")
Back to Journals » Clinical Interventions in Aging » Volume 18
Unmet Needs and Barriers in Providing Hospital Care for Older Adults: A Qualitative Study Using the Age-Friendly Health System Framework
Authors Yi Y , Lee Y, Kang S, Kwon YH, Seo YM, Baek JY , Jang IY , Lee E , Koh Y, Jung HW , Park CM
Received 20 February 2023
Accepted for publication 26 July 2023
Published 11 August 2023 Volume 2023:18 Pages 1321—1332
DOI https://doi.org/10.2147/CIA.S409348
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Prof. Dr. Nandu Goswami
Youngseok Yi,1 Yura Lee,2 Selin Kang,3 Young Hye Kwon,4 Yeon Mi Seo,4 Ji Yeon Baek,1 Il-Young Jang,1 Eunju Lee,1 Younsuck Koh,5 Hee-Won Jung,1,* Chan Mi Park6,*
1Division of Geriatrics, Department of Internal Medicine, Asan Medical Center, University of Ulsan College of Medicine, Seoul, South Korea; 2Department of Information Medicine, Asan Medical Center, University of Ulsan College of Medicine, Seoul, Republic of Korea; 3Department of Economics, The Graduate School, Yonsei University, Seoul, South Korea; 4Department of Nursing, Asan Medical Center, Seoul, South Korea; 5Department of Pulmonary and Critical Care Medicine, Health Screening and Promotion Center, Asan Medical Center, Seoul, South Korea; 6Marcus Institute for Aging Research, Hebrew Senior Life, Harvard Medical School, Boston, MA, USA
*These authors contributed equally to this work
Correspondence: Chan Mi Park, Marcus Institute for Aging Research, Hebrew SeniorLife, Harvard Medical School, 1200 Centre Street, Boston, MA, 02131, USA, Tel +1-617-363-8000, Email [email protected] Hee-Won Jung, Division of Geriatrics, Department of Internal Medicine, Asan Medical Center, University of Ulsan College of Medicine, 88 Olympic-ro 43-gil, Songpa-gu, Seoul, 05505, South Korea, Tel +82-2-3010-1852, Email [email protected]
Purpose: This study aims to identify unmet needs and barriers for improving inpatient care for older adults at an academic hospital in Korea by using a qualitative focus group design and the Age-Friendly Health Systems (AFHS) framework.
Patients and Methods: A total of 14 healthcare providers and employees participated in focus group interviews. Participants included medical doctors, registered nurses, a receptionist, a patient transporter, a pharmacist, a physical therapist, and a social worker. The data were analyzed qualitatively, as per the Consolidated Criteria for Reporting Qualitative Research guidelines. The analysis method encompassed a thematic framework analysis via the AFHS 4Ms framework, consisting of the four domains “What Matters”, “Medication”, “Mentation”, and “Mobility”.
Results: Multiple barriers and unmet needs were identified using the AFHS 4Ms framework in the provision of inpatient care for older adults at the hospital. The main barriers identified in the “What matters” domain are a lack of shared decision-making and individualized care plans, as well as economic and safety-conscious preferences among some older patients. In the “Medications” domain, the main barriers to providing adequate and safe pharmacotherapy include patient and caregiver-related factors, increased complexity of medication use, and lack of institutional support systems. In the “Mentation” domain, the main issues identified are communication barriers related to patients, caregiver factors, and insufficient delirium management due to a lack of adequate processes/environments such as delirium identification. In the “Mobility” domain, the main challenges include reduced mobility and geriatric complications, unnecessary mobility restrictions, and the increased risk of falls due to lack of resources and environmental factors.
Conclusion: The study highlighted the need for improvements in inpatient care for older adults at an academic hospital in Korea. Identified unmet needs and barriers can be used to guide a more patient-centered approaches for an age-friendly inpatient environment.
Keywords: geriatrics, age-friendly health systems, 4M framework, patient-centered care, geriatric adverse outcomes
Introduction
Older patients often have complex healthcare needs encompassing multiple chronic conditions and functional impairments. These factors increase the risk of negative outcomes during their hospitalization — outcomes such as delirium, pressure ulcers, and falls.1–4 These geriatric adverse consequences can further worsen the functional status of older patients, leading to a greater likelihood of unplanned readmission, longer hospital stays, and long-term care institutionalization after discharge. In addition, older patients carry a higher risk of death following hospitalization.5–7
Previous studies have shown that patient-centered approaches combined with geriatric frameworks can improve health outcomes for older adults with complex health needs during hospitalization.8–10 These approaches often involve coordinating care across multiple healthcare services and various personnel, personalizing treatment to meet the unique needs of each patient, and providing education and support for the self-management and transition to long-term care settings. One of the most widely-adopted framework is the Age-Friendly Health Systems (AFHS) initiative, which aims to create age-friendly health systems through the implementation of the 4Ms framework, relating to: “What matters”, “Medication”, “Mentation”, and “Mobility”. This framework is led by the John A. Hartford Foundation and the Institute for Healthcare Improvement (IHI) in partnership with the American Hospital Association and the Catholic Health Association of the United States.2,11 The AFHS initiative provides health institutes with conceptual guidelines based on the 4M framework and the Plan-Do-Study-Act (PDSA) cycle practice for age-friendly health systems, while considering the limitations of resource availability. Moreover, by sharing case studies of hospitals that have successfully implemented AFHS guidelines, the initiative promotes the sharing of practical tips among the participating health institutes (called as the “AFHS action community”). IHI also encourages non-participating institutes worldwide to become members of the AFHS.
Although Korea is facing a rapidly-aging population, hospitals in the country have not fully adopted to delivering patient-centered geriatric care. This is due to the extant medical system being largely based upon a fragmented, specialty-oriented approach developed in the late 20th century.12–15 To address this issue, Asan Medical Center (the largest academic hospital in Korea) established an intramural acting group — the Asan Multidisciplinary Committee for Seniors (AMCS) — in 2020 with the goal of a cultural adaptation and implementation of the AFHS framework in the practice system.
To the best of our knowledge, this study is the first focus group interview research for healthcare providers and employees involved in the inpatient care for older adults using the 4M framework approach proposed by AFHS. There have been numerous studies investigating the barriers to providing health care for older adults,1,16–20 with some studies making use of quantitative methods in conjunction with multiple-choice surveys covering various questions. The advantage of a quantitative approach is that it synthesizes multiple opinions and produces intuitive, numerical summaries. On the other hand, a qualitative approach is advantageous in capturing more detailed and specific results, thereby offering a consilient perspective.21,22
The ultimate object of our study was to develop an age-friendly health system suitable for our environment and culture, including both patients and the national health system. Therefore, the study made use of focus group interviews with healthcare providers and hospital employees so as to identify unmet needs and barriers for improving patient care. The study aims to use the findings to guide the development of greater patient-centered and age-friendly inpatient care in a rapidly-aging country.
Materials and Methods
Study Design
This study was conducted from September 2021 to October 2021, and uses a qualitative focus group design to identify the existing unmet needs and barriers of older adults receiving inpatient care at an academic hospital in Korea. Six to nine participants were included in each focus group, in accordance with the recommended size for focus group interviews.23,24 Data collection and analysis followed the Consolidated Criteria for REporting Qualitative research (COREQ) guidelines.25
Sampling Strategy
A purposeful sampling strategy was employed to recruit participants for the focus group interviews. Despite the disadvantage of relatively low generalizability, this strategy allows researchers to obtain rich information by selecting participants aligned with the research objectives, ensures diversity in perspectives and experiences, and enables efficient use of limited resources.26,27 Approximately 30 potential participants were recommended by the Asan Multidisciplinary Committee for Seniors (the steering group for adopting AFHS in the hospital) based on the individual’s current involvement in older adult care. The sample was targeting a composition of 30% physicians, 30% nurses, and at least one pharmacist, physical therapist, social worker, receptionist, and patient transporter (each). In addition, the sample was also planned so as to take work experience in to account, with more than half of the participants having been in their (then) current position for five years or more. In total, 14 healthcare providers and employees volunteered to participate in the study. Most of the reasons for non-participation were attributable to an overlap between working and interview times. The first and second focus groups consisted of nine and six participants, respectively. Each interview session was designed to last one hour.
Data Collection
The focus group interviews were conducted by a moderator (Bioinformatics scientist) who was a member of the digital information innovation team at Asan Medical Center. A semi-structured interview guide was used to facilitate the discussion and to ensure that all relevant topics were covered. The guide was based on the AFHS framework and the 4Ms, and included open-ended questions regarding participants’ experiences and perspectives on hospital care for older adults. The interviews were conducted in Korean and were audio-recorded with the participants’ consent.
The interview protocol included icebreaker questions to encourage participation, and introductory questions regarding the roles and specialties of the participants. The interview then progressed to transition questions and key questions (listed in Table 1) which were aimed at providing insight into the unmet needs of older patients from the participants’ perspectives (main research objectives).
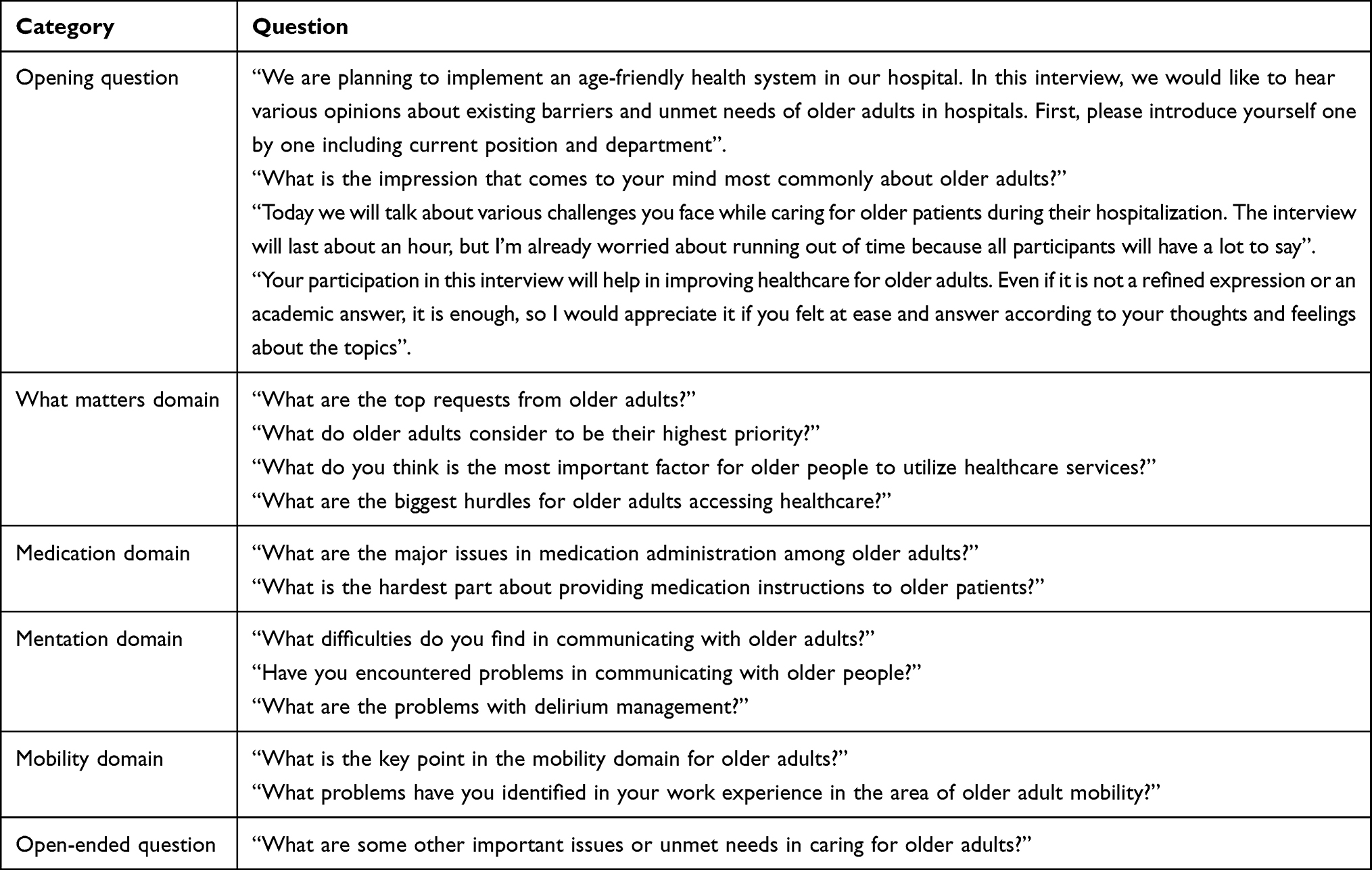 |
Table 1 Key Questions Included in the Interview |
Data Analysis
The audio-recorded interviews were transcribed verbatim. The transcripts were reviewed for accuracy and checked against the original audio recordings. The data were analyzed using a thematic analysis approach, a qualitative content analysis method in which the transcripts were coded and categorized according to themes related to the research questions. The analysis was conducted by two geriatric researchers independently, and any discrepancies were discussed and resolved through consensus. The interview data was analyzed using the framework method for thematic analysis, which is a systematic and rigorous approach to analyzing qualitative data.28,29
The transcribing process was assisted by an AI-based speech recognition application named CLOVA Note beta version (Naver Corp., Korea). We also made use of Microsoft Excel Office 365 (Microsoft Corp., Redmond, WA, USA) for charting descriptive code (initial coding), indexing, categorizing, and creating core thematic phrases (final coding).
Framework Analysis
A thematic analysis is a representative analysis method of qualitative research, with the interview results having been analyzed using framework analysis (one of the deductive thematic analysis methods).28,29 The framework used within this study is the AFHS 4M framework. The framework analysis process involves five main stages: familiarization, identifying a thematic framework, indexing, charting, and mapping/interpretation. In the “familiarization stage”, the researchers became accustomed to the data, identifying possible themes by reviewing the interview transcripts. In the “identifying a thematic framework” stage, key themes, issues, or discussion points embedded in the transcript were ascertained and assigned codes/names so as to capture their essence. The interview topic guide was used as a starting point in creating overarching categories. Any emergent themes identified from the transcripts were coded as responses to each question. In the “indexing stage”, codes that shared commonalities/consistencies were clustered together and appropriately named. In the “charting stage”, the data and thematic framework were rearranged to create order and synthesize the final coding framework through an abstraction process. Finally, in the “mapping/interpretation stage”, the data were interpreted and a narrative/story explaining the findings in relation to the research questions was developed. We also identified any patterns or themes that emerged from the data and applied them to develop recommendations for addressing the unmet needs of older patients.
AFHS 4M Framework
We used AFHS’ 4M framework for a semi-structured interview guide and data analysis. The 4Ms stand for “What Matters” (health outcome goals and care preferences), “Medication” (age-friendly medication reconciliation), “Mentation” (dementia, delirium, depression, and other neuropsychiatric conditions, along with their effects on communication abilities) and “Mobility” (individualized mobility plans and creating mobility-enabling clinical environments). As a semi-structured interview guide, A moderator asked participants key interview questions for each 4M domain in the focus group interview (Table 1). However, the participants might give episode-oriented answers which overlapped and mixed areas of the 4M domains. Therefore, in the data analysis process, each answer was reclassified along the 4M domains through the indexing and categorizing processes.
Ethical Considerations
The study was approved by the Institutional Review Board of Asan Medical Center, and all participants provided written informed consent before participating in the interviews (IRB No. 2021–1485). The participants informed consent included the publication of anonymized responses. Confidentiality was maintained throughout the study, and all identifying information was removed from the transcripts before analysis.
Results
Participant Characteristics
A total of 14 healthcare providers and hospital employees participated in the interviews. The first and second interviews were conducted with nine and six participants, respectively. Both interviews lasted approximately 80 minutes. One interviewee participated in both interviews. Four interviewees were medical doctors, two attending physicians in the geriatrics department. Five interviewees were registered nurses (four in the inpatient ward and one in the outpatient clinic). The other interviewees included a receptionist, a patient transporter, a pharmacist, a physical therapist, and a social worker. Eleven out of the 14 participants were women. The mean age group was 30–39, and the mean period of work experience in current position was approximately 5 years and 10 months (details in Table 2).
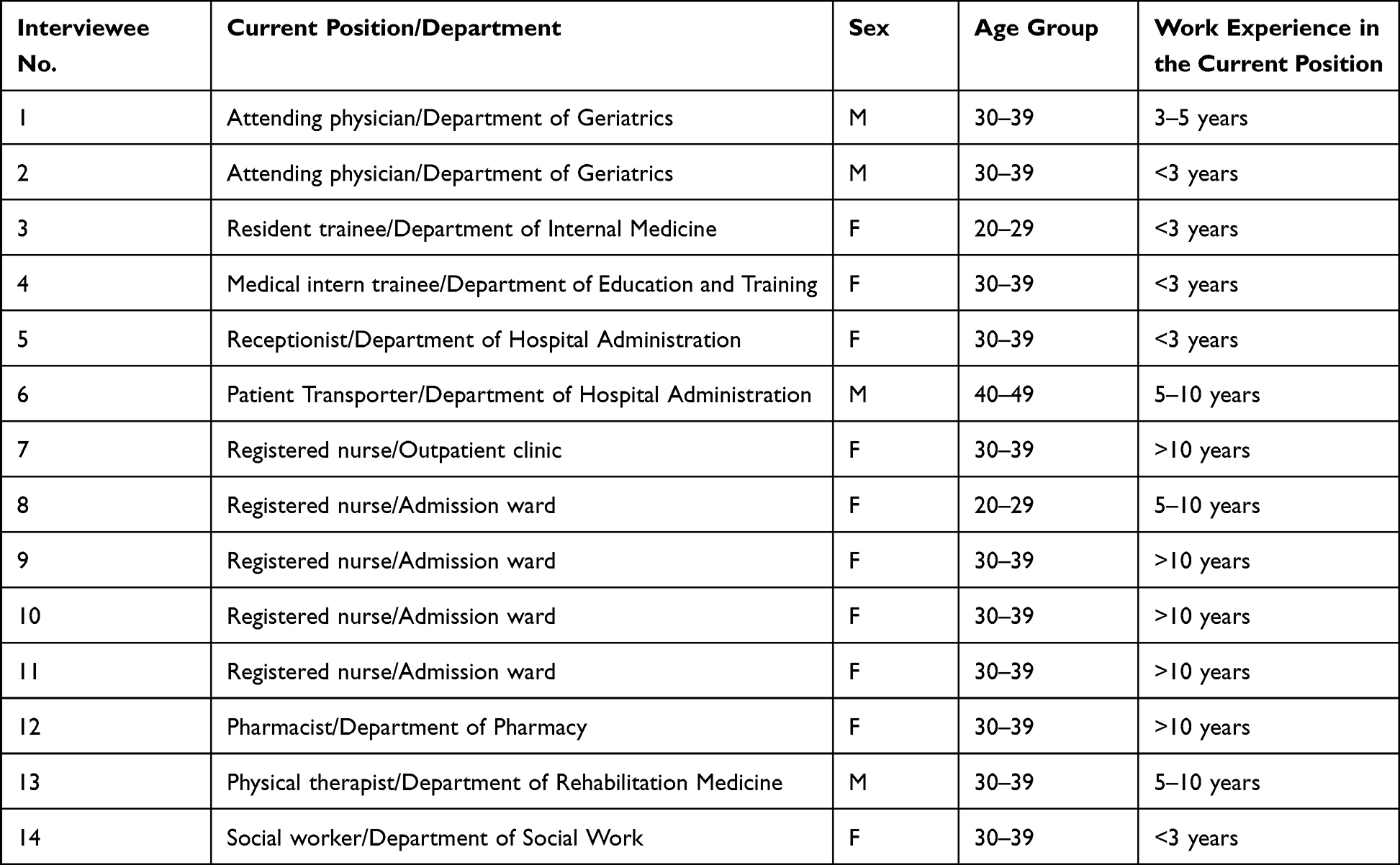 |
Table 2 Participant Characteristics |
Existing Unmet Needs and Barriers – 4M Framework Analysis
The 4Ms framework was applied to identify unmet needs and barriers in healthcare for older adults through thematic framework analysis of focus group interviews (Figure 1, Supplementary Table S1). Through the analysis process, the interview data was categorized into four domains of the 4Ms and summarized, eventually creating key themes.
 |
Figure 1 Existing problems and unmet needs in the 4Ms framework from the Age-Friendly Health System. The important key themes related to the barriers and unmet needs for improving care for older adults in the hospital setting were identified as per the 4Ms framework (“What matters”, “Medication”, “Mentation”, and “Mobility”), led by the John A. Hartford Foundation and the Institute for Healthcare Improvement (IHI). |
What Matters
The “what matters” domain includes key themes concerning health outcome goals and the care preferences of older adults. The core concepts analyzed through this domain are a variety of preferences in medical care service utilization, heterogeneities in the pattern of care demands in frail older patients, and the complex care needs present in acute clinical environments.
In reference to the variety of preferences in medical care service utilization, one participant said that
[a]lthough they are ill (sick) now, older patients have also led their own daily lives before. They don’t want to be considered as subjects of care.
Another participant noted that[o]lder patients are usually burdened with medical expenses. In particular, most older patients who are hospitalized only for diagnostic tests feel a great burden…
As such, participants noted that individuals have various priorities in medical care service utilization. Some older adults might consider economic factors as a priority. Participants also noted safety-conscious preferences in some patients, including pursuing less-invasive treatments/interventions. These notions on inter-individual heterogeneities — even with similar underlying comorbidities — and main medical/surgical issues are associated with unmet need for shared decision-making in clinical goal-setting, including palliative care and advanced care plans. Providers were unfamiliar with the concepts of frailty, complex care needs, and geriatric care, and reported difficulties in establishing individualized care plans. However, the participants agreed that the healthcare system should strive to create a patient-centered environment that is supportive of the values and goals of the individual.
Participants recognized the heterogeneities in the pattern of care demands, especially among individuals with frailty and a higher burden of deficits. This heterogeneity implies that healthcare providers must take a more comprehensive and individualized approach when caring for older adults with frailty. Participants agreed that providers should focus on individuals’ functional capacities and burden of frailty to develop personalized care plans, and that an interprofessional team with diverse skillsets/expertise is essential to provide comprehensive care that accounts for the heterogeneous care needs.
Also, participants noted several unmet demands for complex care needs in the setting of treatment goals, as the current clinical environments have been designed for younger, less-frail individuals with standardized clinical protocols. For example, one noted that,
[e]specially in geriatric wards, older patients need treatments focusing on functional recovery or nutrition status management
Therefore, the participants recognized that in order to adequately meet the needs of frail elderly persons in an acute hospital setting, healthcare providers should be able to provide personalized goals and care plans that suit the patient’s unique needs and capabilities.
From the results of the focus group interview data in this domain, the most important unmet needs and barriers concerning the “What matters” for older adults is the lack of a patient-centered healthcare system that considers the unique needs and preferences of each older adults (as opposed to a widespread disease-centered healthcare system).
Medication
The “Medication” domain pertains to themes concerning age-friendly medication reconciliation. In this domain, the interview data were categorized to patient and caregiver related factors of medication administration, increased complexity of medication use, and a lack of institutional support systems.
Patient-related and caregiver-related factors may contribute to difficulties in ensuring adequate and safe medication use. A participant noted that
[t]hey (elderly patients) usually face difficulties in listening to lengthy instructions about medication due to lower attention spans
Another participant cited that
[m]any older patients have [an] excessive insistence on their own medication and fears about prescription changes
Caregiver factors could also pose obstacles to adequate medication administration. One participant noted that
[t]here are cases where mismatches occur between the caregiver educated about the patient’s medication during hospitalization and the caregiver who provides post-discharge patient care. Potential barriers/concerns are noted in such cases.
Another participant cited that
[t]he type of medications taken in the older patient group tend to be different from those taken by other patient groups
Older patients with a higher burden of deficits and comorbidities tend to have a higher number of prescribed medications and diverse/complicated medication schedules. Participants noted that, in order to prevent polypharmacy-related adverse impacts, it is essential to comprehensively evaluate the patient’s medication history/medication-related issues — such as potential drug interactions, inappropriate medications, and drug-disease interactions — combined with interprofessional team discussions leading to prescription adjustments.
Participants noted that the current healthcare system in Korea presents significant challenges in accurately identifying and managing the medications of individual patients. This is partly due to a lack of information-sharing between medical institutions, which makes it difficult to determine the duration of medication use and to properly administer/discontinue medications. Providers agreed that these barriers in medication review may have serious consequences, particularly for older persons, as the lack of a unified information exchange system and that insufficient educational resources (both manpower and funding) can compromise the safety and effectiveness of medications. A pharmacist urged that resources should be allocated to medication review, medication education, and other services that can promote the safe and effective use of medications — including automatized software developments incorporated in the electronic health records systems to facilitate medication reviews.
When analyzing these finding in the “Medication” domain, the unmet needs and barriers that should have been addressed first were the lack of understanding of the characteristics and complexity of the older patients when it comes to medication use and the insufficient services and institutional supporting system tailored to them.
Mentation
The “Mentation” domain consists of themes concerning dementia, delirium, depression, and other neuropsychiatric conditions, along with their effects on communication abilities. The key themes have been classified as patient-related communication problems, caregiver-related communication problems, and insufficient delirium management.
Participants noted that many older individuals experience physical or cognitive declines —as exemplified by hearing impairments, visual disturbances, or cognitive impairments — which can make communication difficult. One interviewee stated that
…[e]ven when an explanation or instruction is repeated, they show ambiguous or blank expressions, making it difficult to know whether they understood the explanation or instruction.
These issues suggest that communication difficulties caused by patient factors require particular attention. Participants agreed that healthcare professionals should be aware of age-related changes in patients’ physical and cognitive abilities so as to effectively communicate and educate the patients. They urged that text-based materials should be designed with larger fonts, greater contrast, and simplified language so as to aid those with decreased vision (supporting the concept of universal design).
Participants indicated that older patients in Korea are often cared for by their spouses, who may have difficulty communicating with medical staff or other family members. One participant pointed out that
misunderstandings may occur when the older informal caregiver conveys information in an inappropriate manner to another caregiver.
Additionally, there may be a mismatch between the caregiver and the decision-maker, leading to communication barriers. Participants recommended the implementation of the following strategies during ward rounds: clear, accurate communication of medical information to older patients and caregivers ensuring their understanding, identifying the key familial decision-maker in discussions/decision-making processes, and ensuring communication and information-sharing among caregivers, medical staff, and other family members.One participant cited that
[p]atients admitted to the geriatrics ward, who often exhibit limited mobility and multimorbidity, are at risk of developing delirium and may be subjected to physical restraint as a result.
Delirium management is crucial for addressing unmet needs pertaining to mentation. However, delirium is often overlooked as an accidental and incurable condition. In Korean academic hospitals, instances of inappropriate delirium management occur frequently due to a lack of adequate processes/environments, often involving restraints and repeated antipsychotics usage. In-depth evaluation of the clinical circumstances and other potential contributing factors is essential in such cases. The same is true for the prevention of delirium. Participants recommended the development of strategies for the education, early identification, and treatment of underlying causes of delirium, the use of non-pharmacological interventions, and the minimization of the use of physical restraints.
The results of the “Mentation” domain showed that addressing communication barriers related to older adults and caregivers, along with insufficient delirium management owing to a lack of adequate processes/environments, were the most important unmet needs and barriers.
Mobility
The ‘Mobility domain explains key themes concerning individualized mobility plans and creating mobility-enabling clinical environments. The unmet needs and barriers were analyzed and categorized into three subdomains: reduced mobility and geriatric complications, unnecessary mobility restrictions, and the increased risk of falls due to scarce resources and environment factors (individualized mobility plans and creating mobility-enabling clinical environments).
One participant stated that “
[a]mong older patients who visit geriatric outpatient clinics, around 10 to 20% typically arrive in a wheelchair or with the support of a caregiver
Frail older adults often have difficulty walking and show mobility impairments. Frail individuals are at high risk of falls due to physical, neuropsychologic, and personality factors and are also at risk of developing pressure ulcers due to immobilization. Participants recommended the implementation of new strategies to improve mobility and reduce the risk of falls among frail older adults. This may include providing assistive devices, physical therapy, and fall-prevention education to help frail older adults maintain their mobility and independence. Caregivers should also be trained on how to safely transfer and assist frail older patients so as to prevent falls and other accidents; protocols for the prevention and management of pressure sores should also be included.
One participant cited that
[t]here were many cases of older patients who were able to walk with a cane at the time of admission, but [who] later became unable to walk without assistance or [who had] even became bedridden.
Participants noted that even short-term mobility limitations can lead to reduced mobility among older patients. Overly-rigid hospital policies that focus on fall prevention may also restrict the mobility of older patients. To address these issues, participants agreed on the regime change from passive fall prevention towards an active, mobility-promoting strategy for older, frail individuals. This may involve implementing strategies to support mobility, such as providing assistive devices and physical therapy, and promoting a culture of mobility within the hospital. It is also important to implement evidence-based measures such as identifying and addressing fall risks, providing education on fall prevention, and using non-pharmacological interventions.
Participants identified an increased risk of falls in older patients due to scarcity in resources and environmental factors, with one participant noting that this is especially true
In the case of frail older patients who may have various intravenous lines or drain lines that take longer to set up and require additional nursing staff assistance.
The inpatient room environment was also cited to include potential fall hazards, with “outdated beds, toilets, and handrails, potentially contributing to the risk of falls”. Participants recommended increasing resources and staffing (including nursing staff) to support the safe movement/transport of older patients. They noted that the risk of falls may be reduced by evaluating and updating equipment and infrastructure to meet current standards.
When analyzing the interview data concerning the “Mobility” domain, the most important unmet needs and barriers were those concerning a lack of awareness of the risk of reduced mobility and falls associated with frailty and a lack of resources to prevent geriatric complications among inpatients.
Discussion
This study aimed to identify key themes related to unmet needs and barriers in improving hospital care for older adults using the 4Ms framework (What Matters, Medication, Mentation, and Mobility). The results of this study reveal that individualized and patient-centered care is crucial for addressing the heterogeneity among older patients and their unique needs and preferences. Moreover, challenges in providing adequate pharmacotherapy, addressing communication barriers and delirium management, mobility issues, and geriatric complications were identified.
Overall, these findings have important clinical implications for the care of older adults in hospital settings. These findings underline the need for patient-centered, coordinated care which considers the unique needs and preferences of each older patient. This includes the development of individualized care plans, comprehensive assessments, and ongoing monitoring of functional status, medications, patient preferences, and care needs.
Our findings are consistent with the result of a recent study conducted by van der Kluit et al, which used open interviews with individuals in teaching hospitals who were 70 years and older. The study found that essential goals for older inpatients were “knowing what the matter is (sic), controlling disease, maintaining independence, [and] improving daily/social functioning”.20 In addition, the study presented different perspectives on the healthcare goal in that the results were gleaned from interviews with patients rather than healthcare providers. Although the research population was different, Abdi et al show similar findings in a scoping review which includes 40 studies on the care and support needs of older adults living at home with chronic conditions using the WHO International Classification of Functioning, Disability and Health framework.18 As with our findings, the study highlighted the fact that many services and care models are still not based on the needs of older adults. Additionally, similar barriers were observed in a previous focus group interview study for establishing efficient transition care plans for older patients in Korea.19 In the conclusion of the study, a slightly difference is that the study emphasizes effective communication strategies accounting for medical and functional problems.
One potential strategy for adopting the AFHS framework in Korean academic hospitals is to use the PDSA cycle approach, as currently ongoing in Asan Medical Center. This involves identifying existing unmet needs and barriers, developing and implementing interventions to address these issues, evaluating the effectiveness of these interventions, and making necessary adjustments. The PDSA cycle proceeded in the following four stages. First, the “Plan” stage was to understand the current state. We assembled a team and analyzed barriers through the lens of the 4M framework, and designed solutions to overcome these barriers. In this stage, we reviewed the evidence-based medical literature and widespread initiatives on age-friendly health care, discussed it through regular meetings, and shared the knowledge throughout the course of a year.1,2,9,30–35 Afterwards we provided practical service in the “Do” stage and reviewed the practice in the “Study” stage; we then modified the process in the “Act” stage.
This approach allows for a gradual and systematic process of cultural adoption and embedding of the AFHS framework within clinical practice. For example, as the interviews have revealed, healthcare providers in the hospital (of the participants) were unfamiliar with the concept of frailty, and experienced difficulties in determining patient-specific care needs for establishing therapeutic goals; we incorporated the Clinical Frailty Scale — a measure of frailty and functional capacities with pictograms and brief descriptions — in the assessment of “What matters.”36–39 Furthermore, we established an inpatients medication reconciliation liaison service with a polypharmacy management program developed by the Korean national health insurance system (NHIS), leveraging the government-based fee-support regime and the interdisciplinary collaboration between geriatricians and geriatric pharmacists.8,40,41 It is also important to involve a wide range of healthcare professionals in the process of implementing the AFHS framework. This includes doctors, nurses, pharmacists, social workers, and other healthcare providers who have direct contact with older patients. These professionals can play a key role in identifying and addressing the unique needs and preferences of older patients, as well as by providing education and support for self-management and transition to long-term care settings. For example, we have established a fast-track rehabilitation program — as provided by the department of physical medicine and rehabilitation — involving doctors, physical therapists, and geriatric nurses.42,43 From 2021, the Asan Multidisciplinary Committee for Seniors gradually increased eligible wards in the hospital with the aim to cover the whole inpatient unit by early 2023. In 2022, Asan Medical Center was recognized as reaching the desired level of being “Committed to Care Excellence” as per the IHI’s AFHS.44
There are several limitations to this study. First, the focus group sample was relatively small, and the results may not be generalizable to all academic hospitals in Korea. Second, the interview only involved providers and employees, and did not include patients and caregivers. Our next project involves in-depth interviews with patient-caregivers, and we plan to analyze their responses in the same way by using the 4M framework so as to supplement this limitation. Unfortunately, we skipped the formal pre-test process. Instead, we conducted two focus group interviews with the same modulator and guide. There was no structural difference between the two interviews evident as per the data analysis’ results. Meanwhile, the condition of requiring a single moderator to conduct the interviews may have presented a weakness in potentially having influenced the responses of the participants. Finally, the study relied on the self-reported experiences and perspectives of the participants, indicating that recall bias and other subjective errors cannot be ruled out. Despite these limitations, the results of this study provide important insights into the barriers and potential solutions for improving hospital care for older adults, as well as highlighting the need for patient-centered, coordinated care that takes into account the unique needs and preferences of each patient.
Conclusion
In conclusion, this study identified a number of key themes related to the unmet needs and barriers for improving care for older adults in the hospital setting, as per the 4Ms framework. According to 4M framework analysis, there are major unmet needs concerning a variety of preferences in medical care service along the “What matters” domain. In the “Medication” domain, barriers to medication administration, increased complexity of medication use, and a lack of institutional supporting system were identified. In the “Mentation” domain, communication barriers between healthcare providers and patient-caregivers, and insufficient delirium management were emphasized. In the “Mobility” domain, the most prescient among the unmet needs and barriers were those situations that brought about reduced mobility, unnecessary mobility restrictions, and increased risk of falls. To address these unmet needs and barriers, the cultural adoption and gradual expansion of the 4Ms framework in Asan Medical Center are ongoing. Further research involving patients, caregivers, and providers is needed to confirm these findings and to explore the feasibility and effectiveness of implementing the AFHS framework in clinical practice in Korean academic hospitals.
Acknowledgments
This study is the result of work supported by the Asan Multidisciplinary Committee for Seniors (AMCS). The AMCS members are as follows; Younsuck Koh, Soo-Sung Park, Eunju Lee, Dae Yul Kim, Hyouk-Soo Kwon, Eun hee Cho, Hye won Han, Sun hee Lee, Young gi Cho, Jung sook Choi, Hyun jin Oh, Joo hyun Nam, Won gu Yi, Ju yeon Oh, Ki Young Son, Young hye Kwon, Yeon mi Seo, Ji Yeon Baek, Il-Young Jang, Hee-Won Jung. The authors wish to express their gratitude to all the focus group participants for their invaluable comments. This study was also supported by a grant (2022IP0057-2) from the Asan Institute for Life Science, Asan Medical Center, Seoul, Republic of Korea.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Bláhová H, Bártová A, Dostálová V, Holmerová I. The needs of older patients in hospital care: a scoping review. Aging Clin Exp Res. 2021;33(8):2113–2122. doi:10.1007/s40520-020-01734-6
2. Fulmer T, Mate KS, Berman A. The age-friendly health system imperative. J Am Geriatr Soc. 2018;66(1):22–24. doi:10.1111/jgs.15076
3. Sager MA, Franke T, Inouye SK, et al. Functional outcomes of acute medical illness and hospitalization in older persons. Arch Intern Med. 1996;156(6):645–652. doi:10.1001/archinte.1996.00440060067008
4. Calderón-Larrañaga A, Vetrano DL, Ferrucci L, et al. Multimorbidity and functional impairment-bidirectional interplay, synergistic effects and common pathways. J Intern Med. 2019;285(3):255–271. doi:10.1111/joim.12843
5. Lakhan P, Jones M, Wilson A, Courtney M, Hirdes J, Gray LC. A prospective cohort study of geriatric syndromes among older medical patients admitted to acute care hospitals. J Am Geriatr Soc. 2011;59(11):2001–2008. doi:10.1111/j.1532-5415.2011.03663.x
6. Wallis SJ, Wall J, Biram RW, Romero-Ortuno R. Association of the clinical frailty scale with hospital outcomes. QJM. 2015;108(12):943–949. doi:10.1093/qjmed/hcv066
7. Clegg A, Young J, Iliffe S, Rikkert MO, Rockwood K. Frailty in elderly people. Lancet. 2013;381(9868):752–762. doi:10.1016/s0140-6736(12)62167-9
8. McNabney MK, Green AR, Burke M, et al. Complexities of care: common components of models of care in geriatrics. J Am Geriatr Soc. 2022;70(7):1960–1972. doi:10.1111/jgs.17811
9. Mate KS, Berman A, Laderman M, Kabcenell A, Fulmer T. Creating age-friendly health systems – a vision for better care of older adults. Healthc. 2018;6(1):4–6. doi:10.1016/j.hjdsi.2017.05.005
10. De Biasi A, Wolfe M, Carmody J, Fulmer T, Auerbach J. Creating an age-friendly public health system. Innov Aging. 2020;4(1):igz044. doi:10.1093/geroni/igz044
11. Age-Friendly Health Systems (AFHS). Institute for Healthcare Improvement (IHI)’s initiatives (online); 2023. Available from: https://www.ihi.org/Engage/Initiatives/Age-Friendly-Health-Systems/Pages/default.aspx.
12. Ga H. Ten years of long-term care insurance in Korea: light and shade from a geriatric point of view. Ann Geriatr Med Res. 2017;21(4):147–148. doi:10.4235/agmr.2017.21.4.147
13. Kwon S. Payment system reform for health care providers in Korea. Health Policy Plan. 2003;18(1):84–92. doi:10.1093/heapol/18.1.84
14. Lee JY, Jo MW, Yoo WS, Kim HJ, Eun SJ. Evidence of a broken healthcare delivery system in Korea: unnecessary hospital outpatient utilization among patients with a single chronic disease without complications. J Korean Med Sci. 2014;29(12):1590–1596. doi:10.3346/jkms.2014.29.12.1590
15. Park CM, Jung HW. We need better solutions for care transitions after hospitalizations in Korea. Ann Geriatr Med Res. 2021;25(1):60–62. doi:10.4235/agmr.21.0019
16. Slaboda JC, Nelson SH, Agha Z, Norman GJ. A national survey of caregiver’s own experiences and perceptions of U.S. health care system when addressing their health and caring for an older adult. BMC Health Serv Res. 2021;21(1):101. doi:10.1186/s12913-021-06086-z
17. McGilton KS, Vellani S, Yeung L, et al. Identifying and understanding the health and social care needs of older adults with multiple chronic conditions and their caregivers: a scoping review. BMC Geriatr. 2018;18(1):231. doi:10.1186/s12877-018-0925-x
18. Abdi S, Spann A, Borilovic J, de Witte L, Hawley M. Understanding the care and support needs of older people: a scoping review and categorisation using the WHO international classification of functioning, disability and health framework (ICF). BMC Geriatr. 2019;19(1):195. doi:10.1186/s12877-019-1189-9
19. Park CM, Han SJ, Lee JH, et al. A focus group interview with health professionals: establishing efficient transition care plan for older adult patients in Korea. BMC Health Serv Res. 2022;22(1):397. doi:10.1186/s12913-022-07802-z
20. van der Kluit MJ, Dijkstra GJ, de Rooij SE. Goals of older hospitalised patients: a qualitative descriptive study. BMJ Open. 2019;9(8):e029993. doi:10.1136/bmjopen-2019-029993
21. Giacomini MK, Cook DJ. Users’ guides to the medical literature: XXIII. Qualitative research in health care A. Are the results of the study valid? Evidence-Based Medicine Working Group. JAMA. 2000;284(3):357–362. doi:10.1001/jama.284.3.357
22. Côté L, Turgeon J. Appraising qualitative research articles in medicine and medical education. Med Teach. 2005;27(1):71–75. doi:10.1080/01421590400016308
23. Krueger RA. Focus Groups: A Practical Guide for Applied Research.
24. Carlsen B, Glenton C. What about N? A methodological study of sample-size reporting in focus group studies. BMC Med Res Methodol. 2011;11:26. doi:10.1186/1471-2288-11-26
25. Tong A, Sainsbury P, Craig J. Consolidated criteria for reporting qualitative research (COREQ): a 32-item checklist for interviews and focus groups. Int J Qual Health Care. 2007;19(6):349–357. doi:10.1093/intqhc/mzm042
26. Palinkas LA, Horwitz SM, Green CA, Wisdom JP, Duan N, Hoagwood K. Purposeful sampling for qualitative data collection and analysis in mixed method implementation research. Adm Policy Ment Health. 2015;42(5):533–544. doi:10.1007/s10488-013-0528-y
27. Luciani M, Campbell K, Tschirhart H, Ausili D, Jack SM. [How to design a qualitative health research study. Part 1: design and purposeful sampling considerations] Come Disegnare uno Studio di Ricerca Sanitaria Qualitativa. Parte 1: considerazioni sui Disegni e sul Campionamento Propositivo. Prof Inferm. 2019;72(2):152–161. Italian.
28. Gale NK, Heath G, Cameron E, Rashid S, Redwood S. Using the framework method for the analysis of qualitative data in multi-disciplinary health research. BMC Med Res Methodol. 2013;13:117. doi:10.1186/1471-2288-13-117
29. Ritchie J, Spencer L. Qualitative data analysis for applied policy research. In: Analyzing Qualitative Data. Routledge; 2002:173.
30. Senior Friendly Hospital (SFH) Framework. Regional geriatric program of Toronto; 2023. Available from: https://www.rgptoronto.ca/initiatives/senior-friendly-hospitals.
31. Chiou S, Hu Y. Identification and improvement on organizational weaknesses in age-friendly health care in Taiwan. Innovation Aging. 2017;1(suppl_1):771. doi:10.1093/geroni/igx004.2798
32. World Health Organization. Towards Age-Friendly Primary Health Care. World Health Organization; 2004.
33. Wong KS, Ryan DP, Liu BA. A system-wide analysis using a senior-friendly hospital framework identifies current practices and opportunities for improvement in the care of hospitalized older adults. J Am Geriatr Soc. 2014;62(11):2163–2170. doi:10.1111/jgs.13097
34. Chiou ST, Chen LK. Towards age-friendly hospitals and health services. Arch Gerontol Geriatr. 2009;49(Suppl 2):S3–S6. doi:10.1016/s0167-4943(09)70004-4
35. Kuo YL, Chen IJ. Facilitating a change model in age-friendly hospital certification: strategies and effects. PLoS One. 2019;14(4):e0213496. doi:10.1371/journal.pone.0213496
36. Theou O, Pérez-Zepeda MU, van der Valk AM, Searle SD, Howlett SE, Rockwood K. A classification tree to assist with routine scoring of the clinical frailty scale. Age Ageing. 2021;50(4):1406–1411. doi:10.1093/ageing/afab006
37. Rockwood K, Song X, MacKnight C, et al. A global clinical measure of fitness and frailty in elderly people. Cmaj. 2005;173(5):489–495. doi:10.1503/cmaj.050051
38. Leahy A, O’Connor M, Condon J, et al. Diagnostic and predictive accuracy of the clinical frailty scale among hospitalised older medical patients: a systematic review and meta-analysis protocol. BMJ Open. 2021;11(1):e040765. doi:10.1136/bmjopen-2020-040765
39. Ko RE, Moon SM, Kang D, et al. Translation and validation of the Korean version of the clinical frailty scale in older patients. BMC Geriatr. 2021;21(1):47. doi:10.1186/s12877-021-02008-0
40. Ceschi A, Noseda R, Pironi M, et al. Effect of medication reconciliation at hospital admission on 30-day returns to hospital: a randomized clinical trial. JAMA Netw Open. 2021;4(9):e2124672. doi:10.1001/jamanetworkopen.2021.24672
41. Varkey P, Cunningham J, O’Meara J, Bonacci R, Desai N, Sheeler R. Multidisciplinary approach to inpatient medication reconciliation in an academic setting. Am J Health Syst Pharm. 2007;64(8):850–854. doi:10.2146/ajhp060314
42. Kosse NM, Dutmer AL, Dasenbrock L, Bauer JM, Lamoth CJ. Effectiveness and feasibility of early physical rehabilitation programs for geriatric hospitalized patients: a systematic review. BMC Geriatr. 2013;13:107. doi:10.1186/1471-2318-13-107
43. Handoll HH, Cameron ID, Mak JC, Panagoda CE, Finnegan TP. Multidisciplinary rehabilitation for older people with hip fractures. Cochrane Database Syst Rev. 2021;11(11):Cd007125. doi:10.1002/14651858.CD007125.pub3
44. Institute for Healthcare Improvement (IHI)’s initiatives. Health systems recognized by Institute for Healthcare Improvement (IHI) as age-friendly; 2023. Available from: https://www.ihi.org/Engage/Initiatives/Age-Friendly-Health-Systems/Pages/recognized-systems.aspx.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.