Back to Journals » Clinical, Cosmetic and Investigational Dentistry » Volume 18
Use of a Customized Milled Metal Surgical Guide for Esthetic Crown Lengthening: A Case Report
Authors Alhumaidan A, Fita S ![]()
Received 5 May 2026
Accepted for publication 13 June 2026
Published 23 June 2026 Volume 2026:18 622098
DOI https://doi.org/10.2147/CCIDE.S622098
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Christopher E. Okunseri
Abdulkareem Alhumaidan, Sarah Fita
Department of Preventive Dental Sciences, College of Dentistry, Imam Abdulrahman Bin Faisal University, Dammam, Saudi Arabia
Correspondence: Sarah Fita, Department of Preventive Dental Sciences, College of Dentistry, Imam Abdulrahman Bin Faisal University, Dammam, Saudi Arabia, Email [email protected]
Purpose: Excessive gingival display (EGD) resulting from altered passive eruption (APE) is a clinical condition that is commonly managed by esthetic crown lengthening to achieve stable and symmetrical gingival margins. Determining the appropriate gingival and osseous resection levels remains a key step in achieving predictable surgical outcomes. Although digitally printed resin guides have been widely discussed, clinical data regarding milled metal dual-purpose guides remain limited.
Patients and Methods: This single case report (n=1) describes the digital workflow for designing and fabricating a dual-purpose cobalt–chromium surgical guide to assist both gingivectomy and osteoectomy. The guide dimensions were determined by superimposing cone-beam computed tomography (CBCT) data with intraoral scan files to identify the cementoenamel junction (CEJ). The guide was fabricated using a subtractive milling process and used during esthetic crown lengthening in a patient diagnosed with altered passive eruption type I.
Results: The milled metal guide appeared to provide stable positioning during surgery and helped guide both soft- and hard-tissue resection. At 6-month follow-up, gingival margins remained stable, symmetrical contouring was achieved, patient satisfaction was high, and no immediate postoperative complications were observed.
Conclusion: This report presents a CBCT-integrated workflow for dual-purpose surgical guidance. The rigidity of the milled metal framework may assist intraoperative stability and support favorable short-term clinical outcomes in this case.
Keywords: cone-beam computed tomography, CAD/CAM, digital workflow, crown lengthening, guided surgery, milled metal guide
Introduction
Excessive gingival display (EGD) is a multifactorial condition that requires accurate diagnosis and precise treatment planning to achieve stable and esthetic outcomes.1 Altered passive eruption (APE) represents one of the most common etiological factors contributing to EGD and is commonly managed through esthetic crown-lengthening procedures.2 Depending on the clinical presentation, esthetic crown lengthening may involve gingivectomy alone or a combination of soft- and hard-tissue resection, including apically positioned flap surgery and osseous reduction.2 Despite its routine application, esthetic crown lengthening remains a technically demanding procedure, with potential risks of gingival margin relapse or postoperative recession if soft- and hard-tissue reduction is not accurately planned and executed.3,4 Postoperative rebound and recession were found associated with anatomic factors such as periodontal phenotype; where thick phenotype was more likely to present with rebound at 1-year follow-up.5 In addition, operator factors play a role where experienced periodontists tend to remove more bone; and still not as preoperatively planned.6 Additionally, surgical technique such as flap repositioning in relation to the bone crest is associated with the amount of tissue rebound at 6 months.7
To help address these multiple variables; surgical guides have been introduced to improve intraoperative precision and reduce operator-dependent variability during esthetic crown-lengthening procedures.1 Conventional approaches include bone sounding, bleeding points, surgical gauges, and reliance on restorative reference points, while custom-designed surgical guides—either manually fabricated or digitally planned—have been introduced to assist clinicians in achieving more controlled gingival and osseous reduction.1 Such guides may be intended to assist gingivectomy alone (single-purpose) or both gingivectomy and osteoectomy (dual-purpose).
Digital guides can be produced using additive manufacturing (three-dimensional printing) or subtractive manufacturing (milling) and fabricated from a range of materials including resin, polymer, ceramic, or metal.1 Recent studies have demonstrated that digitally guided crown-lengthening procedures can improve the accuracy of gingival and bone reduction compared with freehand techniques and may reduce operative time.8,9 However, most of the available evidence focuses on three-dimensionally printed resin guides, while data regarding the clinical application of milled guides—particularly those fabricated from metal—remain limited. Reports describing their use in routine clinical settings are still scarce.
Therefore, the aim of this case report is to present the design and clinical application of a CBCT-based, dual-purpose milled metal surgical guide for esthetic crown lengthening. This guide integrates both CBCT and intraoral scan data to enable simultaneous planning of soft- and hard-tissue resection within a single device. The report describes the digital workflow, surgical application, and short-term clinical outcome of this approach in a patient with altered passive eruption.
Materials and Methods
Case Summary
A 29-year-old female patient presented to the College of Dentistry clinics at Imam Abdulrahman Bin Faisal University with a complaint of “gummy smile.” Upon initial examination, the patient did not show any gingival tissue at rest; however, during a full smile, 2 mm of gingival display was visible below the lower border of the maxillary lip, along with square-shaped teeth (Figure 1). The medical history was non-contributory, while dental history revealed that the patient had completed orthodontic alignment with clear aligner therapy 6 months earlier. Furthermore, there were no significant findings on the extraoral examination, and the patient was generally symmetrical.
 |
Figure 1 Preoperative frontal view showing short clinical crown and excessive gingival display. |
Specific diagnostic measurements were conducted clinically and radiographically to arrive at the diagnosis of the patient’s chief complaint (Table 1). Lip mobility was assessed by measuring the vertical distance from the inferior border of the upper lip to the incisal edge of the maxillary central incisors at rest and during a full smile. The difference between the two measurements was recorded as lip mobility. A CBCT scan (CS 9300, Carestream Health Inc., USA) was acquired to analyze the level of the alveolar bone crest in relation to the cementoenamel junction. The radiographic parameters were set at 90 kVp/4 mA/s, with voxel size 200 µm, according to the manufacturer’s exposure settings, with a field of view of 10×5 cm (diameter × height). The distance between the bone crest and the cementoenamel junction was measured at the sagittal cross-section of the maxillary anterior teeth (Figure 2). The midfacial distance between the CEJ and bone crest ranged between 1.5–2 mm. However, the bone crest at the line angles was located at or within approximately 0.5 mm of the CEJ, resulting in an uneven osseous architecture.
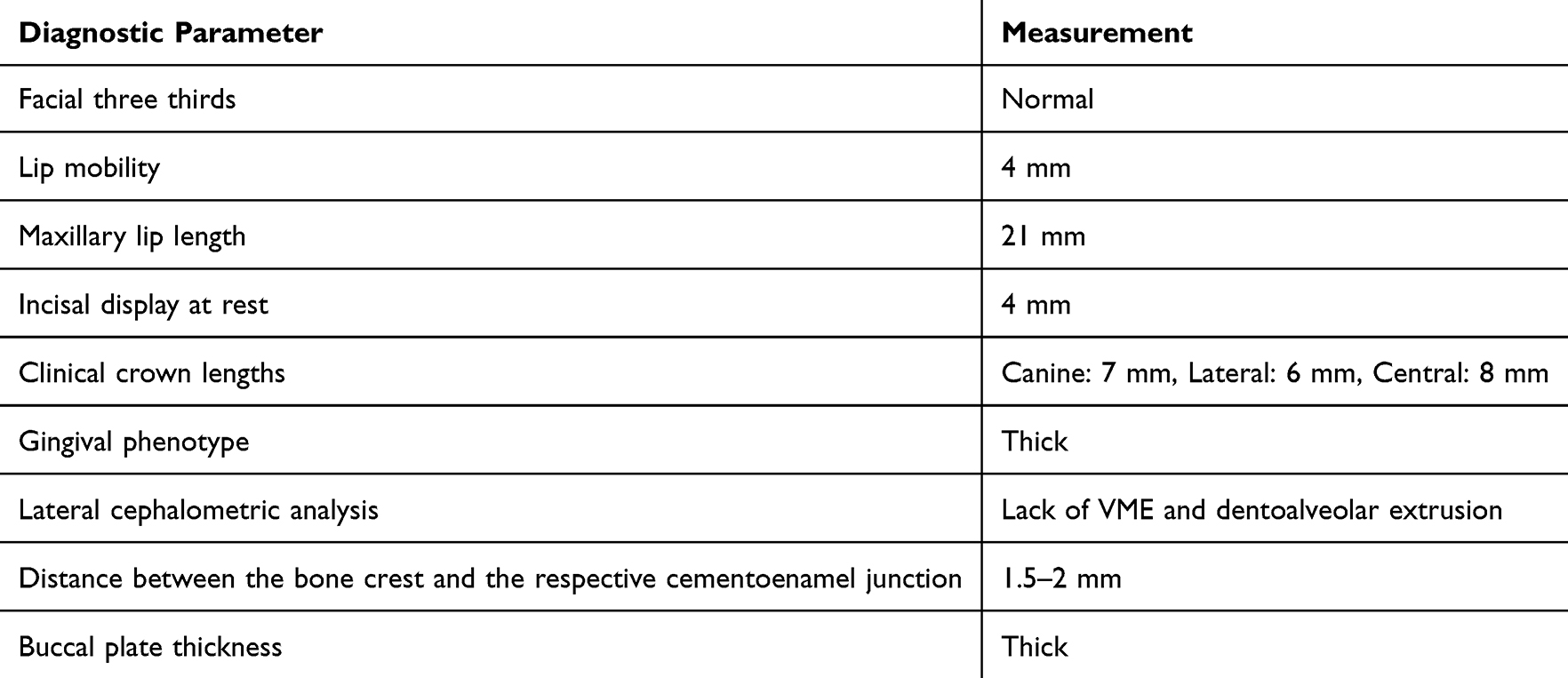 |
Table 1 Preoperative Clinical and Radiographic Measurements |
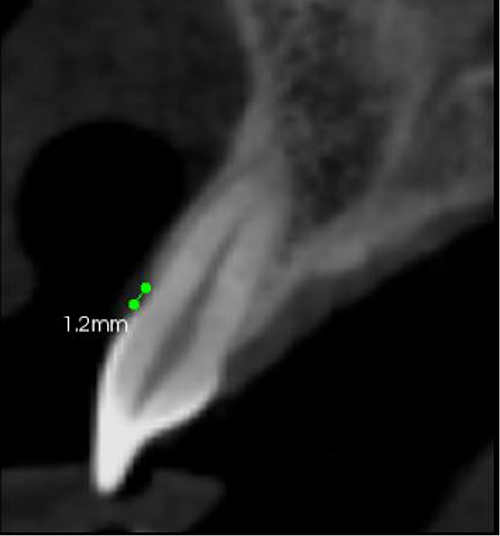 |
Figure 2 Distance from cementoenamel junction to facial bone crest as measured on cone-beam computed tomography (CBCT). |
Based on the clinical findings, short clinical crowns, and the square-shaped appearance of the teeth, the patient was diagnosed with excessive gingival display associated with altered passive eruption (Coslet Type IA).2 Treatment options were discussed with the patient, and esthetic crown lengthening with bone resection was proposed. This case report was conducted in accordance with the Declaration of Helsinki and approved by the Institutional Review Board of Imam Abdulrahman Bin Faisal University (Approval No. IRB-2025-02-0886). Written informed consent was obtained from the patient to perform the surgical procedure and separate consent for publication of this case report and accompanying images. The clinical timeline included surgical treatment at baseline, followed by postoperative evaluations at 2 weeks (suture removal), 4 weeks, 3 months, and 6 months, at which time final assessment of gingival margin stability, symmetry, and esthetic outcome was performed.
Design and Milling of Surgical Guide
An intraoral scanner (TRIOS, 3Shape, Denmark) was acquired to aid in fabricating a surgical guide. Digital Imaging and Communications in Medicine (DICOM) files were converted to Standard Tessellation Language (STL) format and then superimposed with STL files acquired from the intraoral scan using an implant planning software (coDiagnostiX 9.7, Dental Wings Inc., Canada).
Using a dental CAD software (3Shape Premium Dental System, 3Shape, Denmark), the level of the cementoenamel junction was marked (Figures 3 and 4) to guide the gingivectomy incision line, followed by a second line 3 mm apical to the cementoenamel junction to guide bone resection. The virtual design of the surgical guide was then completed. The surgical guide framework was fabricated using a cobalt–chromium dental alloy (BEGO, Germany) using a metal laser-sintering system (Profeta, Italy). The guide design incorporated three stabilization points to provide a tripodal effect. These consisted of rest seats located on the maxillary right and left first molars, in addition to an anterior stabilization point positioned between the maxillary central incisors. Prior to surgery, the guide was verified for fit and stability on the cast (Figure 5), then sterilized using a standard steam autoclave protocol prior to surgery and was verified for fit and stability intraorally (Figure 6). The planned gingivectomy was also measured as the visible amount when guide is seated intraorally, then cross-referenced with the digital plan.
 |
Figure 3 Digital workflow of dimensions calculation and guide fabrication: intraoral scan superimposed on the bone model from the CBCT. The measurement shows the distance from CEJ to the bone crest to guide the gingivectomy incision line. |
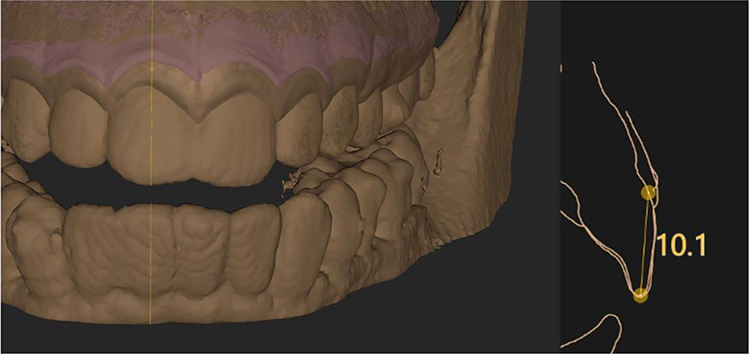 |
Figure 4 Digital workflow of dimensions calculation and guide fabrication: intraoral scan superimposed on the bone model from the CBCT with measurement showing the anatomic crown length—distance from incisal edge to CEJ. |
 |
Figure 5 Milled surgical guide. |
 |
Figure 6 Preoperative surgical guide. |
Surgical Procedure and Postoperative Care
Local anesthesia was administered using buccal infiltration of lidocaine with epinephrine (1:100,000). The surgical guide was then positioned intraorally, and a 15C blade was used to perform the gingivectomy incision following the inferior border of the guide. A straight internal bevel incision was extended from the maxillary first molar on one side to the contralateral first molar. The guide was subsequently removed, and a sulcular incision was performed. The excised gingival collar was removed using a Younger–Good curette, allowing visualization of the newly established clinical crown lengths (Figure 7).
 |
Figure 7 Teeth length after gingivectomy incision according to the guide. |
A full thickness mucoperiosteal flap was then elevated beyond the mucogingival junction to provide adequate access to the underlying alveolar bone (Figure 8). The surgical guide was repositioned intraorally to determine the extent of osteoectomy required. The planned level of bone removal was marked using a round carbide bur. Ostectomy was performed following the superior border of the surgical guide using an end-cutting carbide bur, followed by osteoplasty to eliminate buccal bone buttressing and achieve a physiologic osseous contour (Figure 9).
 |
Figure 8 Mucoperiosteal flap elevated. |
 |
Figure 9 Bone level after osteoectomy and osteoplasty. |
The flap was repositioned and secured using internal vertical mattress sutures placed with a monofilament non-resorbable polypropylene suture (Prolene, Ethicon Inc., USA) (Figure 10). Hemostasis was achieved, and postoperative follow-up was performed at two weeks, 4 weeks, 3 months, and 6 months (Figure 11). No clinically significant guide displacement was observed during the procedure.
 |
Figure 10 Immediate postoperative. |
 |
Figure 11 Six months postoperative visit. |
At postoperative appointments, plaque removal, suture removal, and monitoring for normal healing were performed. At the 6-month follow-up, evaluation of gingival margin stability, symmetry, and esthetic outcomes was performed and considered satisfactory by the patient.
Patient Reported Outcomes
Patient-reported outcomes were assessed at the 6-month follow-up using a previously published questionnaire evaluating patient satisfaction following crown-lengthening procedures.10 The questionnaire assessed satisfaction with smile appearance, gingival display during smiling and speaking, dental appearance, and overall treatment outcome. Responses were recorded using a five-point Likert scale ranging from “Not at all” to “Extremely”.
Results
The milled metal guide demonstrated stable intraoperative positioning and facilitated both soft- and hard-tissue resection. At 6-month follow-up, gingival margins remained stable, symmetrical contouring was achieved, and no immediate postoperative complications were observed such as infection, excessive bleeding, flap necrosis, or guide-related trauma.
At the 6-month follow-up, both clinical and patient-reported outcomes were assessed. Clinical crown lengths increased from baseline values of 7 mm, 6 mm, and 8 mm for the maxillary canines, lateral incisors, and central incisors, respectively, to 10 mm, 8 mm, and 11 mm, respectively. Patient-reported outcomes demonstrated a high level of satisfaction with the treatment. The patient reported being “Extremely satisfied” with smile appearance, gingival display during speech, tooth size, tooth shape, and the overall treatment outcome, and “Very satisfied” with the amount of gingival display during smiling and the amount of tooth display during smiling and speaking.
Discussion
Crown-lengthening procedures are associated with variable soft-tissue responses, including gingival rebound or recession. These possible outcomes are influenced by biologic width re-establishment, surgical technique, flap management, and the accuracy of soft- and hard-tissue resection.5 Inaccurate determination of gingival and osseous reduction levels may compromise esthetic outcomes and long-term stability. To address these challenges, surgical guides have been introduced to improve intraoperative precision and reduce operator-dependent variability during esthetic crown-lengthening procedures.1
The evolution of guidance methods for crown lengthening has progressed from indirect clinical references, such as bleeding points and periodontal probing, to the use of surgical gauges and vacuum-formed templates, and more recently to digitally designed guides. Digital guides may be configured as single guides to direct gingivectomy alone or as dual guides to control both gingival and osseous resection.1 Several studies have demonstrated that digitally guided crown-lengthening procedures can improve the accuracy of soft- and hard-tissue reduction compared with freehand approaches, while also reducing operative time. However, most reported digital workflows rely on three-dimensionally printed resin guides.9–11
Although printed resin guides offer advantages in accessibility and cost, their mechanical properties may limit performance during combined soft- and hard-tissue surgery. Reported limitations, primarily derived from implant-guided surgery literature, include reduced rigidity, dimensional instability, and susceptibility to deformation under functional or mechanical stress.12,13 In the context of crown lengthening, these limitations may affect guide stability during flap elevation and osteoectomy, particularly when rotary instruments are used in close proximity to the guide surface.
The present clinical report demonstrates the application of a CBCT-based, dual-purpose milled metal surgical guide designed to guide both gingivectomy and osteoectomy during esthetic crown lengthening. The material properties of metal contribute to the clinical performance of the guide. Increased structural rigidity may allow the guide to maintain its intended geometry throughout the surgical procedure, which contributes to stable intraoral positioning without perceptible movement. In addition, resistance to rotary cutting instruments may allow the guide to function as a physical reference during bone resection without apparent risk of damage or distortion.
From a clinical standpoint, the smooth surface finish and color contrast of the metal guide relative to surrounding soft tissues enhanced intraoperative visibility, even in the presence of bleeding. This may facilitate clear identification of the planned gingival and osseous resection boundaries and support controlled execution of the surgical steps. Furthermore, the durability of the milled metal guide allowed repeated insertion and removal during the procedure without loss of accuracy, which may contribute to improved workflow efficiency.
While the advantages of metal surgical guides have been described in computer-guided implant surgery,13 their application in esthetic crown-lengthening procedures has been limited. This report describes the design and short-term clinical performance of a dual-purpose milled metal guide for crown-lengthening surgery. At six months of follow-up, stable gingival margins and satisfactory esthetic outcomes were observed, suggesting that controlled soft- and hard-tissue resection may contribute to favorable early outcomes in this case. Furthermore, the favorable patient-reported outcomes observed in the present case are consistent with previous findings by Enfedaque-Prat et al, who reported high levels of esthetic satisfaction following guided crown-lengthening procedures.10
While the milled metal guide provided advantages such as good rigidity, stability, and visibility in this case, there are practical limitations, such as higher cost, greater fabrication complexity, and more limited availability than resin-based guides. In addition, this is a single-case report with short follow-up and long-term soft tissue stability (>1 year) was not assessed and biological width re-establishment was not confirmed radiographically. Therefore, no firm conclusions can be made about long-term soft tissue stability or comparative effectiveness. Nevertheless, the findings suggest a potential clinical role for milled metal guides in esthetic crown-lengthening procedures. Further controlled studies are needed to evaluate their performance against printed resin guides.
Conclusion
Within the limitations of a single case, the use of a customized milled metal surgical guide appeared to support controlled soft- and hard-tissue resection during esthetic crown lengthening. The described workflow may serve as a clinically applicable approach for guiding crown-lengthening procedures. Further studies are required to evaluate long-term outcomes and compare this approach with other guide materials.
Acknowledgments
The authors acknowledge Charismatic Dental Lab Dubai, lab technician Mr. Ayham Chaaban.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Alhumaidan A, Al-Qarni F, AlSharief M, AlShammasi B, Albasry Z. Surgical guides for esthetic crown lengthening procedures: periodontal and prosthetic aspects. J Am Dent Assoc. 2022;153(1):31–9. doi:10.1016/j.adaj.2021.07.005
2. Coslet JG, Vanarsdall R, Weisgold A. Diagnosis and classification of delayed passive eruption of the dentogingival junction in the adult. Alpha Omegan. 1977;70(3):24–28.
3. Dominguez E, Pascual-La Rocca A, Valles C, et al. Stability of the gingival margin after an aesthetic crown lengthening procedure in the anterior region using a replaced flap and buccal osseous surgery: a prospective study. Clin Oral Investig. 2020;24:3633–3640. doi:10.1007/s00784-020-03239-y
4. Lanning SK, Waldrop TC, Gunsolley JC, Maynard GC. Surgical crown lengthening: evaluation of the biologic width. J Clin Periodontol. 2003;30(6):468–474. doi:10.1902/jop.2003.74.4.468
5. Pontoriero R, Carnevale G. Surgical crown lengthening: a 12-month clinical wound healing study. J Periodontol. 2001;72:841–848. doi:10.1902/jop.2001.72.7.841
6. Herrero F, Scott JB, Maropis PS, Yukna RA. Clinical comparison of desired versus actual amount of surgical crown lengthening. J Periodontol. 1995;66(7):568–571. doi:10.1902/jop.1995.66.7.568
7. Deas DE, Moritz AJ, McDonnell HT, Powell CA, Mealey BL. Osseous surgery for crown lengthening: a 6-month clinical study. J Periodontol. 2004;75(9):1288–1294. doi:10.1902/jop.2004.75.9.1288
8. Li Y, Liu M, Zhou T, Lyu J, Tan J, Liu X. Accuracy of three types of digital guides for crown lengthening surgery: an in vitro study. J Dent Sci. 2024;19(1):39–45. doi:10.1016/j.jds.2023.06.007
9. Borham E, Abuel-Ela HA, Mohamed IS, Fouad YA. Treatment of excessive gingival display using conventional esthetic crown lengthening versus computer-guided esthetic crown lengthening: a randomized clinical trial. BMC Oral Health. 2024;24(1):317. doi:10.1186/s12903-024-04080-5
10. Enfedaque-Prat M, González-Barnadas A, Jorba-García A, et al. Accuracy of guided dual technique in esthetic crown lengthening: a prospective case-series study. J Esthet Restor Dent. 2025;37(6):1284–1296. doi:10.1111/jerd.13405
11. Kim J, Lin YC, Danielak M, et al. Virtual planning and rapid 3D prototyping surgical guide for anterior crown lengthening surgery: a clinical case report. J Prosthodont. 2022;31(4):275–281. doi:10.1111/jopr.13471
12. Lan D, Luo Y, Qu Y, Man Y. The three-dimensional stability and accuracy of 3D printing surgical templates: an in vitro study. J Dent. 2024;144:104936. doi:10.1016/j.jdent.2024.104936
13. Lo Russo L, Pierluigi M, Zhurakivska K, et al. Three-dimensional accuracy of surgical guides for static computer-aided implant surgery: a systematic review. Prosthesis. 2023;5(3):809–825. doi:10.3390/prosthesis5030057
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
In vitro Assessment of Open-Access Digital Workflow for Presurgical Nasoalveolar Molding in Unilateral Cleft Lip and Palate
Genovesi EA, Canallatos JE, Hulyalkar LD, Varsani RV, Makowka S, Atalla D, Arany P
Clinical, Cosmetic and Investigational Dentistry 2026, 18:588444
Published Date: 23 April 2026