Back to Journals » Journal of Multidisciplinary Healthcare » Volume 19
Usability Challenges and Safety Risks of Medical Infusion Pumps: A User-Centered Analysis Across Clinical Roles and Experience Levels in Saudi Arabia
Authors Jabali AK ![]() , Hourani RJ
, Hourani RJ
Received 20 October 2025
Accepted for publication 25 January 2026
Published 6 February 2026 Volume 2026:19 575534
DOI https://doi.org/10.2147/JMDH.S575534
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Charles V Pollack
A Karim Jabali, Rana J Hourani
Biomedical Engineering Department, Imam Abdulrahman Bin Faisal University, Dammam, Saudi Arabia
Correspondence: A Karim Jabali, Email [email protected]
Background: Medication errors involving intravenous (IV) therapy remain a major patient safety challenge. Evaluating the usability and safety of Medical Infusion Pumps (MIPs) is critical to identifying risk sources and improving clinical practice.
Objective: This study aims to characterize the types, frequencies, and severities of MIP-related medication errors in Saudi Arabia and to identify statistically significant factors associated with these errors.
Methods: A cross-sectional survey was administered to 387 healthcare providers across multiple hospitals. Participants rated the frequency and impact of 26 MIP problems across five domains. Statistical analyses included ANOVA and effect size calculations.
Results: Significant differences were found across job roles for nearly all problem classes (p < 0.05). Less experienced users reported significantly higher frequencies of Human Factors issues (p = 0.024). Specialty pumps demonstrated significantly higher User Interface problem frequencies compared with traditional pumps (p = 0.046). Pump connectivity to Hospital Information Systems (HIS) was also significantly associated with higher perceived problem frequencies across all domains (p < 0.05).
Conclusion: The findings highlight critical usability concerns—particularly related to UI design, human factors, and system integration—that significantly impact MIP safety. Targeted training for less experienced users and user-centered design improvements are essential to reducing medication errors.
Keywords: medical infusion pumps, medical errors, usability, risks, safety
Introduction
Medical infusion pumps (MIPs) are fundamental components of modern clinical care, delivering intravenous (IV) fluids, medications, and nutrients across a wide range of patient populations. Their widespread use underscores their clinical value but simultaneously raises concern about an increasing dependence on technologies that continue to introduce safety risks. Despite compliance with engineering and regulatory requirements, infusion pumps remain strongly associated with adverse events, suggesting that existing frameworks may not fully address the complexities of real-world clinical environments and human–machine interaction.1
Device recalls and incident reports consistently reveal patterns of preventable harm associated with design flaws, programming challenges, and workflow mismatches. These incidents—some resulting in serious injury or death—highlight systemic shortcomings rather than isolated technical failures. Persistent issues such as incorrect dosage settings and infusion-rate errors point to a fundamental misalignment between pump design and the cognitive and operational demands of clinical workflow.2 Regulatory initiatives, including FDA summits, continue to underscore the limitations of current mechanisms in preemptively reducing these risks.3
At the same time, research demonstrates that smart infusion pumps can offer substantial safety benefits when implemented appropriately. Several systematic reviews have shown reductions in medication administration errors, improved adherence to drug libraries, and decreased rates of high-risk infusion events through automated alerts and decision-support features.4,5 A recent systematic literature review published in 2025 further found that smart infusion pump interoperability significantly reduced medication administration errors in every included study, with improvements in dosing accuracy, automated error interception, and adherence to medication protocols when pump systems were integrated with electronic health records.6 These findings illustrate that infusion device automation can meaningfully enhance safety, reinforcing the need for a balanced evaluation that considers both risks and benefits.
International regulatory frameworks also emphasize the importance of usability engineering in reducing device-related errors. The US Food and Drug Administration (FDA) requires manufacturers to conduct robust human-factors engineering and validation testing as part of premarket submissions for infusion pumps.7 Likewise, the IEC 62366 standard specifies usability engineering processes aimed at minimizing use-related hazards and ensuring that device design aligns with clinical workflow and user needs.8 These standards highlight a global shift toward integrating human-factors principles as core components of medical device safety, further supporting the relevance of examining real-world usability challenges such as those explored in this study.
Despite regulatory advances and documented benefits, the global literature on infusion pump safety remains heavily skewed toward high-income countries. This disparity creates a notable evidence gap regarding device performance, training variability, and user challenges in developing or rapidly evolving healthcare systems. Regions such as Saudi Arabia illustrate this gap clearly, where differences in healthcare delivery models, staffing structures, multilingual clinical teams, and diverse pump brands may influence usability patterns and error risks.9 The multinational workforce in Saudi hospitals, combined with inconsistent training and variability in device familiarity, further complicates standardization and effective use of MIPs.
Alarm fatigue is another persistent and well-documented challenge across healthcare environments. The high frequency of alerts—many of which are non-actionable—contributes to clinician desensitization, delayed responses, and increased risk of overlooking critical warnings. Although widely recognized, this issue continues to occur across pump models and care settings, highlighting an ongoing disconnect between technical capability and practical usability.10
In parallel, the rapid expansion of the global infusion pump market raises additional concerns. While commercial growth is often viewed as a marker of technological advancement, it can reinforce longstanding design issues if usability challenges remain unaddressed.11 Without corresponding improvements in human-factors integration, training, and workflow alignment, new devices risk perpetuating the same limitations documented over the past decade.
Given these gaps, the present study examines the safety and usability challenges associated with MIPs within Saudi Arabian hospitals from the perspective of healthcare professionals. Rather than focusing solely on technical specifications or isolated incident reports, the study emphasizes lived user experiences and contextual factors—elements that are often underrepresented in regulatory and design discussions. By characterizing error frequency, perceived severity, and contributing factors across different clinical roles and experience levels, this research aims to inform more effective, context-sensitive interventions that enhance both safety and usability in infusion pump use.
Materials and Methods
This study employed a cross-sectional descriptive design to evaluate the usability and safety challenges associated with Medical Infusion Pumps (MIPs) in Saudi hospitals. The aim was to quantify healthcare professionals’ perceptions of MIP-related problems and identify contextual factors that contribute to these challenges across diverse clinical environments.
Survey Development and Validation
A structured survey instrument was developed by a multidisciplinary team consisting of biomedical engineers, clinical researchers, and patient safety specialists. The survey was informed by a comprehensive literature review conducted across PubMed, Scopus, and IEEE Xplore using search terms such as “infusion pump errors,” “device usability,” and “human factors in healthcare technology.” From this review, 26 commonly reported MIP problems were identified and categorized into five domains:
• User Interface (UI)
• Software (SW)
• Mechanical (M)
• Electrical (E)
• Human Factors (HF)
These classifications are summarized in Table 1. To establish content validity, five subject-matter experts in clinical engineering and risk management reviewed the draft instrument. A pilot test with 30 healthcare professionals was then conducted to assess the clarity, relevance, and usability of survey items. Feedback from the pilot phase led to minor wording and formatting adjustments. Internal consistency of the final instrument was evaluated using Cronbach’s alpha, yielding a reliability coefficient of 0.87, indicating high internal reliability.
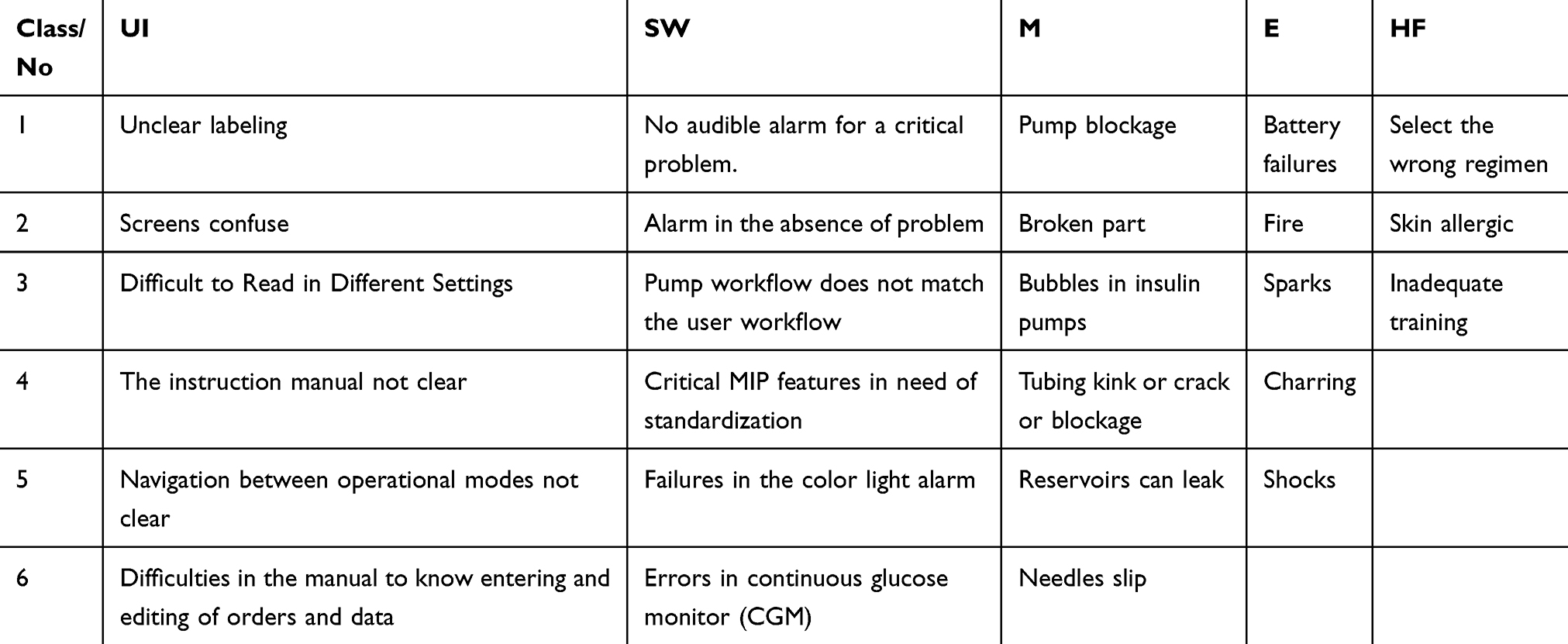 |
Table 1 Classification of Most Encountered MIPs Problems |
Sampling and Participants
A total of 677 healthcare professionals were invited to participate through stratified sampling. Invitations were disseminated via hospital communication channels, professional organization mailing lists, and institutional Email networks. The sampling strategy ensured diversity across:
- Professional roles (physicians, nurses, biomedical engineers)
- Healthcare facility types (public and private; tertiary and secondary)
- Clinical departments (ICU, emergency, operating theatre, general wards).
Inclusion criteria required participants to have direct experience using, monitoring, or managing MIPs. Ultimately, 387 completed responses were obtained and included in the analysis. A formal a priori power analysis was not conducted because the study followed a cross-sectional survey design; however, the final sample exceeds the commonly recommended ratio of 10–20 participants per variable, supporting adequate statistical power for subgroup and multivariable comparisons. This sample size is considered sufficient to provide stable estimates across different roles and experience levels.
Survey Structure
The final survey comprised four components:
- Demographic Information: Profession, years of experience, hospital type, MIP brands used, HIS integration, and internal error-reporting procedures.
- Problem Frequency Ratings: Participants rated the frequency of each of the 26 identified problems using a 5-point Likert scale (1 = least frequent; 5 = most frequent).
- Safety Impact Ratings: Using a parallel 5-point scale (1 = no impact; 5 = remarkably high impact), participants rated the perceived severity of each problem.
- Open-Ended Feedback: Space for additional comments or suggestions related to MIP usability and safety.
This structure enabled a risk-weighted assessment of challenges by examining both the likelihood and perceived clinical impact of each problem.
Data Collection Procedures
The survey was administered electronically using a secure, web-based platform. Data were collected between February 2023 and August 2023. Participants accessed the survey via personalized or institution-specific links to ensure broad geographic reach across Saudi Arabia. No identifiable personal or patient information was collected.
Statistical Analysis
Data were analyzed using IBM SPSS (version X). Descriptive statistics (means and standard deviations) were calculated for each of the five problem domains (UI, SW, M, E, HF). Inferential analyses included:
- Cross-tabulations examining relationships between demographic variables and problem ratings.
- One-way ANOVA to evaluate statistically significant differences in frequency and impact across subgroups (job role, experience level, pump type)
- Effect size measures, including Cohen’s d and partial eta squared (η2), to assess practical significance beyond p-values.
A significance level of p < 0.05 was applied. This mixed quantitative approach allowed comprehensive exploration of how user characteristics and device attributes shape perceptions of MIP-related usability and safety challenges.
Results
Participant Characteristics
A total of 387 healthcare professionals from hospitals across multiple cities in Saudi Arabia participated in the study. Of these, 272 (70.3%) were from government hospitals and 115 (29.7%) from private hospitals. Participants represented diverse professional roles and experience levels (Table 2 and 3) and were distributed across several geographic regions (Table 4), supporting the representativeness of the sample across healthcare environments and operational contexts.
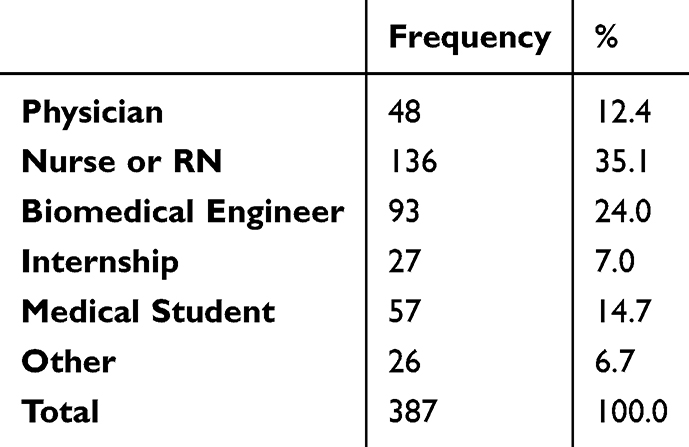 |
Table 2 Distribution of Participants by Job Roles |
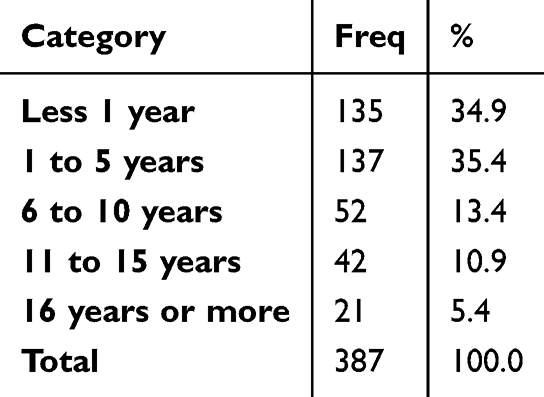 |
Table 3 Distribution of Participants by Years of Experience |
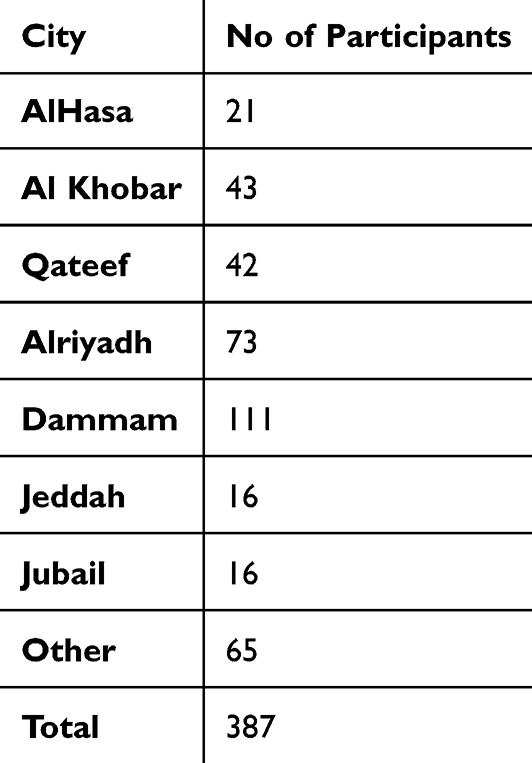 |
Table 4 Geographical Distribution of Participants by City |
Overview of Problem Class Ratings
Table 5 provides an initial summary of how participants rated the five major MIP problem classes—User Interface (UI), Software (SW), Mechanical (M), Electrical (E), and Human Factors (HF)—in terms of both perceived frequency and safety impact. These baseline ratings help contextualize subsequent subgroup analyses.
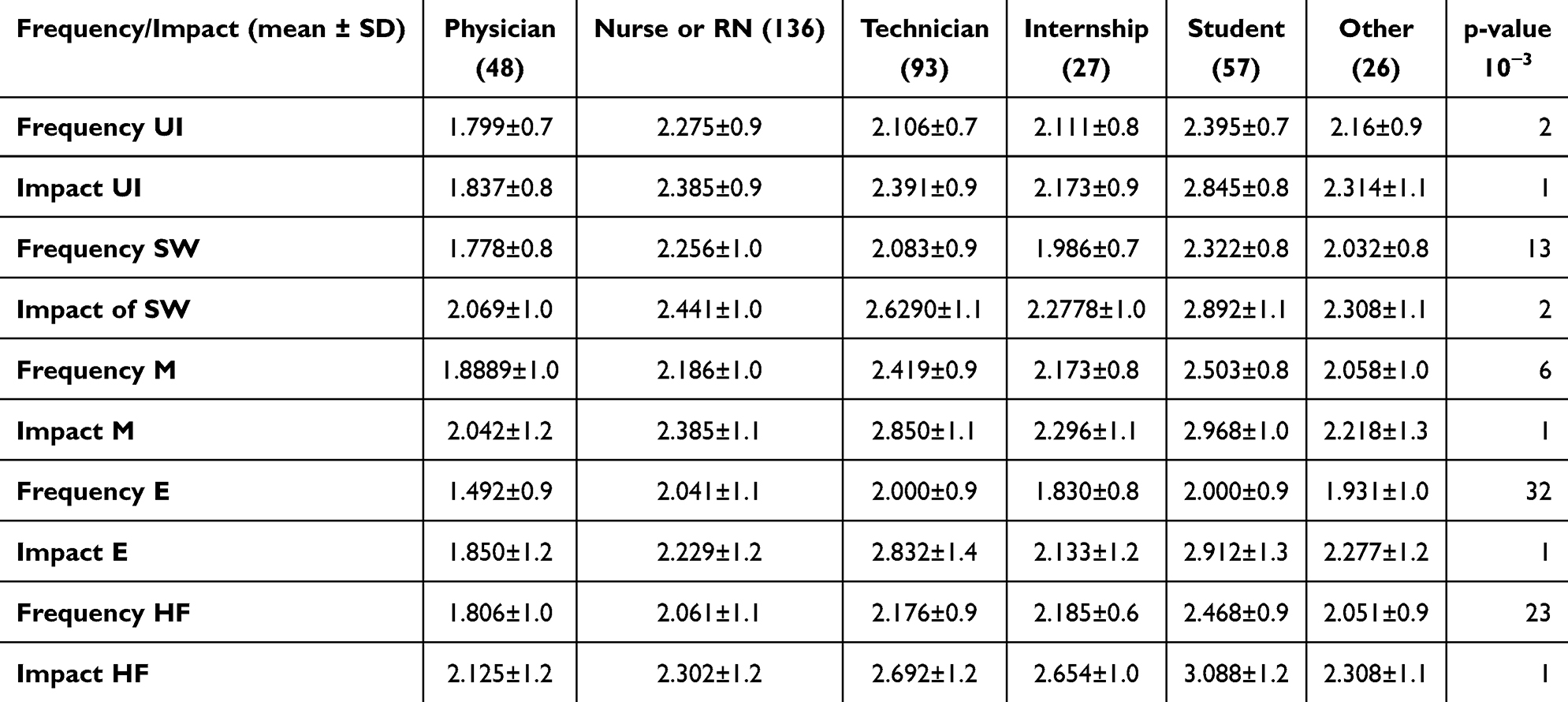 |
Table 5 Mean Frequency and Impact Ratings Across Problem Domains |
Influence of Job Role
As shown in Table 5, statistically significant differences (p < 0.05) were identified across job roles for both the frequency and impact of MIP-related problems. Different professional groups evaluated each problem class differently, highlighting the importance of incorporating role-specific needs into MIP design, usability considerations, and training strategies.
Influence of Experience Level
Findings presented in Table 6 demonstrate that users with fewer years of professional experience reported higher frequencies and greater safety impacts for several problem categories. Differences reached statistical significance in the Human Factors (HF) domain. These results suggest that early-career healthcare professionals may perceive increased vulnerability to MIP-related errors, underscoring the potential value of structured orientation and consistent supervision during the early stages of practice.
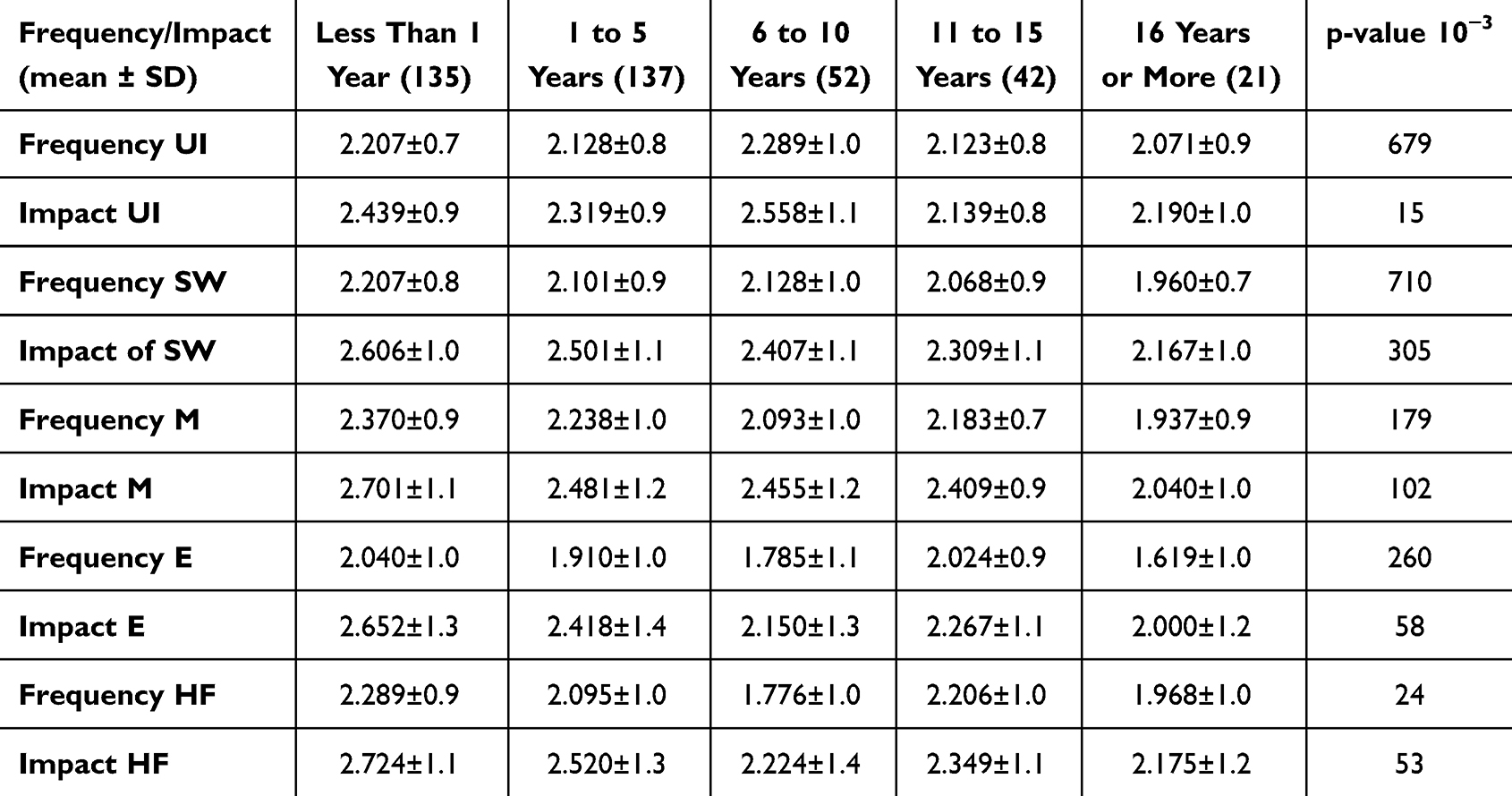 |
Table 6 Impact of Experience on Frequency/Impact of MIP Problems |
Impact of MIP Connectivity
The influence of Hospital Information System (HIS) connectivity was examined in Table 7 by cross-tabulating responses (“Yes,” “No,” “Not sure”) with frequency and impact ratings. Significant differences emerged in several areas, indicating that HIS integration may shape how users recognize, interpret, or report device problems. These findings highlight both the benefits and complexities associated with connected pump systems.
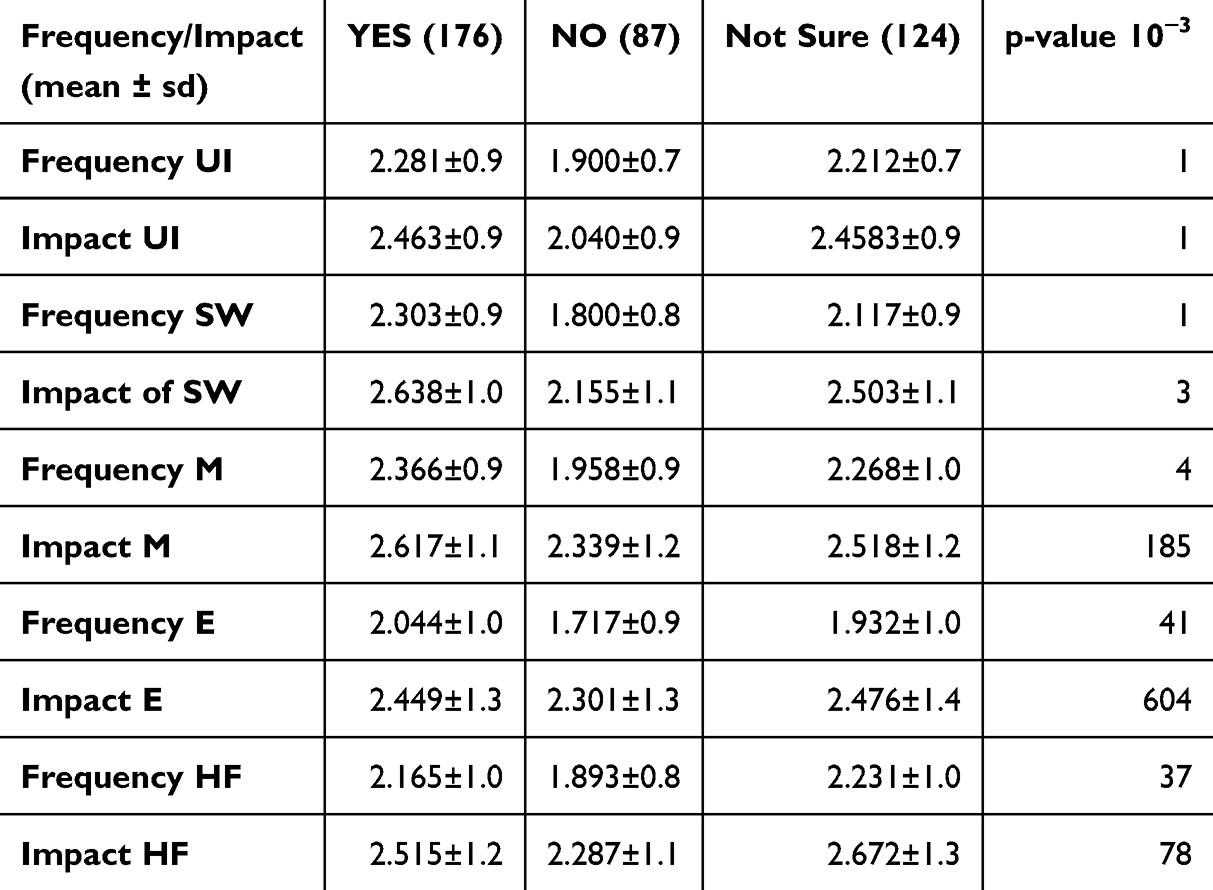 |
Table 7 Comparison of Problem Ratings by HIS Connectivity |
Traditional vs Specialty MIPs
As summarized in Table 8, most comparisons between Traditional and Specialty infusion pumps did not yield statistically significant differences. However, Specialty pumps showed a significantly higher frequency of User Interface (UI) problems (p = 0.046), pointing to a potential area for targeted usability enhancements in devices designed for more complex therapies.
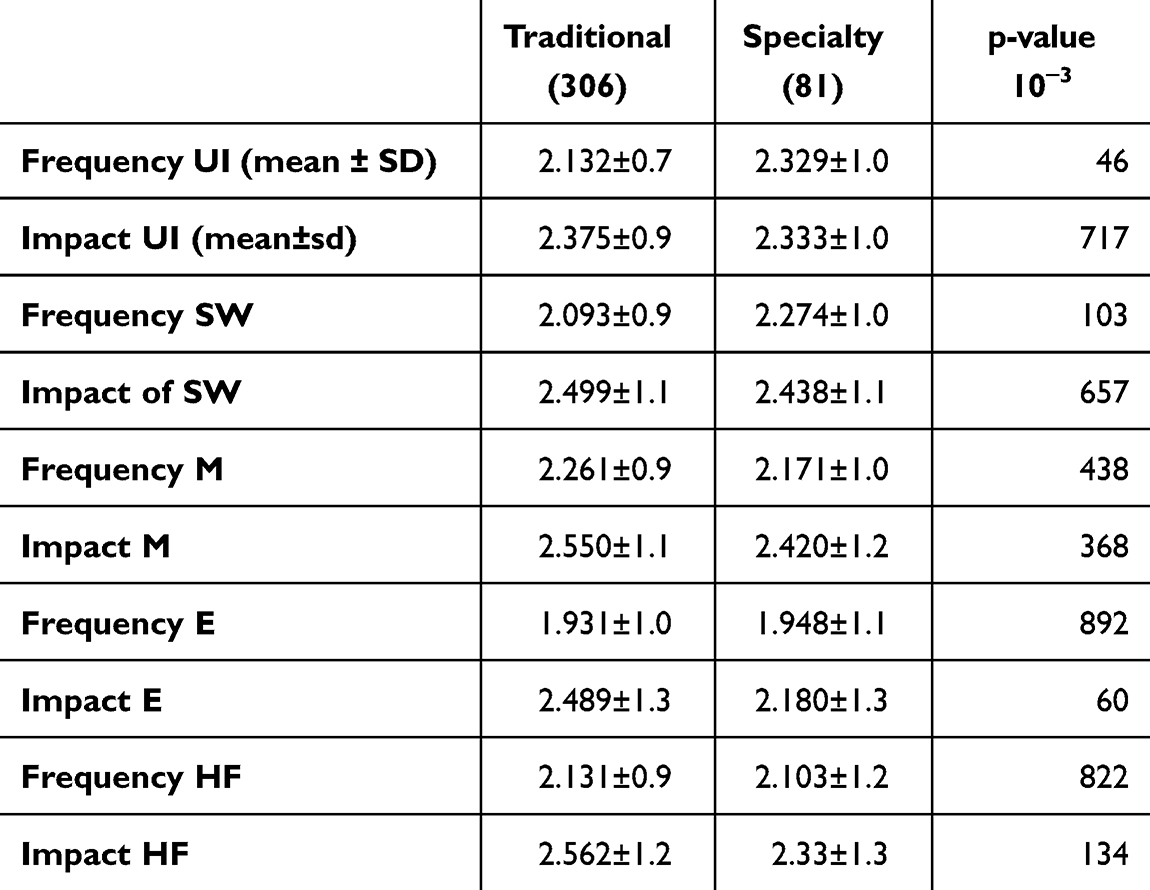 |
Table 8 Comparison of Traditional vs Specialty MIPs Problem Class |
Pump Type Variation
Table 9 details problem ratings across specific MIP types, including syringe, PCA, and elastomeric pumps. Although most differences were not statistically significant, PCA and elastomeric devices showed higher reported frequencies for certain issues. These trends emphasize the importance of tailoring device training and design improvements to the unique characteristics of each pump type.
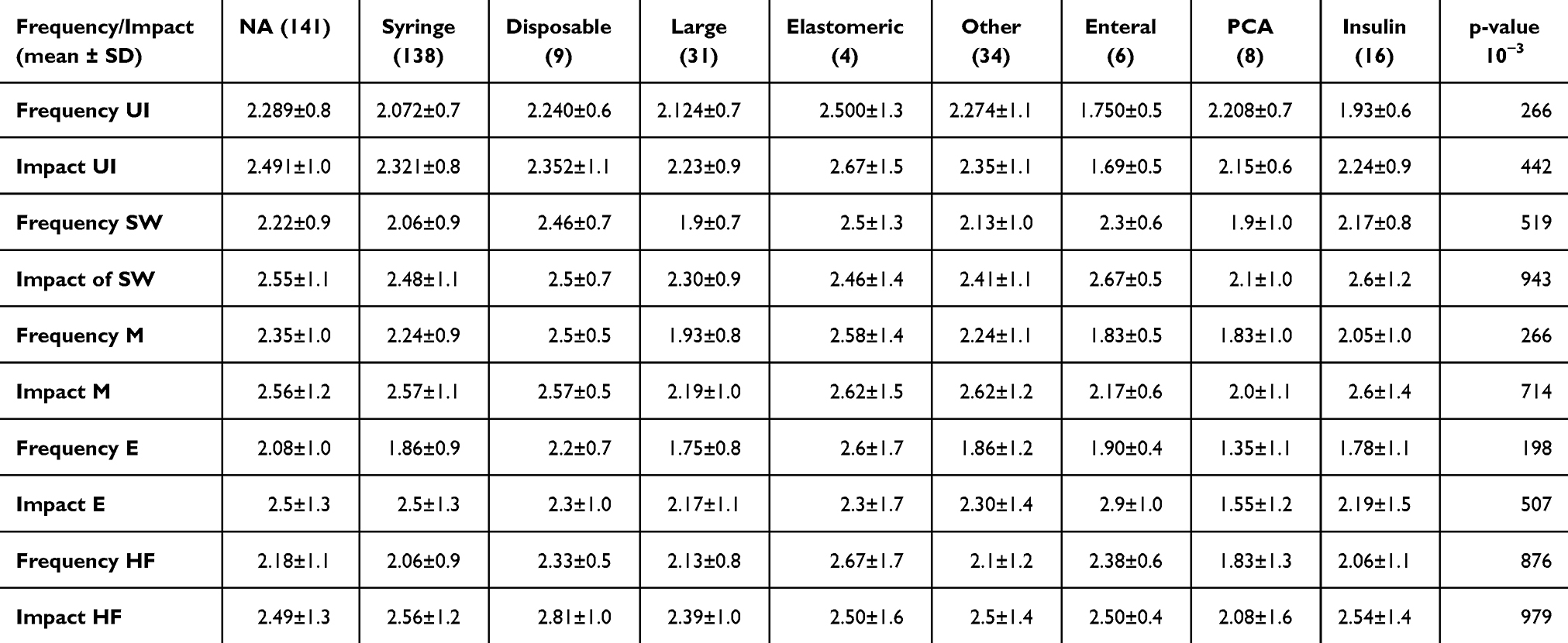 |
Table 9 Cross Tabulation of MIP Problem Classes by Pump Type |
Alert and Notification Types
The analysis in Table 10 explores how different alert modalities—such as visual cues, audible tones, and numerical displays—affect perceptions of problem frequency and impact. No single alert type was strongly associated with higher error belief, but the variation in responses indicates differences in how alerts are interpreted, reinforcing the need for clearer and more standardized alert mechanisms.
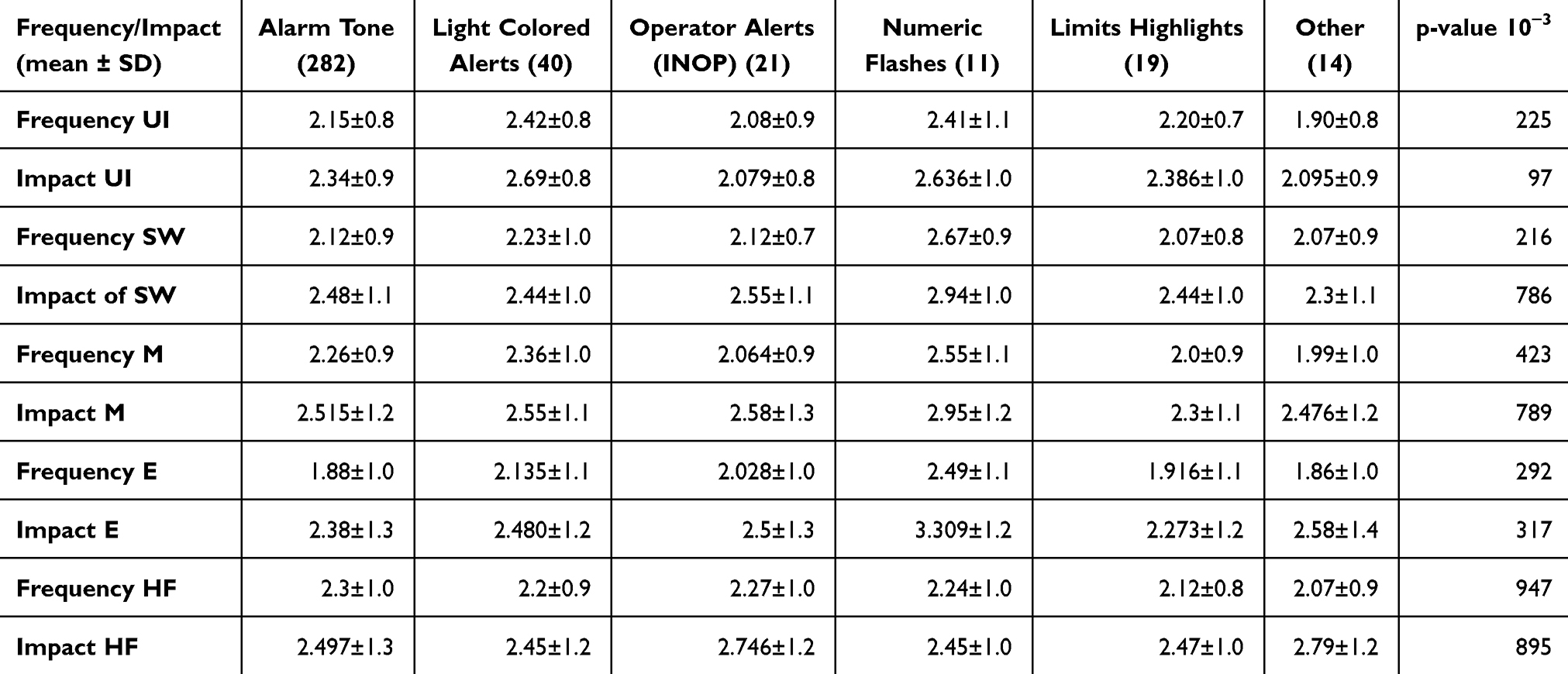 |
Table 10 Impact of Different Alert Types on MIP Problem Frequency and Impact |
Error Reporting Mechanisms
Table 11 examines how reporting methods (manual reporting, HIS-based reporting, and others) relate to perceived MIP issues. Although between-group differences were not statistically significant, devices integrated with HIS showed the highest frequencies and impacts, potentially due to improved visibility and more systematic capture of device-related issues.
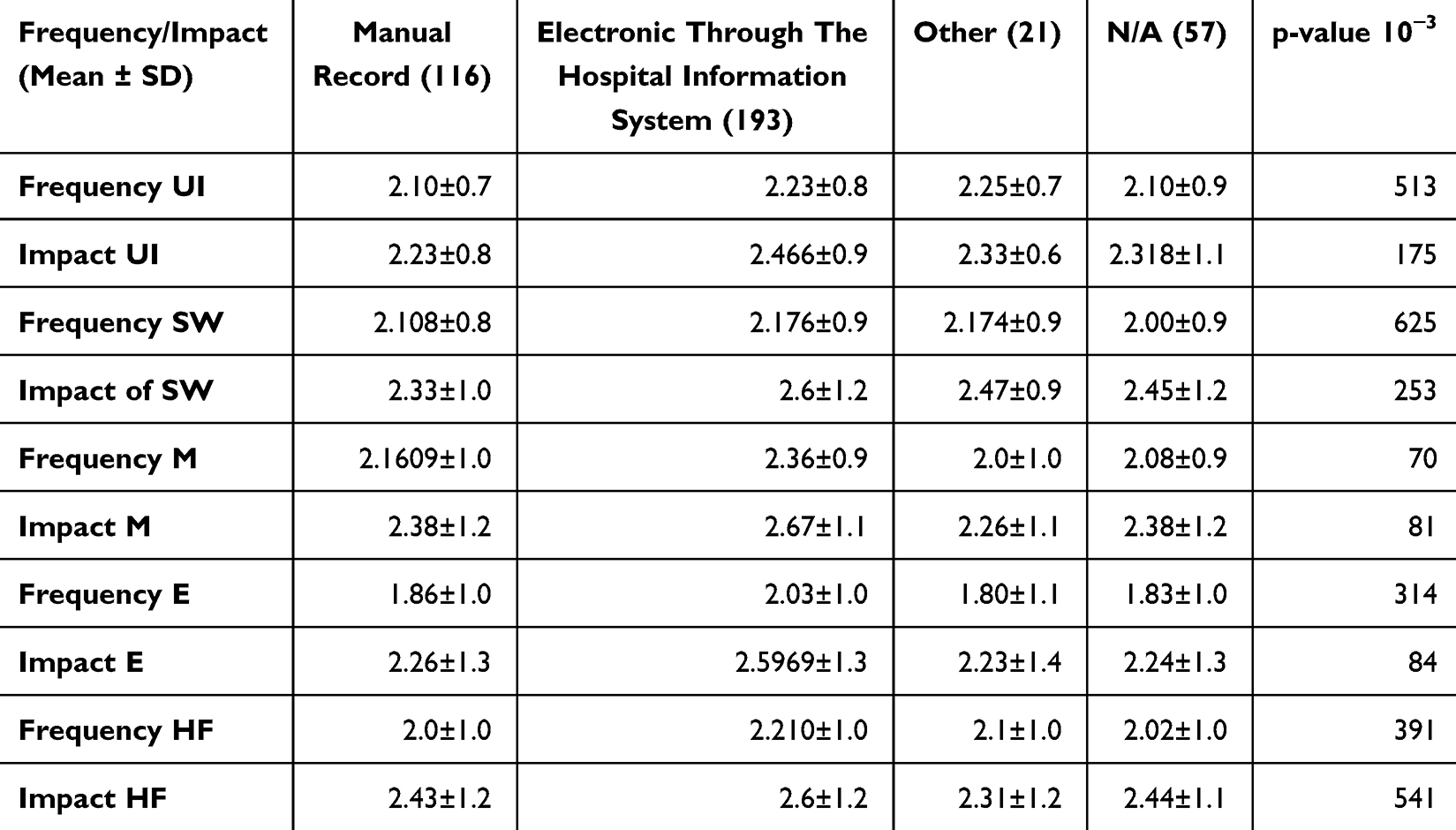 |
Table 11 Effect of Reporting Methods on Frequency and Impact of MIP Problems |
Summary of Statistically Significant Findings
Table 12 consolidates all statistically significant outcomes across subgroups. Significant associations were observed for job role, experience level, and certain MIP types. These findings provide actionable insights to inform targeted training, procurement decisions, and safety strategies aimed at enhancing MIP usability and clinical performance.
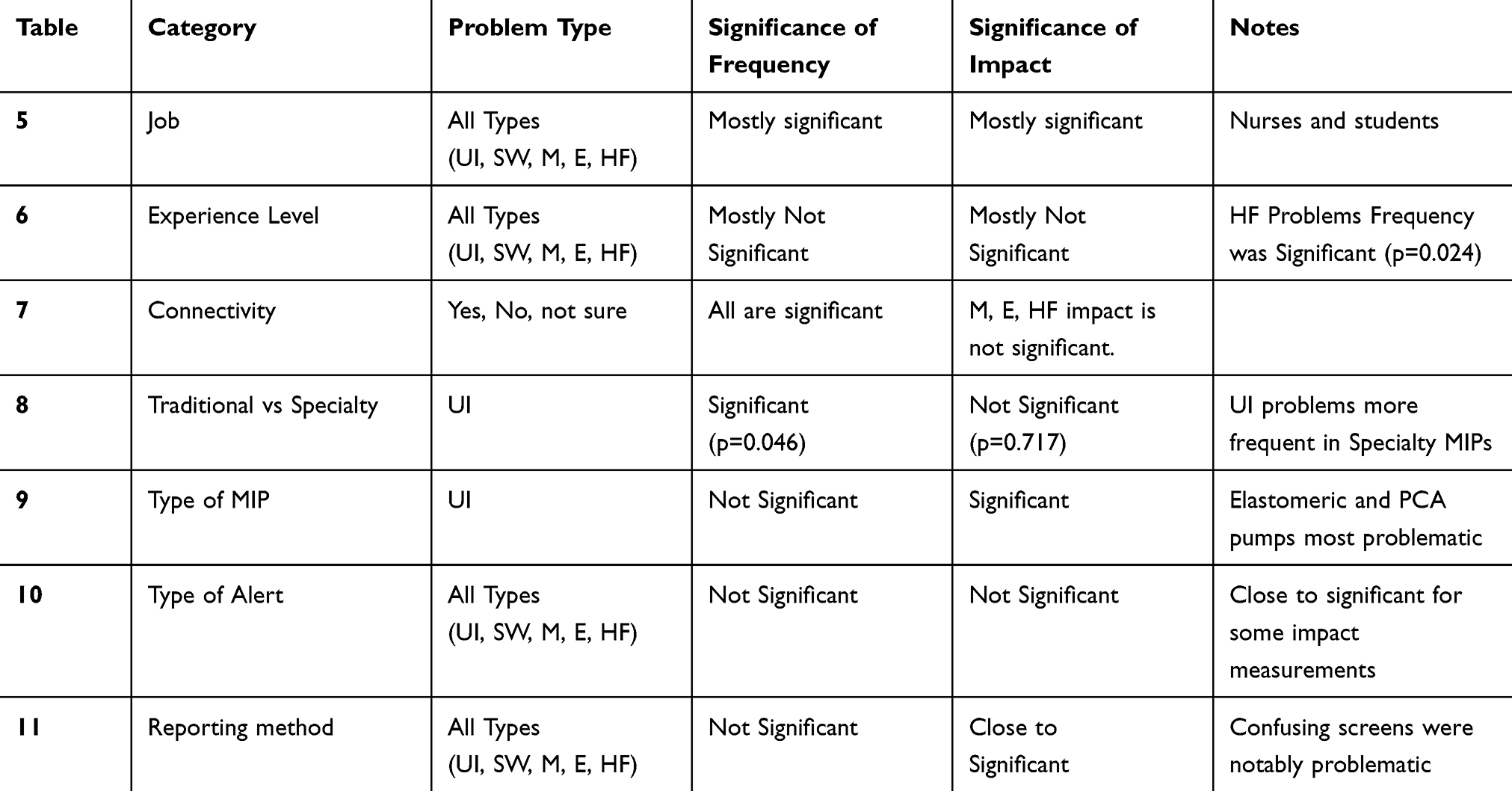 |
Table 12 Summary of Statistical Significance for Factors Affecting MIP Problems |
Discussion
Despite growing attention to patient safety and advances in healthcare technology, medication errors and usability issues with medical infusion pumps (MIPs) continue to present substantial risks in clinical practice.12,13 Many of these issues stem from design limitations, particularly when pump development relies on single-method approaches such as observational studies or heuristic evaluations. More reliable and user-centered designs can be achieved through integrated, multi-method approaches.14
This study sought to characterize how healthcare professionals perceive MIP-related problems and to highlight areas requiring improvement. The results demonstrate that user experience and training levels significantly influence perceived frequency and severity of MIP issues. These findings are consistent with earlier work emphasizing the role of usability and human factors in medication administration errors.15–18 For example, PCA and elastomeric pumps have repeatedly been shown to be more error-prone due to complex programming steps and unintuitive interfaces.18
Our results also showed that less experienced users reported higher frequencies and severities of user interface (UI) problems, supporting prior evidence that clinical experience reduces susceptibility to device-related errors.,19–21 This underscores the need for ongoing, tailored training programs to support safe pump use. Another important finding relates to the integration of MIPs with Hospital Information Systems (HIS). Although HIS connectivity can enhance treatment personalization and safety,22,23 it also introduces new error pathways and workflow complexity.24 The significant associations observed between HIS connectivity and perceived problem frequency reinforce the importance of phased implementation strategies accompanied by comprehensive training.
The study further found that specialty pumps are more often associated with UI-related issues than traditional pumps (p = 0.046), likely reflecting their more advanced and intricate functionalities. This is consistent with earlier reports indicating that specialty and high-acuity devices require more sophisticated training and interface design.17 Improvements in intuitive design and human-factors–driven UX methodologies remain essential to reducing errors and improving usability.12,17,19,24
To contextualize these findings, it is important to compare them with provider survey–based research examining smart infusion pump implementation. Prior surveys conducted in the United States and Europe have reported similar challenges, including high alert burden, difficulties with UI navigation, and variable compliance with drug libraries.25,26 Nurses and less experienced clinicians were consistently identified as facing more difficulty with advanced pump functions—patterns that closely resemble those observed in our sample.
Other provider surveys and evaluation studies also document both challenges and benefits associated with smart pump implementation. These reports confirm that issues such as interface complexity and alert overload are common across settings,25,26 but they also highlight substantial benefits when smart pumps and interoperability features are appropriately implemented. Improved compliance with drug libraries, enhanced workflow efficiency, reduced programming deviations, and increased productivity have been widely reported through health-system evaluations.27–29 Optimized pump–EHR interoperability has been shown to reduce non-actionable alerts, minimize workarounds, and support more consistent clinical practice.28,30 From an operational perspective, recent economic analyses demonstrate that interoperability can improve medication safety, enhance charge capture, and reduce system-level inefficiencies.31 To date, no large-scale provider surveys examining smart infusion pump use have been conducted in the Middle East, underscoring the regional relevance of the present work.
When used appropriately, smart infusion pump technologies offer important operational and safety benefits that extend beyond error reduction. Studies have demonstrated that successful implementation can yield high drug-library compliance rates—often exceeding 85–95%—improved dosing accuracy, and more efficient pump programming workflows.32,33 Clinicians also report reduced time spent on manual checks, faster workflow transitions in high-acuity contexts, and fewer non-actionable alerts due to optimized drug library logic.34,35 These benefits highlight how training quality, system governance, and workflow alignment play critical roles in realizing the full value of smart pump technologies.
International regulatory frameworks reinforce this perspective by emphasizing usability engineering as a core element of device safety. The US Food and Drug Administration (FDA) requires manufacturers to provide evidence of rigorous human-factors engineering and usability validation during pump development.7 Similarly, the IEC 62366 standard outlines structured usability engineering processes aimed at identifying and mitigating use-related hazards in medical devices.8 These frameworks highlight the inseparability of device performance and human-machine interaction and underscore the need for continuous evaluation of real-world usability issues.
Finally, the findings of the present study support the importance of strong institutional guidelines and continuous quality-assurance practices. Standardized protocols, structured training programs, and robust reporting systems are essential to capturing both human errors and systemic weaknesses.36 Trends in FDA data illustrate the scale of these concerns; more than 23,000 malfunction and injury reports related to large-volume IV smart pumps were submitted between 2015 and 2017.37 Many incidents involved alert overrides and incomplete drug libraries—issues frequently linked to UI design limitations and workflow mismatches.38 Collectively, the evidence suggests that improving MIP safety requires a multifaceted approach that combines user-centered design, structured training, thoughtful HIS integration, and institution-level governance. Without such strategies, even technologically advanced infusion systems risk undermining patient safety.39,40
Conclusion
The study’s findings highlight the need for focused interventions to address the usability challenges associated with Medical Infusion Pumps (MIPs). Targeted training is essential, particularly for less experienced staff, who reported higher frequencies of errors. Training should be tiered by experience level and emphasize hands-on practice, troubleshooting, and risk awareness, supported by periodic refresher sessions to reinforce safe operation.
Improvements in device design are also necessary. Specialty pumps—such as PCA and elastomeric devices—require clearer, more intuitive interfaces. Incorporating user-centered design principles and providing real-time feedback features (eg, prompts or alerts) can help reduce recurring errors and support safer decision-making.
Alert systems should be optimized to distinguish critical from non-critical notifications, reducing alert fatigue and improving response accuracy during demanding clinical situations.
Finally, proactive monitoring is needed. Continuous evaluation, incident reporting, and structured feedback loops should guide ongoing enhancements in both device design and training strategies. Implementing these recommendations can reduce MIP-related risks, enhance efficiency, and improve overall patient safety.
Recommendations
The study’s findings highlight the need for focused interventions to address the usability challenges associated with Medical Infusion Pumps (MIPs). Targeted training is essential, particularly for less experienced staff, who reported higher frequencies of errors. Training should be tiered by experience level and emphasize hands-on practice, troubleshooting, and risk awareness, supported by periodic refresher sessions to reinforce safe operation.
Improvements in device design are also necessary. Specialty pumps—such as PCA and elastomeric devices—require clearer, more intuitive interfaces. Incorporating user-centered design principles and providing real-time feedback features (eg, prompts or alerts) can help reduce recurring errors and support safer decision-making.
Alert systems should be optimized to distinguish critical from non-critical notifications, reducing alert fatigue and improving response accuracy during demanding clinical situations.
Finally, proactive monitoring is needed. Continuous evaluation, incident reporting, and structured feedback loops should guide ongoing enhancements in both device design and training strategies. Implementing these recommendations can reduce MIP-related risks, enhance efficiency, and improve overall patient safety.
Declaration of Generative AI and AI-Assisted Technologies in the Writing Process
During the preparation of this work the authors used ChatGPT in order to improve language and readability, with caution. After using this tool/service, the authors reviewed and edited the content as needed and takes full responsibility for the content of the publication.
Ethics and Consent Statements
Imam Abdulrahman bin Faisal Internal Review Board (IRB; IRB-2023-07-354) approved the project. All human participants provided their consent before starting.
Funding
The project has no funding.
Disclosure
The authors declare that there is no conflict of interest in this work.
References
1. Carayon E, Waterson P, Holden RJ. Human factors of complex sociotechnical systems. Appl Ergon. 2014;45(1):45–13. doi:10.1016/j.apergo.2013.03.023
2. Zhang J, Patel VL, Johnson DR. Medical error: is the solution medical or cognitive? J Am Med Inform Assoc. 2002;9(6 Suppl 1):S75–S77. doi:10.1197/jamia.M1209
3. Hart SG, Staveland LE. Development of NASA-TLX (Task Load Index): results of empirical and theoretical research. Adv Psychol. 1988;52:139–183. doi:10.1016/S0166-4115(08)62386-9
4. Ohashi K, Doi M, Fujisawa Y, Seki Y. Impact of smart infusion pumps on medication error reduction: a systematic review. Drug Saf. 2014;37(12):1011–1020. doi:10.1007/s40264-014-0222-2
5. Vandersmissen G, Wyffels P. Smart pump technology and its impact on medication safety: a systematic review. J Patient Saf. 2023;19(1):e12–e20. doi:10.1097/PTS.0000000000000867
6. Borrelli EP, Lucaci JD, Wilson NS, Taneja A, Weiss M, Beer I. Evaluating the impact of smart infusion pump interoperability on reducing medication administration errors: a systematic literature review. Med Devices. 2025;18:247–260. doi:10.2147/MDER.S522534
7. Reason DG. Human error: models and management. BMJ. 2000;320(7237):768–770. doi:10.1136/bmj.320.7237.768
8. Vicente KJ. The Human Factor: Revolutionizing the Way People Live with Technology. Routledge; 2004.
9. Carayon P, Wetterneck AS, Kianfar S. Human factors and ergonomics as a patient safety practice. BMJ Qual Saf. 2014;23(3):196–205. doi:10.1136/bmjqs-2013-001812
10. Lin K, Vicente J, Doyle M, Cimino JJ, Bakken S. A framework for analyzing the safety of infusion pump software. J Biomed Inform. 2012;45(1):120–132. doi:10.1016/j.jbi.2011.10.002
11. Park SK. Designing for patient safety: developing a human factors framework for infusion pump design. Hum Fact. 2011;53(6):663–673. doi:10.1177/0018720811413385
12. Gurses AP, Carayon P. Exploring performance obstacles of intensive care nurses. Appl Ergon. 2007;38(4):440–451. doi:10.1016/j.apergo.2006.07.009
13. ECRI Institute. Top 10 health technology hazards for 2020. Available from: https://www.ecri.org/Resources/Whitepapers_and_reports/2020_Top_10_Hazards.pdf.
14. Bates DW, Teich JM, Lee J, et al. The impact of computerized physician order entry on medication error prevention. J Am Med Inform Assoc. 1999;6(4):313–321. doi:10.1136/jamia.1999.0060313
15. Keers RN, Williams SD, Cooke J, Ashcroft DM. Causes of medication administration errors in hospitals: a systematic review. Drug Saf. 2013;36(11):1045–1067. doi:10.1007/s40264-013-0090-2
16. Battles JB, Lilford RJ. Organizing patient safety research to identify risks and hazards. Qual Saf Health Care. 2003;12(Suppl 2):ii2–ii7. doi:10.1136/qhc.12.suppl_2.ii2
17. Waldron AD, Bonnerup DK, Brock B. Infusion pump errors: a systematic review. J Patient Saf. 2018;14(2):74–81. doi:10.1097/PTS.0000000000000215
18. Husch M, Sullivan C, Rooney D, et al. Insights from the sharp end of intravenous medication errors: implications for infusion pump technology. Qual Saf Health Care. 2005;14(2):80–86. doi:10.1136/qshc.2004.010553
19. Giuliano KK. Improving medication safety with smart infusion pumps: a survey of frontline clinicians. J Patient Saf. 2015;11(1):38–44. doi:10.1097/PTS.0000000000000035
20. Manrique-Rodríguez S, Sánchez-Galindo AC, López-Herce J, et al. Smart infusion technology in pediatric intensive care: a national survey. Int J Med Inform. 2018;113:180–185. doi:10.1016/j.ijmedinf.2018.03.010
21. Vanderveen TW. Drug library compliance and smart pump safety: a review. Hosp Pharm. 2017;52(1):25–32. doi:10.1310/hpj5201-25
22. Larsen GY, Parker HB, Cash J, O’Connell M. Impact of smart infusion pumps on medication safety. J Patient Saf. 2018;14(3):145–150. doi:10.1097/PTS.0000000000000163
23. Lyons I, Furniss D, Blandford A. Efficiency and workload benefits of smart infusion pump use in high-acuity settings. Int J Med Inform. 2017;107:39–48. doi:10.1016/j.ijmedinf.2017.08.005
24. Ohashi K, Cochran GL, Hayashi K. Reducing alert burden through optimized smart pump drug libraries: a multicenter evaluation. Drug Saf. 2015;38(4):365–374. doi:10.1007/s40264-015-0280-y
25. Wei W, Coffey W, Adeola M, Abbasi G. Impact of smart pump–electronic health record interoperability on patient safety and finances. Am J Health Syst Pharm. 2021;78(24):2260–2268. doi:10.1093/ajhp/zxab287
26. Sowan A, Ha B. Maximizing the impact of smart pump–EHR interoperability in critical care. Intensive Crit Care Nurs. 2024;85:103809. doi:10.1016/j.iccn.2024.103809
27. Ubanyionwu S, Khandekar D, Mara KC, Teaford H. Enterprise standardization and convergence of large-volume infusion pump drug libraries. Am J Health Syst Pharm. 2023;80(23):1743–1751. doi:10.1093/ajhp/zxad172
28. Borrelli EP, Taneja A, Abdallah S, et al. Enhancing patient safety and charge capture through smart pump interoperability: a health economic analysis. Clinicoecon Outcomes Res. 2025;17:507–518. doi:10.2147/CEOR.S534748
29. Gurses AP, Carayon P, Wall M. Impact of performance obstacles on intensive care nurses’ workload and perceived safety. Health Serv Res. 2009;44(2):422–443. doi:10.1111/j.1475-6773.2008.00934.x
30. Blumenthal D. The role of health information technology in patient safety. Health Aff. 2010;29(4):546–552. doi:10.1377/hlthaff.2010.0041
31. Gorski LA, Hadaway L, Hagle ME. Infusion Nurses Society. Infusion therapy standards of practice. J Infus Nurs. 2021;44(1S):S1–S224. doi:10.1097/NAN.0000000000000396
32. U.S. Food and Drug Administration (FDA). Manufacturer and User Facility Device Experience (MAUDE) database. Published 2017. Available from: https://www.accessdata.fda.gov/scripts/cdrh/cfdocs/cfmaude/search.cfm.
33. Cohen MD. The effect of experience on the use of decision-support tools in infusion pump programming. J Biomed Inform. 2012;45(1):149–155. doi:10.1016/j.jbi.2011.10.003
34. Patel AR, Cohen JA. Training and retraining: the key to safe infusion pump use. Nurs Manage. 2019;50(2):24–30. doi:10.1097/01.NUMA.0000553204.45678.9b
35. A ADDED)B, Vincent CJ, de Bruijne M, Spreeuwenberg P, Wagner C. Patient safety and usability in medical technology design. BMJ Qual Saf. 2015;24(9):561–564. doi:10.1136/bmjqs-2015-004614
36. P ADDED)W, Catchpole K. Human factors in healthcare: lessons from patient safety research. BMJ Qual Saf. 2016;25(9):649–652. doi:10.1136/bmjqs-2016-005981
37. P ADDED)C, Hundt AS, Kush MA. Human factors and usability in health information technology. J Biomed Inform. 2020;107:103421. doi:10.1016/j.jbi.2020.103421
38. U.S. Food and Drug Administration (FDA). Infusion Pumps Total Product Life Cycle: Guidance for Industry and FDA Staff. Silver Spring, MD; 2014.
39. International Electrotechnical Commission (IEC). IEC 62366-1: Medical Devices—Usability Engineering. IEC; 2015.
40. Lyons KJ, Donnelly RF, et al. Smart pump implementation: lessons learned from multi-hospital rollouts. Hosp Pharm. 2019;54(1):32–40. doi:10.1177/0018578718812345
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.