Back to Journals » Open Access Journal of Contraception » Volume 14
Unmet Family Planning Need Globally: A Clarion Call for Sharpening Current Research Frame Works
Authors Pillai VK ![]() , Nagoshi JL
, Nagoshi JL
Received 23 December 2022
Accepted for publication 21 June 2023
Published 20 July 2023 Volume 2023:14 Pages 139—147
DOI https://doi.org/10.2147/OAJC.S378042
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Igal Wolman
Vijayan K Pillai,1 Julieann Lynn Nagoshi2
1School of Social Work, University of Texas at Arlington, Arlington, Texas, USA; 2Southwest Interdisciplinary Research Center, School of Social Work, Arizona State University, Phoenix, Arizona, USA
Correspondence: Vijayan K Pillai, School of Social Work, University of Texas at Arlington, 211 South Cooper Street, Arlington, TX, 76019, USA, Email [email protected]
Introduction
Contraceptive use was a contentious issue during the course of the 19th century with it being illegal to provide contraception information in the US well into the 20th century.1,2 In a rapid about-face, the period that followed was marked by the introduction of several birth control methods as well as a feverish stage of contraceptive research and development.3 The impetus for the innovations in birth control technology was provided by Margaret Sanger, whose activism paved the way for the landmark 1965 Supreme Court case Griswold v. Connecticut which overturned the ban on contraceptives for married couples.4 In the 1900s, the family planning movement took hold in the US, during a period of intense concern over the socio-economic consequences of overpopulation, poverty, and insecurity, as foretold by Malthus more than two centuries ago.4
As early as the second decade of the twentieth century, organizations, such as the International Labor Organizations had declared “Poverty anywhere is poverty everywhere”.5 Partly as a measured defense against security concerns, Dr Reimert Ravenholt, the first director of the Office of Population at the US Agency for International Development (USAID), and Global family planning assistance program spearheaded a massive international family planning program primarily to contain poverty.6 He oversaw the disbursement of nearly 1.4 billion dollars for family planning programs worldwide during his 14 years at the office, 1965–1979. According to the United Nations Population Fund (UNFPA), the largest bilateral donor of family planning assistance in 2018 was the United States, followed by the United Kingdom and Sweden.7
Nearly six decades since the entry of the family planning program on the world stage, the original mission of provision of suitable contraception for all women of reproductive age has not yet been realized. Furthermore, the family planning program vision as stated in SDG 3.7.1 was to guarantee all women currently aged 15 to 45 universal access to family planning information and education and sexual and reproductive health-care services under the national development strategies and programs.8 These targets are far from being met resulting in high levels of unmet need among women in reproductive age groups in developing countries.
According to new estimates for the year 2019, sexual and reproductive health services in low- and middle-income countries (LMICs) are inadequate to meet the needs of their populations. The estimates for low- and middle-income countries indicate that approximately 218 million women of reproductive age (between 15 and 49 years old) have an unmet need for modern contraception. Furthermore, about 49% of pregnancies in LMICs, which amounts to 111 million annually, are unintended.9 In West & Central Africa, low coverage coexists alongside high unmet family planning.10–13 Family planning programs in LMICs, such as India, have responded to high levels of unmet need through an array of measures, such as improving the variety and mix of contraceptive methods; enhancing the availability, accessibility, and affordability of contraceptives; and boosting the capacity among family planning workers to connect with women from marginalized communities and respond to their family planning needs.14
These measures appear to have only marginally yielded anticipated results, in light of the fact that the percentage of women with unmet needs for family planning globally has remained steady at about 10%, over the last two decades.15 Subsequently, a large proportion of women in reproductive age groups have been driven to the use of permanent methods of contraception. According to NFHS-5 data, 50% of currently married women in India are utilizing modern contraceptive methods, while 38% exclusively rely on female sterilization.16
While improving the availability and accessibility of family planning services is crucial to decreasing the unmet need for contraception, it is insufficient in and of itself. While supply-side interventions, such as increasing the availability of contraceptives have been effective in increasing contraceptive use in developing countries, the impact of these interventions has been limited.17 The authors suggest that this is because demand-side factors, such as individual-level beliefs, attitudes, and preferences towards contraception have not been adequately addressed. While there has been extensive research on the socio-demographic factors that influence contraceptive use, there has been relatively little research on the individual-level factors that affect contraceptive use.18 A person-centered approach to understanding contraceptive use can help to identify the multilevel factors, which takes into account the individual-level factors that may influence contraceptive use, as well as the broader social, cultural, and economic factors that may contribute to unmet need and inform the development of more effective programs to reduce unmet family planning need in developing countries.19,20
Moreover, medical problems like infertility, chronic illness, or disabilities can either restrict an individual’s ability to use contraception or raise their need for particular types of contraception. For instance, certain medical conditions may require women to use specific types of contraceptives, and not doing so can lead to negative health consequences. Furthermore, the concern about the potential adverse effects of hormonal contraception on reproductive tract infections has been identified as a noteworthy contributor to the decision to not use contraception.21 Addressing reproductive health problems and providing specialized family planning services can help to decrease the unmet need for family planning. Despite this, the significance of reproductive health problems as a compelling cause of contraceptive use decision-making is less recognized compared to supply and demand side factors. In several developing regions such as Uttar Pradesh in India, the prevalence of Reproductive Tract Infections/Sexual Tract Infections among women aged 15–45 has been reported as high as 52.2%.22 Globally, 4 in 100 women in reproductive age (15 −45) suffer from one of the four STIs, which include trichomoniasis, bacterial vaginosis, chlamydia, and gonorrhea.23 The importance of reproductive health concerns in relation to reproductive rights and contraceptive decision-making by women, as well as the role of service agencies in meeting women’s family planning requirements, was initially addressed during the 1994 Beijing Conference.
The Beijing 1994 meeting, also known as the International Conference on Population and Development (ICPD), played a significant role in highlighting the importance of family planning and reproductive rights in improving global reproductive health. The conference recognized that reproductive health encompasses not only the physical but also the mental and social well-being of individuals in relation to their reproductive system and processes. Reproductive rights, on the other hand, emphasize the individual’s right to make informed choices about their reproductive health, including the right to access and use contraception, seek family planning services, and make decisions about the timing, number, and spacing of their children. The link between reproductive health and reproductive rights lies in the fact that access to comprehensive family planning services, including information, education, and contraception, empowers individuals to make informed choices about their reproductive health, which can have positive impacts on their overall well-being and contribute to improved reproductive health outcomes globally.
This focus on reproductive health and rights emerged with the Post-2015 development agenda from the convergence of three streams of development goals: the United Nations Conference on Environment and Development (Rio 1992), the International Conference on Population and Development (ICPD 1994), and the Millennium Development Goals (MDGs). The Post-2015 agenda placed a new emphasis on family planning programs that cater to the demand for contraceptive use, based on the principles of reproductive rights.24 The goal was to provide rights-based family planning programs that prioritize individual and couples’ choices and needs.
The study of the demand for contraceptive use among women of reproductive age requires well-defined theoretical and methodological approaches that take into account the diverse utilities associated with this behavior. This entails examining how these utilities change over time, considering the multilevel effects of individual-level physical and mental health, as well as the meso and macro-level effects of the environment on contraceptive use in different populations.25
Furthermore, it is essential to adopt a person-centered perspective and consider reproductive health issues that women face over time. For instance, the transition from childhood to adolescence is often fraught with uncertainties and may be influenced by unpleasant memories and experiences from childhood, which can impact the smooth and healthy progression into the teenage years. Therefore, a comprehensive understanding of contraceptive use must consider the broader reproductive health context in which women navigate these transitions in life stages.
The cumulative and interactive effects of mental and physical health risks during childhood may unduly limit teenagers’ capacity to make contraceptive use decisions and to effectively plan births during later years.26,27 Lack of research on the identification of such pathways necessary for building capacity for effective contraceptive use remains limited.
Though there has been extensive research on unmet family planning needs focusing on the role of socioeconomic and cultural factors, studies on the inter-relatedness of determinants of contraceptive use as they relate to past and present use are few and far between.28 In most LMICs, as women enter into marriage, they are faced with several familial expectations such as the number of desired children and the number of male children which impact contraceptive use decision-making.
Understanding the Complexities of Women’s Contraceptive Decision-Making
The interrelatedness of many social and individual factors that influence contraceptive use, as well as the pattern of change in the causative factors over time, constrain women’s life-stage dependent contraceptive choices. For example, as women age, decisions with respect to starting and spacing children over time are impacted by their past as well as present experiences of social, economic, and physical well-being. Edmeades, Lee-Rife and Malhotra,29 and Edmeades30 observe that the current research on contraceptive use is limited to our narrow understanding of how and why temporary contraceptive methods change over the course of women’s lives. Current theories of unmet family planning have not yet developed an adequate framework to systematically identify the independent, cumulative, and interactive effects of social, health, economic, and life stage-related influences pertaining to contraceptive decision-making and use.31,32
The difficulties facing current programs and policies to reduce unmet need call for new conceptual schemes that enable women to build the capacity to make healthy contraceptive use decisions, thus taking into consideration the health and social relationship histories across life stages. In this regard, there are three theoretical approaches, which suggest a number of micro, meso, and macro-level factors associated with pregnancy and fertility intentions underlying unmet needs. Two of the models are rooted in social scientific disciplines, such as sociology and demography, and the third is a medical model.
The first approach takes into account the direct and indirect effects of environmental factors that influence fertility control during the course of a specific period into which women are born, socialized, and plan births. This approach is broadly referred to as the cohort–historical model. The cohort-historical model proposes that the processes whereby people are born, live out their lives, and are replaced in a society, underlie social changes such as shifts in fertility and trends in opinions and values. Social change is seen as stemming from the fresh contacts new cohorts make with contemporary social heritage.33 The interaction between new cohort members and the existing social system makes it possible for the social system to influence the members’ characteristics.
Conversely, the cohort members may bring about new rules of behavior and/or alter the environment so as to fulfill social and economic needs. Such normative and environmental changes, along with changes in the size of the cohorts can bring about inter-cohort differences in terms of starting, spacing, and stopping childbearing. For example, young men born in the early fifties returning from World War II found a robust socio-economic environment with plenty of job opportunities. Encouraged by the presence of a strong economy, many not only started having children early but also paced them slightly faster than their counterparts a generation earlier. This approach explicitly considers the impact of women’s age as well as the birth cohort.33,34
The second approach broadens the cohort–historical model by taking into consideration the accumulated effects of reproductive health experiences as well as gains and losses with respect to building the capacity to achieve desired family size. The framework helps explain how the structure and quality of women’s social relationships change across life stages and how these independently, cumulatively, and interactively influence and build women’s capacity for healthy contraceptive use over time.
This approach is labeled “life course” since it takes into consideration a number of social, economic, psychological, and environmental forces impinging on individuals going through various life stages. The life course is indicated by multilevel, interdependent past and current events, some of which have a significant and abiding influence on the individual.35,36 Life course theory segments the life course into several trajectories. Each trajectory is made up of interrelated events, actions, and incidents shaping long-lasting involvement with social institutions, such as marriage and family. These trajectories which either occur or are timed as per social expectations are often age-related. Within a trajectory, individuals may likely experience such events as social roles and status changes referred to as transitions. Some of these transitions may significantly modify the trajectory resulting in “turning points” in an individual’s life inciting significant priority-based decisions.
The journey through life stages is accompanied by a focus on generating subjective well-being and maintaining social relations. More importantly, the passage through life stages is marked by accomplishing socially accepted goals at desired intervals against ongoing social, economic, and political changes.
Within these broad-level changes, individuals live out their lives responding to norms and values with respect to several aspects of their being including family formation involving contraceptive decisions with respect to starting, spacing, and stopping childbirth. As reproductive careers unfold, social relationships within the household may change contributing to dynamic modifications in power relationships linked to accessibility to contraceptives. In addition, variations in health status also may impact contraceptive use decisions.
The third came about as a product of a long history of involvement of the medical community in the development and promotion of contraception as a widely used modern medical method to plan family formation as well as to improve reproductive health. While the socio-historical and the life course models remained within the confines of the social sciences; sociology and demography in particular, the emphasis was mostly on socio-economic and environmental determinants. This to some extent resulted in the dearth of efficient research designs to explain contraceptive use behavior considering the likely susceptibility to illness and contagions that have emerged over time. Not surprisingly, this also led to a focus on the observation of environmental factors as well the biological ones over time. This approach has now culminated in the development of life-course epidemiology based on the premise that biological and social factors operating over time and across life stages influence likely occurrences of disease as well as health behaviors.37–39
This focus has resulted in scrutinizing contraceptive use within the life stage-specific etiology of diseases. At the epidemiological level, the incorporation of the life course approach has contributed to the development of life course epidemiology; the study of the contribution of biological and social factors acting independently, interactively, and cumulatively, therefore impacting health outcomes such as contraceptive use.
A summary of the differences and similarities among the precepts of Cohort-historical; Life Courseand Life course Epidemiological Models is presented in Table 1.
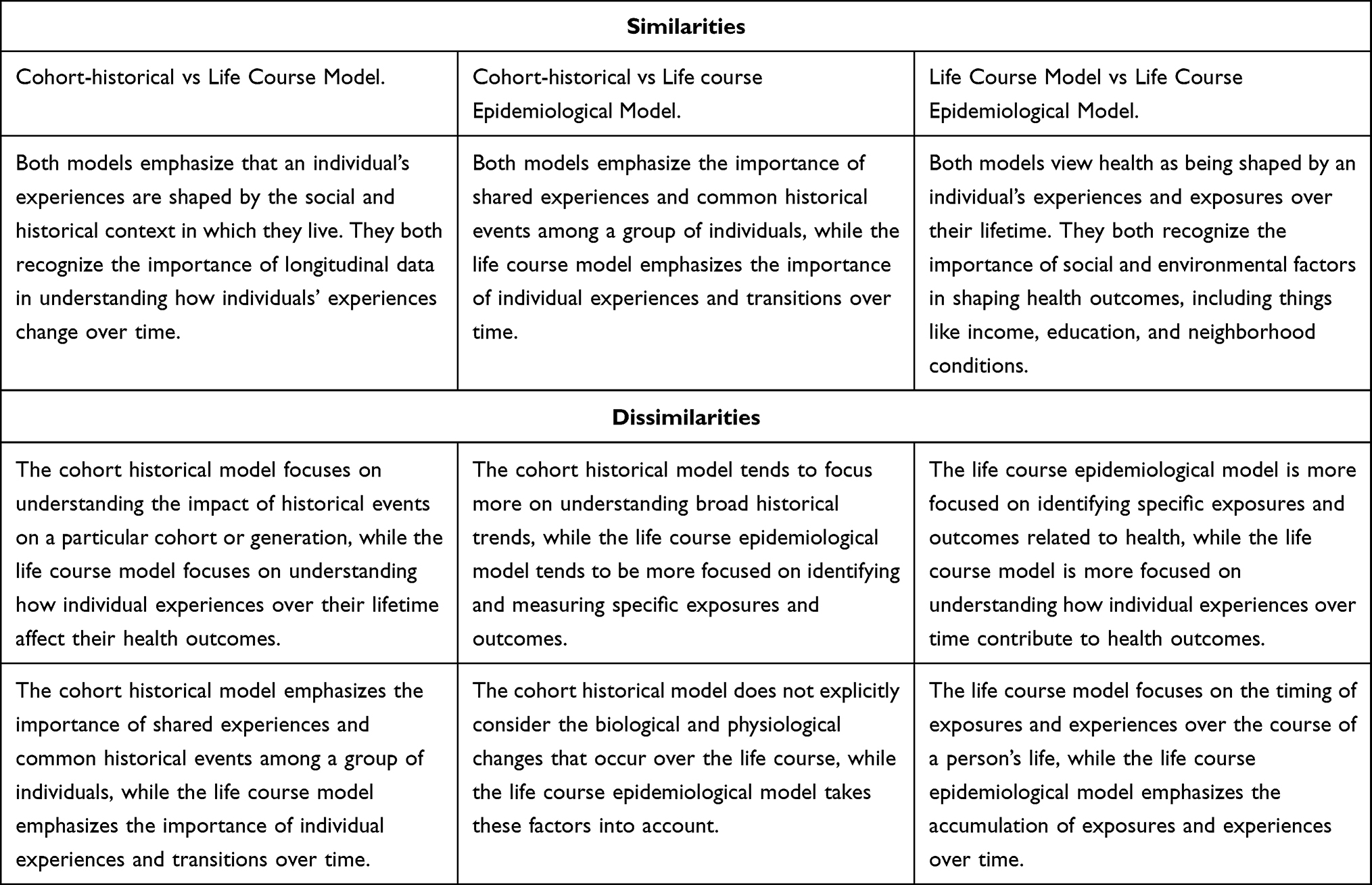 |
Table 1 Similarities and Dissimilarities Among the Cohort-Historical; Life Course, and Life Course Epidemiological Models |
Instead of positioning contraceptive use as an independent isolated event, the life course epidemiological view takes into consideration the dynamic process of family formation modulated through contraceptive use while being exposed to the cumulative intrinsic as well as socio-economic and environmental factors impinging on women’s capabilities throughout the course family formation and beyond.
The disparate and somewhat independent development of these theoretical approaches have not yet been impactful on the unmet family planning need research which has been molded by feminist and human rights values to focus on reproductive health aspects more than on population development objectives.40 In essence, research on unmet needs calls for investigative studies on the determinants of unmet needs to focus on the impact of the procedural nature of events including life events differentiated by life stages and life courses.
Though the well-known and well-utilized social determinants approach toward identifying direct factors related to unmet needs41 has indeed proven useful, the same research outcome enunciated by a life course perspective may unfold far more information hidden in the complex relationships among selected determinants of unmet needs.30,42 Consider the use of indicators, such as pregnancy/fertility intention of unmet family planning needs. As indicators of unmet family planning needs, information on “fertility intentions” is sought when the researcher’s interest is in exploring the desired number of children. Pregnancy intentions are of importance if the objective is to reduce the number of unwanted pregnancies and induced abortion; clearly, a reproductive health objective. Responses on intentions could be clear and firm, neutral, or ambivalent. Clarity on intentions may be dependent upon a number of socio-psycho-biological factors impacting contraceptive use decisions. A life course perspective is suitable for extracting the information necessary to promote efficient contraceptive use.
Furthermore, such an approach is of relevance to the human rights agenda underlying the reproductive health perspective on unmet family planning needs. For example, life stage as well as life course epidemiological studies on the effect of son preference on abortion unraveled a far more expansive reproductive health effect than on abortion.29,43 Edmeades, Lee Rife & Malhotra13,14 examined the effect of past life course experiences on contraceptive use and abortion. They utilized the life course perspective to systematically examine factors influencing changes in contraceptive use patterns and found that abortion attempts have over time effects across life stages on contraceptive use. In addition, there are several methodological issues, which need to be considered in tandem with the theoretical views on the concept of unintended pregnancy to grasp the utility of life course and the life course epidemiological to strengthen research on unmet family planning needs.
Implications for Family Planning Capacity Building
Family planning programs have played an important role in addressing the issue of unmet needs in LMICs.44–48 Community Health Family Planning workers have effectively increased the use of modern contraception.49,50 This approach has increased reliance and dependence on researchers of unmet needs, and policymakers to generate a large amount of knowledge to help guide family planning workers.26,51 In this regard, life course and life course epidemiological approaches are helpful in generating data to help women improve contraceptive use capacities. Greater exploration of women’s views on their contraceptive use needs and expectations could lead to increased knowledge and more effective discussions with family planning workers and healthcare providers resulting in a greater likelihood of informed contraceptive choice.
Though the objective and goals of research on unmet family planning needs may differ across a wide spectrum and context in which research is undertaken, the life course framework provides guidance with regard to categorizing and organizing information.36,52–54 For example, the Cohort historical model and life course approaches suggest gathering information on a number of current and past demographic attributes and individual-level risk, and protective factors. The risk factors expose and increase barriers to acquiring and building contraceptive use capabilities. The protective factors improve an individual’s contraceptive use capabilities.
In this regard, Kuh37,55 proposes a number of suggestions for data generation within the ambit of life course epidemiology. Such data may include information on place of residence at birth, age, class, ethnicity, and family or origin. The data on life stage-specific characteristics may include, information on specific events of significance; both risk and protective to the individual in terms of bringing about long-lasting effects. A focus on events that can be considered “turning points” is valuable. In case of illness, information on duration, and time of occurrence is useful Data related to this dimension may focus on relevant exposure that may intensify or abate past and current risk and protective factors linked to contraceptive use capability. Researchers may ask if there are “transitions” and “turning points”, such as status changes that may be associated with either intensification or abatement of risk and protective factors. Data related to the onset of illness and factors that either intensify or reduce individuals’ assessment of contraceptive use capability as well as data on risk and protective factors that influence capacity and resilience to overcome barriers and promote contraceptive use capability can be potentially useful for family planning counselors and workers.
Discussion
The global vision of meeting the need for family planning among women of reproductive ages has not yet been realized even as supply-oriented strategies have been successful in improving the availability and access to family planning services. But this alone is not enough to address the unmet need for family planning. A person-centered approach that considers multilevel factors can help inform the development of more effective family planning programs. In this respect, the impact of life events and reproductive health problems loom large significantly influencing contraceptive use decisions.
By taking a life course perspective, researchers can identify individual-level, social and cultural, and structural factors that may influence family planning decisions and develop tailored interventions that meet the specific needs of individuals and populations at different stages of life.
For example, studies utilizing life course theory have investigated the psychological and social impact of reproductive health problems and found that contraceptive use interventions may need to be tailored to the specific needs of women at different life stages.
By addressing unmet family planning need early in the life course, these frameworks can help prevent long-term reproductive health consequences associated with unintended pregnancies and promote better health outcomes for both individuals and their families. A more intersectional approach to research that considers the social and cultural contexts in which women’s reproductive health decisions are made is also necessary to address the gaps in our understanding of unmet family planning need in developing countries.
In general, research on unmet family planning needs is essential to achieve several targets under the reproductive health objectives related to SDG 3.7.1 goals. Studies using developmental theoretical frameworks are likely to be useful for strengthening the role of family planning workers throughout the developing world. In this regard, this is a clarion call for a broader range of research on unmet family planning needs. Family planning programs focused on reducing unmet need still remains our best course of action to achieve several targets under the reproductive health objectives related to SDG 3.7.1 goals. Research studies on unmet family planning needs using developmental theoretical frameworks are likely to be useful for strengthening the role of family planning workers throughout the developing world.
Abbreviation
USAID, United States Agency for International Development.
Ethics Approval and Consent to Participate
Ethics clearance was not necessary as no primary data collection was conducted.
Funding
There is no funding received from any source in support of this work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Tone A. Devices and Desires: A History of Contraceptives in America. Macmillan; 2002.
2. Furgerson J. The Battle for Birth Control: Exploring the Lasting Consequences of the Movement’s Early Rhetoric. Rowman & Littlefield; 2022.
3. Krovi SA, Johnson LM, Luecke E, Achilles SL, van der Straten A. Advances in long-acting injectables, implants, and vaginal rings for contraception and HIV prevention. Adv Drug Deliv Rev. 2021;176:113849. doi:10.1016/j.addr.2021.113849
4. Chandrasekhar S. A Dirty, Filthy Book: The Writings of Charles Knowlton and Annie Besant of Reproductive Physiology and Birth Control and an Account of the Bradlaugh-Besant Trial. University of California Press; 1981.
5. Therien JP. Beyond the North-South divide: the two tales of world poverty. Third World Q. 1999;20(4):723–742. doi:10.1080/01436599913523
6. Bracke MA. Women’s rights, family planning, and population control: the emergence of reproductive rights in the united nations (1960s–70s). Intern Hist Rev. 2022;44(4):751–771. doi:10.1080/07075332.2021.1985585
7. Ahmed Z. The unprecedented expansion of the global gag rule: trampling rights, health and free speech. Guttmacher Policy Rev. 2020;23:13–18.
8. Biswas RK, Farzana M, Bhar S, Bhowmik J. Contraceptive use in South and South-East Asian region: assessment of sustainable development goal 3.7 through indicator 3.7.1. J Public Health. 2022;105. doi:10.1093/pubmed/fdac105
9. Bearak J, Popinchalk A, Ganatra B, et al. Unintended pregnancy and abortion by income, region, and the legal status of abortion: estimates from a comprehensive model for 1990–2019. Lancet Global Health. 2020;8(9):e1152–e1161. doi:10.1016/S2214-109X(20)30315-6
10. Hellwig F, Coll CV, Ewerling F, Barros AJ. Time trends in demand for family planning satisfied: analysis of 73 countries using national health surveys over a 24-year period. J Glob Health. 2019;9(2). doi:10.7189/jogh.09.020423
11. Uthman MK, Bello IS, Fadugbagbe AO, Olajubu TO, Ismail WO, Ibrahim AO. Unmet needs for family planning and its determinants among women of reproductive age in Ilesha Southwest Nigeria: a cross-sectional study. J Med Access. 2022;6:27550834221115979. doi:10.1177/27550834221115979
12. Ofurum IC, Mba OG, Enyindah CE. Factors associated with unmet needs for family planning among people living with HIV/AIDS in the South-South Region of Nigeria. J Adv Med Pharm Sci. 2023;251:10–22.
13. Ewerling F, Victora CG, Raj A, Coll CV, Hellwig F, Barros AJ. Demand for family planning satisfied with modern methods among sexually active women in low-and middle-income countries: who is lagging behind? Reprod Health. 2018;15:1. doi:10.1186/s12978-018-0483-x
14. Kulczycki A. Overcoming family planning challenges in Africa: toward meeting unmet need and scaling up service delivery. Afr J Reprod Health. 2018;221:9–19.
15. Woldemicael G, Beaujot R. Currently married women with an unmet need for contraception in Eritrea: profile and determinants. Can Stud Popul. 2011;38(1–2):61–81. doi:10.25336/P6GS4S
16. Bansal A, Dwivedi LK, Shirisha P. Sterilization incentives and associated regret among ever married women in India, NFHS, 2015–16. BMC Health Serv Res. 2022;22(1):1063. doi:10.1186/s12913-022-08401-8
17. Ali M, Azmat SK, Hamza HB, Rahman MM. Assessing effectiveness of multipurpose voucher scheme to enhance contraceptive choices, equity, and child immunization coverage: results of an interventional study from Pakistan. J Multidiscip Healthc. 2020;13:1061–1074. doi:10.2147/JMDH.S245900
18. Sedgh G, Hussain R. Reasons for contraceptive nonuse among women having unmet need for contraception in developing countries. Stud Fam Plann. 2014;45(2):151–169. doi:10.1111/j.1728-4465.2014.00382.x
19. Waidler J, Gilbert U, Mulokozi A, Palermo T. A “Plus” Model for safe transitions to adulthood: impacts of an integrated intervention layered onto A national social protection program on sexual behavior and health seeking among tanzania’s youth. Stud Fam Plann. 2022;53(2):233–258. doi:10.1111/sifp.12190
20. Jabeen S, Rathor A, Riaz M, Zakar R, Fischer F. Demand-and supply-side factors associated with the use of contraceptive methods in Pakistan: a comparative study of demographic and health surveys, 1990–2018. BMC Womens Health. 2020;20(1):1. doi:10.1186/s12905-020-01112-4
21. Akter T, Festin M, Dawson A. Hormonal contraceptive use and the risk of sexually transmitted infections: a systematic review and meta-analysis. Sci Rep. 2022;12(1):20325. doi:10.1038/s41598-022-24601-y
22. Sharma S, Saxena V, Mundhra R, Garg D, Mallick BK, Bahadur A. Pattern and clinico-epidemiological profile of female patients of RTI/STIs attending an STI clinic in Uttarakhand, India. J Fam Med Prim Care. 2022;11(11):7357–7361. doi:10.4103/jfmpc.jfmpc_1397_22
23. Parve S, Acharya S, Rawat S, Kulkarni R. A study of sexually transmitted infections and reproductive tract infections among the bar girls in Mumbai, India. J Fam Med Prim Care. 2023;12(1):10–14. doi:10.4103/jfmpc.jfmpc_216_21
24. Fabic MS, Choi Y, Bongaarts J, et al. Meeting demand for family planning within a generation: the post-2015 agenda. Lancet. 2015;385(9981):1928–1931. doi:10.1016/S0140-6736(14)61055-2
25. Senderowicz L, Maloney N. Supply-side versus demand-side unmet need: implications for family planning programs. Popul Dev Rev. 2022;48(3):689–722. doi:10.1111/padr.12478
26. Gold N, Viviano M, Yaron M. Contraception: what is the resistance all about? Eur J Contracept Reprod Health Care. 2021;26(1):62–72. doi:10.1080/13625187.2020.1837362
27. Maqbool S, Shan H, Qureshi I, Shaheen L. Barriers to use contraceptive methods among post-abortion clients in Sargodha, Pakistan. Malaysian J Public Health Med. 2022;22(1):220–226. doi:10.37268/mjphm/vol.22/no.1/art.1397
28. Guillaume A, Du Loû AD. Fertility regulation among women in Abidjan, Côte d’Ivoire: contraception, abortion or both? Int Fam Plann Persp. 2002;28(3):159–166. doi:10.2307/3088259
29. Edmeades J, Lee Rife SM, Malhotra A. Women and reproductive control: the nexus between abortion and contraceptive use in Madhya Pradesh, India. Stud Fam Plann. 2010;41(2):75–88. doi:10.1111/j.1728-4465.2010.00228
30. Edmeades J. The legacies of context: past and present influences on contraceptive choice in Nang Rong, Thailand. Demography. 2008;45(2):283–302. doi:10.1353/dem.0.0004
31. Hindin MJ. Women’s autonomy, women’s status and fertility-related behavior in Zimbabwe. Popul Res Pol Rev. 2000;19(3):255–282. doi:10.1023/A:1026590717779
32. Zimmerman LA, Sarnak DO, Karp C, et al. Family planning beliefs and their association with contraceptive use dynamics: results from a longitudinal study in Uganda. Stud Fam Plann. 2021;52(3):241–258. doi:10.1111/sifp.12153
33. Ryder NB. The Cohort as a concept in the study of social change. Am Sociol Rev. 1965;30(6):843–861. doi:10.2307/2090964
34. Pillai VK. The postwar rise and decline of American fertility: the pace of transition to motherhood among 1950–1969 marital cohorts of white women. J Fam Hist. 1987;12(4):421–436. doi:10.1177/036319908701200405
35. Elder GH Jr. Time, human agency, and social change: perspectives on the life course. Social Psychol Quar. 1994;57(1):4–15. doi:10.2307/2786971
36. Elder GH, Johnson MK, Crosnoe R. The emergence and development of life course theory. In: Handbook of the Life Course. Boston, MA: Springer; 2003:3–19.
37. Kuh D, Hardy R. A Life Course Approach to Women’s Health. Oxford University Press; 2002.
38. Spallek J, Zeeb H, Razum O. What do we have to know from migrants’ past exposures to understand their health status? A life course approach. Emerg Themes Epidemiol. 2011;8(1):6. doi:10.1186/1742-7622-8-6
39. Blane D, Netuveli G, Stone J. The development of life course epidemiology. Revue d’Épidémiologie et de Santé Publique. 2007;55(1):31–38. doi:10.1016/j.respe.2006.12.004
40. Cook RJ. International human rights and women’s reproductive health. Women Med Ethics Law. 2020;10:37–50.
41. Wulifan JK, Brenner S, Jahn A, De Allegri M. A scoping review on determin ants of unmet need for family planning among women of reproductive age in low and middle-income countries. BMC Womens Health. 2015;16(1):1–5.
42. Wilson LC, Rademacher KH, Rosenbaum J, et al. Seeking synergies: understanding the evidence that links menstrual health and sexual and reproductive health and rights. Sex Reprod Health Matters. 2021;29(1):44–56. doi:10.1080/26410397.2021.1882791
43. Maximova K, Quesnel-Vallée A. Mental health consequences of unintended childlessness and unplanned births: gender differences and life course dynamics. Soc.Sci.Med. 2009;68(5):850–857. doi:10.1016/j.socscimed.2008.11.012
44. Sunil TS, Pillai VK, Pandey A. Do incentives matter?–Evaluation of a family planning program in India. Popul Res Pol Rev. 1999;18(6):563–577. doi:10.1023/A:1006386010561
45. Mehata S, Paudel YR, Mehta R, Dariang M, Poudel P, Barnett S. Unmet need for family planning in Nepal during the first two years postpartum. BioMed Res Int. 2014;2014:649567. doi:10.1155/2014/64956
46. Simmons R, Baqee L, Koenig MA, Phillips JF. Beyond supply: the importance of female family planning workers in rural Bangladesh. Stud Fam Plann. 1988;19(1):29–38. doi:10.2307/1966737
47. Sharma SK, Pratap N, Ghimire DR. Ethnic differentials of the impact of Family Planning Program on contraceptive use in Nepal. Demogr Res. 2011;25:837–868. doi:10.4054/DemRes.2011.25.27
48. Merki-Feld GS, Caetano C, Porz TC, Bitzer J. Are there unmet needs in contraceptive counselling and choice? Findings of the European TANCO Study. Eur J Contracept Reprod Health Care. 2018;23(3):183–193. doi:10.1080/13625187.2018.1465546
49. Zhu D, Chung HF, Dobson AJ, et al. Age at natural menopause and risk of incident cardiovascular disease: a pooled analysis of individual patient data. Lancet Public Health. 2019;4(11):e553–64. doi:10.1016/S2468-2667(19)30155-0
50. Scott VK, Gottschalk LB, Wright KQ, et al. Community health workers’ provision of family planning services in low and middle-income countries: a systematic review of effectiveness. Stud Fam Plann. 2015;46(3):241–261. doi:10.1111/j.1728-4465.2015.00028
51. Rossier C. Attitudes towards abortion and contraception in rural and urban Burkina Faso. Demogr Res. 2007;17:23–58. doi:10.4054/DemRes.2007.17.2
52. Pampel FC, Krueger PM, Denney JT. Socioeconomic disparities in health behaviors. Annu Rev Sociol. 2010;36:349–370. doi:10.1146/annurev.soc.012809.102529
53. Elder GH. The life course as developmental theory. Child Dev. 1998;69(1):1–20. doi:10.1111/j.1467-8624.1998.tb06128.x
54. Brady SS, Bavendam TG, Berry A, et al. The Prevention of Lower Urinary Tract Symptoms (PLUS) in girls and women: developing a conceptual framework for a prevention research agenda. Neurourol Urodyn. 2018;37(8):2951–2964. doi:10.1002/nau.23787
55. Kuh D, Ben-Shlomo Y, Lynch J, Hallqvist J, Power C. Life course epidemiology. J Epidemiol Community Health. 2003;57(10):778. doi:10.1136/jech.57.10.778
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.