Back to Journals » Infection and Drug Resistance » Volume 15
Updated Seroprevalence of Hepatitis B Surface Antigen and Anti-Hepatitis Core Antibody Among Blood Donors in Yemen
Authors Alzubiery TKA ![]() , Alhazari T
, Alhazari T ![]() , Alcantara JC
, Alcantara JC ![]() , Majed SA, Bazaid AS
, Majed SA, Bazaid AS ![]() , Aldarhami A
, Aldarhami A ![]()
Received 20 January 2022
Accepted for publication 3 May 2022
Published 31 May 2022 Volume 2022:15 Pages 2787—2796
DOI https://doi.org/10.2147/IDR.S357819
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Héctor Mora-Montes
Tawfique KA Alzubiery,1 Talal Alhazari,2,3 Jerold C Alcantara,2 Saleh A Majed,4 Abdulrahman S Bazaid,2 Abdu Aldarhami5
1Department of Medical Laboratory, Faculty of Medical and Health Sciences, Taiz University Al-Turbah Branch, Taiz, Yemen; 2Department of Medical Laboratory Sciences, College of Applied Medical Sciences, University of Hail, Hail, Saudi Arabia; 3Department of Medical Microbiology and Immunology, Faculty of Medicine and Health Sciences, Taiz University, Taiz, Yemen; 4National Blood Transfusion and Research Center, Sana’a, Yemen; 5Department of Medical Microbiology, Qunfudah Faculty of Medicine, Umm Al-Qura University, Makkah, Saudi Arabia
Correspondence: Talal Alhazari, Department of Medical Laboratory Sciences, College of Applied Medical Sciences, University of Hail, Hail, Saudi Arabia, Tel +966 531036805, Email [email protected]
Purpose: Hepatitis B virus (HBV) is one of the most common infectious pathogens worldwide. Various studies found a prevalence of HBV infection among blood donors ranging from 2% to 18%. Hence, this study aimed to provide an updated prevalence of HBsAg and anti-HBcAb among blood donors.
Patients and Methods: This was a cross-sectional study to investigate the donation records of blood donors in Sana’a, Yemen, over one year (January to December 2019). Eligible blood donors were included in the study. The serum samples of blood donors were tested for HBsAg and anti-HBcAb (IgG & IgM) using the electrochemiluminescence (ECL) and enzyme immunoassay (EIA) techniques.
Results: A total of 16,367 blood donors were recruited in this study, of whom 14,300 (87.4%) donated only once during this study (single, non-duplicated blood donors), while 2067 (12.6%) were repeated or duplicated. The overall prevalence of HBsAg and anti-HBcAb was 2.4% and 10.8%, respectively. Among single non-duplicated blood donors, HBsAg and Anti-HBcAb were 2.3% and 10.6% and 3.0% and 12.5% for repeated blood donors, respectively. There were statistically significant differences between HBsAg and Anti-HBcAb in terms of donor type and testing techniques.
Conclusion: The seroprevalence of HBsAg and anti-HBcAb among the blood donors was 2.0% and 10.3%, respectively. The ECL technique is more sensitive, has a lower error rate, and shows an advantage over the manual EIA technique. Duplicated blood donors influence the accuracy of the seroprevalence of HBsAg and anti-HBcAb.
Keywords: hepatitis infections, serological markers, transfusion transmissible infections, blood transfusion, Yemen
Introduction
The World Health Organization (WHO) Global Database on Blood Safety estimates over 92 million blood donations annually.1 However, blood transfusion is not entirely free from the risk of transmission of infectious agents, such as Hepatitis B Virus (HBV), Hepatitis C Virus (HCV), Human Immunodeficiency Virus (HIV), Treponema pallidum, and malarial parasites.1 Due to infectious agents such as HIV, HBV, HCV, and syphilis, about 1.6 million units are discarded.2 WHO has recommended that pathogens causing transfusion-transmissible infections (TTIs) must be tested on all blood collected from blood donors.1 HBV has infected over 2 billion people, with 360 million having chronic HBV infections and 3.0 million new infections per year.3,4 Furthermore, over 1.1 million deaths per year are associated with HBV infections, and is the fifth leading cause of cancer in the world.5,6
Several studies reported different rates of HBsAg in blood donors, from 1.2%, 1.4%, and 2.3% in Saudi Arabia,9 Jordan7 and Iraq,8 to 4.3%, 5.1%, and 5.62% in Sudan,10 Syria,11 and Egypt,12 respectively. In Yemen, the prevalence of HBV infection among blood donors ranges from 2% to 18%, as documented by many studies, where Yemen consequently falls into the intermediate to high endemicity category.13–15
Previous studies revealed different results regarding viral hepatitis and HIV prevalence among blood donors.14,16 It was noted that there was a discrepancy in the results, necessitating more investigation to improve and understand these variations and their impact. Hence, the purpose of this study was to update the prevalence rate of HBsAg and anti-HBc among blood donors and determine the reliability of using chemiluminescence and ELISA techniques as well as identifying the effect of duplicated or repeated blood donations on the results.
Materials and Methods
Study Population
The study is a prospective, cross-sectional design from January 2019 to December 2019. Serological testing of donor samples was done in the Virology laboratory. This study was conducted on all blood donors who visited the National Blood Transfusion and Research Centre in Sana’a, Yemen. Donors were divided into two groups: those who donated once during the study and those who donated more than once.
Study Tools
A designed, self-administered questionnaire was used in collecting the data. Blood donors who could not read and write were interviewed face-to-face by a trained public health specialist to fill out the questionnaire. The questionnaire included demographic information (age, gender, residency, occupation) and blood donation history. The NBTRC has no electronic or digital donor registry records and relies mainly on the blood donor logbooks recorded manually by the staff members. Hence, a critical issue is monitoring donation history for repeated blood donors who are still not eligible to donate due to inadequate donation intervals.
Individuals coming for blood donations were divided into four (4) groups according to occupation: students, professionals, manual workers, and military personnel. Professional workers are individuals who have educational qualifications, such as teachers, engineers, health workers, and employees, among others. Manual workers have low academic qualifications or have their own businesses, such as carpenters, plumbers, drivers, and waiters, among others.
Routine examinations, including blood pressure, hemoglobin level, pulse rate, and other general health checkups, were performed on all the blood donors. Healthy individuals aged 16 to 65 years old and weighing more than 45 kg were considered for blood donations. Both voluntary and replacement blood donors who met the required criteria for blood donation were included in the study.
Assessment of HBsAg and Anti-HBcAb
During the study, two techniques were employed. The Electrochemiluminescence (ECL) technique was used as the primary method for detecting HBsAg and Anti-HBcAb, and the enzyme immunoassay (EIA) technique (manual) was used as a backup if the ECL technique is not available.
Blood samples (5 mL) were aseptically collected by trained lab technicians using a disposable syringe. The blood sample was allowed to clot in a sterile tube before centrifugation. A total of 11,121 (77.8%) serum samples were separated and analyzed for HBsAg and Anti-HBcAb (IgG and IgM) by the ECL technique using the Immunoassay Cobas e 411 analyzers (Roche ELECSYS® 2010 GmbH; Germany). The remaining 3178 (22.2%) serum samples were analyzed for HBsAg and total anti-HBcAb (IgG, IgM) by the enzyme immunoassay (EIA) technique (MonolisaTM HBsAg ultra, no.72348; MonolisaTM anti-HBc plus, no.72316; MonolisaTM; BioRad Diagnostics, 92430 Marnes-la-Coquette, France) according to manufacturer instructions.
The HBsAg is the first line of screening for HBV infections in blood donors prior to donation. Samples that have initially reactive results are tested repeatedly in duplicate. If one or both tests are positive, the blood donor is deferred indefinitely for donation. Confirmatory testing using HBV NAT (Nucleic acid testing) is not routinely done but is available in the Blood Center and special private laboratories at the blood donor’s expense.
Study Ethics
Consent to conduct this study was reviewed and approved by the Faculty of Medicine, Taiz University (IRB-2019-01-012) and the National Blood Transfusion and Research Centre in adherence to the Declaration of Helsinki. Informed consent was obtained from the study participants prior to study commencement. Blood donors’ data confidentiality was strictly observed, and all related ethics were fully considered.
Statistical Analysis
The HBsAg and Anti-HBcAb prevalence were observed and expressed as frequencies and percentages. Socio-demographic variables and other population characteristics were computed an analyzed using SPSS (version 21). The Chi-squared test was employed to determine the statistical difference. The significance level was set at P value <0.05.
Results
Screening for HBsAg and Anti-HBcAb was determined for all blood donors. A total of 16,367 blood donor specimens were collected and subjected to routine investigations and detection of HBsAg and Anti-HBcAb. The overall HBsAg and anti-HBcAb were 2.4% and 10.8%, respectively. Of the total blood donors, 14,300 (87.4%) were single, non-duplicated blood donors, while 2067 (12.6%) were recorded as repeated or duplicated blood donors. Single, non-duplicated blood donors were selected for further data analysis, whereas repeated or duplicated blood donors were excluded to prevent result duplications. The seropositivity of HBsAg and Anti-HBcAb among 14,300 selected (single or non-duplicated) blood donors was 2.3% and 10.7%, compared to 3.1% and 11.7% of HBsAg and Anti-HBcAb among 2067 repeated or duplicated blood donors, respectively. This difference in the rates of HBsAg and Anti-HBcAb was found to be statistically significant (P<0.05) (Table 1). Further analysis revealed that the seropositivity of anti-HBc alone was higher (10.8%) in comparison to the seropositivity of HBsAg/anti-HBc (1.2%) in all blood donors. For non-duplicated blood donors, 10.6% (CI: 1.044–1.329) was reactive to Anti-HBc only but 1.7% (CI: 0.532–1.101) was reactive to both HBsAg and anti-HBc, whereas, 12.5% (CI: 0.955–0.995) for duplicated blood donors were positive for anti-HBc, and only 1.6% (CI: 0.921–2.012) for HBsAg and anti-HBc (Table 2).
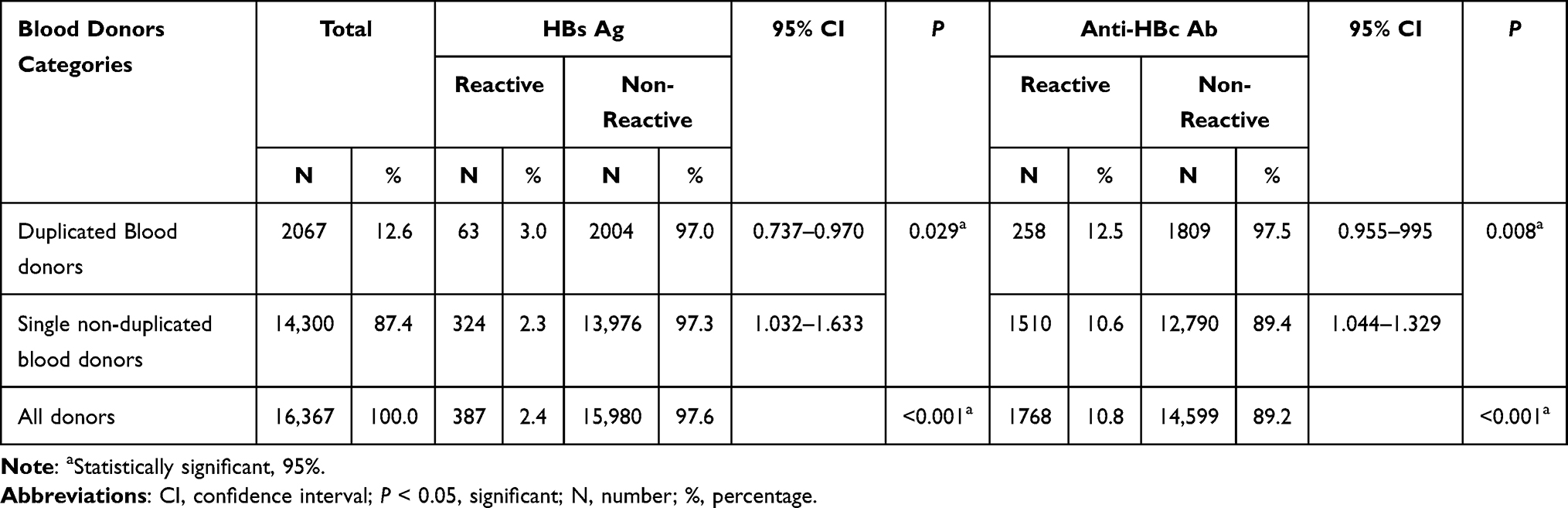 |
Table 1 The Overall Frequency of HBs Ag and Anti-HBc Ab Among Population of the Study |
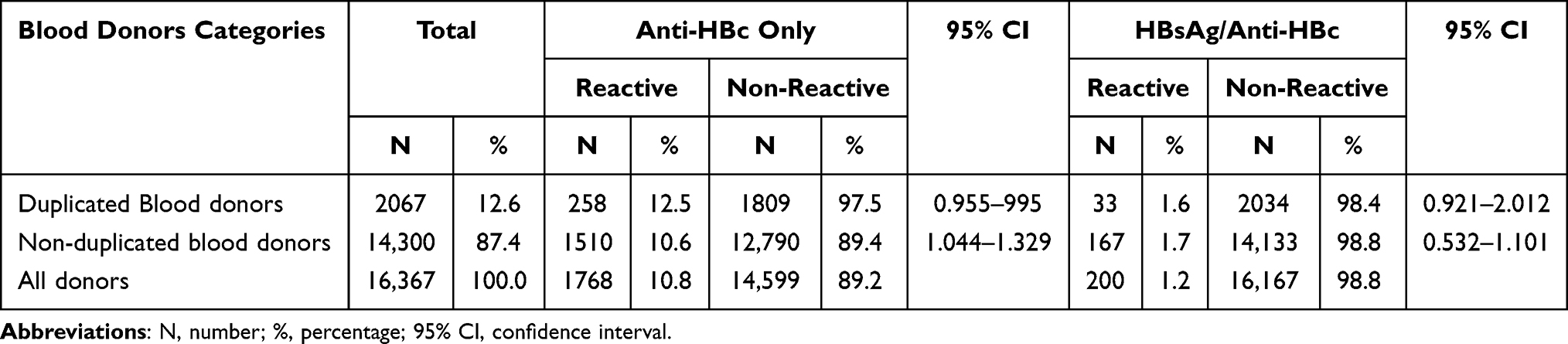 |
Table 2 The Frequency of Anti-HBc Ab and HBsAg/Anti-HBc Among Population of the Study |
Among the single non-duplicated blood donors, the number of males was 14,148 (98.9%), with a mean age of 30.07 years. Of those, 10,369 (72.5%) were replacement donors, and 3933 (27.5%) were voluntary donors (Table 3). Moreover, the seropositivity of HBsAg and anti-HBcAb was higher among males, with 2.3% and 10.6% rates, respectively. Predominantly, blood donors were manual workers (32.7%) and professionals (32.2%). The seropositive rates of HBsAg and Anti-HBcAb among the blood donors ranged from 2.2% to 2.3% and from 10.0% to 11.1% for HBsAg and Anti-HBcAb, respectively. The difference in the rates of HBsAg and Anti-HBcAb, according to occupational categories, was found to be statistically insignificant (χ2= 0.3 and P = 0.961).
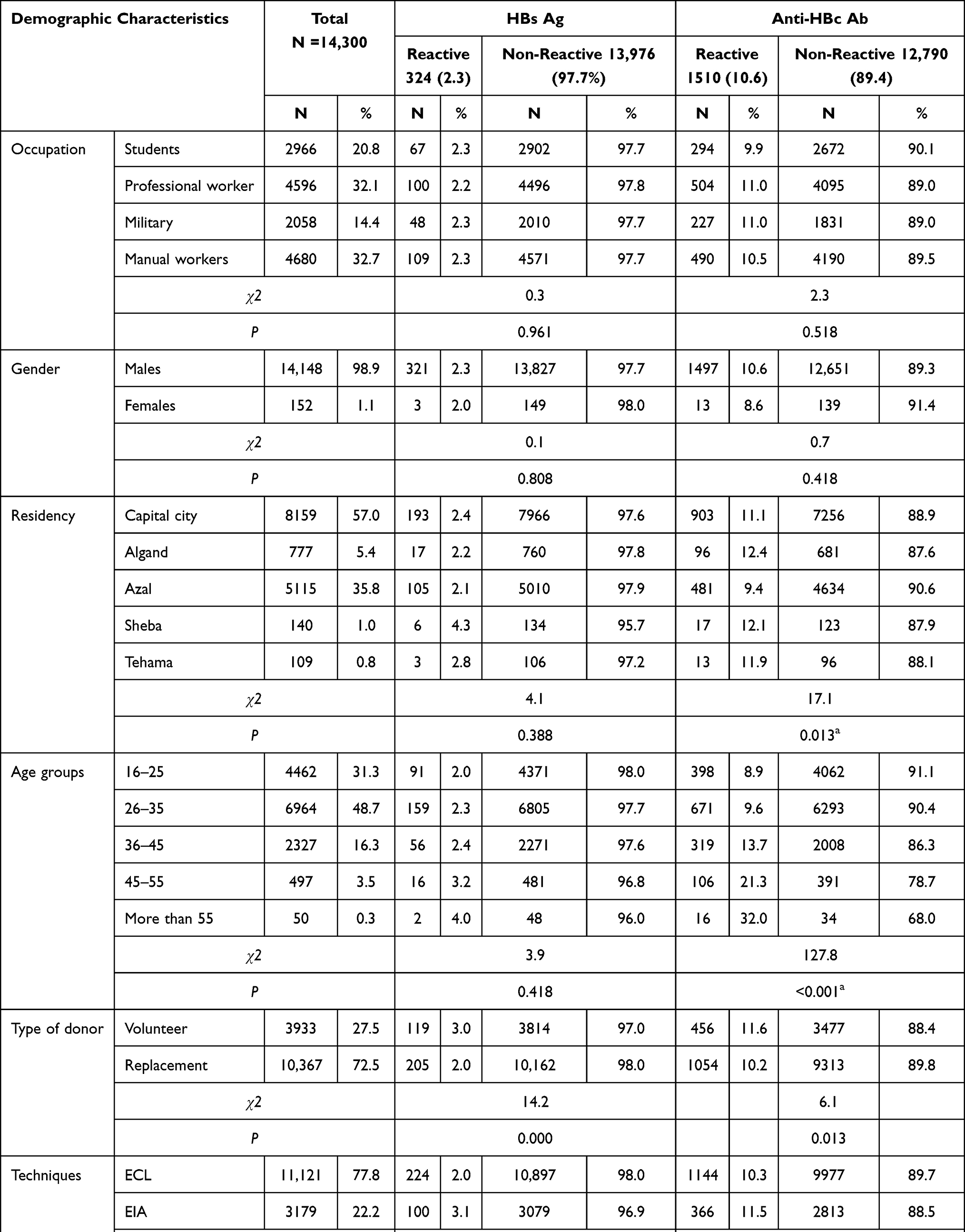 |
Table 3 Seropositive Rates of HBs Ag, and Anti-HBc Ab in Relation to Demographic Characteristics of Blood Donors |
There was no statistical significance in the difference in the prevalence of HBsAg or Anti-HBcAb among donors according to their residency. The lowest positivity rates of HBsAg (2.1%) and Anti-HBcAb (9.4%) were observed among blood donors from Azal, while the highest seropositive rates were found in Sheba and Algand regions, with a rate of 2.1% (HBsAg) and 12.4% (Anti-HBcAb), respectively.
Most blood donors were aged 26 to 35 years, accounting for nearly half of the donor population (48.7%). Notably, the seropositivity rate of HBsAg and Anti-HBcAb gradually rises as age increases, with the highest rates of 4.0% and 32.0%, respectively. In contrast to HBsAg, the results of anti-HBcAb among the various age groups were found to be statistically significant.
Furthermore, the difference in the prevalence rates of HBsAg among voluntary (3.0%) and replacement donors (2.0%) was statistically significant (χ2 = 14.2 and P <0.001). Similar observations were found for anti-HBcAb among volunteers (11.6%) compared to replacement (10.3%) donors (χ2= 6.1 and P = 0.013). As shown in Table 3, we calculated the difference between the results of HBsAg using ECL (2.0%) and EIA (3.1%) techniques, and it was found to be statistically significant (χ2= 14.3 and P <0.001). Similarly, a significant difference exists (χ2= 3.9 and P = 0.047) in the results of anti-HBcAb using the 2 techniques (ECL, 10.3%; EIA, 11.5%).
Blood groups were also carried out on 11,069 donors. Of these, 10,076 (91.0%) and 993 (9.0%) were positive and negative for the Rhesus factor, respectively. The rates of O, A, B, and AB blood groups were 55.6%, 32.8%, 8.9%, and 2.7, respectively (Table 3). Positivity of HBsAg was found to be highest in group A (6.6%) blood donors, while anti-HBcAb was found in group B blood donors (26.7%). However, the difference between the results of blood groups and HBs Ag (χ2= 0.1 and P = 0.707) and Anti-HBc Ab (χ2= 0.8 and P = 0.359) was found to be statistically insignificant (Table 4).
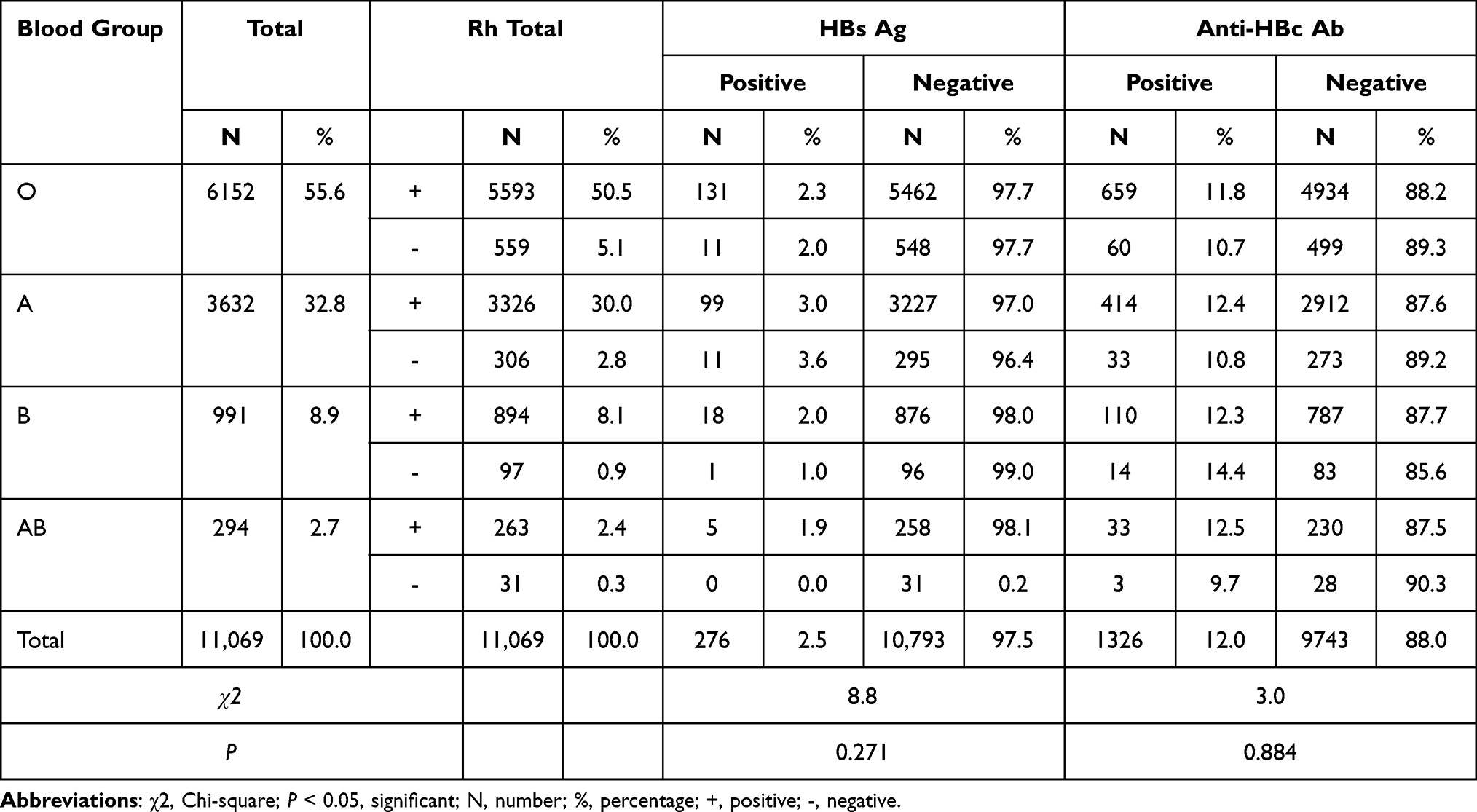 |
Table 4 Distributions of Blood Groups and Rh in Relation to HBs Ag and Anti-HBc Ab |
Discussion
The overall prevalence rate (2.4%) of HBsAg among blood donors in this study was analogous to the studies carried out in various locations such as Yemen (2.6%),17 Ethiopia (2.6%),18 and India (2.12%).19 However, the seropositivity rate of the present study was higher than our previous study (1.9%).16 A low prevalence of HBsAg was reported in Iraq (0.24%),20 Jordan (0.3%),21 and Malaysia (0.03%).22 The present study revealed a lower prevalence rate of HBsAg than those reported rates in Saudi Arabia (3.24%),23 Yemen (4.1%),14 Sudan (5.8%),24 Nigeria (5.8%),25 Ethiopia (3.0%),26 Cameroon (11.2%),27 the Central African Republic (16.7%)28 and Mauritania (11.8%).29
The positivity rate of anti-HBcAb in the present study was 10.9%. Comparable rates were reported in Syria30 (10.3%) and Tamil, India (10.9%).31 A higher rate of anti-HBcAb was found in Ibadan (16.9%), Iran,32 and Abuja (17.7%), Nigeria.33 Lower rates, however, were reported in studies in Iran34 (4.9%), Saudi Arabia (5.7%),35 and Jordan (2.0–4.1%).21
Notably, significantly higher seropositivity for HBsAg (3.1%) and Anti-HBcAb (11.7%) among duplicated blood donors compared to single non-duplicated blood donors was observed. This could be explained by duplicating test results for donors who donated more than once. Since digital donor registry records are not available in the center, test results could have been recorded repeatedly. Similarly, repeated blood donors, who were ineligible to donate due to inadequate donation interval, could have contributed to the increased seroprevalence of infection. Monitoring donation history is a critical and currently existing problem. Another possible explanation for this was that most of the duplicated blood donors could be paid blood donors chosen by patients’ relatives without care if free for viral hepatitis infections. The prevalence of infection is extremely high among paid donors and making blood donation their source of income.36 It was reported that HCV prevalence among paid blood donors was as high as 5.7% or more.6 On the contrary, lower HCV prevalence is seen among voluntary donors and employer-organized blood donations, with rates of between 1.1 to 2.3% and 0.46%, respectively.37,38 The present study also found that the difference in results between these two groups was statistically significant. To get the acceptable prevalence rate of HBsAg and Anti-HBcAb, we excluded all duplicated cases of blood donors.
This present study further revealed that a significant difference exists between the results of ECL and manual EIA techniques. This could be related to the advantage of fully automatic ECL over manual colorimetric EIA, where the anticipation of contamination is higher. The difference in the results obtained by these techniques could be linked to the sensitivity of ECL, where another study found that the ECL assay was two to four times more sensitive than the colorimetric EIA, at least for the detection of protein antigens or antibodies.39 This explained the difference in the prevalence rates of HBsAg (2.0% and 3.1%) and Anti-HBcAb (10.3% and 11.5%) by ECL and EIA in this present study and the previous study, where the rate of HBs was 4.1% and 1.9% by ECL and EIA, respectively.14,16
Results of this study showed that the frequency of HBsAg in blood donors was not associated with their occupation. This was similar to the results found in the previous study.14 Nevertheless, the incidence of HBsAg and anti-HBcAb in the present study, according to their occupational categories, was lower than the reported rate in the first study. This could be attributed to the different techniques used in the present study (ECL) than our previous study14 (EIA). The present study confirms this validity, where the difference in the prevalence rates of HBsAg (2.0% and 3.1%) and Anti-HBcAb (10.3% and 11.5%) was obtained by ECL, and manual colorimetric EIA was found to be statistically significant.
The prevalence rate (2.3%) of HBsAg in this study with respect to the occupation of blood donors was similar to the findings in Cameroon (2.4%).27 A higher rate of HBsAg (8.9% to 11.0%) was reported in Sierra Leone40 This study also observed a lower (2.3%) prevalence of HBsAg among students than the studies in Ethiopia (4.7%),41 (3.4%),42 and Sierra Leone (10.7%).40 In contrast to this present study, our previous study revealed statistical significance (χ2 = 1.2 and P <0.001) in the different rates of anti-HBcAb (ranging from 8.8% to 16.2%) concerning their occupational categories. These differences could be related to the larger sample size and greater precision of the ECL technique used in the present study compared to the smaller sample size and low precision of the manual EIA technique employed during the previous study.14 Higher HBsAg among students (11.7% and 6.9%) and the military (5.1% and 8.4%) were reported in Saudi Arabia43 and Gabon.44
Male donors showed a seropositivity rate of 2.3% for HBsAg. This is consistent with the study carried out in Basra, Iraq (2.3%), and Sana’a, Yemen (2.7%).16 Statistically, no difference exists between HBsAg rates in males and females (P = 0.808). Similarly, the prevalence was reported with the same findings (P = 0.464) with rates of 2.4% and 1.7% in males and females,45 respectively. Lesser positivity rates of HBsAg were reported in the study in Jordan, with 0.013% and 0.37% in males and females, respectively.46 Furthermore, a similar rate of HBsAg among females was reported in Kenya (1.3%)47 while a higher rate was found in the other studies (3.7%)9 and (17.7%).48 A lower rate (1.0%) of HBsAg among females than in the present study was reported in Cameroon27 and Kenya47 with an account of 1.0% and 1.3%, respectively. However, higher rates of HBsAg positivity in males were documented in other studies (13.1%),47 (10.5%),27 and (10.6%).28
Notably, the seropositivity of HBsAg and Anti-HBcAb rises as age increases. This was also noted in various studies conducted internationally.14,35,49 A recent study revealed prevalence rates of HBsAg and Anti-HBc Ab among the different age groups fairly similar to that study conducted in Sana’a city, Yemen.16
The rates of anti-HBcAb in relation to the residence of blood donors were statistically significant (P = 0.013). In contrast, the positivity rates of HBsAg were not significant. This result is consistent with the study conducted in Sana’a city, Yemen.14 In the current study, the prevalence of HBsAg and Anti-HBcAb ranged from 2.1% to 4.3% for HBsAg and 9.4% to 12.4% for Anti-HBcAb, which was lower than in the previous study,14 as it ranged from 3.3% to 10.8% for HBsAg and 12.7% to 35.1% for Anti-HBcAb.
The variation of HBsAg and Anti-HBcAb prevalence rates in the present study compared to our previous study14 could be related to several reasons. First, the exclusion of duplicated donors in the present study; second, the advantage and quality of ECL employed in the present study over the manual EIA technique, which was used in the previous study; and lastly, the former study classified the residency of donors based on their governorates of residence. Hence, to overcome the problem of the low number of donors representing such governorates, we classify the residency of donors according to the new Republic of Yemen classification system, which is based on the province classification system. All the aforementioned reasons could play a significant role in obtaining reliable results, which can reflect the exact rate of HBsAg among this segment of the Yemeni population.
The positivity rate (3.0%) of HBsAg among the voluntary in the present study was higher than the studies in Saudi Arabia (2.4%)35 and Ethiopia. (2.5%).42 There was a lower prevalence (2.0%) among replacement donors in this study than in the studies of Saudi Arabia (4.5%)35 and Ethiopia (4.1%).42 The high rates of HBsAg and Anti-HBcAb among voluntary blood donors as compared to replacement donors can be explained as a result of the careful selection of patients’ relatives as family replacement donors. Hence, most such donors have prior knowledge, as they are free of infection and eligible to donate blood, in contrast to volunteers who have no prior knowledge of infections that affect blood donation. Hepatitis B reactive blood donors are informed of their infection status verbally and are advised to seek for more medical consultation. They are deferred to donate indefinitely.
Methods used for screening blood donors in Yemen may differ from one blood bank to another, but mostly use high-accuracy techniques, especially in central blood banks and donation centers, which use ELISA and Chemiluminescence, while others use chromatography, particularly in remote areas. The lack of materials and kits caused an acute shortage of supplies during the war, which prevented the use of the previously mentioned modern methods in detecting hepatitis viruses in blood donors.
The WHO recommended Hepatitis B vaccinations among the Yemeni population, to be part of the national immunization program of Yemen in 1998, especially among neonates who are at a higher risk of vertical transmission.50 According to the latest WHO/UNICEF Estimates of National Immunization Coverage (WUENIC) for Yemen,51 which are based on data reported until 5 October 2021, the vaccination coverage of the country is 73% for HepB3 (Hepatitis B vaccine, third dose). Vaccine coverage is defined as the percentage of infants (children under one year of age) who received certain vaccine-doses.51 Moreover, Hepatitis B vaccinations are carried out by health workers, and are available to citizens.
Conclusion
The seroprevalence of HBsAg and anti-HBcAb among Yemeni donors was 2.0% and 10.3%, respectively. The ECL technique showed enhanced sensitivity and advantage over the manual EIA technique. Duplicated blood donors influence the accuracy of the seroprevalence of HBs Ag and Anti-HBc Ab. Further study on first-time volunteer donors is required to better understand the prevalence of HBV among healthy adults. Screening of other infections, including HIV, HCV, and the prevalence of other transfusion-related infections is necessary among Yemeni blood donors.
Acknowledgment
We sincerely appreciate the staff members of the Virology unit and Blood Bank at the National Blood Transfusion and Research Centre in Sana’a, Yemen.
Disclosure
The authors report no conflicts of interest in this work.
References
1. World Health Organization. Blood safety and availability, WHO fact sheet. No. 279; 2017. Available from: http://www.who.int/mediacentre/factsheets/fs279/en/.
2. World Health Organization. Blood donor selection: guidelines on assessing donor suitability for blood donation. World Health Organization; 2012 Available from: https://apps.who.int/iris/handle/10665/76724.
3. World Health Organization. Global progress report on HIV, viral hepatitis and sexually transmitted infections, 2021. Accountability for the global health sector strategies 2016–2021: actions for impact. Available from: https://www.who.int/publications/i/item/9789240027077.
4. United Nations Office on Drugs and Crime. HIV prevention, treatment, care and support for people who use stimulant drugs. technical guide; UNODC; Vienna; 2019. Available from: https://www.unodc.org/documents/hiv-aids/publications/People_who_use_drugs/19-04568_HIV_Prevention_Guide_ebook.pdf.
5. Quadri SA, Dadapeer HJ, Arifulla M, Khan N. Prevalence of Hepatitis B surface antigen in hospital based population in Bijapur, Karnataka. Al Ameen J Med Sci. 2013;6(2):180–182.
6. Sood S. Serological evaluation of Hepatitis B virus in outpatient department patients of a private hospital in North – west India. National J of Community Medicine. 2013;4:485–488.
7. Alcantara JC, Alenezi FK, Haj Ali OH. Seroprevalence and trends of markers of transfusion transmissible infections among blood donors: a 3-year hospital based-study. Int J Community Med Public Health. 2018;5(12):5031–5035. doi:10.18203/2394-6040.ijcmph20184773
8. Al-Gani FA. Prevalence of HBV, HCV and HIV-1, 2 infections among blood donors in Prince Rashed Ben Al-Hassan hospital in North region of Jordan. Int J Biol Med Res. 2011;2(4):912–916.
9. Al-Rubaye A, Tariq Z, Alrubaiy L. Prevalence of hepatitis B seromarkers and hepatitis C antibodies in blood donors in Basra, Iraq. BMJ Open Gastroenterol. 2016;3(1):e000067. doi:10.1136/bmjgast-2015-000067
10. Karim M, Lahham H. Prevalence of viral hepatitis B and C in Syria. Syr Epidemiol Bull. 2008;2(3):10–11.
11. Nagi AM, Altyeb HA, Ahmed AM. Seroprevalence of Hepatitis B and C viral infections among blood donors in Shendi, River Nile State, Sudan. Res J Med Sci. 2007;2(2):122–126.
12. El-Gilany AH, El-Fedawy S. Bloodborne infections among student voluntary blood donors in Mansoura University, Egypt. East Mediterr Health J. 2006;12(6):742–748.
13. Alodini AQ. Prevalence of Hepatitis B Virus (HBV) and Hepatitis C Virus (HCV) infections among blood donors at Al-Thawra Hospital Sana’a City Yemen. Yemeni J Med Sci. 2014;6:54–63.
14. Alzubiery T, Alharazi T, Alsumairy H, Amar J, Manal M, Majedi S. Prevalence of HBS Ag and anti-HBc among blood donors at the National Blood Transfusion and Research Center, Sana’a, Yemen. World J of Pharmaceutical Med Res. 2017;3(5):69–74.
15. Al-Shamahy H. Prevalence of hepatitis B surface antigen and risk factors of HBV infection in a sample of healthy mothers and their infants in Sana’a Yemen. Ann Saudi Med. 2016;20(5–6):464–467. doi:10.5144/0256-4947.2000.464
16. Al-Zubiery T, Alharazi T, Alsumairy H, Al-Zubiery A. Seroprevalence of HBs Ag, HCV and HIV among blood donors in three blood bank centers in Sana’a city: Yemen. J Biotechnol Biomed. 2017;1(1):1–26. doi:10.14302/issn.2576-6694.jbbs-17-1853
17. Alnwany NT. Prevalence of Hepatitis B virus infection and associated factors among blood donors in 48 Hospital Sana’a City- Yemen during 2016. J Med Pharm Allied Sci. 2020;4(1):111–126.
18. Mekuria SA, Legesse TG, Yalew AW. Prevalence of Hepatitis B and C viruses among blood donors at national blood bank Addis Ababa, Ethiopia. Int j Collab Res Intern Med Public Health. 2020;12(5):1037–1042.
19. Bommanahalli B, Javali R, Swamy CM, Gouda K, Siddartha K, Shashikala KP. Seroprevalence of Hepatitis B and Hepatitis C Viral infections among blood donors of central Karnataka, India. Int J Med Sci Public Health. 2014;3:1. doi:10.5455/ijmsph.2013.151220131
20. Al-Dafaee ME, Jasim AZ, Mohammed TK, Mohammed RQ, Abdullah HN, Harhoosh MA. Serological detection of viral Hepatitis B and C among the blood donors in Baghdad City. J Res Lepid. 2020;51(3):220–225. doi:10.36872/LEPI/V51I3/301181
21. Souan L, Siag M, Al-Salahat H, Al-Atrash T, Sughayer MA. Changing trends in seroprevalence rates of transfusion-transmitted diseases among blood donors in Jordan. BMC Infect Dis. 2021;21:508. doi:10.1186/s12879-021-06196-3
22. Ramli M, Zulkafli Z, Chambers GK, Amani RS, Zilan R, Edinur HA. The prevalence of transfusion-transmitted infections among blood donors in hospital universiti Sains Malaysia. Oman Med J. 2020;35(6):e189. doi:10.5001/omj.2020.86
23. Alzahrani FM, Muzaheed SSS, Alomar AI, Acharya S, Elhadi N, Elhadi N. Prevalence of Hepatitis B Virus (HBV) among blood donors in Eastern Saudi Arabia: results from a five-year retrospective study of HBV seromarkers. Ann Lab Med. 2019;39:81–85. doi:10.3343/alm.2019.39.1.81
24. Bazie EA, Alhasan Ali MM, Hamza HB, Magzoub OS, Salih MSM, Haroun BE. Sero-prevalence of viral transfusion-transmissible infections among blood donors at Kosti Teaching Hospital, White Nile State/Sudan. Int J Curr Microbiol App Sci. 2015;4(5):1132–1138.
25. Umolu PI, Okoror LE, Orhue P. Human immunodeficiency virus (HIV) seropositivity and hepatitis B surface antigenemia (HBSAG) among blood donors in Benin City, Edo state, Nigeria. Afr Health Sci. 2005;5:1.
26. Abebe M, Alemnew B, Biset S. Prevalence of Hepatitis B virus and HepatitisC virus among blood donors in nekemte blood bank, Western Oromia, Ethiopia: retrospective 5Years Study. J Blood Med. 2020;11:543–550. doi:10.2147/JBM.S282099
27. Nwobegahay JM, Njukeng PA, Kengne M, et al. Prevalence of Hepatitis B virus infection among blood donors at the Yaounde Military Hospital. Microbiol Res Int. 2016;4:6–10.
28. Police SMC, Bessanguem B, Mofini E, et al. High prevalence of Hepatitis B virus infection compared to human immunodeficiency virus among blood donors in Bangui. Open J Gastroenterol. 2020;10:137–143. doi:10.4236/ojgas.2020.106014
29. Boushab BM, Limame OCMM, Zahra FMF, Mamoudou S. Estimation of seroprevalence of HIV, hepatitis B and C virus and syphilis among blood donors in the hospital of Aïoun, Mauritania. Pan African Medl J. 2017;8:118.
30. Muselmani W, Habbal W, Monem F. Prevalence of “anti-HBc alone” among Syrian blood donors. J Infect Dev Ctries. 2014;8(8):1013–1015. doi:10.3855/jidc.3827
31. Lavanya V, Viswanathan T, Malar SAS, Malarvizhi A, Moorthy K. Prevalence of hepatitis B virus infection among blood donors with antibodies to hepatitis B core antigen. Int J Med Medical Sci. 2012;4(6):128–137.
32. Ebenezer BO, Toyin OO, Adebisi AY. Serological markers of Hepatitis B virus infectivity among Hepatitis B surface antigen negative blood donors at the University College Hospital, Ibadan. Niger Postgrad Med J. 2017;7(4):1–7.
33. Ikerionwu B. Prevalence of Hepatitis B surface antigen and Hepatitis B core antibody among prospective blood donors in Abuja, Nigeria. Arch Blood Transfus Disord. 2017;1(5):1–5.
34. Karimi G, Zadsar M, Vafaei N, Sharifi Z, Tafti MF. Prevalence of antibody to Hepatitis B core antigen and Hepatitis B virus DNA in HBsAg negative healthy blood donors. Virol J. 2016;13(36):1–6. doi:10.1186/s12985-016-0492-8
35. Abdullah SM. Prevalence of Hepatitis B and C in donated blood from the Jazan Region of Saudi Arabia. Malays J Med Sci. 2013;20(2):41–46.
36. Chen YT, Jiang JJ. Epidemic situation of hepatitis C virus. Strait J Prev Med. 2009;15:19–21. Chinese.
37. Shan H, Wang JX, Ren FR, et al. Blood banking in China. Lancet. 2002;360:1770–1775. doi:10.1016/S0140-6736(02)11669-2
38. Zhao SM, Jiang TL, Gao FX, et al. Analysis of true voluntary blood donors with anti-HCV prevalence and implications for donor management in Chongqing, China. Transfus Med. 2007;17:210–211. doi:10.1111/j.1365-3148.2007.00752.x
39. Guglielmo-Viret V, Attrée O, Blanco-Gros V, Thullier P. Comparison of electrochemiluminescence assay and ELISA for the detection of Clostridium botulinum type B neurotoxin. J Immunol Methods. 2005;301(1–2):164–172. doi:10.1016/j.jim.2005.04.003
40. Tognona F, Sevalie S, Gassimu J, et al. Seroprevalence of hepatitis B and hepatitis C among blood donors in Sierra Leone: a multi-year retrospective study. Int J Infect Dis. 2020;99:102–107. doi:10.1016/j.ijid.2020.07.030
41. Kabato AA, Weldearegay GM. Prevalence and associated risk factors of Hepatitis B and Hepatitis C virus among volunteer blood donors in Arba Minch blood bank SNNPR, Ethiopia. J Med Lab Diagn. 2016;7(4):20–27. doi:10.5897/JMLD2016.0122
42. Habte Y, Seyoum B, Alemayehu T. Hepatitis B virus infection and associated factors among blood donors at Dire Dawa, Eastern Ethiopia. J Antivir Antiretrovir. 2016;8(4):103–106. doi:10.4172/jaa.1000144
43. El Beltagy KE, Al Balawi IA, Almuneef M, Memish ZA. Prevalence of hepatitis B virus markers among blood donors in a tertiary hospital in Tabuk, Northwestern Saudi Arabia. Int J Infect Dis. 2008;12:495–499. doi:10.1016/j.ijid.2008.01.010
44. Eko Mba JM, Bisseye C, Ntsame Ndong JM, et al. Prevalent hepatitis B surface antigen among first-time blood donors in Gabon. PLoS One. 2003;13(4):e0194285. doi:10.1371/journal.pone.0194285
45. Paul CM, Moise KK, Blood BND, et al. Seroprevalence of Hepatitis B among blood donors in Mbuji-Mayi, “Case of Dipumba General Hospital” (DRC). Open Access Libr J. 2017;4:e3503. doi:10.4236/oalib.1103503
46. Al Hroob AM, Saghir SAM, Almaiman AA, et al. Prevalence and association of transfusion transmitted infections with ABO and Rh blood groups among blood donors at the national blood bank, Amman, Jordan. Medicina. 2020;56(701):1–11. doi:10.3390/medicina56120701
47. Mulakoli F, Gichure M. The prevalence of antibodies to Hepatitis B core antigen among blood donors in a tertiary institution in Nairobi County, Kenya. East Africa Science. 2020;2(1):36–44. doi:10.24248/EASci-D-19-00012
48. Keklik Z, Koruk I, Allahverdi S. Syrian Refugees at risk of Hepatitis diseases in Turkey. Saudi J Med. 2019;4(12):749–758. doi:10.36348/sjm.2019.v04i12.002
49. Ikerionwu B. Prevalence of Hepatitis B surface antigen and Hepatitis B core antibody among prospective blood donors in Abuja, Nigeria. Arch Blood Transfus Disord. 2017;1(5):1–5.
50. Al-Shamahy HA, Hanash SH, Rabbad IA, et al. Hepatitis B Vaccine coverage and the immune response in children under ten years old in Sana’a, Yemen. Sultan Qaboos Univ Med J. 2011;11(1):77–82.
51. World Health Organization, UNICEF 2020. Immunization regional snapshot 2020 Middle East and North Africa. WHO-UNICEF Estimates of National Immunization Coverage (WUENIC), revision 2020/the world population prospects – 2019 revision, UN population division, New York, USA. Available from: https://data.unicef.org/resources/regional-immunization-snapshots/.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Detection of Transfusion Transmissible Infections Among Voluntary Blood Donors at a Regional Blood Bank in Western Uganda: A Cross-Sectional Study
Asiimwe M, Nabawanuka B, Olebo DF, Kayiira M, Lubwama C, Turyamuhika L, Bahizi A, Rubaihayo J
Research and Reports in Tropical Medicine 2026, 17:539585
Published Date: 3 March 2026