Back to Journals » Clinical Ophthalmology » Volume 20
Update on Therapy for Non-Infectious Scleritis
Authors Richey A, Sattarova V, Kopplin LJ, Armbrust KR ![]()
Received 1 December 2025
Accepted for publication 15 March 2026
Published 30 March 2026 Volume 2026:20 563490
DOI https://doi.org/10.2147/OPTH.S563490
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Sotiria Palioura
Allison Richey,1 Victoria Sattarova,2 Laura J Kopplin,3 Karen R Armbrust1
1Department of Ophthalmology and Visual Neurosciences, University of Minnesota, Minneapolis, MN, USA; 2Department of Ophthalmology, Hennepin County Medical Center, Minneapolis, MN, USA; 3Department of Ophthalmology and Visual Sciences, University of Wisconsin-Madison, Madison, WI, USA
Correspondence: Karen R Armbrust, Department of Ophthalmology and Visual Neurosciences, University of Minnesota, 420 Delaware Street SE, MMC 493, Minneapolis, MN, 55455, USA, Fax +1 612 626 7882, Email [email protected]
Abstract: Non-infectious scleritis is a potentially vision threatening inflammatory disease which often requires long-term treatment. The general approach to management consists of a thorough systemic workup and subsequent selection of the most appropriate therapeutic agent(s) for inflammatory control. This article reviews current and emerging therapies for scleritis treatment, including topical agents, systemic non-steroidal anti-inflammatory drugs and corticosteroids, conventional immunomodulatory therapies, and biologics.
Keywords: glucocorticoids, immunosuppressive agents, non-steroidal anti-inflammatory agents, therapeutics
Introduction
Scleritis is a typically painful and potentially vision threatening disease characterized by inflammation of the scleral tissue. Inflammation in scleritis also may involve neighboring ocular structures, including the cornea, episclera, and underlying uveal tract. Scleritis has been shown to have a higher incidence in females than males, with multiple studies reporting female predominance rates ranging between 62 to 67%.1–4 Although regional differences in scleritis incidence and etiology are well-documented, scleritis remains a rare disease. A systematic review and meta-analysis consisting of 74 studies with greater than 16,000 patients reported the annual incidence of scleritis to be 2.67 per 100,000 individuals in ophthalmological centers and 1.38 per 100,000 individuals in broader population based studies.1 An evaluation of scleritis in the United States TriNetX database showed an incidence of 6.8 per 100,000 person-years and the 10-year prevalence was 35.4 cases per 100,000 persons, with annual prevalence increasing from 2014 to 2023.2 Conversely, a large retrospective cross-sectional and population cohort study in the United Kingdom from 1997–2018 showed that the incidence of scleritis declined from 4.23 to 2.79 per 100,000 person-years between 1997 and 2018, and the prevalence in 2018 was 93.62 per 100,000 person-years.3
Scleritis is often associated with systemic disease, both infectious and non-infectious. In the United States, scleritis is more often non-infectious, with infectious etiologies accounting for fewer than 20% of uveitis/scleritis cases in a United States medical claims database.5 However, the more common pathogenic organisms and the incidence rates of infectious scleritis versus non-infectious scleritis vary greatly by location, so it is beneficial to understand the local incidence patterns. For example, a meta-analysis found that prevalence of infectious scleritis attributed to tuberculosis ranged from 0.7% in the United Kingdom to 16.6% in Portugal and prevalence of herpetic scleritis ranged from 1.8% in Columbia to 12% in Taiwan.1 Although overlapping features in clinical presentation may make distinguishing infectious scleritis from non-infectious scleritis difficult, clinical features such as the presence of purulent exudates, scleral ulcers, scleral abscesses, scleritis associated with hypopyon, and necrotizing scleritis may increase clinical suspicion for an infectious etiology.6 Infectious scleritis treatment varies depending on the causative organism and will not be discussed further in the present review except as a reminder to rule out infection during clinical evaluation of scleritis.
Scleritis can be categorized based on clinical features and anatomic location. A general approach to anatomic classification was described by Watson and Hayreh and uses the equator of the globe to define anterior and posterior scleritis.7 Anterior scleritis is more common and refers to scleritis that occurs anterior to the equator of the globe. Watson and Hayreh further subdivided anterior scleritis into diffuse, nodular, and necrotizing subtypes, with necrotizing scleritis further subdivided into categories of “with inflammation” or “without inflammation (scleromalacia perforans)”.7 The diffuse subtype may involve the entire anterior sclera or just a portion, and may be accompanied by conjunctival edema (Figures 1A and B). The nodular subtype often presents with a distinct nodule or nodules, with the nodule(s) being deep red in color and frequently tender to palpation.7 The necrotizing subtype is considered the most destructive form, and typically presents with severe pain and progressive necrosis of the sclera (Figure 1C).8 This is in contrast to scleromalacia perforans, which is typically painless (Figure 1D).7 Scleromalacia perforans is a type III hypersensitivity reaction that often occurs in association with systemic inflammatory diseases and leads to scleral necrosis. Sclerokeratitis refers to scleritis with corneal inflammation, often near the corneal limbus, in addition to scleral inflammation.2 Posterior scleritis refers to scleritis that occurs posterior to the equator and often presents with severe eye pain, especially with eye movement or palpation, and vision loss. Clinical features of posterior scleritis include optic disc edema (Figure 2A), choroidal folds (Figure 2B), scleral wall thickening (Figure 2C), and a T-sign on ocular ultrasound (Figure 2D). Additionally, optical coherence tomography (OCT) may be useful in diagnosing and managing scleritis. A recent study by Shoughy et al evaluated the use of anterior segment OCT in the diagnosis of scleritis, showing a mean scleral thickness significantly thicker than normal eyes and eyes with episcleritis, with hyporeflective areas reflecting intrascleral edema, which was not present in non-scleritis eyes.9 Spectral domain OCT may also be useful in detecting associated macular pathology in patients with scleritis, including cystoid macular edema, diffuse macular edema, epiretinal membrane, or serous retinal detachment.10 In conjunction with clinical examination, OCT may provide objective data for scleritis diagnosis and management of ocular inflammation.
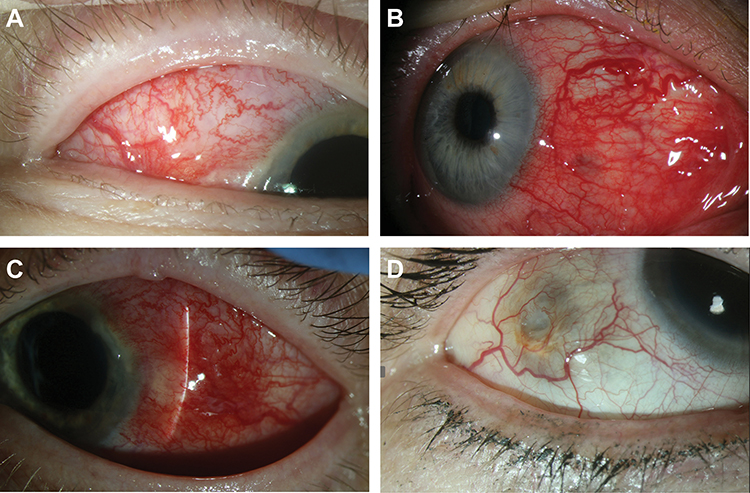 |
Figure 1 Clinical features of non-infectious anterior scleritis. (A) Diffuse anterior scleritis with moderate scleral injection, (B) Diffuse anterior scleritis with severe scleral injection, (C) Diffuse anterior scleritis, necrotizing subtype, with a white avascular area of necrosis between limbus and slit beam, (D) Scleromalacia perforans, with a rapidly enlarging area of dark scleral discoloration resulting from progressive scleral thinning despite minimal scleral injection. |
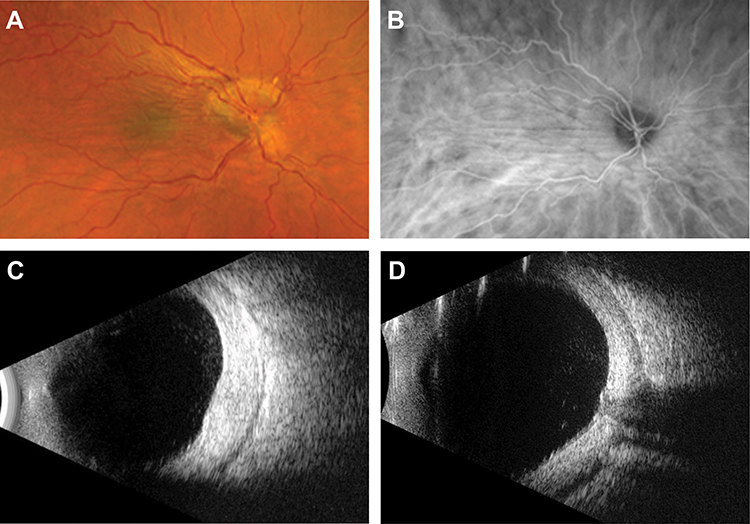 |
Figure 2 Clinical features of non-infectious posterior scleritis. (A) Posterior scleritis with optic disc edema and choroidal folds, (B) Indocyanine green angiography of the same eye showing choroidal folds and choroidal flow voids, (C) B-scan ultrasonography showing marked scleral wall thickening in posterior scleritis, (D) B-scan ultrasonography showing T sign in posterior scleritis. |
Certain scleritis subtypes and associated ocular features are more frequently associated with vision loss and may warrant more aggressive therapy. Marked scleral thinning in the necrotizing anterior scleritis subtype can cause decreased vision and/or lead to globe perforation. It is important to consider these serious risks in treatment of scleromalacia perforans, despite its often painless presentation.2,7 In addition to scleral thinning, keratitis is an ocular feature that may alert the clinician to an increased risk of vision loss in the setting of anterior scleritis. Compared to anterior scleritis, vision-threatening ocular complications are more likely to occur in posterior scleritis, with statistically higher rates of retinal detachment, orbital inflammation, macular edema, glaucoma, choroidal involvement, and uveal effusion.4,11
Clinical Evaluation of Scleritis
A thorough clinical evaluation is indicated in patients presenting with scleritis (Figure 3). A review of the patient’s medical history may reveal a previously diagnosed autoimmune condition associated with scleritis. Scleritis is most frequently associated with rheumatoid arthritis (RA), although the rate varies geographically.12,13 In studies from Taiwan, the United Kingdom, the United States, Columbia, and Bangladesh, the prevalence of RA among scleritis patients was 2.9%, 5.0%, 6.8%, 19.2%, and 10%, respectively.1 Patients with RA are more likely to present with the diffuse or necrotizing forms of anterior scleritis than patients with idiopathic scleritis.13 Scleritis in RA patients is associated with a longer and more recurrent disease course, and RA patients with scleritis were found to have a higher risk of mortality than those without ocular involvement.1 Another important systemic disease association is anti-neutrophil cytoplasmic antibody (ANCA)-associated vasculitis. A study by Hoang et al found positive ANCA testing in 18% of patients with scleritis. Patients with positive ANCA testing had more severe ocular disease with complications and undiagnosed primary vasculitis, requiring more aggressive therapy.14 ANCA-associated scleritis is more likely to present with scleromalacia perforans than idiopathic scleritis.15 Case reports of scleritis associated with systemic lupus erythematosus (SLE) have been reported in the literature, with two cases who had posterior scleritis as the presenting sign of the underlying condition.16 Additionally, a retrospective study of 98 patients with SLE found ocular involvement in 29 patients, with 3.1% diagnosed with scleritis.17 Another study found an incidence rate of episcleritis/scleritis of 2.51 per 1,000 person-years, compared to 0.38 in the non-SLE comparison cohort.18 Occasionally, scleritis can be associated with HLA-B27, with one study showing 5.7% of scleritis cases associated with HLA-B27 related disease.19 There have also been case reports of scleritis associated with sarcoidosis,20 which have been substantiated by large scale cohort studies.4,19
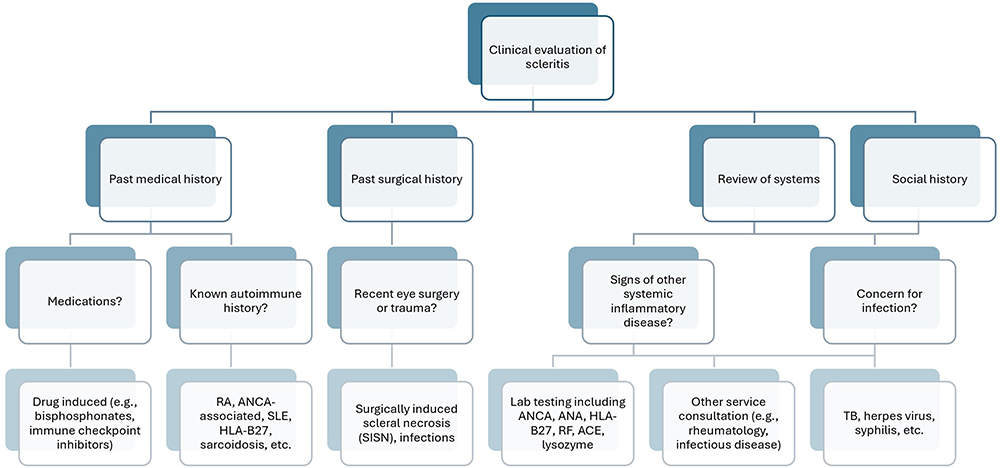 |
Figure 3 Clinical evaluation of scleritis. |
In addition to assessment of previously diagnosed systemic conditions, the patient’s medical history should include a comprehensive review of medications, including those used to treat conditions unrelated to the eye. Drug-induced scleritis is an uncommon but important etiology to identify, as scleritis treatment in these cases may include modification of systemic medications. A retrospective cohort study evaluating patients in British Columbia who were first-time users of oral bisphosphonates showed they were at a higher risk of scleritis compared with non-users.21 Additionally, immune checkpoint inhibitors have been identified as associated with scleritis as well as uveitis.22
Reviewing the patient’s surgical history may raise clinical suspicion for infection or surgically induced necrotizing scleritis (SINS). The pathogenesis of SINS is poorly understood, but ocular trauma-inducing lytic action of collagenases and subsequent collagen degradation, vascular disruption, and immune complex deposition activating the complement cascade are thought to play a role in scleral necrosis.23 The most common procedures associated with scleral necrosis include pterygium excision and cataract surgery. A study of the clinical features, treatment, and visual outcome of 52 eyes which developed scleritis following surgical intervention found that scleritis developed adjacent to the surgical wound in all eyes, with the vast majority developing necrotizing scleritis, and 63% of patients had an associated systemic inflammatory disease.24 To further evaluate this systemic disease association with SINS, Ruiz-Lozano et al performed a retrospective, multicentric, comparative cohort study evaluating clinical course and outcomes in patients with autoimmune versus non-autoimmune SINS. In this study, 37.8% of eyes were classified as autoimmune, indicating a previous or subsequent diagnosis of systemic autoimmune disease, and 62.2% were classified as non-autoimmune, indicating no diagnosis of systemic autoimmune disease. Ruiz-Lozano et al found that eyes with autoimmune SINS had higher rates of cataract surgery, severe scleral inflammation, and higher incidence of ocular complications when compared to the non-autoimmune group.25
In addition to the patient’s past medical and surgical history, a thorough review of systems may raise suspicion for possible yet-to-be diagnosed underlying systemic conditions and help guide laboratory testing. A detailed social history is also important, including sexual history, possible exposures or ocular trauma, travel, animal contact, and current/previous places of residency. This, along with the review of systems, may help determine one’s level of concern for possible infectious process underlying scleritis diagnosis. Etiologic testing to consider in most patients with scleritis includes ANCA, RF, anti-CCP, ANA, HLA-B27, ACE, CXR, ESR, CRP, CBC, and evaluation to exclude treponemal and tubercular disease. The results of these tests may help elucidate possible associated autoimmune/infectious etiologies, as well as play a role in treatment selection. Bacterial, viral, fungal, or parasitic organisms can cause infectious scleritis. The most common infectious organism reported is Mycobacterium tuberculosis, the causative organism of ocular tuberculosis (TB). Although ocular TB typically manifests as uveitis, it has been found to cause necrotizing, non-necrotizing, nodular, or diffuse scleritis, and may lead to scleromalacia perforans, sclerokeratitis, and scleritis.1 Another common causative organism is a member of the herpes virus family, such as herpes simplex virus and varicella zoster virus, and the clinician should be suspicious of this especially in cases of scleritis with concurrent keratitis. Treponema pallidum, the causative organism of syphilis, may present with ocular involvement, including scleritis, at any stage of the disease. Additional organisms reported in the literature are extensive, including corynebacterium, Borrelia, Mycobacterium leprae, Pseudomonas aeruginosa, Brucella, Epstein-Barr virus, Measles virus, Chikunguyna, Mumps virus, Rubella virus, Cytomegalovirus, Toxoplasma gondii, Aspergillus, and Acanthamoeba species,1,3,6 and clinical suspicion for these organisms can be further elucidated based on a thorough social history and review of systems.
General Approach to Treatment
The general approach to non-infectious scleritis treatment is to utilize the least aggressive form of therapy needed to adequately control inflammation, often termed the stepladder approach (Figure 4). The stepladder approach may start with topical therapy alone, especially in cases of mild anterior scleritis, or with systemic non-steroidal anti-inflammatory drugs (NSAIDs) with or without topical therapy. Systemic corticosteroids are often the next step if adequate control is not achieved or if NSAIDs are contraindicated, with escalation to steroid-sparing systemic immunomodulatory therapy if additional treatment is needed. Although systemic NSAIDs and corticosteroids are often used to control inflammation in the short term, steroid-sparing systemic immunomodulatory agents are more appropriate for long-term inflammatory control. Additionally, biologic, small molecule targeted inhibitor, or cytotoxic drugs may be needed.26 Scleritis relapses often occur, with reported rates of relapse ranging from 35.9% to 69% depending on the study population.12,27 Given these relapse rates, it is common for patients to require long term treatment. Approximately 50% of patients with scleritis require treatment with steroid-sparing immunomodulatory therapies,28 which emphasizes the important role of thorough systemic workup and potential involvement of rheumatology colleagues for multidisciplinary expertise.
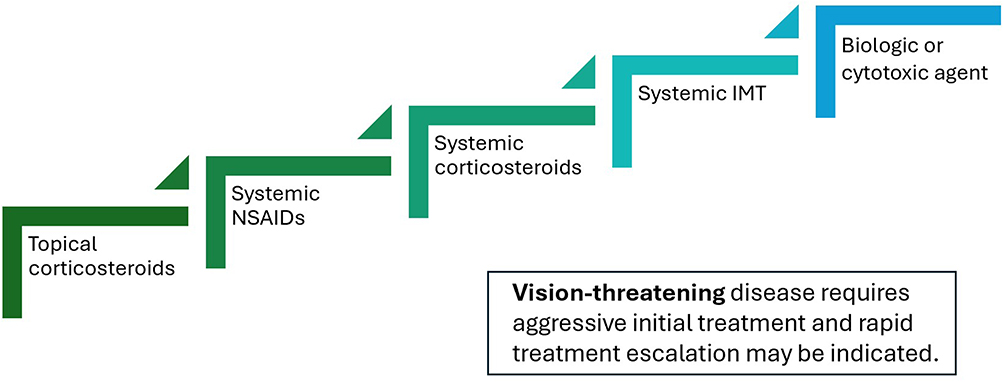 |
Figure 4 General approach to non-infectious scleritis treatment. |
In addition to lack of adequate response to initial therapy, there are reasons to more quickly escalate treatment beyond systemic NSAIDs and corticosteroids. Vision-threatening sequelae of scleritis include sclerokeratitis, cystoid macular edema, optic disc edema, and serous retinal detachment.4 Additionally, the posterior scleritis subtype and any type of necrotizing scleritis can progress quickly to vision-threatening disease and often require rapid escalation of treatment. Dutta Majumder and coauthors recommend that in contrast to other forms of scleritis for which a stepladder approach is recommended, necrotizing scleritis requires aggressive treatment from the time of diagnosis.8 Beyond ocular disease, systemic inflammatory diseases occurring in association with scleritis may also require systemic therapy, particularly to address life or organ-threatening manifestations. Depending on the associated systemic inflammatory condition, treatment may be tailored based on known efficacy of certain medications for systemic diseases. In patients with scleritis and a systemic inflammatory disease, a reasonable approach in selecting immunomodulatory therapies is to prioritize medications that are not only efficacious for scleritis but also approved for treating the patient’s systemic inflammatory disease.
Beyond medications, important aspects of scleritis treatment include ocular protection and potentially modifiable risk factors. Ocular protection may be considered while patients are sleeping and possibly during the day, especially for patients who are at risk for ocular perforation, such as those with scleromalacia perforans or necrotizing scleritis. Additionally, there may be a role for addressing patient-modifiable factors in the course of scleritis. One study showed a possible association between low vitamin D levels and increased risk of scleritis.29 Another possible patient-modifying factor is smoking status. One study showed a delay in response to treatment in patients with scleritis who were actively smoking during treatment, resulting in more intense therapy than those who were not smoking.30 Another study reported an association of smoking with bilateral ocular inflammation and reduced visual acuity upon presentation, and an increased risk of disease recurrence compared to nonsmokers.31 A large study analyzing scleritis in the IRIS® Registry (Intelligent Research in Sight) showed active smoking as a risk factor for substantial vision loss and elevated IOP in scleritis patients.4 Although addressing these modifiable factors is yet to be proven, treating vitamin D deficiency and encouraging smoking cessation are low risk interventions and may be beneficial for scleritis treatment.
Therapeutic Agents for Non-Infectious Scleritis
Topical Treatment
Topical corticosteroid therapy may be considered for mild anterior scleritis. A Canadian study of patients with non-necrotizing anterior scleritis reported a 2-month treatment success rate of 47% with 1% prednisolone acetate eye drops administered initially every 2 hours.32 However, ocular inflammatory disease specialists at tertiary referral centers observed lower rates of treatment success and as a result, were less likely to utilize topical corticosteroid monotherapy from scleritis treatment regimens.28,33 This preference for systemic treatment was not isolated to tertiary referral centers. Even in a community-based practice cohort, 93% of patients with scleritis seen between 2001 and 2007 received systemic treatment.34
More recent research with difluprednate, a more potent topical corticosteroid, has renewed interest in topical corticosteroid therapy for scleritis. A retrospective review of patients with anterior scleritis treated with difluprednate monotherapy reported a 83% treatment success rate.35 The same group conducted a second retrospective review evaluating the effect of adding difluprednate to pre-existing systemic treatment for anterior scleritis and reported a treatment success rate of 80%.36 In these two studies, intraocular pressure elevation was recorded in 26% and 25% of eyes and cataract progression occurred in 6% and 11% of eyes.35,36
Although the evidence is limited, case reports indicate that topical cyclosporine37 and topical tacrolimus38–40 may be efficacious for certain subtypes of anterior scleritis. Topical cyclosporine and tacrolimus tend to be well-tolerated and do not have the side effects of intraocular pressure elevation and cataract progression associated with topical corticosteroids.
Subconjunctival Injections
Subconjunctival corticosteroid injections had been contraindicated in scleritis treatment due to concern for scleral necrosis, a rare but serious side effect.41 However, a multi-center study of non-necrotizing, noninfectious anterior scleritis showed that subconjunctival 40 mg/mL triamcinolone acetonide injection (2–8 mg) was effective in 97% of eyes.42 Side effects included ocular hypertension (21%), glaucoma (6%), and cataract development (3%). There were no cases of scleral necrosis in any of the 68 eyes. Still, concern for scleral necrosis continues to limit use of subconjunctival corticosteroids in the setting of scleritis, and subconjunctival corticosteroids are only recommended in eyes with non-necrotizing scleritis. An open label pilot study of patients with non-necrotizing noninfectious anterior scleritis treated with subconjunctival sirolimus showed improvement and/or resolution of disease activity by week 8 in all 5 patients.43
Systemic NSAIDs
Many ocular inflammatory disease specialists use systemic NSAIDs as a first-line treatment for non-necrotizing anterior scleritis. The reported treatment success rate was 57% in patients with nodular anterior scleritis and 33% in patients with diffuse anterior scleritis prescribed oral indomethacin 25 mg four times a day.33 Other NSAIDs may be prescribed (Table 1), and ibuprofen and certain doses of naproxen are available without a prescription in the United States. Although the reported treatment success rate is lower in posterior scleritis, oral NSAID monotherapy is effective for some patients with posterior scleritis.44,45 However, NSAIDs increase patients’ risk of renal dysfunction, gastrointestinal (GI) bleeding, and cardiovascular events, and patients >65 years of age are more likely to develop these side effects.46 Selective COX-2 inhibitors, such as celoxocib, the only selective COX-2 inhibitor available in the United States, have shown promise in effectively managing scleritis while reducing the risk of gastrointestinal, platelet dysfunction, and renal side effects.47 NSAIDs are contraindicated during the third trimester of pregnancy because they pose an increased risk of both oligohydramnios and premature closure of the fetal ductus arteriosus, and many physicians avoid prescribing NSAIDs in the first trimester as well given an association with miscarriage in some studies.48
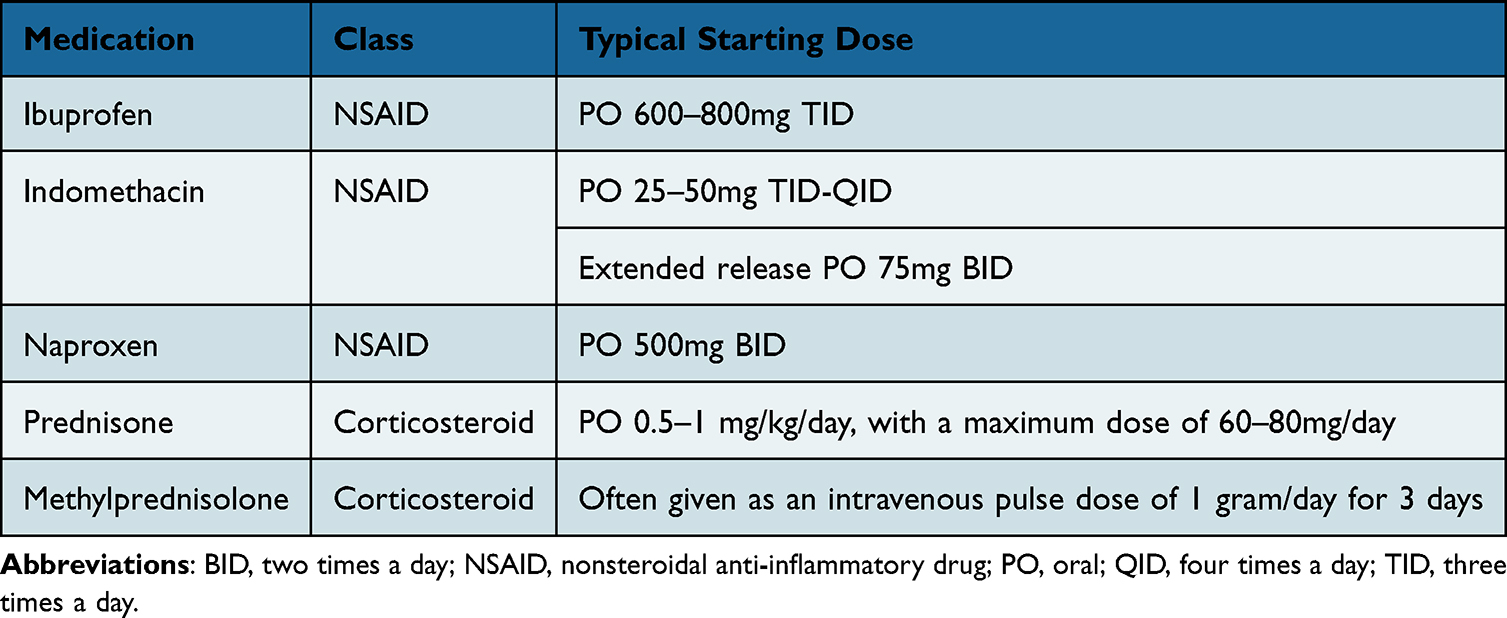 |
Table 1 Common Systemic Medications for Initial Treatment of Non-Infectious Scleritis |
Systemic Corticosteroids
Oral prednisone is a mainstay of treatment and is widely used when there is no or incomplete treatment response with NSAIDs or topical therapy alone, or in those with posterior or necrotizing disease. Dosage can vary, but is often started at 1 mg/kg/day, with a gradual taper over at least 4–6 weeks.49 In addition to oral prednisone, clinicians may use pulse dose intravenous methylprednisolone (Table 1), particularly in patients intolerant to oral corticosteroids or in cases of aggressive scleritis, such as necrotizing scleritis.8 Side effects of corticosteroids must be considered and discussed with the patient, including but not limited to weight gain, mood changes, gastrointestinal issues, insomnia, Cushing syndrome, glucose intolerance, elevated blood pressure and avascular necrosis of the hip. Oral and intravenous corticosteroids are often used as acute treatment for scleritis, but consideration of other immune-modifying treatments should be considered in cases refractory to corticosteroids or with chronic/recurrent disease.
Conventional Immunomodulatory Therapies
Steroid-sparing immunomodulatory therapies (IMT) are widely used for long-term inflammatory control in patients with scleritis. Conventional immunomodulatory therapies include antimetabolites, calcineurin inhibitors, and alkylating agents (Table 2).
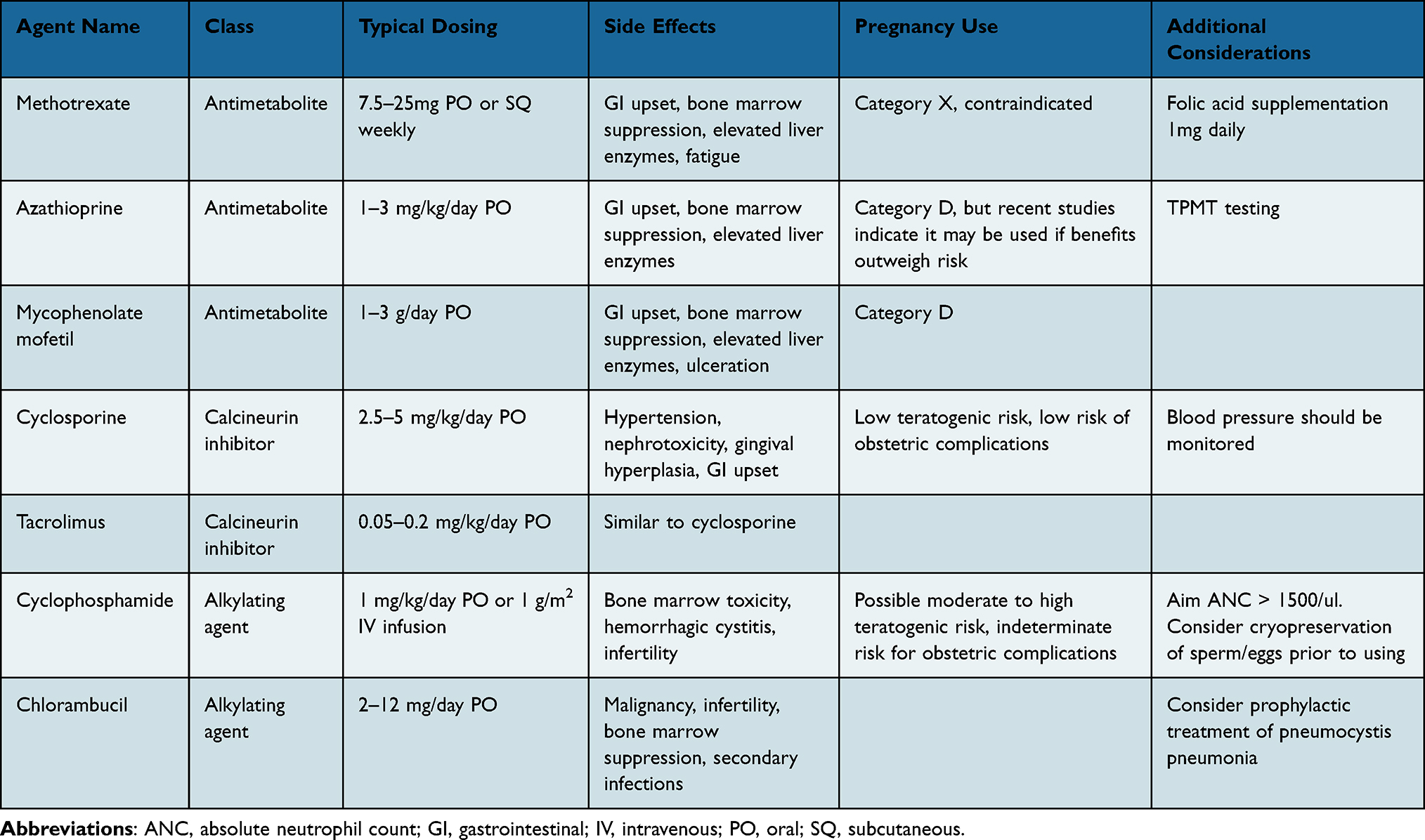 |
Table 2 Common Immunomodulatory Therapies for Treatment of Non-Infectious Scleritis |
One of the most commonly used antimetabolites is methotrexate, and this has been shown to be effective for treatment of ocular inflammation in both children and adults.49 It was introduced in 1948, was originally used as an antineoplastic agent, and was approved for rheumatoid arthritis treatment by the United States Food and Drug Administration in 1988.50 Methotrexate is an inhibitor of dihydrofolate reductase, which results in interference of DNA synthesis, repair, and cellular replication. It reduces the rate of cellular proliferation, increases the rate of T-cell apoptosis, increases endogenous concentrations of adenosine, and alters the production of cytokines and humoral response. In the Systemic Immunosuppressive Therapy for Eye Diseases Cohort Study (SITE), 55.6% of eyes with scleritis treated with methotrexate as the only immunosuppressive therapy (n=56 eyes) achieved inflammatory control with less than or equal to 5mg daily prednisone at 12 months.50 Commonly reported side effects with methotrexate include gastrointestinal upset, bone marrow suppression, and elevated liver enzymes. Importantly, methotrexate is a known teratogen. It should not be prescribed for patients attempting conception and appropriate contraceptive counseling is required in patients with reproductive potential. Overall, methotrexate tends to be well tolerated and is commonly used as a first line steroid-sparing agent in both adults and children for treatment of scleritis.49
Mycophenolate mofetil is another antimetabolite commonly used in scleritis treatment. It is widely used for immunosuppression in transplant patients. It reversibly binds to inosine monophosphate dehydrogenase, inhibiting the de novo synthesis of purine nucleotides, resulting in decreased B and T cell proliferation, as well as antibody production. The SITE Cohort Study showed that in 33 patients with scleritis treated with mycophenolate, control of inflammation with less than or equal to 5mg of prednisone was seen in 44.7% of patients at 12 months.51 Interestingly, in a study conducted by Ozzello et al, practice patterns among uveitis specialists and rheumatologists differed when treating scleritis in regards to use of mycophenolate mofetil. While 44.4% of uveitis specialists chose methotrexate as first line, 27.8% chose mycophenolate mofetil. This contrasts with rheumatologists, with 78.6% choosing methotrexate as first line, and only 5.4% choosing mycophenolate.52 This study emphasizes the lack of evidence-based medicine as well as differences in specialty practice leading to a wide array of potential management courses for patients with scleritis. Similar to other antimetabolites, commonly reported side effects include gastrointestinal upset, bone marrow suppression, and elevated liver enzymes.
Another commonly used antimetabolite in the treatment of scleritis is azathioprine. Azathioprine is a purine nucleoside analog which acts by interfering with DNA and RNA synthesis. A review by Pasadhika et al of patients from the SITE Cohort Study examined response to azathioprine in 16 patients with scleritis. Among those, 76.6% showed improved inflammation by 12 months, with 29.9% achieving inflammatory control on less than or equal to 5mg of prednisone.53 Similar to methotrexate and mycophenolate, common side effects include gastrointestinal upset, bone marrow suppression, and elevated liver enzymes. Additionally, some clinicians advocate for testing for thiopurine methyltransferase (TPMT) prior to initiation of azathioprine.49 Patients with low or absent TPMT activity are at risk for developing severe myelosuppression if treated with azathioprine, so testing can help determine need for dose adjustments or avoidance of therapy.
Calcineurin inhibitors such as tacrolimus and cyclosporine can be used in treatment of scleritis. Cyclosporine is the more commonly used medication in the T-cell inhibitor class. It prevents the translocation of Nuclear Factor of Activated T-Cells (NFAT) by binding to calcineurin, which prevents cell replication and the upregulation of various cytokines including IL-2 and interferon-gamma. The SITE Cohort Study showed that in 15 patients treated with cyclosporine as the only immunosuppressive therapy, 50.6% of patients showed inflammatory control with less than or equal to 5mg of prednisone at 12 months.54 Adverse events reported with cyclosporine use include hypertension, renal toxicity, gingival hyperplasia, and elevated liver enzymes. Tacrolimus is another medication from the T-cell inhibitor class. It is a macrolide antibiotic that works to inhibit T-cells by inhibiting calcineurin and subsequently NFAT.49 Review of current literature documenting its role in scleritis is limited, but it can be considered for patients unresponsive to other treatments.
Biologics
Additional immunomodulatory therapies include biologics, which have gained favor in recent years as evidence of their efficacy continues to grow and new inflammatory targets are discovered. Classes of biologics with reported efficacy in scleritis include tumor necrosis factor (TNF) inhibitors, CD20 inhibitors, interleukin (IL)-6 inhibitors, and IL-1 inhibitors (Table 3).
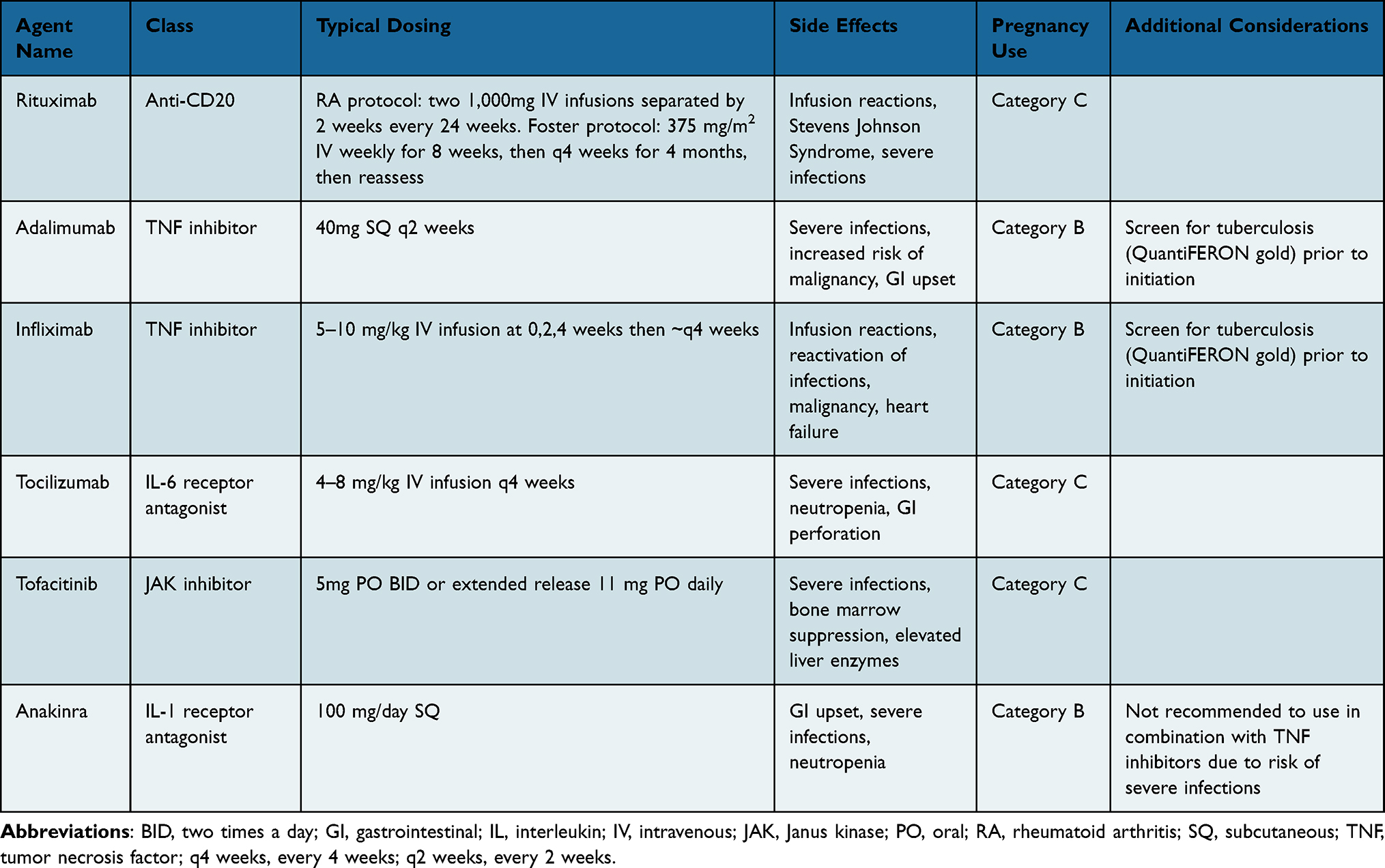 |
Table 3 Biologic Agents and Small Molecule Targeted Inhibitors for Treatment of Non-Infectious Scleritis |
TNF inhibitors are a class of biologics commonly used to treat noninfectious ocular inflammation. Among this class are adalimumab, infliximab, golimumab, certolizumab, and etanercept. TNF-alpha is found in scleral tissue of patients with scleritis and therefore may be an appropriate target for inflammatory control.49 A multicenter chart review showed that at 6 months, 82.2% of subjects achieved disease quiescence with TNF inhibitors, with a statistically significant decrease in baseline daily corticosteroid use. Adalimumab was the most commonly used TNF inhibitor, followed by infliximab, certolizumab, and etanercept.55 Another study of 28 eyes from 19 patients showed the complete resolution of scleritis with TNF inhibitor use in 13/21 eyes, improvement in 4/21 eyes, and no improvement in 4/21 eyes. The remaining 7 eyes were quiescent at baseline, and remained quiescent during the 12 month follow up period. Concurrent corticosteroid dosing also significantly decreased during the follow up period. Additionally, nearly 60% of eyes demonstrated control of inflammation within 3 months of starting treatment.56 Among the TNF inhibitors, etanercept is considered less efficacious for treatment of ocular inflammatory diseases and has been associated with increased risk of ocular inflammation,57 so is less likely to be an initial choice. Side effects of TNF inhibitors include risk of serious infections including reactivation of latent tuberculosis, demyelinating disease and a possible increased risk of dermatologic malignancy.58 Screening for latent tuberculosis, hepatitis B, and hepatitis C should be performed in patients prior to initiating TNF inhibitor therapy.
Rituximab is a human-mouse chimeric monoclonal antibody that targets the CD20 receptor on B lymphocytes, resulting in the depletion of B cells and B cell precursors.49 It is commonly used in the treatment of rheumatoid arthritis, granulomatosis with polyangiitis, and B cell malignancies. A prospective, randomized control trial by Suhler et al in 2014 demonstrated a positive therapeutic effect of rituximab in 9 of 12 patients with scleritis within 24 weeks of therapy, with more than half of the patients requiring repeat treatment to maintain inflammatory control.59 A retrospective study of 15 patients with noninfectious scleritis showed that 13 of the 15 achieved a scleritis activity score of 0 at 6 months, 6 of whom were using rituximab monotherapy.60 Side effects of rituximab include severe infections, infusion reactions, mucocutaneous reactions, and pulmonary edema.49
Tocilizumab is a monoclonal antibody targeting the IL-6 receptor. Its role in scleritis treatment is still being defined, but multiple small studies have demonstrated efficacy in inflammatory control with this medication. A retrospective review of 4 patients with scleritis showed inflammatory control in 50% of patients at both 6 and 9 months.61 Several case reports found that tocilizumab is efficacious for treatment of recalcitrant scleritis including scleritis that has failed other conventional and biologic immunsuppressives.62–65 Although IL-6 inhibition is a potential alternate option for scleritis control, especially in recalcitrant cases, prospective studies are indicated to better assess its efficacy. Side effects include severe infections, neutropenia, liver enzyme elevation and risk of GI perforation.
IL-1 inhibitors are an additional class demonstrating possible efficacy in scleritis management. IL-1 is a proinflammatory cytokine that plays an important role in the innate immune response. It mediates the acute phase of inflammation by inducing local and systemic inflammatory responses, such as pain, fever, vasodilation, and hypotension.66 Data regarding its use in scleritis is promising but limited. One study by Bottin et al reported 10 patients with scleritis who underwent treatment with an IL-1 inhibitor, anakinra. The mean number of scleritis disease flares on other DMARDs prior to starting anakinra was approximately 7.5 per year. Remission was achieved within 1 month for 8 patients, and within 2 months for 1 patient. The mean scleritis relapse rate decreased from 7.5 to 0.27 per year with anakinra use.67 Additionally, Knickelbein et al performed a prospective pilot trial using gevokizumab, an IL-1B inhibitor, for treatment of non-infectious scleritis.68 They showed that 7 eyes from 7 patients demonstrated a clinical improvement of at least a 2-step reduction or achievement of grade 0 inflammation within 2 weeks following the first gevokizumab injection, with no serious adverse effects related to the study drug. Side effects of IL-1 inhibitors include severe infections, GI upset, and neutropenia.
Small Molecule Targeted Inhibitors
Janus kinase (JAK) inhibitors are a therapeutic class under active investigation for the treatment of ocular inflammatory diseases. Commercially available agents include tofacitinib, upadacitinib, and baricitinib. The JAK pathway plays a role in regulating inflammatory cells, cytokine synthesis, and proinflammatory signal transduction. JAK inhibitors are small molecule inhibitors of the JAK pathway and have shown promising results in autoimmune diseases such as rheumatoid arthritis, systemic sclerosis, SLE, dermatomyositis, Sjogren’s syndrome, and vasculitis.69 A prospective, registry-based cohort study evaluated patients with non-infectious uveitis and scleritis receiving JAK inhibitors. Of these patients, 2 of the 12 had scleritis, with the remainder diagnosed with other ocular inflammatory conditions. The authors report that complete disease control was achieved by the last follow up visit in 12/12 patients, although not all of the patients were on JAK inhibitors alone.70 They did also note a significant reduction in the risk of experiencing recurrences when comparing relapses occurring in the 12 months prior to initiation of JAK inhibitor with those observed during the study period. Additionally, several case reports and case series report a good therapeutic effect of JAK inhibitors in treatment of recalcitrant scleritis.71–78 Continued research into the use of JAK inhibitors is indicated given demonstrated efficacy in these case reports. One such study is the CLARITY trial, a Phase 3 randomized clinical trial of a JAK inhibitor, brepocitinib, in posterior segment uveitis. If efficacious, this may provide additional support for trialing this class of medications in scleritis treatment. Side effects of JAK inhibitors include severe infections, bone marrow suppression, and elevated liver enzymes. Of particular clinical relevance with use of JAK inhibitors is their association with reactivation of varicella-zoster virus,79 emphasizing the importance of zoster vaccination.
Alkylating Agents
Alkylating agents, though known to have potentially severe adverse side effects that prevent wide-spread use, can be utilized as treatment for scleritis, especially in severe or recalcitrant cases unresponsive to other therapies. Cyclophosphamide, both oral and intravenous, has been shown to be efficacious. Cyclophosphamide acts by alkylating nucleophilic groups on DNA bases, leading to abnormal DNA synthesis during mitosis, which profoundly suppresses the function of both B and T cells.80 A study of 4 patients (5 eyes) with necrotizing scleritis treated with cyclophosphamide showed complete remission in 3 of the 5 eyes, with the additional 2 showing response but then subsequently flaring 6 months after cyclophosphamide was stopped.81 The SITE Cohort Study showed that in 48 patients with scleritis treated with cyclophosphamide, 37.8% experienced controlled inflammation with less than or equal to 5mg of prednisone by 12 months.80 Side effects include leukopenia, hemorrhagic cystitis, secondary malignancies and fertility issues.81 Chlorambucil is another alkylating agent used to treat scleritis. A study by Goldstein et al reported 4 of 5 patients with scleritis treated with chlorambucil demonstrated sustained remission after treatment.82 Adverse effects associated with chlorambucil use include malignancy, infertility, bone marrow suppression, and secondary infections, among others.
Surgical Treatment for Non-Infectious Scleritis
The treatment approach for non-infectious scleritis relies heavily on medical management, but surgical treatment may be considered in specific circumstances. In cases of progressive scleral thinning despite maximizing medical management, placement of a tarsorrhaphy with a scleral patch graft may be considered. Graft material options include donor sclera, cornea, fascia lata, periosteum, auricular cartilage, split thickness dermal grafts, oral mucosa, and polytetrafluoroethylene (Gore-Tex), among others.8 A study of 13 eyes requiring scleral patch grafting for various etiologies, most frequently necrotizing scleritis, showed tectonic success in 10 eyes.83 In addition to a scleral patch graft, a conjunctival flap/autograft plus or minus an amniotic membrane could be considered, especially in cases of necrotizing scleritis. Placement of tarsorrhaphy or amniotic membrane alone may be beneficial for milder cases of scleritis without significant scleral thinning requiring a scleral patch. The goal of surgical intervention is tectonic stabilization of the eye, but medical therapy for inflammatory control is still needed in most cases.
Additionally, cataract surgery may be indicated in eyes with scleritis. The incidence of cataract surgery in scleritis patients was found to be relatively low in the Systemic Immunosuppressive Therapy for Eye Diseases cohort study (0.025/eye-year), lower than the incidence in eyes with anterior and intermediate uveitis evaluated in the same study.84 Use of oral corticosteroids significantly increased the incidence of cataract, but no difference in cataract surgery rate was found between high and low dose corticosteroids. Perioperative considerations for cataract surgery in patients with scleritis include inflammatory control prior to surgery and consideration of perioperative systemic steroids. A multi-disciplinary discussion between the cataract surgeon and uveitis specialist or rheumatologist should occur prior to surgery to optimize the surgical outcome. Factors such as scleritis severity, frequency of flares, underlying systemic inflammatory disease, and current scleritis therapies should all be considered during perioperative planning. In general, eyes with a history of scleritis have good visual outcomes after cataract surgery,84–86 but ocular inflammatory control is important in the perioperative period.
Conclusion
In summary, non-infectious scleritis is a potentially vision threatening inflammatory disease which often requires long-term treatment. The general approach to management should consist of a thorough systemic workup and subsequent selection of the most appropriate therapeutic agent(s) based on individual patient characteristics, disease features and course, and side effect profile. Recent clinical studies identify more potent topical corticosteroids and biologic agents as efficacious in the treatment of non-infectious scleritis. We welcome the development and assessment of future therapeutics for scleritis as our understanding of the immune system, disease pathogenesis and potential disease targets continues to improve.
Disclosure
Dr Karen Armbrust reports grants from Research to Prevent Blindness/American Academy of Ophthalmology, outside the submitted work. The authors report no other conflicts of interest in this work.
References
1. Cifuentes-González C, Mejía-Salgado G, Rojas-Carabali W. et al. The Global Epidemiology of Scleritis: a Systematic Review and Meta-analysis. Am J Ophthalmol. 2025;273:13–15. doi:10.1016/j.ajo.2025.01.019
2. Spangler MD, Marshall RF, Kirupaharan N, Armbrust KR, Berkenstock MK. Incidence and Prevalence of Scleritis Subtypes and Associated Ocular Complications in the TriNetX Database. Am J Ophthalmol. 2025;277:365–374. doi:10.1016/j.ajo.2025.05.028
3. Braithwaite T, Adderley NJ, Subramanian A, et al. Epidemiology of Scleritis in the United Kingdom From 1997 to 2018: population-Based Analysis of 11 Million Patients and Association Between Scleritis and Infectious and Immune-Mediated Inflammatory Disease. Arthritis Rheumatol. 2021;73(7):1267–1276. doi:10.1002/art.41709
4. Armbrust KR, Kopplin LJ. Characteristics and Outcomes of Patients with Scleritis in the IRIS® Registry (Intelligent Research in Sight) Database. Ophthalmol Sci. 2022;2(3):100178. doi:10.1016/j.xops.2022.100178
5. Zhang Y, Amin S, Lung KI, Seabury S, Rao N, Toy BC. Incidence, prevalence, and risk factors of infectious uveitis and scleritis in the United States: a claims-based analysis. PLoS One. 2020;15(8):e0237995. doi:10.1371/journal.pone.0237995
6. Murthy SI, Sabhapandit S, Balamurugan S, et al. Scleritis: differentiating infectious from non-infectious entities. Indian J Ophthalmol. 2020;68(9):1818–1828. doi:10.4103/ijo.IJO_2032_20
7. Watson PG, Singh Hayreht S. Scleritis and episcleritis. Br J Ophthalmol. 1976;60(3):163–191. doi:10.1136/bjo.60.3.163
8. Dutta Majumder P, Agarwal S, Shah M, et al. Necrotizing scleritis: a review. Ocul Immunol Inflamm. 2024;32(7):1405–1419. doi:10.1080/09273948.2023.2206898
9. Shoughy SS, Jaroudi MO, Kozak I, Tabbara KF. Optical coherence tomography in the diagnosis of scleritis and episcleritis. Am J Ophthalmol. 2015;159(6):1045–1049.e1. doi:10.1016/j.ajo.2015.03.004
10. Smeller L, Toth-Molnar E, Sohar N. Optical coherence tomography: focus on the pathology of macula in scleritis patients. J Clin Med. 2023;12(14). doi:10.3390/jcm12144825
11. Lane J, Nyugen E, Morrison J, et al. Clinical features of scleritis across the Asia-Pacific region. Ocul Immunol Inflamm. 2019;27(6):920–926. doi:10.1080/09273948.2018.1484496
12. Morrison T, Gottman M, Do T, Rosenbaum JT, Ghetie D, Friedman M. Scleritis and development of immune-mediated disease: a retrospective chart review. J Rheumatol. 2024;51(8):825–830. doi:10.3899/jrheum.2023-0788
13. Promelle V, Goeb V, Gueudry J. Rheumatoid arthritis associated episcleritis and scleritis: an update on treatment perspectives. J Clin Med. 2021;10(10). doi:10.3390/jcm10102118
14. Hoang LT, Lim LL, Vaillant B, Choi D, Rosenbaum JT. Antineutrophil cytoplasmic antibody-associated active scleritis. Arch Ophthalmol. 2008;126(5):651–655. doi:10.1001/archopht.126.5.651
15. Perray L, Nguyen Y, Clavel Refregiers G, et al. ANCA-associated scleritis: impact of ANCA on presentation, response to therapy and outcome. Rheumatology. 2024;63(2):329–337. doi:10.1093/rheumatology/kead252
16. Wong RW, Chan A, Johnson RN, et al. Posterior scleritis in patients with systemic lupus erythematosus. Retin Cases Brief Rep. 2010;4(4):326–331. doi:10.1097/ICB.0b013e3181e1806e
17. Dammacco R, Procaccio P, Racanelli V, Vacca A, Dammacco F. Ocular involvement in systemic lupus erythematosus: the experience of two tertiary referral centers. Ocul Immunol Inflamm. 2018;26(8):1154–1165. doi:10.1080/09273948.2018.1501495
18. Hsu CS, Hsu CW, Lu MC, Koo M. Risks of ophthalmic disorders in patients with systemic lupus erythematosus - a secondary cohort analysis of population-based claims data. BMC Ophthalmol. 2020;20(1):96. doi:10.1186/s12886-020-01360-w
19. Berkenstock MK, Carey AR. Health system wide “big data” analysis of rheumatologic conditions and scleritis. BMC Ophthalmol. 2021;21(1). doi:10.1186/s12886-020-01769-3
20. Dursun D, Akova YA, Bilezikçi B. Scleritis associated with sarcoidosis. Ocul Immunol Inflamm. 2004;12(2):143–148. doi:10.1080/09273940490895353
21. Etminan M, Forooghian F, Maberley D. Inflammatory ocular adverse events with the use of oral bisphosphonates: a retrospective cohort study. CMAJ. 2012;184(8):E431–434. doi:10.1503/cmaj.111752
22. Chaudot F, Sève P, Rousseau A, et al. Ocular inflammation induced by immune checkpoint inhibitors. J Clin Med. 2022;11(17). doi:10.3390/jcm11174993
23. Ruiz-Lozano RE, Garza-Garza LA, Davila-Cavazos O, Foster CS, Rodriguez-Garcia A. The clinical and pathogenic spectrum of surgically-induced scleral necrosis: a review. Surv Ophthalmol. 2021;66(4):594–611. doi:10.1016/j.survophthal.2020.12.008
24. O’Donoghue E, Lightman S, Tuft S, Watson P. Surgically induced necrotising sclerokeratitis (SINS) – precipitating factors and response to treatment. Br J Ophthalmol. 1992;76(1):17–21.
25. Ruiz-Lozano RE, Ramos-Dávila EM, Colorado-Zavala MF, et al. Clinical course and outcomes of autoimmune versus non-autoimmune surgically induced scleral necrosis: a multicentric comparative study. Ocul Immunol Inflamm. 2025;33(1):65–71. doi:10.1080/09273948.2024.2349914
26. Foster CS, Kothari S, Anesi SD, et al. The Ocular Immunology and Uveitis Foundation preferred practice patterns of uveitis management. Surv Ophthalmol. 2016;61(1):1–17. doi:10.1016/j.survophthal.2015.07.001
27. Tuft SJ, Watson PG. Progression of Scleral Disease. Ophthalmology. 1991;98(4):467–471. doi:10.1016/s0161-6420(91)32269-3
28. Sainz De La Maza M, Molina N, Gonzalez-Gonzalez LA, Doctor PP, Tauber J, Foster CS. Scleritis therapy. Ophthalmology. 2012;119(1):51–58. doi:10.1016/J.OPHTHA.2011.07.043
29. Llop SM, Davoudi S, Stanwyck LK, et al. Association of low vitamin D levels with noninfectious uveitis and scleritis. Ocul Immunol Inflamm. 2019;27(4):602–609. doi:10.1080/09273948.2018.1434208
30. Boonman ZFHM, de Keizer RJW, Watson PG. Smoking delays the response to treatment in episcleritis and scleritis. Eye. 2005;19(9):949–955. doi:10.1038/sj.eye.6701731
31. Galor A, Feuer W, Kempen JH, et al. Adverse effects of smoking on patients with ocular inflammation. Br J Ophthalmol. 2010;94(7):848–853. doi:10.1136/bjo.2009.174466
32. McMullen M, Kovarik G, Hodge WG. Use of topical steroid therapy in the management of nonnecrotizing anterior scleritis. Can J Ophthalmol. 1999;34(4):217–221.
33. Jabs DA, Mudun A, Dunn JP, Marsh MJ. Episcleritis and scleritis: clinical features and treatment results. Am J Ophthalmol. 2000;130:469–476.
34. Raiji VR, Palestine AG, Parver DL. Scleritis and systemic disease association in a community-based referral practice. Am J Ophthalmol. 2009;148(6):946–950. doi:10.1016/j.ajo.2009.07.021
35. Liberman P, Burkholder BM, Thorne JE, Berkenstock MK. Effectiveness of difluprednate for the treatment of anterior scleritis. Am J Ophthalmol. 2022;235:172–177. doi:10.1016/j.ajo.2021.09.008
36. Liberman P, Thorne J, Burkholder B, Berkenstock MK. Effectiveness of difluprednate in addition to systemic therapy for the treatment of anterior scleritis. Br J Ophthalmol. 2024;108(7):951–955. doi:10.1136/bjo-2022-322841
37. Grullon JR, Mueller C, Iacob CE, Swan R. Use of cyclosporine A 0.05% ophthalmic emulsion for a distinctive intrapalpebral phenotype of anterior scleritis. BMJ Case Rep. 2025;18(2). doi:10.1136/bcr-2024-264327
38. Lee YJ, Kim SW, Seo KY. Application for tacrolimus ointment in treating refractory inflammatory ocular surface diseases. Am J Ophthalmol. 2013;155(5):804–813. doi:10.1016/j.ajo.2012.12.009
39. Miyazaki D, Tominaga T, Kakimaru-Hasegawa A, Nagata Y, Hasegawa J, Inoue Y. Therapeutic effects of tacrolimus ointment for refractory ocular surface inflammatory diseases. Ophthalmology. 2008;115(6). doi:10.1016/j.ophtha.2007.07.025
40. Yazu H, Miyazaki D, Fujishima H. Experience With 0.1% tacrolimus eye drop for noninfectious, non-necrotizing anterior scleritis. Eye Contact Lens. 2021;47(4):185–190. doi:10.1097/ICL.0000000000000696
41. Watson PG. The diagnosis and management of scleritis. Ophthalmology. 1980;87(7):716–720. doi:10.1016/s0161-6420(80)35177-4
42. Sohn EH, Wang R, Read R, et al. Long-term, multicenter evaluation of subconjunctival injection of triamcinolone for non-necrotizing, noninfectious anterior scleritis. Ophthalmology. 2011;118(10):1932–1937. doi:10.1016/j.ophtha.2011.02.043
43. Bhatt N, Dalal M, Tucker W, Obiyor D, Nussenblatt R, Sen HN. Subconjunctival sirolimus in the treatment of autoimmune non-necrotizing anterior scleritis: results of a Phase I/II clinical trial. Am J Ophthalmol. 2015;159(3):601–606. doi:10.1016/j.ajo.2014.12.009
44. Calthorpe CM, Watson PG, McCartney AC. Posterior scleritis: a clinical and histological survey. Eye. 1988;2:267–277. doi:10.1038/eye.1988.52
45. Cheung CMG, Chee SP. Posterior scleritis in children: clinical features and treatment. Ophthalmology. 2012;119(1):59–65. doi:10.1016/j.ophtha.2011.09.030
46. Davis A, Robson J. The dangers of NSAIDs: look both ways. Br J Gen Pract. 2016;66(645):172–173. doi:10.3399/bjgp16X684433
47. Bauer AM, Fiehn C, Becker MD. Celecoxib, a selective inhibitor of cyclooxygenase 2 for therapy of diffuse anterior scleritis. Am J Ophthalmol. 2005;139(6):1086–1089. doi:10.1016/j.ajo.2005.01.030
48. Peterson EA, Lynton J, Bernard A, Santillan MK, Bettendorf B. Rheumatologic medication use during pregnancy. Obstet Gynecol. 2020;135(5):1161–1176. doi:10.1097/AOG.0000000000003755
49. Beardsley RM, Suhler EB, Rosenbaum JT, Lin P. Pharmacotherapy of scleritis: current paradigms and future directions. Expert Opin Pharmacother. 2013;14(4):411–424. doi:10.1517/14656566.2013.772982
50. Gangaputra S, Newcomb CW, Liesegang TL, et al. Methotrexate for ocular inflammatory diseases. Ophthalmology. 2009;116(11). doi:10.1016/j.ophtha.2009.04.020
51. Daniel E, Thorne JE, Newcomb CW, et al. Mycophenolate mofetil for ocular inflammation. Am J Ophthalmol. 2010;149(3). doi:10.1016/j.ajo.2009.09.026
52. Ozzello DJ, Kolfenbach JR, Palestine AG. Uveitis specialists and rheumatologists select different therapies for idiopathic non-necrotizing anterior scleritis. Ophthalmol Ther. 2016;5(2):245–252. doi:10.1007/s40123-016-0067-1
53. Pasadhika S, Kempen JH, Newcomb CW, et al. Azathioprine for ocular inflammatory diseases. Am J Ophthalmol. 2009;148(4). doi:10.1016/j.ajo.2009.05.008
54. Kaçmaz RO, Kempen JH, Newcomb C, et al. Cyclosporine for ocular inflammatory diseases. Ophthalmology. 2010;117(3):576–584. doi:10.1016/j.ophtha.2009.08.010
55. Brown JE, Thomas AS, Armbrust KR, Boyd K, Berkenstock M, Kopplin LJ. Therapeutic outcomes of non-infectious scleritis treated with tumor necrosis factor-alpha inhibitors. Ocul Immunol Inflamm. 2024;32(6):1017–1023. doi:10.1080/09273948.2023.2191712
56. Fabiani C, Sota J, Sainz-De-La-Maza M, et al. Effectiveness of TNF-α blockade in the treatment of refractory non-infectious scleritis: a multicentre study. Clin Exp Rheumatol. 2020;38:1138–1144.
57. Gaujoux-Viala C, Giampietro C, Gaujoux T, et al. Scleritis: a paradoxical effect of etanercept? Etanercept-associated inflammatory eye disease. J Rheumatol. 2012;39(2):233–239. doi:10.3899/jrheum.110865
58. Li J, Zhang Z, Wu X, Zhou J, Meng D, Zhu P. Risk of adverse events after anti-TNF treatment for inflammatory rheumatological disease. a meta-analysis. Front Pharmacol. 2021;12:746396. doi:10.3389/fphar.2021.746396
59. Suhler EB, Lim LL, Beardsley RM, et al. Rituximab therapy for refractory scleritis: results of a phase I/II dose-ranging, randomized, clinical trial. Ophthalmology. 2014;121(10):1885–1891. doi:10.1016/j.ophtha.2014.04.044
60. Cao JH, Oray M, Cocho L, Foster CS. Rituximab in the treatment of refractory noninfectious scleritis. Am J Ophthalmol. 2016;164:22–28. doi:10.1016/j.ajo.2015.12.032
61. Silpa-archa S, Oray M, Preble JM, Foster CS. Outcome of tocilizumab treatment in refractory ocular inflammatory diseases. Acta Ophthalmol. 2016;94(6):e400–e406. doi:10.1111/aos.13015
62. Doctor M, Murthy SI, Rajasekhar L. Tocilizumab in recalcitrant bilateral scleritis in a case of relapsing polychondritis: a 17-year follow up. Ocul Immunol Inflamm. 2023;31(4):870–873. doi:10.1080/09273948.2022.2058555
63. Fabiani C, Sota J, Sainz-De-La-Maza M, et al. New potential weapons for refractory scleritis in the era of targeted therapy. Mediators Inflamm. 2020;2020:8294560. doi:10.1155/2020/8294560
64. Poelman HJ, Van Daele PLA, Rothova A. Successful tocilizumab treatment for scleritis. Ocul Immunol Inflamm. 2020;28(2):285–287. doi:10.1080/09273948.2019.1617885
65. Tode J, Zeuner R, Saeger M, Roider J, Nölle B. Tocilizumab and steroid boli for treatment-resistant anterior necrotizing scleritis. Acta Ophthalmol. 2015;93(8):e683–e684. doi:10.1111/aos.12720
66. Zhukova JV, Lopatnikova JA, Alshevskaya AA, Sennikov SV. Molecular mechanisms of regulation of IL-1 and its receptors. Cytokine Growth Factor Rev. 2024;80:59–71. doi:10.1016/j.cytogfr.2024.09.004
67. Bottin C, Fel A, Butel N, et al. Anakinra in the treatment of patients with refractory scleritis: a pilot study. Ocul Immunol Inflamm. 2018;26(6):915–920. doi:10.1080/09273948.2017.1299869
68. Knickelbein JE, Tucker WR, Bhatt N, et al. Gevokizumab in the treatment of autoimmune non-necrotizing anterior scleritis: results of a phase I/II clinical trial. Am J Ophthalmol. 2016;172:104–110. doi:10.1016/j.ajo.2016.09.017
69. Benucci M, Bernardini P, Coccia C, et al. JAK inhibitors and autoimmune rheumatic diseases. Autoimmun Rev. 2023;22(4):103276. doi:10.1016/j.autrev.2023.103276
70. Vitale A, Palacios-Olid J, Caggiano V, et al. Efficacy and safety of Janus kinase inhibitors in non-infectious inflammatory ocular diseases: a prospective cohort study from the international AIDA network registries. Front Med. 2024;11. doi:10.3389/fmed.2024.1439338
71. Xie X, Jiang P, Li X, Ru J. The sequential therapy for non-infectious scleritis: a case report. SAGE Open Med Case Rep. 2025;13. doi:10.1177/2050313X251346047.
72. Yuge K, Yawata N, Asahara K, Yamana S, Ono N, Sonoda KH. Successful treatment of tofacitinib-refractory scleritis associated with multiple systemic inflammatory diseases using upadacitinib. Immunol Med. 2025;1–9. doi:10.1080/25785826.2025.2588918
73. Dutta Majumder P, Abraham S, Sudharshan S, Janarthanan M, Ramanan AV. Tofacitinib for refractory uveitis and scleritis in children: a case series. Ocul Immunol Inflamm. 2024;32(9):2092–2095. doi:10.1080/09273948.2024.2323671
74. Vidic Krhlikar N, Tomsic M, Jaki Mekjavic P, et al. Janus kinase inhibitors and their use in non-infectious orbital inflammatory disorders: new treatment possibilities? A case series. Orbit. 2025;44(4):465–469. doi:10.1080/01676830.2024.2430356
75. Kim CY, Lee EB, Youn Oh J. Long-term outcome of tofacitinib treatment for systemic autoimmune disease-associated refractory scleritis. Ocul Immunol Inflamm. 2025;33(1):149–153. doi:10.1080/09273948.2024.2359001
76. Sharma S, Kharel R, Parajuli S, Jha S. Rise of biologics in noninfectious uveitis: a retrospective cohort study from Nepal. Ann Med Surg. 2023;85(5):1486–1489. doi:10.1097/MS9.0000000000000546
77. Baquet-Walscheid K, Heinz C, Heiligenhaus A. Beneficial effect of upadacitinib in a refractory course of scleritis: a case report. Ocul Immunol Inflamm. 2024;32(6):1076–1078. doi:10.1080/09273948.2022.2145488
78. Pyare R, Dutta Majumder P, Shah M, Kaushik V, Agarwal M, Biswas J. Tofacitinib in scleritis: a case series. Ocul Immunol Inflamm. 2024;32(6):884–890. doi:10.1080/09273948.2022.2113805
79. Xu Q, He L, Yin Y. Risk of herpes zoster associated with JAK inhibitors in immune-mediated inflammatory diseases: a systematic review and network meta-analysis. Front Pharmacol. 2023;14:1241954. doi:10.3389/fphar.2023.1241954
80. Pujari SS, Kempen JH, Newcomb CW, et al. Cyclophosphamide for ocular inflammatory diseases. Ophthalmology. 2010;117(2):356–365. doi:10.1016/j.ophtha.2009.06.060
81. Karaca I, Tran EM, Park SW, et al. Intravenous cyclophosphamide therapy for patients with severe ocular inflammatory diseases who failed other immunomodulatory therapies. J Ophthalmic Inflamm Infect. 2024;14(1). doi:10.1186/s12348-023-00372-z
82. Goldstein DA, Fontanilla FA, Kaul S, Sahin O, Tessler HH. Long-term follow-up of patients treated with short-term high-dose chlorambucil for sight-threatening ocular inflammation. Ophthalmology. 2002;109:370–377. doi:10.1016/s0161-6420(01)00942-3
83. Sangwan VS, Jain V, Gupta P. Structural and functional outcome of scleral patch graft. Eye. 2007;21(7):930–935. doi:10.1038/sj.eye.6702344
84. Sun MJ, Rosner BA, Newcomb CW, et al. Incidence and outcome of cataract in eyes with scleritis and episcleritis. Ocul Immunol Inflamm. 2025;33(7):1227–1234. doi:10.1080/09273948.2025.2453878
85. Armbrust KR, Kopplin LJ. Cataract surgery in patients with scleritis in the United States: an IRIS Registry (Intelligent Research in Sight) analysis. Cornea. 2025. doi:10.1097/ICO.0000000000003949
86. Palkar A, Sudharshan S, George AE, Ganesh SK, Biswas J, Dutta Majumder P. Cataract surgery in the setting of scleritis. Ocul Immunol Inflamm. 2021;29(7–8):1540–1543. doi:10.1080/09273948.2020.1754434
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.