Back to Journals » Journal of Multidisciplinary Healthcare » Volume 18
Understanding the Mismatch Between Utilization and Demand for Home Medical Care Among Disabled Older Adults in China
Authors Zheng J, Xing R, Wu W, Zeng Y
Received 14 July 2025
Accepted for publication 18 November 2025
Published 24 November 2025 Volume 2025:18 Pages 7679—7689
DOI https://doi.org/10.2147/JMDH.S553601
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr David C. Mohr
Jinxuan Zheng,1,2 Ruobing Xing,1 Weiqian Wu,1 Yanbing Zeng1,2
1School of Public Health, Capital Medical University, Beijing, People’s Republic of China; 2Beijing Key Laboratory of Environment and Aging, Beijing, People’s Republic of China
Correspondence: Yanbing Zeng, School of Public Health, Capital Medical University, Beijing, 100069, People’s Republic of China, Email [email protected]
Purpose: Home medical care has emerged globally as an effective approach to addressing the medical and care needs of disabled older adults due to its comfort, convenience, and cost-effectiveness. Understanding the utilization and demand for home medical care services among this population is a key area. This study aims to analyze the utilization and demand for these services among disabled older adults in China.
Patients and Methods: The data for this study were drawn from national-level data from the 2018 China Longitudinal Healthy Longevity Survey (CLHLS) and a household survey conducted in Beijing, the capital of China, in 2024. Descriptive analyses were employed to examine the utilization and demand for home medical care services among disabled older adults, while chi-squared tests and logistic regression models were used to identify factors associated with these outcomes.
Results: Based on data from 3278 disabled older adults in the CLHLS dataset, which consists of a total of 15874 records, the utilization rate of home medical care services was highest in the Eastern region, while the demand rate exceeded 85% in each regions. Data from the household survey of 958 patients in Beijing indicated that the top three service categories with the largest gaps between utilization and demand were medication treatment, traditional Chinese medicine treatment, and rehabilitation nursing, which the mismatch gap reached 17.7%, 17.6%, and 15.5%, respectively. Region and residential area significantly influenced the utilization for these services, while residential area and age impacted demand.
Conclusion: Currently, home medical care services in China are characterized by a limited range of offerings and a mismatch between utilization and demand. It is recommended that the home medical care service system be further optimized to ensure a more balanced distribution of medical and healthcare resources.
Keywords: disabled older adults, home medical care, cross-sectional study
Introduction
The number and proportion of older adults worldwide are rising. By 2030, one in six people globally will be 60 years or older. Between 2020 and 2030, the population aged 60 and above is projected to grow from 1 billion to 1.4 billion. Additionally, the number of people aged 80 and above is anticipated to double, reaching 426 million by 2050.1 Population aging has become a global challenge. Due to the continuous decline of various physiological functions, the proportion of older adults with mental or physical disabilities who are unable to carry out daily activities is also increasing.2 The World Health Organization predicts that by 2050, the number of disabled older adults will reach 66 million. In China, estimates indicate that by 2030, the number of disabled older adults will exceed 60 million, and by 2050, it will reach 96 million.3
Disability primarily refers to impaired self-care caused by aging, illness, or physical and mental disabilities.4,5 With the accelerating trend of population aging, the social challenges arising from the increasing number of disabled older adults are becoming more pronounced, leading to a growing global focus on medical care for it. Research has found that most disabled older adults, influenced by traditional beliefs and declining physical condition, prefer to spend their later years at home.6,7 The “United Nations Principles for Older Adults” also emphasize that older adults should remain in their homes for as long as possible.8 Despite economic and cultural differences, aging in place is a common preference among most older adults worldwide.9–12 Currently, countries such as the United States,13 Germany,14 the United Kingdom,15 and Japan16 have developed well-established care models for disabled older adults, focusing on home medical care services. This models align with the psychological need of older adults to receive care at home,17,18 address the challenges they face in accessing timely medical care due to mobility issues19 and they facilitate the integration of medical resources and help reduce healthcare costs.20 In addition, with the widespread use of artificial intelligence and digital health tools in home medical care,21–23 the promotion and implementation of home medical care services will encounter greater possibilities and opportunities. China has gradually introduced policies for home medical care services in recent years. Specifically, this involves healthcare professionals providing diagnostic and treatment services, medical care, rehabilitation treatment, pharmaceutical services, palliative care, and traditional Chinese medicine at home. These services primarily target high-risk or disabled older adults, individuals with chronic diseases, patients in recovery or terminal stages, and older adults who continue to require medical care after hospital discharge.24
However, in China, home medical care services for disabled older adults are still in the exploratory stage. The overall policy framework and implementation remain inadequate, lacking both systematization and coherence, resulting in uneven service coverage and quality. Additionally, there is an insufficient understanding of the specific demand for these services among disabled older adults, leading to a lack of targeted service provision. As a result, the utilization rate of these services for this population remains relatively low.25–28 Given the rapid increase in the population of disabled older adults amid China’s aging demographic, it is crucial to gain a comprehensive understanding of the utilization and demand for home medical care services. This study clarifies the utilization, demand, and determinants of these services among disabled older adults in China based on data from the CLHLS. Furthermore, it analyzes the specific gap between demand and utilization in a typical province in China through a household survey. This research aims to provide empirical evidence for further developing a home medical care service system and promoting healthy aging in China.
Materials and Methods
Data Collection
The data for this study were sourced from a national survey in China and a household survey conducted in Beijing, the capital of China, focusing on disabled older adults. The national-level data were obtained from the 2018 CLHLS. This cross-sectional dataset was randomly drawn from 22 out of 31 provinces in China, representing approximately 85% of the country’s population. All information was collected through face-to-face interviews with families using internationally standardized questionnaires.29 The 2018 survey included 15,874 adults aged 65 and older, covering various aspects such as economic status, health conditions, activities of daily living (ADL), and medical service utilization. This study examined the utilization and demand for home medical care services among disabled older adults. Based on the research design, individuals who were not disabled, did not respond to disability-related questions or provided unclear answers regarding these services were excluded. Ultimately, a total of 3278 valid observations were included.
In 2024, a face-to-face household survey was conducted in Beijing. According to previous China surveys, it was estimated that about 29%30 of the elderly with basic impairment of daily living activities receive home medical care services, which was used to estimate the minimum sample size of the survey.
In the formula, let  correspond to the chosen confidence level, let p be the anticipated proportion of elderly home medical care service utilization, set at 0.29. Let E denote the allowable margin of error. In this study, the significance level is α= 0.05, for which
correspond to the chosen confidence level, let p be the anticipated proportion of elderly home medical care service utilization, set at 0.29. Let E denote the allowable margin of error. In this study, the significance level is α= 0.05, for which  = 1.96, and the margin of error is E = 0.03. To ensure the validity of the sample, the sample size was expanded to include 1000 respondents.
= 1.96, and the margin of error is E = 0.03. To ensure the validity of the sample, the sample size was expanded to include 1000 respondents.
Beijing’s urban functional zones are broadly categorized into four types: the Capital Core Area, Urban Expansion Zone, New Development District, and Ecological Conservation Zone. One administrative district from each category was selected as a sampling district. Based on the elderly population and the number of disabled adults in each district, we identified Dongcheng District, Chaoyang District, Daxing District, and Pinggu District as our study sites. The analysis of disabled adults across the five urban functional zones yielded proportions of 12.4%, 43.5%, 28.3%, and 15.8%, respectively. Table 1 presents the adjusted sample sizes for each zone based on the number of disabled adults in the study areas. The research questionnaire was developed by the project team, with an initial draft followed by two rounds of expert consultations to finalize the version. The survey primarily collected data on the demographic characteristics of disabled older adults, their ADL status, and their utilization and demand for various home medical care services, including diagnostic and treatment services, medical nursing, rehabilitation treatment, pharmaceutical services, and hospice services, among which the assessment criteria for the ADL status were consistent with those of CLHLS. Quality control procedures included the development of a standardized investigator training manual and uniform training for all investigators. To ensure data quality, a 5% random sampling check was conducted. Data entry was performed in Epidata with a two-person verification system to ensure accuracy. Auditors conducted real-time data monitoring and auditing, and random re-visit checks were performed to verify data consistency and reliability. In total, 1000 individuals were surveyed, yielding 958 valid responses.
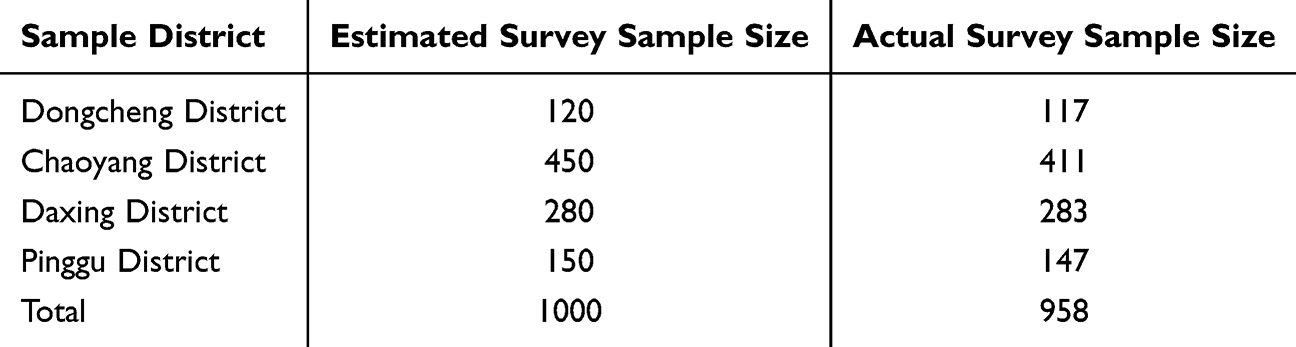 |
Table 1 The Sample Area and Sample Size of the Household Survey in Beijing |
Variables
In this study, several independent variables were incorporated based on relevant literature and the questionnaire design of the CLHLS. These variables included region (Eastern, Central, Western), gender (male, female), residential area (city, town, and rural), age ([65–74], [75–84], [85–94], [95–104], and ≥105 years), disability degree (mild, moderate, and severe), marital status (currently married, separated, divorced, widowed, and never married), social security and insurance coverage (no, yes), and co-residence status (living with household member(s), alone). The dependent variables for this study were whether home medical care services were utilized and whether there was a demand for such services. The region variable was categorized according to China’s economic development status into the Eastern, Central, and Western regions. The degree of disability was determined based on six questions about ADL activities from the CLHLS. If participants could not perform any of the six ADL tasks without assistance, they were classified as disabled. The severity of disability was further categorized as follows: participants unable to complete five or more of the six ADL tasks independently were classified as severely disabled; those unable to perform three to four ADL tasks were categorized as moderately disabled; and those who required assistance with one or two ADL tasks were considered mildly disabled.31
Statistical Analysis
Descriptive statistics were used to analyze the utilization and demand for home medical care services among disabled older adults. A Chi-square test and binary logistic regression analysis were performed to examine further the factors influencing the utilization and demand for these services. All variables in the analysis were adjusted for confounding effects using the variance inflation factor (VIF <5) to eliminate multicollinearity. A two-sided p-value of <0.05 was considered to indicate statistical significance. All analytical processes were conducted using SPS S25.0.
Results
Utilization and Demand for Home Medical Care Services Among Disabled Older Adults in China
Table 2 presents data on 3278 disabled older adults from the 2018 CLHLS cross-sectional dataset. The utilization rate of home medical care services was highest among disabled older adults in the Eastern region, reaching 49.4%, while demand rates exceeded 80% in each regions. Utilization rates for these services were above 40% for both males and females, with demand rates exceeding 85%. Those residing in rural areas exhibited higher utilization and demand rates (47.1% and 88.5%, respectively) than those in city and town areas.
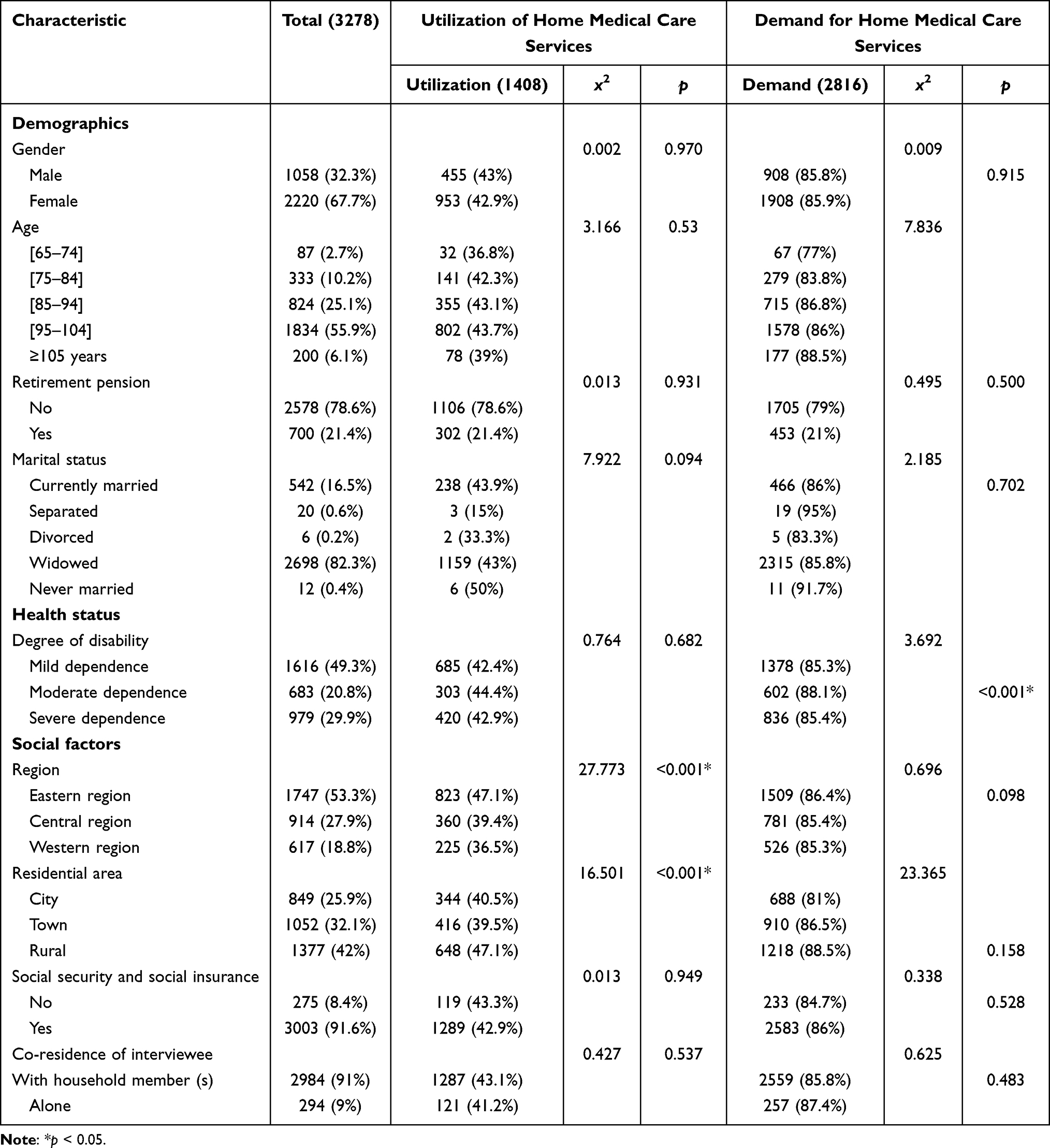 |
Table 2 Basic Characteristics of Disabled Older Adults and Chi-Square Test for the Utilization and Demand of Home Medical Care Services (N, %) |
Table 2 also presents the results of Chi-square tests, indicating statistically significant differences (P < 0.05) in the utilization for home medical care services across different regions and residential areas, and statistically significant differences (P < 0.05) in demand for these services across different residential areas.
The Gap Between Utilization and Demand for Home Medical Care Services in Beijing, China
To further clarify the utilization, demand, and existing challenges associated with home medical care services in China, we selected Beijing as the research site. We conducted a household survey in 2024. Table 3 illustrates the gap between utilization and demand for home medical care services among 958 surveyed disabled older adults in Beijing. The results indicate that the demand rate for these services was significantly higher than the utilization rate. The top three service items with the largest gaps between demand and utilization were medication treatment (17.7%), traditional Chinese medicine treatment (17.6%), and rehabilitation nursing (15.5%). From a service type perspective, both diagnosis and treatment, medical nursing services exhibited relatively high utilization and demand rates. For example, 19% of respondents utilized home health assessment services, while 33.6% expressed a demand for them. Similarly, 11.6% used home basic nursing services, while 25.4% indicated a need for them. Regarding home rehabilitation treatment services, the most commonly utilized service was home rehabilitation assessment, with only 0.9% of respondents using it. And the least utilized service was traditional Chinese medicine rehabilitation, with only four individuals (0.4%) accessing it. However, 15.2% expressed a demand for home rehabilitation assessment services and 14.7% sought traditional Chinese medicine rehabilitation services.
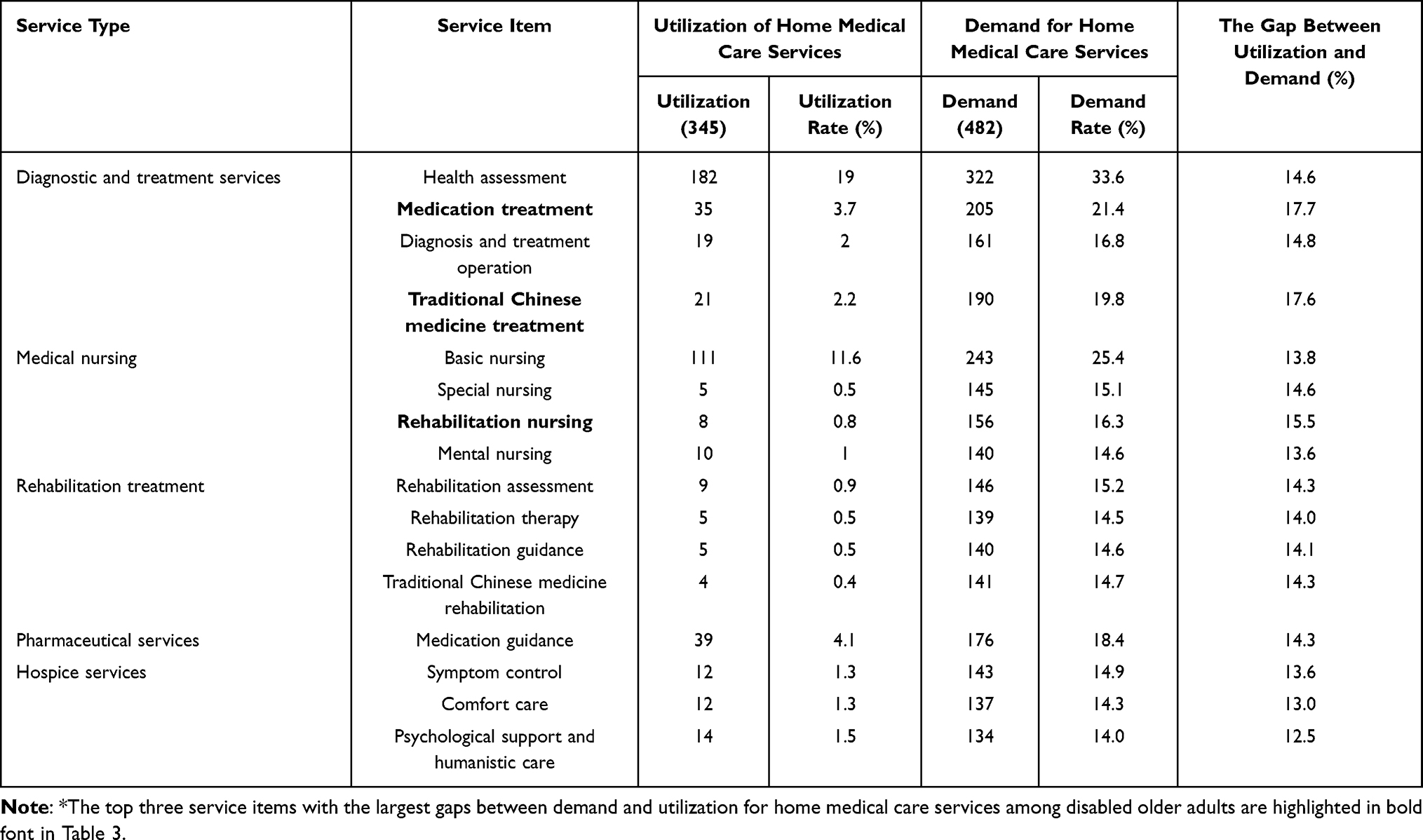 |
Table 3 Utilization and Demand for Home Medical Care Services Among Disabled Older Adults Surveyed in Beijing, China* |
Among the 958 disabled older adults surveyed, a total of 946 instances of home medical services were recorded. Figure 1 presents a word cloud based on the number of specific these services provided. The most frequently utilized services included general physical examinations (180 times), routine assessments (133 times), blood glucose measurements (67 times), comfort care (39 times), cardiovascular risk assessments (35 times), and vital signs measurements (35 times).
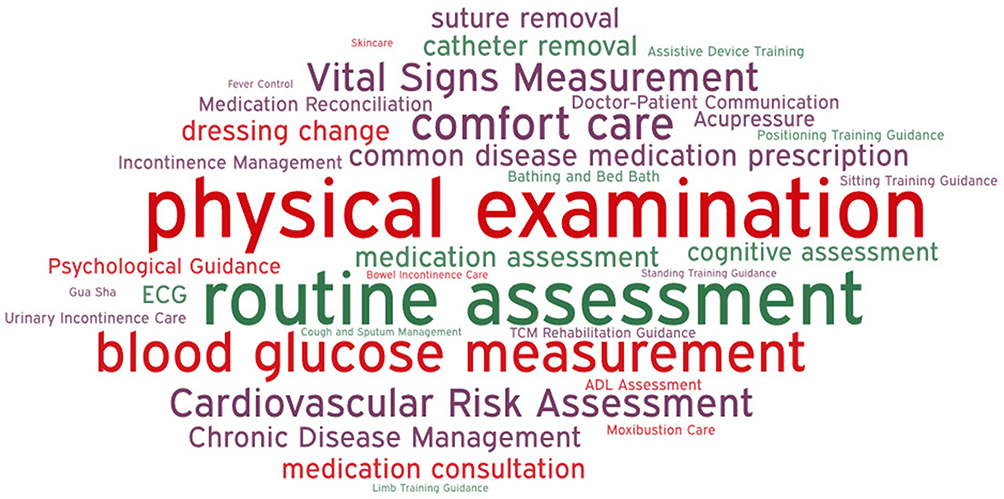 |
Figure 1 Word cloud of specific home medical care services received by disabled older adults in Beijing, China. |
Analysis of Factors Influencing the Utilization and Demand for Home Medical Care Services Among Disabled Older Adults in China
Table 4 analyses factors influencing the utilization and demand for home medical care services among disabled older adults across different regions and residential areas in China (p < 0.05). Region and residential area significantly influenced the utilization for these services, while residential area and age impacted demand. Specifically, compared to the Eastern region, disabled older adults in the Central (odd ratio [OR] = 0.712, 95% confidence interval [CI]: 0.603–0.839), Western (OR = 0.653, 95% CI: 0.539–0.791) were less likely to utilize these services, with approximately 28.8%, 35.7% lower odds, respectively. Disabled older adults residing in rural areas (OR = 1.477, 95% CI: 1.196–1.824) were likelier to utilize these services than those in city areas, with 1.477 times higher odds. Additionally, disabled older adults in towns (OR = 1.444, 95% CI: 1.085–1.923) and rural areas (OR = 1.608, 95% CI: 1.308–2.326) demonstrated a greater demand for home medical care services than their city counterparts, with 1.444 and 1.608 times higher odds, respectively. Regarding the influence of age, disabled older adults aged 85–94 years (OR = 2.590, 95% CI: 1.435–4.677), 95–104 years (OR = 2.538, 95% CI: 1.400–4.600), and ≥105 years (OR = 3.079, 95% CI: 1.486–6.379) exhibited a higher demand for these services compared to those aged 65–74 years, with 2.590, 2.538, and 3.079 times higher odds, respectively.
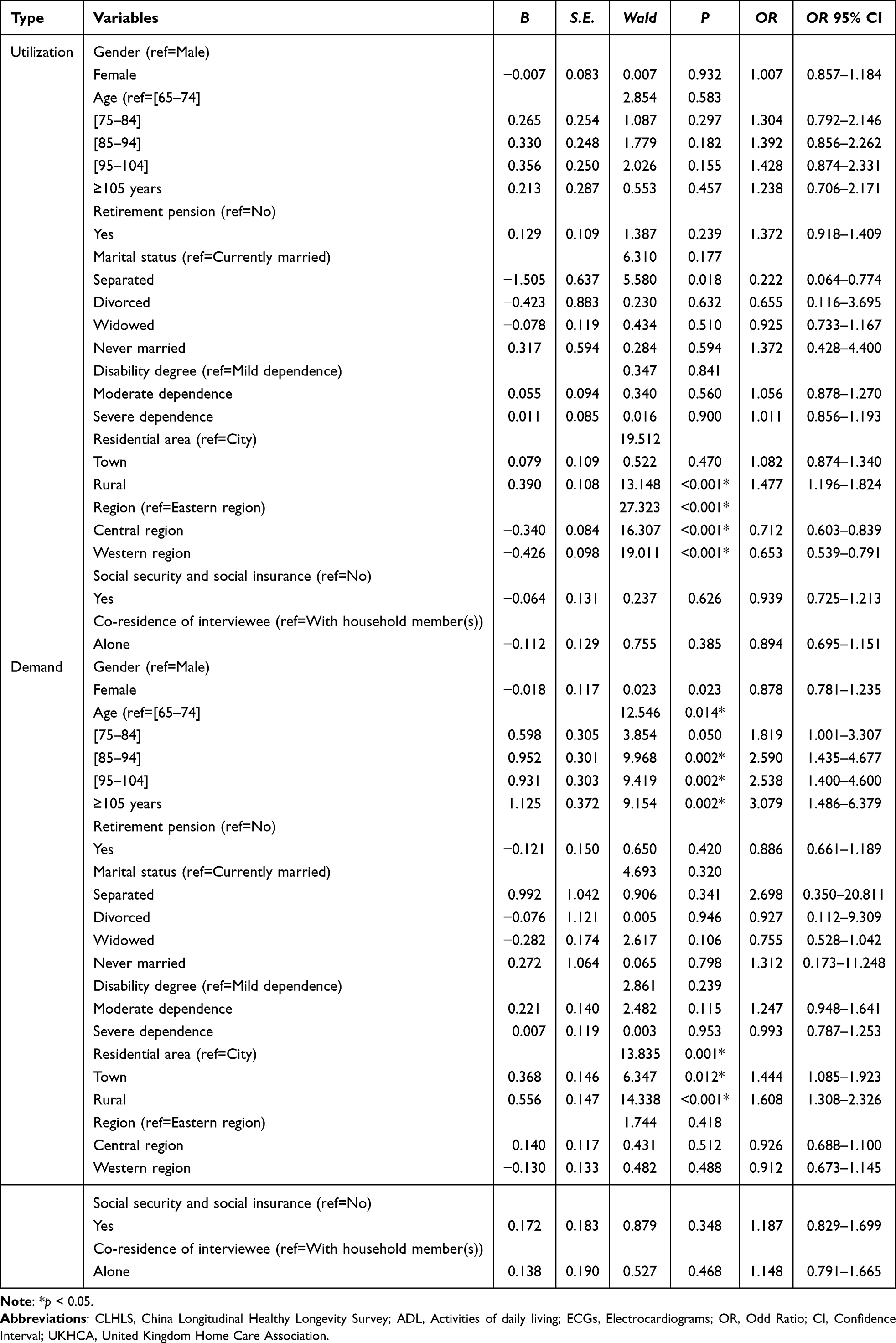 |
Table 4 Logistic Regression Analysis of Factors Influencing the Utilization and Demand for Home Medical Care Services |
Discussion
The results regarding the utilization and demand for home medical care services among disabled older adults indicated that the current supply of such services in China is insufficient and poorly aligned with demand. The gap between utilization and demand across five home medical care services categories was approximately 15%. The highest utilization rate was below 20%, while the lowest was below 1%. These findings suggested that the existing home medical care services do not adequately meet the demand of disabled older adults. Therefore, China must expand the home medical care services supply to this population. However, at present China has not established a systematic and feasible national policy plan for home medical care services for disabled adults. The current approach appears to rely predominantly on family doctors in primary hospitals to deliver home medical care services, which our findings suggest is insufficient to meet the needs of disabled seniors. Regarding management practices, China could draw on the extensive experience of countries that earlier implemented these services. Establishing relevant organizations could help standardize and unify the training and allocation of service personnel, the provision and operation of service programs, and monitor and regulate service quality. For example, the United States32 had established the Centers for Medicare & Medicaid Services to manage the supply of home care services and ensure quality control. Similarly, in the UK,33 the United Kingdom Home Care Association (UKHCA) published manuals for home medical care personnel, guidelines for selecting home care packages, training resources for caregivers, and codes of conduct for service providers to ensure the quality and availability of these services. From a supply strategy perspective, adopting a demand-driven approach was essential to optimize the allocation of home medical care resources based on service content and demand volume.34 In the United Kingdom,35 UKHCA-assisted older adults in finding suitable service organizations and agencies. Expanding the range of providers offering home medical care services was crucial. Commercial institutions in China also provided home medical care services for disabled adults, but issues such as inconsistent service standards and high prices persist. By introducing non-governmental and non-profit organizations, China could increase the availability of home medical care services, improve service quality, and foster innovation in service delivery.36
Findings from Beijing indicated that home medical care services in China primarily fall into two main categories: diagnostic and treatment services and medical nursing services. Specifically, home diagnosis and treatment services mainly include general physical examinations, routine assessments, blood glucose measurements, and similar services. Home medical nursing services primarily focus on comfort care, vital signs measurements, catheter removal, and related procedures. However, home rehabilitation treatment, pharmaceutical, and hospice services are available. These findings suggested that home medical care services in China are characterized by their simplicity, limited scope, ease of implementation, and emphasis on safety. This aligned with conclusions drawn by scholars such as Wang25 and Yi37 regarding these services. The limited range of available services might be related to various challenges in providing home medical care, including complex home environments, potential medical emergencies, and medical waste disposal issues.38,39 This reflected the current deficiencies in China’s home medical care service policies, it was recommended that the home medical care service system be further optimized, the capabilities of medical institutions in delivering these services improved, and the range of available home medical care options be expanded. Integrating modern scientific technology into these services would be particularly beneficial. Devices such as portable ultrasound machines, ECGs, X-ray machines, pulse oximeters, and blood biochemical measurement devices39 could significantly improve these services’ safety, reliability, and operability.
The research findings indicated that region and residential area significantly influenced the utilization for home medical care services among disabled older adults in China, age and residential area impacted the demand for these services within this population. While gender, retirement pension, disability degree, marital status, social security, social insurance and co-residence of interviewee were not significant factors affecting these services. On the one hand, disabled older adults in the economically advantaged Eastern region had greater access to these services compared to those in other regions. Some studies40,41 suggested that economically developed regions possess stronger financial capabilities and more efficient policy implementation, leading to a broader range of healthcare resources, better promotion and execution of home care policies. In summary, the above factors all reflected socioeconomic conditions. It was evident that different socioeconomic conditions in China have a significant impact on how disabled adults utilize home medical care services.42 Consequently, policy formulation should account for inequities arising from socioeconomic disparities across regions. For example, policies could be designed to preferentially support disabled adults in regions with poorer socioeconomic conditions during implementation. On the other hand, disabled older adults residing in rural areas demonstrated higher utilization and demand for home medical care services compared to those living in city areas. Research had shown that two-thirds of disabled older adults in China live in rural areas, where healthcare resources are relatively scattered and family caregiving functions are weakened.43 And due to urban-rural health inequality, residents in rural areas were generally at a disadvantage compared to urban residents in terms of health and access to health services.44,45 These situations led to a greater reliance on these services among rural disabled older adults than among their city counterparts. Therefore, policymakers should prioritize this vulnerable group when designing relevant policies. Moreover, older disabled adults exhibited a higher demand for these services compared to those in younger age brackets (65–74 years). Several scholars argued that advanced age restricts daily living activities, and as individuals age, their ability to perform self-care diminishes, increasing the need for medical assistance.20,46,47 Home medical care services provided timely and convenient medical support for older disabled individuals with mobility challenges, making age a significant factor influencing the demand for these services.
In conclusion, China must identify the specific demands for home medical care services across different regions, balance the distribution of healthcare resources, and provide services based on demand. This approach could help narrow the service supply–demand gap across regions, residential areas, and age groups, ultimately ensuring more equitable access to these services. International practices in-home medical care have demonstrated that leveraging the Internet for information dissemination, communication, and oversight is one of the most effective methods for improving access to adequate home medical care services.36 By digitizing the health, medical, and caregiving records of disabled older adults, internet-based systems could facilitate referrals between care institutions and support remote care arrangements. Additionally, disabled older adults and their caregivers could conveniently access and book services from home, increasing awareness and utilization of home medical care services.
Limitations
Several limitations of this study should be acknowledged. First, all the studies referenced in this paper were based on cross-sectional survey data, which cannot fully and accurately capture the utilization and demand for home medical care services among disabled older adults in China. To gain deeper insights, long-term follow-up studies, and observational data should be incorporated into future research to analyze the development of these services over time. Second, due to the data limitations of CLHLS, some possible confounding factors (such as education) were not included in the analysis due to excessive missing values. In future studies, more possible confounding factors can be considered to improve the accuracy of the study. Third, due to constraints related to time, funding, and manpower, this study selected only one province, Beijing as the survey site, excluding other region of China. As a result, some findings may be subject to regional bias, which should be addressed in future studies with a broader geographic scope. Fourth, this study primarily investigated home medical care services for disabled older adults from the perspective of supply and demand. However, during the survey conducted in the Eastern Chinese province, a significant number of disabled older adults and their caregivers were found to overlook the need for these services due to financial constraints or a lack of awareness about healthcare options. Therefore, an important challenge for future research is comprehensively assessing this population’s potential need. Addressing this issue will be crucial for advancing the development of these services in China.
Conclusion
In summary, there was a mismatch between the supply and demand for home medical care services in China, with a limited variety of available services. Region and residential area significantly influenced the utilization for home medical care services among disabled older adults in China, age and residential area impacted the demand for these services within this population. These findings suggest that China should consider these factors when formulating policies on home medical care services for disabled older adults. Establishing specialized institutions for home medical care and enhancing their service capabilities will be critical steps. Expanding the range of service providers and increasing overall supply capacity will also be necessary. Furthermore, leveraging internet-based information platforms to optimize the distribution of healthcare resources will be vital. Implementing a demand assessment mechanism for home medical care services and improving the accuracy of care delivery systems will enhance the quality and efficiency of this services for disabled older adults in China.
Data Sharing Statement
The original data can be queried on the China Longitudinal Healthy Longevity Survey (CLHLS) – Tracking Data (https://doi.org/10.18170/DVN/WBO7LK).
Ethics Approval and Consent to Participate
Not applicable. This study utilized data from the 2018 China Longitudinal Healthy Longevity Survey (CLHLS) and involved a household survey conducted in 2024. All procedures followed were in accordance with the ethical standards of the institutional research committee. Informed consent was obtained from all participants in the household survey, and all data were anonymized to protect participant confidentiality. Additionally, we have obtained the ethics exemption from Capital Medical University.
Funding
This work was supported by the National Natural Science Foundations of China (No. 72474143) and the Humanities and Social Sciences Programme, Ministry of Education (No. 23YJAZH010). The funders had no role in the study design, data collection and analysis, decision to publish or preparation of the manuscript.
Disclosure
The authors report no conflicts of interest in this work.
References
1. World Health Organization. Aging and health. 2024. Available from: https://www.who.int/zh/news-room/fact-sheets/detail/ageing-and-health.
2. Xin Y, Ren X. Predicting depression among rural and urban disabled elderly in China using a random forest classifier. BMC Psychiatry. 2022;22(1):118. doi:10.1186/s12888-022-03742-4
3. Li X. Research on the current situation, problems and countermeasures of social support for disabled elderly based on literature analysis. Econ Res Guide. 2021;9:147–149.
4. O’Young B, Gosney J, Ahn C. The concept and epidemiology of dis-ability. Phys Med Rehabil Clin N Am. 2019;30(4):697–707. doi:10.1016/j.pmr.2019.07.012
5. Yan W. Research on status quo and influencing factors of elderly dis-ability in China based on CLHLS. Chin Nurs Res. 2021;35(10):1807–1811.
6. Hao X, Gu J, Ying X, Bo T, Fu W. Social support and care needs of the disabled elderly population: an empirical study based on survey data from Beijing. China Biosci Trends. 2017;11(5):507–515. doi:10.5582/bst.2017.01234
7. Zamanzadeh V, Rahmani A, Pakpour V, Chenoweth LL, Mohammadi E. Psychosocial changes following transition to an aged care home: qualitative findings from Iran. Int J Older People Nurs. 2017;12(2). doi:10.1111/opn.12130
8. United Nations. United Nations principles for older persons. 1991. Available from: http://www.ohchr.org/zh/instruments-mechanisms/instruments/united-nations-principles-older-persons.
9. de Jong L, Plöthner M, Stahmeyer JT, Eberhard S, Zeidler J, Damm K. Informal and formal care preferences and expected willingness of providing elderly care in Germany: protocol for a mixed-methods study. BMJ Open. 2019;9(1):e023253. doi:10.1136/bmjopen-2018-023253
10. Plöthner M, Schmidt K, de Jong L, Zeidler J, Damm K. Needs and preferences of informal caregivers regarding outpatient care for the elderly: a systematic literature review. BMC Geriatr. 2019;19(1):82. doi:10.1186/s12877-019-1068-4
11. Glinskaya E, Feng Z. Options for Aged Care in China: Building an Efficient and Sustainable Aged Care System. Washington: The World Bank Group; 2018.
12. McCaffrey N, Gill L, Kaambwa B, et al. Important features of home-based support services for older Australians and their informal carers. Health Soc Care Community. 2015;23(6):654–664. doi:10.1111/hsc.12185
13. Szanton SL, Thorpe RJ, Boyd C, et al. Community aging in place, advancing better livingfor elders: a bio-behavioral-environmental intervention to improve function and health-related quality of life in disabled older adults. J Am Geriatr Soc. 2011;59(12):2314–2320. doi:10.1111/j.1532-5415.2011.03698.x
14. Lehnert T, Günther OH, Hajek A, et al. Preferences for home- and community-based long-term care services in Germany: a discrete choice experiment. Eur J Health Econ. 2018;19(9):1213–1223. doi:10.1007/s10198-018-0968-0
15. Making sense of integrated care systems, integrated care partnerships and accountable care organisations in the NHS in England. The King’s Fund; 2022. Available from: https://www.kingsfund.org.uk/publications/making-sense-integrated-care-systems#acos.
16. Sima L, Itaka Y. Exploration to and inspiration of the development of community-based elderly care service and facility in Japan. Housing Sci. 2024;44(02):38–44. doi:10.13626/j.cnki.hs.2024.02.006
17. Van Houtven CH, Konetzka RT, Taggert E, et al. Informal and formal home care for older adults with disabilities increased, 2004–16. Health Aff. 2020;39(8):1297–1301. doi:10.1377/hlthaff.2019.01800
18. Lin L, Cheng M, Guo Y, et al. Early discharge hospital at home as alternative to routine hospital care for older people: a systematic review and meta-analysis. BMC Med. 2024;22(1). doi:10.1186/s12916-024-03463-3
19. Wang JP, Tang Z, Sun F, et al. Analysis of factors related to the difficulty of medical access for the elderly in Beijing. China Hosp. 2012;16(12):26–28.
20. Zhang X, Liu J, Guo K, et al. Application of community nursing information management platform in home service for disabled elderly people. Chin Nurs Manage. 2022;22(03):396–399.
21. Singh H, Armas A, Law S, et al. How digital health solutions align with the roles and functions that support hospital to home transitions for older adults: a rapid review study protocol. BMJ Open. 2021;11(2):e045596. doi:10.1136/bmjopen-2020-045596
22. Dermody G, Fritz R, Glass C, Dunham M, Whitehead L. Family caregiver readiness to adopt smart home technology to monitor care-Dependent older adults: a qualitative exploratory study. J Adv Nurs. 2024;80(2):628–643. doi:10.1111/jan.15826
23. Street J, Barrie H, Eliott J, et al. Older adults’ perspectives of smart technologies to support aging at home: insights from five world Café forums. Int J Environ Res Public Health. 2022;19(13):7817. doi:10.3390/ijerph19137817
24. Bureau of Medical Administration and Development, National Health Commission of the People’s Republic of China. Notice on strengthening the work of home medical services for the elderly. 2020. Available from: http://www.nhc.gov.cn/yzygj/s7653pd/202012/19a2617ba8e641bea9ac2472ea04c82a.shtml.
25. Wang S, Xiao P, Wu X, et al. Study on the current situation of the use and demand of on-site medical care for the home-based elderly with chronic diseases in Chaoyang district, Beijing city. Chin Nurs res. 2020;34(06):1070–1073.
26. Wang X, Pang YJ, Zhou LZ. Shanghai elderly home care service willingness to pay. Chin J Gerontol. 2017;37(11):2814–2816.
27. Ji JL, Zhi MJ, Hu LL. The willingness to pay for care services and influencing factors among the in-home elderly. Pract Geriatr. 2021;35(01):99–102.
28. Liu Z, Bo T, Hao XN, et al. Study on Beijing nursing home medical care service based on gap analysis. Health Econ Res. 2020;37(02):13–15. doi:10.14055/j.cnki.33-1056/f.2020.02.004
29. Zeng Y, Feng Q, Hesketh T, Christensen K, Vaupel JW. Survival, disabilities in activities of daily living, and physical and cognitive functioning among the oldest-old in China: a cohort study. Lancet. 2017;389:1619–1629. doi:10.1016/S0140-6736(17)30548-2
30. Hu B, Li B, Wang J, Shi C. Home and community care for older people in urban China: receipt of services and sources of payment. Health Soc Care Community. 2020;28(1):225–235. doi:10.1111/hsc.12856
31. Zhang W, Wei M. Disability level of the Chinese elderly: comparison from multiple data sources. Popul Res. 2015;39(3):34–47.
32. Eldercare Locator. Welcome to the Eldercare Locator. 2019. Available from: https://eldercare.acl.gov/Public/Index.aspx.
33. United Kingdom Homecare Association. List of Publications. 2019. Available from: https://portal.ukhca.co.uk/Publications/PublicationsListing.aspx.
34. Qiu WQ, Yan XL, Hu GY, et al. Research progress of evaluation of health planning and health resource allocation. Chin Health Resour. 2017;20(2):118–122.
35. Young J. The development of intermediate care services in England. Arch Gerontol Geriatr. 2009;49(2):21–25. doi:10.1016/S0167-4943(09)70008-1
36. Luo Q, Wang AQ, Chen H, et al. General situation of development and enlightenment of elderly home-based care services in the United States, the United Kingdom, Japan and Australia. Soft Sci Health. 2020;34(06):91–96.
37. Yi YJ, Yuan SS, Huan J, et al. A study on home medical service in Fengtai District of Beijing based on observation method. Chin Prim Health Care. 2022;36(03):35–38.
38. Zhao CY, Liu YJ, Shao S, et al. Evaluation of home health services by general practitioners in Beijing: a qualitative study. Chin Gen Pract. 2018;21(28):3453–3458.
39. Chen T, Yao NL, Su MZ, et al. Challenges of home-based medical care in China: a telephone interview from the perspectives of home care providers. Chin Gen Pract. 2020;23(12):1459–1465.
40. Chen Y. Research on the status and development of home care needs of the elderly in China. Digitization User. 2023;29(6):162–164.
41. Zheng YH, Hao XN, Liu Z, et al. An analysis of the current status of Beijing home health care services. Health Econ Res. 2020;37(02):10–13. doi:10.14055/j.cnki.33-1056/f.2020.02.003
42. Almeida APSC, Nunes BP, Duro SMS, et al. Socioeconomic determinants of access to health services among older adults: a systematic review. Rev Saude Publica. 2017;51:50. doi:10.1590/S1518-8787.2017051006661
43. Zhao QC. Research on the construction of the rural elderly care service system in China. Tsinghua University Press; 2016.
44. Guo B, Xie X, Wu Q, et al. Inequality in the health services utilization in rural and urban China: a horizontal inequality analysis. Medicine. 2020;99(2). doi:10.1097/MD.0000000000018625
45. Xiong YG, Huang J. Inequality in health service between Urban and Rural Areas in China: evidence from CHARLS 2013 data. Popul J. 2016;38(06):62–76. doi:10.16405/j.cnki.1004-129X.2016.06.007
46. Chen R, Hu Q. A study on the role and support system of family care under social elderly care trend. Urban Insight Urban Observations. 2015;2015(03):126–131.
47. Peng HY. Application of community nursing information management platform in home service for disabled elderly people. Contemp Nurse. 2023;4(6). doi:10.12208/j.cn.20230304
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.