Back to Journals » International Journal of General Medicine » Volume 13
Upper Limb Salvage of a Mangled Limb with Reconstruction of Brachial, Ulnar and Radial Arteries Using an Extremely Long Reversed Bifurcated Great Saphenous Vein: A Case Report with Long-Term Follow-Up
Authors Liu J, Dong S ![]() , Wang J, Liu H
, Wang J, Liu H ![]() , Wu Y, Rui Y
, Wu Y, Rui Y
Received 5 September 2020
Accepted for publication 11 November 2020
Published 24 November 2020 Volume 2020:13 Pages 1235—1241
DOI https://doi.org/10.2147/IJGM.S280616
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Jun Liu,* Sheng Dong,* Jianbing Wang, Hao Liu, Yongwei Wu, Yongjun Rui
Department of Orthopedics, Wuxi No.9 People’s Hospital Affiliated to Soochow University, Wuxi, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Yongjun Rui
Department of Orthopedics, Wuxi No.9 People’s Hospital Affiliated to Soochow University, 999 Liangxi Road, Wuxi, People’s Republic of China
Email [email protected]
Abstract: Acute elbow dislocation complicated by arterial injury of upper limb is rare but serious injury. We present the case about destructive injury of brachial, ulnar, and radial arteries with an open posterior dislocation of the right elbow, and a 25cm long reversed bifurcated great saphenous vein graft was applied for arterial reconstruction. The patient had obvious distal pulses after the operation. Ten years’ follow-up showed the good function of the right arm. Using an extremely long vein graft for the upper limb arterial reconstruction is challenging but feasible and provides good results.
Keywords: artery reconstruction, autologous vessel grafts, elbow dislocation, case report
Introduction
Trauma has become a public health problem in the world,1 and vascular injury is a major component of this problem.2 The elbow is the second most commonly dislocated joint.3 Despite this, concurrent vascular injury is uncommon, but it could threaten the viability and the flexibility of the arm and hand.4,5
Due to the anatomic proximity, elbow dislocation may run the risk of concomitant arterial injuries. The brachial artery is most commonly injured, occasionally involving the radial and ulnar arteries.6 At a rough estimate, the arterial injury is occurred in 5–13% of elbow dislocations, frequently encountered in the cases of open injuries.7,8
In this case report, we present a rare case about destructive injury of the brachial, ulnar, and radial arteries, with an accompanying open posterior elbow dislocation. We apply autologous vascular transplantation techniques to repair traumatic upper limb arteries. The destructive injury between the brachial, ulnar, and radial arteries was bridged by a 25cm long reversed bifurcated great saphenous vein. As we know, this is a novel case report where an autologous vascular transplantation technique was employed to repair very large arterial defect of upper limb with a long-term follow-up.
Case Presentation
A 35-year-old machinist on routine duty injured his right arm. He was a right-hand dominant man. This was an open injury and there was obvious arterial bleeding from a 15cm long wound over the antecubital fossa. On admission to the emergency department, the dressing was removed and the pulsatile bleeding was not obvious. The patient received a tetanus booster and antibiotic treatment. He was also given opioids to ease the pain. The patient continued to receive intravenous infusion and blood transfusion. Right upper extremity examination revealed a large laceration to the antecubital fossa and adipose, muscle, nerve, blood vessels, and bone tissue exposed. There was also swelling in the right forearm. The hand was noticed to be cold and decreased capillary refill. The radial artery and ulnar artery pulsation were disappeared. Sensory and motoric loss persisted. The examination of the nerves was not able to be performed due to the injury. Radiographs showed the right elbow posterior dislocation, radius and ulna diaphyseal fractures and distal radial fracture. These fractures were remarkable for severe angulation and displacement (Figure 1). It was a Gustilo-Anderson type-IIIC open injury,9 the mangled extremity severity score (MESS) was 8.10
 |
Figure 1 (A and C) X-ray demonstrated a posterior dislocation of the right elbow and fracture of radius and ulna. (B and D) Photographs above showed a massive musculoskeletal and neurovascular trauma with acute elbow dislocation. |
The patient then was taken to the operation room to explore the antecubital fossa in half an hour. A longitudinal machine direction incision about 25cm long was made over the antecubital fossa under the general anesthesia (Figure 2A). This patient had severe soft tissue, muscle, and nerve damage in the right forearm. The deep branch and the superficial branch of radial nerve were continuous but contused seriously. The median nerve was sheared off like a horsetail. The ulnar nerve was continuous. We performed debridement of all nonviable tissue (including inactivated and necrotic muscles), removed foreign bodies. We rinsed the wound immediately with plenty of diluted iodophor and isotonic saline. The joint reduction was the first priority. Then a lightweight external fixator was applied at 90° to protect the elbow from excessive movement. Fractures of the radius were treated by reduction, internal fixation with locking plates. A 20cm longitudinal incision was made on the dorsal side of the right forearm to expose the ulna fracture. It was also treated by reduction and internal fixation (Figure 2D). With clear evidence of distal ischemia, angiography was omitted to expedite surgical exploration of the antecubital fossa. Operative exploration of the antecubital fossa showed a destructive injury of the brachial artery, ulnar artery and radial artery and large arterial defect approximately 20cm in length. Direct suturing was impossible. After removing all bruised segments of the injured arteries, a 25cm long single reversed bifurcated great saphenous vein graft was performed to restore arterial continuity, because of a combination of ease of access and suitability of the vessel (Figure 2B). The successful arterial reconstruction was evaluated by the return of distal pulses (Figure 2C). We provided sketches in Figure 3. Because of the risk of compartment syndrome secondary to prolonged ischemia, substantial hemorrhage, and tissue reperfusion, prophylactic forearm fasciotomies were performed. The time from injury to vascular repair was ten hours.
 |
Figure 2 (A) A longitudinal machine direction incision about 25cm long was made over the antecubital fossa. (B and C) Intraoperative photographs before and after the reconstruction. (D) X-ray showed the internal fixation of fractures. |
 |
Figure 3 Diagrammatic sketch of this operation. (A) Select suitable saphenous vein. (B) Reverse. (C) Transplant. |
For postoperative management, the right elbow was fixed in place for four weeks. Then a limited range of motion from 20 to 100 degrees of flexion accompanied by physiotherapy for two weeks until the removal. Additional surgery was performed in the following years, including revision of fasciotomies, nerve repair (end to side neurorrhaphy of median nerve stump with ulnar nerve), tendon repair, further wound debridement, scar organization excise (skin soft-tissue expansion technique) and internal fixation removal (Figure 4). These surgeries were also key steps to get a good functional outcome. A timeline from the time of injury to the final surgery was listed in Figure S1.
 |
Figure 4 (A and B) Intraoperative photographs showed the scar organization excise (skin soft-tissue expansion technique). (C) Nerve repair (end to side neurorrhaphy of median nerve stump with ulnar nerve). (D) Postoperative photo. |
One year after the injury, the patient was able to use his fingers correctly. Two years after the injury, his hand function recovered well under the guidance of subsequent rehabilitation protocol and having S3 sensibility score on the thumb, index, and middle finger, S4 sensibility score on the ring finger and little finger by the evaluation standard of British Medical Institute. The patient has been followed for 10 years clinically. Although he was unable to return to his original occupation, he found an alternative employment. He was very satisfied with this limb salvage surgery. In the final outcome evaluated by Mayo elbow performance score (MEPS) was 90 which was considered excellent. The range of motion at the elbow joint had gradually improved with physical therapy. The movement of his right elbow was from 20 degrees of elbow extension to 100 of elbow flexion with slightly joint instability (Figure 5). Without any symptoms of impaired vascularity and confirmed by US Doppler. The hemodynamics of the reconstructed artery showed no signs of stenosis or aneurysm (Figure 6).
 |
Figure 5 (A–F) The photographs showed good functional results 10 years after the injury. (G) Wound healing of saphenous vein donor area. |
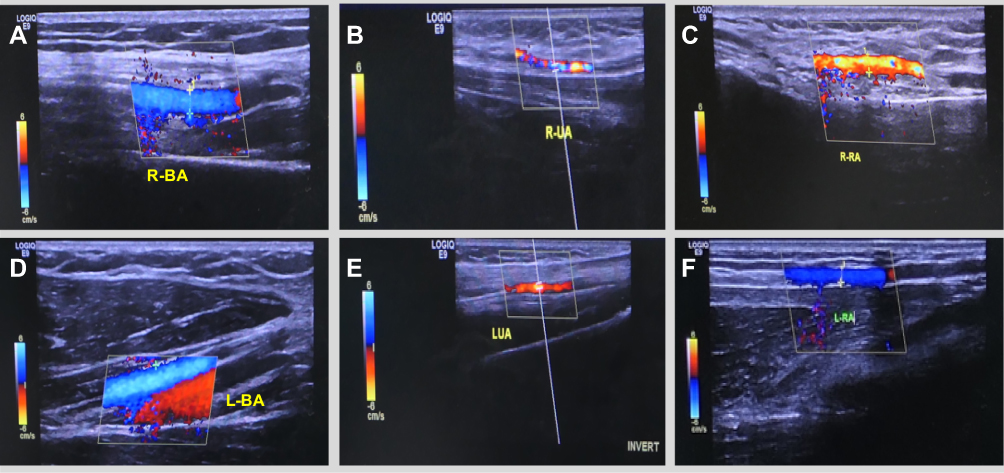 |
Figure 6 (A–C) The US Doppler result after reconstruction of the brachial, ulnar, and radial arteries via saphenous. (D–F) Left arm contrast. |
Discussion and Conclusion
The clinical diagnosis of upper limb arterial injury in the patient with acute elbow dislocation obvious because of the local signs of physical injury, distal pulse deficits, and sensory and motor deficits associated.11 Urgent operation is necessary.12,13 As a delay in operation is related to a poorer outcome.14
Some researchers have acquired a successful outcome with simple ligation of upper limb arterial lacerations following elbow dislocations to increase the pressure in the collateral circulation and gained satisfied results.15 These researchers attribute these satisfied results without vascular reconstruction to the extensive collateral anastomoses about the elbow. Although the collateral circulation around the elbow is deemed plentiful, Louis et demonstrated in cadaveric experiments that when the elbow dislocation was associated with arterial injury, the collateral vessels were disrupted in most cases.16 Besides, other researchers noted the complications of cold intolerance, numbness, ulcer, and gangrene after simple ligation of main upper limb arterial lacerations. They recommended immediate surgical exploration and rebuild the main arteries about the elbow.17–19 These findings have led to an intense debate regarding the best operation to treat these rare injuries. We believe vascular reconstruction must be essential because collateral circulation around the elbow is always disrupted after severe injury. Arterial reconstruction is believed to reduce the risk of delayed complications mentioned above.
Satisfactory emergency surgical management includes reduction of the elbow dislocation, fracture reduction and fixation, arterial reconstruction. We use different arterial reconstruction techniques according to the location, type and degree of arterial injury. Techniques for arterial reconstruction have included direct anastomosis of the two lacerated vascular ends, venous grafting with a reversed saphenous vein, and artificial vascular graft. Primary reconstruction of the vessel is preferable. If the defect between two ends of vessels is too large to access should be bridged with autogenous tissue or artificial vascular graft. As far as we are concerned, at the brachial artery bifurcation where end-to-end anastomosis is not possible, saphenous vein graft interposition is the first choice to maintain arterial continuity. The operation also includes repair the soft tissue and release the pressure on the nerves. Venous reconstruction is not compulsory, because there are usually enough collateral vessels. Fasciotomy may be necessary in patients with elevated compartment pressure, severe soft tissue injury, or ischemia for more than 4 hours.20
The successful treatment of the main artery injury can be life-saving. At the same time, allowing limb salvage and restoration of function. Reported rates of reconstructive major blood vessel thrombosis exceed 50% and a defect of the brachial artery longer than 10cm is extremely large and possibilities for revascularization are decreased.21 Late complications include anastomotic stenosis and graft thrombosis. By happy coincidence, after several operations, this patient demonstrates a successful long-term result of early reconstruction of the brachial, ulnar, and radial arteries using the extremely long bifurcated saphenous vein as an interposition autograft. The new venous conduit is free-flowing. There was also no sign of dilation or aneurysm degeneration. During the 10 years’ follow-up, the patients had normal vascular examinations, and the range of motion of right elbow was slightly limited.
Einstein once said, “In the middle of difficulty lies opportunity.” The authors made appropriate decisions leading to the operation of using an extremely long bifurcated saphenous vein for the upper limb arterial reconstruction. This operation is challenging but feasible and provides good results. With no implants and no immunosuppressive regimen needed, this operation also provides an excellent outcome.
In summary, the elbow dislocations are common and their association with main artery injuries is rare. Time is directly related to the outcome. Knowing the most effective treatment can be limb-saving.22 For very large arterial defect, especially at the brachial artery bifurcation where end-to-end arterial anastomosis is not possible, the application of an extremely long reversed bifurcated great saphenous vein as a vascular graft is feasible.
Abbreviations
MEPS, Mayo elbow performance score; MESS, The Mangled Extremity Severity Score; US Doppler, Ultrasound Doppler.
Data Sharing Statement
The data generated during the current research are not publicly available due to ethical restrictions.
Ethics and Consent
The study protocol was approved by the ethics committee of Wuxi No.9 People’s Hospital affiliated to Soochow University. Written informed consent was obtained from the patient for publication of this case report and any accompanying images.
Funding
There is no funding to report.
Disclosure
The authors declare no conflicts of interest.
References
1. Vecino-Ortiz PAI, Jafri PA, Health AAHJLG. Effective interventions for unintentional injuries: a systematic review and mortality impact assessment among the poorest billion. Lancet Glob Health. 2018;6(5):e523–e534.
2. Compton C, Rhee R, Therapy E. Peripheral vascular trauma. Perspect Vasc Surg Endovasc Ther. 2005;17(4):297.
3. Kuhn MA, Ross G. Acute elbow dislocations. Orthop Clin N Am. 2008;39(2):155–161.
4. Martin DJ, Fazzi UG, Leach WJ. Brachial artery transection associated with closed and open dislocation of the elbow. Eur J Emerg Med. 2005;12(1):30–32. doi:10.1097/00063110-200502000-00008
5. Dabboussi NA, Fakih RR, Kassar TA, Abtar HK. Occult closed posterior elbow dislocation with intimal rupture of the brachial artery in a 71-year-old male†. J Surg Case Rep. 2014;2014(12):rju140–rju140. doi:10.1093/jscr/rju140
6. Rodríguez-Niedenführ M, Sañudo JR, Vázquez T, Nearn L, Logan B, Parkin I. Anastomosis at the level of the elbow joint connecting the deep, or normal, brachial artery with major arterial variations of the upper limb. J Anat. 2000;196(1):115–119. doi:10.1017/S0021878299005737
7. Nazli Y, Colak N, Uras I, Komurcu M, Cakir OJV. Brachial artery transection associated with open elbow dislocation in a 12-year-old: a case report. Vascular. 2013;21(1):27–30.
8. Thomas LG, Williams DT. Simple posterior elbow dislocation and brachial artery transection. J R Army Med Corps. 2012;158(1):50–52. doi:10.1136/jramc-158-01-13
9. Gustilo RB, Anderson JTJJBJSA. Prevention of infection in the treatment of one thousand and twenty-five open fractures of long bones: retrospective and prospective analyses. J Bone Joint Surg Am. 1976;58(4):453–458.
10. Helfet DL, Howey T, Sanders R, Johansen KJCO. Limb salvage versus amputation. Preliminary results of the mangled extremity severity score. Clin Orthop Relat Res. 1990;256(256):80–86.
11. Endean ED, Veldenz HC, Schwarcz TH, Hyde GL. Recognition of arterial injury in elbow dislocation. J Vasc Surg. 1992;16(3):402–406. doi:10.1016/0741-5214(92)90374-H
12. Shalabi R, Al Amri Y, khoujah EJJVB. Vascular injuries of the upper extremity. J Vasc Bras. 2006;5(4):271–276.
13. Steinke A, Grosel J. A guideline to efficiently treating traumatic brachial artery injury. JAAPA. 2013;26(12):1–4. doi:10.1097/01.Jaa.0000438242.87331.93
14. Ergüneş K, Yazman S, Yetkin U, Cakır V, Gurbuz A. Axillary artery transection after shoulder dislocation. Ann Vasc Surg. 2013;27(7):
15. Wolfswinkel EM, Weathers WM, Siy RW, Horowitz KS, Hollier LH. Less is more in the nonoperative management of complete brachial artery transection after supracondylar humeral fracture. Ann Vasc Surg. 2014;28(3):
16. Louis DS, Ricciardi JE, Spengler DM. Arterial injury: a complication of posterior elbow dislocation. A clinical and anatomical study. J Bone Joint Surg Am. 1974;56(8):1631–1636. doi:10.2106/00004623-197456080-00012
17. Fleischer G, Fletcher JP, Whiteway DW. Compound elbow dislocation and brachial artery rupture. Aust N Z J Surg. 1980;50(4):408–409. doi:10.1111/j.1445-2197.1980.tb04151.x
18. Manouel M, Minkowitz B, Shimotsu G, Haq I, Feliccia J. Brachial artery laceration with closed posterior elbow dislocation in an eight year old. Clin Orthop Relat Res. 1993;(296):109–112.
19. Phang ZH, Miskon MFB, Ibrahim SB. Blunt trauma to the antecubital fossa causing brachial artery injury and minor fractures around the elbow joint, an easily missed diagnosis with potential devastating consequences: a case report. J Med Case Rep. 2018;12(1):211. doi:10.1186/s13256-018-1751-7
20. Ferrera PC. Elbow dislocation complicated by brachial artery laceration. Am J Emerg Med. 1999;17(1):103–105. doi:10.1016/s0735-6757(99)90032-3
21. Pavić R. Major defect to the brachial artery following blunt trauma – a five year follow-up. Coll Antropol. 2011;35(1):203–205.
22. Redjil N, Dabire MN, Weber P. Open elbow dislocation associated with distal ischemia in children about one case and review of the literature. Pan Afr Med J. 2015;21:128. doi:10.11604/pamj.2015.21.128.6553
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.