Back to Journals » Journal of Pain Research » Volume 15
Unilateral Percutaneous Kyphoplasty with O-Arm Navigation for the Treatment of Kümmell’s Disease
Authors Jia Y, Peng Z, Li J ![]() , Qin Y, wang G
, Qin Y, wang G
Received 4 September 2021
Accepted for publication 20 December 2021
Published 2 February 2022 Volume 2022:15 Pages 257—266
DOI https://doi.org/10.2147/JPR.S337715
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Erika Petersen
Yukun Jia,1 Zhan Peng,1 Jin Li,1 Yuantian Qin,2 Guangye Wang1
1Spine Surgery, Affiliated Baoan Hospital of Shenzhen, Southern Medical University; The Second School of Clinical Medicine, Southern Medical University, Shenzhen, Guangdong Province, People’s Republic of China; 2Teaching Department, Nanjing University of Aeronautics and Astronautics, Nanjing, Jiangsu Province, People’s Republic of China
Correspondence: Zhan Peng; Guangye Wang, Email [email protected]; [email protected]
Purpose: To evaluate the efficacy and safety of unilateral O-arm navigation-assisted percutaneous kyphoplasty (PKP) for the treatment of Kümmell’s disease.
Methods: The clinical data from patients with Kümmell’s disease who attended our hospital between January 2015 and January 2019 were retrospectively analyzed. For each patient, the visual analog scale (VAS) score, anterior height of the vertebral body, sagittal kyphotic angle, Oswestry Disability Index (ODI), and postoperative cement leakage rate were recorded before and after surgery. Any surgical complications were documented.
Results: The patients were followed up for 12 to 18 months. The average preoperative VAS score, kyphotic angle, and ODI decreased from 8.6 ± 0.5, 18.0 ± 3.7°, and 86.027%, respectively, to 2.2 ± 0.2, 5.8 ± 0.8°, and 26.720% three days after surgery. The anterior height of the vertebral body increased significantly from 14.5 ± 1.2 mm preoperatively to 19.4 ± 1.2 mm three days after surgery, and this improvement was maintained until the last follow-up. After surgery, bone cement leakage occurred in one vertebral body; this patient exhibited leakage to the intervertebral disc space, a complete pedicle and spinal canal structure, no clinical symptoms, and required no treatment.
Conclusion: This study shows that unilateral PKP assisted by O-arm navigation is safe and effective. Moreover, the observed improvements can be maintained over the longer term.
Keywords: percutaneous kyphoplasty, navigation, unilateral, Kümmell’s disease, efficacy, safety
Introduction
With the aging population, the incidence of osteoporotic vertebral compression fractures (OVCFs) continues to increase. OVCFs have become an important health problem due to their high mortality rate and direct and indirect economic costs.1 Kümmell’s disease is a delayed complication of OVCFs; it was first described by Kümmell in 1895.2 Patients experience lower back pain and kyphosis months or even years following mild spinal trauma. The most common imaging manifestations include delayed vertebral collapse and intravertebral fissures. Kümmell’s disease generally does not heal naturally and conservative treatments such as bed rest and brace fixation are often ineffective. Ultimately, without treatment, patients experience chronic lower back pain and paralysis.3 Most patients with Kümmell’s disease are elderly people with osteoporosis and secondary complications. Surgical intervention for Kümmell’s disease remains challenging and there is no single standard or effective treatment for Kümmell’s disease. PKP is an effective and minimally invasive method for the treatment of Kümmell’s disease.4–6 The main goal of surgical treatment is to inject polymethyl methacrylate into the fracture to fill the cracks. However, fresh bone and sclerotic bone coexist in the collapsed vertebrae of patients with Kümmell’s disease,7 and there can be many sclerotic bones in the puncture passage; this can lead to high puncture resistance and puncture difficulty. Thus, balloon dilation and mastery of puncture technology are required. In addition, it is difficult to accurately locate the vacuum fissures in the vertebral body with the use of manual surgery or X-ray-guided surgery, which, in turn, makes it technically difficult to perform PKP for the treatment of Kümmell’s disease.
With the development and improvement of computer-assisted surgery systems, computer-guided surgery has been applied in various spinal surgeries. Computer-guided surgery has several advantages, including reduced X-ray radiation exposure time and improved accuracy of pedicle screw placement. In recent years, an intraoperative computed tomography (CT) scanning device, the O-arm, has been widely used in the field of spinal surgery. Combined with a navigation system, the O-arm can provide intraoperative 3D imaging for most spinal surgeries. The O-arm navigation approach is characterized by a visible track that allows the working tube to be inserted into the correct surgical site and thus an appropriate incision location can be selected; this is difficult to achieve with the use of X-ray images.8,9 Therefore, with the help of O-arm navigation, surgeons can confirm the needle entry point under the guidance of computer navigation and then puncture into the pedicle and accurately locate the vacuum fissure cavity of the collapsed vertebral body in patients with Kümmell’s disease. Such an approach reduces the possibility of spinal cord and nerve injury, allows for more accurate and easier control of the surgery, and thus greatly reduces the difficulty of the surgical application of this technique. However, to the best of our knowledge, there are few reports on the application of navigation technology in PKP surgery, especially in Kümmell’s disease.
In the current study, navigation-assisted unilateral PKP surgery was performed and patients were followed up for up to 14 months. The purpose of this study was to evaluate the feasibility of O-arm navigation-assisted PKP for the treatment of Kümmell’s disease and to analyze the efficacy and safety of the surgery.
Materials and Methods
Patient Data
This was a retrospective study of 20 patients with Kümmell’s disease who were treated with PKP assisted by O-arm navigation. Each patient’s demographic and clinical characteristics were collected from their electronic medical records. Informed consent was obtained from all patients. The patient demographics are presented in Table 1. The sample comprised 7 males and 13 females aged from 52 to 83 years, with an average age of 63.1±6.6 years. All 20 patients had severe back pain that could not be cured by conservative treatment, and imaging examinations showed vacuum phenomenon, cracks, pseudoarthrosis, or fracture stump sclerosis, with an average symptom duration of three months. Patients with neurological deficits, history of spinal surgery, infections, vertebral metastatic tumors, or pathological fractures associated with a primary tumor were excluded. The treatment levels were T10 (2), T11 (5), T12 (9), L1 (3), and L2 (1), respectively. The VAS score, kyphotic angle, anterior height of the vertebral body, and ODI were compared before and after surgery. The kyphotic angle was defined as the angle at which the vertical lines of the upper and lower endplates of the injured vertebra intersect,10 while the anterior height of the vertebra was defined as the distance between the upper and lower endplates of the anterior wall of the vertebra.11 All patients underwent X-ray (Figure 1), including orthostatic and lateral X-rays, CT (Figure 2), and magnetic resonance imaging (MRI) examinations (Figure 2). Even if a fissure was only observed in one of the three examinations, this was confirmation of the presence of a fissure.
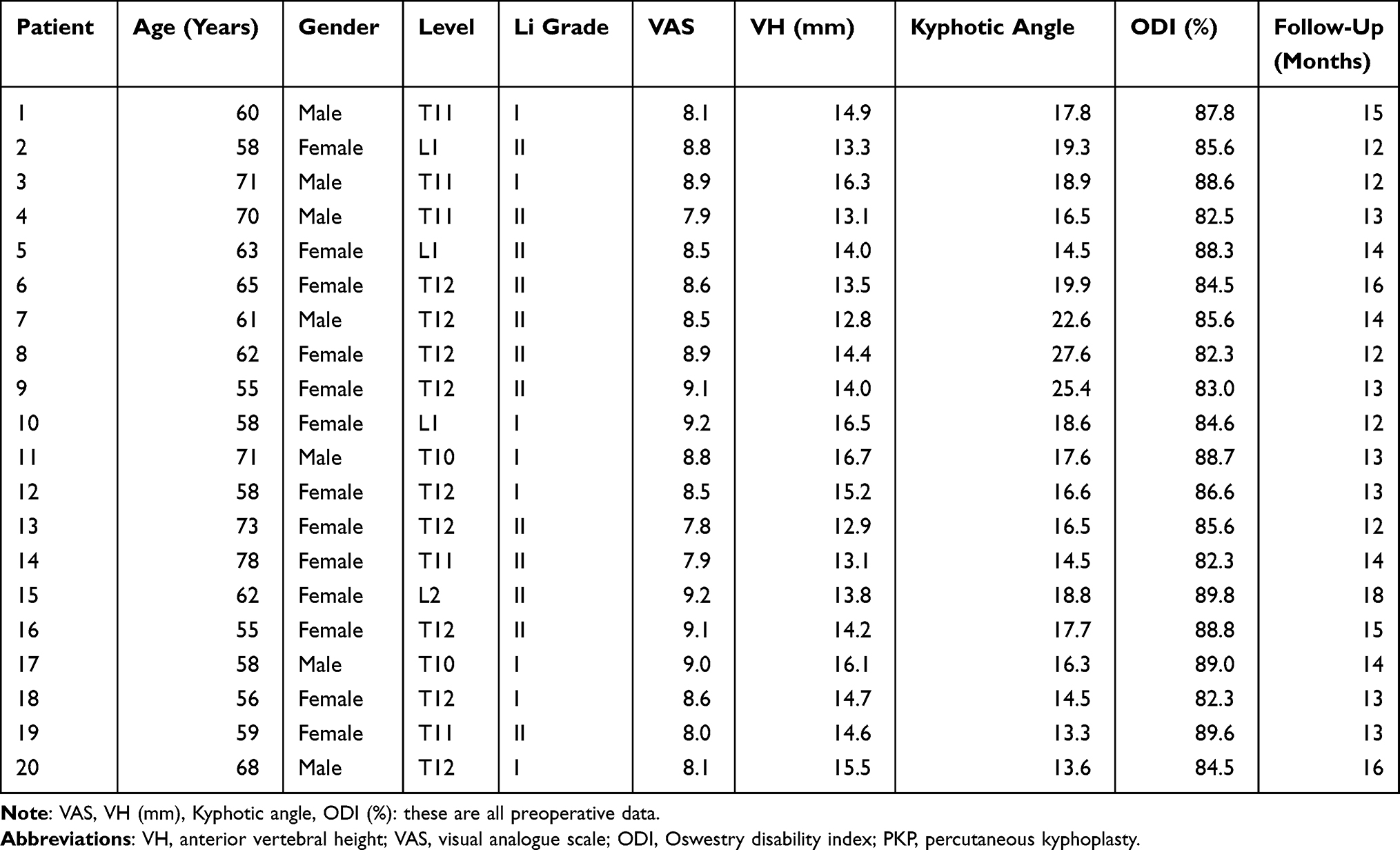 |
Table 1 Clinical Characteristics of Patients with Kümmell Disease (n=20) |
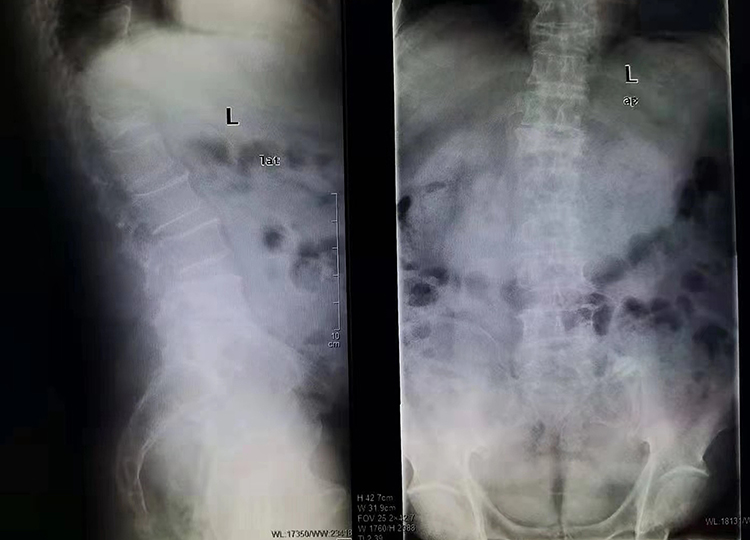 |
Figure 1 Preoperative X-ray showed collapsed vertebral body and fractures in the vertebral body. |
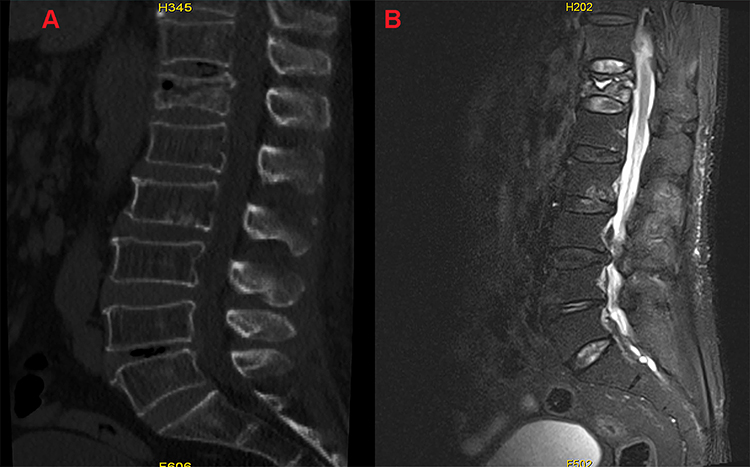 |
Figure 2 (A) Preoperative CT showed collapsed vertebral body and fractures in the vertebral body; (B) preoperative MRI showed collapsed vertebral body and fractures in the vertebral body. |
The Li12 classification was made as follows: stage I, reduction in the height of the vertebral body of less than 20% with no adjacent degenerative intervertebral disc disease, narrowing of the intervertebral disc space, lower back pain, or symptoms, but with observed changes in MRI signals; stage II, decrease in the height of the vertebral body exceeding 20% with adjacent intervertebral disc degeneration, dynamic mobile fracture, and lower back pain with or without radiculopathy; stage III, substantial decrease in the height of the vertebral body, break in the posterior cortex of the vertebral body with spinal cord compression, and back pain with or without spinal cord injury. Based on these criteria, eight cases were classified as stage I, and 12 cases were classified as stage II; none of the cases were classified as stage III.
Surgical Procedure
After induction of general anesthesia, the patient was placed in the prone position on a special pad for spinal surgery. The abdomen was suspended, and the navigation and positioning rod was placed at the right posterior superior iliac crest. Then, the fractured vertebral body was scanned with the O-arm machine and the collapsed vertebral body was located. The left entry point was determined, approximately 1.5 cm from the horizontal midline of the vertebral body. After determination of the entry point under navigation guidance, the pedicle was punctured (Figures 3 and Figure 4). After successful puncture of the pedicle, the guide needle was removed. Then, the balloon was placed into the vertebral fissure cavity of the collapsed vertebra through the working channel and the contrast medium was injected. Under O-arm fluoroscopy, the balloon was stretched, sucking out the contrast medium. The bone cement was then prepared; when the bone cement was a thin paste consistency, the bone cement injector was connected to a syringe. Using the O-arm X-ray machine for monitoring, the cavity of the vertebral body was filled with bone cement along the puncture channel, with about 6 mL of bone cement injected. After pulling out the bone cement injector, the surgeon checked that the height and shape of the collapsed vertebral body were restored, and that the bone cement was in a good position (Figure 5). All of the above processes were completed using an O-arm for monitoring.
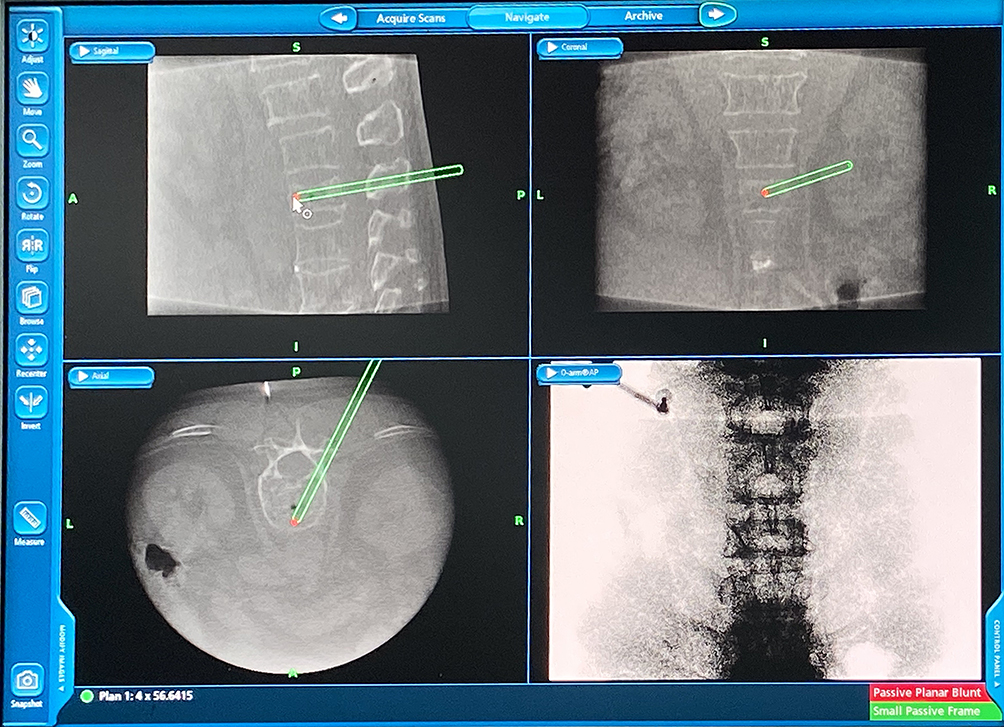 |
Figure 3 Computer navigation planning route, accurate for identifying the fracture of the vertebral fissure. |
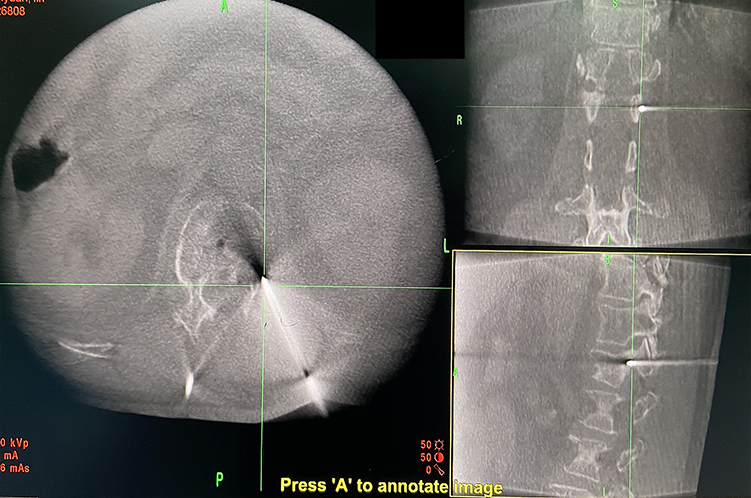 |
Figure 4 Accurate puncture to the fissure during surgery. |
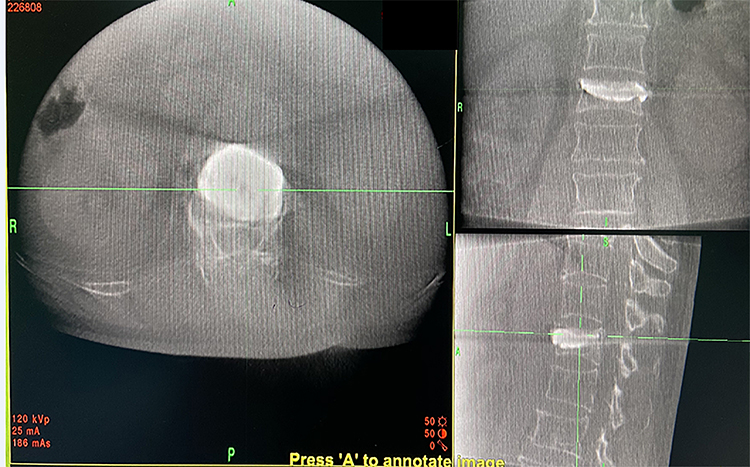 |
Figure 5 Bone cement was injected into the crack of the collapsing vertebral body during surgery. |
Evaluation of Efficacy and Safety
In order to evaluate the efficacy of PKP for the treatment of Kümmell’s disease, the VAS, ODI, kyphotic angle, and anterior vertebral height were analyzed. The VAS and ODI were examined before surgery and three days, three months, and one year after surgery, with measurements completed during outpatient follow-up appointments. Measurements of the kyphotic angle and anterior height of the vertebral body were collected before surgery and three days, three months, and one year after surgery. The safety of PKP was assessed by evaluating surgical complications, including cement leakage, nerve injury, and postoperative infection. Postoperative infection assessment was based on serum leukocytes and inflammatory markers, including C-reactive protein, and the erythrocyte sedimentation rate.
Data Analysis
SPSS 20.0 statistical software (PASW Statistics, IBM) was used for analysis. The data are expressed as mean±standard deviation. Paired t-tests were used to evaluate the changes in VAS scores, kyphotic angle, and vertebral height before and after surgery (significance indicated by P < 0.05). All radiological measurements were carried out by two doctors in a double-blind manner.
Results
Clinical and Imaging Results
All 20 patients tolerated the surgery. All surgical times were very short, with an average surgery time for each vertebral body of 28 min (25–45 min). The patients experienced very little operative blood loss, with an average blood loss of 2.5 mL (1–5 mL). The operative segments were T10 (2), T11 (5), T12 (9), L1 (3), and L2 (1).
During the surgeries, there were no serious toxic reactions (circulatory failure, shock, or cardiac arrest, which can cause the surgery to be stopped). One day after surgery, all patients had significantly reduced back pain, were able to walk, and were able to take care of themselves. The patients were followed up for 12 to 18 months (mean of 14 months). The mean VAS score decreased from 8.6±0.5 before surgery to 2.2±0.2 three days after surgery (P<0.001), indicating a significant improvement in lower back pain. At the last follow-up, the average pain score increased slightly to 2.3±0.2, but this was not significantly different from the score three days after surgery (P<0.055). Thus, the pain relief effect of the surgery was lasting and effective. There was a similar change in the average ODI score. The ODI score decreased from 86.0±2.7 before surgery to 26.7±2.0 three days after surgery and 27.6±1.7 at the last follow-up. This indicates that patients experienced significant improvements in their functional ability to carry out daily activities following surgery. The height of the anterior edge of the vertebral body increased to 19.4±1.2 mm three days after surgery and decreased slightly to 18.6±1.1 at the last follow-up. There was no significant difference between the result of the immediate postoperative evaluation and that of the last postoperative evaluation. The kyphotic angle was 18.0 ±3.7° preoperatively and 5.8±0.8° postoperatively (P<0.05); it increased slightly to 9.9±0.8° at the last follow-up, but this increase was not significant compared to the immediate postoperative assessment (Figure 6). The detailed evaluation results are shown in Table 2.
 |
Table 2 Efficacy Evaluation |
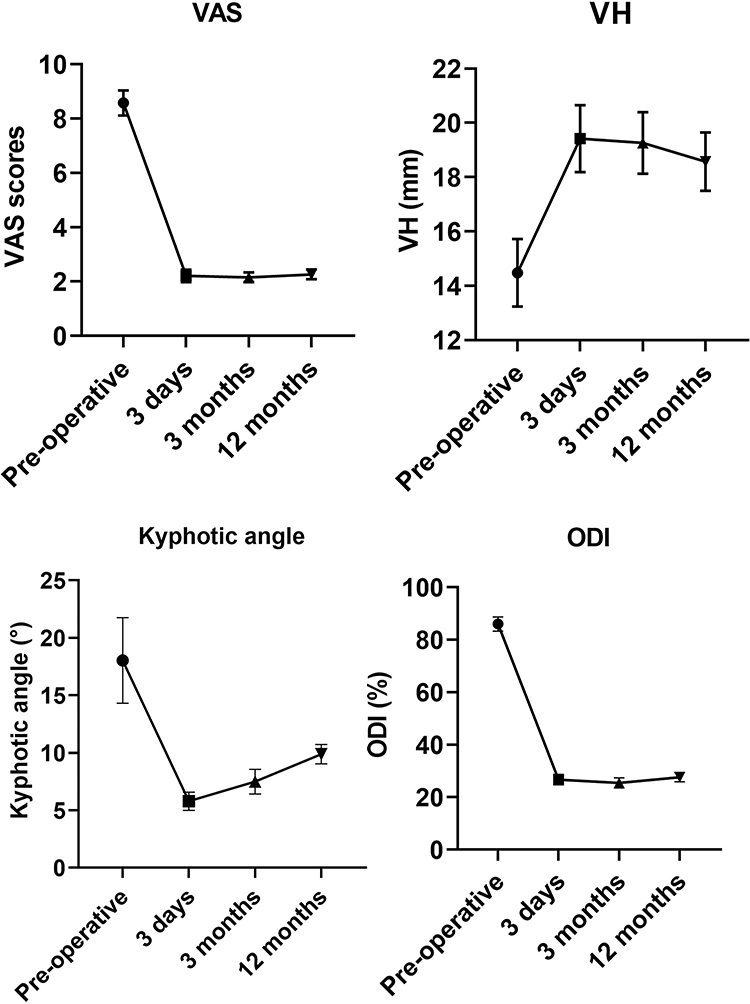 |
Figure 6 Changes in VAS score, anterior height of the vertebral body, kyphotic angle, and ODI score before and after surgery. |
Complications
CT scans showed asymptomatic cement leakage in the intervertebral space in one case after PKP surgery. This patient exhibited no cement infiltration into the spinal canal, no further displacement of the posterior segment of the vertebral body, and no clinical symptoms. During the follow-up period, no neurological deficits were observed, and no other complications occurred, including spinal cord compression, inflammation, or pulmonary embolism. There was no significant loss of vertebral height or kyphotic angle.
Discussion
Intraspinal fractures caused by trauma are considered to be the most important feature in the diagnosis of Kümmell’s disease, with an incidence of 79%. Intraspinal fissures can lead to vertebral collapse and spinal canal stenosis which aggravate clinical symptoms. Stage I and II Kümmell’s disease present with no neurological symptoms; therefore, in these stages, the main purpose is to eliminate the vertebral fractures and restore spinal stability. PKP surgery under an image-guided system allows for accurate localization of fissures in the vertebral body, injection of bone cement into the fissures, effective stabilization of the collapsed vertebrae, and enhanced intervertebral stability, thus maximizing the patient’s clinical improvement. This approach allows for the individualized design of the puncture path before surgery and real-time dynamic guidance and monitoring of the puncture path along multiple planes during the puncture process. The approach also provides greater accuracy than the conventional approach for PKP puncture.
In the current study, patients were followed up for more than 12 months. The results of this study indicated that O-arm navigation-assisted PKP surgery produced satisfactory results, relieving back pain, correcting kyphosis, and restoring vertebral height; these improvements were sustained until the last follow-up evaluation. At the last follow-up, kyphosis was corrected, and the kyphotic angle had increased slightly. It is believed that this increase in the kyphotic angle is due to the normal aging of the human body. This study did not examine if there was a statistical difference in the kyphotic angle between the last follow-up and the follow-up three days after surgery; however, the kyphotic angle three days after surgery and that at the last follow-up were significantly different from the pre-surgery kyphotic angle. Moreover, there was no significant correlation between these imaging changes and the patients’ clinical symptoms. The results of this study are also consistent with those of the study by Zhang et al.13
Nakamae et al14 demonstrated that vertebral instability after a fracture is the main cause of the symptoms of Kümmell’s disease. Lee15 also reported a serious conus medullaris injury caused by dynamic instability associated with Kümmell’s disease. The incidence of delayed neurological deficits after vertebral collapse in OVCFs is 19%. The main factor contributing to neurological deficits is the instability of the vertebral body at the fracture site, rather than mechanical compression of the spinal cord by bone fragments. In order to improve the patient’s symptoms and the efficacy of treatment, the most important thing is to reconstruct the stability of the spine. In the current study, through the precise injection of bone cement into the fissure using PKP, each patient’s collapsed vertebral body was effectively stabilized. This process significantly relieved the patients’ symptoms, with a decrease in the VAS score from 8.6 before surgery to 2.2 three days after surgery. The ODI score also decreased from 86% before surgery to 26.7% three days after surgery. Thus, the surgery relieved the patients’ symptoms and improved their quality of life.
The complications of PKP include bone cement leakage, pulmonary embolism, thermal injury caused by bone cement, nerve injury caused by surgery, and infection.16 The most common complication is cement leakage (14–18%),17,18 which usually infiltrates into the epidural space, intervertebral foramen, intervertebral disc, and paraspinal vein, and can affect the prognosis of the surgery. Overall, 73% of PKP complications are related to bone cement leakage. If the bone cement seeps into the spinal canal and causes compression of the spinal cord, it can cause paralysis.19 If the bone cement seeps into the vascular system, it can lead to pulmonary embolism and even death. In order to avoid bone cement leakage, preoperative CT scans should confirm whether the surrounding wall of the vertebral body is damaged. It is also very important to choose the appropriate puncture point and angle before minimally invasive puncture. If this is not done, important adjacent blood vessels and nerves can be easily damaged, resulting in paralysis and even death. In this study, the puncture point was determined under the guidance of real-time navigation images with dynamic O-arm monitoring throughout the whole process of bone cement filling, and real-time dynamic monitoring of bone cement distribution. As soon as the bone cement reached the lateral edge of the vertebral body or 1/4 of the distance from the posterior wall, the filling process was immediately stopped. The cement leakage rate in the current study was 3.8%, which is much lower than the reported rate of 14% in the literature. This result indicates that it is safe to perform PKP surgery with the assistance of O-arm navigation.
Unilateral PKP was used in all surgeries. A 2018 meta-analysis showed that compared with bilateral PKP, unilateral PKP has a shorter surgical time, less cement consumption, and lower risk of cement leakage.20 Unilateral PKP is more advantageous than bilateral PKP and should be regarded as an effective choice for the treatment of OVCFs. Moreover, previous biomechanical studies have shown that both unilateral PKP and bilateral PKP significantly increase the strength and stiffness of the vertebral body.21 Furthermore, when unilateral PKP is used, the cement extends along the midline and fills the unpunctured side, which can make both sides of the vertebral body biomechanically stable. However, during unilateral puncture, it is necessary to increase the internal inclination angle to ensure the bone cement crosses the midline, and while this makes it easier to penetrate the pedicle, it also increases the surgical risk and difficulty. Intraoperative navigation helps to overcome these risks.22 In the current study, the balloon was placed in the first third of the vertebra. Navigation was used to determine the puncture route before surgery and real-time multiplane monitoring was performed during the surgery, which improved the safety of the surgery. The average surgical time for each vertebral body was 28 min. Compared with previous studies,6,23 the current surgical time under navigation was not increased significantly. This may be related to several factors. First, the surgical time of unilateral PKP is shorter than that of bilateral PKP. Second, navigation-assisted PKP eliminates the need for repeated intraoperative fluoroscopy,24 which also reduces the surgical time.
This study has several limitations that should be noted. First, patients with severe spinal cord compression, neurological impairment, or a history of spinal surgery were excluded. As the main purpose of PKP is to strengthen the vertebrae without restoring the nervous system, selective bias seems inevitable and may have affected the results of this study. Second, this study had a small sample size, the follow-up period was short, and long-term patient complications were not evaluated. Although navigation-assisted PKP is associated with improved safety and surgical accuracy, the cost of the surgery is also increased accordingly, and this study did not consider the economic costs of this surgical approach. The surgical time of unilateral PKP is shorter than that of bilateral PKP, but we have not designed a case-control study of bilateral vs unilateral PKP at this stage. This was only a preliminary study, and future studies on Kümmell’s disease should be designed more carefully. Increased sample sizes and longer follow-up periods are needed to verify the effectiveness of this method for the treatment of Kümmell’s disease.
Conclusion
O-arm navigation-assisted unilateral PKP is a safe and effective minimally invasive method for the treatment of Kümmell’s disease. This surgery can effectively relieve pain, restore physiological spinal curvature, and improve functional status.
Data Sharing Statement
Anyone who wishes to access those data could contact the corresponding author (Guangye Wang) by email.
Ethical Approval
The Ethics Committee of Shenzhen Baoan District People’s Hospital considered this study ethically exempt because it was a retrospective case series study and used only raw data that was completely de-identified and anonymous. The study was conducted in accordance with the provisions of the Declaration of Helsinki. Informed consent was obtained from all of the participants. All patients consent to publish.
Funding
The authors have no sources of funding to declare for this manuscript.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Ehsanbakhsh AR, Akhbari H, Iraee MB, et al. The prevalence of undetected vertebral fracture in patients with back pain by Dual-Energy X-ray Absorptiometry (DXA) of the lateral thoracic and lumbar spine. Asian Spine J. 2011;5(3):139–145. doi:10.4184/asj.2011.5.3.139
2. Kim YC, Kim YH, Ha KY. Pathomechanism of intravertebral clefts in osteoporotic compression fractures of the spine. Spine J. 2014;14(4):659–666. doi:10.1016/j.spinee.2013.06.106
3. Chen GD, Lu Q, Wang GL, et al. Percutaneous kyphoplasty for Kummell disease with severe spinal canal stenosis. Pain Physician. 2015;18(6):E1021–E1028.
4. Wei H, Dong C, Zhu Y, Ma H. Analysis of two minimally invasive procedures for osteoporotic vertebral compression fractures with intravertebral cleft: a systematic review and meta-analysis. J Orthop Surg Res. 2020;15(1):401. doi:10.1186/s13018-020-01938-6
5. Huang Y, Peng M, He S, Tang X, Dai M, Tang C. Clinical efficacy of percutaneous kyphoplasty at the hyperextension position for the treatment of osteoporotic Kümmell disease. Clin Spine Surg. 2016;29(4):161–166. doi:10.1097/BSD.0000000000000259
6. Yang H, Gan M, Zou J, et al. Kyphoplasty for the treatment of Kümmell’s disease. Orthopedics. 2010;33(7):479. doi:10.3928/01477447-20100526-07
7. Feng SW, Chang MC, Wu HT, Yu JK, Wang ST, Liu CL. Are intravertebral vacuum phenomena benign lesions? Eur Spine J. 2011;20(8):1341–1348. doi:10.1007/s00586-011-1789-3
8. Peng P, Chen K, Chen H, et al. Comparison of O-arm navigation and microscope-assisted minimally invasive transforaminal lumbar interbody fusion and conventional transforaminal lumbar interbody fusion for the treatment of lumbar isthmic spondylolisthesis. J Orthop Translat. 2020;20:107–112. doi:10.1016/j.jot.2019.10.001
9. Chen K, Chen H, Zhang K, et al. O-arm navigation combined with microscope-assisted MIS-TLIF in the treatment of lumbar degenerative disease. Clin Spine Surg. 2019;32(5):E235–e240. doi:10.1097/BSD.0000000000000804
10. Phillips FM, Isaacs RE, Rodgers WB, et al. Adult degenerative scoliosis treated with XLIF: clinical and radiographical results of a prospective multicenter study with 24-month follow-up. Spine. 2013;38(21):1853–1861. doi:10.1097/BRS.0b013e3182a43f0b
11. Pflugmacher R, Schroeder RJ, Klostermann CK. Incidence of adjacent vertebral fractures in patients treated with balloon kyphoplasty: two years’ prospective follow-up. Acta Radiol. 2006;47(8):830–840. doi:10.1080/02841850600854928
12. Li K-C, Wong T-U, Kung F-C, Li A, Hsieh C-H. Staging of Kümmell’s disease. J Musculoskelet Res. 2004;8(1):43–55.
13. Zhang J, Fan Y, He X, et al. Is percutaneous kyphoplasty the better choice for minimally invasive treatment of neurologically intact osteoporotic Kümmell’s disease? A comparison of two minimally invasive procedures. Int Orthop. 2018;42(6):1321–1326. doi:10.1007/s00264-018-3832-z
14. Nakamae T, Fujimoto Y, Yamada K, Takata H, Shimbo T, Tsuchida Y. Percutaneous vertebroplasty for osteoporotic vertebral compression fracture with intravertebral cleft associated with delayed neurologic deficit. Eur Spine J. 2013;22(7):1624–1632. doi:10.1007/s00586-013-2686-8
15. Lee SH, Cho DC, Sung JK. Catastrophic intramedullary hematoma following Kümmell’s disease with large intravertebral cleft. Spine J. 2008;8(6):1007–1010. doi:10.1016/j.spinee.2007.07.397
16. Lane JI, Maus TP, Wald JT, Thielen KR, Bobra S, Luetmer PH. Intravertebral clefts opacified during vertebroplasty: pathogenesis, technical implications, and prognostic significance. AJNR Am J Neuroradiol. 2002;23(10):1642–1646.
17. Lee MJ, Dumonski M, Cahill P, Stanley T, Park D, Singh K. Percutaneous treatment of vertebral compression fractures: a meta-analysis of complications. Spine. 2009;34(11):1228–1232. doi:10.1097/BRS.0b013e3181a3c742
18. Zhan Y, Jiang J, Liao H, Tan H, Yang K. Risk factors for cement leakage after vertebroplasty or kyphoplasty: a meta-analysis of published evidence. World Neurosurg. 2017;101:633–642. doi:10.1016/j.wneu.2017.01.124
19. Wang HS, Kim HS, Ju CI, Kim SW. Delayed bone cement displacement following balloon kyphoplasty. J Korean Neurosurg Soc. 2008;43(4):212–214. doi:10.3340/jkns.2008.43.4.212
20. Tan G, Li F, Zhou D, Cai X, Huang Y, Liu F. Unilateral versus bilateral percutaneous balloon kyphoplasty for osteoporotic vertebral compression fractures: a systematic review of overlapping meta-analyses. Medicine. 2018;97(33):e11968. doi:10.1097/MD.0000000000011968
21. Chen B, Li Y, Xie D, Yang X, Zheng Z. Comparison of unipedicular and bipedicular kyphoplasty on the stiffness and biomechanical balance of compression fractured vertebrae. Eur Spine J. 2011;20(8):1272–1280. doi:10.1007/s00586-011-1744-3
22. Dalton BE, Kohm AC, Miller LE, Block JE, Poser RD. Radiofrequency-targeted vertebral augmentation versus traditional balloon kyphoplasty: radiographic and morphologic outcomes of an ex vivo biomechanical pilot study. Clin Interv Aging. 2012;7:525–531. doi:10.2147/CIA.S37025
23. Xiong XM, Sun YL, Song SM, et al. Efficacy of unilateral transverse process-pedicle and bilateral puncture techniques in percutaneous kyphoplasty for Kummell disease. Exp Ther Med. 2019;18(5):3615–3621. doi:10.3892/etm.2019.7980
24. Wang H, Hu P, Wu D, Zhang N, Wu J, Xiang L. Age, gender, level and side differences in the anatomical distinctions of unilateral percutaneous kyphoplasty through the transverse process-pedicle approach. Pain Physician. 2019;22(2):E91–e96. doi:10.36076/ppj/2019.22.E91
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.