")
Back to Journals » Clinical, Cosmetic and Investigational Dermatology » Volume 16
Use of Biological Therapies for the Management of Pustular Psoriasis: A New Era?
Authors Megna M, Camela E , Ruggiero A , Battista T, Martora F , Cacciapuoti S, Potestio L
Received 13 May 2023
Accepted for publication 21 June 2023
Published 28 June 2023 Volume 2023:16 Pages 1677—1690
DOI https://doi.org/10.2147/CCID.S407812
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Jeffrey Weinberg
Matteo Megna,1 Elisa Camela,2 Angelo Ruggiero,1 Teresa Battista,1 Fabrizio Martora,1 Sara Cacciapuoti,1 Luca Potestio1
1Section of Dermatology, Department of Clinical Medicine and Surgery, University of Naples Federico II, Naples, Italy; 2Dermatology Unit, Istituto Dermopatico dell’Immacolata - IRCCS, Rome, Italy
Correspondence: Luca Potestio, Section of Dermatology, Department of Clinical Medicine and Surgery, University of Naples Federico II, Naples, Italy, Tel +39 – 081 – 7462457, Fax +39 – 081 – 7462442, Email [email protected]
Abstract: Generalized pustular psoriasis (GPP) is a severe and rare form of psoriasis, being a potentially life-threatening condition, characterized by recurring episodes or flares of widespread cutaneous erythema with macroscopic sterile pustules. An irregular innate immune response is linked to GPP, which is considered an auto-inflammatory disorder, while innate and adaptive immunopathogenic responses are involved in psoriasis pathogenesis. In consequence, different cytokine cascades have been suggested to be mainly involved in the pathogenesis of each different psoriasis form, with the interleukin (IL)23/IL17 axis implied in plaque psoriasis, and the IL36 pathway in the GPP. As regards GPP treatment, conventional systemic drugs available for plaque psoriasis are usually used as the first-line treatment option. However, contraindications and adverse events often limit the use of these therapies. In this scenario, biologic drugs may represent a promising treatment option. To date, even if 12 different biologics have been approved for plaque psoriasis, none of these is approved for GPP where they are employed off-label. Recently, spesolimab, an anti-IL36 receptor monoclonal antibody, has been recently approved for GPP. The purpose of this article is to assess the current literature about the use of biological therapies for the treatment of GPP to establish the basis for a shared GPP management algorithm.
Keywords: pustular psoriasis, treatment, biologic drugs
Introduction
Psoriasis is a chronic-inflammatory cutaneous disease, with a worldwide prevalence ranging from 2% to 3%.1 Even if plaque psoriasis is the commonest clinical presentation, several phenotypes can be distinguished.2 Among these, generalized pustular psoriasis (GPP) is a severe and rare form, as well as a potentially life-threatening condition.3 It is characterized by recurring episodes or flares of widespread cutaneous erythema with macroscopic sterile pustules.4,5 Its prevalence ranges from 0.18 to 18 cases per 100 000 habitants.4,5 Acute episodes of GPP are often associated with systemic symptoms such as fatigue, high-grade fever, and leukocytosis.4,5 Moreover, the GPP clinical course may be heterogenous, from relapsing disease with recurrent flares developing years after the initial diagnosis to a persistent disease continuously flaring over time. As regards risk factors, GPP is often idiopathic.4,5 However, internal and external factors, such as pregnancy, corticosteroid withdrawal and infections, may trigger GPP flares.4,5
Plaque psoriasis is often present in patients with GPP, suggesting a shared pathogenesis.4,5 However, an irregular innate immune response is linked to GPP, considered an auto-inflammatory disease, while innate and adaptive immunopathogenic responses are involved in psoriasis pathogenesis.4,5 In consequence, different cytokine cascades have been suggested to be prevalent in the pathogenesis of each different psoriasis form, with the interleukin (IL)23/IL17 axis implied in plaque psoriasis, and the IL36 pathway in GPP.6 Indeed, recent knowledge on GPP pathogenesis showed that IL36 plays a key pathogenetic role and the mutation of the IL36 receptor (IL36RN) is associated with more severe forms of disease.6
As regards GPP treatment, conventional systemic drugs used for psoriasis (methotrexate, oral retinoids and cyclosporin) are usually used as first-line treatment options.7 However, there is limited GPP-specific evidence, clinical trials are absent, and contra-indications often limit the use of these therapies.7 In this scenario, biologic drugs may represent a promising treatment option. Indeed, the excellent results in terms of safety and efficacy demonstrated for plaque psoriasis8–10 suggest that these drugs are a valuable option for GPP management too. Currently, 12 biologics have been approved for psoriasis, acting on Tumor necrosis factor (TNF) α, IL 12/23, IL17, and IL23.11 None of these is approved for GPP where they are employed off-label. However, to date only spesolimab, an anti-IL36 receptor monoclonal antibody, has recently been approved specifically for GPP disease.12
Globally, the lack of clinical evidence and guidelines led to the need for more studies investigating the effectiveness and safety of new drugs that can be used for GPP management. The aim of this article is to review current literature on the use of biologic drugs for the management of GPP in order to point out their potential therapeutic role in GPP and to offer a wide current clinical perspective.
Materials and Methods
A search of the current literature on the Embase, Google Scholar, Cochrane Skin, PubMed, and clinicaltrials.gov databases (until March 31, 2023) was performed using the following terms: “psoriasis”, “general pustular psoriasis”, “biologic drugs”, “efficacy”, “safety”, “infliximab”, “certolizumab”, “adalimumab”, “etanercept”, “ustekinumab”, “ixekizumab”, “secukinumab”, “brodalumab”, “bimekizumab”, “tildrakizumab”, “risankizumab”, “guselkumab”, and “spesolimab”. The Preferred Reporting Items for Systematic reviews and Meta-analyses (PRISMA) guidelines were followed to point out relevant data from the screened and analyzed articles. Metanalyses, reviews, clinical trials, case reports and series, and real-life experiences were investigated in our review, selecting the most relevant articles. Only English-language articles were collected. The texts and abstracts of designated manuscripts were reviewed to refine the search. Bibliographies were also examined in order to avoid missing some relevant articles. This article is based on previously performed studies and does not contain any studies involving animals or human participants carried out by any of the authors.
Results
A total of 112 articles were collected in the present review. As regards GPP severity, the Japanese Dermatological Association (JDA) severity index was the most used.13 This score is calculated from the sum of skin score (0–9), which includes 3 factors (erythema area with pustules, overall erythema area, and edema area), plus the systemic/laboratory score (0–8) (pyrexia, white blood cell count, C‐reactive protein concentration and serum albumin concentration).13 The total GPP score is categorized by the JDA severity index as follows: mild (0–6), moderate (7–10), and severe (11–17).13
The main results of the review are summarized in Table 1.
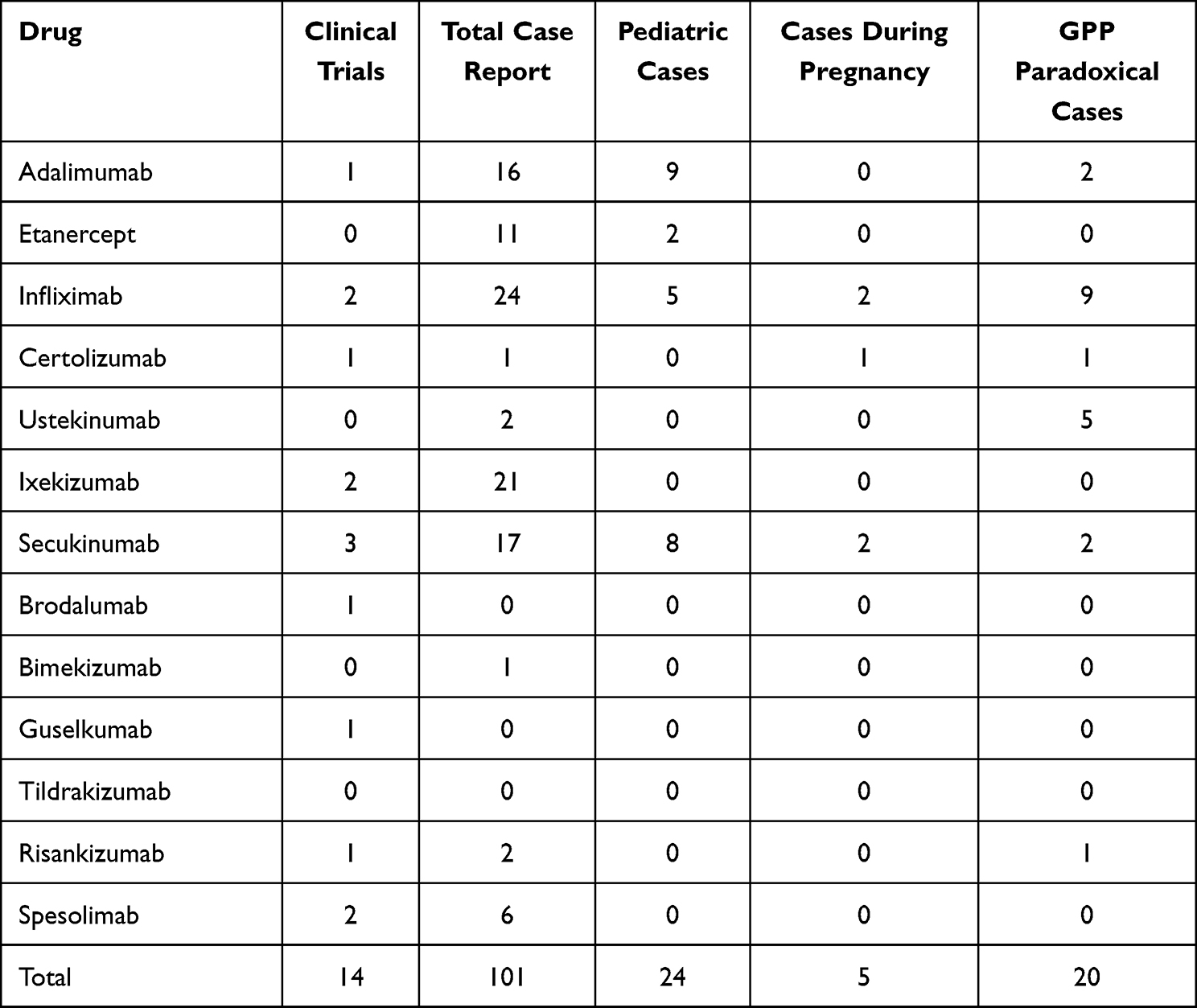 |
Table 1 Detailed Data on Trials and Case Reports on GPP or Paradoxical GPP for Biologic Drugs |
Adalimumab
Adalimumab is an anti-TNFα authorized for the treatment of psoriasis and psoriatic arthritis.14,15 A 52-week, Phase III, multicenter study investigated the efficacy and safety of adalimumab 80 mg at week 0 followed by 40 mg every other week in 10 Japanese subjects affected by GPP.16 The primary endpoint was clinical response, defined as reaching remission (total skin score: 0) or improvement from baseline (reduction of ≥1 point from a baseline total skin score of 3 or ≥2 points from a baseline total skin score of ≥4) at week 16.16 A total of 7 (70.0%) patients achieved a clinical response at week 16, and 5 (50.0%) subjects reached the same score at week 52.16 Of note, 5 (50.0%) subjects increased adalimumab dosage to 80 mg on or after week 8.16 As regards safety, 9 patients experienced at least 1 adverse event (AE), with 3 serious AEs reported (moderate bacterial enterocolitis, renal failure, and chronic sinusitis).16 The commonest AE reported was nasopharyngitis and pruritus (3, 30.0% each).16 Globally, 5 (50.0%) patients completed the study; 3 (30.0%) subjects discontinued prematurely due to lack of efficacy and 2 (20.0%) due to AEs (moderate bacterial enterocolitis and renal failure).16
The efficacy and safety of adalimumab in GPP treatment was also shown by several case reports,17–21 including pediatric patients,22–24 as well as in combination with methotrexate25 and acitretin.26 Finally, two paradoxical GPP were reported during adalimumab treatment.27,28
Etanercept
Etanercept is an anti-TNFα drug. It is a soluble version of the TNF receptor that neutralizes the proinflammatory activity of TNF- α.29
Data on the use of etanercept for the management of GPP are limited to a few case reports. Among these, Esposito et al reported the use of etanercept at different dosages on 6 patients with GPP.30 Mean Psoriasis Area Severity Index (PASI) was 18.6.30 Among these, 2 patients received 25 mg every 2 weeks while the remaining patients received 50 mg every 2 weeks.30 The authors showed that the dosage of 50 mg biweekly was effective, with good efficacy and rapidity of effect. Subjects continuously treated at this dose for 24 weeks presented stable conditions and long-term maintenance until week 48, even after a dosage reduction to 25 mg.30 Indeed, 2 patients received 25 mg every 2 weeks and showed an unsatisfactory response at week 12 (patient 1: PASI 13.5 vs 17.8 at baseline; patient 2: PASI 12.2 vs 19.8 at baseline) and 2 subjects who reduced the dosage from 50 mg to 25 mg at week 12 showed disease worsening.30
A few other case reports showed the efficacy of etanercept in GPP management,31–33 also in pediatric patients.34,35
Infliximab
Infliximab is a chimeric human–murine monoclonal antibody targeting TNFα.36
The efficacy and safety of infliximab in GPP has been reported in a multicenter study involving 7 patients receiving infliximab at the dose of 5 mg⁄ kg at weeks 0, 2 and 6 and then every 8 weeks up to week 46.37 The primary endpoint was the response rate of global improvement, defined as the proportion of subjects assessed as “resolved” or “improved”.37 All of the patients reached a response defined as “improved” at weeks 2 and 6.37 Moreover, the response rate at week 50 was 100.0%, with 3 patients rated as “resolved” and 1 patient as “improved”.37 As regards safety, 7 (100%) patients reported at least 1 AE, with infection as the most common (5, 71.4%).37 Moreover, 5 (71.4%) serious AEs were collected in 2 (28.6%) patients (“pustular psoriasis”, “herpes zoster”, “retroperitoneal abscess”, “intervertebral discitis”, and “spondylitis”).37
Similarly, a large-scale prospective post-marketing surveillance study enrolled 164 patients receiving infliximab 5 mg/kg at weeks 0, 2 and 6, and every 8 weeks thereafter up to 6 months. JDA severity score was used to assess clinical disease. Only 56 subjects (34.1%) had completed data. At baseline, patients with mild, moderate, and severe GPP were 38 (67.9%), 14 (25.0%) and 4 (7.1%) while, at final assessment, there were 53 (94.6%), 1 (1.8%) and 2 (3.6%), respectively. The safety issue specifically in relation to patients with GPP has not been discussed.38 These results were confirmed by several case reports.39–53
Infliximab has been reported to be safe and effective for the management of GPP during pregnancy54–57 and for pediatric patients.58–61
Finally, 9 cases of paradoxical GPP developed during treatment with infliximab have been reported.62–68
Certolizumab
Certolizumab is an anti-TNFα agent which has demonstrated long-term safety and efficacy in treating moderate-to-severe plaque psoriasis.69 Its role in GPP management has been reported in an exploratory analysis of a 52-week, Phase II/III, double-blind, placebo-controlled, multicenter, randomized trial.70 A total of 7 Japanese patients were enrolled and randomized to receive certolizumab 400 mg every 2 weeks (n = 3) or certolizumab 200 mg every 2 weeks after a loading dose of certolizumab 400 mg at weeks 0, 2, and 4 (n = 4).70 At baseline, mean JDA score was 6.3 ± 4.0 and 5.5 ± 2.4 in the certolizumab 400 mg and 200 mg cohorts, respectively. JDA total score improvement was reported at week 16 (2.0–2.5) and continued to improve up to week 52 (1.7–2.0). Moreover, Global Improvement Score (GIS) responders, defined as patients “very much improved”, “much improved”, or “minimally improved”, were 7 (100%) at week 16 and 6 (85.7%) at week 52, respectively.70 All the patients reported at least 1 AE.70 Of note, 2 serious AEs were reported (neutropenia and pustular psoriasis), all without requiring treatment discontinuation.70
Furthermore, case reports reported the effectiveness and safety of certolizumab in GPP management,71 also during pregnancy.72
Finally, a de novo-onset of palmoplantar pustulosis followed by GPP in a patient with rheumatoid arthritis during treatment with certolizumab has been reported.72
Ustekinumab
Ustekinumab is an IL-12/23 inhibitor.73 Daudén et al first described the effectiveness of ustekinumab in a 47‐year‐old man with GPP unresponsive to multiple topical agents, etretinate, acitretin, retinoids with psoralen plus ultraviolet A and methotrexate, infliximab and efalizumab.74 Similarly, Storan et al reported the case of a 90-year-old woman affected by GPP successfully treated with ustekinumab.75
Finally, several cases of paradoxical GPP during treatment with ustekinumab have been reported.76–80
Ixekizumab
Ixekizumab is an IL-17A antagonist, licensed for use in moderate-to-severe plaque psoriasis.81 The effectiveness and safety of ixekizumab (two 80 mg subcutaneous injections at baseline followed by 80 mg every 2 weeks through week 12 and 80 mg every 4 weeks thereafter) for up to 52 weeks has been reported in a Phase III trial (UNCOVER-J) involving 5 patients with GPP.82,83 PASI reduction from baseline (12.8 ± 5.5) was observed as early as week 1 (6.9 ± 3.0).82,83 Moreover, PASI75/90/100 were reached by 4 (80.0%), 3 (60.0%) and 1 (20.0%) patients at week 12, and by 4 (80.0%), 2 (40.0%) and 2 (40.0%) at week 24, respectively.82,83 All patients experienced at least 1 AE, all without requiring treatment discontinuation.82,83
An extension of this study up to week 244 showed the long-term efficacy of ixekizumab, with an observed mean PASI of 1.8 and 1.6 at week 52 and week 244, respectively.84,85 Similarly, all patients had a GIS of “resolved” or “improved” from week 12 onwards; none of the patients had a GIS of “unchanged” or “worsened” during the remaining study period.84,85
The efficacy and safety of ixekizumab for GPP have been reported also in real-life studies. Nagata et al reported a case series on 10 patients with GPP. Mean PASI at baseline was 25.5 ± 9.5).86 PASI75 response was achieved by 6/9 (66.7%) patients at week 4, by 9/9 (100%) subjects at week 12 and by 7/8 (87.5%%) patients at week 24.86 Similarly, PASI90 and PASI100 were achieved by 4/9 (44.4%) and 2/9 (22.2%) subjects at week 4, 6/9 (66.7%) and 2/9 (22.2%) patients at week 12 and by 6/8 (75.0%) and 0 (0%) subjects at week 24.86 Treatment interruption was registered in 3 patients: colon cancer, referral to another hospital because of other disease, or difficulty attending the hospital because of worsening of dementia.86
Other data on the use of ixekizumab in GPP have been reported by Morita et al in their cohort of 7 patients.87 Of these, 1 (14.3%) discontinued treatment for lack of efficacy while 6 (85.7%) subjects reached week 12. Moreover, 2 patients (28.6%) continued the study up to week 20.87 At baseline, mean PASI and GPP severity index scores were 10.2 and 3.1 ± 1.7. At week 12, 4 (57.1%) patients with GPP scored “resolved”, 2 (28.6%) “improved”, and 1 (14.3%) “worsened”. Among the 2 patients continuing treatment until week 20, one scored “resolved” and one “improved”. No drug-related AEs were reported.87
These data in terms of efficacy and safety were also confirmed by several case studies.88–91 Finally, ixekizumab was found to improve inflammatory markers in patients with GPP with systemic inflammation.92
Secukinumab
Secukinumab is a biologic drug acting against IL-17A.93 The efficacy and safety of secukinumab for the management of GPP were investigated in a 52-week Phase III study involving 12 Japanese patients. Secukinumab was administered at the dosage of 150 mg at baseline, weeks 1, 2, 3 and 4, and then every 4 weeks.94 Of note, 2 non-responder subjects were up-titrated to 300 mg at weeks 8 and 24, respectively, and 1 patient discontinued the study for protocol deviation. The main endpoint was treatment success (defined as “minimally improved”, “much improved” or “very much improved” in Clinical Global Impression [CGI] as per the JDA severity index) at week 16.94 Secondary endpoints included the achievement of treatment success and PASI75/90/100 at week 52.94 The mean JDA and PASI scores at baseline were 6 and 17.4, respectively. Globally, 10 (83.3%) reached treatment success at week 16 and at week 52.94 As regards PASI, 8/11 (72.7%) subjects reached PASI75 at week 52 while PASI90 and PASI100 were reached by 7/11 (63.6%) and 3/11 (27.3%) patients at the same timepoint, respectively. No unexpected safety signals were collected, with nasopharyngitis (6, 50.0%) as the most common AE registered.94
Several case reports seem to confirm these results,95–102 also during pregnancy.103,104
Secukinumab seems to be a valuable weapon for GPP also in pediatric patients, as reported in a 48-week retrospective real-world study involving 18 pediatric patients (mean age 7.9 ± 2.3 years) receiving secukinumab 75 mg at weeks 0, 1, 2, 3, and 4 and then every 4 weeks, with the purpose of assessing the change in the Generalized Pustular Psoriasis Area and Severity Index (GPPASI) and Generalized Pustular Psoriasis Physician Global Assessment (GPPGA) scores from the baseline to weeks 2, 4, 12, 24, and 48.105 GPPASI scored from 31.7 (baseline) to 5.1 at week 2, continuing to decrease to 1.3 (week 4), and maintaining clinical response up to week 48.105 GPPASI scores of 90 and 100 at week 48 were reached by 2 (11.1%) and 16 (88.9%) patients, respectively. No serious AEs were reported.105
Of interest, a recent real-world study compared the effectiveness and safety of acitretin (16 patients) and secukinumab (20 patients) in a pediatric population.106 JDA score at baseline was 9.0 ± 3.5 for the secukinumab cohort and 10.1 ± 2.3 for the acitretin group.106 A significant response for patients receiving secukinumab was reported from week 1 (2.8 ± 1.74) up to week 12 (0).106 In the acitretin group, JDA score reduced to 6.1 ± 2.3 at week 1 and to 0.7 ± 0.9 at week 12.106 Globally, the authors reported that the effectiveness of secukinumab was better and more rapid than that of acitretin. Secukinumab was also well tolerated, with no severe AEs reported. The dosages of secukinumab and acitretin has not been reported.106
Another 9 case reports suggest the effectiveness and safety of secukinumab in GPP management.107–111
Finally, two cases of paradoxical GPP induced by secukinumab have been reported.112,113
Brodalumab
Brodalumab is a biologic agent that acts through the blockage of the IL-17 receptor.114 A 52-week, open‐label, multicenter, Phase III study involving 12 Japanese patients affected by GPP investigated the effectiveness and safety of brodalumab (140 mg at day 1 and weeks 1 and 2, and then every 2 weeks) for this form of psoriasis.115 The main outcome was the assessment of the change from baseline of CGI. Secondary endpoints included the assessment of PASI and Pustular Symptom Score (PSS: range 0–17) reduction. At baseline, mean PASI was 15.0 ± 12.1 and mean PSS was 4.4 ± 2.4. A CGI classification of “improved” or “remission” at weeks 2, 12 and 52 was reached by 9 (75.0%), 10 (83.3%) and 11 (91.7%) patients, respectively.115 PASI reduced to 5.2 ± 8.6 at week 12 and to 1.8 ± 4.9 at week 52, respectively, with 4 (33.3%) and 10 (83.3%) patients achieving PASI90 at these timepoints.115 As regards PSS, 4 (33.3%) patients had a score of 1 at week 2, whereas 5 (41.7%) had the same score at weeks 12 and 52. PSS 0 was reached by 3 (25.0%) and 6 (50.0%) patients at weeks 12 and 52, respectively.115 As regards safety, AEs were reported in 11 (91.7%) patients and 3 of these were considered serious (serious AEs occurred in five patients: three of 12 patients with GPP (lumbar vertebral fracture, exacerbation of pustular psoriasis and hepatocellular carcinoma).115 However, none were considered treatment related.115
Finally, the possible rebound of GPP in patients having to discontinue brodalumab for reasons such as pregnancy or surgery has been reported.116
Bimekizumab
Bimekizumab is a humanized antibody that selectively acts on the biologic functions of IL-17A and IL-17F.117–119
Recently, a case of a 69-year-old Japanese woman with GPP successfully treated with bimekizumab in combination granulocyte monocyte adsorption apheresis was reported.120
Guselkumab
Guselkumab is a monoclonal antibody acting through the blockade of the IL-23 cytokine pathway.121 Despite its efficacy and safety for psoriasis management having been widely described,122,123 data on its use for GPP are scant. However, Sano et al reported the results of a 52-week, Phase III, multicenter study investigating the use of guselkumab on 10 Japanese patients with GPP. The main aim of the study was to assess the proportion of patients achieving treatment success, defined as a CGI score of “very much improved”, “much improved” or “minimally improved” (range: 1 = “very much improved” to 7 = “very much worse”) after 16 weeks of treatment.124 Through week 52 the secondary outcomes were also evaluated, which included change of JDA severity index (from 0 [best] to 17 [worst]) and of PASI. Guselkumab was scheduled at the dosage of 50 mg at weeks 0, 4 and every 8 weeks thereafter. At week 20, dose escalation to 100 mg was allowed.124
At week 16, a CGI of “very much improved” or “much improved” or “minimally improved” was reached by 2 (22.2%), 2 (22.2%) and 3 (33.3%) patients, respectively. Two patients discontinued the study (1: squamous cell carcinoma of the skin, 1: lack of efficacy).124 As regards secondary outcomes, a PASI reduction from baseline (29.3 ± 20.0) was observed at week 8 (−13.8 ± 12.68), continuing to decrease up to week 52 (4.8 ± 6.4).124 Similarly, JDA reduction from 5.4 ± 1.8 was observed as early as week 1 (−0.2 ± 2.0) up to week 52 (−3.0 ± 2.4).124 All patients experienced at least one AE, with only two of these considered serious: fall and loss of consciousness and squamous cell carcinoma of skin.124 Of note, guselkumab was administered at a different dosage as compared to a labelled one (100 mg), with the same time of administration.124
Tildrakizumab
Tildrakizumab is a humanized IgG1 monoclonal antibody acting on IL-23 p19.125 Even if several studies have shown its effectiveness and safety in psoriasis management,126–128 data on its use on GPP are still absent.
Risankizumab
Risankizumab is a fully human monoclonal antibody that selectively targets IL-23A.129,130 The effectiveness and safety of risankizumab for the management of GPP have been reported by a primary analysis and 180-week follow-up results of the Phase III, multicenter IMMspire study, involving 8 Japanese patients with GPP, randomized 1:1 to receive risankizumab 150 mg or 75 mg at week 0, week 4 and every 12 weeks up to week 160.131 The main aim was the assessment of the percentage of subjects reaching clinical response at week 16, defined as “slightly improved” in the overall improvement rating from baseline according to the JDA score.131 Secondary end points comprised the percentage of subjects reaching clinical response at week 52 as well as PASI90 response at weeks 16 and 52. Other efficacy end points evaluated in weeks were the achievement of clinical responses, PASI 90, DLQI 0/1, and change from baseline in total JDA score. At baseline, mean PASI was 17.4 ± 9.4 and mean JDA 4.8.131
The primary endpoint at week 16 was reached by all patients, regardless of the dose of risankizumab.131 Clinical response was maintained in all those subjects who continued the study.131 JDA reduction was reported as early as week 4 (−3.5 SD ± 1.9]), continuing to decrease through week 52 and maintaining the response through week 160.131 Globally, 87.5% of patients reached PASI90 at week 16, and most of maintained this result through week 160. Similarly, DLQI 0/1 was reached by 75.0% of subjects at week 16, remaining stable among patients who did not interrupt the study. Finally, no drug-related serious AEs were reported.131 Recently, a case of acute GPP and a flare of GPP following BNT162b2 vaccine successfully treated with risankizumab have been reported.132,133 Finally, a case of risankizumab-induced paradoxical GPP has been described.134
Spesolimab
Recent knowledge on GPP pathogenesis, in particular the role of IL-36 which seems to induce neutrophil chemokine expression, infiltration, and pustule formation, suggests this cytokine as a potential therapeutic target.135 Spesolimab is an IL-36 receptor antagonist recently approved by US FDA (1 September 2022) and by the EMA (9 December 2022) for the treatment of GPP flares in adults at the dosage of a single intravenous dose of 900 mg over 90 minutes followed by a second infusion one week after in the case of persistant symptoms.136 Its efficacy and safety in GPP management have been evaluated in a Phase II randomized trial (Effisayl 1) involving 53 patients randomized to receive a single 900-mg intravenous dose of spesolimab (n = 35) or placebo (n = 18).137 The primary end point was the achievement of a GPPGA pustulation sub-score of 0
(range: 0 [no visible pustules] to 4 [severe pustulation]) at the end of week 1.137 Globally, 19 (54%) and 1 (6%) patient in the spesolimab and placebo group reached a pustulation sub-score of 0 (p<0.001) and 15 (43%) and 2 (11%) subjects reached a GPPGA total score of 0 or 1 in the same groups, respectively (p=0.02) at week 1.137 As regards safety, a total of 23 (65.7%) patients receiving spesolimab experienced at least 1 AE, with infection as the most common (6, 17.1%). Of note, 2 (5.7%) AEs were classified as serious.137
Recently, a placebo-controlled study (Effasyl 2) involving subjects with GPP has been planned to investigate whether spesolimab maintenance treatment can prevent flares, providing sustained control of the disease.138 Patients will be randomized 1:1:1:1 to receive a spesolimab 600-mg subcutaneous loading dose followed by a 300-mg maintenance dose managed every 4 or 12 weeks, or a spesolimab 300-mg induction dose followed by a 150-mg dose every 12 weeks, or placebo, for 48 weeks.138 The main endpoint is time to first GPP flare.138 Finally, 6 cases of GPP successfully treated with spesolimab have been reported.139,140
Discussion
The introduction of biologic drugs positively impacted on the treatment of moderate-to-severe forms of plaque psoriasis.141–143 Their effectiveness and safety were also confirmed during the Covid-19 pandemic period,144,145 which completely changed daily clinical practice.146–148 However, there is still an unmet need for the treatment of rare forms of the disease. Among these, GPP is characterized as primary, sterile, macroscopically visible pustules on non-acral skin (excepting cases where pustulation is limited to psoriatic plaques) and may or may not be associated with systemic inflammation and/or plaque psoriasis.149 As regards clinical presentation, GPP flares are acute events, which may be elicited by several factors, such as corticosteroid withdrawal, infections, drugs (including paradoxical reaction to biologic drugs), and stressful life events.149,150 The management of GPP is challenging, particularly because of the different pathogeneses with respect to plaque psoriasis. Indeed, different cytokine cascades seem to be predominant in the pathogenesis of each different psoriasis form, with the IL23/IL17 axis implied in plaque psoriasis, and the IL36 pathway in GPP.151 In particular, GPP derives from dysregulation of the innate immune system, mainly the IL36 pathway, which leads to an inflammatory keratinocyte response, with the recruitment of neutrophils.151 This pathogenetic mechanism has been confirmed by studies reporting that mutations in IL36RN (the most common), CARD13, MPO, TNIP1, AP1S3, SERPINA1, and SERPINA3 are associated with GPP.151 In particular, IL36RN, MPO, and SERPINA 1/3 mutations lead to the upregulation of the IL36 pathway, which further stimulates the downstream proinflammatory NF-κB and MAPK cascade.151 Similarly, the loss-of-function mutation of AP1S3 and TNIP1 as well as the gain-of-function mutations of CARD14 are involved in IL36 signaling by hyperactivating the NF-κB pathway.151 Globally, upregulation of the IL36 cascade triggers the proliferation of IL-17-producing CD4+Th17 cells, which continue to spread these inflammatory responses by stimulating the expression of IL-36 and other inflammatory cytokines.151 Finally, the interaction of the IL36 and the IL17/IL23 pathways indicates that both the innate and the adaptive immune responses intertwine in the GPP pathogenesis.151
Thus, the different pathogenesis of GPP, as compared with plaque psoriasis, may lead to the need for a personalized approach.152 Indeed, conventional systemic drugs are often ineffective or contraindicated and use of biologics approved for plaque psoriasis is off-label.153 Moreover, the reduced prevalence of GPP makes clinical trials challenging and current management recommendations are founded on insufficient evidence.153 In this scenario, we performed a review of current literature with the aim of evaluating the effectiveness of biologic drugs for the management of GPP in order to offer a wide current clinical perspective.
The efficacy of biologics targeting IL23, IL17 and TNFα has been reported by a few clinical trials (adalimumab, infliximab, certolizumab, ixekizumab, secukinumab, brodalumab, guselkumab, risankizumab) and limited case reports. However, all of the clinical trials involved only Japanese patients and up to 10% of subjects did not respond to treatment. Moreover, drug dosage was often different and inferior compared to EMA- or FDA-approved dosage for psoriasis. Finally, clinical outcomes investigated in clinical trials are often different, making a standardized endpoint necessary to allow an indirect comparison among these drugs.
As regards real-life data, infliximab has the highest number of case reports collected (24/101, 23.8%) (Table 1). In our opinion, the most frequently reported use of infliximab may derive from its longer period of approval as compared with other biologics. Some biologics have been successfully used in pediatric GPP (adalimumab, etanercept, infliximab, secukinumab), with adalimumab as the most common (9/24, 37.5%) (Table 1). Furthermore, the use of biologic drugs in GPP management has also been reported in patients during pregnancy (infliximab, secukinumab, and certolizumab).
Finally, 20 cases of paradoxical GPP have been reported during biologic treatment (adalimumab, certolizumab, infliximab, secukinumab, ustekinumab, and risankizumab). However, the possible pathogenetic mechanism of these paradoxical reactions has not been identified.
Recently, spesolimab, an IL-36 receptor antagonist, has been approved for the management of GPP.136 In particular, it is the first biologic drug licensed for this use and the unique on-label biologic available for GPP management. The use of spesolimab revealed excellent results in terms of efficacy and safety in the management of GPP. Indeed, Effisayl 1 showed that 54% of patients receiving spesolimab reached a pustulation sub-score of 0 as compared with 6% in the placebo group (p<0.001); 43% and 11% of participants reached a GPPGA total score of 0 or 1 in the same groups, respectively (p= 0.02) after 1 week of treatment.137 The safety of spesolimab was suggested, with AEs reported in 65.7% of patients.137
Despite its recent approval, real-life data are limited to 6 cases of GPP successfully treated with spesolimab being reported.139,140 Moreover, concerns regarding the effectiveness of maintenance treatment with spesolimab in the prevention of GPP flares were raised. The Effasyl 2 trial will try to address these concerns.138
To sum up, several gaps in GPP knowledge still remain. On the one hand, variations in response to spesolimab and other biologic therapies across different ethnic groups should be investigated; on the other hand, the recent approval of spesolimab led to the need for new guidelines/treatment algorithms. In this scenario, more data on the efficacy of other biologic drugs are required, especially in the long term for flare up prevention.
Conclusion
GPP is a severe and potentially life-threatening form of psoriasis which requires an effective and rapid approach. Our review highlights the current available data on biologics for GPP. Although several studies investigating the use of biologics in GPP have been conducted, an indirect comparison of biologics is not allowed, as clinical evaluation differ. Certainly, the rarity of the disease is the main challenge for the definition of targeted guidelines. This scenario may be completely changed by spesolimab, the first biologic approved for GPP, specifically acting on the IL-36 pathway. Promising data have been reported in clinical trials and long-term studies are ongoing. However, real-life data are still scant and the efficacy of this drug in preventing GPP flares has yet to be elucidated. Thus, more studies are required in order to better define the most adequate GPP treatment algorithm.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Michalek IM, Loring B, John SM. A systematic review of worldwide epidemiology of psoriasis. J Eur Acad Dermatol Venereol. 2017;31(2):205–212. doi:10.1111/jdv.13854
2. Armstrong AW, Read C. Pathophysiology, clinical presentation, and treatment of psoriasis: a review. JAMA. 2020;323(19):1945–1960. doi:10.1001/jama.2020.4006
3. Choon SE, Navarini AA, Pinter A. Clinical course and characteristics of generalized pustular psoriasis. Am J Clin Dermatol. 2022;23(Suppl 1):21–29. doi:10.1007/s40257-021-00654-z
4. Rivera-Díaz R, Daudén E, Carrascosa JM, Cueva P, Puig L. Generalized pustular psoriasis: a review on clinical characteristics, diagnosis, and treatment. Dermatol Ther. 2023;13(3):673–688. doi:10.1007/s13555-022-00881-0
5. Choon SE, Lebwohl MG, Turki H, et al. Clinical Characteristics and outcomes of Generalized Pustular Psoriasis (GPP) flares. Dermatology. 2023;239:345–354. doi:10.1159/000529274
6. Javor J, Buc M, Bucová M. Autoinflammatory process in the pathogenesis of generalized pustular psoriasis and perspectives of its targeted therapy. Epidemiol Mikrobiol Imunol Cas Spol Pro Epidemiol Mikrobiol Ces Lek Spol JE Purkyne. 2021;70(3):199–207.
7. Hoegler KM, John AM, Handler MZ, Schwartz RA. Generalized pustular psoriasis: a review and update on treatment. J Eur Acad Dermatol Venereol. 2018;32(10):1645–1651. doi:10.1111/jdv.14949
8. Megna M, Potestio L, Fabbrocini G, Camela E. Treating psoriasis in the elderly: biologics and small molecules. Expert Opin Biol Ther. 2022;1–18. doi:10.1080/14712598.2022.2089020
9. Megna M, Camela E, Battista T, et al. Efficacy and safety of biologics and small molecules for psoriasis in pediatric and geriatric populations. Part II: focus on elderly patients. Expert Opin Drug Saf. 2023:1–16. doi:10.1080/14740338.2023.2173171
10. Megna M, Camela E, Battista T, et al. Efficacy and safety of biologics and small molecules for psoriasis in pediatric and geriatric populations. Part I: focus on pediatric patients. Expert Opin Drug Saf. 2023;22(1):25–41. doi:10.1080/14740338.2023.2173170
11. Dave R, Alkeswani A. An overview of biologics for psoriasis. J Drugs Dermatol. 2021;20(11):1246–1247. doi:10.36849/jdd.6040
12. Baum P, Visvanathan S, Garcet S, et al. Pustular psoriasis: molecular pathways and effects of spesolimab in generalized pustular psoriasis. J Allergy Clin Immunol. 2022;149(4):1402–1412. doi:10.1016/j.jaci.2021.09.035
13. Umezawa Y, Ozawa A, Kawasima T, et al. Therapeutic guidelines for the treatment of generalized pustular psoriasis (GPP) based on a proposed classification of disease severity. Arch Dermatol Res. 2003;295(Suppl 1):S43–54. doi:10.1007/s00403-002-0371-6
14. Megna M, Fornaro L, Potestio L, et al. Efficacy and safety of anti-TNF biosimilars for psoriasis in pediatric and geriatric populations: a 72-week real-life study. Psoriasis. 2022;12:199–204. doi:10.2147/PTT.S365493
15. Zangrilli A, Bavetta M, Bianchi L. Adalimumab in children and adolescents with severe plaque psoriasis: a safety evaluation. Expert Opin Drug Saf. 2020;19(4):433–438. doi:10.1080/14740338.2020.1752659
16. Morita A, Yamazaki F, Matsuyama T, et al. Adalimumab treatment in Japanese patients with generalized pustular psoriasis: results of an open-label Phase 3 study. J Dermatol. 2018;45(12):1371–1380. doi:10.1111/1346-8138.14664
17. Zangrilli A, Papoutsaki M, Talamonti M, Chimenti S. Long-term efficacy of Adalimumab in generalized pustular psoriasis. J Dermatolog Treat. 2008;19(3):185–187. doi:10.1080/09546630701759587
18. Jordan J, Bieber T, Wilsmann-Theis D. Adalimumab: safe and successful in severe pustular psoriasis. J Eur Acad Dermatol Venereol. 2009;23(5):592–593. doi:10.1111/j.1468-3083.2008.02972.x
19. Kimura U, Kinoshita A, Sekigawa I, Takamori K, Suga Y. Successful treatment with Adalimumab in a patient with psoriatic arthritis and generalized pustular psoriasis. J Dermatol. 2012;39(12):1071–1072. doi:10.1111/j.1346-8138.2012.01563.x
20. Gkalpakiotis S, Arenberger P, Gkalpakioti P, et al. A case of acute generalized pustular psoriasis of von Zumbusch treated with Adalimumab. J Eur Acad Dermatol Venereol. 2015;29(10):2063–2064. doi:10.1111/jdv.12597
21. Matsumoto A, Komine M, Karakawa M, Kishimoto M, Ohtsuki M. Adalimumab administration after infliximab therapy is a successful treatment strategy for generalized pustular psoriasis. J Dermatol. 2017;44(2):202–204. doi:10.1111/1346-8138.13632
22. Du Y, Yan Q, Chen M, Dong Z, Wang F. Efficacy of Adalimumab in pediatric generalized pustular psoriasis: case series and literature review. J Dermatolog Treat. 2022;33(6):2862–2868. doi:10.1080/09546634.2022.2089327
23. Callen JP, Jackson JH. Adalimumab effectively controlled recalcitrant generalized pustular psoriasis in an adolescent. J Dermatolog Treat. 2005;16(5–6):350–352. doi:10.1080/09546630500430604
24. Hansel K, Marietti R, Tramontana M, et al. Childhood generalized pustular psoriasis: successful long-term treatment with Adalimumab. Dermatol Ther. 2020;33(3):e13294. doi:10.1111/dth.13294
25. Kawakami H, Maeda T, Abe N, et al. Efficacy of Adalimumab and methotrexate combination therapy on generalized pustular psoriasis patients unresponsive to infliximab monotherapy due to anti-infliximab antibody development. J Dermatol. 2015;42(1):94–95. doi:10.1111/1346-8138.12704
26. Gallo E, Llamas-Velasco M, Daudén E, García-Diez A. Refractory generalized pustular psoriasis responsive to a combination of Adalimumab and Acitretin. Int J Dermatol. 2013;52(12):1610–1611. doi:10.1111/j.1365-4632.2012.05472.x
27. Kimura U, Kinoshita A, Haruna K, et al. Generalized pustular psoriasis-like eruptions induced after the first use of Adalimumab in the treatment of psoriatic arthritis. J Dermatol. 2012;39(3):286–287. doi:10.1111/j.1346-8138.2011.01344.x
28. Rallis E, Korfitis C, Stavropoulou E, Papaconstantis M. Onset of palmoplantar pustular psoriasis while on Adalimumab for psoriatic arthritis: a “class effect” of TNF-alpha antagonists or simply an anti-psoriatic treatment adverse reaction? J Dermatolog Treat. 2010;21(1):3–5. doi:10.3109/09546630902882089
29. Strober BE. The treatment of psoriasis with etanercept. Semin Cutan Med Surg. 2005;24(1):28–36. doi:10.1016/j.sder.2005.01.003
30. Esposito M, Mazzotta A, Casciello C, Chimenti S. Etanercept at different dosages in the treatment of generalized pustular psoriasis: a case series. Dermatology. 2008;216(4):355–360. doi:10.1159/000117706
31. Kamarashev J, Lor P, Forster A, Heinzerling L, Burg G, Nestle FO. Generalised pustular psoriasis induced by cyclosporin a withdrawal responding to the tumour necrosis factor alpha inhibitor etanercept. Dermatology. 2002;205(2):213–216. doi:10.1159/000063919
32. Ephrem G, Jour G, Smith BL. Successful treatment of von Zumbusch generalized pustular psoriasis with cyclosporine after eruption post etanercept injection. J Med Liban. 2011;59(3):168–169.
33. Vine K, Votava HJ, Smith BL. Generalized pustular psoriasis of Zambusch: case report of successful disease control with cyclosporine and etanercept. Cutis. 2012;90(3):132–136.
34. Fialová J, Vojáčková N, Vaňousová D, Hercogová J. Juvenile generalized pustular psoriasis treated with etanercept. Dermatol Ther. 2014;27(2):105–108. doi:10.1111/dth.12065
35. Georgesen C, Wildman H, Wang X, Magro C. Pediatric pustular psoriasis responsive to cyclosporine bridged to etanercept: a treatment approach. Dermatol Online J. 2017;23(11):1. doi:10.5070/D32311037267
36. Papoutsaki M, Osório F, Morais P, et al. Infliximab in psoriasis and psoriatic arthritis. BioDrugs. 2013;27(Suppl 1):13–23. doi:10.1007/BF03325638
37. Torii H, Nakagawa H. Long-term study of infliximab in Japanese patients with plaque psoriasis, psoriatic arthritis, pustular psoriasis and psoriatic erythroderma. J Dermatol. 2011;38(4):321–334. doi:10.1111/j.1346-8138.2010.00971.x
38. Torii H, Terui T, Matsukawa M, Takesaki K, Ohtsuki M, Nakagawa H. Safety profiles and efficacy of infliximab therapy in Japanese patients with plaque psoriasis with or without psoriatic arthritis, pustular psoriasis or psoriatic erythroderma: results from the prospective post-marketing surveillance. J Dermatol. 2016;43(7):767–778. doi:10.1111/1346-8138.13214
39. Samotij D, Gawron E, Szczęch J, Ostańska E, Reich A. Acrodermatitis continua of hallopeau evolving into generalized pustular psoriasis following COVID-19: a case report of a successful treatment with infliximab in combination with acitretin. Biologics. 2021;15:107–113. doi:10.2147/BTT.S302164
40. Ito M, Akutsu K, Isobe M, et al. Generalized pustular psoriasis complicated with idiopathic retroperitoneal fibrosis successfully treated with infliximab. J Dermatol. 2021;48(9):e436–e437. doi:10.1111/1346-8138.15974
41. Fujisawa T, Moriya C, Shibuya Y, Kanoh H, Seishima M. Combination therapy of infliximab and granulocyte/monocyte adsorption apheresis for refractory pustular psoriasis with psoriatic arthritis. Acta Derm Venereol. 2013;93(3):364–365. doi:10.2340/00015555-1463
42. Smith N, Harms KL, Hines AC, et al. Acute treatment of generalized pustular psoriasis of von Zumbusch with single-dose infliximab. J Am Acad Dermatol. 2013;68(6):e187–9. doi:10.1016/j.jaad.2012.11.017
43. Sugiura K, Endo K, Akasaka T, Akiyama M. Successful treatment with infliximab of sibling cases with generalized pustular psoriasis caused by deficiency of interleukin-36 receptor antagonist. J Eur Acad Dermatol Venereol. 2015;29(10):2054–2056. doi:10.1111/jdv.12590
44. Saito K, Ito A, Ishikawa K, et al. Pustular psoriasis occurring after total colectomy for ulcerative colitis and relieved by administration of infliximab. J Dermatol. 2014;41(11):1033–1034. doi:10.1111/1346-8138.12629
45. Kim HS, You HS, Cho HH, et al. Two cases of generalized pustular psoriasis: successful treatment with infliximab. Ann Dermatol. 2014;26(6):787–788. doi:10.5021/ad.2014.26.6.787
46. Li M, Dai W, Yan W, Liu Y, Wang L, Li W. A dramatic response to a single dose of infliximab in a patient with prolonged pustular psoriasis derived from inverse psoriasis. Dermatol Ther. 2017;30(4):e12492. doi:10.1111/dth.12492
47. Newland MR, Weinstein A, Kerdel F. Rapid response to infliximab in severe pustular psoriasis, von Zumbusch type. Int J Dermatol. 2002;41(7):449–452. doi:10.1046/j.1365-4362.2002.01543.x
48. Elewski BE. Infliximab for the treatment of severe pustular psoriasis. J Am Acad Dermatol. 2002;47(5):796–797. doi:10.1067/mjd.2002.128382
49. Schmick K, Grabbe J. Recalcitrant, generalized pustular psoriasis: rapid and lasting therapeutic response to antitumour necrosis factor-alpha antibody (infliximab). Br J Dermatol. 2004;150(2):367. doi:10.1111/j.1365-2133.2004.05719.x
50. Benoit S, Toksoy A, Bröcker EB, Gillitzer R, Goebeler M. Treatment of recalcitrant pustular psoriasis with infliximab: effective reduction of chemokine expression. Br J Dermatol. 2004;150(5):1009–1012. doi:10.1111/j.1365-2133.2004.05960.x
51. Weishaupt C, Metze D, Luger TA, Ständer S. Treatment of pustular psoriasis with infliximab. J Ger Soc Dermatol JDDG. 2007;5(5):397–399. doi:10.1111/j.1610-0387.2007.06296.x
52. Barland C, Kerdel FA. Addition of low-dose methotrexate to infliximab in the treatment of a patient with severe, recalcitrant pustular psoriasis. Arch Dermatol. 2003;139(7):949–950. doi:10.1001/archderm.139.7.949
53. Routhouska SB, Sheth PB, Korman NJ. Long-term management of generalized pustular psoriasis with infliximab: case series. J Cutan Med Surg. 2008;12(4):184–188. doi:10.2310/7750.2008.07036
54. Adachi A, Komine M, Hirano T, et al. Case of generalized pustular psoriasis exacerbated during pregnancy, successfully treated with infliximab. J Dermatol. 2016;43(12):1439–1440. doi:10.1111/1346-8138.13429
55. Beksac B, Adisen E, Gurer MA. Treatment of generalized pustular psoriasis of pregnancy with infliximab. Cutis. 2021;107(3):E2–E5. doi:10.12788/cutis.0210
56. Babuna Kobaner G, Polat Ekinci A. Infliximab for the treatment of recalcitrant generalized pustular psoriasis of pregnancy: report of a challenging case. Dermatol Ther. 2020;33(4):e13571. doi:10.1111/dth.13571
57. Sheth N, Greenblatt DT, Acland K, Barker J, Teixeira F. Generalized pustular psoriasis of pregnancy treated with infliximab. Clin Exp Dermatol. 2009;34(4):521–522. doi:10.1111/j.1365-2230.2008.02963.x
58. Lu J, Li Y, Yu N, Chen F, Ding Y, Yi X. Successful treatment of juvenile generalized pustular psoriasis with infliximab therapy: two case reports. J Int Med Res. 2020;48(3):300060520912091. doi:10.1177/0300060520912091
59. Tsang V, Dvorakova V, Enright F, Murphy M, Gleeson C. Successful use of infliximab as first line treatment for severe childhood generalized pustular psoriasis. J Eur Acad Dermatol Venereol. 2016;30(11):e117–e119. doi:10.1111/jdv.13388
60. Skrabl-Baumgartner A, Weger W, Salmhofer W, Jahnel J. Childhood generalized pustular psoriasis: longtime remission with combined infliximab and methotrexate treatment. Pediatr Dermatol. 2015;32(1):e13–4. doi:10.1111/pde.12457
61. Pan J, Qiu L, Xiao T, Chen HD. Juvenile generalized pustular psoriasis with IL36RN mutation treated with short-term infliximab. Dermatol Ther. 2016;29(3):164–167. doi:10.1111/dth.12325
62. Thurber M, Feasel A, Stroehlein J, Hymes SR. Pustular psoriasis induced by infliximab. J Drugs Dermatol. 2004;3(4):439–440.
63. Martínez-Morán C, Sanz-Muñoz C, Morales-Callaghan AM, Torrero V, Miranda-Romero A. Pustular psoriasis induced by infliximab. J Eur Acad Dermatol Venereol. 2007;21(10):1424–1426. doi:10.1111/j.1468-3083.2007.02230.x
64. Pourciau C, Shwayder T. Occurrence of pustular psoriasis after treatment of Crohn disease with infliximab. Pediatr Dermatol. 2010;27(5):539–540. doi:10.1111/j.1525-1470.2010.01267.x
65. Kato Y, Yamamoto T. Generalized pustular psoriasis triggered by infliximab in two patients with Crohn’s disease. J Dermatol. 2013;40(11):932–933. doi:10.1111/1346-8138.12268
66. Almutairi D, Sheasgreen C, Weizman A, Alavi A. Generalized pustular psoriasis induced by infliximab in a patient with inflammatory bowel disease. J Cutan Med Surg. 2018;22(5):507–510. doi:10.1177/1203475418758986
67. Zheng J, Gao Y, Ding Y. Successful management of infliximab-induced generalized pustular psoriasis without therapy discontinuation in a patient with psoriatic arthritis. Dermatol Ther. 2019;32(6):e13132. doi:10.1111/dth.13132
68. Xia P, Li YH, Liu Z, et al. Recalcitrant paradoxical pustular psoriasis induced by infliximab: two case reports. World J Clin Cases. 2021;9(15):3655–3661. doi:10.12998/wjcc.v9.i15.3655
69. Strain J, Leis M, Lee KO, Fleming P. Certolizumab pegol in plaque psoriasis: considerations for pregnancy. Skin Therapy Lett. 2021;26(2):1–5.
70. Okubo Y, Umezawa Y, Sakurai S, Hoshii N, Nakagawa H. Efficacy and safety of certolizumab pegol in Japanese patients with generalized pustular psoriasis and erythrodermic psoriasis: 52-week results. Dermatol Ther. 2022;12(6):1397–1415. doi:10.1007/s13555-022-00741-x
71. Yatsuzuka K, Matsumoto T, Sakane Y, et al. The use of certolizumab pegol to successfully treat generalized pustular psoriasis combined with psoriatic uveitis. J Dermatol. 2022. doi:10.1111/1346-8138.16704
72. Mizutani Y, Mizutani YH, Matsuyama K, et al. Generalized pustular psoriasis in pregnancy, successfully treated with certolizumab pegol. J Dermatol. 2020;47(7):e262–e263. doi:10.1111/1346-8138.15355
73. Yiu ZZ, Warren RB. Ustekinumab for the treatment of psoriasis: an evidence update. Semin Cutan Med Surg. 2018;37(3):143–147. doi:10.12788/j.sder.2018.040
74. Daudén E, Santiago-et-Sánchez-Mateos D, Sotomayor-López E, García-Díez A. Ustekinumab: effective in a patient with severe recalcitrant generalized pustular psoriasis. Br J Dermatol. 2010;163(6):1346–1347. doi:10.1111/j.1365-2133.2010.09995.x
75. Storan ER, O’Gorman SM, Markham T. Generalized pustular psoriasis treated with ustekinumab. Clin Exp Dermatol. 2016;41(6):689–690. doi:10.1111/ced.12868
76. Hay RAS, Pan JY. Paradoxical flare of pustular psoriasis triggered by ustekinumab, which responded to Adalimumab therapy. Clin Exp Dermatol. 2014;39(6):751–752. doi:10.1111/ced.12392
77. Caca-Biljanovska N, V’lckova-Laskoska M, Laskoski D. Successful management of ustekinumab-induced pustular psoriasis without therapy discontinuation. Acta Dermatovenerol Croat. 2013;21(3):202–204.
78. Wenk KS, Claros JM, Ehrlich A. Flare of pustular psoriasis after initiating ustekinumab therapy. J Dermatolog Treat. 2012;23(3):212–214. doi:10.3109/09546634.2010.534430
79. Gregoriou S, Kazakos C, Christofidou E, Kontochristopoulos G, Vakis G, Rigopoulos D. Pustular psoriasis development after initial ustekinumab administration in chronic plaque psoriasis. Eur J Dermatol. 2011;21(1):104–105. doi:10.1684/ejd.2011.1164
80. Benzaquen M, Flachaire B, Rouby F, Berbis P, Guis S. Paradoxical pustular psoriasis induced by ustekinumab in a patient with Crohn’s disease-associated spondyloarthropathy. Rheumatol Int. 2018;38(7):1297–1299. doi:10.1007/s00296-018-4034-0
81. Megna M, Potestio L, Camela E, Fabbrocini G, Ruggiero A. Ixekizumab and brodalumab indirect comparison in the treatment of moderate to severe psoriasis: results from an Italian single-center retrospective study in a real-life setting. Dermatol Ther. 2022;35:e15667. doi:10.1111/dth.15667
82. Saeki H, Nakagawa H, Nakajo K, et al. Efficacy and safety of ixekizumab treatment for Japanese patients with moderate to severe plaque psoriasis, erythrodermic psoriasis and generalized pustular psoriasis: results from a 52-week, open-label, phase 3 study (UNCOVER-J). J Dermatol. 2017;44(4):355–362. doi:10.1111/1346-8138.13622
83. Saeki H, Nakagawa H, Ishii T, et al. Efficacy and safety of open-label ixekizumab treatment in Japanese patients with moderate-to-severe plaque psoriasis, erythrodermic psoriasis and generalized pustular psoriasis. J Eur Acad Dermatol Venereol. 2015;29(6):1148–1155. doi:10.1111/jdv.12773
84. Okubo Y, Mabuchi T, Iwatsuki K, et al. Long-term efficacy and safety of ixekizumab in Japanese patients with erythrodermic or generalized pustular psoriasis: subgroup analyses of an open-label, phase 3 study (UNCOVER-J). J Eur Acad Dermatol Venereol. 2019;33(2):325–332. doi:10.1111/jdv.15287
85. Egawa G, Honda T, Kabashima K. Long-term efficacy of ixekizumab in erythrodermic and generalized pustular psoriasis patients. J Eur Acad Dermatol Venereol. 2019;33(2):259. doi:10.1111/jdv.15416
86. Nagata M, Kamata M, Fukaya S, et al. Real-world single-center experience with 10 cases of generalized pustular psoriasis successfully treated with ixekizumab. J Am Acad Dermatol. 2020;82(3):758–761. doi:10.1016/j.jaad.2019.09.040
87. Morita A, Okubo Y, Morisaki Y, Torisu-Itakura H, Umezawa Y. Ixekizumab 80 mg every 2 weeks treatment beyond week 12 for Japanese patients with generalized pustular psoriasis and erythrodermic psoriasis. Dermatol Ther. 2022;12(2):481–494. doi:10.1007/s13555-021-00666-x
88. Burlando M, Salvi I, Paravisi A, Cozzani E, Parodi A. Severe generalized pustular psoriasis successfully treated with ixekizumab: a case report. Case Rep Dermatol. 2022;14(3):326–329. doi:10.1159/000526037
89. Huang D, Liu T, Li J, Lu Y, Ma H. Generalized pustular psoriasis recurring during pregnancy and lactation successfully treated with ixekizumab. Dermatol Ther. 2022;35(12):e15878. doi:10.1111/dth.15878
90. Dattola A, Manfreda V, Esposito M, Bianchi L, Giunta A. A case of generalized pustular psoriasis and arthritis treated with ixekizumab. J Dermatolog Treat. 2020;31(7):754–755. doi:10.1080/09546634.2019.1606395
91. Megna M, Abategiovanni L, Annunziata A, et al. Generalized pustular psoriasis rapidly and successfully treated with ixekizumab in a Caucasian patient. Dermatol Ther. 2022;35(5):e15382. doi:10.1111/dth.15382
92. Ito M, Kamata M, Uchida H, et al. Ixekizumab rapidly improves inflammatory markers in patients with generalized pustular psoriasis. Br J Dermatol. 2022;187(5):793–795. doi:10.1111/bjd.21701
93. Blauvelt A. Safety of secukinumab in the treatment of psoriasis. Expert Opin Drug Saf. 2016;15(10):1413–1420. doi:10.1080/14740338.2016.1221923
94. Imafuku S, Honma M, Okubo Y, et al. Efficacy and safety of secukinumab in patients with generalized pustular psoriasis: a 52-week analysis from phase III open-label multicenter Japanese study. J Dermatol. 2016;43(9):1011–1017. doi:10.1111/1346-8138.13306
95. Böhner A, Roenneberg S, Eyerich K, Eberlein B, Biedermann T. Acute generalized pustular psoriasis treated with the IL-17A antibody secukinumab. JAMA Dermatol. 2016;152(4):482–484. doi:10.1001/jamadermatol.2015.4686
96. Reymundo A, Vilarrasa E, Baniandrés O, et al. Effectiveness and safety profile of secukinumab for the treatment of patients with generalized pustular psoriasis in daily practice. J Eur Acad Dermatol Venereol. 2022;36(10):e849–e851. doi:10.1111/jdv.18317
97. Wu X, Yan T, Han C, et al. Rapid and sustained response of acute generalized pustular psoriasis of von Zumbusch to Secukinumab. J Eur Acad Dermatol Venereol. 2023;37(3):e338–e341. doi:10.1111/jdv.18609
98. Sun ZL, Liu ZL, Xu YY, Zhang XL, Zhang CL, Guan X. Successful treatment of generalized pustular psoriasis with secukinumab: a report of two cases. Chin Med J. 2020;133(24):3015–3016. doi:10.1097/CM9.0000000000001244
99. Akaji K, Nakagawa Y, Kakuda K, et al. Generalized pustular psoriasis associated with systemic lupus erythematosus successfully treated with secukinumab. J Dermatol. 2021;48(1):e43–e44. doi:10.1111/1346-8138.15645
100. Gabeff R, Safar R, Leducq S, et al. Successful therapy with secukinumab in a patient with generalized pustular psoriasis carrying homozygous IL36RN p.His32Arg mutation. Int J Dermatol. 2019;58(1):e16–e17. doi:10.1111/ijd.14293
101. Mugheddu C, Atzori L, Lappi A, Pau M, Murgia S, Rongioletti F. Successful Secukinumab treatment of generalized pustular psoriasis and erythrodermic psoriasis. J Eur Acad Dermatol Venereol. 2017;31(9):e420–e421. doi:10.1111/jdv.14234
102. Polesie S, Lidholm AG. Secukinumab in the treatment of generalized pustular psoriasis: a case report. Acta Derm Venereol. 2017;97(1):124–125. doi:10.2340/00015555-2467
103. Liu N, Zhu L, Cheng Y, Yu N, Yi X, Ding Y. Successful treatment of recurrent pustular psoriasis of pregnancy with secukinumab: a case report. Acta Derm Venereol. 2020;100(15):adv00251. doi:10.2340/00015555-3611
104. Xue G, Lili M, Yimiao F, Miao W, Xiaohong Y, Dongmei W. Case report: successful treatment of acute generalized pustular psoriasis of puerperium with secukinumab. Front Med. 2022;9:1072039. doi:10.3389/fmed.2022.1072039
105. Ruan SF, Zhang LL, Liu Z, et al. Real-world data on the clinical use of secukinumab in pediatric generalized pustular psoriasis: a 48-week retrospective study. J Am Acad Dermatol. 2023;88(1):243–246. doi:10.1016/j.jaad.2022.04.064
106. Miao C, Chen Y, Wang Z, Xiang X, Liu Y, Xu Z. Real-world data on the use of secukinumab and Acitretin in pediatric generalized pustular psoriasis. J Dermatol. 2023;50(2):258–261. doi:10.1111/1346-8138.16551
107. Zhu H, Song P, Du D, Tian H. Successful treatment of a 3-year-old girl with generalized pustular psoriasis using secukinumab monotherapy. Pediatr Dermatol. 2021;38(5):1366–1367. doi:10.1111/pde.14795
108. Nishida M, Takeichi T, Kono M, et al. Successful secukinumab treatment of recalcitrant juvenile generalized pustular psoriasis. J Dermatol. 2020;47(3):e77–e78. doi:10.1111/1346-8138.15228
109. Guevara BEK, Aquino JMRM, Diaz RBS, et al. Infantile generalized pustular psoriasis with excellent response to secukinumab: a case report. Exp Dermatol. 2023. doi:10.1111/exd.14784
110. López-Sánchez C, Falla LM, Roé-Crespo E, et al. Excellent response to secukinumab in an infant with severe generalized pustular psoriasis. J Dermatol. 2021;48(6):907–910. doi:10.1111/1346-8138.15673
111. Albela H, Begum S, Leong KF. Successful treatment of paediatric generalized pustular psoriasis with secukinumab: a case series. J Dermatolog Treat. 2022;33(3):1769–1773. doi:10.1080/09546634.2021.1899111
112. Dogra S, Bishnoi A, Narang T, Handa S. Secukinumab-induced paradoxical pustular psoriasis. Clin Exp Dermatol. 2019;44(1):72–73. doi:10.1111/ced.13731
113. Abbruzzese A, Venerito V, Lopalco G, Fornaro M, Giannotta M, Iannone F. Paradoxical pustular psoriasis in a patient with psoriatic arthritis on secukinumab treatment. J Clin Rheumatol Pract Rep Rheum Musculoskelet Dis. 2020;26(6):e208–e209. doi:10.1097/RHU.0000000000001076
114. Iznardo H, Puig L. The safety of brodalumab for the treatment of psoriasis. Expert Opin Drug Saf. 2020;19(4):365–372. doi:10.1080/14740338.2020.1730326
115. Yamasaki K, Nakagawa H, Kubo Y, Ootaki K. Efficacy and safety of brodalumab in patients with generalized pustular psoriasis and psoriatic erythroderma: results from a 52-week, open-label study. Br J Dermatol. 2017;176(3):741–751. doi:10.1111/bjd.14702
116. Khemis A, Cavalié M, Montaudié H, Lacour JP, Passeron T. Rebound pustular psoriasis after brodalumab discontinuation. Br J Dermatol. 2016;175(5):1065–1066. doi:10.1111/bjd.14627
117. Ruggiero A, Potestio L, Camela E, Fabbrocini G, Megna M. Bimekizumab for the treatment of psoriasis: a review of the current knowledge. Psoriasis. 2022;12:127–137. doi:10.2147/PTT.S367744
118. Megna M, Battista T, Potestio L, et al. A case of erythrodermic psoriasis rapidly and successfully treated with Bimekizumab. J Cosmet Dermatol. 2023;22(3):1146–1148. doi:10.1111/jocd.15543
119. Ruggiero A, Potestio L, Martora F, Villani A, Comune R, Megna M. Bimekizumab treatment in patients with moderate to severe plaque psoriasis: a drug safety evaluation. Expert Opin Drug Saf. 2023;1–8. doi:10.1080/14740338.2023.2218086
120. Shukuin R, Koizumi H, Ebata A, et al. Successful combination therapy of bimekizumab and granulocyte monocyte adsorption apheresis for generalized pustular psoriasis complicated with microscopic polyangiitis. J Dermatol. 2023;50. doi:10.1111/1346-8138.16707
121. Megna M, Potestio L, Ruggiero A, Camela E, Fabbrocini G. Guselkumab is efficacious and safe in psoriasis patients who failed anti-IL17: a 52-week real-life study. J Dermatolog Treat. 2022;1–18. doi:10.1080/09546634.2022.2036674
122. Megna M, Potestio L, Fabbrocini G, Ruggiero A. Long-term efficacy and safety of guselkumab for moderate to severe psoriasis: a 3-year real-life retrospective study. Psoriasis. 2022;12:205–212. doi:10.2147/PTT.S372262
123. Megna M, Tommasino N, Potestio L, et al. Real-world practice indirect comparison between guselkumab, risankizumab, and tildrakizumab: results from an Italian 28-week retrospective study. J Dermatolog Treat. 2022:1–8. doi:10.1080/09546634.2022.2081655
124. Sano S, Kubo H, Morishima H, Goto R, Zheng R, Nakagawa H. Guselkumab, a human interleukin-23 monoclonal antibody in Japanese patients with generalized pustular psoriasis and erythrodermic psoriasis: efficacy and safety analyses of a 52-week, phase 3, multicenter, open-label study. J Dermatol. 2018;45(5):529–539. doi:10.1111/1346-8138.14294
125. Ruggiero A, Camela E, Potestio L, Fabbrocini G, Megna M. Drug safety evaluation of tildrakizumab for psoriasis: a review of the current knowledge. Expert Opin Drug Saf. 2022;21(12):1445–1451. doi:10.1080/14740338.2022.2160447
126. Megna M, Potestio L, Fabbrocini G, Cinelli E. Tildrakizumab: a new therapeutic option for erythrodermic psoriasis? Dermatol Ther. 2021;34:e15030. doi:10.1111/dth.15030
127. Ruggiero A, Potestio L, Cacciapuoti S, et al. Tildrakizumab for the treatment of moderate to severe psoriasis: results from a single center preliminary real-life study. Dermatol Ther. 2022;35(12):e15941. doi:10.1111/dth.15941
128. Ruggiero A, Fabbrocicni G, Cacciapuoti S, Potestio L, Gallo L, Megna M. Tildrakizumab for the treatment of moderate-to-severe psoriasis: results from 52 weeks real-life retrospective study. Clin Cosmet Investig Dermatol. 2023;16:529–536. doi:10.2147/CCID.S402183
129. Megna M, Potestio L, Ruggiero A, Camela E, Fabbrocini G. Risankizumab treatment in psoriasis patients who failed anti-IL17: a 52-week real-life study. Dermatol Ther. 2022;35(7):e15524. doi:10.1111/dth.15524
130. Megna M, Ruggiero A, Battista T, Marano L, Cacciapuoti S, Potestio L. Long-term efficacy and safety of risankizumab for moderate to severe psoriasis: a 2-year real-life retrospective study. J Clin Med. 2023;12(9):3233. doi:10.3390/jcm12093233
131. Yamanaka K, Okubo Y, Yasuda I, Saito N, Messina I, Morita A. Efficacy and safety of risankizumab in Japanese patients with generalized pustular psoriasis or erythrodermic psoriasis: primary analysis and 180-week follow-up results from the phase 3, multicenter IMMspire study. J Dermatol. 2023;50(2):195–202. doi:10.1111/1346-8138.16667
132. Pavia G, Gargiulo L, Spinelli F, et al. Generalized pustular psoriasis flare in a patient affected by plaque psoriasis after BNT162b2 mRNA COVID-19 vaccine, successfully treated with risankizumab. J Eur Acad Dermatol Venereol. 2022;36(7):e502–e505. doi:10.1111/jdv.18032
133. Heyer S, Seiringer P, Eyerich S, et al. Acute generalized pustular psoriasis successfully treated with the IL-23p19 antibody risankizumab. J Ger Soc Dermatol JDDG. 2022;20(10):1362–1364. doi:10.1111/ddg.14857
134. McFeely O, Pender E, Victory L, Almutlaq H, Storan E. Risankizumab-induced paradoxical pustular psoriasis. Clin Exp Dermatol. 2022;47(3):616–617. doi:10.1111/ced.15006
135. Johnston A, Xing X, Wolterink L, et al. IL-1 and IL-36 are dominant cytokines in generalized pustular psoriasis. J Allergy Clin Immunol. 2017;140(1):109–120. doi:10.1016/j.jaci.2016.08.056
136. Blair HA. Spesolimab: first approval. Drugs. 2022;82(17):1681–1686. doi:10.1007/s40265-022-01801-4
137. Bachelez H, Choon SE, Marrakchi S, et al. Trial of spesolimab for generalized pustular psoriasis. N Engl J Med. 2021;385(26):2431–2440. doi:10.1056/NEJMoa2111563
138. Morita A, Choon SE, Bachelez H, et al. Design of effisayilTM 2: a randomized, double-blind, placebo-controlled study of spesolimab in preventing flares in patients with generalized pustular psoriasis. Dermatol Ther. 2023;13(1):347–359. doi:10.1007/s13555-022-00835-6
139. Müller VL, Kreuter A. [Remission of recalcitrant generalized pustular psoriasis under interleukin-36 receptor inhibitor spesolimab]. Dermatologie. 2023:1–4. German. doi:10.1007/s00105-023-05140-7
140. Ran D, Yang B, Sun L, et al. Rapid and sustained response to Spesolimab in five Chinese patients with generalized pustular psoriasis. Clin Exp Dermatol. 2023. doi:10.1093/ced/llad108
141. Marasca C, Fornaro L, Martora F, Picone V, Fabbrocini G, Megna M. Onset of vitiligo in a psoriasis patient on ixekizumab. Dermatol Ther. 2021;34(5):e15102. doi:10.1111/dth.15102
142. Ruggiero A, Picone V, Martora F, Fabbrocini G, Megna M. Guselkumab, risankizumab, and tildrakizumab in the management of psoriasis: a review of the real-world evidence. Clin Cosmet Investig Dermatol. 2022;15:1649–1658. doi:10.2147/CCID.S364640
143. Camela E, Potestio L, Fabbrocini G, Pallotta S, Megna M. The holistic approach to psoriasis patients with comorbidities: the role of investigational drugs. Expert Opin Investig Drugs. 2023;1–16. doi:10.1080/13543784.2023.2219387
144. Ruggiero A, Martora F, Picone V, et al. The impact of COVID-19 infection on patients with psoriasis treated with biologics: an Italian experience. Clin Exp Dermatol. 2022;47:2280–2282. doi:10.1111/ced.15336
145. Megna M, Potestio L, Battista T, et al. Immune response to Covid-19 mRNA vaccination in psoriasis patients undergoing treatment with biologics. Clin Exp Dermatol. 2022;47:2310–2312. doi:10.1111/ced.15395
146. Megna M, Camela E, Villani A, Tajani A, Fabbrocini G, Potestio L. Teledermatology: a useful tool also after COVID-19 era? J Cosmet Dermatol. 2022;21(6):2309–2310. doi:10.1111/jocd.14938
147. De Lucia M, Potestio L, Costanzo L, Fabbrocini G, Gallo L. Scabies outbreak during COVID-19: an Italian experience. Int J Dermatol. 2021;60(10):1307–1308. doi:10.1111/ijd.15809
148. Marasca C, Annunziata MC, Camela E, et al. Teledermatology and inflammatory skin conditions during COVID-19 era: new perspectives and applications. J Clin Med. 2022;11(6):1511. doi:10.3390/jcm11061511
149. Bellinato F, Gisondi P, Marzano AV, et al. Characteristics of patients experiencing a flare of generalized pustular psoriasis: a multicenter observational study. Vaccines. 2023;11(4):740. doi:10.3390/vaccines11040740
150. Megna M, Ocampo-Garza SS, Potestio L, et al. New-onset psoriatic arthritis under biologics in psoriasis patients: an increasing challenge? Biomedicines. 2021;9(10):1482. doi:10.3390/biomedicines9101482
151. Young KZ, Sarkar MK, Gudjonsson JE. Pathophysiology of generalized pustular psoriasis. Exp Dermatol. 2023. doi:10.1111/exd.14768
152. Camela E, Potestio L, Fabbrocini G, Ruggiero A, Megna M. New frontiers in personalized medicine in psoriasis. Expert Opin Biol Ther. 2022;1–3. doi:10.1080/14712598.2022.2113872
153. Kodali N, Blanchard I, Kunamneni S, Lebwohl MG. Current management of generalized pustular psoriasis. Exp Dermatol. 2023. doi:10.1111/exd.14765
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.