Back to Journals » International Journal of Women's Health » Volume 17
Understanding Preferences, Needs, and Expectations for Pharmaceutical Treatment of Symptomatic Uterine Fibroids Based on Surveys of Healthcare Providers and Patients
Authors Madueke-Laveaux OS, Hunsche EG ![]() , Rakov VG
, Rakov VG ![]() , Lickert C, Hauber B, Sukumar R, Agarwal SK
, Lickert C, Hauber B, Sukumar R, Agarwal SK ![]()
Received 20 February 2025
Accepted for publication 10 September 2025
Published 9 October 2025 Volume 2025:17 Pages 3527—3540
DOI https://doi.org/10.2147/IJWH.S523846
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Matteo Frigerio
O Sandra Madueke-Laveaux,1 Elke GI Hunsche,2 Viatcheslav G Rakov,2 Cassandra Lickert,3 Brett Hauber,4 Ramamirtham Sukumar,5 Sanjay K Agarwal6
1Department of Obstetrics and Gynecology, University of Chicago, Chicago, IL, USA; 2Sumitomo Pharma Switzerland GmbH, Basel, Switzerland; 3Sumitomo Pharma America, Marlborough, MA, USA; 4Pfizer Inc., New York, NY, USA; 5Optimal Strategix Group, Bensalem, PA, USA; 6Department of Obstetrics, Gynecology and Reproductive Sciences, University of California, San Diego, CA, USA
Correspondence: Elke GI Hunsche, Sumitomo Pharma Switzerland GmbH, Basel, Switzerland, Tel +41 43 210 8129, Email [email protected]
Background: Limited evidence is available regarding preferences of women with uterine fibroids (UF) and treating healthcare providers (HCPs) regarding treatment attributes; this evidence could contribute to patient-centered shared decision-making. The aim of this study was to understand HCP and patient preferences when evaluating pharmaceutical treatments for symptomatic UF, and to identify HCP and patient segments that differ in their preferences.
Methods: HCPs involved in UF management and patients diagnosed with UF completed a survey assessing the importance of treatment attributes in the UF therapy choice; an adaptive self-explication method was applied to estimate relative importance (RI), indexed to an average of 100. Attributes with RI > 100 or < 100 indicated a larger or lesser influence, respectively, in driving treatment choice. A clustering (K-means) algorithm was used to determine HCP and patient segments. Attribute RI was estimated for the overall sample and segments. Segment-specific RI estimates that were > 10 points higher or lower than the overall study population mean were considered key differentiating drivers for that segment.
Results: In total, 375 HCPs and 300 patients responded to the survey. Four HCP and four patient segments were identified. Healthcare provider segments identified were: “efficacy-focused” (n=99), “safety-focused” (n=97), “convenience-focused” (n=93), and “economics-focused” (n=86). Patient segments identified were: “symptom-relief-driven” (n=127), “information-driven” (n=67), “cost-sensitive and surgery-averse” (n=58), and “risk-averse” (n=48).
Conclusion: HCPs and patients consider a variety of factors when assessing uterine fibroid treatments. For HCPs, segmentation may elucidate motivations behind treatment choices, while segmentation of patients into distinct groups, each with specific needs, goals, and behaviors, allows for more tailored care. Understanding treatment decision drivers can support patient-centered shared decision-making by enabling HCPs to recognize patient segments and engage with patients accordingly. Shared decision-making may help optimize UF management by focusing discussions on patients’ priorities, increasing patient engagement, and improving health equity.
Keywords: uterine fibroids, shared decision making, patient choice, patient reported outcomes
Introduction
Uterine fibroids (UF) are solid neoplasms of the uterus estimated to occur in up to 70% of women before menopause.1–3 Approximately 20–50% of women with UF experience symptoms,4 including heavy menstrual bleeding (HMB; with/without anemia), pelvic pressure, pelvic pain, urinary symptoms, and obstructive symptoms.2–5 Symptoms can cause significant distress, decreased quality of life,6 absenteeism, and decreased work productivity.7
The American College of Obstetricians and Gynecologists (ACOG) recommendations for pharmacological UF interventions include progestins, oral contraceptives, gonadotropin-releasing hormone (GnRH) agonists and antagonists, tranexamic acid, and nonsteroidal anti-inflammatory drugs.2,3 The most common surgical intervention for UF is hysterectomy;8,9 approximately 30% of women undergo hysterectomy in the first year post-diagnosis.8 Interventions such as myomectomy and minimally invasive procedures may preserve fertility.4
ACOG guidelines for symptomatic UF highlight the importance of shared decision-making (SDM) between healthcare providers (HCPs) and patients.3 A patient-centered approach to SDM is advised, whereby HCPs and patients discuss the risks and benefits of treatments in the context of symptoms, lifestyle, and reproductive goals of the patient,3,10 allowing patients to make informed decisions regarding the most suitable treatment to meet their specific needs.3 Currently, there is limited evidence regarding HCP and patient treatment preferences for symptomatic UF. Understanding these preferences could aid HCP–patient dialogue and strengthen SDM for UF management by enabling HCPs to focus discussions on patients’ priorities, which may improve patient engagement. The segmentation of patient populations into distinct groups, each with specific needs, goals, and behaviors, allows for tailored care.11 Similarly, identifying HCP segments and preferences may clarify motivations behind UF treatment recommendations. Understanding the preferences of both patients and HCPs may facilitate SDM during consultations, potentially enhancing satisfaction for all involved.12 Previous studies that have explored patients’ preferences for pharmaceutical treatment of UF have not compared subgroups that may differ in their preferences. Additionally, they have not directly compared patients’ preferences with those of HCPs.
A previously published study introduced, described, and validated the adaptive self-explication (ASE) method for multi-attribute preference measurement, in which the importance of different attributes can be estimated.13 While this was initially developed using data on consumer preferences, the methodology is broadly applicable to any situation in which there is a need to understand the respective importances of different respondent preferences. Hence, this method can be adapted to allow research into patient and physician preferences around UF treatments.
This study aimed to understand key drivers of HCP and patient preferences for attributes of pharmaceutical treatments indicated for symptomatic UF in premenopausal women. It also aimed to identify and explore HCP and patient segments that differed in treatment preferences and describe the characteristics of these segments.
Materials and Methods
Study Design
This real-world US-based study invited HCPs involved in UF management and patients with UF to complete an online survey designed to quantify the relative importance (RI) of different UF treatment attributes. An ASE approach13 quantified preferences regarding treatment attributes and their levels that can influence UF treatment decisions.
The study took place between October 2021 and June 2022, including field research, data collection and analysis, and was conducted in accordance with the International Council on Harmonisation E6 Good Clinical Practice14 as well as with the ethical principles outlined in the Declaration of Helsinki 2013.15 The protocol was approved by an independent institutional review board (Castle Institutional Review Board; expedited review [protocol number: B7981082]; approval: 15/03/2022). All participants provided informed consent to participate. Case details, personal information, and images of patients or other individuals are not reported.
Study Populations
To ensure the recruitment of random samples, participants were recruited from a database (sampling frame) using a screening questionnaire. The sampling frame was managed by a specific panel service provider, who sent invitations and surveys to targeted groups involved in UF treatment decision-making, ie, obstetrician-gynecologists (OB/GYN), OB/GYN surgeons, family practice physicians, and OB/GYN nurse practitioners. For the recruitment of the patient sample consisting of premenopausal women (aged 18–55 years) with self-reported diagnoses of UF and HMB from a range of ethnic/socioeconomic backgrounds, the panel service provider used a multimodal approach (telephone calls and emails). Patients were also recruited via word-of-mouth referrals. Inclusion and exclusion criteria are shown in Table 1.
 |
Table 1 Inclusion/Exclusion Criteria for HCPs and Patients |
Development and Implementation of the Survey
An ASE preference elicitation method, based on a previously reported methodology,13 assessed HCPs’ and patients’ stated importance of treatment attributes in decision-making for pharmacological UF management. Attributes included efficacy/safety features, dosing/administration, cost considerations, and manufacturer support items. Each attribute included several levels to capture variations in the performance of each treatment feature. Attributes and levels were based on a literature review and product monographs. To inform the final survey and selection of treatment attributes for inclusion, qualitative interviews were performed with 19 HCPs and 15 patients who did not participate in the final quantitative survey. The final HCP and patient surveys were developed using Decipher (Forsta Ltd., London, UK) and included 42 and 38 attributes, respectively. Attributes were categorized into “efficacy” (HCP survey: n=23 attributes; patient survey: n=21), “safety” (n=6; n=5), “dosing” (n=2; n=2), and “other” (n=11; n=10). Both surveys assessed the same attributes; however, the language was tailored to each audience (Supplementary Table 1).
HCPs and patients rated desirability of improvement for each attribute on a 0–10 scale (0 = Not at all desirable; 10 = Extremely desirable). Respondents sorted the full set of attributes into three, approximately equal-sized groups: the most, the middle, and the least important. After sorting, each respondent ranked attributes within each group from the most to the least important. Preferences were collected by the ASEMAP™ program and, based on ranking across the three groups, pairs of attributes were presented, for which respondents allocated 100 points between the two. If two attributes were equally important, the respondent allocated 50 points to each, while different allocations indicated the relative importance of one attribute over the other. Each respondent was asked to evaluate 13–15 pairs of attributes. The initial three pairs shown to each respondent were based on the results of the respondent’s ranking exercise. Subsequent pairs were generated based on an adaptive design that maximized information provided by each question.13 Data provided estimates of RI for each attribute for each respondent, along with preference scores for level improvements of each attribute.
Statistical Analysis
The RI for each attribute was estimated for the full sample by log-linear regression in which the ratios of points from the pairwise comparisons comprised the dependent variable, and the design matrix used to generate the attribute pairs comprised the independent variables.13 The RI of attributes was indexed to 100, representing the average importance in driving choice. At 100, all attributes had an equal chance of driving treatment choice. Attributes with RI values >100 had above-average influence on choice, while those with RI values <100 had below-average influence.
A clustering (K-means) algorithm (IBM-SPSS, IBM, Armonk, New York, USA) was used to determine HCP and patient segments.16 The algorithm identified respondents with similar preferences within a segment, while ensuring that individual segments were disparate or had attribute RI values reflecting different preferences. Statistical analyses (eg, F-test) were performed to ensure that the within-group sum of squared deviations were the smallest and the across groups sum of squared deviations were the largest, and were assessed along with other criteria, including face validity of the average preference importance scores.16 An empirical approach (bootstrapping) was used to estimate the statistical significance of the estimates of the preference (RI) index.13 RI scores with a difference of >10 points across any two segments reflected a statistically significant difference across groups in interpreting the treatment drivers of the segments. Therefore, mean RI values within a segment that differed from the sample mean by >10 points were interpreted as differentiating drivers for that segment.
Respondent characteristics in each segment were compared across segments to identify characteristics associated with the likelihood that a respondent would be in a given segment. Differences in characteristics were compared using a one-tailed T-test for statistical significance. P-values ≤0.05 indicated statistically significant differences in characteristics across segments.
As the patient sample was not entirely representative of the US patient population, it was weighted against women with UF-associated HMB in Commercial and Medicaid claims data (Optum Clinformatics Data Mart and IMB Medicaid; data on file) to align with the patient population in clinical practice. The key demographics used for weighting were age, insurance type, and ethnicity. For insurance coverage, the patient sample was weighted against population data from the US Census Bureau. The HCP sample was not weighted.
Results
Overall Characteristics and Demographics
In total, 375 HCPs (200 gynecologists, 125 family physicians, and 50 OB/GYN nurse practitioners) and 300 patients diagnosed with UF responded to the survey. Response rates for those invited to participate in the survey were 18% for HCPs and 35% for patients. Most (53%) HCPs were OB/GYNs (Supplementary Table 2). The mean age of patients was 42 years, mean age at first UF diagnosis was 37 years, and most (46%) had privately funded insurance coverage (Supplementary Table 3).
Relative Importance Estimates
RI values for treatment attributes across the HCP and patient samples by segment are presented in Supplementary Tables 4 and 5, respectively.
HCP Segments
Four HCP segments were identified: “efficacy-focused”, “safety-focused”, “convenience-focused”, and “economics-focused.”
HCPs in the “efficacy-focused” segment (N=99) prioritized “improvement in Bleeding Pelvic Discomfort Scale17 at 6 months from baseline” (RI: 137 vs 111 overall HCP population mean), “achieving clinically meaningful menstrual blood loss (MBL) at 6 months from baseline” (RI: 134 vs 108), and “mean percentage reduction in MBL at 6 months from baseline” (RI: 128 vs 107; Table 2). Compared with the overall sample mean, a higher proportion of these HCPs spent ≥50% of their time on patient education (23% vs 17%; p=0.04) and were practicing in a rural location (9% vs 5%; p=0.02; Table 3).
 |
Table 2 Key Differentiating Drivers for HCPs |
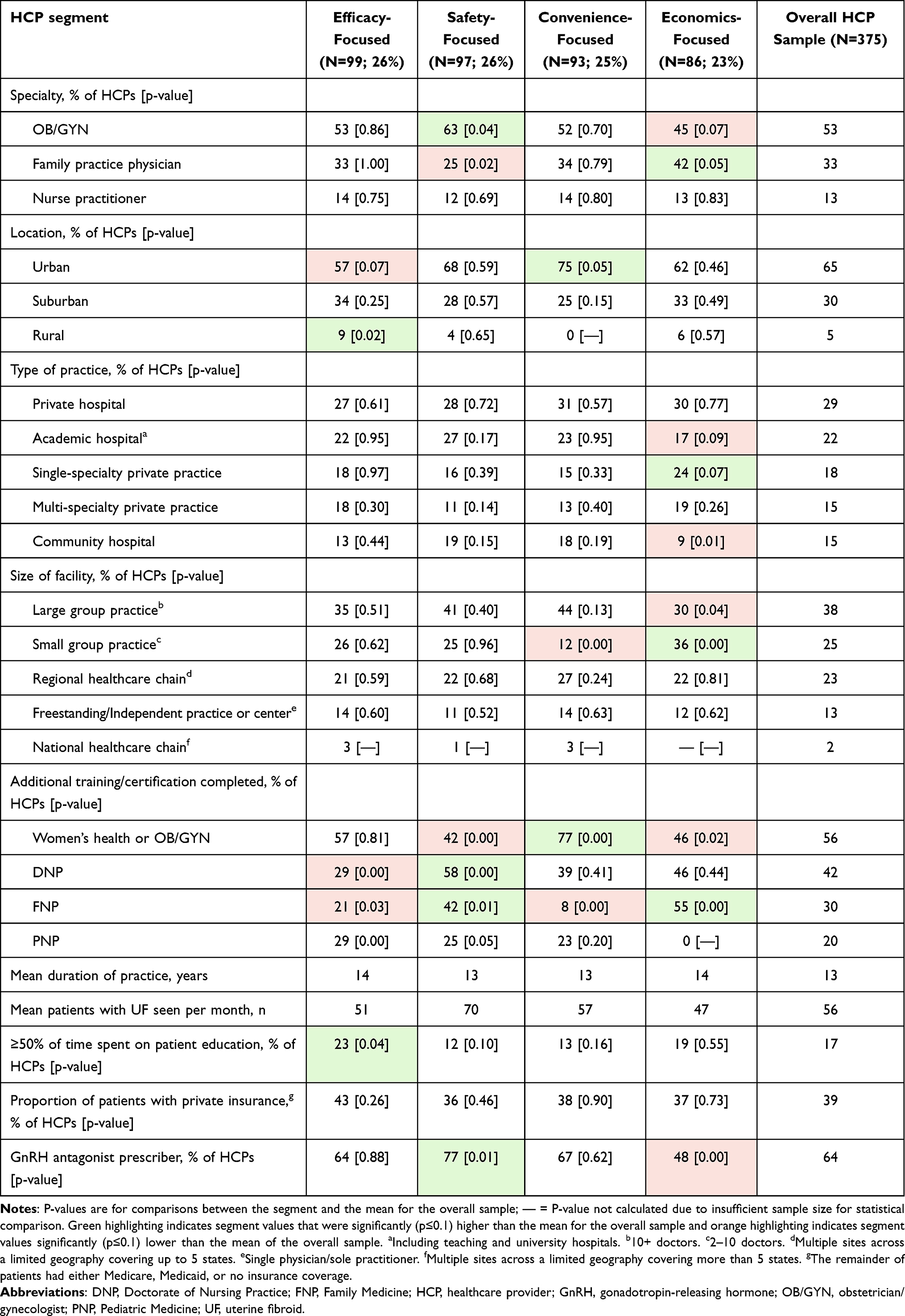 |
Table 3 Key Demographics of HCP Segments |
HCPs in the “safety-focused” segment (N=97) prioritized “percentage of patients with treatment-related hair loss” (RI: 111 vs 92) and “drug effects on bone mineral density” (BMD; RI: 108 vs 96) along with “patient out-of-pocket cost” (RI: 130 vs 124; Table 2). Compared with the overall sample mean, a higher proportion of these HCPs were OB/GYN specialists (63% vs 53%; p=0.04) and were prescribers of GnRH antagonists (77% vs 64%; p=0.01; Table 3).
HCPs in the “convenience-focused” segment (N=93) prioritized “treatment that provides contraceptive effects without need for a concomitant contraceptive” (RI: 132 vs 97), “simplified dosing schedules” (RI: 120 vs 103), and “manufacturer provision of treatment-related support to patients after drug approval” (RI: 118 vs 91; Table 2). Compared with the overall sample mean, a higher proportion of these HCPs were practicing in an urban location (75% vs 65%; p=0.05) and a lower proportion of these HCPs were working at a small group practice (12% vs 25%; p<0.01; Table 3).
HCPs in the “economics-focused” segment (N=86) prioritized “insurance coverage” (RI: 188 vs 121), “patient out-of-pocket cost” (RI: 164 vs 124) and “impact of medication on need for future hysterectomy” (RI: 153 vs 110; Table 2). Compared with the overall sample mean, a higher proportion of these HCPs were family practice physicians (42% vs 33%; p=0.05), had completed family medicine training (55% vs 30%; p<0.01), and worked at a small group practice (36% vs 25%; p<0.01) or single-specialty private practice (24% vs 18%; p=0.07), and a lower proportion were prescribers of GnRH antagonists (48% vs 64%; p<0.01; Table 3).
Patient Segments
Four patient segments were identified: “symptom-relief-driven”, “information-driven”, “cost-sensitive and surgery-averse”, and “risk-averse.”
Patients in the “symptom-relief-driven” segment (N=127) prioritized “improvement in menstrual bleeding that impacts daily life” (RI: 116 vs 107), “reduction in MBL” (RI: 114 vs 102), and “improvement in symptom severity” (RI: 113 vs 102; Table 4). Compared with the overall sample mean, a higher proportion of these patients were on employer/union-funded insurance plans (49% vs 38%; p=0.04), and a lower proportion felt that they had comprehensive knowledge of the available treatment options (20% vs 32%; p=0.02; Table 5).
 |
Table 4 Key Differentiating Drivers for Patients |
 |
Table 5 Key Demographics of Patient Segments |
Patients in the “information-driven” segment (N=67) prioritized “availability of features within a one-stop-shop patient program” (RI: 135 vs 98), “provision of educational support for patients” (RI: 134 vs 113), and “study duration of a medication before it is approved” (RI: 129 vs 101; Table 4). Compared with the overall population sample mean, a higher proportion of these patients had obtained a bachelor’s degree (69% vs 46%; p<0.01), were in full-time employment (97% vs 84%; p=0.01) and felt that they had comprehensive knowledge of the available treatment options (47% vs 32%; p=0.03; Table 5).
Patients in the “cost-sensitive and surgery-averse” segment (N=58) prioritized “impact of medication on the need for hysterectomy” (RI: 150 vs 115), “out-of-pocket cost” (RI: 146 vs 99), and “reduction in fibroid size” (RI: 130 vs 99; Table 4). Compared with the overall sample mean, a higher proportion of these patients were Asian (18% vs 4%; p<0.01), had obtained an associate degree (30% vs 19%; p=0.05), and had military/veteran insurance (10% vs 3%; p<0.01), and a lower proportion felt a lack of knowledge about the available treatment options (16% vs 28%; p=0.05; Table 5).
Patients in the “risk-averse” segment (N=48) prioritized “medications with warnings related to increased risk of cardiovascular events” (RI: 171 vs 112), “drug effects on BMD” (RI: 154 vs 107), and “impact of medication on the need for myomectomy” (RI: 137 vs 105; Table 4). Compared with the overall sample mean, a higher proportion of these patients identified as Latin American or Hispanic (21% vs 12%; p=0.05), had obtained a graduate degree (39% vs 24%; p=0.02), were on a patient-funded insurance plan (64% vs 46%; p=0.01), and felt that they had comprehensive knowledge of the available treatment options (47% vs 32%; p=0.03, Table 5).
Discussion
In this study, HCPs were categorized into four preference segments based on treatment attributes: efficacy-focused, safety-focused, convenience-focused, and economics-focused. Patients were grouped into four preference segments: symptom-relief, information-driven, cost-sensitive and surgery-averse, and risk-averse. Key characteristics that differed between HCP segments included specialist training, practice location, time spent on patient education, and additional OB/GYN training; those that differed between patient segments included race/ethnicity, level of education, and insurance type.
There is a lack of HCP and patient preference studies for UF management. One study reporting patient preferences in UF used a best-worst scaling preference elicitation approach to rank factors associated with surgical UF treatments; factors influencing choice included symptom relief and complications,18 reflecting key treatment drivers in “symptom-relief-driven” and “risk-averse” patient segments in the current study. Patient preference studies have been reported for other gynecological conditions. In endometriosis, three discrete choice experiment (DCE) studies have been published to date;19–21 factors influencing preferences included symptom improvement, administration route, and risk of undesirable effects (eg, hot flashes, irregular bleeding).19–21 Despite similarities in treatment preferences to the present study, results cannot be directly compared considering differences in disease and methodology.
Based on the present analysis, it is not possible to establish definitive causal relationships between respondent characteristics and preference segments. While hypotheses have been proposed, some relationships remain unexplained. “Efficacy-focused” HCPs showed a higher proportion of time spent on patient education and thus were likely more informed of patient needs. Most practiced in rural locations where referrals to expert centers may be difficult; hence, these HCPs need to address symptoms themselves. “Safety-focused” HCPs were mostly OB/GYN specialists and prescribers of GnRH antagonists. These specialists were likely well-informed about newer therapies (including efficacy/safety profiles) and, therefore, more likely to prescribe GnRH antagonists. “Convenience-focused” HCPs mainly practiced in urban locations and larger clinics, with fewer working in small group practices. This may suggest a high patient flow, limiting time for patient education, and increasing the importance of ease-of-use. “Economics-focused” HCPs were largely family practice physicians, few of whom prescribed GnRH antagonists. Family practice physicians may not have access to certain treatments and hence may not be key prescribers of specialty products (eg, GnRH antagonists). A high proportion of “symptom-relief-driven” patients had employer/union-funded insurance plans, suggesting that symptom relief, which impacts ability to work, is likely a concern of employed patients. “Information-driven” patients were characterized by a higher percentage holding a bachelor’s degree and feeling they had comprehensive knowledge of treatments. A greater understanding of treatments may explain their classification in this segment. “Risk-averse” patients comprised a higher proportion of Latin American or Hispanic individuals, those with graduate degrees, and those covered by patient-funded insurance plans. As risk aversion is highly individualistic, it is not possible to reliably explain this segment’s characteristics.
With a greater variety of pharmacological interventions, there is an opportunity to individualize treatment. ACOG guidelines recommend patient-centered SDM for UF management.3 The current study can support SDM in UF by providing insights on treatment attributes important to patients, ensuring that these are discussed in the SDM process. Patient segmentation provides evidence of heterogeneity in preference for UF treatments; understanding treatment attribute preferences may assist HCPs in bringing patient perspectives to bear and help to tailor treatments to meet their needs.22 Engaging patients in SDM may facilitate greater patient agency and autonomy in UF management, treatment acceptance, and health equity.23,24
This analysis also evaluated HCP segmentation. HCPs are responsible for ensuring patients are adequately informed about treatment decisions, allowing effective participation in SDM. However, HCPs may influence the clarity and tailoring of information for patients, and may unintentionally provide biased information towards a specific outcome.25,26 This study provides knowledge of HCP segments that differ in their treatment preferences. It may, therefore, help HCPs to understand and challenge biases and barriers, and accept decisions that they may not perceive as the most appropriate course, but that are preferred by their patients.22
Future research should assess the generalizability and reproducibility of the HCP and patient segments and whether findings can be used for SDM in clinical practice. Pre-consultation questionnaires that predict patient preference may help guide decision-making and improve patient–provider communication. This is of substantial value, as fractured patient–provider relationships result in poor post-visit adherence and negatively impact health.27
Strengths of the study include the ASE methodology. DCE questionnaires assess a brief list of attributes and may exclude some relevant attributes. DCEs are also limited in terms of capturing the RI of each factor, and repeated choice tasks can cause decision fatigue and affect accuracy.13,21 The ASE approach addresses limitations through overall attribute ranking and comparisons within pairs of attributes adapted for each respondent.13 This allows a relatively large number of attributes to be studied whilst ensuring that only the most relevant questions are presented to the participant, reducing decision fatigue.13 Additionally, ASE-based questionnaires can improve predictive validity versus traditional methods.13 Another strength is the uniqueness of the study design, with parallel assessment of HCP and patient preferences, and selections made from similar sets of attributes, helping to assess the heterogeneity of preferences within and between both groups.
Limitations include how additional attributes outside of those measured may influence treatment preferences. Additionally, as most enrolled patients had commercial insurance, the sample may not be representative of the US population of women with UF. Furthermore, boundaries between identified HCP/patient segments are fluid; in practice it may be challenging to determine which drivers motivate individual HCPs and patients. As with most survey-based studies, there is a risk that some participants may not have fully understood the attributes within the questionnaire.
Conclusions
Various drivers influence HCPs and patients when choosing pharmacological treatments for UF management. Knowledge of these drivers can aid SDM between HCPs and patients with symptomatic UF. Understanding HCP and patient segments that differ by treatment choice can help identify care that meets patients’ needs and may improve general patient management in routine clinical practice.
Abbreviations
ACOG, American College of Obstetricians and Gynecologists; ASE, adaptive self-explication; BMD, bone mineral density; DCE, discrete choice experiment; GnRH, gonadotropin-releasing hormone; HCP, healthcare provider; HMB, heavy menstrual bleeding; MBL, menstrual blood loss; OB/GYN, obstetrician-gynecologist; RI, relative importance; SDM, shared decision-making; UF, uterine fibroids.
Data Sharing Statement
Pseudonymized individual level data, questionnaires, attributes, and level labels/descriptions will be shared upon reasonable request from the corresponding author.
Acknowledgments
This study was funded by Sumitomo Pharma Switzerland GmbH (formerly Myovant Sciences GmbH). The analysis was performed by Optimal Strategix Group (Pennsylvania, USA). The authors would like to acknowledge Darin Lewis (formerly of Optimal Strategix Group) for his contribution to the study design and data analysis, and Nicole Ansani (formerly of Pfizer) for her contribution to the study design and interpretation of findings. The authors would like to thank Jennifer Virro for her role as Principal Investigator in submission to the independent institutional review board. The authors would also like to acknowledge editorial support and medical writing from AXON Communications (London, UK), funded by Sumitomo Pharma Switzerland GmbH (formerly Myovant Sciences GmbH).
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Consent to Participate
The protocol was approved by an independent institutional review board (Castle Institutional Review Board; expedited review [protocol number: B7981082]; approval: 15/03/2022). All participants provided informed consent to participate. Case details, personal information, and images of patients or any other individuals are not reported.
Funding
This study and editorial support for the article was funded by Sumitomo Pharma Switzerland GmbH (former Myovant Sciences GmbH) and Pfizer.
Disclosure
OSML is a speaker for Intuitive Surgical and has received consulting fees from Sumitomo Pharma America and Pfizer. EH and VR are employed by Sumitomo Pharma Switzerland GmbH. CL is employed by Sumitomo Pharma America. BH is employed by Pfizer, Inc. RS is employed by Optimal Strategix Group, which was compensated by Sumitomo Pharma Switzerland GmbH (formerly Myovant Sciences GmbH at the time the study was performed) to conduct this research. SKA has received consulting fees from Sumitomo Pharma America and Pfizer. The authors report no other conflicts of interest in this work.
References
1. Stewart EA, Cookson CL, Gandolfo RA, et al. Epidemiology of uterine fibroids: a systematic review. BJOG. 2017;124:1501–1512. doi:10.1111/1471-0528.14640
2. De La Cruz MS, Buchanan EM. Uterine fibroids: diagnosis and treatment. Am Fam Physician. 2017;95:100–107.
3. The American College of Obstetricians and Gynecologists. Management of symptomatic uterine leiomyomas: ACOG practice bulletin, number 228. Obstet Gynecol. 2021;137:e100–e115. doi:10.1097/AOG.0000000000004401
4. Vilos GA, Allaire C, Laberge PY, et al. The management of uterine leiomyomas. J Obstet Gynaecol Can. 2015;37:157–178. doi:10.1016/S1701-2163(15)30338-8
5. Stewart EA, Solomon CG. Clinical practice. Uterine fibroids. N Engl J Med. 2015;372(17):1646–1655. doi:10.1056/NEJMcp1411029
6. Marsh EE, Al-Hendy A, Kappus D, et al. Burden, prevalence, and treatment of uterine fibroids: a survey of U.S. women. J Womens Health. 2018;27:1359–1367. doi:10.1089/jwh.2018.7076
7. Downes E, Sikirica V, Gilabert-Estelles J, et al. The burden of uterine fibroids in five European countries. Eur J Obstet Gynecol Reprod Biol. 2010;152:96–102. doi:10.1016/j.ejogrb.2010.05.012
8. McKain L, Edsall K, Dufour R, et al. Treatment patterns in patients with uterine fibroids with and without a diagnosis of heavy menstrual bleeding: results from a large U.S. claims database. J Womens Health. 2023;32:332–340. doi:10.1089/jwh.2022.0056
9. Madueke-Laveaux OS, Elsharoud A, Al-Hendy A. What we know about the long-term risks of hysterectomy for benign indication—a systematic review. J Clin Med. 2021;10:5335. doi:10.3390/jcm10225335
10. Stewart EA, Lytle BL, Thomas L, et al. The Comparing Options for Management: PAtient-centered REsults for Uterine Fibroids (COMPARE-UF) registry: rationale and design. Am J Obstet Gynecol. 2018;219:95.e91–95.e10. doi:10.1016/j.ajog.2018.05.004
11. Vuik SI, Mayer EK, Darzi A. Patient segmentation analysis offers significant benefits for integrated care and support. Health Aff. 2016;35:769–775. doi:10.1377/hlthaff.2015.1311
12. Dobler CC, Sanchez M, Gionfriddo MR, et al. Impact of decision aids used during clinical encounters on clinician outcomes and consultation length: a systematic review. BMJ Qual Saf. 2019;28:499–510. doi:10.1136/bmjqs-2018-008022
13. Netzer O, Srinivasan V. Adaptive self-explication of multiattribute preferences. J Marketing Res. 2011;48:140–156. doi:10.1509/jmkr.48.1.140
14. European Medicines Agency: ICH guideline E6 on Good Clinical Practice (GCP). In (vol 2025), 2025.
15. World Medical Association. World Medical Association Declaration of Helsinki: ethical principles for medical research involving human subjects. JAMA. 2013;310:2191–2194. doi:10.1001/jama.2013.281053
16. Hair JF, Black WC, Babin BJ. Multivariate Data Analysis.
17. Hudgens S, Gauthier M, Hunsche E, et al. Development of the bleeding and pelvic discomfort scale for use in women with heavy menstrual bleeding associated with uterine fibroids. Value Health. 2022;25:1986–1994. doi:10.1016/j.jval.2022.06.005
18. Babalola O, Gebben D, Tarver ME, et al. Patient preferences regarding surgical treatment methods for symptomatic uterine fibroids. Ther Innov Regul Sci. 2023;57:976–986. doi:10.1007/s43441-023-00525-1
19. Akiyama S, Goren A, Basurto E, et al. Treatment preferences among Japanese women with dysmenorrhea: results from a discrete choice experiment study. Patient Prefer Adherence. 2018;12:1627–1640. doi:10.2147/PPA.S166332
20. Poulos C, Soliman AM, Tekin S, et al. Patient preferences for elagolix and leuprolide for treating endometriosis-related pain in the United States. Expert Rev Pharmacoecon Outcomes Res. 2021;21:1091–1099. doi:10.1080/14737167.2021.1832468
21. Poulos C, Soliman AM, Renz CL, et al. Patient preferences for endometriosis pain treatments in the United States. Value Health. 2019;22:728–738. doi:10.1016/j.jval.2018.12.010
22. Légaré F, Witteman HO. Shared decision making: examining key elements and barriers to adoption into routine clinical practice. Health Aff. 2013;32:276–284. doi:10.1377/hlthaff.2012.1078
23. Riggan KA, Stewart EA, Balls-Berry JE, et al. Patient recommendations for shared decision-making in uterine fibroid treatment decisions. J Patient Exp. 2021;8:23743735211049655. doi:10.1177/23743735211049655
24. Langford AT, Williams SK, Applegate M, et al. Partnerships to improve shared decision making for patients with hypertension - health equity implications. Ethn Dis. 2019;29:97–102.
25. Jacobs S, Davies N, Butterick KL, et al. Shared decision-making for children with medical complexity in community health services: a scoping review. BMJ Paediatrics Open. 2023;7:e001866. doi:10.1136/bmjpo-2023-001866
26. Boland L, Graham ID, Légaré F, et al. Barriers and facilitators of pediatric shared decision-making: a systematic review. Implement Sci. 2019;14:7. doi:10.1186/s13012-018-0851-5
27. Satcher D, Dawes DE. Race and the patient-physician relationship in 2021. JAMA. 2021;326:595–596. doi:10.1001/jama.2021.12454
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.