Back to Journals » Integrated Pharmacy Research and Practice » Volume 13
Unlicensed “Special” Medicines: Using the Pillar Integration Model to Understand Stakeholder Perspectives Across Care Settings
Authors Wale A ![]() , Mantzourani E
, Mantzourani E ![]()
Received 11 July 2024
Accepted for publication 10 October 2024
Published 27 November 2024 Volume 2024:13 Pages 209—228
DOI https://doi.org/10.2147/IPRP.S477087
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Professor Walid Al-Qerem
Alesha Wale, Efi Mantzourani
Cardiff School of Pharmacy and Pharmaceutical Sciences, Cardiff University, Cardiff, Wales, UK
Correspondence: Efi Mantzourani, Cardiff School of Pharmacy and Pharmaceutical Sciences, Cardiff University, Cardiff, Wales, UK, Tel +44 2920 870452, Email [email protected]
Background: The use of unlicensed medicines has been associated with safety concerns, availability and accessibility issues, and lack of integrated care across care settings.
Objective: To understand the interaction between the views and experiences of those who prescribe, those who supply and those who receive unlicensed “special” medicines, so that factors affecting the patient journey and successful treatment can be identified and used to inform areas for change.
Methods: A qualitative, phenomenological approach was adopted, with semi-structured interviews with prescribers, community pharmacy staff and patients. A combination of stratified, purposive, snowball and convenience sampling was used to identify participants. Interviews were analysed using reflexive thematic analysis and the findings were integrated using an adapted model of the Pillar Integration Process.
Results: Three pillars were constructed after synthesising results from interviews with patients (n=4), prescribers (n=5) and pharmacy staff (n=6): the awareness of licensing status; perceptions of patient care and acceptability of unlicensed medicine use; and challenges associated with the accessibility of unlicensed medicines. The varying levels of awareness when unlicensed medicines are prescribed and the varying perceptions of responsibility and acceptability of the use of unlicensed medicines help to explain the challenges faced by participants across the patient journey, Challenges identified included understanding what unlicensed medicines are, awareness of the licensing status when unlicensed medicines are prescribed, managing care across care settings to ensure the patient is effectively treated and ensuring continuity of care for patients in the community.
Conclusion: The results highlight a clear need for more integrated care and support for prescribers to reduce the chances of delays between care settings, and more patient-centred care to ensure that any delays when accessing medicines do not lead to treatment disruption for the patient. The new national guidelines informed by findings of this study can support policy-makers across the globe.
Keywords: unlicensed medicine, off-label medicine, prescriber, patient, community pharmacy, patient experience, qualitative, pillar integration model
Introduction
Unlicensed medicines are used commonly in the UK. The term unlicensed medicine encompasses different types of medicines, including extemporaneous preparations, off-label medicines and unlicensed “special” medicines. Off-label medicines are medicines which have been licensed for a specific use in a specific population but are used in a way not specified by the marketing authorisation in the Summary of Product Characteristics (SPC),1 and as such, are used in an unlicensed manner. Unlicensed “special” medicines do not have a marketing authorization. In the UK, regulation 167 of the Human Medicines regulation outlines the exceptions in which a medicine can be supplied without a license.2 Manufactures must hold a manufacturer’s “specials” license to produce “specials”, and they should only be prescribed when there is no alternative licensed medicinal product available to meet the special clinical needs of an individual patient.1–3 Examples of special clinical needs include patients who suffer from rare diseases,4 those unable to take a licensed medicine, for example patients with dysphagia,5 or those who are allergic to specific excipients.6
Prescribers have the important role of determining when the use of unlicensed “special” medicines may be necessary, discussing their decision-making with the patients, and deciding together whether to initiate a therapy via prescribing such medicines, or continue prescriptions for products initiated previously by another prescriber. In line with the Medicines and Healthcare products Regulatory Agency’s (MHRA) guidance,7 prescribers should only prescribe an unlicensed medicine if there are no licensed alternatives available to meet the clinical needs of the patient. The MHRA also states that, even though off-label use of medicines is not recommended, it is preferred to use of a “special”, if it meets the clinical need of the patient.1 However, evidence has shown that the guidance available to healthcare professionals can be confusing and can contain inconsistent information about what unlicensed medicines are,8 which inevitably impacts on prescribers’ attitudes towards initiating or maintaining therapy with an unlicensed medicine.
Community pharmacy is the first point of contact for patients and community pharmacists have a vital role in ensuring unlicensed medicines can be accessed. The role of a community pharmacist has evolved overtime from checking and dispensing medicines to a more patient-focussed role, such as assisting patients in self care of minor conditions or running successful interventions, such as smoking cessation services.9,10 Difficulties for community pharmacy staff accessing unlicensed medicines relate to the cost, storage and often short expiry dates. The available literature from within the UK has highlighted that patients have experienced issues when accessing their unlicensed medicines after discharge, with pharmacy staff being unable to find a supplier or manufacturer for a certain product or specific formulation,11,12 although this was reported from the patient perspective.
Wale et alconducted a systematic review to better understand factors affecting the patient journey and patient care when receiving an unlicensed “special” medicine, highlighting a clear need for consistent information to be provided to healthcare professional and patients alike to support the safe and effective use of unlicensed medicines across care settings.13 No studies were identified whereby the views and experiences of prescribers, pharmacists and patients were triangulated using an appropriate framework, to obtain a holistic perspective. By obtaining an insight into the views and perceptions of those who prescribe, supply or receive unlicensed medicines, factors affecting the patient journey and successful treatment can be identified and used to inform areas for change, while supporting previous evidence or highlighting findings specific to patients in different localities. As such, the aim of this study was two-fold: to first explore the views and experiences of prescribers, in primary and secondary care, who have experience of initiating or maintaining therapy with unlicensed “special” medicines, pharmacists in the community who obtain and supply unlicensed “special” medicines, and patients (or the parents and carers of those) who receive unlicensed “special” medicines in the community; to then understand the interaction between prescriber, pharmacist and patient views as well as the impact on patient care.
Methods
A qualitative phenomenological approach was taken involving semi-structured interviews of three stakeholder groups involved in the patient’s journey: prescribers in primary and secondary care, community pharmacists, and patients or parents and carers of those who receive unlicensed medicines. This paper is based on the thesis of Wale, A.14 An inductive thematic analysis of interviews with the community pharmacy sample has been published elsewhere,15 but for the purpose of this study all findings were re-analysed with an adapted version of the Pillar Integration Process16 in order to triangulate the findings from the different population groups involved.
Sample
A combination of stratified, purposive, snowball and convenience sampling was used to identify participants. The sampling frame included patients and the parents/carers of patients who were currently being prescribed an unlicensed “special” medicine and were receiving this in the community in Wales (this sample will hereto be referred to as the patient group); prescribing clinicians working in primary and secondary care in Wales, with experience in prescribing unlicensed “special” medicines; community pharmacy staff with experience ordering and supplying unlicensed “special” medicines. Eligibility criteria for the interviews can be seen in Table 1.
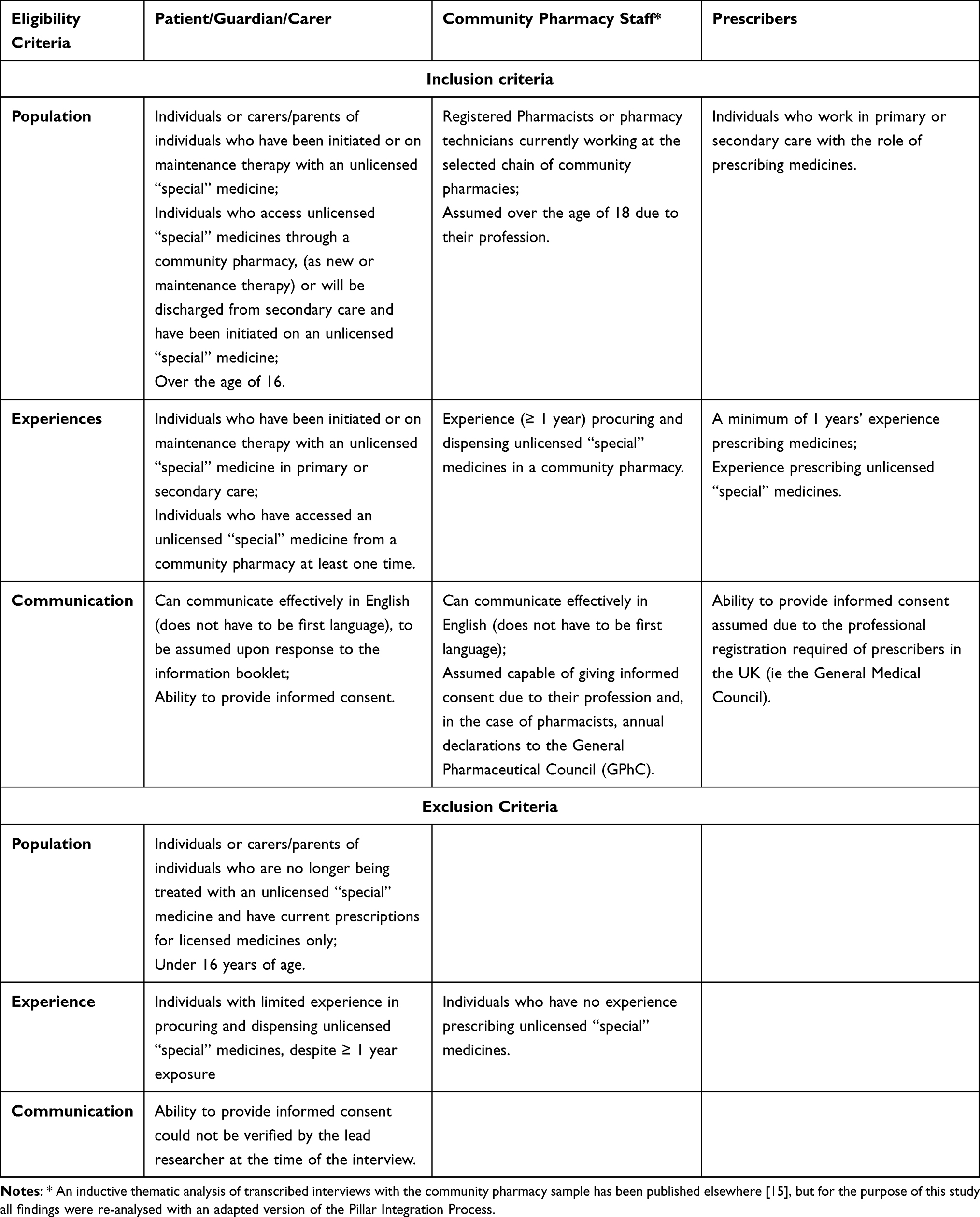 |
Table 1 Eligibility Criteria for the Interviews with the Three Stakeholder Groups in the Sampling Frame: Patients and the Parents/Carers of Patients; Prescribing Clinicians Working in Primary and Secondary Care; Community Pharmacy Staff |
Recruitment
Participants in the patient group were recruited in a number of ways including online advertisements, through community pharmacies and within secondary care. The lead author (AW) contacted HealthWise Wales (an online platform with a register of members of the public who have agreed to be informed about research).17 The study advert was disseminated in a newsletter through email to their members across Wales. Patients were also recruited directly through their community pharmacy after the lead author had disseminated the study documents to multiple community pharmacies. When recruiting from secondary care, some gatekeepers from the different organisations responsible for planning and providing health and wellbeing services (health boards) where the hospitals were based agreed to disseminate the study information directly to individuals within the departments that were reported by stakeholders14 as using unlicensed medicines more frequently (paediatrics, dermatology and gastroenterology), while others provided contact details for key hospital staff who would act as gatekeepers themselves, for the lead author to reach out to directly.
Community pharmacy staff were recruited from a small chain of community pharmacies in South Wales. One pharmacist agreed to act as a gatekeeper in recruiting other pharmacists and pharmacy technicians. The gatekeeper was sent a personalised email invitation containing all relevant study information and disseminated this information by email to all other pharmacists and pharmacy technicians who fit the eligibility criteria.
Prescribers were recruited from primary and secondary care. Health board facilitators were asked to provide contacts within gastroenterology, dermatology and paediatric departments who could act as gatekeepers for the study. Where the health board facilitator agreed to act as a gatekeeper, the lead author sent the study information directly to them to be disseminated to potential participants. Where contacts were provided, the author then contacted the individuals and sent them the study information asking them to act as a gatekeeper for the study and to disseminate the study documents to potential participants.
All participants were self-selected; participants were provided with a cover letter and an information sheet with the contact details of the research team. If a participant wished to take part in an interview, they were asked to contact the research team directly, the lead author then contacted the participants and arranged a suitable time to conduct the interview.
Data Collection
Semi-structured interviews were conducted to allow participants to address individual experiences or perceptions that may not have been identified in the existing literature. Topic guides for the interviews were informed by literature and finalised in collaboration with external stakeholders, part of the study’s steering group. Further details about the interview schedules and an in-depth description of the methods used has been published elsewhere.14 Using the principles of information power,18 it was estimated that between 4–5 participants from all different populations would be needed to gain valuable data across Wales, to account for a representative sample. Interviews were conducted by the lead author (AW), either in person or online, lasting between 10–40 minutes. Data collection for community pharmacy staff was conducted between September 2018 until January 2019. Data collection for prescribers and patients was conducted during the COVID-19 period between November 2020 and continued until June 2021. All interviews were audio-recorded, with consent, either via Microsoft Teams™ or a recorder and transcribed verbatim, with audio recordings being deleted directly after transcription. Informed consent included the publication of anonymised responses and direct quotes.
Data Analysis
Data was first analysed for the three qualitative samples using reflexive thematic analysis with an inductive approach, following the method suggested by Braun and Clarke.19 Even though the data was only qualitative, it came from three sources and a robust and transparent process for integrating findings was sought. An adapted model of the Pillar Integration Process was developed to allow for data from the three separate qualitative studies to be integrated, based on the four stages of integration outlined by Jonson et al.16 The qualitative data gained from prescribers was analysed first, followed by the qualitative data gained from community pharmacy staff and patients/carers.
One member of the research team (EM) was a pharmacist. To minimise any risk of bias in the data analysis, transcribing was completed initially by the other member of the team (AW), and checked by EM. Mapping against the PIP was conducted independently by both researchers and any identified differences were discussed and resolved.
Ethical Considerations
When recruiting community pharmacy staff, the community pharmacy chain approved the research within their company. Approvals were also sought from Cardiff University’s School of Pharmacy and Pharmaceutical Sciences Research Ethics Committee and ethical approval was granted on the 9th of August 2018. For the recruitment of prescribers and patients full Health Research Authority and Health and Care Research Wales approvals were granted on 23rd December 2019. This report has been based on the Standards for Reporting Qualitative Research (Supplementary File 1).20
Results
Qualitative Analysis for Prescribers
A total of five participants took part in an interview, four were primary care prescribers and one was a secondary care prescriber. Reflexive thematic analysis of transcribed interviews was used to construct three themes: understanding of what unlicensed “special” medicines are, acceptability of their use and awareness of licence status when prescribing; factors influencing the confidence and decision to prescribe unlicensed “special” medicines; and patient interactions and perceived patient awareness of licensing status and acceptability of the therapy received.
Qualitative Analysis for Community Pharmacy Staff
A total of six participants took part and completed an interview, five pharmacists and one pharmacy technician. Reflexive thematic analysis of transcribed interviews revealed three main themes: requirement for additional patient responsibilities; influences on the confidence felt by pharmacy staff when accessing and supplying unlicensed “special” medicines; and continuity of supply.
Qualitative Analysis for Patients
A total of four patients took part and completed an interview, two were patients receiving unlicensed “special” medicines themselves and two were parents accessing unlicensed “special” medicines for their child. Through reflexive thematic analysis three themes were constructed: awareness of licensing status and acceptability of receiving an unlicensed “special” medicine; patient perceptions of healthcare professionals impacted by issues experienced; and strategies adopted by patients to ensure timely access and continuity of supply when receiving unlicensed “special” medicines.
Integration of Qualitative Results
The results were synthesised together using an adapted version of the Pillar Integration Process. After integration three main pillars were constructed; the awareness of licensing status; perceptions of patient care and acceptability of unlicensed medicine use; and challenges associated with the accessibility of unlicensed medicines (Tables 2, 3 and 4).
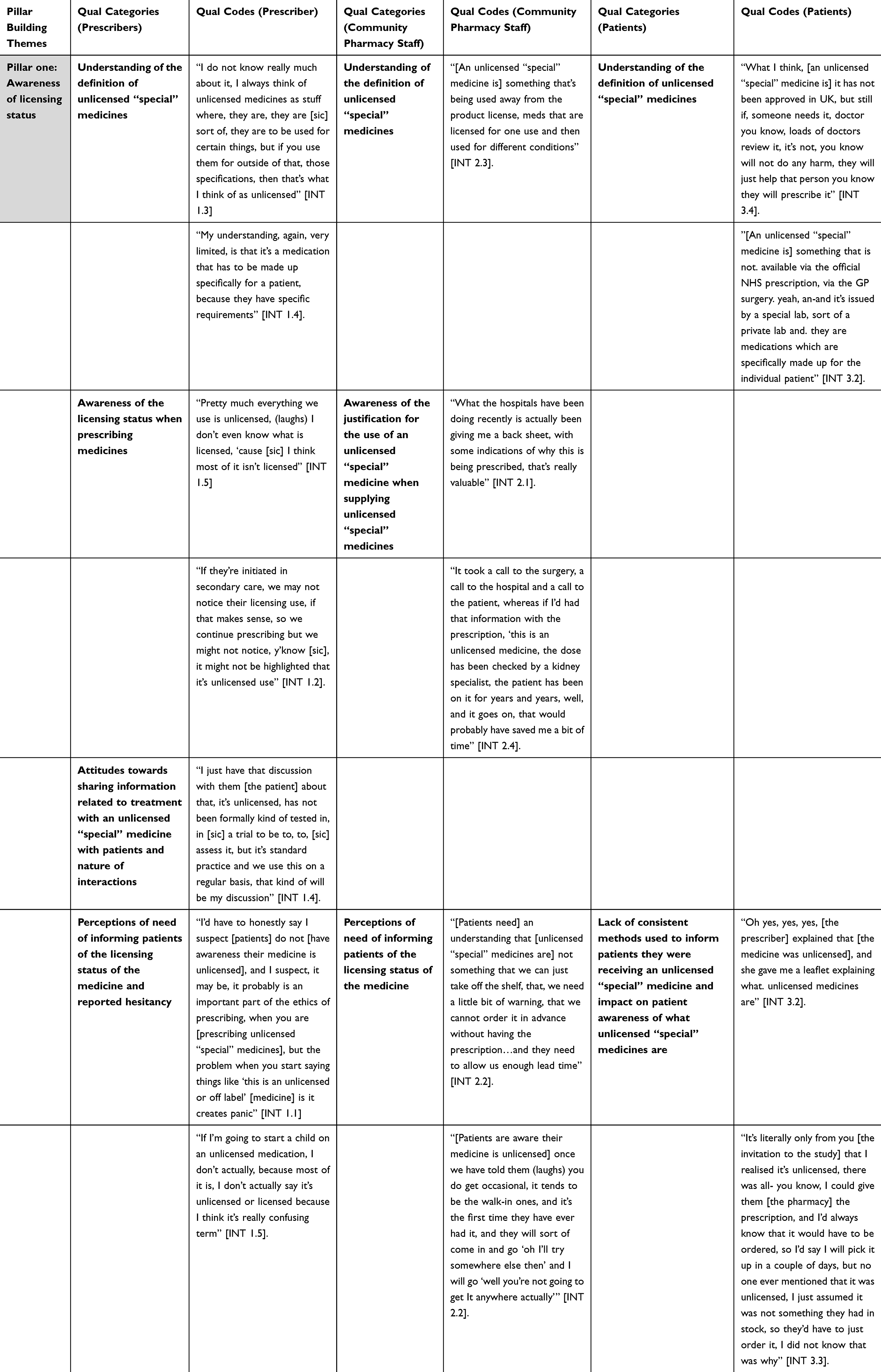 |
Table 2 Pillar One of the Adapted Pillar Integration Model, Constructed After Integration of Results from the Three Qualitative Studies |
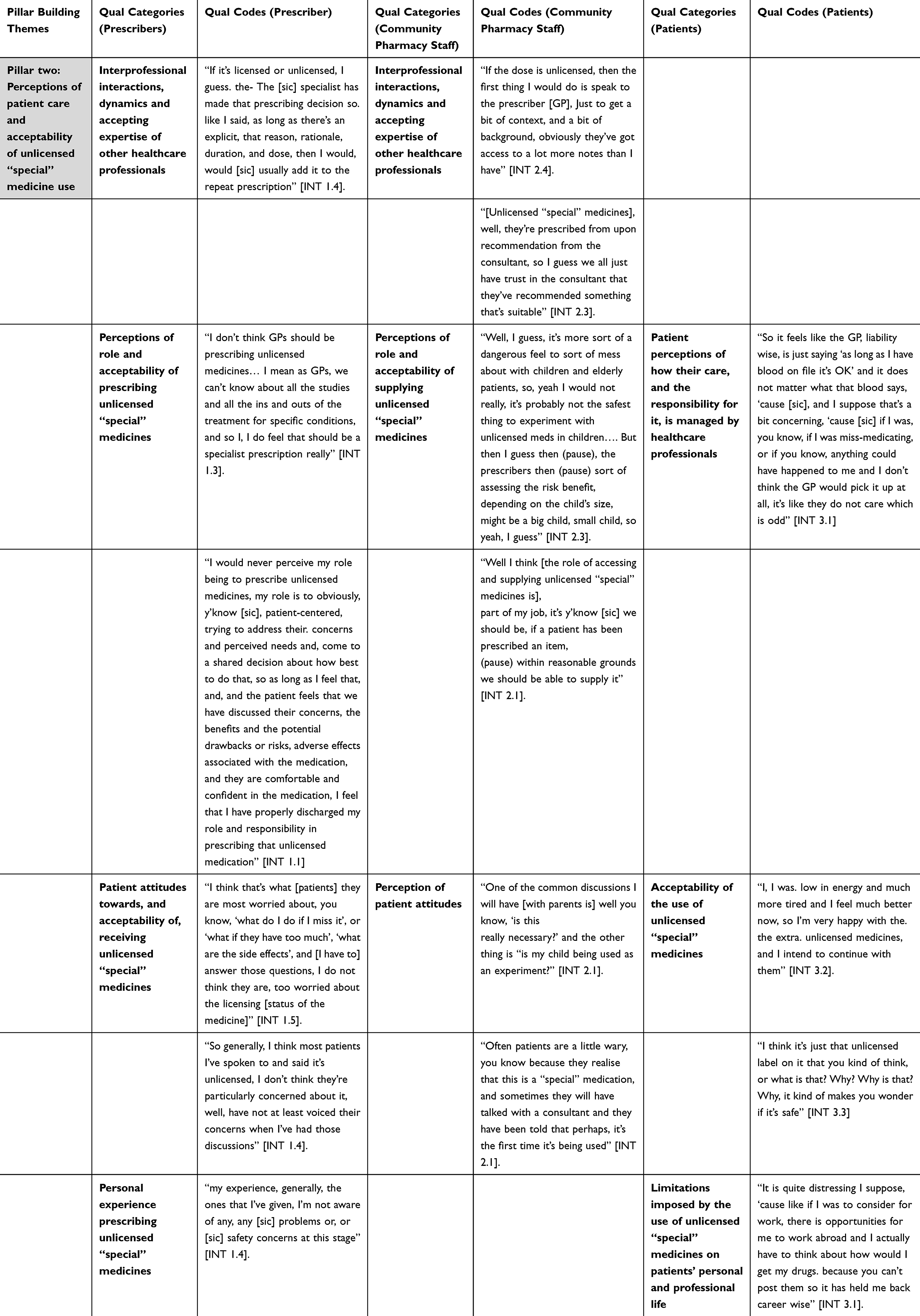 |
Table 3 Pillar Two of the Adapted Pillar Integration Model, Constructed After Integration of Results from the Three Qualitative Studies |
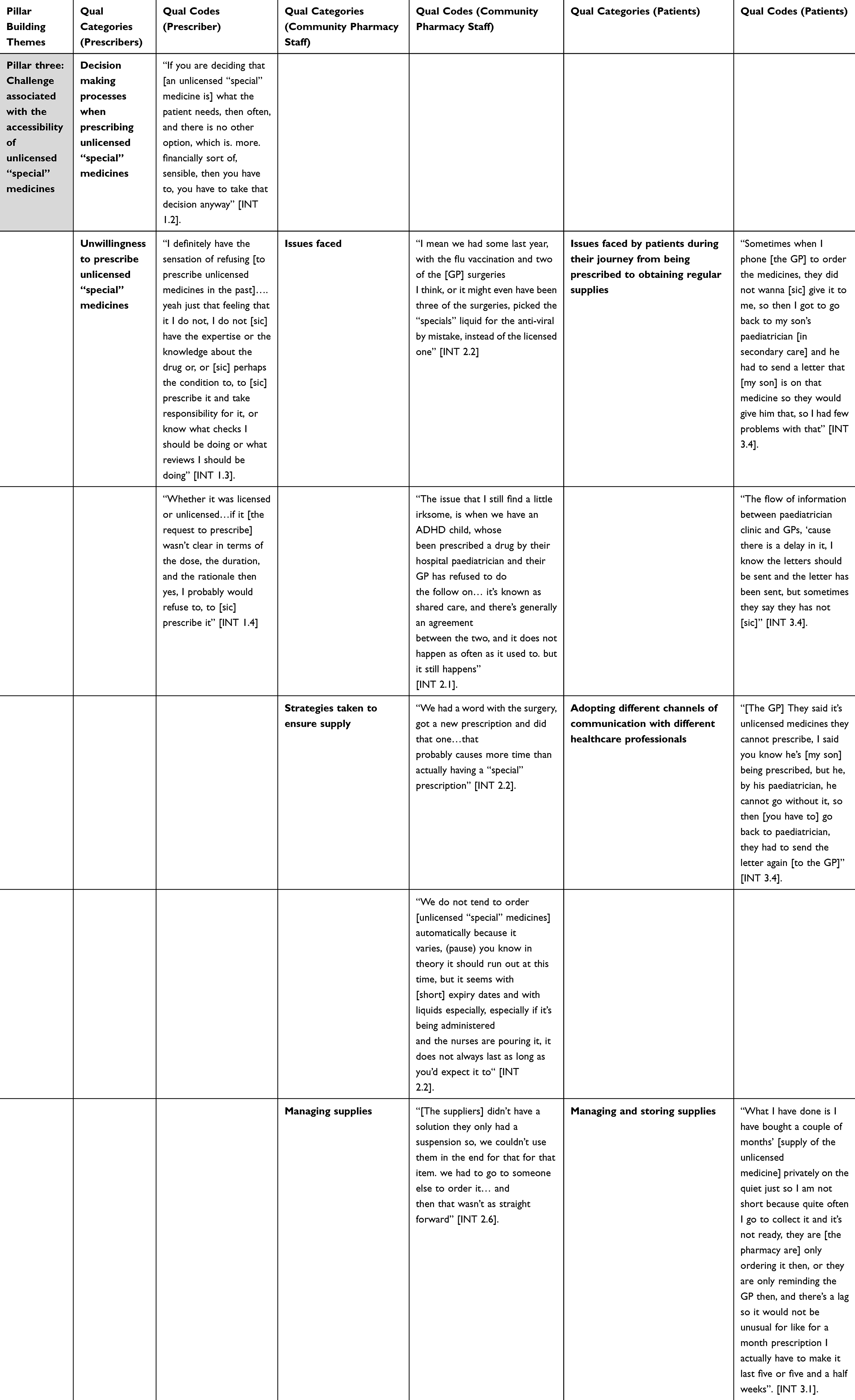 |
Table 4 Pillar Three of the Adapted Pillar Integration Model, Constructed After Integration of Results from the Three Qualitative Studies |
Pillar One: Awareness of Licensing Status
Qualitative findings from the prescriber and patient groups revealed varying levels of understanding around the licensing status of medicines. Prescribers reported differing definitions for what an unlicensed “special” medicine is, and the term off-label was often used interchangeably with “special” medicine, reiterating the confusion around the terminology and definition around unlicensed medicines. They highlighted how, when they were asked to continue in primary care prescriptions that originated in secondary care, it may not be adequately noted when a medicine is unlicensed. This led to a lack of awareness of the licensing status on the part of some GPs, with one GP explaining how they had looked through the repeat prescriptions they had signed in preparation for the interview, and discovered they had been prescribing unlicensed medicines without realising. The lack of awareness of the licensing status when prescribing unlicensed medicines was not only due to the lack of information provided across care settings, but also as a result of the prescribing software not effectively alerting prescribers when unlicensed medicines were selected.
As some prescribers described not being confident in their understanding of the terminology around unlicensed medicines, this impacted their decision to inform patients, with some prescribers suggesting that informing patients would lead to concerns or that it was simply too confusing. This was supported from findings from the patient interviews where again differing definitions were provided for what an unlicensed “special” medicine is, with one patient not being aware they were receiving an unlicensed “special” medicine for their child until they were invited to participate in the study. However, the importance of patients being aware when receiving unlicensed “special” medicines was highlighted by community pharmacy staff who stated that due to the short expiry dates and cost of unlicensed “special” medicines, they could not be ordered in advance and stored in the pharmacy. As such, patients were required to order further supplies of their unlicensed “special” medicines in advance, and that if they were not aware of this, the delay in ordering could lead to a delay in accessing the medicine and could lead to treatment delays or disruption.
Pillar Two: Perceptions of Patient Care and Acceptability of Unlicensed “Special” Medicine Use
Qualitative findings from participants in all groups showed varying perceptions of patient care and acceptability of unlicensed “special” medicine use. While some prescribers viewed the use of unlicensed “special” medicines as a last resort and therefore the only available option for the patient, others felt that prescribing of unlicensed “special” medicines should be the responsibility of secondary care prescribers due to their perceived expertise and familiarity with their uses. Pharmacy staff viewed prescribers as having increased expertise and this resulted in a level of trust that, when the medicine had been prescribed, it was suitable Patients also viewed secondary care prescribers as being more responsible, giving as examples how they experienced secondary care prescribers having to repeatedly contact primary care prescribers to ensure the medicine would be supplied. One patient described the primary care prescribers as being “less caring” and “not understanding the patient condition”, which caused the patient concerns about the quality of care they were receiving. This was a direct result of the care they had received, as their GP had decided against prescribing the unlicensed “special” medicine on numerous occasions, which resulted in delays for the patient when accessing their medicine, negatively impacting the doctor-patient relationship. This was coupled with the secondary care doctor having to write letters to repeatedly ask the GP to continue the prescription. It was requested that a note would be added on the medicine box stating “as prescribed by the endocrinologist”, which was interpreted by the patient as the GP only having the administrative role of signing a new prescription, and not being clinically or legally responsible for the continuation of the treatment.
Despite some concerns when prescribing unlicensed “special” medicines all prescribers felt that patients were accepting when prescribed an unlicensed medicine, and they stated they were not aware of any issues after prescribing the medicine. Pharmacy staff on the other hand highlighted specific concerns patients receiving unlicensed “special” medicines occasionally raised, such as the perceived safety of the medicine. During patient interviews, some patients did state that the term “unlicensed” had caused them some concerns about the safety of the medicine, and that needing an unlicensed “special” medicine actually impacted their day to day life, with one patient describing feeling that they could not move away for career opportunities as they did not feel confident they would be able to access their medicine elsewhere. However, overall, patients’ acceptability of receiving an unlicensed “special” medicine was mainly impacted by a cost-benefit analysis between the perceived need for the medicine and the potential risks. Patients described the risk of not receiving the medicine as being more important than the risk of potential side effects. The most frequent concern described by patients was being unable to access their medicines, rather than any safety implications.
Pillar Three: Challenge Associated with the Accessibility of Unlicensed Medicines
Prescribers reported how, when they had experienced more integrated care, such as good quality information transfer between settings or the use of shared care protocols, their confidence in their own practice increased. Similarly, pharmacy staff also reported their confidence increasing when information about the medicine itself and the clinical need for the specific patient was provided to them by the original prescriber. Patients also highlighted the need for further integrated working citing many of the issues with access they had experienced being related to differences in acceptability among healthcare professionals in different care settings or a lack of communication across care settings.
Qualitative findings from pharmacy staff and patients showed how, when prescribers were uncomfortable with, or unwilling to, continue prescriptions for unlicensed “special” medicines, this led directly to challenges for pharmacy staff who were then unable to obtain and supply the medicines and for patients trying to access their medicines. To mitigate this pharmacists reported having to contact GPs and hospital prescribers on behalf of the patients, to ensure the prescription could be accessed, and in some cases having to wait until a different member of the prescribing team who was willing to continue the prescription became available. Patients described having to adopt multiple methods to handle these challenges as well, such as having increased communication with healthcare professionals and managing and ordering supplies to ensure continuity of care. While prescribers in primary care shared their own concerns and reasons that would lead them to be unwilling to prescribe or continue a prescription for an unlicensed “special” medicine initiated in secondary care, pharmacy staff and patients described the impact of this on patient care. As unlicensed “special” medicines require ordering in advance patients described some potentially dangerous methods to ensure continuity of treatment, such as syringing the medicine off the floor when dropped, or buying supplies privately and using the medicine out of date to manage the delays they often experienced with accessing further supplies in the community.
Discussion
This study uses a formal integration tool to triangulate findings from interviews with three key stakeholder groups directly involved throughout the entire patient journey, from the decision to initiate treatment with an unlicensed medicine to the point at which treatment is supplied through a community pharmacy or ends. Overall, results build the body of evidence showing varying levels of awareness around what unlicensed medicines are, varying perceptions of how patient care is managed and varying perceptions of acceptability around the use of unlicensed “special” medicines in general. The findings also suggest that prescribers in primary care may not only be unaware of the challenges patients face when trying to access their unlicensed “special” medicine in the community, but may inadvertently cause challenges to patients and pharmacy staff when being uncomfortable with, or unwilling to continue a prescription that was initiated in secondary care.
Prescribers reported varying levels of understanding around what unlicensed “special” medicines are, often using the term interchangeably with off-label medicines, which could reflect the varying definitions provided in guidance documents for healthcare professionals,8 with the lack of consistency in terminology leading to confusion.21 Prescribers in primary care also reported that when unlicensed medicines were initiated in secondary care, they may be unaware of the licensing status, exacerbated by the prescribing software not effectively alerting them when unlicensed medicines were selected. Similar findings were reported by Donovan et al,22 where prescribers also acknowledged that the prescribing software may not alert them to the licensing status when unlicensed medicines are selected. Issues have also been reported in the wider literature that show other types of alerts on prescribing software are not effective and can sometimes be viewed by prescribers as irrelevant.23 This suggests there needs to be a more effective way to alert prescribers when unlicensed medicines have been selected. Varying levels of understanding and awareness about what unlicensed medicines are have been reported across countries, with many studies highlighting that doctors may be prescribing off-label medicines unknowingly.24 If prescribers are not aware when they have prescribed unlicensed medicines, they would be unable to effectively inform patients of the licensing status of the medicine. This could explain why one of the patients interviewed in this study was unaware their child was receiving an unlicensed “special” medicine and could explain the varying rates in how often patients were informed of the licensing status when prescribed an unlicensed medicine described within the wider literature.25,26
Prescribers also reported varying perceptions of acceptability when prescribing unlicensed “special” medicines, with some primary care prescribers suggesting this should be the responsibility of secondary care prescribers. This view has been reported in previous literature, where GPs have expressed concerns around taking on the legal and clinical responsibility for specialist prescribing that was initiated by another doctor in secondary care, feeling as though they should not be held responsible for someone else’s prescribing decision, especially in an area where they have little experience.27 However, concerns around the safety of unlicensed medicines as well as the legal responsibility have also been reported by secondary care prescribers within the international literature.28–30 This concern arises as prescribers are legally responsible for any prescription they sign and are recommended not to sign a prescription for an unlicensed medicine unless they feel comfortable that the medicine is the most suitable option and has enough evidence to support its use.31 However, when disagreements occur over the responsibility to prescribe, this can leave patients without the medicine they need.32
Transfer of care across settings had been recognised as an area where medication errors often occur.33 Within the literature doctors have expressed the need for integration between primary and secondary care in the UK, believing that the barriers faced between care settings can negatively impact on the quality of care provided to patients.34 The findings from the patient interviews show how the lack of integration between primary and secondary care can directly result in delays or disruptions when trying to access unlicensed “special” medicines in the community, further exacerbating patient concerns around accessibility. The lack of integrated care was also described by community pharmacy staff, who shared examples where primary care prescribers did not feel comfortable to continue a prescription for an unlicensed “special” medicine, and gave examples of prescriptions sent directly by secondary care prescribers where patient-specific information was not provided with the prescription. This led to an increased workload for community pharmacy staff, who had to take steps to access the prescription for the patient, and to try to confirm the clinical need for the medicine. Some of the issues experienced arise as pharmacists are not usually provided with information about discharge medicines.35 Experiencing delays and disruption in this way led to one patient to perceive GPs as less caring and less responsible. The perception of GPs just being responsible for signing the prescription has been reported within the literature by other patients receiving unlicensed medicines.12 This could also reflect the general public’s perception with previous literature suggesting GPs are viewed as “the middle man” and that care would be of higher quality in hospitals.36,37 The findings highlight the importance of informing patients about GP roles and responsibilities so that patients can appreciate when valid concerns arise, and the GP-patient relationship can be improved.
Despite some concerns when prescribing unlicensed “special” medicines, all prescribers felt that patients were accepting of unlicensed “special” medicines when needed. Results from the patient and pharmacy staff interviews highlighted that concerns existed, showing that prescribers may be unaware of concerns patients held and the impact receiving an unlicensed “special” medicine had on the patients’ lives. Despite these concerns, all patients felt like they needed their unlicensed medicine, so much so that the most frequent concern described by patients was being unable to access their medicines. This is in line with the necessity-concerns framework,38 showing that patients perform a cost benefit analysis between the perceived need and the potential risks.
Patients and pharmacy staff highlighted how those who receive unlicensed “special” medicines are required to take on increased responsibilities, and manage access across care settings. Patients taking on specific strategies to manage the ordering of and access to unlicensed medicines has also been reported in England.12 The evidence from this study and the wider literature has shown that patients across the UK may be faced with a need to manage access to unlicensed medicines across care settings, or else put themselves at risk of delays or treatment disruption. This finding further emphasises the importance that patients are informed not only of the licensing status of their medicines, but also the implications this has on accessibility.
Internationally, a range of guidance documents exist around the use of unlicensed medicines, all of which have similar requirements related to the justification of using unlicensed medicines, however their content varies.39,40 In response to the issues across the patient pathway highlighted by this study, the All Wales Medicines Strategy Group engaged further with stakeholders and have created updated national guidance on understanding unlicensed medicines to support those involved in the access or supply of unlicensed medicines and the patients who receive them.41 This guidance, which can be used by policy-makers internationally, covers the entire patient journey and provides a supportive framework for stakeholders across all care settings, including prescribers, community pharmacists and community pharmacy staff, clarifying everyone’s role in the supply chain and ensuring awareness of challenges at different stages that could increase the lead time that is often required when accessing and supplying unlicensed medicines. In turn, this could help to reduce treatment delays or disruptions and improve both patient safety and the patient experience. The guidance also includes a patient information leaflet that can be provided to patients and carers to ensure they are aware of the licensing status what this means and the potential challenges with accessibility in the community. Further research could be conducted to see how this updated guidance is perceived by prescribers, pharmacists and patients and conducted overtime to see how well the guidance is utilised by those involved. Further research could also be conducted to compare the content and utilisation of guidance documents for unlicensed medicines internationally.
Limitations
Data collection for this study overlapped with the COVID-19 period, with increased workplace pressures in primary and secondary care. We mitigated against the anticipated impact on recruitments by using principles of information power to determine sample size, so that the final sample included different types of prescribers, and patients recruited from both primary and secondary care. The desirable minimum sample size was reached, but the final number of participants was small, with sample populations not homogenous in some instances (eg, only one secondary care prescriber), which may mean that results may not be fully representative. Despite this, we collected rich data from all the different sample populations, giving an insight into their experiences. To the authors’ knowledge, none of the included patients were treated by the prescribers or accessed their medicines from the community pharmacists included in this study. In this way the individual populations may have had largely differing experiences. Further research could follow patients through their medical journey and interview the patients and the healthcare professionals they interact with at different stages, in order to observe how one stage and the decisions of those involved could directly affect another.
Conclusion
The results of this study highlight that there are varying levels of awareness among healthcare professionals and patients when unlicensed “special” medicines are prescribed. This, coupled with the varying perceptions of responsibility and acceptability of the use of unlicensed “special” medicines among healthcare professionals led to a range of challenges experienced by participants in this study. These include managing care across care settings to ensure the patient is effectively treated, and ensuring continuity of care for patients in the community to reduce the chance of treatment delay or disruption. Further evidence is needed to validate and expand on these findings. There is a clear need for more support for healthcare professionals to increase awareness when unlicensed “special; medicines are used, and to ensure consistent understanding about each healthcare professional”s role in the supply chain. There is also a clear need for integrated and patient-centred care to ensure that any delays experienced when accessing unlicensed medicines do not lead to treatment disruption or harm for the patient. New national guidance developed as a result of the findings can be used by policy-makers internationally to support a reflective review of their own systems and processes.
Author Statement
All co-authors have made substantial contributions to conception, design, or acquisition of data, or analysis and interpretation of data; been involved in drafting and revising the manuscript; given final approval of the version to be published; agreed to be accountable for all aspects of the work.
Funding
The original data collection upon which this research was based, was funded by a Knowledge Economy Skills Scholarship (KESS) going towards a PhD. The analysis was conducted after the PhD completion, as part of our routine work.
Disclosure
The authors declare no conflicts of interest.
References
1. Medicines and Healthcare products Regulatory Agency. 2014a. The supply of unlicensed medicinal products (“specials”). MHRA guidance note 14. Available from: https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/1156182/The_supply_of_unlicensed_medicinal_products__special_GN14.pdf.
2. The Human Medicines Regulations. 2012. Legislation.gov.uk. Available from: http://www.legislation.gov.uk/uksi/2012/1916/contents/made.
3. Royal Pharmaceutical Society. 2015. Professional Guidance for the Procurement and Supply of Specials. Available from: https://www.rpharms.com/Portals/0/RPS%20document%20library/Open%20access/Support/toolkit/specials-professional-guidance.pdf.
4. Dani KA, Murray LJ, Razvi S. Rare neurological diseases: a practical approach to management. Pract Neurol. 2013;13(4):219–227. doi:10.1136/practneurol-2012-000379
5. Stone M. Prescribing in patients with dysphagia. Nurse Prescribing. 2014;12(10):504–507. doi:10.12968/npre.2014.12.10.504
6. Association of Pharmaceutica Specials Manufacturers. Pharmaceutical specials For individual patient clinical needs. 2019. Available from: https://www.apsm-uk.com/specials.
7. Medicines and Healthcare products Regulatory Agency. Off-label or unlicensed use of medicines: prescribers’ responsibilities. 2014b. Available from: https://www.gov.uk/drug-safety-update/off-label-or-unlicensed-use-of-medicines-prescribers-responsibilities.
8. Donovan G, Parkin L, Brierley-Jones L, Wilkes S. Unlicensed medicines use: a UK guideline analysis using AGREE II. Int J Pharm Pract. 2018;26(6):515–525. doi:10.1111/ijpp.12436
9. Paudyal V, Hansford D, Cunningham S, Stewart D. Pharmacy assisted patient self care of minor ailments: a chronological review of UK health policy documents and key events 1997–2010. Health Policy. 2011;101(3):253–259. doi:10.1016/j.healthpol.2011.05.010
10. Peletidi A, Nabhani-Gebara S, Kayyali R. Smoking cessation support services at community pharmacies in the UK: a systematic. Hellenic J Cardiol. 2016;57:7–15. doi:10.1016/s1109-9666(16)30012-4
11. Wong ICK, Basra N, Yeung VW, Cope J. Supply problems of unlicensed and off-label medicines after discharge. Arch Dischildhood. 2006;91(8):686–688. doi:10.1136/adc.2006.093724
12. Husain NR, Davies JG, Tomlin S. Supply of unlicensed medicines to children: semi-structured interviews with carers. BMJ Paediatrics Open. 2017;1(1):1–5. doi:10.1136/bmjpo-2017-000051
13. Wale A, Young Z, Zhang W, et al. Factors affecting the patient journey and patient care when receiving an unlicensed medicine: a systematic review. Res Social Administrative Pharm. 2023;19(7):1024–1041. doi:10.1016/j.sapharm.2023.04.120
14. Wale A Unlicensed ‘special’ medicines; improving the patients’ experience. PhD diss. Cardiff University, 2022. Available from: https://orca.cardiff.ac.uk/id/eprint/151400/1/2022WaleAPhD.pdf.
15. Wale A, Ireland M, Yemm R, et al. Unlicensed “special” medicines: understanding the community pharmacist perspective. Integ Pharm Res Pract. 2020;9:93–104. doi:10.2147/IPRP.S263970
16. Johnson RE, Grove AL, Clarke A. Pillar integration process: a joint display technique to integrate data in mixed methods research. J Mixed Methods Res. 2019;13(3):301–320. doi:10.1177/1558689817743108
17. Hurt L, Ashfield-Watt P, Townson J, et al. Cohort profile: healthWise Wales. A research register and population health data platform with linkage to national health service data sets in Wales. BMJ Open. 2019;9:e031705. doi:10.1136/bmjopen-2019-031705
18. Malterud K, Siersma VD, Guassora AD. Sample size in qualitative interview studies: guided by information power. Qual Health Res. 2016;26(13):1753–1760. doi:10.1177/1049732315617444
19. Braun V, Clarke V. Using thematic analysis in psychology. Qual Res Psychol. 2006;3:77–101. doi:10.1191/1478088706qp063oa
20. O’Brien BC, Harris IB, Beckman TJ, Reed DA. Cook Standards for reporting qualitative research: a synthesis of recommendations. Acad Med. 2014;89:1245–1251. doi:10.1097/ACM.0000000000000388
21. Aronson JK, Ferner RE. Unlicensed and off‐label uses of medicines: definitions and clarification of terminology. Br J Clin Pharmacol 2017;83(12):2615–2625. doi:10.1111/bcp.13394
22. Donovan G, Parkin L, Brierley-Jones L, Wilkes S. Supporting patients with unlicensed medicine use: analysing the script schemas for prescribing, pharmaceutical assessment and supply. Exploratory Res Clin Soc Pharm. 2021;2:100017. doi:10.1016/j.rcsop.2021.100017
23. Magnus D, Rodgers S, Avery AJ. GPs’ views on computerized drug interaction alerts: questionnaire survey. J Clin Pharm Ther. 2002;27(5):377–382. doi:10.1046/j.1365-2710.2002.00434.x
24. Balan S, Hassali MA, Mak VS. Awareness, knowledge and views of off‐label prescribing in children: a systematic review. Br J Clin Pharmacol. 2015;80(6):1269–1280. doi:10.1111/bcp.12750
25. Ghosh S, Arulrajan AE, Baldwin D. Unlicensed applications of licensed psychotropic drugs in an intellectual disability clinical service: retrospective case-note study. J Intellect Disabil. 2010;14(3):237–243. doi:10.1177/1744629510381943
26. Mukattash T, Hawwa AF, Trew K, McElnay JC. Healthcare professional experiences and attitudes on unlicensed/off-label paediatric prescribing and paediatric clinical trials. Eur J Clin Pharmacol. 2011;67(5):449–461. doi:10.1007/s00228-010-0978-z
27. Horne R, Mailey E, Frost S, Lea R. Shared care: a qualitative study of GPs’ and hospital doctors’ views on prescribing specialist medicines. Br J Gen Pract. 2001;51(464):187. PMCID: PMC1313949.
28. Balan S, Ahmad Hassali MA, Mak VS. Attitudes, knowledge and views on off-label prescribing in children among healthcare professionals in Malaysia. Int j Clinl Pharm. 2019;41(4):1074–1084. doi:10.1007/s11096-019-00862-y
29. Joret-Descout P, Bataille J, Brion F, Bourdon O, Hartmann JF, Prot-Labarthe S. Attitudes and experiences of off-label prescribing among paediatricians in a French university teaching hospital. InAnnales Pharmaceutiques Francaises. 2016;74(3):222–231. doi:10.1016/j.pharma.2015.08.002
30. Ellul I, Grech V, Attard-Montalto S. Maltese prescribers use of off-label and unlicensed medicines in children: perceptions and attitudes. Int j Clinl Pharm. 2016;38:788–792. doi:10.1007/s11096-016-0306-5
31. General Medical Council. Prescribing unlicensed medicines. Good practice in prescribing and managing medicines and devices content. 2021. Available from: https://www.gmc-uk.org/-/media/documents/prescribing-guidance-updated-english-20210405_pdf-85260533.pdf.
32. National Health Service. Responsibility for prescribing between primary & secondary/tertiary care. 2018. Available from https://www.england.nhs.uk/wp-content/uploads/2018/03/responsibility-prescribing-between-primary-secondary-care-v2.pdf.
33. World Health Organisation. Medication Safety Transitions Care. 2019. Available from: https://www.who.int/publications/i/item/WHO-UHC-SDS-2019.9.
34. British Medical Association. Caring, supportive, collaborative? Doctors’ views on working in the NHS. 2018. Available from: https://www.bma.org.uk/media/2035/bma-caring-supportive-collaborative-survey-report-sept-2018.pdf.
35. Wilcock M, Bearman D. Community pharmacist management of discharge medication summaries in primary care. Drug Ther Bull. 2019;57(12):179–180. doi:10.1136/dtb.2019.000052
36. Biddle L, Donovan JL, Gunnell D, Sharp D. Young adults’ perceptions of GPs as a help source for mental distress: a qualitative study. Br J Gen Pract. 2006;56(533):924–931. PMCID: PMC1934052.
37. MacKichan F, Brangan E, Wye L, et al. Why do patients seek primary medical care in emergency departments? An ethnographic exploration of access to general practice. BMJ Open. 2017;7(4):e013816. doi:10.1136/bmjopen-2016-013816
38. Clifford S, Barber N, Horne R. Understanding different beliefs held by adherers, unintentional nonadherers, and intentional nonadherers: application of the necessity–concerns framework. J Psychosomatic Res. 2008;64(1):41–46. doi:10.1016/j.jpsychores.2007.05.004
39. Department of Health. 2017. Special access scheme guidance for health practitioners and sponsors. Available from: https://www.tga.gov.au/sites/default/files/special-access-scheme-guidance-for-health-practitioners-and-sponsors.pdf.
40. Health Canada. Special access program for drugs: guidance for industry and practitioners. 2022. Available from: https://www.canada.ca/content/dam/hc-sc/documents/services/drugs-health-products/special-access/drugs/guidance/sap-drugs-guid-ld-eng.pdf.
41. All Wales Medicines Strategy Group. 2023. Understanding unlicensed medicines. Available from:https://awttc.nhs.wales/files/guidelines-and-pils/understanding-unlicensed-medicines-pdf/.
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.