Back to Journals » Infection and Drug Resistance » Volume 14
Urinary Bacterial Profile and Antibiotic Susceptibility in Pregnant Adolescents and Pregnant Low Obstetric Risk Adult Women
Authors Diorio de Souza H ![]() , Hase EA, Knippel Galletta MA, Rodrigues Mota Diorio G, Lippi Waissman A, Pulcineli Vieira Francisco R, Zugaib M
, Hase EA, Knippel Galletta MA, Rodrigues Mota Diorio G, Lippi Waissman A, Pulcineli Vieira Francisco R, Zugaib M
Received 11 March 2021
Accepted for publication 9 June 2021
Published 23 July 2021 Volume 2021:14 Pages 2829—2841
DOI https://doi.org/10.2147/IDR.S310696
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Prof. Dr. Héctor Mora-Montes
Henrique Diorio de Souza,1,2 Eliane Azeka Hase,3 Marco Aurelio Knippel Galletta,1 Giselle Rodrigues Mota Diorio,2 Adriana Lippi Waissman,3 Rossana Pulcineli Vieira Francisco,1 Marcelo Zugaib1
1Disciplina de Obstetrícia, Departamento de Obstetrícia e Ginecologia, Faculdade de Medicina FMUSP, Universidade de São Paulo, São Paulo, Brazil; 2Faculdade de Medicina, Universidade Federal de Juiz de Fora, Juiz de Fora, Minas Gerais, Brazil; 3Divisão de Clínica Obstétrica, Hospital das Clínicas HCFMUSP, Faculdade de Medicina, Universidade de São Paulo, São Paulo, Brazil
Correspondence: Marco Aurelio Knippel Galletta
Departmento de Obstetrícia e Ginecologia, Universidade de São Paulo, Avenida Doutor Enéas de Carvalho Aguiar, 155, São Paulo, 05403-000, SP Tel +55 11 2661-6445
Email [email protected]
Introduction: Significant bacteriuria is associated with clinical and obstetric complications. The existing studies on the profile of urinary pathogens in pregnant women have widely divergent results and they hardly include data on pregnant adolescents.
Methods: This observational retrospective study was conducted in a tertiary hospital in the city of São Paulo with 388 pregnant adolescents and 2547 pregnant low-risk obstetric care adults who began prenatal care between January 2010 and January 2016. They were compared in terms of urine sediment, urine culture, and antibiogram results.
Results: The prevalence of bacteriuria was 17.01% (66/388) among adolescents and 10.13% (258/2547) among adults. Adolescence was a risk factor for bacteriuria in pregnancy (OR=1.82, CI95%=1.35– 2.44, p=0.08). The most frequently isolated pathogen in urine culture was Escherichia coli, both in adolescents (49%) and in adults (42.18%). In positive urine cultures, urinary leukocytes were present in greater numbers in adolescents than in adults (p< 0.001). Resistance to quinolones in general was more frequent among adults (OR=5.86, CI95%=0.78– 44.20, p< 0.001), but the tendency was not statistically significant.
Conclusion: Escherichia coli and the less frequent Streptococcus agalactiae were the etiologic agents most often found in the urine cultures both of adolescents and adults. Higher rates of bacteriuria and of abnormal urine sediments prevailed among adolescents.
Keywords: pregnant women, bacteriuria, pregnancy in adolescence, anti-bacterial agents, drug resistance, bacterial, microbial sensitivity tests
Introduction
The term bacteriuria refers to the isolation of at least one bacterial species in a medium-jet urine culture. The clinical spectrum of bacteriuria ranges from lack of symptoms to a symptomatic urinary tract infection (UTI), be it in the lower urinary tract (cystitis) or in the upper urinary tract (pyelonephritis).1
A diagnosis of bacteriuria is made when the growth of a species of pathogens reaches a count of at least 105 colony-forming units (CFU) per milliliter (mL) in the urine culture of a woman with no urinary symptoms.1,2 This diagnosis is established in approximately 2% to 7% of pregnancies, a prevalence similar to that found in nonpregnant women.3,4 Pregnancy promotes relaxation of the ureter smooth muscle and dilation of the urinary tract, facilitating microbial ascension. When detected in pregnancy, bacteriuria has been associated with an increased risk for preterm birth and low birthweight.5,6
Cystitis occurs in approximately 1% to 5% of pregnant women.4 As indicated above, there is some evidence to support a correlation between acute cystitis in pregnancy and an increase in the risk for preterm birth and low birthweight.5,6
Pyelonephritis develops in 1% to 2% of pregnancies; however, such incidence is dependent on the frequency of occurrence and treatment of asymptomatic bacteriuria.3,4 A few studies have demonstrated that age under 20, smoking, pregestational diabetes, and nulliparity are associated with a higher risk for pyelonephritis.3,7,8 Nevertheless, maternal morbidity and obstetric outcomes seem not to differ per trimester.9,10
Bacterial colonization of the urinary tract tends to be more frequent in the subgroup of pregnant adolescents, with figures ranging from 3.5% in the United States to 30% in Turkey.11,12
The chronological limits of adolescence are set by the World Health Organization (WHO) as 10 and 19 years of age.13 In Brazil, the Child and Adolescent Statute establishes for legal purposes that the upper limit of the age range for adolescence is 18 years of age as is the case in many other nations.14 Nonetheless, adolescence is a phase of higher susceptibility to certain health complications during pregnancy, such as prematurity, fetal growth restriction, and pregnancy-specific hypertensive disorders.15
The most frequently isolated bacterium in the urine culture of pregnant women in general is Escherichia coli, and figures vary from 28.4% in Nigeria to 83% in Brazil.16,17 The other frequently isolated species are the following: Klebsiella sp., coagulase-negative staphylococci, Staphylococcus aureus, and Lancefield group B streptococci.
The existing studies of bacteriuria and antimicrobial sensitivity profile of urinary tract pathogens have widely divergent results, which are tied to the locality where they were conducted. Furthermore, there are scarcely any data on the subgroup of pregnant adolescents. Hence, this study aimed at comparing the profile of bacterial sensitivity to antibiotics between the urinary tract pathogens of pregnant adolescents and those of pregnant low obstetric risk adults, in search of a possible difference between the two profiles.
Methods
This observational retrospective study was conducted in a tertiary teaching hospital, the Hospital das Clínicas da Faculdade de Medicina da Universidade de São Paulo, located in São Paulo, the most populous city in Brazil.
All pregnant female patients ranging from 10 through 18 years of age were selected by means of convenience sampling from among the patients receiving prenatal care at the obstetric clinic of the afore mentioned hospital between January 2010 and January 2016. A control group, put together for comparative purposes, was made up of pregnant, low obstetric risk adult women 19 years of age or older, who initiated prenatal care at the same time as the adolescents. Were excluded women who missed prenatal care before collection for the urine test, whose medical records were incomplete, or who lacked access to their medical records. Medical features, sociodemographic characteristics, obstetric history, and laboratory tests were obtained through access to medical files and the health service database. Gestational age was defined using the onset date of the last menstruation or the first ultrasound scan of prenatal care. According to the protocol of the base hospital of the study and taking as a reference the methodology used in other studies,18,19 a second urine culture was requested only in case of the appearance of some irritating urinary symptom in a previously asymptomatic pregnant woman or about 7 to 14 days after termination of treatment for any infectious pathology of the urinary tract.
Procedures
Urinalysis and uroculture were requested of all pregnant females at the first prenatal care visit. They were instructed to collect a sample of about 20 mL of medium-jet urine and observe the techniques for perineal asepsis.
The women were instructed to send the samples to the laboratory within 02 hours after collection or to keep the samples refrigerated at a temperature of 4 degrees Celsius, in case it was not possible to send them to the laboratory within a period of up to 02 hours. All urine cultures with at least 105 CFU/mL of a sole species of bacterial pathogens were included in the analysis.
Bacterial Isolation
Upon reaching the laboratory, the urine was homogenized, but not centrifuged. The flask was opened and a sterile calibrated handle was immersed in an upright position, only once, in the container. The plates were inoculated using a calibrated 0.001 mL loop. The culture medium used was the chromogenic agar chromID® CPS® (bioMérieux), which is a non-selective medium composed of 2 specific chromogenic substrates, which can be cleaved by the bacterial enzymes beta-glucuronidase and beta-glucosidase. The medium also allows spontaneous detection of deaminase for the Proteeae tribe. The media were incubated aerobically at 35±2 degrees Celsius for 18 to 24 hours. After this period, the medium was examined macroscopically for bacterial growth. The quality control strains consisted of E. coli ATCC® 25922, K. pneumoniae ATCC® 700603, E. faecalis ATCC® 29212, S. epidermidis ATCC® 12228, P. vulgaris ATCC® 6380, C. albicans ATCC® 14053, S. aureus ATCC® 25923 e S. saprophyticus ATCC® BAA-750.
Procedures for Urinalysis
Urinalysis comprised a set of three procedures: visual examination, with assessment of physical properties (color, transparency); chemical examination, looking for abnormal elements (ph, glucose, density, urobilinogen, ketone bodies, proteins, blood); and sedimentoscopy.
The chemical examination was carried out using reagent tapes, which are plastic tapes with small absorbent papers impregnated with chemical substances, which change color when immersed in the urine. The reagent strips were read in an automated way. To perform the sedimentoscopy, ten milliliters of homogenized urine were centrifuged at 1500 to 2000 revolutions per minute, for 05 minutes. The supernatant was discarded and the pellet was suspended again. About 0.05 mL were transferred to a slide and covered by a coverslip. Sedimentoscopy was performed with the aid of a 100x objective for general observation of the sediment and for quantification of casts. The 400x objective was used to quantify leukocytes, erythrocytes, crystals, epithelia, bacterial flora and other elements that could be identified in the urine. Leukocytes and erythrocytes were observed in at least 20 fields; the final result was the average of all counts.
Direct Bacterial Identification Using Vitek 2 or Vitek MS Systems
Bacterial identification was performed using the automated method VITEK® 2 (bioMérieux) (January 2010 to December 2014) or VITEK® MS (bioMérieux) (January 2015 to January 2016). In the VITEK® 2 system, the colonies are suspended in 0.45% sodium chloride, in a turbidity of 0.5 on the McFarland scale, and inoculated on a card for bacterial biochemical identification. The VITEK® 2 equipment database is managed by the Advanced Expert System (AES) software. Some additional information for the final microbial identification, such as the morpho-staining characteristics visualized by Gram staining and the aerotolerance tests, are entered manually by the microbiologist in the software. As quality control, strains of S. maltophilia ATCC® 17666 and E. cloacae ATCC® 700323 were used for the GN card and E. casseliflavus ATCC® 700327 and S. saprophyticus ATCC® BAA-750 for the GP card of the VITEK® 2 system. In the matrix assisted laser desorption ionization-time of flight mass spectrometry (MALD-TOF MS) (VITEK® MS), a sample of the colony is placed on a stainless steel plate and added with 1 microliter of the α-cyano-4-hydroxycinnamic acid (CHCA) matrix. In the mass spectrometer, some beams with pre-established laser wavelengths are emitted. The mass spectra are obtained and compared with the reference library Myla® Software 2.0 (bioMérieux). The international reference strain Escherichia coli ATCC® 8739 was used as a calibrator and the strains K. aerogenes ATCC® 13048 and C. glabrata ATCC® mya-2950 were used as controls.”
Antimicrobial Sensitivity Test Using the VITEK ® 2 AST System
The susceptibility tests were carried out using the automated VITEK® 2 system (bioMérieux). The strains are inoculated and incubated in plastic letters that contain lyophilized antimicrobials. For gram negative microorganisms, the AST238 card was used. ESBL screening was performed by assessing bacterial growth in response to ceftazidime, cefepime and cefotaxime in combination or not with clavulanic acid. AST585 card was used for gram positive microorganisms. All results were interpreted using the Advanced Specialist System (AES) and according to the Clinical & Laboratory Standards Institute (CLSI) cutoff points.
Data Management and Statistical Analysis
Microsoft Excel software for Office 365 was used for building the database, and the IBM SPSS Statistics for Windows 20.0 (IBM Corp., Armonk, NY) was used for statistical calculations.
The qualitative data were described through measures of absolute and relative frequencies (percentages) and were compared by means of the chi-square test and the Fisher exact test. The quantitative data were described with measures of central tendency (mean, median) and measures of dispersion (standard deviation), and they were tested for normality of distribution using the Shapiro–Wilk and the Kolmogorov–Smirnov tests. The means of the variables with a normal distribution were compared with the Student t tests. The medians of the nonparametric data were compared through the Mann–Whitney tests (bivariate analyses). The odds ratios (ORs) were also calculated. If a cell was expressed as 0 (zero), 0.5 was added to each cell and the odds ratio was calculated with the adjusted values (Haldane-Anscombe correction). Associations with p<0.05 were deemed statistically significant.
Ethics
The present study was approved by the institutional board review of the Hospital das Clínicas da Faculdade de Medicina da Universidade de São Paulo (Project CAAE 65511617.0.0000.0068). An informed consent form was waived because the project was a retrospective study with data retrieved from the patients’ medical histories, with no direct contact with the patients. All precautions were taken to protect the privacy of the research subjects and the confidentiality of personal information. The hospital’s database identifies patients by numbers. Soon, the names of the women became anonymous to the researchers. The study was conducted in accordance with the Declaration of Helsinki (as revised in 2013).
Results
Throughout the study period, 388 pregnant adolescents and 2547 pregnant adult women receiving low-risk prenatal care were selected. Among the adolescents, a total of 100 urine cultures, corresponding to 66 patients, tested positive. Among the adult women, 358 urine cultures, corresponding to 258 patients, turned out to be positive. The prevalence of bacteriuria among the pregnant females younger than 19 years of age was 17% (66/388), while that of the pregnant women aged 19 years or older was 10.1% (258/2547), a statistically significant difference (p=0.0001, OR=1.82, CI 1.35–2.44) (Table 1).
 |
Table 1 Association Between Pregnant Female’s Age and Occurrence of Bacteriuria |
The characteristics of the study women are shown in Table 2. Among the adolescents diagnosed with bacteriuria, the mean age was 15.3 ± 1.28 years, the mean number of previous pregnancies was 1.1 ± 0.34, the mean number of previous deliveries was 0.06 ± 0.30, and the mean number of previous abortions/miscarriages was 0.03 ± 0.17. Most had a partner (81.8%) and did not smoke (95.4%). Among the adults diagnosed with bacteriuria, the mean age was 28.9 ± 6.1 years, the mean number of previous pregnancies was 2.25 ± 1.39, the mean number of previous deliveries was 0.95 ± 1.11, and the mean number of previous abortions/miscarriages was 0.27 ± 0.67. Slightly over half of the women (55%) had a partner and only 6.6% smoked (Table 2).
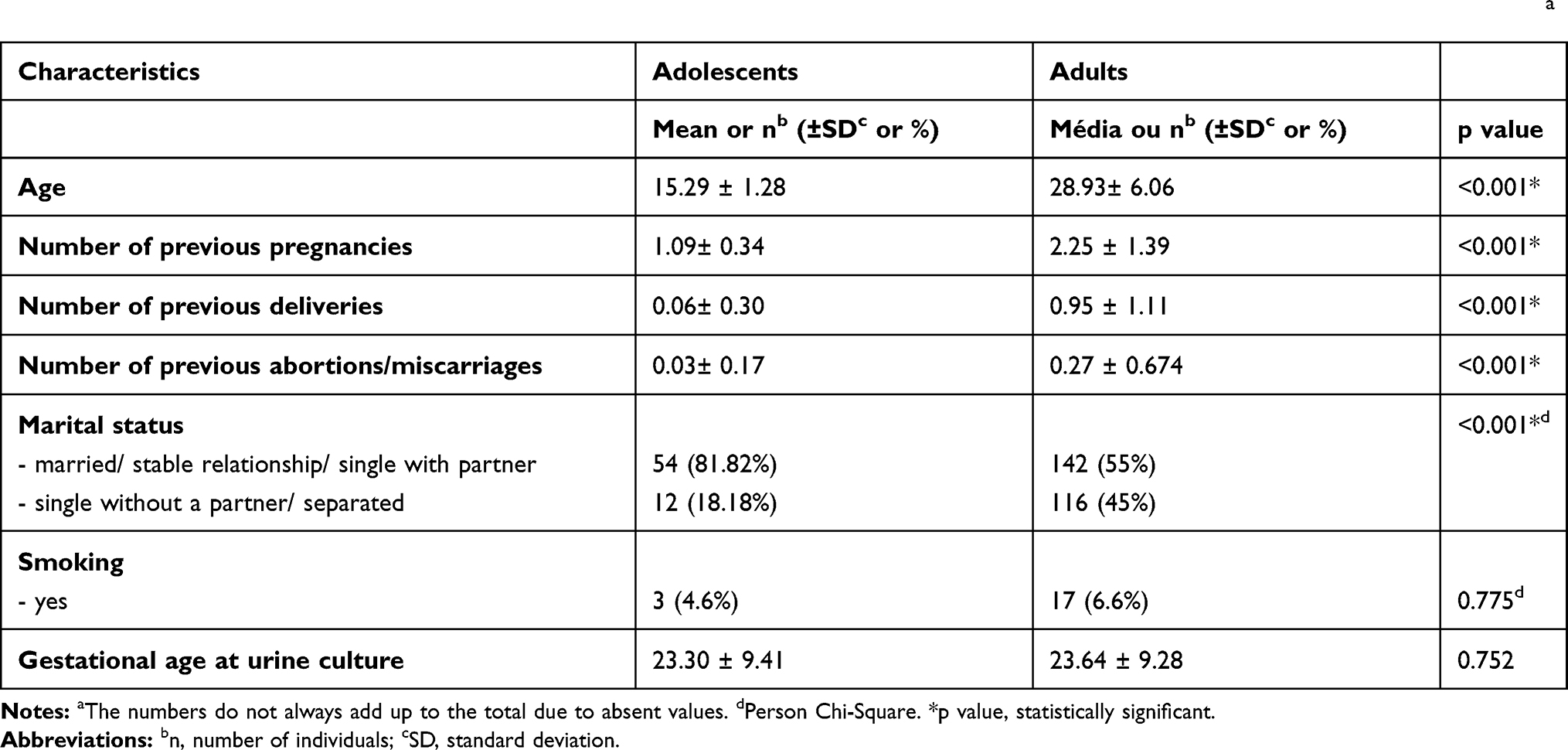 |
Table 2 Sociodemographic Characteristics and Obstetric History of Pregnant Adolescents and Adults Diagnosed with Bacteriuriaa |
The pregnant adults of low-risk obstetric care had a larger number of pregnancies (p< 0.001), more parity (p< 0.001), a greater number of abortions/miscarriages (p< 0.001), and a higher percentage of absentee partners throughout pregnancy (p< 0.001). Although the percentage of smokers among the adult women was higher, the difference was not statistically significant (p=0.775) (Table 2).
Among the pregnant adolescents, the most frequently isolated pathogen in urine culture was Escherichia coli (49%), which was followed by Streptococcus agalactiae (18%), then by Klebsiella pneumoniae (7%), next by Proteus mirabilis (5%) and Staphylococcus saprophyticus (5%), and finally by Enterococcus faecalis (4%) as shown in Table 3. Among the pregnant adults, the number of pathogens involved was larger and the proportions were more balanced. The most frequently isolated pathogen was also Escherichia coli (42,18%), which again was followed by Streptococcus agalactiae (20.11%). Coming up in third place, however, was Enterococcus faecalis (13.1%), followed by coagulase-negative staphylococci (5.6%), Staphylococcus saprophyticus (4.5%), Proteus mirabilis (4.2%) and Klebsiella pneumoniae (3.6%) (Table 3). Some bacterial species were isolated only in the urine culture of adult pregnant women, including Serratia marcescens (7/358), Corynebacterium sp. (1/358), Alcaligenes sp. (1/358) and Pseudomonas shigelloides (1/358). Other species were isolated only in the urine cultures of adolescents, including Acinetobacter calcoaceticus-baumannii complex (1/100), Citrobacter koseri (1/100) and Morganella morganii (1/100) (Table 3).
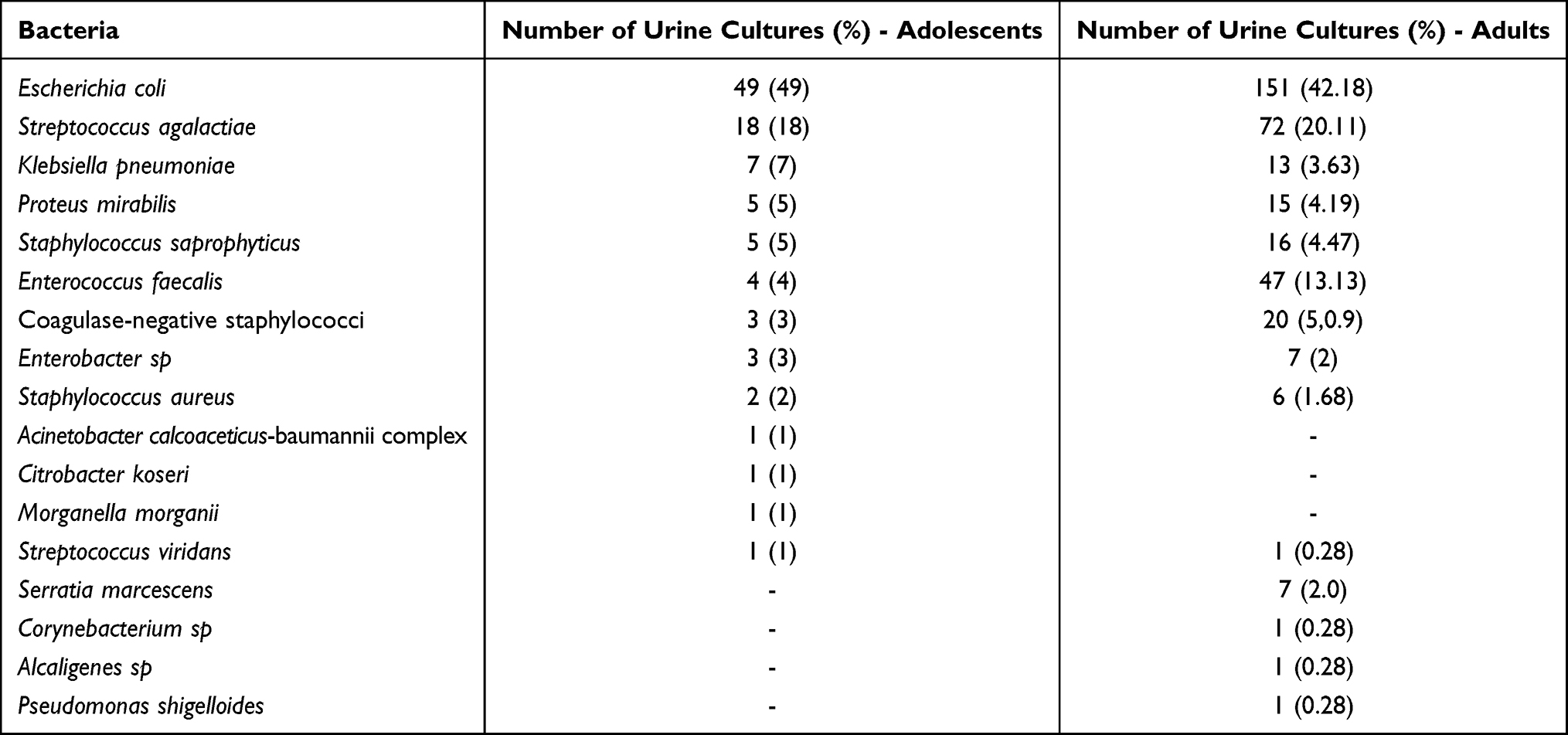 |
Table 3 Main Pathogens Involved in the Occurrence of Bacteriuria Among the Pregnant Adolescents and Adults |
In positive urine cultures, the leukocytes in the urine of pregnant adults were less numerous than those in the urine of pregnant adolescents (p<0.001) (Table 4).
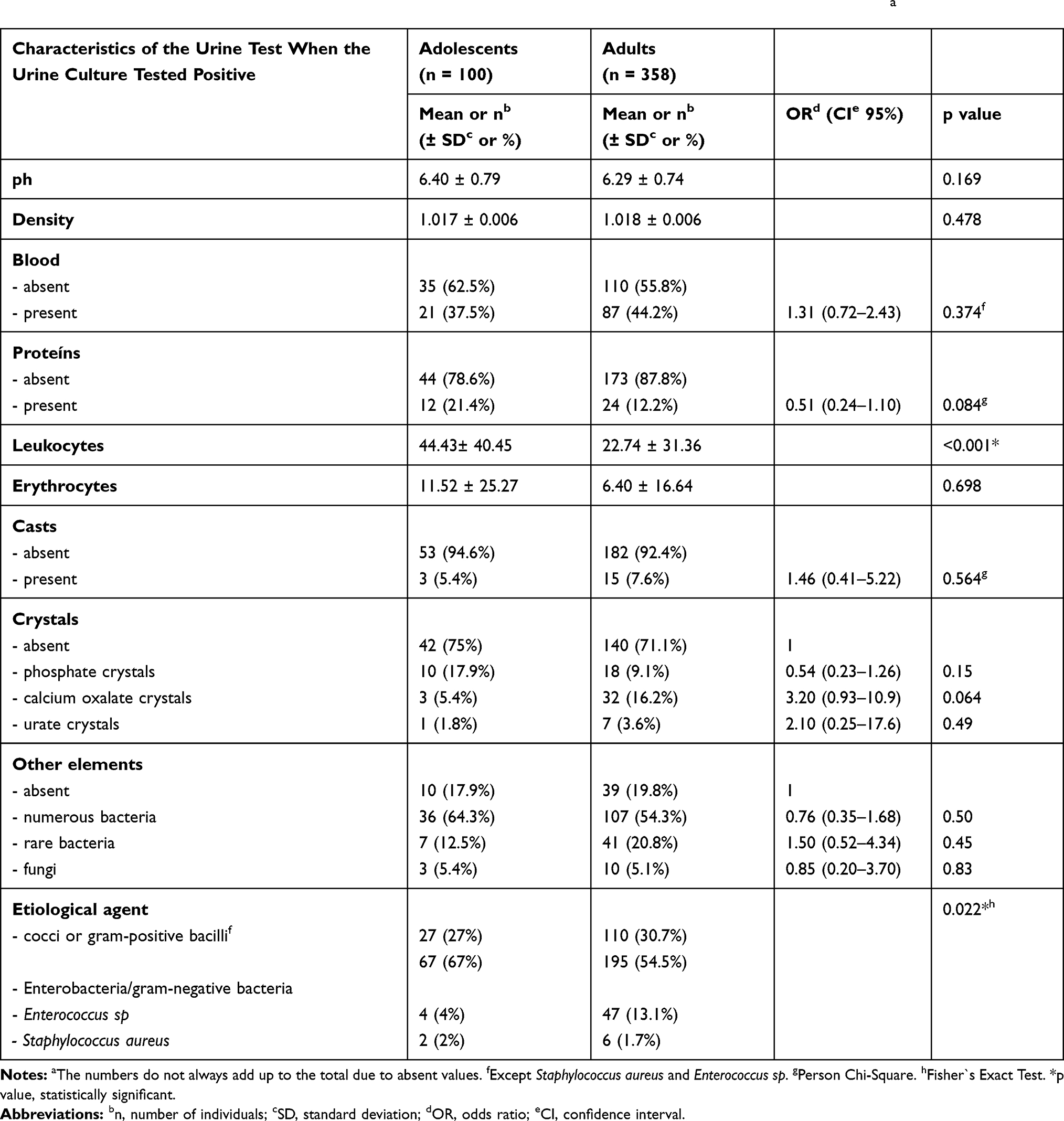 |
Table 4 Characteristics of the Urine Test of Adolescents and Adults When the Urine Culture Tested Positivea |
Also, in positive urine cultures, adult women tended to have higher levels of calcium oxalate crystals (p = 0.064, OR = 3.20, CI = 0.93–10.9) and a lower frequency of proteinuria (p = 0.084, OR = 0.51, 95% CI = 0.24–1.10) compared to adolescents, although the differences were not statistically significant (Table 4).
As for the other characteristics of urine tests in the presence of positive urine culture, pregnant women younger than 19 years old tended to have a higher urinary ph value (p = 0.169), but the results were not statistically significant. There was no difference between pregnant adolescents and adults regarding the following parameters of urinalysis: blood (p = 0.374), casts (p = 0.564) and other urinary elements (fungi or bacteria) (Table 4).
The pregnant adolescents were more likely to have a higher percentage of enterobacteria or gram-negative bacteria and a smaller percentage of enterococci in the urine culture than the pregnant adults (p = 0.022) (Table 4).
Each bacterial species was evaluated separately for the profile of sensitivity to antibiotics (Tables 5 and 6). When we analyzed Escherichia coli strains, isolated from adult pregnant women, regarding the sensitivity profile to beta-lactams, we observed a 42.4% resistance to ampicillin, 12.6% to amoxicillin-clavulanate, 47.7% to cephalothin, 4.6% to cefuroxime, 2% to ceftriaxone and 2% to cefepime. The strains of Escherichia coli isolated from adolescents showed a resistance of 44.9% to ampicillin, 18.4% to amoxicillin-clavulanate, 38.8% to cephalothin, 8.2% to cefuroxime, 2% to ceftriaxone and 4.1% to cefepime. Almost all strains of E. coli isolated from adolescents were sensitive to the fluoroquinolones tested, with only one (2%) being resistant to ciprofloxacin and levofloxacin. Also, few adult strains showed some level of resistance to fluoroquinolones: 4% to norfloxacin, 5.3% to ciprofloxacin and 0.7% to levofloxacin. Considering an antibiotic of frequent use in the treatment of infectious pathologies of the urinary tract during pregnancy, such as nitrofurantoin, we observed a resistance frequency of 7.3% among adults and 6.1% among adolescents. The frequency of multisensitivity reached 40.8% among adolescents and 33.1% among adults (Table 5).
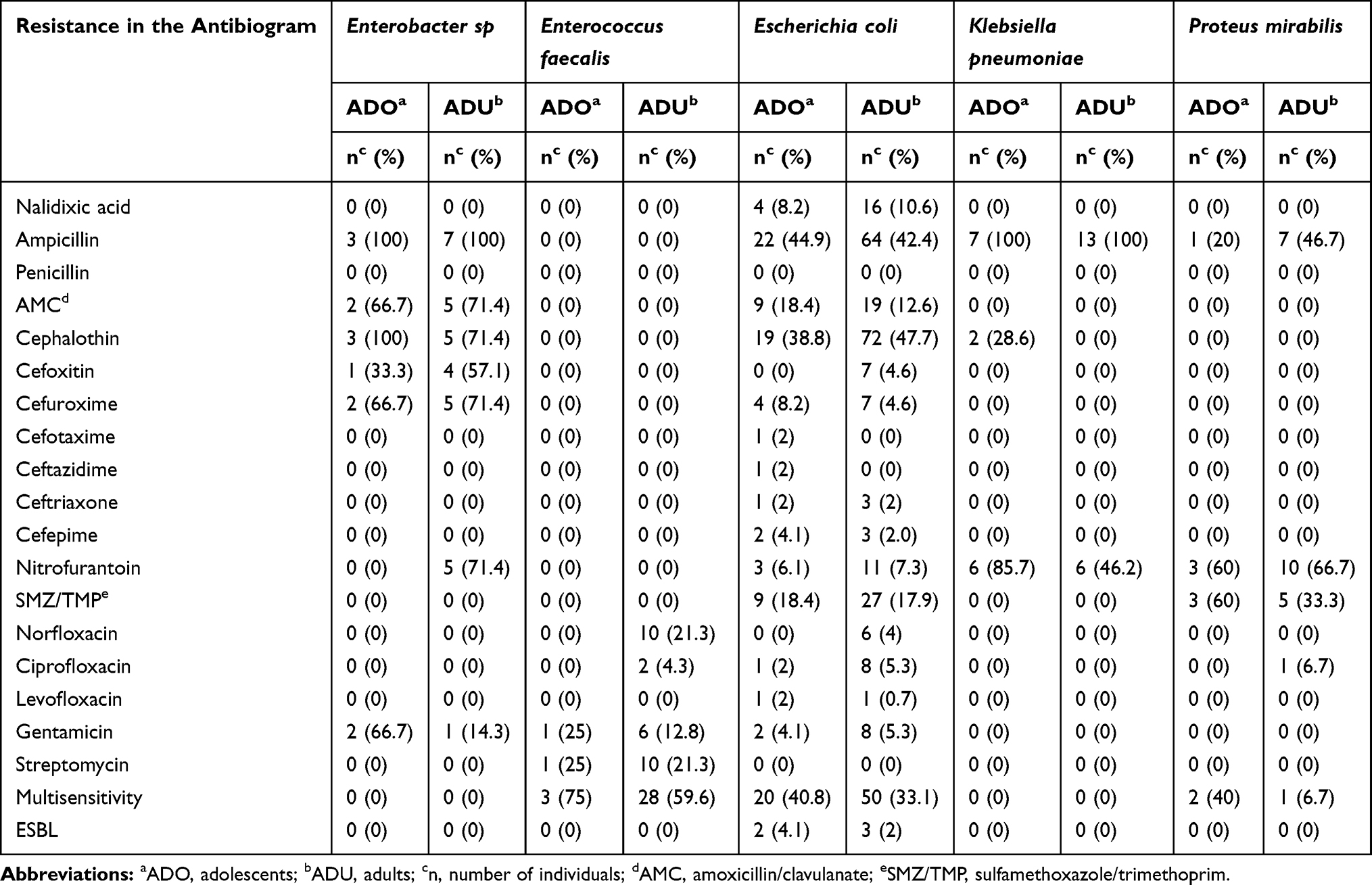 |
Table 5 Microbial Resistance Profile of Gram-Negative Bacteria and Enterococcus Sp Isolated in the Urine of Pregnant Adolescents and Adults |
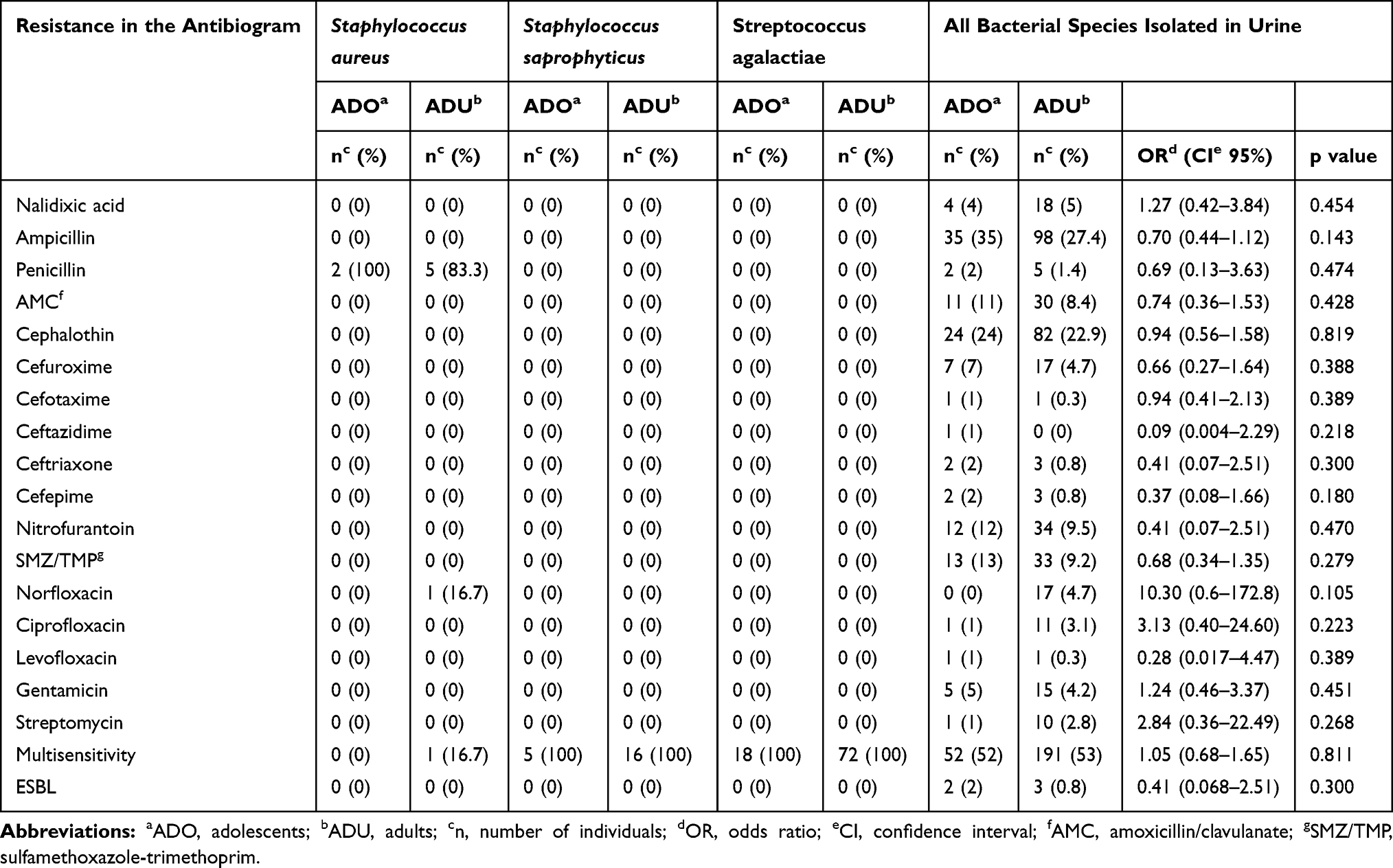 |
Table 6 Microbial Resistance Profile of Gram-Positive and All Bacteria Isolated in the Urine of Pregnant Adolescents and Adults |
Of a total of 100 positive urine cultures among pregnant women under the age of 19, in only 4 (4%) the isolated bacterium was Enterococcus faecalis. Among women aged 19 years or over, of a total of 358 positive urine cultures, 47 (13.13%) were from Enterococcus faecalis. All strains found among adolescents were sensitive to quinolones, unlike adults, who had the following resistance profile: 21.3% (10/47) to norfloxacin and 4.3% (2/47) to ciprofloxacin. Regarding aminoglycosides, E. faecalis strains found in pregnant teenagers showed a resistance of 25% (1/4) to streptomycin, while among adults resistance to streptomycin was 21.3% (10/47) (Table 5).
Of all 458 positive urine cultures, only 20 (4.4%) isolated Klebsiella pneumoniae. Among these bacterial isolates, all were resistant to ampicillin (20/20) and more than half (60%) were resistant to nitrofurantoin (12/20). All Klebsiella pneumoniae strains found in adults were sensitive to first generation cephalosporins (13/13); a fact not observed among the adolescents, who presented a resistance of 28.6% (2/7) (Table 5).
Enterobacter sp. was isolated in only 2.2% (10/458) of urine cultures of pregnant women. All were resistant to ampicillin and sensitive to third and fourth generation cephalosporins. The strains also showed a high degree of resistance to first and second generation cephalosporins: 80% to cephalothin, 50% to cefoxitin and 70% to cefuroxime. Among adolescents, no isolate was resistant to nitrofurantoin (0/3); unlike adults, who had a frequency of resistance to nitrofurantoin around 71.4% (5/7). Of all 10 strains of Enterobacter sp. found, 3 (30%) were resistant to gentamicin (Table 5).
Staphylococcus aureus was found in 1.75% (8/458) of pregnant women. Only one strain (12.5%) was not resistant to penicillin and only one strain, isolated from adult pregnant women, was resistant to norfloxacin (Table 6). When we assessed the antibiotic sensitivity profile of the strains of Staphylococcus saprophyticus (21/458) and Streptococcus agalactiae (90/458), they were all multisensitive (Table 6).
When evaluating all classes of bacteria together, a greater resistance to norfloxacin (p = 0.10, OR=10.30, CI= 0.61–172.80), ciprofloxacin (p = 0.28, OR = 3.13, CI = 0.40–24.60), and any quinolone (p = 0.08, OR = 5.86, CI = 0.78–44.20) was found among the adults than among the adolescents; however, the results had no statistical significance (Table 6).
Discussion
This study has reported a prevalence of 17% of bacteriuria among the pregnant adolescents; such a rate lies within the range of international studies, from 3.5% in the United States to 30% in Turkey.11,12 Among the adults with low-risk obstetric care, the frequency of bacteriuria was 10.1%, in consonance with the existing literature on bacterial colonization of the urinary tract during pregnancy, whose range for adults is even wider than that for adolescents, from 1.4% in the United States to 60% in Zambia.11,20,21
Adolescence has presented itself as a risk factor for bacteriuria in pregnancy. A study undertaken in Saudi Arabia and another carried out in Turkey reached similar conclusions.12,22 This greater frequency of bacterial colonization of the urinary tract among adolescents may be related to inadequate habits of perineal hygiene after urination, especially among the younger ones.23
Analysis of the bacterial profile of the urine culture of the pregnant females in this study reveals that Escherichia coli was the most frequently isolated microorganism both in adolescents (49%) and in adults (42.18%). Similar percentages have been reported in Ethiopia (45.7%), Nigeria (50.8%), India (43.9%), and Kenya (38.8%).24–27 There are, however, studies which report even higher percentages of Escherichia coli among the isolated urinary tract pathogens, such as studies conducted in Brazil (83%), Ireland (74.4%), Portugal (71.4%), and the Netherlands (71%).17,28–31
The second most often isolated bacterial species was Streptococcus agalactiae both in adolescents (18%) and in adults (20.11%). These percentages are much superior to the results found in the international literature, which range from 0% to 10%, and they point to an increased risk for pregnant females and a higher risk of streptococcal disease for the newborn.29,32,33
Among the adults provided with low-risk obstetric prenatal care, the third most frequently isolated pathogen was Enterococcus faecalis (13,13%), at a rate superior to the rates found in other studies in Brazil (2.1% and 7%) or abroad, as in a Dutch study, in which the pathogen rate reached approximately 8%.17,31,34 There are studies indicating a relationship between an infection caused by Enterococcus faecalis and a life in close proximity to poultry and/or the consumption of poultry.35,36 We could raise the hypothesis that adults have different eating habits from adolescents.
Taking pregnant adults and adolescents together, when the antimicrobial sensitivity profile of Escherichia coli strains were evaluated, 43% (86/200) showed resistance to ampicillin, 45.5% (91/200) to cephalothin, 14% (28/200) to amoxicillin/clavulanate, and 7% (14/200) to nitrofurantoin. Our review of international studies of the sensitivity profile of urinary tract Escherichia coli among pregnant females showed that resistance to ampicillin is in the 41% to 100% range; resistance to 1st-generation cephalosporins is in the 55.8% to 66.67% range; resistance to amoxicillin/clavulanate is in the 30% to 83.3% range; and resistance to nitrofurantoin is in the 5.1% to 70.88% range.30,37–41 The enterobacteria in our study appeared to be more highly sensitive to beta-lactam antibiotics than the Escherichia coli strains in international studies. The strains of this bacterial species evaluated in our study also showed a frequency of resistance to sulfamethoxazole/trimethoprim of 18% (36/200), to ciprofloxacin of 4.5% (9/200) and to gentamicin of 5% (10/200) and a frequency of ESBL strains of 2.5% (5/200). International studies demonstrate resistance to sulfamethoxazole/trimethoprim ranging from 16.5% to 99.2%, to ciprofloxacin ranging from 0% to 41.4% and to some aminoglycoside ranging from 0 to 94.93%.24,26,37,41,42 This reinforces the trend towards greater sensitivity to sulfamethoxazole/trimethoprim among the strains isolated in our study compared to the world literature.
Our review of Brazilian studies with pregnant females in general have led to the observation that the Escherichia coli strains have a rate of resistance to ampicillin ranging from 29.62% to 53.4% 38.39), to 1st- generation cephalosporins ranging from 7% to 39.2%, to amoxicillin/clavulanate ranging from 0% to 15.3%, and to nitrofurantoin ranging from 0% to 15.3%.43–46 Thus, the enterobacteria in our study are prone to a greater resistance to beta-lactam antibiotics and to nitrofurantoin than the Escherichia coli strains in other Brazilian research data.34,43,46
The Enterococcus sp strains analyzed in our research showed a rate of resistance to quinolones of 27.45% (14/51). The international data are in agreement with our findings, with values in the 25% to 33.42% range.26,47
Analysis of Staphylococcus aureus in our research yielded a rate of resistance to penicillin of 87.5% (7/8) and to norfloxacin of 12.5% (1/8). The international data are compatible with our findings: one study demonstrated resistance to penicillin of 71.4% and other studies demonstrated resistance to norfloxacin of 0% to 75%.26,27,48
The bacteria isolated in the urine culture of the pregnant adults tended to be less sensitive to quinolones than those from the pregnant adolescents, although the difference had no statistical significance. There are animal studies showing that quinolone use increases the risk for arthropathy in growth cartilages, which limits the use of this class of antibiotics in the pediatric and obstetric populations. This shorter exposure of the child population to quinolones may explain the finding that there was greater sensitivity to quinolones among adolescents.
There are studies that provide evidence of the association between the previous prescription of antibiotics and the identification of bacterial resistance to antimicrobials. This association tends to be stronger in the first month after prescription, but it can be detected for at least 12 months after prescription.49 The recommendations of some guidelines for the use of fluoroquinolones as an empirical treatment option for bacterial colonization of the urinary tract, as well as the prescription of quinolones for the treatment of other clinical conditions, may contribute to the development of bacterial resistance to this class of antimicrobials.49 Resistance to fluoroquinolones can be observed in studies carried out in several parts of the world, especially in Asia.50–52
The strains of Klebsiella pneumoniae isolated from the urine cultures of pregnant women included in our study showed 100% resistance to ampicillin (20/20), 10% to cephalothin (2/20) and 60% to nitrofurantoin (12/20). These data are in correspondence with the values reported in the international literature.24,34,38,41
Ninety strains of Streptococcus agalactiae (GBS) were isolated from a total of 458 positive urine cultures. All strains were sensitive to the main antibiotics used in clinical practice, mainly penicillin, clindamycin and vancomycin. This finding is important, since GBS is the main cause of early neonatal sepsis in newborns.53,54 This bacterial species colonizes the gastrointestinal tract and the urinary tract, infecting the fetus during delivery. Identifying this profile of sensitivity to the main antimicrobials allows the establishment of empirical treatments with antibiotics of lower price and easier access. Some studies show an almost complete absence of rectovaginal isolates resistance to penicillin or ampicillin.53,54 However, other studies demonstrate the emergence of resistance to penicillin, reaching figures of 77.3% in Ethiopia, and resistance to vancomycin, reaching figures of 21% in Palestine.55,56
In short, as was observed, adolescents have a narrower spectrum of pathogens involved in the bacterial colonization of the urinary tract with an overall lower resistance and with more abnormal urine sediment exams than adults. Adding the fact that pregnant adolescents have nearly a twofold risk of preterm births compared to adults, the outcome is extremely favorable for a diagnosis of bacteriuria and for their treatment, even those which are asymptomatic.57,58
On the other hand, it must not be forgotten that this research was carried out at a teaching referral hospital in the largest city in Brazil. That is, care is required in interpreting the results, given that they may not be able to be generalized to other health care realities. Notwithstanding the fact that São Paulo is a pole of wealth and development within the country, the hospital which is source of this study assists women of an underprivileged socioeconomic status who have an urban lifestyle. Thus, the sample which was evaluated may not reliably correspond to other populations.
Even though the novelty of this piece of work is commendable, it ends up being somewhat self-limiting in that assessment of the importance of its findings is curtailed by the few studies in the literature for comparison, be it in the sense of corroborating or even refuting possible inferences.
Conclusion
Pregnancy in adolescence was shown to be a factor of risk for the occurrence of bacterial colonization of the urinary tract. Bacteriuria among pregnant females is a frequent laboratory finding; it is more usual among adolescents, who tend to present a larger number of leukocytes in urine when a urine culture tests positive. Escherichia coli was the most often found etiological agent in the urine culture of adolescents and adults, with Streptococcus agalactiae coming in second. Among adults, the range of pathogens was wider and bacterial resistance tended to be greater. Bacteria isolated from the urine cultures of adolescent pregnant women tended to have a greater sensitivity in vitro to quinolones when compared to adult pregnant women. However, this finding was not statistically significant.
Escherichia coli strains tended to have a good sensitivity profile to beta-lactams and trimethoprim/sulfamethoxazole when compared to the literature. The profile of antibiotic resistance among the other enterobacteria was similar to that reported in international studies. All strains of Streptococcus agalactiae were sensitive to the main antimicrobials used in clinical practice, including penicillin, ampicillin, clindamycin and vancomycin.
The antibiotics analyzed in our study and which are recommended during pregnancy were the beta-lactam antibiotics, nitrofurantoin and sulfamethoxazole/trimethoprim. These drugs were offered the least resistance overall by the most common urinary tract bacteria, and recommendation of their use should thus be prioritized in our environment. Furthermore, it is worth highlighting that it is important pregnant females be routinely checked with a urine culture at the end of the first trimester.
Abbreviations
UTI, urinary tract infection; CFU, colony-forming units; WHO, World Health Organization; OR, odds ratio; ATCC, American Type Culture Collection; AES, Advanced Expert System; MALD-TOF MS, matrix assisted laser desorption ionization-time of flight mass spectrometry; CHCA, α-cyano-4-hydroxycinnamic acid; CLSI, Clinical & Laboratory Standards Institute; CAAE, Certificado de Apresentação de Apreciação Ética (Certificate of Presentation for Ethical Consideration); CI, confidence interval; ICMJE, International Committee of Medical Journal Editors; SD, standard deviation; ESBL, Extended spectrum beta-lactamases.
Acknowledgments
The authors would like to thank all of the pregnant women who participated in the study and all of the employees of the Clínica Obstétrica do Hospital das Clínicas da Faculdade de Medicina da Universidade de São Paulo. The authors whose names are listed above all helped to write the first draft of the manuscript. No payment was made to anyone to produce the manuscript. The corresponding author would also like to state that everyone who made a significant contribution to this piece of work has been included in the list above.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Gilstrap LC, Ramin SM. Urinary tract infections during pregnancy. Obstet Gynecol Clin North Am. 2001;28(3):581–591. doi:10.1016/S0889-8545(05)70219-9
2. Nicolle LE, Gupta K, Bradley SF, et al. Clinical practice guideline for the management of asymptomatic bacteriuria: 2019 update by the Infectious Diseases Society of America. Clin Infect Dis. 2019;68(10):E83–E75. doi:10.1093/cid/ciz021
3. Nicolle LE, Bradley S, Colgan R, Rice JC, Schaeffer A, Hooton TM. Infectious Diseases Society of America Guidelines for the Diagnosis and Treatment of Asymptomatic Bacteriuria in Adults. Clin Infect Dis. 2005;40(5):643–654. doi:10.1086/427507
4. Patterson TF, Andriole VT. Detection, significance, and therapy of bacteriuria in pregnancy. Update in the managed health care era. Infect Dis Clin North Am. 1997;11(3):593–608. doi:10.1016/S0891-5520(05)70375-5
5. Mazor-Dray E, Levy A, Schlaeffer F, Sheiner E. Maternal urinary tract infection: is it independently associated with adverse pregnancy outcome? J Maternal-Fetal Neonatal Med. 2009;22(2):124–128. doi:10.1080/14767050802488246
6. Mittendorf R, Williams MA, Kass EH. Prevention of Preterm Delivery and Low Birth Weight Associated with Asymptomatic Bacteriuria. Clin Infect Dis. 1992;14(4):927–932. doi:10.1093/clinids/14.4.927
7. Wing DA, Fassett MJ, Getahun D.Acute pyelonephritis in pregnancy: an 18-year retrospective analysis. Am J Obstet Gynecol.2014;210:
8. Farkash E, Weintraub AY, Sergienko R, Wiznitzer A, Zlotnik A, Sheiner E. Acute antepartum pyelonephritis in pregnancy: a critical analysis of risk factors and outcomes. Eur J Obstet Gynecol Reprod Biol. 2012;162(1):24–27. doi:10.1016/j.ejogrb.2012.01.024
9. Le J, Briggs GG, McKeown A, Bustillo G. Urinary tract infections during pregnancy. Ann Pharmacother. 2004;38(10):1692–1701.
10. Gratacós E, Torres PJ, Vila J, Alonso PL, Cararach V. Screening and treatment of asymptomatic bacteriuria in pregnancy prevent pyelonephritis. J Infect Dis. 1994;169(6):1390–1392. doi:10.1093/infdis/169.6.1390
11. Pastore LM, Savitz DA, Thorp JM, Koch GG, Hertz-Picciotto I, Irwin DE. Predictors of symptomatic urinary tract infection after 20 weeks’ gestation. J Perinatol. 1999;19(7):488–493. doi:10.1038/sj.jp.7200264
12. Gunes G, Gunes A, Tekiner S, Karaoglu L, Kaya M, Pehlivan E. Bacteriuria and socioeconomic associations among pregnant women in Malatya, Turkey. Public Health. 2005;119(11):1039–1041. doi:10.1016/j.puhe.2004.11.007
13. Eisenstein E. Adolescência: definições, conceitos e critérios. Adolesc Saúde (Online). 2005;6–7.
14. Magalhães MDLC, Furtado FM, Nogueira MB, et al. Gestação na adolescência precoce e tardia - Há diferença nos riscos obstétricos? Revista Brasileira De Ginecologia e Obstetricia. 2006;28(8):446–452. doi:10.1590/S0100-72032006000800002
15. Obed JY, Zarma A, Mamman L. Antenatal Complications in Adolescent Mothers Aged Below 14 Years. Afr J Med Med Sci. 1997;26(3–4).
16. Onu FA, Ajah LO, Ezeonu PO, Umeora OUJ, Ibekwe PC, Ajah MI. Profile and microbiological isolates of asymptomatic bacteriuria among pregnant women in Abakaliki, Nigeria. Infect Drug Resist. 2015;8:231–235.
17. Calegari SS, Konopka CK, Balestrin B, Hoffmann MS, de Souza FS, Resener EV. Resultados de dois esquemas de tratamento da pielonefrite durante a gravidez e correlação com o desfecho da gestação. Revista Brasileira De Ginecologia e Obstetricia. 2012;34(8):369–375.
18. Hooton TM, Scholes D, Stapleton AE, et al. A Prospective Study of Asymptomatic Bacteriuria in Sexually Active Young Women. New Engl J Med. 2000;343(14):992–997. doi:10.1056/NEJM200010053431402
19. Geerlings SE, Stolk RP, Camps MJL, et al. Asymptomatic bacteriuria may be considered a complication in women with diabetes. Diabetes Care. 2000;23(6):744–749. doi:10.2337/diacare.23.6.744
20. Yeta KI, Michelo C, Jacobs C. Antimicrobial Resistance among Pregnant Women with Urinary Tract Infections Attending Antenatal Clinic at Levy Mwanawasa University Teaching Hospital (LMUTH), Lusaka, Zambia. Int J Microbiol. 2021;2021. doi:10.1155/2021/8884297
21. Belete MA, Saravanan M. A systematic review on drug resistant urinary tract infection among pregnant women in developing countries in Africa and Asia; 2005–2016. Infect Drug Resist. 2020;13:1465–1477. doi:10.2147/IDR.S250654
22. Al-Sibai MH, Saha A, Rasheed P. Socio-Biological Correlates of Bacteruria in Saudi Pregnant Women. Public Health. 1989;103(2):113–121. doi:10.1016/S0033-3506(89)80025-3
23. Edae M, Teklemariam Z, Weldegebreal F, Abate D. Asymptomatic Bacteriuria among Pregnant Women Attending Antenatal Care at Hiwot Fana Specialized University Hospital, Harar, Eastern Ethiopia: magnitude, Associated Factors, and Antimicrobial Susceptibility Pattern. Int J Microbiol. 2020;2020:1763931. doi:10.1155/2020/1763931
24. Demilie T, Beyene G, Melaku S, Tsegaye W. Urinary bacterial profile and antibiotic susceptibility pattern among pregnant women in north west ethiopia. Ethiop J Health Sci. 2012;22(2):121–128.
25. Onoh R, Umeora E, Ezeonu P, Onoh T, Umeora O. Antibiotic sensitivity pattern of uropathogens from pregnant women with urinary tract infection in Abakaliki, Nigeria. Infect Drug Resist. 2013;6:225–233. doi:10.2147/IDR.S46002
26. Ayoyi AO, Kikuvi G, Bii C, Kariuki S. Prevalence, aetiology and antibiotic sensitivity profile of asymptomatic bacteriuria isolates from pregnant women in selected antenatal clinic from Nairobi, Kenya. Pan Afr Med J. 2017;26:41. doi:10.11604/pamj.2017.26.41.10975
27. Sibi G, Kumari P, Kabungulundabungi N. Antibiotic sensitivity pattern from pregnant women with urinary tract infection in Bangalore, India. Asian Pac J Trop Med. 2014;7(S1):S116–S120. doi:10.1016/S1995-7645(14)60216-9
28. Dempsey C, Harrison RF, Moloney A, Darling M, Walshe J. Characteristics of Bacteriuria in a Homogeneous Maternity Hospital Population. Eur J Obstet Gynecol Reprod Biol. 1992;44(3):189–193. doi:10.1016/0028-2243(92)90097-I
29. Baleiras C, Campos A, Lourenço I, Revez AI. Urinary tract infections and pregnancy. Acta Med Port. 1998;11(10):839–846.
30. Sujatha R, Nawani M. Prevalence of asymptomatic bacteriuria and its antibacterial susceptibility pattern among pregnant women attending the antenatal clinic at Kanpur, India. J Clin Diagn Res. 2014;8(4).
31. Kazemier BM, Koningstein FN, Schneeberger C, et al. Maternal and neonatal consequences of treated and untreated asymptomatic bacteriuria in pregnancy: a prospective cohort study with an embedded randomised controlled trial. Lancet Infect Dis. 2015;15(11):1324–1333.
32. Johnson B, Stephen BM, Joseph N, Asiphas O, Musa K, Taseera K. Prevalence and bacteriology of culture-positive urinary tract infection among pregnant women with suspected urinary tract infection at Mbarara regional referral hospital, South-Western Uganda. BMC Pregnancy Childbirth. 2021;21(1). doi:10.1186/s12884-021-03641-8
33. Tchente Nguefack C, Okalla Ebongue C, Nouwe Chokotheu C, Ebong Ewougo C, Nana Njamen T, Mboudou E. Clinical presentation, risk factors and pathogens involved in bacteriuria of pregnant women attending antenatal clinic of 3 hospitals in a developing country: a cross sectional analytic study. BMC Pregnancy Childbirth. 2019;19(1):1–6. doi:10.1186/s12884-019-2290-y
34. Schenkel DF, Dallé J, Antonello VS, Schenkel DF, Dallé J, Antonello VS. Prevalência de uropatógenos e sensibilidade antimicrobiana em uroculturas de gestantes do Sul do Brasil. Revista Brasileira De Ginecologia e Obstetrícia. 2014;36(3):102–106. doi:10.1590/S0100-72032014000300002
35. Poulsen LL, Bisgaard M, Son NT, Trung NV, An HM, Dalsgaard A. Enterococcus faecalis clones in poultry and in humans with urinary tract infections, Vietnam. Emerg Infect Dis. 2012;18(7):1096–1100. doi:10.3201/eid1807.111754
36. Abat C, Huart M, Garcia V, Dubourg G, Raoult D. Enterococcus faecalis urinary-tract infections: do they have a zoonotic origin? J Infect. 2016;73(4):305–313. doi:10.1016/j.jinf.2016.07.012
37. Alemu A, Moges F, Shiferaw Y, et al. Bacterial profile and drug susceptibility pattern of urinary tract infection in pregnant women at University of Gondar Teaching Hospital, Northwest Ethiopia. BMC Res Notes. 2012;5:197. doi:10.1186/1756-0500-5-197
38. Oli AN, Okafor CI, Ibezim EC, Akujiobi CN, Onwunzo MC. The prevalence and bacteriology of asymptomatic bacteriuria among antenatal patients in Nnamdi Azikiwe University Teaching Hospital Nnewi; South Eastern Nigeria. Niger J Clin Pract. 2010;13(4):409–412.
39. Sire J-M, Nabeth P, Perrier-Gros-Claude J-D, et al. Antimicrobial Resistance in Outpatient Escherichia coli Urinary Isolates in Dakar, Senegal. J Infect Develop Countries. 2007;1(03):263–268. doi:10.3855/jidc.362
40. Thomas T, Tony RL, Thomas A, et al. Antibiotic Resistance Pattern in Urinary Tract Infection during Pregnancy in South Indian Population. Asian J Pharm. 12;2:3.
41. Enayat K, Fariba F, Bahram N. Asymptomatic Bacteriuria among Pregnant Women Referred to Outpatient Clinics in Sanandaj, Iran. Asymptomatic Bacteriuria Among Pregnant Women Int Braz J Urol Int Braz J Urol. 34(34):699–707. doi:10.1590/S1677-55382008000600004.
42. Mathai E, Grape M, Go¨ G, Kronvall G. Integrons and multidrug resistance among Escherichia coli causing community-acquired urinary tract infection in southern India. APMIS. 2004;112:159–164. doi:10.1111/j.1600-0463.2004.apm1120301.x
43. Pancotto C, Lovison OVA, Cattani F. Perfil de resistência, etiologia e prevalência de patógenos isolados em uroculturas de gestantes atendidas em um laboratório de análises clínicas da cidade de Veranópolis, Rio Grande do Sul. Revista Brasileira De Análises Clínicas. 2019;51(1). doi:10.21877/2448-3877.201900799
44. Silva LMD, Macedo CFCE, Vasconcelos DP, Gomides MDA, Sadoyama G. Escherichia coli isoladas de infecção urinária em gestantes: perfil de resistência aos antimicrobianos. Enciclopédia Biosfera, Centro Científico Conhecer. 2014;10(19):231–239.
45. Yanase LE. Microbiotherapy pattern in uroculturas of the pregnant of the hospital santo antônio from blumenau and the patterns of sensitivity to antimicrobials. Arq Catarin Med. 2018;47(4):73–79.
46. Pereira AC, Bordignon JC. Infecção urinária em gestantes: perfil de sensibilidade dos agentes etiológicos de gestantes atendidas pelo SUS na cidade de Palmas - PR. Rev bras anal clin. 2011;43(2):96–99.
47. Oladeinde BH, Omoregie R, Oladeinde OB. Asymptomatic urinary tract infection among pregnant women receiving ante-natal care in a traditional birth home in Benin City, Nigeria. Ethiop J Health Sci. 2015;25(1):3–8. doi:10.4314/ejhs.v25i1.2
48. Tadesse E, Teshome M, Merid Y, Kibret B, Shimelis T. Asymptomatic urinary tract infection among pregnant women attending the antenatal clinic of Hawassa Referral Hospital, Southern Ethiopia. BMC Res Notes. 2014;7:155. doi:10.1186/1756-0500-7-155
49. Costelloe C, Metcalfe C, Lovering A, Mant D, Hay AD. Effect of antibiotic prescribing in primary care on antimicrobial resistance in individual patients: systematic review and meta-analysis. BMJ (Online). 2010;340(7756):1120.
50. van Driel AA, Notermans DW, Meima A, et al. Antibiotic resistance of Escherichia coli isolated from uncomplicated UTI in general practice patients over a 10-year period. Eur J Clin Microbiol Infect Dis. 2019;38(11):2151–2158. doi:10.1007/s10096-019-03655-3
51. Stapleton AE, Wagenlehner FME, Mulgirigama A, Twynholm M. Escherichia coli resistance to fluoroquinolones in community-acquired uncomplicated urinary tract infection in women: a systematic review. Antimicrob Agents Chemother. 2020;64(10). doi:10.1128/AAC.00862-20
52. Shigemura K, Tanaka K, Adachi M, Yamashita M, Arakawa S, Fujisawa M. Chronological change of antibiotic use and antibiotic resistance in Escherichia coli causing urinary tract infections. J Infect Chemother. 2011;17(5):646–651. doi:10.1007/s10156-011-0241-2
53. Joachim A, Matee MI, Massawe FA, Lyamuya EF. Maternal and neonatal colonisation of group B streptococcus at Muhimbili National Hospital in Dar es Salaam, Tanzania: prevalence, risk factors and antimicrobial resistance. BMC Public Health. 2009;9.
54. Rao GG, Nartey G, McAree T, et al. Outcome of a screening programme for the prevention of neonatal invasive early-onset group B Streptococcus infection in a UK maternity unit: an observational study. BMJ Open. 2017;7(4).
55. Aila NAE, Esleem SE, Elmanama AA. Prevalence of Group B Streptococcus Colonization among Pregnant Women in Gaza Strip. Palestine. 2017;25(3).
56. Gizachew M, Tiruneh M, Moges F, Tessema B. Streptococcus agalactiae maternal colonization, antibiotic resistance and serotype profiles in Africa: a meta-analysis. Ann Clin Microbiol Antimicrob. 2019;18:14. doi:10.1186/s12941-019-0313-1
57. Kawakita T, Wilson K, Grantz KL, Landy HJ, Huang CC, Gomez-Lobo V. Adverse Maternal and Neonatal Outcomes in Adolescent Pregnancy. J Pediatr Adolesc Gynecol. 2016;29(2):130–136. doi:10.1016/j.jpag.2015.08.006
58. Scholl TO, Hediger ML, Belsky DH. Prenatal care and maternal health during adolescent pregnancy: a review and meta-analysis. J Adolescent Health. 1994;15(6):444–456. doi:10.1016/1054-139X(94)90491-K
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.