")
Back to Journals » Drug, Healthcare and Patient Safety » Volume 12
Updated Evaluation of the Safety, Efficacy and Tolerability of Pirfenidone in the Treatment of Idiopathic Pulmonary Fibrosis
Authors Gulati S, Luckhardt TR
Received 23 July 2019
Accepted for publication 29 January 2020
Published 7 May 2020 Volume 2020:12 Pages 85—94
DOI https://doi.org/10.2147/DHPS.S224007
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Hemalkumar B Mehta
Swati Gulati,1 Tracy R Luckhardt1,2
1Division of Pulmonary, Allergy, and Critical Care Medicine, University of Alabama at Birmingham, Birmingham, AL, USA; 2Department of Medicine, University of Alabama at Birmingham, Birmingham, AL, USA
Correspondence: Swati Gulati
Division of Pulmonary, Allergy, and Critical Care Medicine, University of Alabama at Birmingham, 1900 University Blvd THT 541E, Birmingham, AL 35294-2180, USA
Tel +1 205 975 6376
Fax +1 205 934 1721
Email [email protected]
Abstract: Idiopathic Pulmonary Fibrosis (IPF) is a chronic fibrotic disease characterized by a progressive decline in lung function with a median survival of 3– 5 years after diagnosis. The course of disease is highly variable and unpredictable, often punctuated by episodes of acute respiratory failure, known as acute exacerbations. The incidence of IPF is on the rise due to the aging population, as age is the most important risk factor for this disease. Pirfenidone and nintedanib are the two anti-fibrotic drugs approved for IPF which have shown reduction in lung function decline. This review will discuss the efficacy, safety and tolerability profile of pirfenidone from clinical trials and the real-world clinical experience. Pirfenidone reduces the decline in lung function and improves progression-free survival in patients with IPF. It is generally well tolerated with the most common side effects being gastrointestinal and phototoxicity.
Keywords: Pirfenidone, idiopathic pulmonary fibrosis, efficacy, safety, tolerability
Introduction
Idiopathic Pulmonary Fibrosis (IPF) is a chronic fibrotic disease characterized by a progressive decline in lung function from irreversible destruction of lung architecture, subsequently culminating in respiratory failure.1 It usually occurs in individuals older than 50 years and its incidence remarkably increases with age.1,2 Median survival is 3–5 years following diagnosis, however, course of the disease is unpredictable and highly variable.3 Patients will sometimes experience a period of disease stability followed by sudden onset of acute respiratory failure, also known as an exacerbation. IPF exacerbations markedly shorten the median survival to 3–4 months and precede almost half of deaths in patients with IPF.4
Pirfenidone and nintedanib are the two anti-fibrotic drugs approved for treatment of IPF.5–7 Pirfenidone was the first licensed therapy for IPF and was approved by the European Medicines Agency (EMA) in 2011, followed by The US Food and Drug Administration (FDA) approval in 2014. Pirfenidone is an orally available drug known to mediate its anti–inflammatory and anti-fibrotic effects through modulation of cytokines and growth factors, although the precise mechanism of its action remains unclear.8,9 Treatment with pirfenidone has been shown to reduce the rate of decline in lung function, improve progression-free survival and also reduces all-cause mortality at 1 year.6,10,11
This review will discuss and summarize the efficacy, tolerability and safety profile of pirfenidone based on clinical trials and real-world clinical experience to date.
Efficacy of Pirfenidone in Patients with IPF
Clinical Trials
The first Phase II double-blind placebo-controlled trial evaluated the efficacy of Pirfenidone (1800mg/day) as compared to placebo in 109 patients.11 Pirfenidone group showed reduction in vital capacity decline as compared to the placebo group (−30 mL vs −130 mL, p=0.032). However, this trial was prematurely aborted in favor of Pirfenidone due to an increased number of IPF exacerbations in the placebo group (14% vs 0%, p=0.003).11 Following the encouraging results of this trial, the first Phase III, placebo-controlled, randomized clinical trial evaluated pirfenidone at high (1800mg/d) and low (1200mg/d) doses as compared to placebo in 275 patients with IPF. The trial showed that patients in the high-dose group had a reduction in vital capacity decline as compared to placebo (−90 mL vs −160 mL, p=0.04) and had an improved progression-free survival (p=0.03).12
Since then, pirfenidone has been evaluated in three multinational, randomized, and placebo-controlled trials, documenting its efficacy in preserving lung function and conferring a progression free survival benefit. Of these 3 trials, CAPACITY 004 and CPAPCITY 006 (Clinical Studies Assessing Pirfenidone in idiopathic pulmonary fibrosis: Research of Efficacy and Safety Outcomes) were two concurrent trials completed in 2010 leading to pirfenidone approval for use in IPF patients in Europe.5 ASCEND (Assessment of Pirfenidone to Confirm Efficacy and Safety in Idiopathic Pulmonary Fibrosis) study was the third trial specifically requested by US FDA, which was completed in 2014.6
CAPACITY trials assessed pirfenidone (2073mg/day) in a total of 770 patients with IPF with a forced vital capacity (FVC) of ⩾50% predicted and diffusing capacity for carbon monoxide (DLCO) of ⩾35% predicted. The primary end-point was change in FVC % predicted from baseline to week 72. Pirfenidone significantly reduced the decline in FVC % predicted from baseline over 72 weeks as compared to placebo in the CAPACITY 004 trial (−8% vs −12.4%, respectively, p=0.001). CAPACITY 006 also recorded a significant difference in FVC % predicted up to week 48 in pirfenidone group, although this difference was not maintained at week 72.5
Pre-specified pooled data analysis from both studies showed a significant treatment effect for pirfenidone, with mean change in FVC % predicted over time of −8.5% for pirfenidone vs −11.0% for placebo (p=0.005). Pirfenidone group also showed a positive treatment effect vs placebo for secondary end points of progression-free survival (defined as time to confirmed ≥10% decline in FVC % predicted, ≥15% decline in diffusing capacity of the lung carbon monoxide % predicted, or death), categorical decline in FVC ≥10% and the 6-min walk test (6MWT) distance. Although the CAPACITY study was not powered for mortality analysis, a pooled analysis did show a non-statistically significant trend towards lower all-cause mortality at week 72 in the pirfenidone group compared to the placebo group (4.4% vs 7.9%, respectively, p=0.315).5
Since the primary end point of predicted FVC % change from baseline to week 72 was not met in CAPACITY 006 trial, US FDA requested another clinical trial to demonstrate the efficacy of Pirfenidone.
ASCEND trial then assessed pirfenidone (2073mg/day) in 555 IPF patients with FVC of 50–90% predicted and DLCO of ⩾30% predicted. The pirfenidone group showed a significant reduction in primary-end point, which was the mean FVC decline at 52 weeks, as compared to placebo (253 mL vs 428 mL, p<0.001) and also reduced the relative risk of death or disease progression by 43% (confidence interval [CI], 0.43 to 0.77; p<0.001).6
In a pre-specified analysis of the pooled population of all three trials (CAPACITY 004, CAPACITY006 AND ASCEND), pirfenidone reduced the risk of death at 1 year by 48% compared to placebo (HR 0.52,95% CI 0.31−0.87; p<0.01) and also reduced the risk of treatment-emergent death due to IPF at 1 year by 68% (HR 0.32; 95% CI 0.14−0.76; p=0.006).6,10
Similarly, pooled data analysis from these trials by Noble et al showed that pirfenidone reduced the proportion of patients with ⩾10%decline in FVC% predicted or death by 44% (95% CI 29.3–55.4%) and increased the proportion of patients with no lung function decline by 59.3% (95% CI 29–96.8%).13
Longitudinal FVC data from these three trials have demonstrated that even in patients who had a 10% decline in FVC % during treatment, continued treatment with pirfenidone resulted in a lower risk of subsequent FVC decline or death as compared to placebo. (5.9% vs 27.9%, respectively, p=0.009).14
Long-Term Observational Studies
RECAP Study (an Open-Label Study of the Long-Term Safety of Pirfenidone in Patients with Idiopathic Pulmonary Fibrosis)
RECAP was an open-label roll-over study evaluating the long-term safety of pirfenidone 2043mg/day in patients who completed the CAPACITY and ASCEND trials.15 Of the 1058 patients who entered RECAP from both the trials, 40.4% completed the study at the time of analysis in 2015. Median duration of Pirfenidone was 88 weeks (ranging from >0 to 349 weeks) with a mean dose of 2091.1 mg/day. In patients who completed CAPACITY trials and entered RECAP, the mean change in FVC % predicted from RECAP baseline at 180 weeks was −9.6%. Median on-treatment survival from the first pirfenidone dose was 77.2 months.15 Efficacy data in terms of FVC decline was not recorded in patients from ASCEND trial.
In real-world clinical practice, sometimes there is hesitation in starting anti-fibrotics in patients with advanced disease. Costabel et al recently analyzed data from RECAP study to evaluate and compare the efficacy of pirfenidone in IPF patients across different categories of disease severity.16 Patients were categorized according to baseline lung function at the time of entry into the RECAP study: more advanced (FVC% predicted <50% and/or DLco <35%, n=189) and less advanced (FVC% predicted ≥50% and/or DLco ≥35%, n=409). Long-term treatment with pirfenidone resulted in a similar rate of FVC percent decline and safety profile in patients with more advanced and less advanced IPF. However, the discontinuation rate was higher for patients with more advanced disease.16 This study supports considering anti-fibrotics in patients who are diagnosed with IPF at an advanced stage.
Results from the Czech IPF Registry
Zurkova et al evaluated the overall 2- and 5-year survival and lung function decline in 601 patients from Czeck IPF registry who were diagnosed with IPF between 2012 and 2017.17 Of 601 patients, 63.7% of patients received pirfenidone treatment and the rest were not on any anti-fibrotic. The pirfenidone treated group had overall longer survival at 12, 24 and 60 months as compared to those treated with no antifibrotics. More than half of the patients (55.9%) were still alive at the end of 5 years in the pirfenidone group as compared to 31.5% in the no antifibrotic group (p=0.002). Patients in the pirfenidone group also showed a non- statistically significant trend towards the reduction in rate of FVC % decline at 6, 12 and 24 months as compared to the no antifibrotic group.17
Single Center Studies
Since its approval for use in IPF patients, various centers from different countries have published their real-world experience with Pirfenidone in terms of efficacy, safety and tolerability. The overall trend in efficacy has been consistent with the findings from the clinical trials and no significant new trends were noted. The findings from all these single-center trials to date are summarized in Table 1.
 |
Table 1 Efficacy, Side Effects and Tolerability of Pirfenidone |
Pirfenidone and Acute IPF Exacerbations
Acute exacerbation of IPF (AE-IPF) is defined as an unexplained worsening of dyspnea in the past 30 days in patients with previous or concurrent diagnosis of IPF, a high-resolution computed tomography with evidence of new bilateral ground-glass opacities or consolidation, and exclusion of alternative causes.1
AE-IPF has an annual incidence of up to 20% and is typically associated with a median survival of 3 months or less.4,18,19 Acute exacerbation of IPF accounts for over half of all hospital admissions and can account for nearly 40% of all deaths in IPF patients.20
No treatments have been shown to be effective in the treatment of acute exacerbations. Patients are usually managed with supplemental oxygen, antibiotics, high doses of corticosteroids.21 Mechanical ventilation is not recommended, however, a subset of patients have shown to benefit from non-invasive ventilation.22,23 The role of anti-fibrotics in management or prevention of IPF exacerbation remains largely unexplored.
Pirfenidone has been shown to lower the risk of respiratory-related hospitalization when compared to placebo over 1 year in a pooled analysis of all three phase −3 trials (7% vs 12%, p=0.001).24 While this study could be inferred in favor of pirfendone to reduce mortality associated with acute exacerbations, its role in acute exacerbation remains largely uninvestigated and unclear. In the pre-approval era, a small Phase 2 trial of 107 patients evaluating the efficacy of pirfenidone showed a numerically small but statistically significant reduction in acute exacerbation in patients receiving pirfenidone, but these results were not replicated in a larger 275-subject trial.11,12
One single center retrospective study of 47 patients with AE-IPF showed that patients who were on pirfenidone prior to the onset of exacerbation (n= 9) had improved 3-month survival as compared to patients who were not on pirfenidone (n= 18) (55% vs 34%, p=0.042).25 The treatment protocol in this study also used recombinant human thrombomodulin which has shown to be beneficial for AE-IPF and could be a confounding factor in the analysis.26 Although encouraging, but the results of this study need to be validated in larger cohorts.
Pirfenidone and Patient Reported Outcome Measures (PROMs)
Cough and dyspnea are the most incapacitating symptoms experienced by patients with IPF.27 An observational study of 43 IPF patients assessed the effect of pirfenidone on cough and cough-related quality of life (QoL) in patients with IPF. All patients underwent baseline 24-h cough recording with the Leicester Cough Monitor, which is a validated ambulatory cough monitoring system, prior to starting pirfenidone, and then after 4 and 12 weeks of treatment. After 12 weeks of treatment, 74% patients reported subjective improvement in cough and the objective 24-h cough decreased by 34% as measured by Leicester cough monitor. This was the first study showing clinically meaningful improvement in cough with pirfenidone.28
Dyspnea is now recognized as the most important factor for determining health-related quality of life in patients with IPF and is more likely to worsen in patients with more severe disease versus less severe disease. Post hoc analysis of all the three phase −3 trials has recently showed that treatment with pirfenidone slows the worsening of patient-reported breathlessness over 12 months vs placebo in patients with more advanced disease (FVC <80%) as measured by University of San Diego Shortness of Breath Questionnaire (UCSD-SOBQ).29 Further research is needed to examine the effects of pirfenidone on IPF-related symptoms and patient-related outcome measures.
Dosing and Tolerability of Pirfenidone
The recommended dose for Pirfenidone is 2403 mg/day in three divided doses to be taken with meals. Co-administration of food is thought to reduce gastrointestinal side effects by reducing the maximum plasma concentration of the drug.30 Pirfenidone has a well-characterized safety profile and is generally well tolerated. Most common side effects are gastrointestinal and photosensitivity, and most common laboratory abnormality is the elevation in transaminases. These side effects generally lead to temporary dose reductions or interruptions and in some cases, permanent discontinuation of the drug.31,32 However, many patients are unable to tolerate the full dose due to the above-listed side effects. The reduction in the rate of FVC decline is thought to be dose dependent and could be affected by dose reductions.5 There is limited data on the efficacy and tolerability of pirfenidone at lower doses.
Nathan et al recently conducted a post hoc analysis of ASCEND and CAPACITY 004/006 trials to evaluate the effect of pirfenidone dose reductions and interruptions on the annual rate of FVC decline.31 Patients in pirfenidone and placebo groups were stratified using a dose intensity threshold (DI) of >90% or <90%. DI was calculated as the actual total drug dose a patient received divided by the planned dose (2403mg/day for the entire study duration). There were no significant differences in the baseline characteristics of patients in DI >90% and DI< 90% groups in both, pirfenidone and placebo arms. Majority of the dose interruptions occurred in the first 6 months and more patients receiving pirfenidone had permanent dose reductions as compared to those receiving placebo (31.5% vs 20.8%, respectively).
The study showed that the annual rate of FVC decline and proportion of patients experiencing death at 12 months or >50 m decline in 6MWD were lower in pirfenidone group as compared to placebo group in both DI>90% and DI<90% groups. However, the relative difference of patients who experienced decline FVC or death who were randomized to receive placebo or pirfenidone was −33.1% in the ≤90% DI and −54.8% in the >90% DI, with a greater difference observed in the >90% DI.31
The results from this post hoc analysis demonstrated treatment benefit at different dosing intensities and hence, supports the approach of dose modification as a tool to reduce the rate of treatment discontinuation. However, the minimum dose of pirfenidone required through the modification period to maintain efficacy is still unknown. A recent report from Japan suggests that pirfenidone dose adjustment by body surface area in patients with IPF could be adequate to prevent adverse effects while achieving efficacy and treatment effect.33
Age is an important factor in determining the tolerability of pirfenidone. Recent study from Japan has shown that amongst a group of 120 IPF patients, the rate of drug discontinuation at 1 year was 29% higher in elderly patients (>75 years) when compared with the younger age group (<75 years).34 In regards to the adverse events, gastrointestinal side effects and discontinuation of drug due to gastrointestinal disorders were significantly higher in elderly patients as compared to younger patients (77% vs 45%, p 0.007; 35% vs 15%, p=0.019, respectively).34
Safety Profile of Pirfenidone
Treatment Emergent Side Effects in Phase III Trials
The most commonly reported adverse effects in the CAPACITY and ASCEND trials were gastrointestinal and skin related. Gastrointestinal events reported in the pirfenidone (n=623) and placebo (n=624) groups, respectively, were diarrhea (18.8% vs 14.4%), nausea (32.4% vs 12.2%), and dyspepsia (16.1% vs 5%). Skin events reported in the pirfenidone and placebo groups, respectively, were photosensitivity (9.3% vs 1.1%) and rash (26.2% vs 7.7%). Both, gastrointestinal and dermatologic adverse events, were generally mild to moderate and reversible. Only 9 (1.7%) patients discontinued pirfenidone treatment due to gastrointestinal adverse events and 12 (1.9%) due to skin-related adverse events.5,6,15,35
Table 2 shows the most common side effects experienced by patients in Phase 3 trials. Most common laboratory abnormality was elevated transaminases in the pirfenidone group (14.4%), which normalized after discontinuation of the drug.
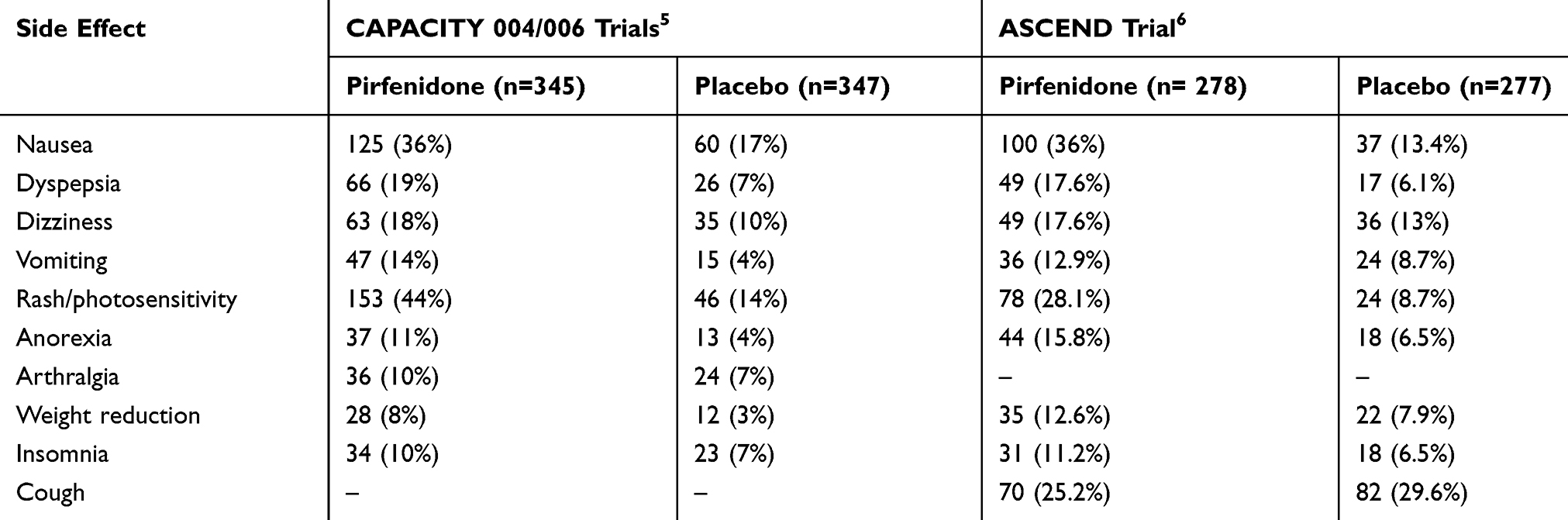 |
Table 2 Adverse Drug Reactions in Phase III Trials |
RECAP
RECAP was an open-label extension study to evaluate drug safety in patients who completed CAPACITY and ASCEND trials. It followed 1058 patients for 7 years, of which 40.4% completed the study. Adverse drug reactions were reported by 786 patients (74.3%). The most frequent adverse drug reactions were nausea (21.6%), diarrhea (12.3%), and rash (11.6%). Discontinuation of treatment due to an adverse drug reaction occurred in 120 patients (11.3%) and the most common reaction leading to discontinuation was rash and nausea.15
In contrast to the ASCEND and CAPACITY trials, the frequency and adjusted rate of adverse drug reactions were, in fact, lower in RECAP study (74.3% vs 89.2%), which in part can be attributed to positive selection bias.15
PASSPORT – Pirfenidone Post-Authorization Safety Registry
PASSPORT was a multicenter, post-authorization, and prospective study of IPF patients (n=1009) who were newly prescribed pirfenidone and followed for 2 years thereafter. The aim of the study to evaluate long-term safety of pirfenidone. Median pirfenidone exposure was 442.0 days. Overall, 73.4% patients experienced adverse drug reaction, most commonly gastrointestinal symptoms (38.3%), photosensitivity/rash (29%), nausea (20.6%) and fatigue (18.5%). These adverse events led to treatment discontinuation in 28.7% of patients. Older age, use of steroids prior to the study and female sex were associated with early treatment discontinuation. These adverse drug reactions also led to dose adjustment in 48.3% of patients. More patients completed treatment following a dose adjustment than those who had no dose adjustment (38.8 vs 26.1%, respectively).
Overall, the study showed similar side effect profile of pirfenidone in the post-marketing era as in the clinical trials. It also showed that dose adjustment had a favorable effect on treatment persistence.32
Real-World Experience
There is emerging data from various single and multi-centers on the safety and tolerability profile of pirfenidone in IPF patients. So far, the safety profile of pirfenidone is consistent across all groups of IPF patients. These findings are summarized in Table 1.
Prevention and Management of Pirfenidone Related Side Effects
Dose titration and modification protocols have been shown to be effective in reducing discontinuation rates due to gastrointestinal discomfort.31 A 2-week dose titration schedule has been recommended by the manufacturing company.36 In LOTUSS trial, a longer 4-week titration schedule was compared with the standard 2-week titration schedule in patients with scleroderma ILD to test the safety and tolerability of pirfenidone. The longer 4-week titration schedule was shown to have less dose modifications and dose interruptions as compared to standard 2-week titration (21.9 vs 3.2, p=0.053; 12.5% vs 0%, p=0.113, respectively).37 The two titration schedules are listed in Table 4. Strategies to manage common extra-gastrointestinal side effects are listed in Table 3
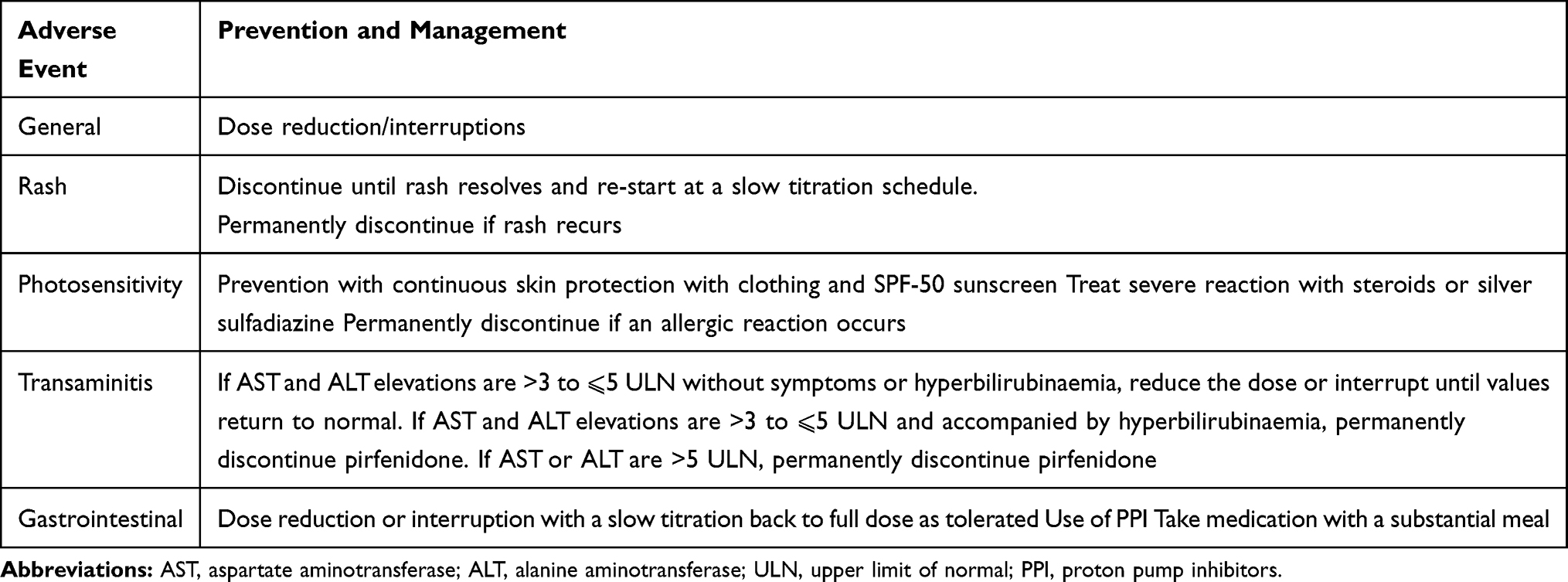 |
Table 3 Prevention and Management of Pirfenidone Related Side Effects |
 |
Table 4 Pirfenidone Dose Titration Protocol |
Pirfenidone and Nintedanib
Nintedanib is the other anti-fibrotic drug approved for treatment for IPF.7 It is an intracellular inhibitor and targets multiple tyrosine kinases, such as the VEGF, FGF, and PDGF receptors.38 Nintedanib was shown to reduce decline in FVC in IPF patients as compared to the placebo group in both, INPULSIS I (−114.7 mL vs −239.9 mL, p <0.001) and INPULSIS II (−113.6 mL VS −207.3 mL, p<0.001) over 52 weeks.7 The most common side effect of nintedanib was diarrhea with incidence as high as 63%; however, the rate of permanent discontinuation due to diarrhea is reported to be less than 10% in clinical trials and real-world data.39 In both the INPULSIS trials, the proportion of patients with serious adverse events was similar in the nintedanib and placebo groups. However, nintedanib group had higher rates of myocardial infarction as compared to the placebo group in both INPULSIS I (1.6% vs 0.5%) and II trials (1.5% vs 0.5%). A recent post hoc analyses of TOMORROW and INPULISIS clinical trials showed that the incidence of myocardial infarction was higher in the nintedanib group than the placebo group among patients with higher cardiovascular risk, whereas the incidence rate of other ischemic heart disease was lower in the nintedanib group than the placebo group.40 The clinical significance of this finding remains unknown.
There are no trials directly comparing pirfenidone and nintedanib in IPF patients. Both the drugs have been shown to be effective in reducing the lung function decline in IPF patients when compared to placebo. Observation studies have shown comparable tolerability and efficacy of these agents and now new safety signals have been identified.39,41,42
Conclusion
Pirfenidone slows disease progression in IPF and likely improves survival, decreases the rate of respiratory-related hospitalizations and improves PROMs. It is generally well tolerated and has few known interactions with commonly prescribed drugs. Gastrointestinal and photosensitivity are the most frequently experienced side effects and are usually managed by dose reductions, which in turn can decrease the effectiveness of the drug. In real-world experience, most sites have reported treatment discontinuation rates to be around 10–20%. Discontinuation rates can be higher in elderly patients and dose modification is now recognized as an important tool to maintain medication compliance and minimize side effects.
In conclusion, pirfenidone is an anti-fibrotic drug that is a viable, well-tolerated, real-world option for the treatment of patients with IPF.
Disclosure
Tracy R Luckhardt reports personal fees from Boehringer Ingelheim and France Foundation, outside the submitted work. The authors report no other conflicts of interest in this work.
References
1. Raghu G, Remy-Jardin M, Myers JL, et al. Diagnosis of idiopathic pulmonary fibrosis. An official ATS/ERS/JRS/ALAT clinical practice guideline. Am J Respir Crit Care Med. 2018;198(5):e44–e68. doi:10.1164/rccm.201807-1255ST
2. Raghu G, Chen S-Y, Yeh W-S, et al. Idiopathic pulmonary fibrosis in US medicare beneficiaries aged 65 years and older: incidence, prevalence, and survival, 2001-11. Lancet Respir Med. 2014;2(7):566–572. doi:10.1016/S2213-2600(14)70101-8
3. Ley B, Collard HR, King TE. Clinical course and prediction of survival in idiopathic pulmonary fibrosis. Am J Respir Crit Care Med. 2011;183(4):431–440. doi:10.1164/rccm.201006-0894CI
4. Collard HR, Ryerson CJ, Corte TJ, et al. Acute exacerbation of idiopathic pulmonary fibrosis. An international working group report. Am J Respir Crit Care Med. 2016;194(3):265–275. doi:10.1164/rccm.201604-0801CI
5. Noble PW, Albera C, Bradford WZ, et al. Pirfenidone in patients with idiopathic pulmonary fibrosis (CAPACITY): two randomised trials. Lancet Lond Engl. 2011;377(9779):1760–1769. doi:10.1016/S0140-6736(11)60405-4
6. King TE, Bradford WZ, Castro-Bernardini S, et al. A phase 3 trial of pirfenidone in patients with idiopathic pulmonary fibrosis. N Engl J Med. 2014;370(22):2083–2092. doi:10.1056/NEJMoa1402582
7. Richeldi L, Du Bois RM, Raghu G, et al. Efficacy and safety of nintedanib in idiopathic pulmonary fibrosis. N Engl J Med. 2014;370(22):2071–2082. doi:10.1056/NEJMoa1402584
8. Conte E, Gili E, Fagone E, Fruciano M, Iemmolo M, Vancheri C. Effect of pirfenidone on proliferation, TGF-β-induced myofibroblast differentiation and fibrogenic activity of primary human lung fibroblasts. Eur J Pharm Sci off J Eur Fed Pharm Sci. 2014;58:13–19. doi:10.1016/j.ejps.2014.02.014
9. Oku H, Shimizu T, Kawabata T, et al. Antifibrotic action of pirfenidone and prednisolone: different effects on pulmonary cytokines and growth factors in bleomycin-induced murine pulmonary fibrosis. Eur J Pharmacol. 2008;590(1–3):400–408. doi:10.1016/j.ejphar.2008.06.046
10. Nathan SD, Albera C, Bradford WZ, et al. Effect of pirfenidone on mortality: pooled analyses and meta-analyses of clinical trials in idiopathic pulmonary fibrosis. Lancet Respir Med. 2017;5(1):33–41. doi:10.1016/S2213-2600(16)30326-5
11. Azuma A, Nukiwa T, Tsuboi E, et al. Double-blind, placebo-controlled trial of pirfenidone in patients with idiopathic pulmonary fibrosis. Am J Respir Crit Care Med. 2005;171(9):1040–1047. doi:10.1164/rccm.200404-571OC
12. Taniguchi H, Ebina M, Kondoh Y, et al. Pirfenidone in idiopathic pulmonary fibrosis. Eur Respir J. 2010;35(4):821–829. doi:10.1183/09031936.00005209
13. Noble PW, Albera C, Bradford WZ, et al. Pirfenidone for idiopathic pulmonary fibrosis: analysis of pooled data from three multinational phase 3 trials. Eur Respir J. 2016;47(1):243–253. doi:10.1183/13993003.00026-2015
14. Nathan SD, Albera C, Bradford WZ, et al. Effect of continued treatment with pirfenidone following clinically meaningful declines in forced vital capacity: analysis of data from three phase 3 trials in patients with idiopathic pulmonary fibrosis. Thorax. 2016;71(5):429–435. doi:10.1136/thoraxjnl-2015-207011
15. Costabel U, Albera C, Lancaster LH, et al. An open-label study of the long-term safety of pirfenidone in patients with idiopathic pulmonary fibrosis (RECAP). Respir Int Rev Thorac Dis. 2017;94(5):408–415. doi:10.1159/000479976
16. Costabel U, Albera C, Glassberg MK, et al. Effect of pirfenidone in patients with more advanced idiopathic pulmonary fibrosis. Respir Res. 2019;20(1):55. doi:10.1186/s12931-019-1021-2
17. Zurkova M, Kriegova E, Kolek V, et al. Effect of pirfenidone on lung function decline and survival: 5-yr experience from a real-life IPF cohort from the Czech EMPIRE registry. Respir Res. 2019;20(1):16. doi:10.1186/s12931-019-0977-2
18. Agarwal R, Jindal SK. Acute exacerbation of idiopathic pulmonary fibrosis: a systematic review. Eur J Intern Med. 2008;19(4):227–235. doi:10.1016/j.ejim.2007.04.024
19. Bafadhel M, McKenna S, Terry S, et al. Acute exacerbations of chronic obstructive pulmonary disease: identification of biologic clusters and their biomarkers. Am J Respir Crit Care Med. 2011;184(6):662–671. doi:10.1164/rccm.201104-0597OC
20. Natsuizaka M, Chiba H, Kuronuma K, et al. Epidemiologic survey of Japanese patients with idiopathic pulmonary fibrosis and investigation of ethnic differences. Am J Respir Crit Care Med. 2014;190(7):773–779. doi:10.1164/rccm.201403-0566OC
21. Raghu G, Collard HR, Egan JJ, et al. An official ATS/ERS/JRS/ALAT statement: idiopathic pulmonary fibrosis: evidence-based guidelines for diagnosis and management. Am J Respir Crit Care Med. 2011;183(6):788–824. doi:10.1164/rccm.2009-040GL
22. Gaudry S, Vincent F, Rabbat A, et al. Invasive mechanical ventilation in patients with fibrosing interstitial pneumonia. J Thorac Cardiovasc Surg. 2014;147(1):47–53. doi:10.1016/j.jtcvs.2013.06.039
23. Vianello A, Arcaro G, Battistella L, et al. Noninvasive ventilation in the event of acute respiratory failure in patients with idiopathic pulmonary fibrosis. J Crit Care. 2014;29(4):562–567. doi:10.1016/j.jcrc.2014.03.019
24. Ley B, Swigris J, Day B, et al. Pirfenidone reduces respiratory-related hospitalizations in idiopathic pulmonary fibrosis. Am J Respir Crit Care Med. 2017;196(6):756–761. doi:10.1164/rccm.201701-0091OC
25. Furuya K, Sakamoto S, Shimizu H, et al. Pirfenidone for acute exacerbation of idiopathic pulmonary fibrosis: a retrospective study. Respir Med. 2017;126:93–99. doi:10.1016/j.rmed.2017.03.026
26. Kataoka K, Taniguchi H, Kondoh Y, et al. Recombinant human thrombomodulin in acute exacerbation of idiopathic pulmonary fibrosis. Chest. 2015;148(2):436–443. doi:10.1378/chest.14-2746
27. van Manen MJG, Birring SS, Vancheri C, et al. Cough in idiopathic pulmonary fibrosis. Eur Respir Rev off J Eur Respir Soc. 2016;25(141):278–286. doi:10.1183/16000617.0090-2015
28. van Manen MJG, Birring SS, Vancheri C, et al. Effect of pirfenidone on cough in patients with idiopathic pulmonary fibrosis. Eur Respir J. 2017;50:4. doi:10.1183/13993003.01157-2017
29. Glassberg MK, Wijsenbeek MS, Gilberg F, Petzinger U, Kirchgaessler K-U, Albera C. Effect of pirfenidone on breathlessness in patients with idiopathic pulmonary fibrosis. Eur Respir J. 2019;54:1900399. doi:10.1183/13993003.00399-2019
30. Rubino CM, Bhavnani SM, Ambrose PG, Forrest A, Loutit JS. Effect of food and antacids on the pharmacokinetics of pirfenidone in older healthy adults. Pulm Pharmacol Ther. 2009;22(4):279–285. doi:10.1016/j.pupt.2009.03.003
31. Nathan SD, Lancaster LH, Albera C, et al. Dose modification and dose intensity during treatment with pirfenidone: analysis of pooled data from three multinational phase III trials. BMJ Open Respir Res. 2018;5(1):e000323. doi:10.1136/bmjresp-2018-000323
32. Cottin V, Koschel D, Günther A, et al. Long-term safety of pirfenidone: results of the prospective, observational PASSPORT study. ERJ Open Res. 2018;4:4. doi:10.1183/23120541.00084-2018
33. Uehara M, Enomoto N, Karayama M, et al. Evaluation of pirfenidone dose adjusted by body weight or body surface area in the treatment for Japanese patients with interstitial pneumonia. In:
34. Sakayori M, Terada J, Abe M, et al. Differences in tolerability of pirfenidone between elderly and younger patients with idiopathic pulmonary fibrosis. Drug Des Devel Ther. 2019;13:2295–2303. doi:10.2147/DDDT.S208733
35. Side effects and safety data | esbriet® (pirfenidone) HCP. Available from: https://www.esbriethcp.com/safety-tolerability-dosing/safety-tolerability.html.
36. Lederer DJ, Martinez FJ, Longo DL. Idiopathic pulmonary fibrosis. N Engl J Med. 2018;378(19):1811–1823. doi:10.1056/NEJMra1705751
37. Khanna D, Albera C, Fischer A, et al. An open-label, phase II study of the safety and tolerability of pirfenidone in patients with scleroderma-associated interstitial lung disease: the LOTUSS trial. J Rheumatol. 2016;43(9):1672–1679. doi:10.3899/jrheum.151322
38. Chaudhary NI, Roth GJ, Hilberg F, et al. Inhibition of PDGF, VEGF and FGF signalling attenuates fibrosis. Eur Respir J. 2007;29(5):976–985. doi:10.1183/09031936.00152106
39. Noth I, Oelberg D, Kaul M, Conoscenti CS, Raghu G. Safety and tolerability of nintedanib in patients with idiopathic pulmonary fibrosis in the USA. Eur Respir J. 2018;52:1. doi:10.1183/13993003.02106-2017
40. Noth I, Wijsenbeek M, Kolb M, et al. Cardiovascular safety of nintedanib in subgroups by cardiovascular risk at baseline in the TOMORROW and INPULSIS trials. Eur Respir J. 2019;54:3. doi:10.1183/13993003.01797-2018
41. Barratt SL, Mulholland S, Al Jbour K, et al. South-West of England’s experience of the safety and tolerability pirfenidone and nintedanib for the treatment of Idiopathic Pulmonary Fibrosis (IPF). Front Pharmacol. 2018;9:1480. doi:10.3389/fphar.2018.01480
42. Okuda R, Hagiwara E, Baba T, Kitamura H, Kato T, Ogura T. Safety and efficacy of pirfenidone in idiopathic pulmonary fibrosis in clinical practice. Respir Med. 2013;107(9):1431–1437. doi:10.1016/j.rmed.2013.06.011
43. Wijsenbeek MS, Van Beek FT, Geel AL, et al. Pirfenidone in daily clinical use in patients with idiopathic pulmonary fibrosis in the Netherlands. In:
44. Ravaglia C, Gurioli C, Romagnoli M, et al. Pirfenidone treatment in idiopathic pulmonary fibrosis: an Italian case series. Eur Respir J. 2013;42(Suppl 57):P3370.
45. Bonella F, Wessendorf TE, Costabel U. Clinical experience with pirfenidone for the treatment of idiopathic pulmonary fibrosis. Dtsch Med Wochenschr. 2013;138(11):518–523. doi:10.1055/s-0032-1332930
46. Arai T, Inoue Y, Sasaki Y, et al. Predictors of the clinical effects of pirfenidone on idiopathic pulmonary fibrosis. Respir Investig. 2014;52(2):136–143. doi:10.1016/j.resinv.2013.09.002
47. Oltmanns U, Kahn N, Palmowski K, et al. Pirfenidone in idiopathic pulmonary fibrosis: real-life experience from a German tertiary referral center for interstitial lung diseases. Respir Int Rev Thorac Dis. 2014;88(3):199–207. doi:10.1159/000363064
48. Chaudhuri N, Duck A, Frank R, Holme J, Leonard C. Real world experiences: pirfenidone is well tolerated in patients with idiopathic pulmonary fibrosis. Respir Med. 2014;108(1):224–226. doi:10.1016/j.rmed.2013.11.005
49. Hanta I, Cilli A, Sevinc C. The effectiveness, safety, and tolerability of pirfenidone in idiopathic pulmonary fibrosis: a retrospective study. Adv Ther. 2019;36(5):1126–1131. doi:10.1007/s12325-019-00928-3
50. Yoon H-Y, Kim DS, Song JW. Efficacy and safety of pirfenidone in advanced idiopathic pulmonary fibrosis. Respir Int Rev Thorac Dis. 2019;97(3):242–251. doi:10.1159/000492937
51. Tzouvelekis A, Ntolios P, Karampitsakos T, et al. Safety and efficacy of pirfenidone in severe idiopathic pulmonary fibrosis: a real-world observational study. Pulm Pharmacol Ther. 2017;46:48–53. doi:10.1016/j.pupt.2017.08.011
52. Margaritopoulos GA, Trachalaki A, Wells AU, et al. Pirfenidone improves survival in IPF: results from a real-life study. BMC Pulm Med. 2018;18(1):177. doi:10.1186/s12890-018-0736-z
53. Salih GN, Shaker SB, Madsen HD, Bendstrup E. Pirfenidone treatment in idiopathic pulmonary fibrosis: nationwide Danish results. Eur Clin Respir J. 2016;3:32608. doi:10.3402/ecrj.v3.32608
54. Esbriet® (pirfenidone) information for healthcare professionals. Available from: https://www.esbriethcp.com/index.html?c=esb-1631d3792bb&gclid=Cj0KCQiAgebwBRDnARIsAE3eZjT6zHuuSFTLEn1qp7upWzTKgjKDQbbrrOH5Fs0oOdnV8vnQisd4J3YaAqsjEALw_wcB&gclsrc=aw.ds.
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.