")
Back to Journals » Patient Preference and Adherence » Volume 16
Understanding the Treatment Preferences of People Living with Schizophrenia in Australia; A Patient Value Mapping Study
Authors Fifer S , Keen B , Newton R, Puig A , McGeachie M
Received 21 March 2022
Accepted for publication 18 June 2022
Published 19 July 2022 Volume 2022:16 Pages 1687—1701
DOI https://doi.org/10.2147/PPA.S366522
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Johnny Chen
Simon Fifer,1 Brittany Keen,1 Richard Newton,2 Andrea Puig,3 Marija McGeachie4
1Community and Patient Preference Research, Sydney, NSW, Australia; 2Monash University, Melbourne, VIC, Australia; 3Real World Evidence Department, Janssen-Cilag Australia Pty Ltd, Sydney, NSW, Australia; 4Department of Medical and Scientific Affairs, Janssen-Cilag Australia Pty Ltd, Sydney, NSW, Australia
Correspondence: Andrea Puig, Real World Evidence Department, Janssen-Cilag Australia Pty Ltd, 66 Waterloo Road, Macquarie Park, Sydney, NSW, 2113, Australia, Tel +61-4-2912-8695, Fax +61 2 9815 3200, Email [email protected]
Purpose: To examine the treatment and long-term outcome preferences for people living with schizophrenia.
Patients and Methods: Sixty-six Australian adults, living with schizophrenia completed a novel online survey with six sections: Demographic characteristics; Disease history; Quality-of-life; Patient support programmes; Discrete Choice Experiment, and Best-Worst Scaling exercise.
Results: Participants indicated that they preferred to be involved in treatment decision with their doctor. A minority of participants reported having been previously involved in a patient support programme (28.8%) and only one in six participants had a National Disability Insurance Scheme (NDIS) package (16.7%) with over a third of participants indicating that they were ineligible (37.9%). Participants’ average quality-of-life score was 60%.
Conclusion: Recent hospitalisation influenced the relative importance of treatment attributes, with effectiveness on hearing voices being the most important treatment attribute. The most important long-term goals were having a stable place to live, being independent, and physical health. People with schizophrenia care about their long-term functional recovery outcomes, rating symptom control and independence as their highest priority. They want to be part of the treatment conversation with their doctors. Therefore, psychiatrists are encouraged to use shared decision-making to establish the treatment course that best aligns with individuals’ long-term goals.
Keywords: discrete choice experiment, patient preference, patient value mapping, schizophrenia, shared decision-making, treatment goals
Introduction
Schizophrenia is a psychotic disorder associated with problems in social and occupational functioning and self-care.1 The most recent estimates suggest that Australians aged between 18 and 45 years have a lifetime morbid risk of developing schizophrenia of 2.37 per 1000 people.2 The current Australian clinical guidelines recommend that schizophrenia is managed through a multidisciplinary team approach, with comprehensive psychosocial support and appropriate pharmacological treatment.3 Antipsychotic medicines remain the cornerstone of schizophrenia treatment both for acute episodes and ongoing maintenance therapy.3 Antipsychotic medicines effectively treat the symptoms of schizophrenia3 and are available in both oral and long-acting injectable (LAI) forms. LAIs have been found to be superior to oral medication at preventing hospitalisation and reducing relapse in randomised controlled trials as well as real-world use.4 However, LAI uptake among people living with schizophrenia is relatively low at 19% to 30%.5
Despite advances in the treatment options available, only one in seven individuals meet the criteria for recovery from schizophrenia.6 Non-adherence to prescribed drug treatment can be considered the most challenging aspect of treating schizophrenia,7 with discontinuation rates for oral antipsychotics ranging from 26% to 44%.8 This may be due to a combination of factors, including the severe side effects (such as extrapyramidal effects, metabolic or cardiac effects),3 as well as the clinical manifestations of the disease itself (which can include poor insight and cognitive dysfunction).7,9 Social, economic and health system barriers may also contribute to medication non-adherence.9 Non-adherence leads to a high risk of relapse, hospital readmission, and poor long-term outcomes.8 Even a small gap, of one to ten days, in treatment compliance increases the risk of hospitalisation (odds ratio = 1.98).10 These findings have led clinical guidelines to recommend that psychosocial interventions include strategies to encourage adherence to medicines.3
While use of LAI antipsychotics may improve medication adherence, these are often underutilised due to the perceived negative beliefs and attitudes of both people with schizophrenia and their health-care providers.8 Psychiatrists often believe that their patients will refuse LAIs, despite positive patient attitudes towards LAIs, which includes feeling more supported due to regular contact with health-care professionals.9
Shared decision-making is recognised as a way of increasing collaboration between the person with schizophrenia and the clinician.11 It has been defined as “an approach where clinicians and patients make decisions together using the best available evidence”.12 Shared decision-making is seen “as the pinnacle of patient centred care”.13 Supporting patients to consider their options and express informed preferences towards treatment and management options can improve long-term compliance,14 increase acceptance of LAIs,11 and improve wellbeing and treatment satisfaction among people living with schizophrenia.15
To date, few studies have investigated antipsychotic treatment preferences of those living with schizophrenia.16,17 However, incorporating the values of people with lived experience into health outcomes is becoming increasingly important and is known as patient value mapping.18–20 Patient value mapping, is a term used to capture patient preferences for hypothetical treatment options that can be used to map value back to real treatments.21 This methodology has previously been used to assess the preferences of patients living with treatment-resistant depression,22 inflammatory arthritis,20 type-2 diabetes,18 and multiple myeloma.19,21 This study aimed to develop a greater understanding of the treatment preferences and preferred long-term outcomes of people with a lived experience of schizophrenia.
Materials and Methods
Sample
Australian adults with a lived experience of schizophrenia were recruited through consumer organisations (SANE Australia, One Door Mental Health, Neami National, Lived Experience Australia, and Mental Illness Fellowship of Australia (MIFA)); Healthcare professionals’ networks (mental health practitioners, psychiatrists, etc.) and online market research companies (Dynata and Stable Research).
Participants that completed the online survey were offered AU$40 as a bank transfer (or equivalent panel points, for those recruited through market research companies) or a donation of this amount to a consumer organisation involved in recruiting for the study.
The study was approved by the Bellberry Limited Human Research Ethics Committee (Application no. 2019–12-1161-A-1), as no author was affiliated with a research institution at the time of seeking ethics approval. The study complied with the Declaration of Helsinki.23 Informed consent was obtained by asking participants to read an information sheet about the benefits and risks of the study and then confirming their consent to take part by clicking a checkbox in the online survey. All information and consent forms were delivered online at the beginning of the online survey. Participants were able to withdraw from the study at any time.
Design
Participants who met the eligibility criteria completed an online survey (Supplementary Table 1), which took approximately 20 to 30 minutes. The survey instrument was designed based on a review of the academic literature and in consultation with two external advisers – a clinician and a person with lived experience of schizophrenia. The final survey had six sections which covered the following areas: 1. Demographic characteristics; 2. Disease history; 3. Quality-of-life (QoL); 4. Patient support programmes; 5. A Discrete Choice Experiment (DCE) to evaluate the relative importance of treatment attributes, and 6. A Best-Worst Scaling exercise (BWS) to determine the importance of long-term outcomes. Consumer groups advised on the DCE attributes.
Demographic Information and Disease Background
Information was collected about the participants’ demographic characteristics and their disease history. This included time since diagnosis, comorbid conditions, recent hospitalisations, experience with antipsychotic medications, attitudes towards LAIs, and involvement in treatment decisions (therapeutic alliance, time with therapist, discussion around LAIs).
Quality-of-Life
QoL was measured by the Quality-of-Life Enjoyment and Satisfaction Questionnaire – Short Form (Q-LES-Q-SF). The Q-LES-Q-SF contains 16 items which represents the “general activities” subscale of the long-form Q-LES-Q.24,25 Q-LES-Q has been used widely to measure life satisfaction in patients during pre- and post-treatment phases of therapy.
Patient Support
The authors developed questions relating to patient support, the National Disability Insurance Scheme (NDIS – an Australian government scheme that fund the costs associated with disability) and the impact of COVID-19.
The Discrete Choice Experiment
The DCE was used to evaluate the importance of treatment features of oral versus LAI medication. DCEs are a methodological approach to studying choice behaviour, with a theoretical background in psychology and economics.26–28 DCEs are used by many fields to understand and model the preferences and trade-offs revealed by the choices people make.29
DCEs present participants with a number of scenarios and ask them to choose the alternative that they prefer based on their own value framework (Supplementary Figure 1). It is an assumption of the underlying theory that participants choose the alternative that maximises their utility (ie, satisfaction, or utility maximisers). In this instance, the DCE asked participants to choose between two hypothetical treatment alternatives (Supplementary Methods). Each treatment had various attributes, including method of administration. The treatment alternatives were described by the various attributes and levels shown in Table 1. The attributes and their levels were derived from existing market research, the literature, and expert opinion. Participants had three response options. Participants could choose either of the hypothetical medications or the opt out which represented “continue to do what you are doing now”.
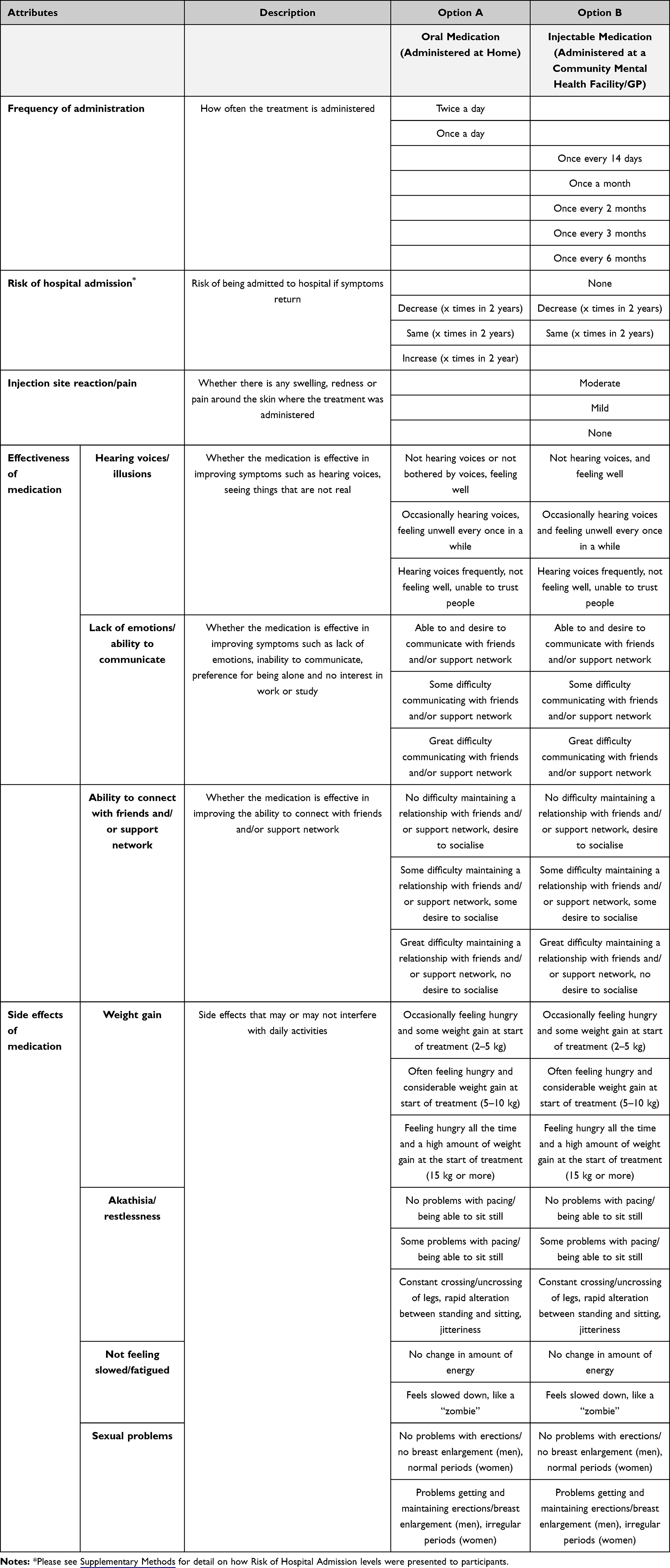 |
Table 1 DCE Attributes and Levels |
In DCEs, sample size calculations require knowledge of the expected parameter estimates, and therefore these calculations are typically not performed a priori.22 During the experimental design process, the minimum required sample size is approximated based on the utility function being estimated (which is a function of the number of parameters). This study utilised a Bayesian efficient design approach, where knowledge of attributes, such as size and direction, is used to optimise the design given sample constraints.30 The experimental design follows good practice guidelines.31,32
The econometric software, Nlogit version 6 (Econometric Software, Inc.), was used to model the DCE data. Preference data were assessed using a mixed multinomial logit (MMNL) model, which allowed for preference heterogeneity (variation) between participants.32,33 The model was used to quantify the overall value of treatments and the relative importance to participants of each of the defining attributes. Additional details of the model specifications and utility functions can be found in the Supplementary Methods.
Best – Worst Scaling (BWS) Exercise
The BWS exercise was used to determine the importance of long-term treatment outcomes and built upon previous work in this area.16 BWS tasks avoid many of the scaling problems associated with Likert ratings. Participants are shown different combinations of sets and asked to select the best and worst option in each comparison.34 The BWS exercise included a total of 15 items which described possible outcomes from receiving treatment for schizophrenia. Participants were shown several subsets of seven items and asked to choose the most important and the least important aspect in each set (Supplementary Figure 2). The full list of items included in the BWS were:
- Having an income and/or work
- Having personal relationships with family
- Having personal relationships friends/partner
- Pursuing hobbies and interests
- Being independent/autonomous
- Having a stable place to live
- Being physically healthy
- Staying out of hospital
- Not feeling the stigma of having the disease
- Not having side effects from treatment
- Not feeling controlled by the doctor or health-care system
- Not being embarrassed by the side effects of treatment
- Being able to stop medication
- Having a medical team that is sympathetic to my needs
- Not feeling lonely
Data from the BWS exercise were computed into scores by calculating the difference between the number of times it was chosen as most important and least important, and then dividing it by the total number of times it appeared throughout the exercise. The BWS scores are a number between one and minus one and represent the relative ranking of the 15 items in terms of their importance.
Data Cleaning
Prior to data cleaning, 89 participants had completed the survey. Participants who finished the survey too quickly (<11 mins), gave nonsensical answers or were suspected duplicates were removed during the data cleaning process (n = 13). Additionally, participants who admitted to a poor understanding of the DCE (a rating of less than six on a scale from 0 [Did not understand at all] to 10 [Understood perfectly]) were excluded from the analysis (n = 10) leaving a total sample of 66 participants. Data for additional survey questions not reported in the results section are provided in the Supplementary Methods. A thorough description of the data analysis process is provided in the Supplementary Methods.
Results
Participant Characteristics
The majority of participants were Australian (50; 75.76%) and lived in a city (54; 81.82%). Full participant demographics can be found in Table 2. Most participants (44; 66.7%) had been diagnosed with schizophrenia more than ten years ago, had not been admitted to hospital in the past two years (37; 56.06%), and had been seeing their current psychiatrist for over a year (36; 54.55%). Half of the participants reported having a diagnosis of depression (33; 50%) and a substantial proportion also reported having an anxiety disorder (27; 40.91%).
 |
Table 2 Demographic Characteristics of Participants |
Disease Background and Treatment History
Most participants (58/66; 88%) were taking antipsychotic medication, with 44 reporting being on monotherapy and 14 taking more than one antipsychotic. Most participants were taking an oral medication (49/58; 84%). Twenty-nine participants (44%) had taken an LAI prior to their current medication, with nine participants using an LAI at the time of the survey (14%). From this, 30 participants (45%) were categorised as having current or previous experience with LAIs. Thirty-six participants (55%) had no experience of LAIs and of those who had not previously taken an LAI only four had ever been offered LAI medication.
Involvement in Treatment Decisions and Therapeutic Alliance
Participants were asked to rank their most to least preferred involvement in treatment decisions. According to first- and second-order preferences, participants preferred that their doctor share responsibility with them, or at least seriously considers their opinion in treatment decisions (Supplementary Table 2). The least preferred option was to leave treatment decisions entirely to their doctor (n = 34 [51.52%] Supplementary Table 2).
Participants were asked to rank their top three support options for transitioning to GP care. Finding a GP who understands mental health and education around treatment options were ranked most important (Supplementary Table 3). Participants were also asked to rank barriers to maintaining treatment. The most important barriers were side effects of treatment and finding a health-care practitioner who understands them (Supplementary Table 3).
Quality-of-Life and Patient Support
Participants in the current study scored an average Q-LES-Q-SF of 60%. The most useful patient supports were digital appointment reminders (36; 54.5%), access to support workers (36; 54.5%), and exercise programmes (31; 47.0%). A minority of participants reported having been previously involved in a patient support programme (19; 28.8%).
Only one in six participants had an NDIS package (11; 16.7%). This was primarily used to provide support to participate in community activities such as recreation, education, training and employment (9/11; 81.8%); and assistance to build capacity to live independently and achieve goals, such as building social relationships, financial management and tenancy management skills (8/11; 72.7%). More than 10% of participants had been rejected for an NDIS package (8; 12.1%). Nearly one-in-five (12; 18.18%) had not been told about an NDIS package and what it offers, and over a third of participants thought that they would not be eligible for an NDIS package (25; 37.9%).
Covid-19
The impact of the COVID-19 outbreak on participants’ mental health was assessed in the survey. Two-thirds of the sample (43; 65.15%) were able to access psychosocial support as normal and most (53; 80.30%) did not require additional support during the outbreak. Participants were asked to rate the impact of the outbreak on their mental health on a scale (0 = no impact to 10 = major impact) with a median result of seven.
The DCE
The DCE measured the relative importance of each attribute by estimating associated parameters for each level (Table 3). These parameters represent the magnitude of influence of each level on patient utility (satisfaction). Only some treatment attributes significantly predicted choice in the DCE model. These were risk of hospital admission (oral treatment only), effectiveness on hearing voices, effectiveness on inability to communicate with friends/support network, impact on restlessness and impact on sexual health. Treatment attributes which did not significantly predict choice were: frequency of administration; injection site reaction/pain; effectiveness on inability to connect/maintain relationships with friends/support network; impact on appetite and weight; and impact on energy levels and fatigue. This is not to say that these treatment features are not important in decision-making but that they did not have a significant influence on decision-making, relative to the other attributes, in this experiment.
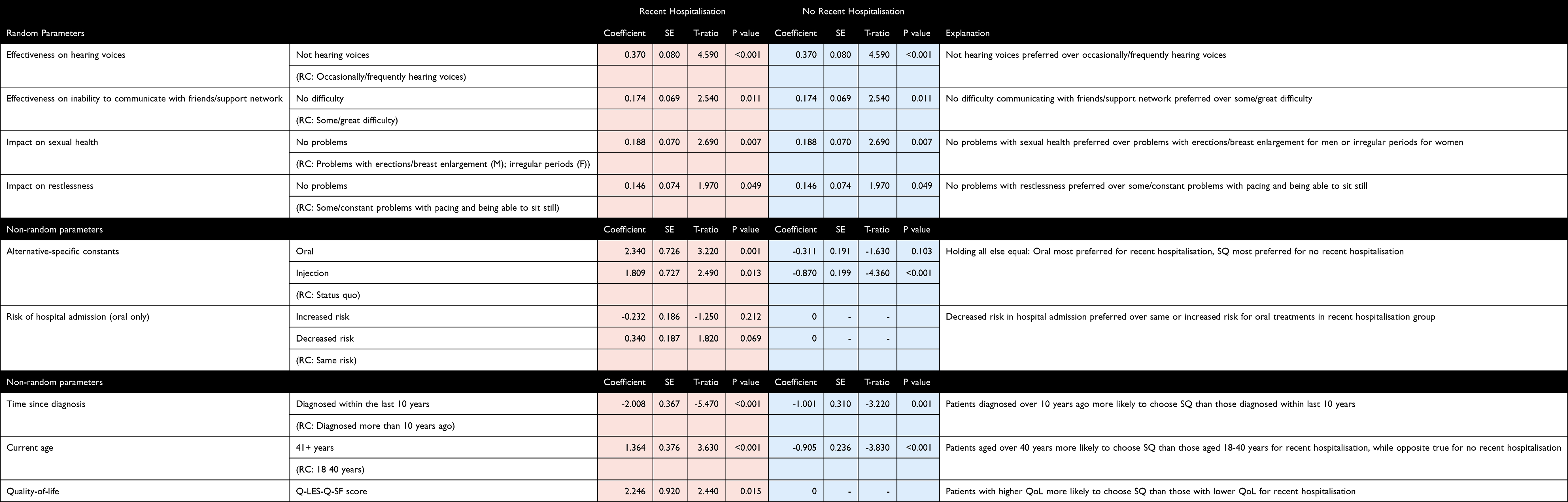 |
Table 3 DCE Parameter Estimate |
Preference for the Status Quo
Some individual characteristics were found to influence participants’ preference to remain with their current treatment (status quo). Younger participants (≤40 years) and those who were diagnosed with schizophrenia more than 10 years ago were more likely to prefer their current treatment. Participants with a higher QoL, who had been hospitalised in the last two years were also more likely to prefer the status quo. Participant characteristics did not directly affect choice of the oral or injectable treatments (these remained proportional as uptake for the status quo increased or decreased).
See https://cappre.shinyapps.io/Janssen_SCHZ/ for a visual representation of the model results and to simulate the effect of different treatment scenarios on participants’ choices.
Recent hospitalisation influenced the relative importance of treatment attributes, therefore the DCE model was segmented into two groups: 1. Those who have had at least one hospitalisation in the past two years; and 2. Those who have not been hospitalised in the past two years.
Recently Hospitalised
For those recently hospitalised, the most important treatment attributes were effectiveness on hearing voices, impact on sexual health and effectiveness on inability to communicate (Figure 1). When taking into account the unique effect of the treatment type in the hypothetical scenario (holding all other treatment attributes constant), both treatment alternatives were preferred to the status quo (reference category), and preference for oral administration (β = 2.340, T-ratio = 3.220) was stronger than preference for injectable administration (β = 1.809, T-ratio = 2.490). Decreased risk of hospital admission (β = 0.340, T-ratio = 1.820) was preferred over the same risk (reference category) or increased risk (β = −0.232, T-ratio = −1.250) for oral treatments.
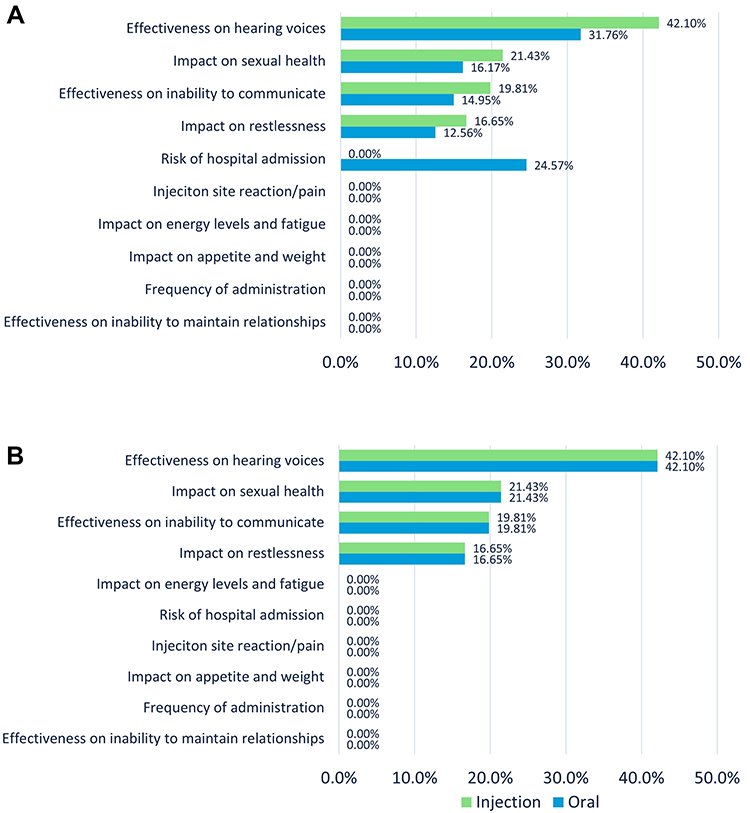 |
Figure 1 (A) Attribute importance for those hospitalised in the past two year. (B) Attribute importance for those not hospitalised in the past 2 years. |
No Recent Hospitalisation
For those not recently hospitalised, the most important attributes to affect treatment choice were effectiveness on hearing voices, impact on sexual health, effectiveness on inability to communicate and impact on restlessness (Figure 1). When holding other attributes constant (ie, no effect of other treatment attributes), the treatment status quo was preferred over injectable treatments (β = −0.870, T-ratio = −4.360) and to a lesser extent, the oral treatments (β = −0.311, T-ratio = −1.630). Between the two treatment modes, preference was greater for the oral over the injectable administration mode. However, if the injectable medication was more efficacious in managing hearing voices compared to the oral treatment, then some participants would switch treatments (see dashboard URL for more treatment scenario simulations).
BWS
The most valued long-term outcomes were having stable accommodation, being independent/autonomous and having good physical health (Figure 2). The least important outcomes included reducing the stigma associated with schizophrenia, reducing embarrassment due to the side effects of treatment, and being able to stop taking medication (Figure 2).
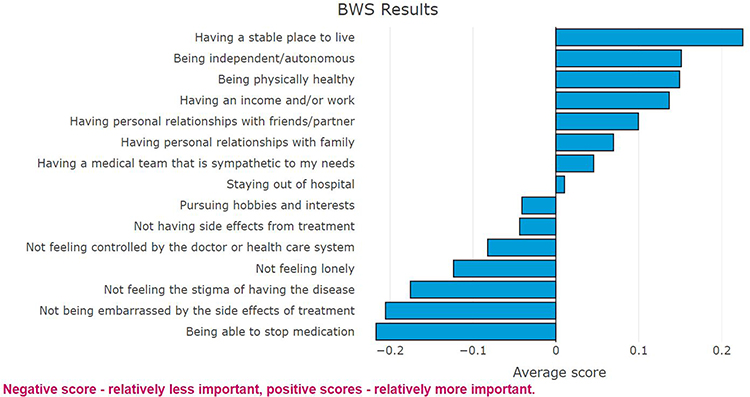 |
Figure 2 Best-Worst Scaling scores for long-term treatment outcomes. |
Discussion
The results from this study provide us with a better understanding of what aspects of treatment planning and outcomes are important to people with schizophrenia. A range of tools were used to obtain insights from this cohort, to uncover the value that people with schizophrenia place on their long-term outcomes. This research was undertaken within the context of assessing the importance of treatment attributes, treatment planning processes, and support programmes that these individuals need on their journey to recovery.
Despite adherence to antipsychotic medications remaining low among people living with schizophrenia7,9 and practice guidelines recommending that LAIs be offered to patients early in the clinical course of schizophrenia,3 most participants in the current study reported using oral antipsychotics (80.3%), and a general preference for oral administration modes. However, more than half of participants reported no experience with LAIs (54.5%) and only four people in this group had ever been offered LAIs by their treating clinicians. These low experience rates with LAIs and preference for oral modalities may be due to the perception that LAIs are more stigmatising and result in a loss of autonomy.35 Particularly as this cohort highly valued being independent/autonomous as a long-term treatment outcome. These beliefs are at odds with people who have used LAIs, who reported positive experiences, including better support and fewer relapses.8,36
This study provides an insight into the QoL of people living with schizophrenia in Australia. Compared to other published studies, participants reported a considerably lower QoL (60%) than those experiencing any mental illness (72.7%), those not mentally ill but who have experienced mental illness in the past (78.4%) and those who have never experienced mental illness (81.8%).25
Previous research has shown the importance of support services being tailored to the specific needs of people living with schizophrenia.37 However, we found that the use of patient support programmes was low (28.8%). Even more concerning was the large proportion of participants who did not know about or did not think that they would be eligible for NDIS support (56.7%). In Australia, an NDIS package enables access to patient support programmes and funding for ongoing day-to-day psychosocial, vocational and other support. The desire for patient support programmes, and barriers to understanding and accessing the NDIS should be considered in the context of current mental health reforms.
When looking at the treatment attributes that impact a person’s choice of treatment, the most important attribute was symptom control (hearing voices) and effectiveness on inability to communicate. Participants weighed up these benefits against the potential side effects, particularly their impact on sexual health, impact on restlessness and increased risk of hospitalisation (for those who have been recently hospitalised only). The treatment attributes that did not seem to affect the preferences of people with lived experience of schizophrenia included: frequency of administration, injection site pain, impact on appetite and weight and impact on energy levels and fatigue. This contrasts with the perceptions of clinicians that these are important.9,36 It should be noted that these results do not mean that non-significant DCE attributes were not important to participants. However, when faced with competing treatment attributes, these became significantly less important relative to the other attributes, when deciding between treatments.
The importance of long-term goals was assessed using the Best-Worst Scaling exercise and has provided further rationale for preferred treatment attributes that provide symptom stability. The most important long-term goal was to maintain autonomy, through which symptom control provides the foundations (eg, effectiveness on hearing voices attribute). Side effects and limitations of medications were found to be the least important long-term treatment outcomes. Although this may suggest that people with schizophrenia may be willing to trade-off treatment side effects in order to obtain symptom stability, it is still critically important to address the side effects associated with treatment. Not addressing these side effects can ultimately affect treatment adherence.3 However, these findings do add to a growing body of evidence indicating that people with schizophrenia are comfortable trading disadvantages associated with LAIs, particularly those related to injection pain and location of injection, in order to benefit from effective symptom reduction and long-term stability.5,16 As such, conversations about LAIs should be considered, as part of the treatment planning process.
There was a clear preference among this cohort to participate in the treatment decision process with their clinicians. This finding is consistent with prior research on shared decision-making among a cohort of people living with schizophrenia spectrum disorders in Australia.15 These findings suggest that shared decision-making should be utilised across all support services, including psychiatry, psychology, nursing, and general practice. Previously identified barriers to such an approach include extended consultation times and require the integration of inter-professional collaboration.38 This current study highlighted the importance of knowing and incorporating an individual’s long-term goals within a shared decision-making framework. The treatment planning process should also include the discussion and management of treatment side effects. Future studies could explore when patients want to be involved in shared decision-making themselves and when they would prefer for their family to have a role in the process.
Limitations
Due to the nature of the study design, the findings from this study may be limited in their representativeness of Australian adults living with schizophrenia. It is possible that participants able to access and complete an online survey may represent a higher functioning sample of people living with schizophrenia. However, the investigators acted on recommendations from consumer groups in order to reach as wide a sample as possible during recruitment. Additionally, data were collected through self-reported responses at one point in time. Furthermore, while all attributes were explained to participants, we cannot be certain that the participants properly understood the treatment options presented. It is also possible that despite our best efforts, all relevant attributes were not tested in our model. The relatively small sample size should also be considered when discussing the applicability of these results to everyday practice. It is for this reason that it is most important that people living with schizophrenia are consulted on their individual treatment preferences, as the aggregate data from this small sample may not adequately reflect the views of all.
While the study was sponsored by a pharmaceutical company, this was clearly disclosed at all stages of the research. Further, the study was run and administered by a third party, CaPPRe. Any possible biases in the study design, execution and reporting were also balanced by the inclusion of an independent clinician on the study team.
Conclusion
To date, there has been a lack of research around the treatment preferences of people living with schizophrenia treatment, particularly in the Australian setting, and the results from this study begin to fill this gap. Our findings show that people with schizophrenia would prefer to be included in the treatment conversations with their clinicians. It also highlights the importance of uncovering long-term goals of each individual and discussing all available treatment options that may facilitate this goal attainment, while managing personally relevant side effects and maintaining physical health. Participants cared most about long-term stability and effective symptom reduction, and these should be part of any treatment conversations.
Ethics Statement
The study was approved by the Bellberry Limited Human Research Ethics Committee (Application no. 2019-12-1161-A-1), as no author was affiliated with a research institution at the time of seeking ethics approval. The study complied with the Declaration of Helsinki.
Acknowledgments
The authors would like to acknowledge the valuable assistance provided by consumer organisations SANE Australia, One Door Mental Health, Neami National, Lived Experience Australia, and Mental Illness Fellowship of Australia (MIFA) who helped raise awareness of this study. Further, the authors would like to thank Karen Winkler, Senior Research Manager, CaPPRe for her contributions to the study design and data collection. Finally, the authors would like to thank Pippa Burns, PhD CMPP of WriteSource Medical Pty Ltd, Sydney, Australia, for providing medical writing support. Medical writing support was funded by Janssen-Cilag Australia Pty Ltd, Australia in accordance with Good Publication Practice (GPP3) guidelines (http://www.ismpp.org/gpp3).
Funding
Community and Patient Preference Research (CaPPRe) was commissioned by Janssen Australia and New Zealand to explore how patient value mapping could be used to examine preferences of people with a lived experience of schizophrenia. Janssen Australia are the manufacturers of Haldol, Invega Sustenna, Invega Trinza, Invega, Risperdal Consta and Risperdal. Editorial support for the development of this article was funded by Janssen-Cilag Australia Pty Ltd, Australia.
Disclosure
S Fifer and B Keen are employed by CaPPRe. CaPPRe has consulted to AbbVie, Amgen, AstraZeneca, Celgene, CSL Behring, Edwards, GSK, Ipsen, Janssen, Novo Nordisk, Roche, Sanofi, Shire and UCB, outside of the submitted work. A Puig and M McGeachie are employees of Janssen-Cilag Australia Pty Ltd. The authors report no other conflicts of interest in this work.
References
1. Mueser KT, McGurk S. Schizophrenia. Lancet. 2004;363(9442):2063–2072. doi:10.1016/S0140-6736(04)16458-1
2. Morgan VA, McGrath JJ, Jablensky A, et al. Psychosis prevalence and physical, metabolic and cognitive co-morbidity: data from the second Australian national survey of psychosis. Psychol Med. 2014;44(10):2163–2176. doi:10.1017/S0033291713002973
3. Galletly C, Castle DJ, Dark F, et al. Royal Australian and New Zealand College of Psychiatrists clinical practice guidelines for the management of schizophrenia and related disorders. Aust N Z J Psychiatry. 2016;50(5):1–117. doi:10.1177/0004867416641195
4. Kishimoto T, Hagi K, Kurokawa S, Kane JM, Correll CU. Long-acting injectable versus oral antipsychotics for the maintenance treatment of schizophrenia: a systematic review and comparative meta-analysis of randomised, cohort, and pre–post studies. Lancet Psychiatry. 2021;8(5):387–404. doi:10.1016/s2215-0366(21)00039-0
5. Lindenmayer JP, Glick ID, Talreja H, Underriner M. Persistent barriers to the use of long-acting injectable antipsychotics for the treatment of schizophrenia. J Clin Psychopharmacol. 2020;40(4):346–349. doi:10.1097/JCP.0000000000001225
6. Jaaskelainen E, Juola P, Hirvonen N, et al. A systematic review and meta-analysis of recovery in schizophrenia. Schizophr Bull. 2013;39(6):1296–1306. doi:10.1093/schbul/sbs130
7. Higashi K, Medic G, Littlewood KJ, Diez T, Granstrom O, De Hert M. Medication adherence in schizophrenia: factors influencing adherence and consequences of nonadherence, a systematic literature review. Ther Adv Psychopharmacol. 2013;3(4):200–218. doi:10.1177/2045125312474019
8. Kaplan G, Casoy J, Zummo J. Impact of long-acting injectable antipsychotics on medication adherence and clinical, functional, and economic outcomes of schizophrenia. Patient Prefer Adherence. 2013;7:1171–1180. doi:10.2147/PPA.S53795
9. Kane JM, Correll CU. Optimizing treatment choices to improve adherence and outcomes in schizophrenia. J Clin Psychiatry. 2019;80(5). doi:10.4088/JCP.IN18031AH1C
10. Weiden P, Kozma C, Grogg A, Locklear J. Partial compliance and risk of rehospitalization among California medicaid patients with schizophrenia. Psychiatr Serv. 2004;55(8):886–891. doi:10.1176/appi.ps.55.8.886
11. Fiorillo A, Barlati S, Bellomo A, et al. The role of shared decision-making in improving adherence to pharmacological treatments in patients with schizophrenia: a clinical review. Ann Gen Psychiatry. 2020;19:43. doi:10.1186/s12991-020-00293-4
12. Elwyn G, Laitner S, Coulter A, Walker E, Watson P, Thomson R. Implementing shared decision making in the NHS. BMJ. 2010;341:c5146. doi:10.1136/bmj.c5146
13. Barry MJ, Edgman-Levitan S. Shared decision making–pinnacle of patient-centered care. N Engl J Med. 2012;366(9):780–781. doi:10.1056/NEJMp1109283
14. Hamman J, Cohen R, Busch R, Busch R, Kissling W. Shared decision making and long-term outcome in schizophrenia treatment. J Clin Psychiatry. 2007;68(7):992–997. doi:10.4088/JCP.v68n0703
15. Carrotte ER, Hartup ME, Lee-Bates B, Blanchard M. “I think that everybody should be involved”: what informs experiences of shared decision-making in supporting people living with schizophrenia spectrum disorders? Patient Educ Couns. 2021;104(7):1583–1590. doi:10.1016/j.pec.2020.11.012
16. Bridges JF, Beusterien K, Heres S, et al. Quantifying the treatment goals of people recently diagnosed with schizophrenia using best-worst scaling. Patient Prefer Adherence. 2018;12:63–70. doi:10.2147/PPA.S152870
17. Blackwood C, Sanga P, Nuamah I, et al. Patients’ preference for long-acting injectable versus oral antipsychotics in schizophrenia: results from the patient-reported medication preference questionnaire. Patient Prefer Adherence. 2020;14:1093–1102. doi:10.2147/PPA.S251812
18. Fifer S, Rose J, Hamrosi KK, Swain D. Valuing injection frequency and other attributes of type 2 diabetes treatments in Australia: a discrete choice experiment. BMC Health Serv Res. 2018;18(1):675. doi:10.1186/s12913-018-3484-0
19. Fifer SJ, Ho KA, Lybrand S, Axford LJ, Roach S. Alignment of preferences in the treatment of multiple myeloma - A discrete choice experiment of patient, carer, physician, and nurse preferences. BMC Cancer. 2020;20(1):546. doi:10.1186/s12885-020-07018-6
20. Ho KA, Acar M, Puig A, Hutas G, Fifer S. What do Australian patients with inflammatory arthritis value in treatment? A discrete choice experiment. Clin Rheumatol. 2020;39(4):1077–1089. doi:10.1007/s10067-019-04843-4
21. Fifer S, Galinsky J, Richard S. Myeloma patient value mapping: a discrete choice experiment on myeloma treatment preferences in the UK. Patient Prefer Adherence. 2020;14:1283–1293. doi:10.2147/PPA.S259612
22. Fifer S, Puig A, Sequeira V, et al. Understanding treatment preferences of Australian patients living with treatment-resistant depression. Patient Prefer Adherence. 2021;15:1621–1637. doi:10.2147/PPA.S311699
23. World Medical Association. World medical association declaration of Helsinki: ethical principles for medical research involving human subjects. JAMA. 2013;310(20):2191–2194. doi:10.1001/jama.2013.281053
24. Endicott J, Nee J, Harrison W, Blumenthal R. Quality of life enjoyment and satisfaction questionnaire: a new measure. Psychopharmacol Bull. 1993;29(2):321–326.
25. Schechter D, Endicott J, Nee J. Quality of life of ‘normal’ controls: association with lifetime history of mental illness. Psychiatry Res. 2007;152(1):45–54. doi:10.1016/j.psychres.2006.09.008
26. Thurstone LL. A law of comparative judgment. Psychol Rev. 1927;34(4):273. doi:10.1037/h0070288
27. Lancaster KJ. A new approach to consumer theory. J Polit Econ. 1966;74:132–157. doi:10.1086/259131
28. McFadden D. Conditional logit analysis of qualitative choice behaviour. In: Frontiers of Econometrics. Academic Press; 1974.
29. Soekhai V, de Bekker-Grob EW, Ellis AR, Vass CM. Discrete choice experiments in health economics: past, present and future. Pharmacoeconomics. 2019;37(2):201–226. doi:10.1007/s40273-018-0734-2
30. Rose J, Bliemer M. Constructing efficient stated choice experimental designs. Transp Rev. 2009;29(5):587–617. doi:10.1080/01441640902827623
31. Reed Johnson F, Lancsar E, Marshall D, et al. Constructing experimental designs for discrete-choice experiments: report of the ISPOR conjoint analysis experimental design good research practices task force. Value Health. 2013;16(1):3–13. doi:10.1016/j.jval.2012.08.2223
32. Bridges JF, Hauber AB, Marshall D, et al. Conjoint analysis applications in health–a checklist: a report of the ISPOR good research practices for conjoint analysis task force. Value Health. 2011;14(4):403–413. doi:10.1016/j.jval.2010.11.013
33. Hensher DA, Rose JM, Greene WH. Applied Choice Analysis.
34. Louviere J, Flynn T, Marley A. In Best-Worst Scaling: Theory, Methods and Applications. Cambridge University Press; 2015:316–331.
35. Das AK, Malik A, Haddad PM. A qualitative study of the attitudes of patients in an early intervention service towards antipsychotic long-acting injections. Ther Adv Psychopharmacol. 2014;4(5):179–185. doi:10.1177/2045125314542098
36. Cahling L, Berntsson A, Broms G, Ohrmalm L. Perceptions and knowledge of antipsychotics among mental health professionals and patients. BJPsych Bull. 2017;41(5):254–259. doi:10.1192/pb.bp.116.055483
37. El-Mallakh P, Findlay J. Strategies to improve medication adherence in patients with schizophrenia: the role of support services. Neuropsychiatr Dis Treat. 2015;11:1077–1090. doi:10.2147/NDT.S56107
38. Huang C, Plummer V, Lam L, Cross W. Perceptions of shared decision-making in severe mental illness: an integrative review. J Psychiatr Ment Health Nurs. 2020;27(2):103–127. doi:10.1111/jpm.12558
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.