Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 9 » Issue 1
Update on the pathological processes, molecular biology, and clinical utility of N-acetylcysteine in chronic obstructive pulmonary disease
Received 27 April 2014
Accepted for publication 21 June 2014
Published 6 August 2014 Volume 2014:9(1) Pages 825—836
DOI https://doi.org/10.2147/COPD.S51057
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Hoi Nam Tse, Cee Zhung Steven Tseng
Medical and Geriatric Department, Kwong Wah Hospital, Hong Kong Special Administrative Region
Abstract: Chronic obstructive pulmonary disease (COPD) is a common and morbid disease characterized by high oxidative stress. Its pathogenesis is complex, and involves excessive oxidative stress (redox imbalance), protease/antiprotease imbalance, inflammation, apoptosis, and autoimmunity. Among these, oxidative stress has a pivotal role in the pathogenesis of COPD by initiating and mediating various redox-sensitive signal transduction pathways and gene expression. The protective physiological mechanisms of the redox balance in the human body, their role in the pathogenesis of COPD, and the clinical correlation between oxidative stress and COPD are reviewed in this paper. N-acetylcysteine (NAC) is a mucolytic agent with both antioxidant and anti-inflammatory properties. This paper also reviews the use of NAC in patients with COPD, especially the dose-dependent properties of NAC, eg, its effects on lung function and the exacerbation rate in patients with the disease. Earlier data from BRONCUS (the Bronchitis Randomized on NAC Cost-Utility Study) did not suggest that NAC was beneficial in patients with COPD, only indicating that it reduced exacerbation in an "inhaled steroid-naïve" subgroup. With regard to the dose-dependent properties of NAC, two recent randomized controlled Chinese trials suggested that high-dose NAC (1,200 mg daily) can reduce exacerbations in patients with COPD, especially in those with an earlier (moderately severe) stage of disease, and also in those who are at high risk of exacerbations. However, there was no significant effect on symptoms or quality of life in patients receiving NAC. Further studies are warranted to investigate the effect of NAC at higher doses in non-Chinese patients with COPD.
Keywords: N-acetylcysteine, antioxidant, anti-inflammatory, chronic obstructive pulmonary disease
Pathological processes underlying COPD
Chronic obstructive pulmonary disease (COPD) is a chronic inflammatory disease characterized by progressive, partially reversible airflow limitation. It is associated with both airway and extrapulmonary inflammation, as indicated by increased reactive oxygen species (ROS) levels and proinflammatory markers in peripheral blood. COPD manifests as a spectrum of overlapping phenotypes, including chronic bronchitis, emphysema,1 small airway disease,2,3 and frequent exacerbations.4 Despite differences in pathology, these phenotypes share many common but complex pathogenetic processes, including inflammation, excessive oxidative stress, protease/antiprotease imbalance, apoptosis, and autoimmunity.5–8
Various inflammatory cells, epithelial cells, mediators, and cytokines have been implicated in the pathogenesis of COPD.5 On exposure to toxins and smoke, epithelial cells generate chemotactic mediators and cytokines that subsequently recruit various inflammatory cells, resulting in lung damage.9 Earlier studies showed that inflammatory cell levels were closely correlated with the severity of COPD. For instance, CD8 counts are closely correlated with the severity of pulmonary dysfunction,10–12 while macrophages and neutrophils are elevated in patients with severe COPD.13 Cytotoxic CD8 T-cells release granzyme and perforin, which cause apoptosis and damage to the lung parenchyma directly, and also release interleukin (IL)-3 and IL-4, which induce mucus hypersecretion in the airways.14,15 Macrophage/neutrophils also play an important role by releasing an array of proinflammatory cytokines, such as IL-8, tumor necrosis factor alpha,16,17 and proteinases, which result in inflammation as well as direct destruction of the lung parenchyma.
In addition, there is strong evidence that proteases make a critical contribution to the pathogenesis of COPD. Apart from the well known alpha-1 protease, another focus is the families of metalloproteinases such as matrix metalloproteinase (MMP) and A Disintegrin And Metalloproteases (ADAM), as well as their inhibitors.18,19 MMPs are a family of zinc-dependent endopeptidases that degrade the protein components of the extracellular matrix; their proteolytic activity is important for tissue remodeling and normal body homeostasis.
Macrophages/neutrophils play an important role by releasing not only MMPs but also proinflammatory cytokines that control the activity of MMPs. An imbalance of metalloproteases/antimetalloproteases may cause destruction of the lung parenchyma and development of emphysema.20 A wide variety of MMPs has been identified, and their polymorphisms have significant implications in the pathogenesis of COPD. For instance, MMP12 plays a key role, since it has been shown that MMP12-deficient mice are protected from the pathological changes of emphysema and COPD after prolonged exposure to cigarette smoke.21
Role of oxidative stress in COPD: physiological role of glutathione
Oxidative stress has a pivotal role in the pathogenesis of COPD by initiating and mediating various types of redox-sensitive signal transduction and gene expression, resulting in most of the aforementioned inflammatory processes.5,22–25 Patients with COPD have high levels of oxidative stress and diminished circulating levels of antioxidants,23,25,26 although these can be partially restored by abstinence from tobacco smoking.23 The overwhelming oxidative stress has a detrimental effect on lung function in patients with COPD, as demonstrated by a significant positive correlation between forced expiratory volume in one second (FEV1) and antioxidant levels (including glutathione peroxidase in erythrocytes and the ferric ion-reducing antioxidant power in plasma).25 Moreover, lower antioxidant levels were also associated with a more severe type of COPD as well as a history of exacerbations of COPD.26 Further, patients with COPD also have redox-mediated vascular dysfunction, which may be an important mechanism contributing to their higher risk of cardiovascular disease.27 It was shown that the higher levels of oxidative stress and vascular dysfunction in patients with COPD could be mitigated by an oral antioxidant, as evidenced by an improvement in the carotid–radial pulse wave velocity with antioxidant treatment.27
With regard to the pathogenesis of COPD, the lungs are constantly and inevitably exposed to various oxidants in the form of ROS, eg, the superoxide anion (O2–), hydroxyl radical (OH−), hydrogen peroxide (H2O2), and reactive nitrogen species.28–30 These oxidants are generated constantly at the cellular level by metabolism in the mitochondria and inflammatory cells via ROS/reactive nitrogen species-generating enzymes (nicotinamide adenine dinucleotide phosphate oxidase, xanthine/xanthine oxidase, heme peroxidases, and nitric oxide synthase).31 Further, cigarette smoke, which contains an estimated 1015–1017 oxidants/free radicals per puff,32 together with air pollution, constitutes the major exogenous source of oxidants and further augments oxidative stress in the body. These oxidants are important in initiating various signal transductions in the inflammatory response, attracting more ROS-generating inflammatory cells that further perpetuate the inflammatory response in patients with COPD. Generation of ROS is also directly associated with oxidative modification of proteins, carbohydrates, lipids, and DNA. These carbonyl proteins (reactive aldehydes) further impose oxidative stress and cause various inflammatory and immune responses. Previous studies have demonstrated that levels of 4-hydroxynonenal, a lipid peroxidation product, are elevated in the airways and alveolar epithelial cells of patients with COPD, and the 4-hydroxynonenal level correlated well with the severity of lung dysfunction.33
Endogenous antioxidant defense systems are crucial in order to maintain redox balance. Glutathione, a major cellular thiol antioxidant and redox cycler, is concentrated in the epithelial lining fluid and has a protective role in maintaining the integrity of the airspaces.34 Glutathione exerts its antioxidant effect by donating its reducing equivalents/electron transfer in cells, leading to formation of its oxidized (disulfide) form, which is recycled back to glutathione by glutathione reductase. Further, a number of enzymes also have a protective role. For instance, aldehyde dehydrogenase and aldo-keto reductase can detoxify reactive aldehydes, while other antioxidant enzymes, such as extracellular superoxide dismutase, glutathione S-transferase, and glutamate cysteine ligase, were shown to attenuate cigarette smoke-induced lung inflammation and elastase-induced emphysema.35
However, excessive oxidative stresses will deplete the body’s antioxidant capacity, resulting in an imbalance of the redox system. Overwhelming oxidative stresses can activate various proinflammatory proteins by initiating pathways at the transcription level:5
- Nuclear factor kappa B (NF-κB) is a redox-sensitive transcription factor of paramount importance in the inflammatory response in patients with COPD by regulating proinflammatory genes, resulting in a release of proinflammatory mediators such as IL-1, IL-6, IL-8, and tumor necrosis factor alpha.36 NF-κB transcription factor could be activated by a number of “oxidant-sensitive” pathways,37 both canonical and noncanonical.5
- Histone deacetylase (HDAC), especially HDAC2, can deacetylate histone protein and NF-kB, causing condensation of DNA, and slow down gene transcription. It can therefore attenuate the NF-κB-dependent inflammatory responses and is beneficial to the body.38 Moreover, HDAC2 can increase glucocorticoid sensitivity by deacetylating glucocorticoid receptors.39 Moreover, another HDAC, sirtuin 1, can deacetylate transcription factors like forkhead box class (FOXO3) and p53,40 thereby regulating cell cycle arrest, apoptosis, and cellular senescence. Sirtuin 1 also increases production of nitric oxide and improves endothelial cell function as well as vasorelaxation by deacetylating lysine in nitric oxide synthase.41 Despite the beneficial functions of HDACs, their levels are substantially reduced in patients with COPD, as reported previously.42
- Nuclear erythroid-related factor 2 (Nrf2) is a cytoplasmic transcription factor playing a protective role against excessive oxidative stress and inflammatory responses in COPD.43 Upon activation by ROS, Nrf2 exerts a protective effect by detachment from its inhibitor (kelch-like ECH-associated protein 1) and then translocating into the nucleus, inducing and upregulating various antioxidant and cytoprotective genes like glutathione peroxidase and heme oxygenase 1.43 The Nrf2 pathway can be promoted by enhancing the stabilizer of Nrf2 (DJ-1) and inhibited by post-translational carbonyl modifications of Nrf2.44–46 In patients with COPD, there is a significant reduction in Nrf2 levels along with its associated excessive oxidative stress and protein carbonyls, which can also alter the function and stability of intracellular proteins like Nrf2, kelch-like ECH-associated protein 1, and HDAC, inducing lung and systemic inflammatory responses.47,48
Efficacy of antioxidant supplementation in preventing progression of COPD
Dietary antioxidant supplements such as vitamin C, vitamin E, and beta-carotene, which boost the antioxidant reserve, may have a potential role in the treatment of patients with COPD. Previous epidemiological studies in the general population suggest that a high intake of dietary antioxidants protects lung function (FEV1 and forced vital capacity)49,50 and results in a lower prevalence of chronic bronchitis and dyspnea.51 In a cross-sectional study in the general population, an increase of 20 mmol/L in plasma vitamin C concentration was associated with a 13% reduction in risk of obstructive airway disease (odds ratio 0.87), indicating that vitamin C has a protective role against obstructive airway disease.52 Moreover, n-3 polyunsaturated fatty acids, principally eicosapentaenoic acid and docosahexaenoic acid, which are known to interfere with the body’s inflammatory response, were inversely related to the risk of chronic bronchitis, physician-diagnosed emphysema, and COPD detected by spirometry.52
Polyphenols, another dietary supplement, were also demonstrated to be beneficial in patients with COPD.53 In an epidemiological study, polyphenols such as catechin (eg, green tea, epigallocatechin gallate), flavonol, and flavone were positively associated with FEV1 and inversely associated with COPD symptoms, suggesting a beneficial effect of a high fruit and catechin intake in COPD.54–56 Moreover, the flavonoid resveratrol, a constituent of red wine, was shown to induce synthesis of glutathione57,58 and inhibit inflammatory cytokines from macrophages in patients with COPD.59,60 Another polyphenol, curcumin, has also been shown to inhibit the inflammatory response by inhibiting activation of NF-kB61 and recruitment of neutrophils in the lung.58
Apart from these dietary antioxidant supplements, thiols are the other major potential compounds for treatment of COPD. In addition to having a mucolytic action, thiols can restore the redox imbalance by interacting with the electrophilic groups on free radicals. Apart from the commonly used thiols “NAC” which will be discussed in the Rationale and clinical utility of N-acetylcysteine in COPD section, novel thiols such as carbocisteine, erdosteine, and fudosteine have been developed for their better bioavailability and therapeutic efficacy. For instance, carbocisteine at a dose of 1,500 mg daily for one year was shown to decrease exacerbations and improve quality of life in patients with COPD in the PEACE (Effect of carbocisteine on acute exacerbation of chronic obstructive pulmonary disease) study.62 Another novel thiol, erdosteine (300 mg twice daily), was found to reduce exacerbations, shorten hospitalization time, and improve health-related quality of life in the EQUALIFE (Erdosteine on Quality of Life) study.63,64 At this dose, erdosteine was effective in reducing blood ROS levels in patients with COPD.65 Finally, fudosteine shows better bioavailability than NAC and reduces mucus secretion by inhibiting MUC5AC gene expression.66 Other potential therapeutic agents that are under development include Nrf2 activators, spin traps, redox sensor inhibitors, polyphenols, and enzyme mimetics, the details of which are beyond the scope of the current review.67,68
Rationale and clinical utility of N-acetylcysteine in COPD
Mucolytic effects
NAC, a mucolytic agent with both antioxidant and anti-inflammatory properties, may be beneficial in patients with COPD. It contains a free thiol group that breaks the disulfide bond in the mucin monomer, resulting in depolymerization of mucin oligomers and thereby reducing the viscosity of mucus.69–71 Moreover, it has a mucoregulatory effect, which inhibits mucus secretory cell hyperplasia and enhances expression of the MUC5AC gene.72
Antioxidative and anti- inflammatory effects
NAC also exerts its antioxidant effect by acting directly as a ROS scavenger as well as a precursor of reduced glutathione. NAC restores cellular redox status and modulates the inflammatory pathway in COPD by inhibiting redox-sensitive cell signal transduction and proinflammatory gene expression.73 In a mouse model, NAC was demonstrated to reduce cigarette smoke-induced loss of pulmonary glutathione.74 Moreover, oral NAC has been shown to affect the body’s redox balance by increasing plasma glutathione levels as well as lung lavage glutathione levels in patients with COPD.75 Oral NAC could also reduce ROS production by alveolar macrophages as well as reduce exhaled H2O2 in patients with stable COPD.76
Data on the anti-inflammatory activity of NAC in patients with COPD are limited, but there is in vitro evidence demonstrating that NAC could reduce cigarette smoke-induced abnormalities in polymorphonuclear leukocytes,77 and in alveolar macrophages, fibroblasts, and epithelial cells.78 NAC was also shown to reduce secretory cell hyperplasia and airway wall thickening in a rat model.79
NAC can attenuate a number of inflammatory markers as well as the chemotaxis response in patients with elevated oxidative stress, including chronic smokers and patients with COPD. A 2-week course of NAC (600 mg/day) was shown to increase neutrophil glutathione content and decreased neutrophil chemotaxis in health volunteers. In a study of healthy smokers, administration of NAC at a dose of 200 mg three times daily for 8 weeks reduced the plasma myeloperoxidase and elastase content, decreased lactoferrin and eosinophil cationic protein levels in bronchoalveolar lavage, and attenuated the chemotactic activity of neutrophils.80 The anti-inflammatory effect of NAC in patients with COPD had been demonstrated in a study by Van Overveld et al,81 where chronic use of oral NAC at a dose of 600 mg/day for 10 months reduced neutrophil chemoattractant properties in the sputum of patients with COPD. Moreover, a decrease in exhaled H2O2 level was observed in patients with COPD treated with long-term NAC (600 mg daily for 9–12 months).76
Dose-dependent effect of NAC
Nevertheless, the antioxidative and anti-inflammatory effects of NAC are dose-dependent.73 As a result of the low bioavailability of the drug (6%–10% in humans), a higher dosage is needed for NAC to exert its anti-inflammatory effect. Moreover, there is evidence suggesting that increasing the dose of NAC can increase its bioavailability and reduce the time taken to reach maximal concentrations in plasma.82
The insufficiency of low-dose NAC was demonstrated in a study by Cotgreave and Moldeus,83 in which low-dose NAC (600 mg daily) did not change cysteine and glutathione levels in bronchoalveolar lavage from normal subjects. Similarly, Bridgeman et al84 confirmed that plasma glutathione levels increased in patients with COPD after 5 days of high-dose NAC (600 mg three times daily), but no effect was seen at a low dosage (600 mg daily). Further, while high-dose NAC (1,200 mg daily) effectively reduced exhaled H2O2 (a source of oxidative stress) in patients with stable COPD, there was no effect on exhaled H2O2 with 6 months of low-dose NAC (600 mg daily).85 Kasielski and Nowak76 suggested that low-dose NAC (600 mg daily) may reduce H2O2 levels over 9–12 months, but not over 6 months, implying that a longer treatment duration is needed for low-dose NAC to take effect.
Effect of NAC on lung function
Previous studies failed to demonstrate the beneficial effect of NAC on lung function in patients with COPD. In an older observational survey, patients with COPD on long-term NAC treatment had a lower decline in FEV1 compared with a reference group, especially in older patients (yearly decline of 30 mL versus 54 mL).86 However, this positive effect of NAC on lung function was not reproduced in later randomized trials. BRONCUS (the Bronchitis Randomized on NAC Cost-Utility Study) was a large, 3-year trial87 that used FEV1 as the primary outcome parameter and suggested that NAC 600 mg daily was ineffective in preventing the decline of lung function in patients with COPD. Moreover, a systematic review by Poole et al88 suggested that mucolytics did not result in clinically significant improvement in lung function.
In spite of this, NAC had been proposed to have a beneficial role in small airway function as well as in reduction of lung hyperinflation in patients with COPD.89 In HIACE (the Effect of High Dose N-acetylcysteine on Air Trapping and Airway Resistance of Chronic Obstructive Pulmonary Disease – a Double-blinded, Randomized, Placebo-controlled Trial),90 NAC at a daily dose of 1,200 mg was shown to improve forced expiratory flow 25% to 75% (FEF25%–75%) and forced oscillation technique parameters, including “resonance frequency (Fres), frequency dependency (FDep) and reactance and resistance at low oscillation frequency (X6 Hz and R6 Hz), but no significant effect on FEV1”. The authors suggested that this might be attributable to the fact that forced oscillation technique parameters (Fres, FDep, X6 Hz, and R6 Hz) are superior to FEV1 in assessment of small airway function,91,92 and it was suggested that these forced oscillation technique parameters could detect early small airways disease in susceptible individuals, such as smokers, even when routine pulmonary function parameters (eg, FEV1) were still within normal range.93,94 Further, the effect of NAC in the small airways could be indirectly evidenced by a reduction in air trapping. For instance, secondary analysis of the BRONCUS study87 suggested that NAC has a beneficial role in lung hyperinflation, and the trial by Stav and Raz indicated that NAC at a higher dose (1,200 mg daily) could reduce air trapping at 12 weeks, as manifested by an increase in post-exercise inspiratory capacity and functional residual capacity as well as a reduction in residual volume/total lung capacity ratio.95
This improvement in small airways function may be the result of the antioxidative and anti-inflammatory effect of NAC on the small airways, resulting in a decrease of epithelial thickening, reduction in secretory cell hyperplasia,79 and a decrease in mucus plugging in the small airways.89 Further, NAC could reduce the elastase and attenuate the degree of emphysema in patients with COPD, resulting in less air trapping.96–98
Effect of NAC in COPD exacerbation
A number of randomized controlled trials have investigated the effect of NAC in patients with COPD, but have yielded conflicting results87,90,99–107 (Table 1). Earlier studies and systematic reviews88–110 suggested a beneficial role of mucolytics in reducing COPD exacerbations. The systematic review by Poole et al88 concluded that oral mucolytics could reduce exacerbations in patients with COPD/chronic bronchitis by 0.48 episodes per patient-year, with a higher likelihood of these patients being exacerbation-free (odds ratio 1.84; 95% confidence interval 1.63–2.07) when compared with those treated with placebo.
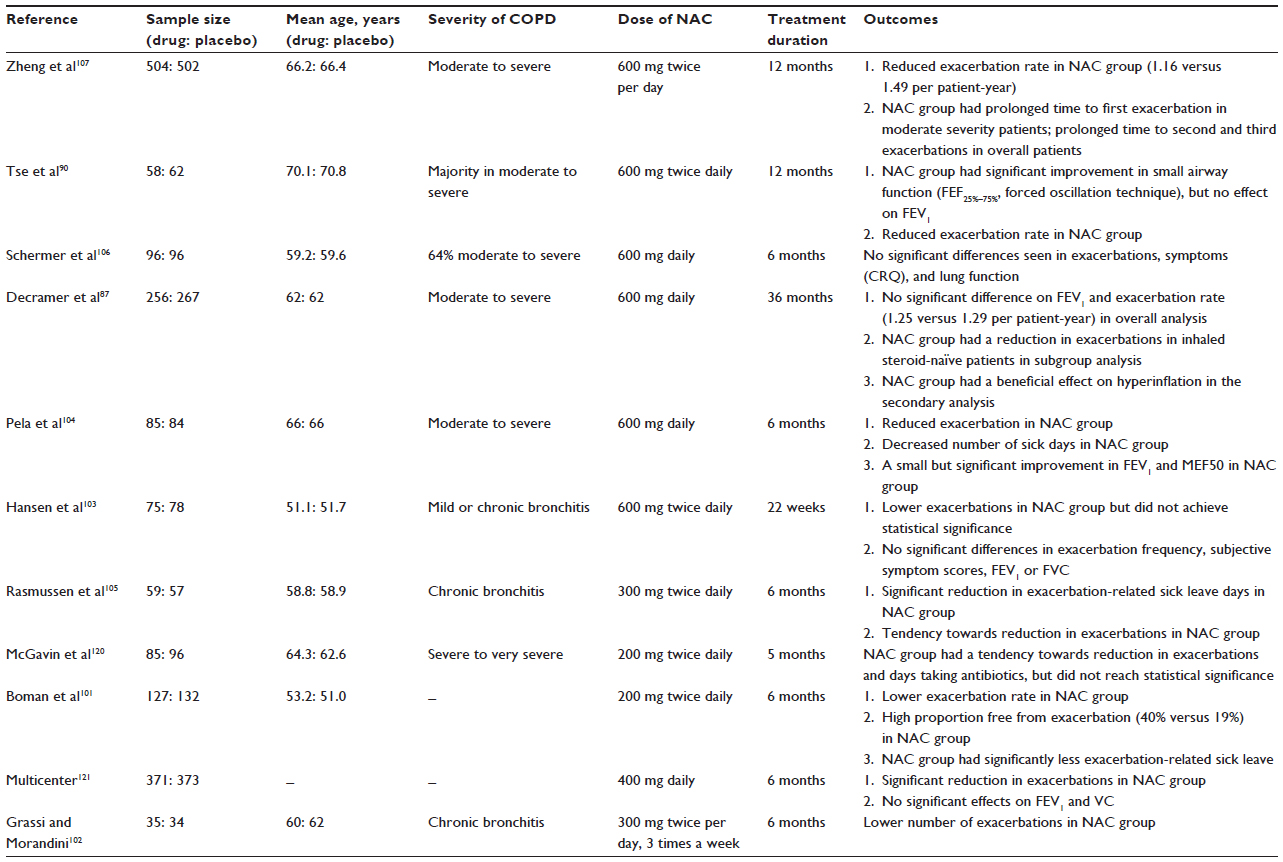 | Table 1 Randomized controlled trials of N-acetylcysteine in patients with COPD |
However, the large 3-year BRONCUS study87 failed to demonstrate that NAC (600 mg daily) was beneficial in terms of improving FEV1 or reducing the exacerbation frequency in patients with COPD, although it did suggest that NAC could reduce exacerbations in a subgroup of “inhaled steroid-naïve” patients with COPD and achieve a significant reduction in hyperinflation in patients with COPD on secondary analysis. In contrast, the randomized, multicenter PEACE study by Zheng et al62 in Chinese patients with COPD, using another mucolytic at a higher dose (carbocisteine 1,500 mg daily), did show a significant reduction in exacerbation rate in the mucolytic-treated group when compared with the placebo-treated group (1.01 versus 1.35, respectively; odds ratio 0.75, P=0.004).
This discrepancy may be attributable to the insufficient dose of NAC used in the previous trials. In vitro and in vivo studies suggested that NAC could only exert its antioxidant effect at a low dose (less than 600 mg), while a larger dose (1,200 mg or above) was need to exert its anti-inflammatory properties.73
Recently, the use of high-dose NAC (1,200 mg or above) in COPD exacerbations has been studied in a number of clinical trials. In the HIACE study,90 chronic use of high-dose NAC (1,200 mg daily for one year) reduced the COPD exacerbation rate (0.96 versus 1.71 exacerbations per year) in Chinese patients with COPD when compared with placebo, and there was also a higher proportion of patients with COPD who remained exacerbation-free in the NAC group at the end of the trial (53.8% versus 37.5%; P=0.088). PANTHEON (the Placebo-controlled study on efficAcy and safety of N-AcetylcysTeine High dose in Exacerbations of chronic Obstructive pulmoNary disease), a large, multicenter, one-year trial107 conducted in Chinese patients with moderate to severe COPD, clearly demonstrated that high-dose NAC (1,200 mg daily) could reduce the frequency of exacerbations (1.16 versus 1.49; odds ratio 0.78, P=0.0011) and prolong the time to second and third exacerbations in the NAC group when compared with the placebo group, with the beneficial effect being more prominent in those with moderate COPD than in those with severe COPD.
Exacerbation of COPD is multifactorial (Table 2). NAC may contribute to a reduction in exacerbation frequency by acting at a number of target sites. It exerts its mucolytic function by reducing the viscosity of sputum and its secretion in the airways, which is important given that viscous sputum, together with consistently inflamed ciliated epithelial cells in the airways, are the preferred sites for bacterial attachment. NAC could further inhibit the attachment of bacteria to the epithelium by disrupting the bacterial receptor sites on the epithelial surface and in mucus.111,112 Patients with COPD have overexpression of adhesion molecules (eg, intercellular adhesion molecule-1, which causes excessive transmigration of neutrophils). It was shown in an in vitro study that NAC could exert its anti-inflammatory effect by inhibiting cytokines that stimulated IL-8 and intercellular adhesion molecule-1 in endothelial and epithelial cells.113
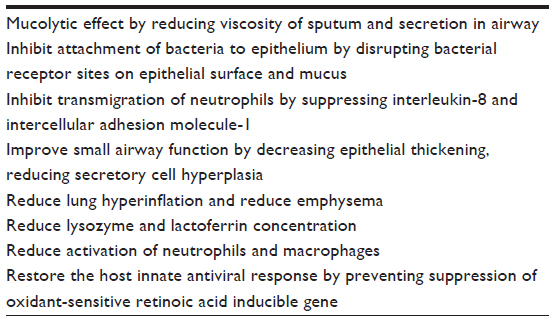 | Table 2 Proposed mechanisms for N-acetylcysteine to reduce exacerbations of chronic obstructive pulmonary disease |
In addition, the antioxidative and anti-inflammatory properties of NAC play a salient role by attenuating chronic inflammation in the airway, improving small airways function, and decreasing air trapping.87,90,95 A recent small pilot study also showed that a short course of NAC 1,200 mg/day can enhance the bronchodilator reversibility potential of antimuscarinic agents.114
Other effects of NAC that have been demonstrated include reduction of lysozyme and lactoferrin concentrations in smokers,115 reduction in the activation and number of neutrophils and macrophages in the bronchoalveolar lavage of smokers,80 and inhibition of adherence of bacteria to ciliated epithelial cells in vitro.116 Last but not least, NAC may also have a role in the host innate immune viral-mediated retinoic acid inducible gene (RIG-I), which is an important pattern recognition receptor for initiating the antiviral response to influenza. NAC, in a dose-related manner, was able to restore the antiviral response by preventing suppression of oxidant-sensitive RIG-1.117
Effect of NAC on symptoms and quality of life
Although NAC may have a beneficial effect in reducing exacerbations, its role in improving symptoms and quality of life has been unclear in patients with COPD. Earlier systematic review suggested that mucolytics improved symptoms in patients with chronic bronchitis,110 but a subsequent meta-analysis suggested that NAC had no significant effect on quality of life.88 Likewise, in the large BRONCUS trial,87 NAC (600 mg daily) did not improve results on the St George’s Respiratory Questionnaire (SGRQ) over a 3-year period. In contrast, the recent PANTHEON study,107 with its larger sample size (n=1,006) and a higher dose of NAC (1,200 mg daily) demonstrated that chronic use of high-dose NAC could significantly improve the isolated “symptom domain” on the SGRQ (−3.37, P=0.043) in Chinese patients with COPD over one year, albeit without reaching the minimum clinically important difference.
Patient-specific considerations
It has been suggested that NAC, especially at a high dose, could have a beneficial role in patients with COPD. However, COPD is a heterogeneous disease with a spectrum of overlapped phenotypes, so further analysis is necessary to delineate the particular group of patients with COPD who can benefit most from treatment with NAC.
Inhaled steroid-naïve patients
Inhaled corticosteroids (ICS) are anti-inflammatory agents frequently used in patients with COPD. However, concerns had been raised about the concomitant use of ICS and NAC in patients with COPD. The BRONCUS study87 showed that NAC could reduce exacerbations in a subgroup of “inhaled steroid-naïve” patients but had no effect overall in patients with COPD. Similarly, the PEACE study62 demonstrated that another mucolytic agent (carbocisteine 1,500 mg daily) could reduce COPD exacerbations; however, the majority of patients in PEACE were “steroid-naïve” (81.87% in the mucolytic group). The effect of NAC being limited to steroid-naïve patients precludes its wider application in patients with COPD.
Despite this, recent studies have suggested that NAC could be effective in reducing COPD exacerbations, even in patients concomitantly using ICS. The HIACE trial,90 in which the majority of patients were on ICS, demonstrated that NAC (1,200 mg daily) could improve small airways function and reduce exacerbations in patients with COPD. In addition, the PANTHEON study,107 which showed a beneficial effect of NAC (1,200 mg daily) in patients with COPD, confirmed no “interaction” between NAC treatment and “steroid use”. This implies that the beneficial effect of NAC is not confined to steroid-naïve patients but may also apply to those who concomitantly use ICS.
Patients with early stage/moderate COPD
The antioxidative and anti-inflammatory effects of NAC have been proposed to be more important in the early stages of COPD, and might prevent disease progression and development of irreversible damage in the later stages of the disease. The PANTHEON study107 showed that the preventive effect of NAC was more prominent in patients with moderate COPD than in those with severe disease, suggesting that NAC might have a more important role in the early stages of COPD. In PANTHEON, the time to first exacerbation was prolonged in the GOLD (Global Initiative for Chronic Obstructive Lung Disease) stage II (moderate) COPD group (P=0.0126) but not in patients with GOLD III (severe) COPD (P=0.76). Moreover, NAC was more effective in reducing the exacerbation rate in patients with GOLD stage II disease (odds ratio 0.61, 95% confidence interval 0.48–0.77, P<0.0001) than in patients with GOLD stage III disease (odds ratio 0.93, confidence interval 0.76–1.13, P=0.46). However, in the PEACE study,62 no significant interaction was detected between mucolytic (carbocisteine) use and GOLD stage.
Frequent exacerbators
Patients with frequent exacerbations have been identified as a specific phenotype, with poorer quality of life, lower physical activity, a greater chance of recurrent exacerbations, a more rapid functional decline, more comorbid extrapulmonary diseases, and increased hospitalization and mortality rates. They are also at particularly high risk of further exacerbations according to the ECLIPSE (Evaluation of COPD Longitudinally to Identify Predictive Surrogate End-points) study.4
NAC might be particularly effective in this phenotype of patients, who have higher levels of oxidative stress and airways and systemic inflammation. The PANTHEON study107 showed that treatment with NAC (1,200 mg daily) did not affect time to first exacerbation in the overall analysis, but it did significantly prolong time to the second and third exacerbations, implying that NAC mainly prevents recurrent exacerbations and may be more effective in the frequent exacerbator phenotype. Further, in the post hoc analysis of HIACE,118 Chinese subjects with COPD were divided into subgroups according to their exacerbation risk at baseline, as outlined in the 2013 GOLD strategy for classification of risk of exacerbation in patients with COPD. High exacerbation risk (categories C and D) was defined as a history of two or more exacerbations per year and/or FEV1 <50%, while low exacerbation risk (categories A and B) was defined as a history of two exacerbations or fewer per year, FEV1 ≥50%, and no recent hospital admissions due to exacerbations of COPD. This post hoc analysis showed that, for patients at high risk of exacerbation, high-dose NAC (1,200 mg daily) significantly reduced the exacerbation frequency, prolonged the time to first exacerbation, and increased the likelihood of being exacerbation-free at one year compared with placebo, but these beneficial effects of NAC over placebo were not significant in low-risk patients, indicating that NAC may be more effective in patients with a high risk of exacerbation.118
Ethnicity
Unlike previous trials, both the PANTHEON107 and HIACE studies90 were conducted in Chinese patients with COPD. However, ethnicity has been of some concern because the pharmacokinetics may be different between Chinese and Caucasian patients. For instance, it was shown that low-dose theophylline could significantly reduce the time to first exacerbation and improve the SGRQ score in Chinese patients with COPD but not in their Caucasian counterparts.119 As a result, the benefit of NAC in patients with COPD may not be generalized to other ethnic groups. Further research may be needed to elucidate the effect of high-dose NAC in Caucasian patients with COPD.
Adverse effects
NAC is a safe and well tolerated treatment modality in patients with COPD. Previous studies have shown no significant difference in the frequency of adverse effects when compared with placebo. The majority of adverse effects, including gastrointestinal upset and diarrhea, are minor. No mortality attributable to NAC was reported in these studies. Further, chronic use of NAC is well tolerated, even at the higher dosage (1,800 mg daily) used in a study of NAC in the treatment of interstitial lung disease.
Conclusion
NAC has mucolytic, antioxidative, and anti-inflammatory properties, as demonstrated by in vitro and in vivo studies. Although no effect of NAC at a low dosage was apparent in the earlier studies, more recent research suggests that NAC at a higher dosage (1,200 mg daily or above) can reduce exacerbations of COPD and prolong the time to first exacerbation in Chinese patients with COPD, especially those with disease of moderate severity or with the frequent exacerbation phenotype. Further large multicenter studies involving other ethnic groups are warranted to elucidate the effect of high-dose NAC in patients with COPD in general.
Disclosure
The authors report no conflicts of interest in this work.
References
Makita H, Nasuhara Y, Nagai K, et al; Hokkaido COPD Cohort Study Group. Characterisation of phenotypes based on severity of emphysema in chronic obstructive pulmonary disease. Thorax. 2007;62(11):932–937. | |
Patel B, Make B, Coxson HO, et al. Airway and parenchymal disease in chronic obstructive pulmonary disease are distinct phenotypes. Proc Am Thorac Soc. 2006;3(6):533. | |
Hogg JC, Chu F, Utokaparch S, et al. The nature of small-airway obstruction in chronic obstructive pulmonary disease. N Engl J Med. 2004;350(26):2645–2653. | |
Hurst JR, Vestbo J, Anzueto A, et al. Susceptibility to exacerbation in chronic obstructive pulmonary disease. N Engl J Med. 2010;363(12):1128–1138. | |
Yao H, Rahman I. Current concepts on oxidative/carbonyl stress, inflammation and epigenetics in pathogenesis of chronic obstructive pulmonary disease. Toxicol Appl Pharmacol. 2011;254(2):72–85. | |
Toyoshima M, Chida K, Suda T, Sato M. Is autoimmunity really related to the pathogenesis of COPD? Am J Respir Crit Care Med. 2011;184(10):1212–1213. | |
Barbu C, Iordache M, Man MG. Inflammation in COPD: pathogenesis, local and systemic effects. Rom J Morphol Embryol. 2011;52(1):21–27. | |
Cornwell WD, Kim V, Song C, Rogers TJ. Pathogenesis of inflammation and repair in advanced COPD. Semin Respir Crit Care Med. 2010;31(3):257–266. | |
Fuke S, Betsuyaku T, Nasuhara Y, Morikawa T, Katoh H, Nishimura M. Chemokines in bronchiolar epithelium in the development of chronic obstructive pulmonary disease. Am J Respir Cell Mol Biol. 2004;31(4):405–412. | |
Lams BE, Sousa AR, Rees PJ, Lee TH. Subepithelial immunopathology of the large airways in smokers with and without chronic obstructive pulmonary disease. Eur Respir J. 2000;15(3):512–516. | |
O’Shaughnessy TC, Ansari TW, Barnes NC, Jeffery PK. Inflammation in bronchial biopsies of subjects with chronic bronchitis: inverse relationship of CD8+ T lymphocytes with FEV1. Am J Respir Crit Care Med. 1997;155(3):852–857. | |
Saetta M, Di Stefano A, Turato G, et al. CD8+ T-lymphocytes in peripheral airways of smokers with chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 1998;157(3 Pt 1):822–826. | |
Baraldo S, Turato G, Badin C, et al. Neutrophilic infiltration within the airway smooth muscle in patients with COPD. Thorax. 2004;59(4):308–312. | |
Miotto D, Ruggieri MP, Boschetto P, et al. Interleukin-13 and -4 expression in the central airways of smokers with chronic bronchitis. Eur Respir J. 2003;22(4):602–608. | |
Saetta M, Turato G, Maestrelli P, Mapp CE, Fabbri LM. Cellular and structural bases of chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2001;163(6):1304–1309. | |
Daheshia M. Therapeutic inhibition of matrix metalloproteinases for the treatment of chronic obstructive pulmonary disease (COPD). Curr Med Res Opin. 2005;21(4):587–594. | |
Macnee W, Rahman I. Oxidants and antioxidants as therapeutic targets in chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 1999;160(5 Pt 2):S58–S65. | |
Mocchegiani E, Giacconi R, Costarelli L. Metalloproteases/anti-metalloproteases imbalance in chronic obstructive pulmonary disease: genetic factors and treatment implications. Curr Opin Pulm Med. 2011;17 Suppl 1:S11–S19. | |
Churg A, Zhou S, Wright JL. Series “matrix metalloproteinases in lung health and disease”: matrix metalloproteinases in COPD. Eur Respir J. 2012;39(1):197–209. | |
Malemud CJ. Matrix metalloproteinases (MMPs) in health and disease: an overview. Front Biosci. 2006;11:1696–1701. | |
Hautamaki RD, Kobayashi DK, Senior RM, Shapiro SD. Requirement for macrophage elastase for cigarette smoke-induced emphysema in mice. Science. 1997;277(5334):2002–2004. | |
Hassett DJ, Borchers MT, Panos RJ. Chronic obstructive pulmonary disease (COPD): evaluation from clinical, immunological and bacterial pathogenesis perspectives. J Microbiol. 2014;52(3):211–226. | |
Wozniak A, Gorecki D, Szpinda M, Mila-Kierzenkowska C, Wozniak B. Oxidant-antioxidant balance in the blood of patients with chronic obstructive pulmonary disease after smoking cessation. Oxid Med Cell Longev. 2013;2013:897075. | |
Cristovao C, Cristovao L, Nogueira F, Bicho M. Evaluation of the oxidant and antioxidant balance in the pathogenesis of chronic obstructive pulmonary disease. Rev Port Pneumol. 2013;19(2):70–75. | |
Ahmad A, Shameem M, Husain Q. Altered oxidant-antioxidant levels in the disease prognosis of chronic obstructive pulmonary disease. Int J Tuberc Lung Dis. 2013;17(8):1104–1109. | |
Nicks ME, O’Brien MM, Bowler RP. Plasma antioxidants are associated with impaired lung function and COPD exacerbations in smokers. COPD. 2011;8(4):264–269. | |
Ives SJ, Harris RA, Witman MA, et al. Vascular dysfunction and chronic obstructive pulmonary disease: the role of redox balance. Hypertension. 2014;63(3):459–467. | |
Aaron SD, Angel JB, Lunau M, et al. Granulocyte inflammatory markers and airway infection during acute exacerbation of chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2001;163(2):349–355. | |
Gompertz S, Bayley DL, Hill SL, Stockley RA. Relationship between airway inflammation and the frequency of exacerbations in patients with smoking related COPD. Thorax. 2001;56(1):36–41. | |
Pinamonti S, Leis M, Barbieri A, et al. Detection of xanthine oxidase activity products by EPR and HPLC in bronchoalveolar lavage fluid from patients with chronic obstructive pulmonary disease. Free Radic Biol Med. 1998;25(7):771–779. | |
Bindoli A, Fukuto JM, Forman HJ. Thiol chemistry in peroxidase catalysis and redox signaling. Antioxid Redox Signal. 2008;10(9):1549–1564. | |
Church DF, Pryor WA. Free-radical chemistry of cigarette smoke and its toxicological implications. Environ Health Perspect. 1985;64: 111–126. | |
Rahman I, van Schadewijk AA, Crowther AJ, et al. 4-Hydroxy-2-nonenal, a specific lipid peroxidation product, is elevated in lungs of patients with chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2002;166(4):490–495. | |
Cantin AM, North SL, Hubbard RC, Crystal RG. Normal alveolar epithelial lining fluid contains high levels of glutathione. J Appl Physiol (1985). 1987;63(1):152–157. | |
Yao H, Arunachalam G, Hwang JW, et al. Extracellular superoxide dismutase protects against pulmonary emphysema by attenuating oxidative fragmentation of ECM. Proc Natl Acad Sci U S A. 2010;107(35):15571–15576. | |
Christman JW, Sadikot RT, Blackwell TS. The role of nuclear factor-kappa B in pulmonary diseases. Chest. 2000;117(5):1482–1487. | |
Pantano C, Reynaert NL, van der Vliet A, Janssen-Heininger YM. Redox-sensitive kinases of the nuclear factor-kappaB signaling pathway. Antioxid Redox Signal. 2006;8(9–10):1791–1806. | |
Sengupta N, Seto E. Regulation of histone deacetylase activities. J Cell Biochem. 2004;93(1):57–67. | |
Ito K, Ito M, Elliott WM, et al. Decreased histone deacetylase activity in chronic obstructive pulmonary disease. N Engl J Med. 2005;352(19):1967–1976. | |
Yang SR, Chida AS, Bauter MR, et al. Cigarette smoke induces proinflammatory cytokine release by activation of NF-kappaB and posttranslational modifications of histone deacetylase in macrophages. Am J Physiol Lung Cell Mol Physiol. 2006;291(1):L46–L57. | |
Potente M, Dimmeler S. Emerging roles of SIRT1 in vascular endothelial homeostasis. Cell Cycle. 2008;7(14):2117–2122. | |
Rajendrasozhan S, Yang SR, Kinnula VL, Rahman I. SIRT1, an antiinflammatory and antiaging protein, is decreased in lungs of patients with chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2008;177(8):861–870. | |
Kensler TW, Wakabayashi N, Biswal S. Cell survival responses to environmental stresses via the Keap1-Nrf2-ARE pathway. Annu Rev Pharmacol Toxicol. 2007;47:89–116. | |
Goven D, Boutten A, Lecon-Malas V, et al. Altered Nrf2/Keap1-Bach1 equilibrium in pulmonary emphysema. Thorax. 2008;63(10):916–924. | |
Malhotra D, Thimmulappa R, Navas-Acien A, et al. Decline in NRF2-regulated antioxidants in chronic obstructive pulmonary disease lungs due to loss of its positive regulator, DJ-1. Am J Respir Crit Care Med. 2008;178(6):592–604. | |
Suzuki M, Betsuyaku T, Ito Y, et al. Down-regulated NF-E2-related factor 2 in pulmonary macrophages of aged smokers and patients with chronic obstructive pulmonary disease. Am J Respir Cell Mol Biol. 2008;39(6):673–682. | |
Adenuga D, Caito S, Yao H, et al. Nrf2 deficiency influences susceptibility to steroid resistance via HDAC2 reduction. Biochem Biophys Res Commun. 2010;403(3–4):452–456. | |
Mercado N, Thimmulappa R, Thomas CM, et al. Decreased histone deacetylase 2 impairs Nrf2 activation by oxidative stress. Biochem Biophys Res Commun. 2011;406(2):292–298. | |
Britton JR, Pavord ID, Richards KA, et al. Dietary antioxidant vitamin intake and lung function in the general population. Am J Respir Crit Care Med. 1995;151(5):1383–1387. | |
Grievink L, Smit HA, Ocke MC, van ‘t Veer P, Kromhout D. Dietary intake of antioxidant (pro)-vitamins, respiratory symptoms and pulmonary function: the MORGEN study. Thorax. 1998;53(3):166–171. | |
Rautalahti M, Virtamo J, Haukka J, et al. The effect of alpha-tocopherol and beta-carotene supplementation on COPD symptoms. Am J Respir Crit Care Med. 1997;156(5):1447–1452. | |
Sargeant LA, Jaeckel A, Wareham NJ. Interaction of vitamin C with the relation between smoking and obstructive airways disease in EPIC Norfolk. European Prospective Investigation into Cancer and Nutrition. Eur Respir J. 2000;16(3):397–403. | |
Arts IC, Hollman PC. Polyphenols and disease risk in epidemiologic studies. Am J Clin Nutr. 2005;81(Suppl 1):317S–325S. | |
Tabak C, Arts IC, Smit HA, Heederik D, Kromhout D. Chronic obstructive pulmonary disease and intake of catechins, flavonols, and flavones: the MORGEN Study. Am J Respir Crit Care Med. 2001;164(1):61–64. | |
Santus P, Sola A, Carlucci P, et al. Lipid peroxidation and 5-lipoxygenase activity in chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2005;171(8):838–843. | |
Walda IC, Tabak C, Smit HA, et al. Diet and 20-year chronic obstructive pulmonary disease mortality in middle-aged men from three European countries. Eur J Clin Nutr. 2002;56(7):638–643. | |
Kode A, Rajendrasozhan S, Caito S, Yang SR, Megson IL, Rahman I. Resveratrol induces glutathione synthesis by activation of Nrf2 and protects against cigarette smoke-mediated oxidative stress in human lung epithelial cells. Am J Physiol Lung Cell Mol Physiol. 2008;294(3):L478–L488. | |
Biswas SK, McClure D, Jimenez LA, Megson IL, Rahman I. Curcumin induces glutathione biosynthesis and inhibits NF-kappaB activation and interleukin-8 release in alveolar epithelial cells: mechanism of free radical scavenging activity. Antioxid Redox Signal. 2005;7(1–2):32–41. | |
Culpitt SV, Rogers DF, Fenwick PS, et al. Inhibition by red wine extract, resveratrol, of cytokine release by alveolar macrophages in COPD. Thorax. 2003;58(11):942–946. | |
Manna SK, Mukhopadhyay A, Aggarwal BB. Resveratrol suppresses TNF-induced activation of nuclear transcription factors NF-kappa B, activator protein-1, and apoptosis: potential role of reactive oxygen intermediates and lipid peroxidation. J Immunol. 2000;164(12):6509–6519. | |
Shishodia S, Potdar P, Gairola CG, Aggarwal BB. Curcumin (diferuloylmethane) down-regulates cigarette smoke-induced NF-kappaB activation through inhibition of IkappaBalpha kinase in human lung epithelial cells: correlation with suppression of COX-2, MMP-9 and cyclin D1. Carcinogenesis. 2003;24(7):1269–1279. | |
Zheng JP, Kang J, Huang SG, et al. Effect of carbocisteine on acute exacerbation of chronic obstructive pulmonary disease (PEACE study): a randomised placebo-controlled study. Lancet. 2008;371(9629):2013–2018. | |
Moretti M, Bottrighi P, Dallari R, et al. The effect of long-term treatment with erdosteine on chronic obstructive pulmonary disease: the EQUALIFE study. Drugs Exp Clin Res. 2004;30(4):143–152. | |
Moretti M, Marchioni CF. An overview of erdosteine antioxidant activity in experimental research. Pharmacol Res. 2007;55(4):249–254. | |
Dal Negro RW, Visconti M, Micheletto C, Tognella S. Changes in blood ROS, e-NO, and some pro-inflammatory mediators in bronchial secretions following erdosteine or placebo: a controlled study in current smokers with mild COPD. Pulm Pharmacol Ther. 2008;21(2):304–308. | |
Rhee CK, Kang CM, You MB, et al. Effect of fudosteine on mucin production. Eur Respir J. 2008;32(5):1195–1202. | |
Rahman I. Antioxidant therapeutic advances in COPD. Ther Adv Respir Dis. 2008;2(6):351–374. | |
Rahman I. Pharmacological antioxidant strategies as therapeutic interventions for COPD. Biochim Biophys Acta. 2012;1822(5):714–728. | |
Davis SS, Scobie S, Inglis A. The effect of sulphydryl compounds and cross linking agents on the viscous and viscoelastic properties of mucus. Biorheology. 1975;12(3–4):225–232. | |
Sadowska AM. N-Acetylcysteine mucolysis in the management of chronic obstructive pulmonary disease. Ther Adv Respir Dis. 2012;6(3):127–135. | |
Sheffner AL. The reduction in vitro in viscosity of mucoprotein solutions by a new mucolytic agent, N-acetyl-L-cysteine. Ann N Y Acad Sci. 1963;106:298–310. | |
Mata M, Ruiz A, Cerda M, et al. Oral N-acetylcysteine reduces bleomycin-induced lung damage and mucin Muc5ac expression in rats. Eur Respir J. 2003;22(6):900–905. | |
Sadowska AM, Manuel YKB, De Backer WA. Antioxidant and anti-inflammatory efficacy of NAC in the treatment of COPD: discordant in vitro and in vivo dose-effects: a review. Pulm Pharmacol Ther. 2007;20(1):9–22. | |
Moldeus P, Cotgreave IA, Berggren M. Lung protection by a thiol-containing antioxidant: N-acetylcysteine. Respiration. 1986;50 Suppl 1: 31–42. | |
Bridgeman MM, Marsden M, MacNee W, Flenley DC, Ryle AP. Cysteine and glutathione concentrations in plasma and bronchoalveolar lavage fluid after treatment with N-acetylcysteine. Thorax. 1991;46(1):39–42. | |
Kasielski M, Nowak D. Long-term administration of N-acetylcysteine decreases hydrogen peroxide exhalation in subjects with chronic obstructive pulmonary disease. Respir Med. 2001;95(6):448–456. | |
Bridges RB. Protective action of thiols on neutrophil function. Eur J Respir Dis Suppl. 1985;139:40–48. | |
Drost E, Lannan S, Bridgeman MM, et al. Lack of effect of N-acetylcysteine on the release of oxygen radicals from neutrophils and alveolar macrophages. Eur Respir J. 1991;4(6):723–729. | |
Jeffery PK, Rogers DF, Ayers MM. Effect of oral acetylcysteine on tobacco smoke-induced secretory cell hyperplasia. Eur J Respir Dis Suppl. 1985;139:117–122. | |
Eklund A, Eriksson O, Hakansson L, et al. Oral N-acetylcysteine reduces selected humoral markers of inflammatory cell activity in BAL fluid from healthy smokers: correlation to effects on cellular variables. Eur Respir J. 1988;1(9):832–838. | |
van Overveld FJ, Vermeire PA, De Backer WA. Induced sputum of patients with chronic obstructive pulmonary disease (COPD) contains adhesion-promoting, therapy-sensitive factors. Inflamm Res. 2000;49(1):8–13. | |
Borgstrom L, Kagedal B. Dose dependent pharmacokinetics of N-acetylcysteine after oral dosing to man. Biopharm Drug Dispos. 1990;11(2):131–136. | |
Cotgreave IA, Moldeus P. Lung protection by thiol-containing antioxidants. Bull Eur Physiopathol Respir. 1987;23(4):275–277. | |
Bridgeman MM, Marsden M, Selby C, Morrison D, MacNee W. Effect of N-acetyl cysteine on the concentrations of thiols in plasma, bronchoalveolar lavage fluid, and lung tissue. Thorax. 1994;49(7):670–675. | |
De Benedetto F, Aceto A, Dragani B, et al. Long-term oral N-acetylcysteine reduces exhaled hydrogen peroxide in stable COPD. Pulm Pharmacol Ther. 2005;18(1):41–47. | |
Lundback BLM, Andersson S. Possible effect of acetylcysteine on lung function. Eur Respir J. 1992;5(Suppl 15):895. | |
Decramer M, Rutten-van Molken M, Dekhuijzen PN, et al. Effects of N-acetylcysteine on outcomes in chronic obstructive pulmonary disease (Bronchitis Randomized on NAC Cost-Utility Study, BRONCUS): a randomised placebo-controlled trial. Lancet. 2005;365(9470):1552–1560. | |
Poole P, Black PN, Cates CJ. Mucolytic agents for chronic bronchitis or chronic obstructive pulmonary disease. Cochrane Database Syst Rev. 2012;8:CD001287. | |
Rubio ML, Sanchez-Cifuentes MV, Ortega M, et al. N-acetylcysteine prevents cigarette smoke induced small airways alterations in rats. Eur Respir J. 2000;15(3):505–511. | |
Tse HN, Raiteri L, Wong KY, et al. High-dose N-acetylcysteine in stable COPD: the 1-year, double-blind, randomized, placebo-controlled HIACE study. Chest. 2013;144(1):106–118. | |
Goldman MD, Saadeh C, Ross D. Clinical applications of forced oscillation to assess peripheral airway function. Respir Physiol Neurobiol. 2005;148(1–2):179–194. | |
Grimby G, Takishima T, Graham W, Macklem P, Mead J. Frequency dependence of flow resistance in patients with obstructive lung disease. J Clin Invest. 1968;47(6):1455–1465. | |
Brochard L, Pelle G, de Palmas J, et al. Density and frequency dependence of resistance in early airway obstruction. Am Rev Respir Dis. 1987;135(3):579–584. | |
Faria AC, Costa AA, Lopes AJ, Jansen JM, Melo PL. Forced oscillation technique in the detection of smoking-induced respiratory alterations: diagnostic accuracy and comparison with spirometry. Clinics (Sao Paulo). 2010;65(12):1295–1304. | |
Stav D, Raz M. Effect of N-acetylcysteine on air trapping in COPD: a randomized placebo-controlled study. Chest. 2009;136(2):381–386. | |
Hanaoka M, Droma Y, Chen Y, et al. Carbocisteine protects against emphysema induced by cigarette smoke extract in rats. Chest. 2011; 139(5):1101–1108. | |
Rubio ML, Martin-Mosquero MC, Ortega M, Peces-Barba G, Gonzalez-Mangado N. Oral N-acetylcysteine attenuates elastase-induced pulmonary emphysema in rats. Chest. 2004;125(4):1500–1506. | |
Cai S, Chen P, Zhang C, Chen JB, Wu J. Oral N-acetylcysteine attenuates pulmonary emphysema and alveolar septal cell apoptosis in smoking-induced COPD in rats. Respirology. 2009;14(3):354–359. | |
Long-term oral acetylcysteine in chronic bronchitis. a double-blind controlled study. Eur J Respir Dis Suppl. 1980;111:93–108. | |
[No authors listed]. Oral N-acetylcysteine and exacerbation rates in patients with chronic bronchitis and severe airways obstruction. British Thoracic Society Research Committee. Thorax. 1985;40(11):832–835. | |
Boman G, Backer U, Larsson S, Melander B, Wahlander L. Oral acetylcysteine reduces exacerbation rate in chronic bronchitis: report of a trial organized by the Swedish Society for Pulmonary Diseases. Eur J Respir Dis. 1983;64(6):405–415. | |
Grassi C, Morandini GC. A controlled trial of intermittent oral acetylcysteine in the long-term treatment of chronic bronchitis. Eur J Clin Pharmacol. 1976;9(5–6):393–396. | |
Hansen NC, Skriver A, Brorsen-Riis L, et al. Orally administered N-acetylcysteine may improve general well-being in patients with mild chronic bronchitis. Respir Med. 1994;88(7):531–535. | |
Pela R, Calcagni AM, Subiaco S, Isidori P, Tubaldi A, Sanguinetti CM. N-acetylcysteine reduces the exacerbation rate in patients with moderate to severe COPD. Respiration. 1999;66(6):495–500. | |
Rasmussen JB, Glennow C. Reduction in days of illness after long-term treatment with N-acetylcysteine controlled-release tablets in patients with chronic bronchitis. Eur Respir J. 1988;1(4):351–355. | |
Schermer T, Chavannes N, Dekhuijzen R, et al. Fluticasone and N-acetylcysteine in primary care patients with COPD or chronic bronchitis. Respir Med. 2009;103(4):542–551. | |
Zheng JP, Wen FQ, Bai CX, et al. Twice daily N-acetylcysteine 600 mg for exacerbations of chronic obstructive pulmonary disease (PANTHEON): a randomised, double-blind placebo-controlled trial. Lancet Respir Med. 2014;2(3):187–194. | |
Gerrits CM, Herings RM, Leufkens HG, Lammers JW. N-acetylcysteine reduces the risk of re-hospitalisation among patients with chronic obstructive pulmonary disease. Eur Respir J. 2003;21(5):795–798. | |
Grandjean EM, Berthet P, Ruffmann R, Leuenberger P. Efficacy of oral long-term N-acetylcysteine in chronic bronchopulmonary disease: a meta-analysis of published double-blind, placebo-controlled clinical trials. Clin Ther. 2000;22(2):209–221. | |
Stey C, Steurer J, Bachmann S, Medici TC, Tramer MR. The effect of oral N-acetylcysteine in chronic bronchitis: a quantitative systematic review. Eur Respir J. 2000;16(2):253–262. | |
Niederman MS, Rafferty TD, Sasaki CT, Merrill WW, Matthay RA, Reynolds HY. Comparison of bacterial adherence to ciliated and squamous epithelial cells obtained from the human respiratory tract. Am Rev Respir Dis. 1983;127(1):85–90. | |
Suer E, Sayrac S, Sarinay E, et al. Variation in the attachment of Streptococcus pneumoniae to human pharyngeal epithelial cells after treatment with S-carboxymethylcysteine. J Infect Chemother. 2008;14(4):333–336. | |
Radomska-Lesniewska DM, Sadowska AM, Van Overveld FJ, Demkow U, Zielinski J, De Backer WA. Influence of N-acetylcysteine on ICAM-1 expression and IL-8 release from endothelial and epithelial cells. J Physiol Pharmacol. 2006;57 Suppl 4:325–334. | |
Sinojia R, Shaikh M, Kodgule R, et al. Priming of beta-2 agonist and antimuscarinic induced physiological responses induced by 1200 mg/day NAC in moderate to severe COPD patients: a pilot study. Respir Physiol Neurobiol. 2014;191:52–59. | |
Linden M, Wieslander E, Eklund A, Larsson K, Brattsand R. Effects of oral N-acetylcysteine on cell content and macrophage function in bronchoalveolar lavage from healthy smokers. Eur Respir J. 1988;1(7):645–650. | |
Riise GC, Qvarfordt I, Larsson S, Eliasson V, Andersson BA. Inhibitory effect of N-acetylcysteine on adherence of Streptococcus pneumoniae and Haemophilus influenzae to human oropharyngeal epithelial cells in vitro. Respiration. 2000;67(5):552–558. | |
Wu W, Patel KB, Booth JL, Zhang W, Metcalf JP. Cigarette smoke extract suppresses the RIG-I-initiated innate immune response to influenza virus in the human lung. Am J Physiol Lung Cell Mol Physiol. 2011;300(6):L821–L830. | |
Tse HN, Raiteri L, Wong KY, Ng LY, Yee KS, Tseng CZ. Benefits of high dose N-acetylcysteine to exacerbation-prone COPD patients. Chest. May 15, 2014. [Epub ahead of print.] | |
Zhou Y, Wang X, Zeng X, et al. Positive benefits of theophylline in a randomized, double-blind, parallel-group, placebo-controlled study of low-dose, slow-release theophylline in the treatment of COPD for 1 year. Respirology. 2006;11(5):603–610. | |
McGavin CR, Macfarlane JT, Prescott RJ, Elmes P, Ferguson A, Nariman S, Stableforth D. Oral N-acetylcysteine and exacerbation rates in patients with chronic bronchitis and severe airways obstruction. Thorax. 1985;40:832–835. | |
Babolini H, Charpin J, Germouty J. Multicenter study group. Long term oral acetylcysteine in chronic bronchitis. A double-blind controlled study. Eur J Respir Dis Suppl. 1980;61(Suppl 111):93–108. |
 © 2014 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2014 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.