")
Back to Journals » Clinical Interventions in Aging » Volume 17
Understanding the Role, Quality of Life and Strategies Used by Older Carers of Older People to Maintain Their Own Health and Well-Being: A National Australian Survey
Authors Lee DCA , Burton E , Slatyer S , Jacinto A, Oliveira D, Bryant C, Khushu A, Tiller E, Lalor A, Watson M, Layton N, Brusco N, Hill KD
Received 29 July 2022
Accepted for publication 5 October 2022
Published 25 October 2022 Volume 2022:17 Pages 1549—1567
DOI https://doi.org/10.2147/CIA.S384202
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Maddalena Illario
Den-Ching A Lee,1,2 Elissa Burton,3,4 Susan Slatyer,5 Alessandro Jacinto,6 Déborah Oliveira,7 Christina Bryant,8 Anjali Khushu,9 Elizabeth Tiller,9 Aislinn Lalor,2,10 Moira Watson,5 Natasha Layton,2 Natasha Brusco,2 Keith D Hill2,11
1School of Primary and Allied Health Care, Faculty of Medicine, Nursing and Health Sciences, Monash University, Frankston, Victoria, 3199, Australia; 2Rehabilitation, Ageing and Independent Living (RAIL) Research Centre, Monash University, Frankston, Victoria, 3199, Australia; 3Curtin School of Allied Health, Faculty of Health Sciences, Curtin University, Bentley, Western Australia, 6102, Australia; 4enAble Institute, Faculty of Health Sciences, Curtin University, Bentley, Western Australia, 6102, Australia; 5Centre for Healthy Ageing, Murdoch University, Murdoch, Western Australia, 6150, Australia; 6Faculty of Geriatric Medicine, Federal University of São Paulo (UNIFESP), São Paulo, Brazil; 7Medical School, Faculty Postgraduate Department of Psychiatry, Federal University of Sao Paulo – UNIFESP, Sao Paulo-SP, Brazil; 8Melbourne School of Psychological Sciences, University of Melbourne, Melbourne, Victoria, 3010, Australia; 9Department of Geriatrics (Falls Prevention Service), Peninsula Health, Frankston, Victoria, 3199, Australia; 10Department of Occupational Therapy, Monash University, Melbourne, Victoria, 3199, Australia; 11National Centre for Healthy Ageing, Monash University and Peninsula Health, Frankston, Victoria, 3199, Australia
Correspondence: Den-Ching A Lee, School of Primary and Allied Health Care, Faculty of Medicine, Nursing and Health Sciences, Monash University, Moorooduc Highway, Frankston, Victoria, 3199, Australia, Tel +613 9904 4662, Email [email protected]
Introduction: Carers play a critical role in supporting older people with health problems to remain living at home. This study aimed to understand the role and quality of life of older carers of older people and identify strategies used to manage their own health and well-being.
Methods: Older carers (aged ≥ 50 years) of older people (aged ≥ 65 years) in Australia participated in a cross-sectional survey focused on carer roles, self-rated health, information and activities used to maintain their carer role and health, barriers to accessing health care, and assessment of quality of life (QoL) using the Dementia Quality of Life Scale for Older Family Carers. Multiple regression analysis examined relationships between variables and the QoL outcome.
Results: The survey was completed by 189 older carers (mean age: 68 years; SD = 9.3). Most were female (83.5%), 80.2% providing care daily and 47.8% provided ≥six hours care daily. Almost half (45.1%) self-reported their health as average or below. Despite rating ensuring personal health as very important (mean importance 8/10), only 46.3% reported receiving support from their general practitioner for their carer role. The most common barrier to accessing care for themselves was “not having enough time”. Factors independently associated with poorer carer QoL were living with the care-recipient, caring for someone with depression/anxiety and poor care-recipient health. Factors independently associated with higher carer QoL were placing high importance on personal health, receiving assistance from a specialist clinic as a carer, and older age.
Conclusion: Older carers of older people provide high levels of care and experience reduced quality of life. Innovative approaches that provide integrated care and support for older carers to promote their QoL are urgently needed.
Keywords: carers, older, health, dementia, quality of life, barriers
Introduction
Many older people who live with chronic illness depend on support from informal carers, along with community services, to live independently at home. Informal carers (hereafter referred to as carers) are defined as
a family member/s and/or friend/s who routinely supports the older person through assistance with household tasks; self-care and mobility; emotional and social support; treatments, medication and responding to acute health needs; advocacy and care coordination; or surrogate decision-making.1
While there can be benefits for carers of older people, such as satisfaction and a sense of meaning,2 personal strength and aging readiness,3 many experience personal health problems and are not able to focus sufficiently on their own well-being.4 Providing care can also have detrimental effects on the physical and mental health of carers.5 For example, carers of people with dementia have demonstrated significantly higher levels of depression and anxiety compared to non-carers,6 and long-term carers of end-stage cancer patients are reported to experience weight loss7 and fatigue.8 Additional challenges in caring for an older person with chronic illnesses may involve a role in which care activities increase in number and complexity as the older person becomes more unwell, frail, and dependent.9 Furthermore, the care support challenges for carers of older people in poor health may also increase over time as the carers themselves age.9
Almost half (47%) of all carers in Australia are aged over 55 years.10 While generic factors can affect the health and well-being of carers of all ages, there are additional factors and potentially different intervention approaches that may be more effective and relevant for older carers. However, studies investigating carer needs and supportive interventions mostly focus on a particular health condition,6,11,12 which may not be relevant to carers of older people more generally. For example, carers of older people with dementia primarily sought information about how to prepare for the role, including working with responsive behaviors of care recipients,13 while other studies have found neuropsychiatric symptoms experienced by people with Parkinson’s Disease are associated with increased carer burden.14 Carer burden can be defined as the strain or load borne by a person who cares for a chronically ill, disabled, or older family member.15 It is an individual’s subjective evaluation of the present caregiving situation and measurement of the degree of difficulties.16 The negative responses include both subjective and objective outcomes. Thus, caregiver burden is a complex, multi-dimensional concept.16
A number of intervention approaches have been shown to promote carers’ health and well-being, and their quality of life (QoL). For this paper, health and well-being of carers refer to their own physical and mental health status. QoL of carers is interpreted as the individual’s point of view towards life as a whole, for example life satisfaction, life contentment and happiness.17 Especially among older carers, aspects such as concerns about their own health and future; energy and vitality in their care provision; role conflicts in being an older carer; identity; the higher impact of financial situations; confidence in providing care whilst being a frail older person; isolation and loneliness derived from a full-time carer role; and sleep deprivation are some of the issues reported by older carers as being important to their own QoL.18 There is evidence that single intervention approaches, such as physical activity19 or psychoeducation20 and multi-component interventions, eg, home environmental equipment and skill building are effective,21 although most of this research focuses on carers of all ages. Currently, the extent to which health services provide needs-based assessment and tailored support to protect older carers from the negative effects of their caring role is unclear.
Given the issues raised above, it is important to better understand the specific needs of older carers, in particular the characteristics of older carers, their caring role, how they manage their health and well-being, and factors influencing their QoL. Therefore, the aims of this study were to 1) describe characteristics of care provided by older carers of an older person; 2) identify what and where information was sought and support strategies used by older carers of older people to manage their own physical and mental health, and perceived barriers to their use; and 3) evaluate their QoL and factors associated with QoL in older carers.
Materials and Methods
Design
A cross-sectional survey.
Participants
Participants were older carers of older people in Australia. The inclusion criteria were being an informal carer who 1) was aged ≥50 years, 2) was community-dwelling, 3) self-reported that they were providing informal care for an older person aged ≥65 years, 4) was providing informal care for at least six months, and 5) was able to read and understand English. There were no exclusion criteria relating to the number and types of health conditions of the care recipient.
Survey Instrument
Researchers and clinicians experienced in carer support and/or carer health developed the survey. Initial items were drafted based on existing research and feedback from a working group that comprised project team members and consumer representatives from a carer’s organization. Further modifications to the survey were made to improve clarity of the items after the survey was piloted with older carers.
The final survey consisted of predominantly closed-ended questions across five sections: 1) demographics, 2) carer role (eg, length of time of care provision, types of care provided, assistance received), 3) information and support service/activity older carers used to maintain their carer role and/or manage their physical and mental health (eg, advice/referral/assistance from the general practitioner or doctor), specialist geriatrics clinics (eg, falls and mobility clinics, memory clinics), and other organizations, 4) carers’ ratings of i) personal health, ii) care recipient’s health, and iii) importance placed on ensuring personal and care recipient’s health and well-being, and 5) perceived barriers identified by older carers to managing their physical and mental health. Several questions provided a range of response options, including an option of “Other” in which participants could provide more detail in an open text box.
Carers’ quality of life (QoL) was assessed using the Dementia Quality of Life Scale for Older Family Carers (DQoL-OC).22 Carers’ ratings of personal and care recipient’s health were structured as a 5-point Likert-styled scale from 1 = “very good” to 5 = “very poor”, with 3 = “average” as the mid-point, whereas importance placed on ensuring personal and care recipient’s health and well-being were presented as an 11-point visual analogue scale where “0” = “no importance” and 10 = “as much as is necessary”.
The DQoL-OC scale is a validated 22-item scale that measures QoL of older carers. It has high re-test reliability (r = 0.835) and internal consistency (Cronbach’s α = 0.936).22 Of the 22 items, six ask for information about different aspects associated with a carer’s role (Likert-styled ratings from “1” to “5” with “Always” scoring 1 point, “Frequently” 2 points, “Occasionally” 3 points, “Rarely” 4 points or “Never” 5 points), 11 items regarding their feelings about different aspects of their life (“Very frequently” scoring 1 point, “Frequently” 2 points, “Occasionally” 3 points, “Rarely” 4 points or “Never” 5 points), and five on different aspects of their life as a carer (“Very dissatisfied” scoring 1 point, “Dissatisfied” 2 points, “Neither satisfied or dissatisfied” 3 points, “Satisfied” 4 points or “Very satisfied” 5 points). Points were added across all items to form an overall carer’s QoL score ranging from 22 (minimum) to 110 (maximum), where a lower score indicates poorer QoL.
The full survey questionnaire is available from the authors on request.
Procedure
Human research ethics approval was obtained prior to recruitment (Monash University project ID: 27,379, South Metropolitan Health Service project ID: 04661, Murdoch University project ID: 2021/083). Survey questions were disseminated via online survey software (www.Qualtrics.com) between July 2021 and December 2021.
Older carers were recruited through organizations and networks, eg, Carers Victoria, Dementia Australia, support groups from Carers’ Victoria and Western Australia, and Western Australia’s Melville Cares, Chorus Australia, Parkinson’s Western Australia, Diabetes Western Australia and Rise Network, who used their contacts, newsletters and social media to promote the survey. Facebook and Twitter were used to promote the survey as well as the e-bulletin of the Rehabilitation, Ageing and Independent Living (RAIL) Research Centre of Monash University, and dissemination through researchers’ contacts/networks. An email including a promotional flyer, an explanatory statement and the URL link to the survey was sent by a researcher to the organizations and networks. Paper-based surveys were provided to the organizations to distribute to older carers who did not have internet access. The STROBE (Strengthening the Reporting of Observational studies in Epidemiology) Checklist: Cross-sectional Studies was followed for reporting this research.23 Consent to participate was implied and obtained when participants returned or submitted their survey.
Data Analysis
Responses to closed-ended questions including “Other” option, and the DQoL-OC scores were summarized using descriptive statistics. Text responses to the “Other” options were categorized and grouped and included with the list of response options provided in the questionnaire.
A data driven approach examined the relationships between variables with older carer’s QoL outcome using univariable linear regression analyses, providing coefficients and 95% confidence intervals. The dependent variable was QoL as measured by the DQoL-OC scale. The independent variables were characteristics of older carers (eg, age, gender), carer role (eg, types of health condition of the care recipient, years of caring role, number of care hours), information and support service/activity used by older carers (eg, whether general practitioner or specialist clinic provided assistance/advice/referrals), carers’ ratings of personal and care recipients’ health, carers’ ratings of importance placed on ensuring personal, and care recipient’s health and well-being. Independent variables that had categorical data were coded as dichotomous variables, eg, each health condition was dichotomized as to whether the care recipient had the health condition or not. Independent variables that had multi-categorical ordinal data, eg, level of education, care hours per day, rating of health, were treated as interval data assuming a linear relationship with the carer’s QoL outcome.
Next, a multiple regression analysis was performed to determine if any significant relationships between independent variables (taken from the univariable regression analysis above) and carer’s QoL outcome remained after adjusting for other potential variables. Assumptions of multiple regression were met for linear relationships between the outcome variable and the independent variables, multivariate normality, absence of multi-collinearity and homoscedasticity. The number of independent variables included in the multiple regression analysis will be limited so that there are a minimum of 10 participants for each covariate. A stepwise backwards elimination approach was taken to build the multiple regression model.24 First, independent variables that had a p-value≤0.20, based on Hosmer et al’s framework,24 for the univariable associations with carer’s QoL outcome were entered into the starting model. Second, any variable that did not have a significant adjusted association with the carer’s QoL outcome was removed one at a time from the model in the order of descending p-values and the remaining model re-examined, until all variables retained in the model had a significant adjusted association with the carer’s QoL outcome. The two-tailed alpha criterion for statistical testing was set at p < 0.05. Data analyses were undertaken using STATA SE version 15.
Results
Two hundred and fourteen people returned the survey. Twenty-five did not meet the eligibility criteria and terminated the survey. Of the 189 participants who completed the survey, 83.5% were female, mean age was 68 years (SD = 9.3), and 73.4% lived with their care recipient (Table 1).
 |
Table 1 Demographics of Older Carers |
The characteristics of participants’ carer roles are presented in Table 2. Over half of the participants (56.2%) were caring for their spouse/partner. Care recipients had a mean age of 81.7 years (SD = 8.7), and 56.2% were male. Dementia (41.9%) was the largest single category of health condition among the care recipients. Nearly 60% of carers reported that they had been providing care for ≥5 years, 47.8% were providing ≥6 hours of care daily, and 80.2% were providing care for 6 to 7 days per week. The most frequent tasks that participants assisted the care recipients with were shopping (89.6%), transport (89.6%), financial/legal/personal administrative matters (89%) and cleaning or tidying the home (85.7%). Half of the participants (50.3%) did not receive help from others in their day-to-day caring role. Of those who did so, home care organizations were the largest source of help (70.3%), compared to family members, friends or other providers combined. The most common type of help sourced was with chores or cleaning around the house (63%). See Table 2.
 |
Table 2 Responses from Older Carers About Characteristics of Their Carer Role |
Information and/or assistance to maintain the carer role were obtained from a variety of sources (see Table 3 for details). Carer’s organizations (eg, Carers Victoria and Carers Western Australia) were the major organizations from which over 70% of participants obtained information to help maintain their carer role. About one-third (30.4%) obtained information from Dementia Australia. Information was commonly accessed from the internet (51.7%) and carers’ websites (42.2%). Despite 83% reporting that their general practitioner knew of their carer role, only 46.3% of these carers reported receiving assistance, guidance or referrals from their general practitioner to help with their carer role. Additionally, 58% of carers had attended a specialist clinic appointment for their care recipient, yet only 19% of these carers reported receiving specific assistance from clinic staff to support them in their carer role.
 |
Table 3 Responses from Older Carers About the Information/Support Service/Activity They Used to Maintain Carer Role and/or Manage Their Personal Physical and Mental Health While Undertaking the Carer Role |
Over 90% of participants reported engaging in at least one activity to maintain their physical and mental health. The most reported activities for maintaining physical health were consulting their general practitioner (62.5%), walking (52.3%), ensuring good diet and nutrition (44.3%), and getting adequate sleep (43.2%). The most reported activities for maintaining mental health were talking to family and friends (62.4%), participating in activities independent of the care recipient (59%), exercise (46.6%) and seeing their general practitioner when required (46.1%) (See Table 3).
Participants rated their personal and care recipient’s health and the importance they placed on ensuring these (see Table 4). Although participants rated highly the importance of ensuring personal health and well-being (mean rating of 8/10) and care recipient’s health and well-being (mean rating of 9.6/10), almost half (45.1%) rated their personal health as “average” or “below average”. Most participants (80%) had encountered at least one barrier to maintaining their personal and care recipient’s health and well-being. The most frequently reported barriers to maintain their own health and well-being were “not having enough time” (54.4%), “competing demands” (36.1%), “the carers’ own health problems” (28.9%) and “Other” (18.9%), which included carer stress and fatigue (5.6%), care recipient’s disability/medical condition (2.8%) and work commitment (1.7%). All carer responses are summarized in Table 4. Similarly, the most reported barriers to ensuring care recipient’s health and well-being were “the carer’s own health problems” (35%), followed by “Other” (31.2%), “not having enough time” and “competing demands” (both 26.8%). Most common items listed under the “Other” option for barriers included care recipient’s refusal to accept help/non-compliance with medical advice (6.6%), care recipient’s disability/medical condition (3.8%) and work commitment (3.3%), and these have been included with other responses in Table 4.
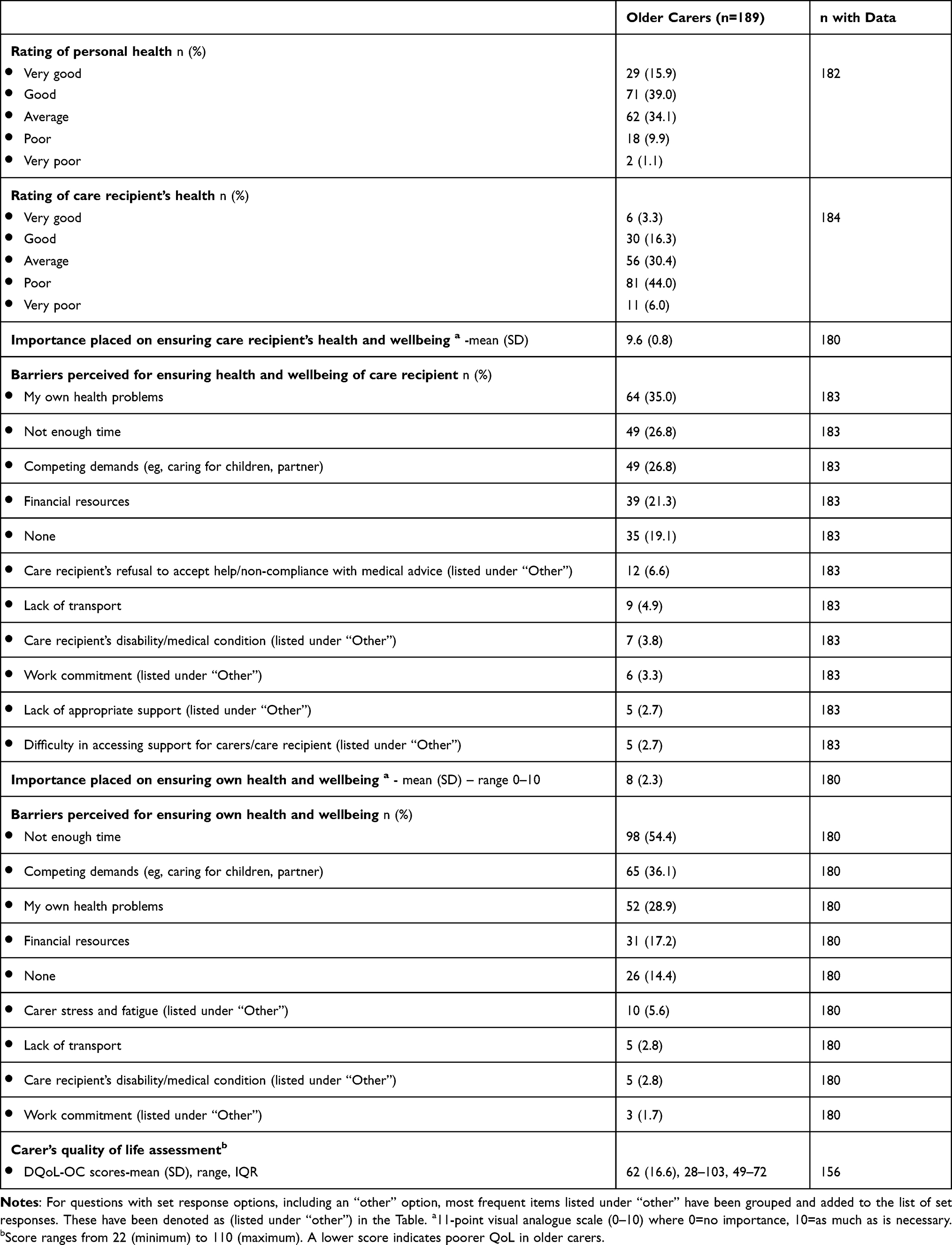 |
Table 4 Carer’s Ratings of Personal and Care Recipient’s Health, Importance Placed on Ensuring Personal and Care Recipient’s Health and Wellbeing, Barriers Perceived for Ensuring Personal and Care Recipient’s Health and Wellbeing, and Carer’s Quality of Life Assessment |
The mean DQoL-OC score of participants was 62 (SD = 16.6, range 28–103, IQR 49–72) indicating moderately reduced QoL (see Table 4). Univariable linear regression analyses showed that a higher carer QoL (indicated by a higher score) was associated with being older [coefficient (95% CI): 0.37 (0.09, 0.65)], having an older care recipient [0.31 (0.01, 0.62)], placing a higher importance on ensuring own health and well-being [1.45 (0.31, 2.59)], or receiving assistance from specialist clinics with their carer role [9.47 (0.57, 18.36)]. A lower carer QoL (indicated by a lower score) was associated with co-residing with the care recipient [coefficient (95% CI): −8.01 (−13.80, −2.21)], caring for someone who had depression or anxiety [−11.37 (−16.71, −6.02)], providing more hours of care per day [−3.83 (−6.20, −1.46)], providing more days of care per week [−5.76 (−9.29, −2.23)], having a poorer rating of personal health [−3.32 (−6.10, −0.53)] or care recipient’s health [−2.86 (−5.67, −0.04)], and having accessed information from organizations to help in their caring role [−6.98 (−12.85, −1.11)] (Table 5).
 |
Table 5 Univariable Associations Between Older Carers’ Quality of Life (DC-QoL-OC Scores) and Characteristics of Older Carers, Carer Role, Information and Support Service/Activity Used to Maintain Carer Role and/or Manage Personal Physical and Mental Health |
The multiple regression model found that carers’ older age [adjusted coefficient (95% CI): 0.44 (0.08, 0.81)], higher self-rated importance on personal health and well-being [1.74 (0.41, 3.07)], or receipt of assistance from specialist clinic staff [8.71 (0.62, 16.79)], were independently associated with a higher carer QoL. In contrast, carers’ poorer QoL was independently associated with living with the care recipient [adjusted coefficient (95% CI): −10.98 (−18.09, −3.87)], caring for someone who had depression or anxiety [−9.68 (−16.27, −3.09)], and rating their care recipient’s health as poor [−3.41 (−6.64, −0.19)]. These factors explained collectively 35% of the variance in the older carer’s QoL.
Discussion
This research highlights factors that contribute to older carers’ QoL when caring for an older person in poor health. The extensive caring role undertaken by many older carers and the barriers this can present to maintaining their own health, as well as strategies used to promote their physical and mental well-being were evident. The survey included older carers from across Australia, the majority (80%) of whom reported providing care to an older person almost daily, with almost 50% providing six or more hours of care in their daily carer role. They were typically caring for older people who had multi-morbidity of more than one disease, with dementia being the most prevalent disease. The most commonly accessed (73%) source of information was websites provided by carer support organizations. In contrast, less than half of these older carers reported receiving support in their caring role from their general practitioner and even fewer (only 19% of the 58% who attended a specialist clinic with the care recipient) received assistance for themselves from specialist clinic staff. This was despite almost half of participants rating their own health as only “average” or “below average”. Participants in this study acknowledged the importance of maintaining their own health to sustain their caring, but reported encountering various barriers to accessing support, most commonly a perceived lack of time to care for themselves. It was not surprising therefore that the self-reported QoL of older carers in this study, using the validated DQoL-OC,22 was low.
The study found an association between lower QoL and living with the care recipient. There is emerging evidence that co-residence may negatively impact carer QoL for carers of people with specific health problems, eg, dementia.25 Caring for someone who had depression or anxiety was also found to be associated with lower carer QoL. These findings were consistent with a study of carers of mental health patients that showed carers had a significantly lower QoL score compared to non-carers.26 In this current study, being an older carer was associated with a higher QoL, although the relationship between carer age and carer QoL was inconsistent with a systematic review of factors influencing QoL in carers of people with dementia.27
This current study’s findings did not show that care burden, which is reflected by the number of care hours, to be related to carer QoL. However, the sample of carers experienced high care burden overall. Some factors are known to increase carer burden. Firstly, the survey found 80% of carers rated their care recipients’ health to be “average” or “below average”, which has been associated with increased carer burden due to a higher level of disability of care recipients.10 Secondly, the survey showed over 40% of care recipients had dementia, which has been associated with higher levels of carer burden in several previous studies.28,29 Thirdly, perceived barriers to accessing support to help with the caring role reported in this study resonate with the many obstacles described elsewhere by carers who balance caregiving with other demands, including career and relationships, putting them at increased risk for burden, stress, depression, and a variety of health complications.30 Indeed, 50% of the participants in this study rated their health as only “average” or “below average”, and a range of modifiable barriers to maintaining their health and well-being were identified. Over 50% of participants did not receive help in their daily care role, which may explain why “not having enough time” was the most reported barrier to maintaining their own health and well-being. Reducing barriers for accessing support services and making the navigation of support services more user-friendly for carers are tangible ways within the current system to enable carers more time to focus on their own health and well-being. Policy and funding allocation to increase availability and reduce waiting time for home care could also reduce carer burden. A recent systematic review found community care coordination, a service that can be provided by community care organizations, may potentially help maintain the carer role and reduce the rate of residential aged care admissions for people living with dementia.31
It is interesting that receiving assistance with their caring role from specialist clinics was associated with a better carers’ QoL. Currently, there is no systematic approach for assessing carer needs and providing tailored support as routine practice in primary health care and health services in Australia. This may have been one of the reasons why a low proportion of carers reported receiving help, assistance, guidance or advice through these sources to maintain their health and carer role. In the United Kingdom, carers have a statutory right to have their needs assessed in addition to the assessments routinely provided for the people they care for.32 There is a need in Australia to explore novel approaches, which may include formal dedicated services, eg, a specialist carers’ clinic such as one that has been developed in Sao Paulo, Brazil,33 to support systematic assessment and support to promote QoL of older carers of older people.
Several limitations associated with this research need to be considered. A data-driven approach was employed to analyze the relationships between variables and older carer’s QoL outcome as an effective method to deal with complex and unknown problems. However, results derived from this analytical approach rely on the breath of data collected, and hence this may affect the interpretation of results.34 For example, there could have been other factors that may have affected older carers’ QoL that were not investigated in the survey, such as stressful life events or care needs of other family members. Moreover, older carers who have more interest in ensuring their health and well-being may be more likely to have participated in this survey. Furthermore, there is a possibility that some terms in the survey may be interpreted differently between carers (eg, what activities are included or not included as carer activities when responding to survey questions, such as number of hours per week performing the caring role), despite providing a definition of a carer, and listing specific activities (not exhaustive though) of carer activities. This may result in some variability in responses to some of the sample characteristics. The sample was limited to people able to complete the survey in English; therefore, carers who were not proficient in English language may have been less likely to participate. Given Australia’s large multicultural population, surveying needs of carers from culturally and linguistically diverse backgrounds, who may have differing needs and factors influencing their caring role and health, is an important area for future research.
Conclusions
Most of the older carers of older people in this survey experienced a high level of carer burden and poor QoL. Assistance or advice on how to maintain carers’ personal health and well-being, and thereby sustaining their carer role, were not routinely provided by primary care or health services. Carers most frequently sought information from carer organizations’ websites and the internet. Strategies to address some modifiable barriers (eg, improve ease in navigating and accessing support services) may help maintain carers’ own health and well-being and that of their care recipients. Providing innovative approaches to specifically target the unmet needs of older carers of older people, such as developing specialist carer clinics to provide integrated care and support for older carers, may improve QoL and help sustain their carer role in the longer term.
Data Availability
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Ethical Approval and Informed Consent
Human research ethics approval was obtained prior to recruitment (Monash University project ID: 27379, South Metropolitan Health Service project ID: 04661, Murdoch University project ID: 2021/083). Consent to participate was implied and obtained when participants returned or submitted their survey.
Author Contributions
All authors have made a significant contribution to the work reported, whether it is the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas. D.C.A. Lee and K.D. Hill have written the article. All other authors have substantially revised or critically reviewed the article. All authors have agreed on the journal to which the article is submitted, reviewed, agreed on all versions of the article before submission, during revision, the final version accepted for publication, and any significant changes introduced at the proofing stage, and agreed to take responsibility and be accountable for the contents of the article.
Funding
This work was supported by the National Centre for Healthy Ageing of Monash University and Peninsula Health Australia. The funding body had no involvement in the study design; in the collection, analysis and interpretation of data; in the writing of the report; and in the decision to submit the article for publication.
Disclosure
Dr Elissa Burton’s time was supported by funding from an NHMRC Investigator Grant. The authors report no other conflicts of interest in this work.
References
1. National Academies of Sciences E, and Medicine. Families caring for an aging America. National Academics press; 2016.
2. Johansson MF, McKee KJ, Dahlberg L, Summer Meranius M, Williams CL, Marmstål Hammar L. Negative impact and positive value of caregiving in spouse carers of persons with dementia in Sweden. Int J Environ Res Public Health. 2022;19(3):1788. doi:10.3390/ijerph19031788
3. Hogstel MO, Linda Cox C, Walker C. Caring for older adults: the benefits of informal family caregiving. J Theory Constr Test. 2005;9(2):55–60.
4. Liu Z, Heffernan C, Tan J. Caregiver burden: a concept analysis. Int J Nurs Sci. 2020;7(4):438–445. doi:10.1016/j.ijnss.2020.07.012
5. Schulz R, Sherwood PR. Physical and mental health effects of family caregiving. Am J Nurs. 2008;108(9 Suppl):23–27. doi:10.1097/01.NAJ.0000336406.45248.4c
6. Madaleno TR, Moriguti JC, Ferriolli E, De Carlo M, Lima NKC. Mood, lifestyle and cardiovascular risk factors among older caregivers of patients with Alzheimer’s disease dementia: a case-control study. Aging Clin Exp Res. 2019;31(11):1609–1614. doi:10.1007/s40520-019-01212-8
7. Lee YH, Liao YC, Shun SC, et al. Trajectories of caregiver burden and related factors in family caregivers of patients with lung cancer. Psychooncology. 2018;27(6):1493–1500. doi:10.1002/pon.4678
8. Ateş G, Ebenau AF, Busa C, et al. ”Never at ease” - family carers within integrated palliative care: a multinational, mixed method study. BMC Palliat Care. 2018;17(1):39. doi:10.1186/s12904-018-0291-7
9. Alves S, Ribeiro O, Paúl C. Unmet needs of informal carers of the oldest old in Portugal. Health Soc Care Community. 2020;28(6):2408–2417. doi:10.1111/hsc.13063
10. Deloitte. The value of informal care in 2020; 2020. Available from: https://www2.deloitte.com/au/en/pages/economics/articles/value-of-informal-care-2020.html.
11. Lök N, Bademli K. Pilot testing of the “First You Should Get Stronger” program among caregivers of older adults with dementia. Arch Gerontol Geriatr. 2017;68:84–89. doi:10.1016/j.archger.2016.09.006
12. Leng M, Zhao Y, Xiao H, Li C, Wang Z. Internet-based supportive interventions for family caregivers of people with dementia: systematic review and meta-analysis. J Med Internet Res. 2020;22(9):e19468–e19468. doi:10.2196/19468
13. Ringer TJ, Wong-Pack M, Miller P, et al. Understanding the educational and support needs of informal care-givers of people with dementia attending an outpatient geriatric assessment clinic. Aging Soc. 2020;40(1):205–228. doi:10.1017/S0144686X18000971
14. Eichel H, Heine J, Wegner F, et al. Neuropsychiatric symptoms in parkinson’s disease patients are associated with reduced health-related quality of life and increased caregiver burden. Brain Sci. 2022;12(1):89. doi:10.3390/brainsci12010089
15. Stucki BR, Mulvey J. Can Aging Baby Boomers Avoid the Nursing Home: Long-Term Care Insurance For” Aging in Place”. American Council of Life Insurers; 2000.
16. Chou KR. Caregiver burden: a concept analysis. J Pediatr Nurs. 2000;15(6):398–407. doi:10.1053/jpdn.2000.16709
17. Ovayolu Ö, Ovayolu N, Tuna D, Serçe S, Sevinç A, Pirbudak Çöçelli L. Quality of life of caregivers: a cross-sectional study. Int J Nurs Pract. 2014;20(4):424–432. doi:10.1111/ijn.12147
18. Oliveira D, Vass C, Aubeeluck A. Quality of life on the views of older family carers of people with dementia. Dementia. 2019;18(3):990–1009. doi:10.1177/1471301217700741
19. Cuthbert CA, King-Shier K, Ruether D, Tapp DM, Culos-Reed SN. What is the state of the science on physical activity interventions for family caregivers? A Systematic review and RE-AIM evaluation. J Phys Act Health. 2017;14(7):578–595. doi:10.1123/jpah.2016-0280
20. Aksoydan E, Aytar A, Blazeviciene A, et al. Is training for informal caregivers and their older persons helpful? A systematic review. Arch Gerontol Geriatr. 2019;83:66–74. doi:10.1016/j.archger.2019.02.006
21. Parker D, Mills S, Abbey J. Effectiveness of interventions that assist caregivers to support people with dementia living in the community: a systematic review. Int J Evid Based Healthc. 2008;6(2):137–172.
22. Oliveira DC, Vass C, Aubeeluck A. The development and validation of the dementia quality of life scale for older family carers (DQoL-OC). Aging Ment Health. 2018;22(5):709–716. doi:10.1080/13607863.2017.1293004
23. STROBE Statement-Checklist of items that should be included in reports of cross-sectional studies; 2021. Available from: www.strobe-statement.org.
24. Hosmer DW, Lemeshow S, Sturdivant RX. Applied Logistic Regression.
25. Bruvik FK, Ulstein ID, Ranhoff AH, Engedal K. The quality of life of people with dementia and their family carers. Dement Geriatr Cogn Disord. 2012;34(1):7–14. doi:10.1159/000341584
26. Wong DFK, Lam AYK, Chan SK, Chan SF. Quality of life of caregivers with relatives suffering from mental illness in Hong Kong: roles of caregiver characteristics, caregiving burdens, and satisfaction with psychiatric services. Health Qual Life Outcomes. 2012;10(1):15. doi:10.1186/1477-7525-10-15
27. Farina N, Page TE, Daley S, et al. Factors associated with the quality of life of family carers of people with dementia: a systematic review. Alzheimers Dement. 2017;13(5):572–581. doi:10.1016/j.jalz.2016.12.010
28. Moon H, Dilworth-Anderson P. Baby boomer caregiver and dementia caregiving: findings from the National Study of Caregiving. Age Ageing. 2015;44(2):300–306. doi:10.1093/ageing/afu119
29. Sheehan OC, Haley WE, Howard VJ, et al. and well-being in dementia and nondementia caregivers: insights from the caregiving transitions study. Gerontologist. 2021;61(5):670–679. doi:10.1093/geront/gnaa108
30. Lee K, Yefimova M, Puga F, Pickering CE. Gender differences in caregiver burden among family caregivers of persons with dementia. J Gerontol Nurs. 2021;47(7):33–42. doi:10.3928/00989134-20210610-03
31. Lee D-CA, Tirlea L, Haines TP. Non-pharmacological interventions to prevent hospital or nursing home admissions among community-dwelling older people with dementia: a systematic review and meta-analysis. Health Soc Care Community. 2020;28(5):1408–1429. doi:10.1111/hsc.12984
32. Hoffmann F, Rodrigues R. Informal carers: who takes care of them? Policy brief 4/2010; 2010. Available from: https://www.euro.centre.org/publications/detail/387.
33. Fiuza AR. Outpatient clinic for elderly carers of the elderly: the perception of patients about a specialised service [Masters thesis]. Brazil: School of Medicine, Federal University of Sao Paulo; 2017.
34. Piechota J, Xu MP. Data-driven hypothesis development; 2021. Available from: https://www.thoughtworks.com/en-es/insights/articles/data-driven-hypothesis-development.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.