. doi:10.2196/12779
7. Evans RS. Electronic Health Records: then, Now, and in the Future. Yearb Med Inform. 2016;Suppl 1(Suppl 1):S48–S61. doi:10.15265/IYS-2016-s006
8. Haug CJ, Drazen JM. Artificial Intelligence and Machine Learning in Clinical Medicine, 2023. N Engl J Med. 2023;388(13):1201–1208. doi:10.1056/nejmra2302038
9. Janett RS, Yeracaris PP. Electronic Medical Records in the American Health System: challenges and lessons learned. Cien Saude Colet. 2020;25(4):1293–1304. doi:10.1590/1413-81232020254.28922019
10. Mukaetova-Ladinska EB, Harwood T, Maltby J. Artificial Intelligence in the healthcare of older people. Arch Psychiatry Ment Heal. 2020;4(1):7–13. doi:10.29328/journal.apmh.1001011
11. Singh N, Lawrence K, Sinsky C, Mann DM. Digital Minimalism — an Rx for Clinician Burnout. N Engl J Med. 2023;388(13):1158–1159. doi:10.1056/nejmp2215297
12. Todd OM, Burton JK, Dodds RM, et al. New Horizons in the use of routine data for ageing research. Age Ageing. 2020;49(5):716–722. doi:10.1093/ageing/afaa018
13. Uslu A, Stausberg J. Value of the Electronic Medical Record for Hospital Care: update From the Literature. J Med Internet Res. 2021;23(12):e26323. doi:10.2196/26323
14. Stypińska J, Franke A. AI revolution in healthcare and medicine and the (re-)emergence of inequalities and disadvantages for ageing population. Front Sociol. 2023;7:1038854. doi:10.3389/fsoc.2022.1038854
15. Peltan ID, Beesley SJ, Brown SM. Can Big Data Deliver on Its Promises?—Leaps but Not Bounds. JAMA Netw Open. 2018;1(8):e185694. doi:10.1001/jamanetworkopen.2018.5694
16. Gilbert T, Neuburger J, Kraindler J, et al. Development and validation of a Hospital Frailty Risk Score focusing on older people in acute care settings using electronic hospital records: an observational study. Lancet. 2018;391(10132):1775–1782. doi:10.1016/S0140-6736(18)30668-8
17. Mak JKL, Hägg S, Eriksdotter M, et al. Development of an Electronic Frailty Index for Hospitalized Older Adults in Sweden. Journals Gerontol Ser A. 2022;77(11):2311–2319. doi:10.1093/gerona/glac069
18. Mak JKL, Religa D, Jylhävä J. Automated frailty scores: towards clinical implementation. Aging. 2023;15(11):4571–4573. doi:10.18632/aging.204815
19. Takenouchi K, Yuasa K, Shioya M, et al. Development of a new seamless data stream from EMR to EDC system using SS-MIX2 standards applied for observational research in diabetes mellitus. Learn Heal Syst. 2018;3(1):e10072–e10072. doi:10.1002/lrh2.10072
20. Kokorelias KM, Danieli E, Dunn S, Feldman S, Ryan DP, Sadavoy J. The DWQ-EMR Embedded Tool to Enhance the Family Physician-Caregiver Connection: a Pilot Case Study. Geriatrics. 2021;6(1):29. doi:10.3390/geriatrics6010029
21. Wilkinson T, Ly A, Schnier C, et al. Identifying dementia cases with routinely collected health data: a systematic review. Alzheimer’s Dement. 2018;14(8):1038–1051. doi:10.1016/j.jalz.2018.02.016
22. Dormosh N, Heymans MW, van der Velde N, et al. External Validation of a Prediction Model for Falls in Older People Based on Electronic Health Records in Primary Care. J Am Med Dir Assoc. 2022;23(10):1691–1697.e3. doi:10.1016/j.jamda.2022.07.002
23. Reuben DB, Hackbarth AS, Wenger NS, Tan ZS, Jennings LA. An Automated Approach to Identifying Patients with Dementia Using Electronic Medical Records. J Am Geriatr Soc. 2017;65(3):658–659. doi:10.1111/jgs.14744
24. Liong-Rung L, Hung-Wen C, Ming-Yuan H, et al. Using Artificial Intelligence to Establish Chest X-Ray Image Recognition Model to Assist Crucial Diagnosis in Elder Patients With Dyspnea. Front Med. 2022;9:893208. doi:10.3389/fmed.2022.893208
25. Kim JH, Hua M, Whittington RA, et al. A machine learning approach to identifying delirium from electronic health records. JAMIA Open. 2022;5(2):ooac042. doi:10.1093/jamiaopen/ooac042
26. Luo J, Liao X, Zou C, et al. Identifying Frail Patients by Using Electronic Health Records in Primary Care: current Status and Future Directions. Front Public Heal. 2022;10:901068. doi:10.3389/fpubh.2022.901068
27. Park S, Kim AJ, Ah YM, et al. Prevalence and predictors of medication-related emergency department visit in older adults: a multicenter study linking national claim database and hospital medical records. Front Pharmacol. 2022;13:1009485. doi:10.3389/fphar.2022.1009485
28. Yoon K, Kim JT, Kwack WG, et al. Potentially Inappropriate Medication Use in Patients with Dementia. Int J Environ Res Public Health. 2022;19(18):11426. doi:10.3390/ijerph191811426
29. Brown T, Rowe TA, Lee JY, et al. Design of Behavioral Economic Applications to Geriatrics Leveraging Electronic Health Records (BEAGLE): a pragmatic cluster randomized controlled trial. Contemp Clin Trials. 2022;112:106649. doi:10.1016/j.cct.2021.106649
30. Polnaszek B, Gilmore-Bykovskyi A, Hovanes M, et al. Overcoming the Challenges of Unstructured Data in Multisite, Electronic Medical Record-based Abstraction. Med Care. 2016;54(10):e65–e72. doi:10.1097/MLR.0000000000000108
31. Floyd JS, Heckbert SR, Weiss NS, Carrell DS, Psaty BM. Use of administrative data to estimate the incidence of statin-related rhabdomyolysis. JAMA. 2012;307(15):1580–1582. doi:10.1001/jama.2012.489
32. Chen L, Li N, Zheng Y, et al. A novel semiautomatic Chinese keywords instrument screening delirium based on electronic medical records. BMC Geriatr. 2022;22(1):779. doi:10.1186/s12877-022-03474-w
33. Chowdhury M, Cervantes EG, Chan WY, Seitz DP. Use of Machine Learning and Artificial Intelligence Methods in Geriatric Mental Health Research Involving Electronic Health Record or Administrative Claims Data: a Systematic Review. Front Psychiatry. 2021;12:738466. doi:10.3389/fpsyt.2021.738466
34. Shao Y, Zeng QT, Chen KK, Shutes-David A, Thielke SM, Tsuang DW. Detection of probable dementia cases in undiagnosed patients using structured and unstructured electronic health records. BMC Med Inform Decis Mak. 2019;19(1):128. doi:10.1186/s12911-019-0846-4
35. McCarty CA, Chisholm RL, Chute CG, et al. The eMERGE Network: a consortium of biorepositories linked to electronic medical records data for conducting genomic studies. BMC Med Genomics. 2011;4:13. doi:10.1186/1755-8794-4-13
36. Clegg A, Bates C, Young J, et al. Development and validation of an electronic frailty index using routine primary care electronic health record data. Age Ageing. 2016;45(3):353–360. doi:10.1093/ageing/afw039
37. Hippisley-Cox J, Coupland C, Brindle P. Development and validation of QRISK3 risk prediction algorithms to estimate future risk of cardiovascular disease: prospective cohort study. BMJ. 2017;357. doi:10.1136/bmj.j2099
38. Ford I, Norrie J. Pragmatic Trials. N Engl J Med. 2016;375(5):454–463. doi:10.1056/nejmra1510059
39. Wiemken TL, Kelley RR. Machine Learning in Epidemiology and Health Outcomes Research. Annu Rev Public Health. 2020;41(1):21–36. doi:10.1146/annurev-publhealth-040119-094437
40. Luo W, Phung D, Tran T, et al. Guidelines for Developing and Reporting Machine Learning Predictive Models in Biomedical Research: a Multidisciplinary View. J Med Internet Res. 2016;18(12):e323–e323. doi:10.2196/jmir.5870
41. Deo RC. Machine Learning in Medicine. Circulation. 2015;132(20):1920–1930. doi:10.1161/CIRCULATIONAHA.115.001593
42. Hashimoto DA, Rosman G, Rus D, Meireles OR. Artificial Intelligence in Surgery: promises and Perils. Ann Surg. 2018;268(1):70–76. doi:10.1097/SLA.0000000000002693
43. Noorbakhsh-Sabet N, Zand R, Zhang Y, Abedi V. Artificial Intelligence Transforms the Future of Health Care. Am J Med. 2019;132(7):795–801. doi:10.1016/j.amjmed.2019.01.017
44. Ben Miled Z, Haas K, Black CM, et al. Predicting dementia with routine care EMR data. Artif Intell Med. 2020;102:101771. doi:10.1016/j.artmed.2019.101771
45. Kumar Y, Koul A, Singla R, Ijaz MF. Artificial intelligence in disease diagnosis: a systematic literature review, synthesizing framework and future research agenda. J Ambient Intell Humaniz Comput. 2023;14(7):8459–8486. doi:10.1007/s12652-021-03612-z
46. Naga Srinivasu P, Ahmed S, Alhumam A, Bhoi Kumar A, Fazal Ijaz M. An AW-HARIS Based Automated Segmentation of Human Liver Using CT Images. Comput Mater Contin. 2021;69(3):3303–3319. doi:10.32604/cmc.2021.018472
47. Voets M, Møllersen K, Bongo LA. Reproduction study using public data of: development and validation of a deep learning algorithm for detection of diabetic retinopathy in retinal fundus photographs. PLoS One. 2019;14(6):e0217541–e0217541. doi:10.1371/journal.pone.0217541
48. Esteva A, Kuprel B, Novoa RA, et al. Dermatologist-level classification of skin cancer with deep neural networks. Nature. 2017;542(7639):115–118. doi:10.1038/nature21056
49. Dayan I, Roth HR, Zhong A, et al. Federated learning for predicting clinical outcomes in patients with COVID-19. Nat Med. 2021;27(10):1735–1743. doi:10.1038/s41591-021-01506-3
50. Rosen T, Zhang Y, Bao Y, et al. Can artificial intelligence help identify elder abuse and neglect? J Elder Abuse Negl. 2020;32(1):97–103. doi:10.1080/08946566.2019.1682099
51. Asan O, Xu J, Montague E. Dynamic Comparison of Physicians’ Interaction Style with Electronic Health Records in Primary Care Settings. J Gen Pract. 2013;2:1000137. doi:10.4172/2329-9126.1000137
52. Hayashi Y, Godai A, Yamada M, et al. Reduction in the numbers of drugs administered to elderly in-patients with polypharmacy by a multidisciplinary review of medication using electronic medical records. Geriatr Gerontol Int. 2016;17(4):653–658. doi:10.1111/ggi.12764
53. Lawrence JE, Cundall-Curry D, Stewart ME, Fountain DM, Gooding CR. The use of an electronic health record system reduces errors in the National Hip Fracture Database. Age Ageing. 2019;48(2):285–290. doi:10.1093/ageing/afy177
54. Arai S, Ishikawa T, Kato H, et al. Multidrug use positively correlates with high-risk prescriptions in the Japanese elderly: a longitudinal study. J Pharm Heal Care Sci. 2019;5:20. doi:10.1186/s40780-019-0150-6
55. Minaya-Freire A, Subirana-Casacuberta M, Puigoriol-Juvanteny E, Ramon-Aribau A. Pain management nursing practice assessment in older adults with dementia. Nurs Open. 2021;8(6):3349–3357. doi:10.1002/nop2.880
56. Munyisia E, Yu P, Hailey D. The effect of an electronic health record system on nursing staff time in a nursing home: a longitudinal cohort study. Australas Med J. 2014;7(7):285–293. doi:10.4066/AMJ.2014.2072
57. Melzer D, Tavakoly B, Winder RE, et al. Much more medicine for the oldest old: trends in UK electronic clinical records. Age Ageing. 2015;44(1):46–53. doi:10.1093/ageing/afu113
58. Wilkinson C, Weston C, Timmis A, Quinn T, Keys A, Gale CP. The Myocardial Ischaemia National Audit Project (MINAP). Eur Hear J - Qual Care Clin Outcomes. 2020;6(1):19–22. doi:10.1093/ehjqcco/qcz052
59. Liebovitz D. Next steps for electronic health records to improve the diagnostic process. Diagnosis. 2015;2(2):111–116. doi:10.1515/dx-2014-0070
60. Agency for Healthcare Research and Quality. Ambulatory Care Safety; 2019. Available from: https://psnet.ahrq.gov/primer/ambulatory-care-safety.
61. Bardach SH, Real K, Bardach DR. Perspectives of healthcare practitioners: an exploration of interprofessional communication using electronic medical records. J Interprof Care. 2017;31(3):300–306. doi:10.1080/13561820.2016.1269312
62. Sommerlad A, Perera G, Mueller C, et al. Hospitalisation of people with dementia: evidence from English electronic health records from 2008 to 2016. Eur J Epidemiol. 2019;34(6):567–577. doi:10.1007/s10654-019-00481-x
63. Lee P, Bubeck S, Petro J. Benefits, Limits, and Risks of GPT-4 as an AI Chatbot for Medicine. N Engl J Med. 2023;388(13):1233–1239. doi:10.1056/nejmsr2214184
64. Car J, Sheikh A, Wicks P, Williams MS. Beyond the hype of big data and artificial intelligence: building foundations for knowledge and wisdom. BMC Med. 2019;17(1):143. doi:10.1186/s12916-019-1382-x
65. Wang S, Bolling K, Mao W, et al. Technology to Support Aging in Place: older Adults’ Perspectives. Healthcare. 2019;7(2):60. doi:10.3390/healthcare7020060
66. Wangmo T, Lipps M, Kressig RW, Ienca M. Ethical concerns with the use of intelligent assistive technology: findings from a qualitative study with professional stakeholders. BMC Med Ethics. 2019;20(1):98. doi:10.1186/s12910-019-0437-z
67. Chen S, Banks WA, Sheffrin M, Bryson W, Black M, Thielke SM. Identifying and categorizing spurious weight data in electronic medical records. Am J Clin Nutr. 2018;107(3):420–426. doi:10.1093/ajcn/nqx056
68. Mittelstadt BD, Allo P, Taddeo M, Wachter S, Floridi L. The ethics of algorithms: mapping the debate. Big Data Soc. 2016;3(2):205395171667967. doi:10.1177/2053951716679679
69. Rosales A, Fernández-Ardèvol M. Structural Ageism in Big Data Approaches. Nord Rev. 2019;40(s1):51–64. doi:10.2478/nor-2019-0013
70. World Health Organization. Ageism in Artificial Intelligence for Health: WHO Policy Brief; 2022.
71. Park JH, Cho HE, Kim JH, et al. Machine learning prediction of incidence of Alzheimer’s disease using large-scale administrative health data. NPJ Digit Med. 2020;3:46. doi:10.1038/s41746-020-0256-0
72. Ford E, Sheppard J, Oliver S, Rooney P, Banerjee S, Cassell JA. Automated detection of patients with dementia whose symptoms have been identified in primary care but have no formal diagnosis: a retrospective case-control study using electronic primary care records. BMJ Open. 2021;11(1):e039248–e039248. doi:10.1136/bmjopen-2020-039248
73. Davis SE, Lasko TA, Chen G, Siew ED, Matheny ME. Calibration drift in regression and machine learning models for acute kidney injury. J Am Med Inform Assoc. 2017;24(6):1052–1061. doi:10.1093/jamia/ocx030
74. Iluz T, Weiss A, Gazit E, et al. Can a Body-Fixed Sensor Reduce Heisenberg’s Uncertainty When It Comes to the Evaluation of Mobility? Effects of Aging and Fall Risk on Transitions in Daily Living. J Gerontol a Biol Sci Med Sci. 2016;71(11):1459–1465. doi:10.1093/gerona/glv049
75. Corradi JP, Thompson S, Mather JF, Waszynski CM, Dicks RS. Prediction of Incident Delirium Using a Random Forest classifier. J Med Syst. 2018;42(12):261. doi:10.1007/s10916-018-1109-0
76. Rahimian F, Salimi-Khorshidi G, Payberah AH, et al. Predicting the risk of emergency admission with machine learning: development and validation using linked electronic health records. PLoS Med. 2018;15(11):e1002695. doi:10.1371/journal.pmed.1002695
77. Jackson L, Saund J, Donnelly G. Improving the Documentation of DNACPR Decisions Following the Transition to Electronic Record Keeping. Age Ageing. 2021;50(Supplement_1):i12–i42. doi:10.1093/ageing/afab030.31
78. Middleton B, Bloomrosen M, Dente MA, et al. Enhancing patient safety and quality of care by improving the usability of electronic health record systems: recommendations from AMIA. J Am Med Informatics Assoc. 2013:20(e1):e2–e8. doi:10.1136/amiajnl-2012-001458
79. Lin HL, Wu DC, Cheng SM, Chen CJ, Wang MC, Cheng CA. Association between Electronic Medical Records and Healthcare Quality. Medicine. 2020;99(31):e21182–e21182. doi:10.1097/MD.0000000000021182
80. Gardner RL, Cooper E, Haskell J, et al. Physician stress and burnout: the impact of health information technology. J Am Med Informatics Assoc. 2019;26(2):106–114. doi:10.1093/jamia/ocy145
81. Steinkamp J, Kantrowitz JJ, Airan-Javia S. Prevalence and Sources of Duplicate Information in the Electronic Medical Record. JAMA Netw Open. 2022;5(9):e2233348–e2233348. doi:10.1001/jamanetworkopen.2022.33348
82. Harry E, Sinsky C, Dyrbye LN, et al. Physician Task Load and the Risk of Burnout Among US Physicians in a National Survey. Jt Comm J Qual Patient Saf. 2021;47(2):76–85. doi:10.1016/j.jcjq.2020.09.011
83. Sinsky C, Colligan L, Li L, et al. Allocation of Physician Time in Ambulatory Practice: a Time and Motion Study in 4 Specialties. Ann Intern Med. 2016;165(11):753. doi:10.7326/m16-0961
84. Holmgren AJ, Downing NL, Tang M, Sharp C, Longhurst C, Huckman RS. Assessing the impact of the COVID-19 pandemic on clinician ambulatory electronic health record use. J Am Med Informatics Assoc. 2022;29(3):453–460. doi:10.1093/jamia/ocab268
85. Flanagan ME, Saleem JJ, Millitello LG, Russ AL, Doebbeling BN. Paper- and computer-based workarounds to electronic health record use at three benchmark institutions. J Am Med Informatics Assoc. 2013;20(e1):e59–e66. doi:10.1136/amiajnl-2012-000982
86. Darmon D, Sauvant R, Staccini P, Letrilliart L. Which functionalities are available in the electronic health record systems used by French general practitioners? An assessment study of 15 systems. Int J Med Inform. 2014;83(1):37–46. doi:10.1016/j.ijmedinf.2013.10.004
87. Krist AH. Electronic health record innovations for healthier patients and happier doctors. J Am Board Fam Med. 2015;28(3):299–302. doi:10.3122/jabfm.2015.03.150097
88. Brault I, Therriault PY, St-Denis L, Lebel P. Implementation of interprofessional learning activities in a professional practicum: the emerging role of technology. J Interprof Care. 2015;29(6):530–535. doi:10.3109/13561820.2015.1021308
89. Grabenbauer L, Skinner A, Windle J. Electronic Health Record Adoption - Maybe It’s not about the Money: physician Super-Users. Electronic Health Records and Patient Care Appl Clin Inform. 2011;2(4):460–471. doi:10.4338/ACI-2011-05-RA-0033
90. Gooch P, Roudsari A. Computerization of workflows, guidelines, and care pathways: a review of implementation challenges for process-oriented health information systems. J Am Med Informatics Assoc. 2011;18(6):738–748. doi:10.1136/amiajnl-2010-000033
91. Jaspers MWM, Smeulers M, Vermeulen H, Peute LW. Effects of clinical decision-support systems on practitioner performance and patient outcomes: a synthesis of high-quality systematic review findings. J Am Med Informatics Assoc. 2011;18(3):327–334. doi:10.1136/amiajnl-2011-000094
92. Menachemi N, Collum TH. Benefits and drawbacks of electronic health record systems. Risk Manag Healthc Policy. 2011;4:47–55. doi:10.2147/RMHP.S12985
93. European Union (EU). General data protection regulation (GDPR). 2017. Available from: https://gdpr.eu/.
94. Mamra A, Sibghatullah AS, Ananta GP, Alazzam MB, Ahmed YH, Doheir M. Theories and factors applied in investigating the user acceptance towards personal health records: review study. Int J Healthc Manag. 2017;10(2):89–96. doi:10.1080/20479700.2017.1289439
95. Barros Pena B, Clarke RE, Holmquist LE, Vines J. Circumspect Users: older Adults as Critical Adopters and Resistors of Technology. Proc 2021 CHI Conf Hum Factors Comput Syst. 2021. doi:10.1145/3411764.3445128
96. Zhang X, Xu X, Cheng J. WeChatting for Health: what Motivates Older Adult Engagement with Health Information. Healthcare. 2021;9(6):751. doi:10.3390/healthcare9060751
97. Wilson J, Heinsch M, Betts D, Booth D, Kay-Lambkin F. Barriers and facilitators to the use of e-health by older adults: a scoping review. BMC Public Health. 2021;21(1):1556. doi:10.1186/s12889-021-11623-w
98. Wang X, Zhao YC. Understanding older adults’ intention to use patient-accessible electronic health records: based on the affordance lens. Front Public Heal. 2022;10:1075204. doi:10.3389/fpubh.2022.1075204
99. Nurgalieva L, Cajander A, Moll J, Åhlfeldt RM, Huvila I, Marchese M. ‘I do not share it with others. No, it’s for me, it’s my care’: on sharing of patient accessible electronic health records. Health Informatics J. 2020;26(4):2554–2567. doi:10.1177/1460458220912559
100. Eriksson-Backa K, Hirvonen N, Enwald H, Huvila I. Enablers for and barriers to using My Kanta – a focus group study of older adults’ perceptions of the National Electronic Health Record in Finland. Informatics Heal Soc Care. 2021;46(4):399–411. doi:10.1080/17538157.2021.1902331
101. Faiola A, Papautsky EL, Isola M. Empowering the Aging with Mobile Health: a mHealth Framework for Supporting Sustainable Healthy Lifestyle Behavior. Curr Probl Cardiol. 2019;44(8):232–266. doi:10.1016/j.cpcardiol.2018.06.003
102. West VL, Borland D, Hammond WE. Innovative information visualization of electronic health record data: a systematic review. J Am Med Informatics Assoc. 2015;22(2):330–339. doi:10.1136/amiajnl-2014-002955
103. Bauermeister S, Orton C, Thompson S, et al. The Dementias Platform UK (DPUK) Data Portal. Eur J Epidemiol. 2020;35(6):601–611. doi:10.1007/s10654-020-00633-4
104. Brayne C, Davis D. Making Alzheimer’s and dementia research fit for populations. Lancet. 2012;380(9851):1441–1443. doi:10.1016/S0140-6736(12)61803-0
105. Benchimol EI, Smeeth L, Guttmann A, et al. The REporting of studies Conducted using Observational Routinely-collected health Data (RECORD) statement. PLoS Med. 2015;12(10):e1001885–e1001885. doi:10.1371/journal.pmed.1001885
106. Liu X, Rivera SC, Moher D. Reporting guidelines for clinical trial reports for interventions involving artificial intelligence: the CONSORT-AI Extension. BMJ. 2020;370:m3164–m3164. doi:10.1136/bmj.m3164
107. Cruz Rivera S, Liu X, Chan AW, et al. Guidelines for clinical trial protocols for interventions involving artificial intelligence: the SPIRIT-AI extension. Lancet Digit Heal. 2020;2(10):e549–e560. doi:10.1016/S2589-7500(20)30219-3
108. Meeks DW, Smith MW, Taylor L, Sittig DF, Scott JM, Singh H. An analysis of electronic health record-related patient safety concerns. J Am Med Informatics Assoc. 2014;21(6):1053–1059. doi:10.1136/amiajnl-2013-002578
109. Elias B, Barginere M, Berry PA, Selleck CS. Implementation of an electronic health records system within an interprofessional model of care. J Interprof Care. 2015;29(6):551–554. doi:10.3109/13561820.2015.1021001
110. Gold JA, Tutsch ASR, Gorsuch A, Mohan V. Integrating the Electronic Health Record into high-fidelity interprofessional intensive care unit simulations. J Interprof Care. 2015;29(6):562–563. doi:10.3109/13561820.2015.1063482
111. Topol EJ. High-performance medicine: the convergence of human and artificial intelligence. Nat Med. 2019;25(1):44–56. doi:10.1038/s41591-018-0300-7
112. Lee JL, Matthias MS, Menachemi N, Frankel RM, Weiner M. A critical appraisal of guidelines for electronic communication between patients and clinicians: the need to modernize current recommendations. J Am Med Informatics Assoc. 2018;25(4):413–418. doi:10.1093/jamia/ocx089
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.