Back to Journals » Patient Preference and Adherence » Volume 17
Understanding Patient Preferences Regarding the Important Determinants of Breast Cancer Treatment: A Narrative Scoping Review
Authors Yeo HY ![]() , Liew AC, Chan SJ, Anwar M
, Liew AC, Chan SJ, Anwar M ![]() , Han CHW
, Han CHW ![]() , Marra CA
, Marra CA ![]()
Received 3 August 2023
Accepted for publication 7 October 2023
Published 31 October 2023 Volume 2023:17 Pages 2679—2706
DOI https://doi.org/10.2147/PPA.S432821
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Hui Yee Yeo,1,2 Ai Ch’i Liew,2 Suz Jack Chan,1 Mudassir Anwar,1 Catherine Hye-Won Han,3 Carlo A Marra1
1School of Pharmacy, University of Otago, Dunedin, New Zealand; 2Clinical Research Center, Hospital Seberang Jaya, Penang, Malaysia; 3Faculty of Medical and Health Sciences, University of Auckland, Auckland, New Zealand
Correspondence: Carlo A Marra, School of Pharmacy, University of Otago, PO Box 56, Dunedin, 9054, New Zealand, Tel +64-34797275, Fax +64-34797034, Email [email protected]
Objective: Conventionally, optimal treatment strategies for breast cancer have been largely determined by physicians, with a scant understanding of patients’ treatment values and preferences. Incorporating patient preferences in the decision-making process for breast cancer treatment is gaining recognition and can potentially improve treatment outcomes and compliance. This scoping review aims to synthesize evidence on the key determinants that are most valued by breast cancer patients when deciding on their treatment options.
Methods: We searched three electronic databases (PubMed/MEDLINE, SCOPUS, and CINAHL Plus) utilizing a systematic scoping review method. Two reviewers independently screened, applied inclusion criteria, reviewed, and synthesized findings. A mixed-method narrative approach combining the inductive thematic analysis and content analysis methodologies was used to synthesize and summarize the findings.
Results: The review included 22 studies, leading to the conceptualization of 5 overarching themes and 17 sub-themes. Among these, the most frequently cited theme was treatment benefits, followed by treatment-related process, treatment-related risk, quality of life, and cost of treatment. Women with breast cancer highly value treatments that offer good effectiveness, prolong survival, prevent recurrence, and maintain quality of life. Patient concerns include treatment-related side effects, safety, the risk of secondary cancer, and direct or indirect out-of-pocket costs. Additionally, patients also consider treatment duration, mode of administration, physician recommendation, and treatment availability and accessibility when deciding on their preferred treatment.
Conclusion: The evidence synthesized in this review offers insights into refining breast cancer treatment strategies to align more closely with patient values. Recognizing and integrating patient perspectives in breast cancer care could potentially lead to improved treatment outcomes, enhanced patient compliance, and more personalized care. Healthcare professionals are encouraged to incorporate these key determinants in their treatment decision-making processes, aiming to deliver a patient-centered care that aligns with the unique preferences and values of each patient.
Plain Language Summary: Breast cancer is a significant health concern, and treatment decisions have traditionally driven by physicians, often without due consideration for patients’ preferences in their treatment choices. This scoping review aimed to explore and summarize what matters most to breast cancer patients when deciding on their treatment options. We found five main themes that were important to patients:Effectiveness: Patients highly value treatments that are effective in fighting cancer, prolonging survival, and preventing recurrence.Treatment-related process: The length of treatment and availability of different therapies influenced patients’ choices. Patients trust their doctors’ expertise but also value being involved in the decision-making process to have their preferences considered.Side Effects and Safety: Concerns about treatment-related side effects and the risk of secondary cancer were critical factors in decision-making.Quality of Life: Maintaining a good quality of life during treatment is crucial for patients.Financial Burden: The additional direct and indirect out-of-pocket costs of treatment were important considerations for patients.
Understanding patients’ preferences is vital in developing personalized treatments that align with their values. Healthcare professionals need to communicate effectively with patients and involve them in the decision-making process. Patient decision aids and tailored financial assistance programs could also be helpful. Further research is needed to identify effective strategies to tailor treatments to meet patients’ preferences. Overall, this review sheds light on what matters most to breast cancer patients, empowering them to be more active participants in their treatment decisions and potentially improving treatment outcomes and overall well-being.
Keywords: breast cancer, patient preference, treatment decision making, narrative scoping review
Introduction
Breast cancer (BC) is the most common cancer in women and the fifth leading cause of cancer-related deaths worldwide.1 According to projections, the incidence of BC is expected to increase significantly in the future, with estimates suggesting that by the year 2070, the annual number of diagnosed cases will surpass four million worldwide, representing a doubling of current rates.2
The prognosis for women with early-stage BC (eBC) is generally positive, whereas those with advanced or metastatic BC (mBC) have a low 5-year survival rate of approximately 20%.3 The primary treatment objectives for eBC involve the surgical removal of the tumour from the breast and regional lymph nodes, preventing locoregional recurrence, and improving survival.4 In addition, systemic therapy may be administered before surgery (neoadjuvant), after surgery (adjuvant), or both, depending on the subtype of BC and the extent of local disease at diagnosis. On the other hand, the primary aims of therapy for mBC are to control the growth of the tumour thereby extending life expectancy and alleviating symptoms for a better quality of life, as mBC is incurable. The current systemic therapy landscape for mBC includes chemotherapy, endocrine therapy, immunotherapy, and targeted therapy.5 Different treatments pose different benefits and drawbacks. Whilst the majority of treatments contribute to an increase in survival rates, they may also bring unwanted adverse effects for patients, which potentially diminish their overall quality of life. Acute adverse effects may manifest in the form of fatigue, alopecia, cytopenia, myalgia and arthralgia, and chemotherapy-induced peripheral neuropathy. Long-term complications may include heart disease, premature menopause, and psychological effects.6
Traditionally, the decision-making process for BC treatment has been predominantly driven by physicians, guided by the treatment guidelines, such as the European Society for Medical Oncology (ESMO) BC Guidelines7 and National Comprehensive Cancer Network (NCCN) Guidelines in Breast Cancer,8 and little is known about patient’s preference for treatment. The preference for characteristics of different therapy choices is subjective and dependent on a variety of cultural and individual factors, and the preferences of patients and healthcare providers regarding the treatment of various diseases, including cancer, have been shown to vary.9 Given the significant variation in the prognosis of distinct stages of BC, there is substantial potential for patient preferences to be incorporated into the decision-making process. Over recent years, the role of patient preference and value has gained growing recognition in individual clinical decision-making and the shaping of public health policy. Patient preference, which reflects their perceptions of risk and general comfort with the various approaches, is an important determinant of treatment selection.10 There has been increasing interest in the integration of patient values and perspectives in the development of treatment recommendations and patient decision aid in clinical practice. For instance, the ESMO guidelines strongly recommend that healthcare providers actively involve patients in all treatment decision-making,11,12 while patient decision aids have demonstrated their value in facilitating shared decision-making between healthcare providers and patients when deciding on treatment options.13,14
Prior systematic review studies in the context of BC treatment from the patient’s perspective have placed a greater emphasis on the type of care, the satisfaction of the healthcare system, post-cancer treatment care, patient-reported outcome measures, and management of treatment-related side effects rather than on values and perceptions of the attributes that may influence treatment preferences.15–19 Therefore, the primary objective of this scoping review is to explore and synthesize evidence regarding the important determinants in BC treatment that are most valued and preferred by patients.
Materials and Methods
We conducted a scoping review to assess and consolidate the evidence concerning important determinants in the treatment of BC that matter to patients, guided by the six-step theoretical frameworks developed by Arksey and O’Malley20 along with the refinements proposed by Levac et al.21 Due to the considerable heterogeneity in the existing literature on this subject, conventional data synthesis methods like systematic reviews or meta-analyses would not have been suitable approaches. Scoping reviews, on the other hand, facilitate the mapping and synthesis of evidence across a wide range of related literature, which aids in addressing broad research questions and enhancing a deeper understanding of the subject.22,23
A research team of five members collaboratively established a research protocol and agreed upon the scope of the review, including the research questions, search strategy, and methodology to be used to conduct the review. The PIOS (population, intervention, outcome, and study type) format was employed to define the research question and the inclusion and exclusion criteria (Table 1). Studies were eligible for inclusion, regardless of methodology, if they empirically determined the attributes or factors associated with the treatment preference of BC patients. To ensure our review encompassed the most up-to-date evidence on significant determinants that matter to patients in the current rapid evolving landscape of BC treatment, we restricted the search period to span from January 2010 to June 2023. The full search strategy in this study was documented according to Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines.24
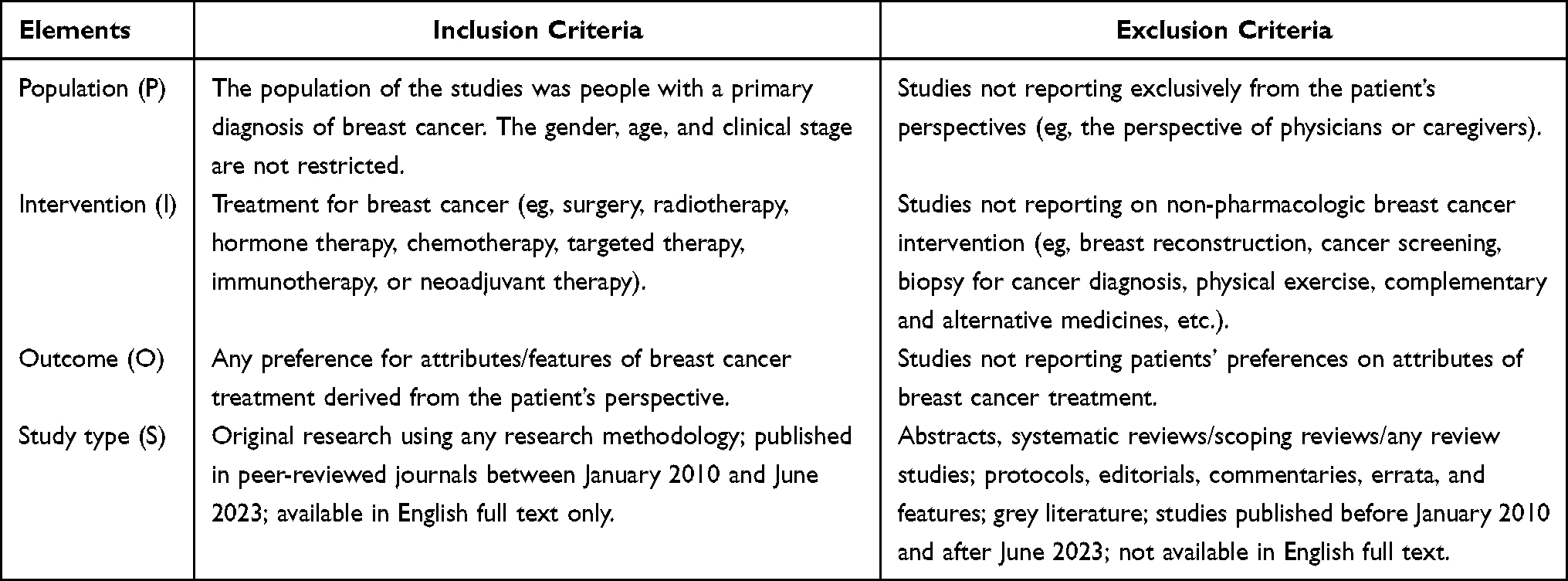 |
Table 1 The PIOS and Inclusion and Exclusion Criteria of the Review |
Search Strategy
In line with rapid review recommendations,25 we limited our searches to three databases: PubMed/MEDLINE, SCOPUS, and CINAHL Plus. A broad search of keywords (titles, abstracts, and subject headings) was conducted to identify relevant studies that combined terms for “breast cancer”, “treatment”, and “patient preference”, adapted to each interface and database. The Medical Subject Headings (MeSH) terms and explosions were applied across the terms where applicable. The detailed search strategy is described in Supplementary Table 1: Search Strategy.
Article Screening and Data Extraction
All search tasks were completed by a single researcher (HYY) in July 2023 and all returned articles were entered into EndNoteTM X9 for screening and data extraction, and duplicates were removed. Two reviewers independently screened the titles and abstracts according to the inclusion and exclusion criteria (HYY and SJC), and full-text articles were retrieved if all inclusion criterion was met. The full-text articles were then independently reviewed and synthesized by two reviewers (HYY and ACL). One reviewer (ACL) extracted the data from the included articles into a pre-defined and piloted data extraction table, while a second reviewer (HYY) cross-checked them for consistency and reliability. Disagreements in data extraction and interpretation were resolved through team discussion with a third reviewer (CM). The information included in the data extraction tables (Microsoft Excel spreadsheet, Microsoft Corporation, Redmond, Washington) were the following: first author; year of publication; country(s); study objective (s); method/design; sample size; cancer stage; treatment type; outcomes; plausible attributes/levels; and strength/limitation. Additionally, to provide more breadth to the analysis, findings from qualitative studies in the form of textual data were extracted, which included either a verbatim quote from patients or statements by the authors that were corroborated by patient-reported data.
Data Analysis
To provide a more comprehensive and nuanced understanding of the research questions, we utilized a mixed-method narrative approach to synthesize and summarize findings in this review, integrating the inductive thematic analysis and content analysis methodologies.26–28 Our analysis followed an inductive approach, meaning that we did not predefine themes or codes to guide data extraction and analysis. Instead, themes were developed using a “constant comparison” method, wherein the data was broken down into discrete “events”, and related events’ were coded into descriptive themes. Key themes that emerged from the studies that correspond to our research objectives were systematically identified by two reviewers (HYY and ACL). First, HYY coded findings from both qualitative and quantitative studies, followed by analysing patterns in the textual data to generate a preliminary thematic layout. Then, ACL reviewed the preliminary thematic layout and refined the themes through a series of discussions with HYY until a consensus was reached. Disagreements in data analysis were resolved through team discussion with a third researcher (CM). A minimum of three papers’ worth of pooled data had to be coded to the same theme for a distinct theme to emerge. The final thematic layout was collectively described as a team with a consensus reached. In addition, the frequency of themes and sub-themes mentioned in the included papers was counted and summarized in a table.
Results
A total of 1984 studies were retrieved electronically after removing duplicates. After titles and/or abstract screening, 1892 studies that did not meet the inclusion criteria were excluded. The full text of the remaining 92 studies was reviewed, and 70 studies that did not meet the inclusion criteria were excluded. Ultimately, 22 studies that met our eligibility criteria were included (Figure 1).
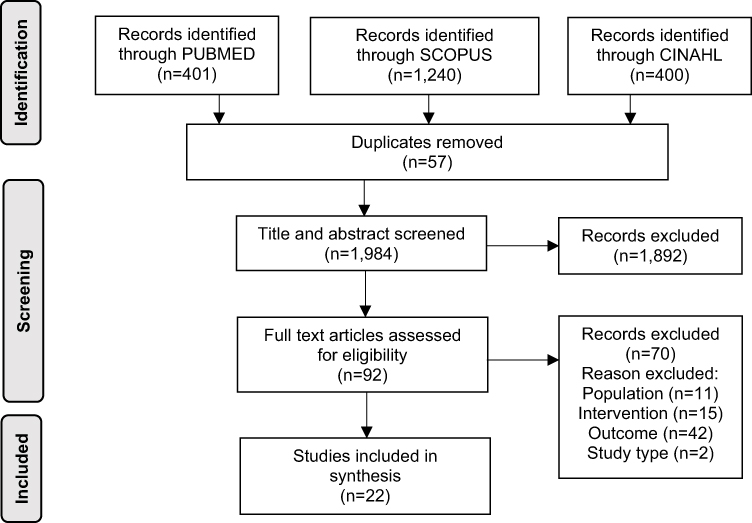 |
Figure 1 PRISMA study flow diagram. Note: Adapted from Moher D, Liberati A, Tetzlaff J, Altman DG, PRISMA Group* t. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. Annals of internal medicine. 2009;151(4):264-269.24.24 |
Characteristics of the Included Studies
A total of 7 studies with a qualitative methodology13,29–34 and 15 studies with a quantitative methodology35–49 were included. The total number of participants in these studies was 3817. The published studies included articles from the United States of America (USA) (n=4,), the Netherlands (n=4), Canada (n=4), United Kingdom (UK) (n=2), Spain (n=2), European countries (n=2), France (n=1), Japan (n=1), Korea (n=1), Germany (n=1), and Australia (n=1). A total of 9 studies reported on population with eBC, 7 studies on mBC, 2 studies on BC of all stages, and 4 studies did not specifically report on the cancer status. Out of the seven qualitative studies conducted, five of them employed individual interviews as the primary method to gather data. One of the studies opted for a focus group discussion, while the remaining study utilized a combination of both individual interviews and focus group discussions. For the quantitative studies included in this review, ten of them relied on surveys as the primary method for data collection, which were conducted either through paper-based, online, or phone-based approaches. Additionally, two studies utilized the conjoint analysis survey method, one employed the discrete choice experiment method, another used the time trade-off method, and one more used the contingent valuation method. The included studies are summarised in Table 2.
 |
Table 2 Summary of Included Studies by Study Design |
Important Determinants in Breast Cancer Treatment That Patient Values
Five broad themes were conceptualized from the important determinants in BC treatment, characterized by 17 sub-themes (Table 3). A narrative summary of themes and sub-themes is illustrated below.
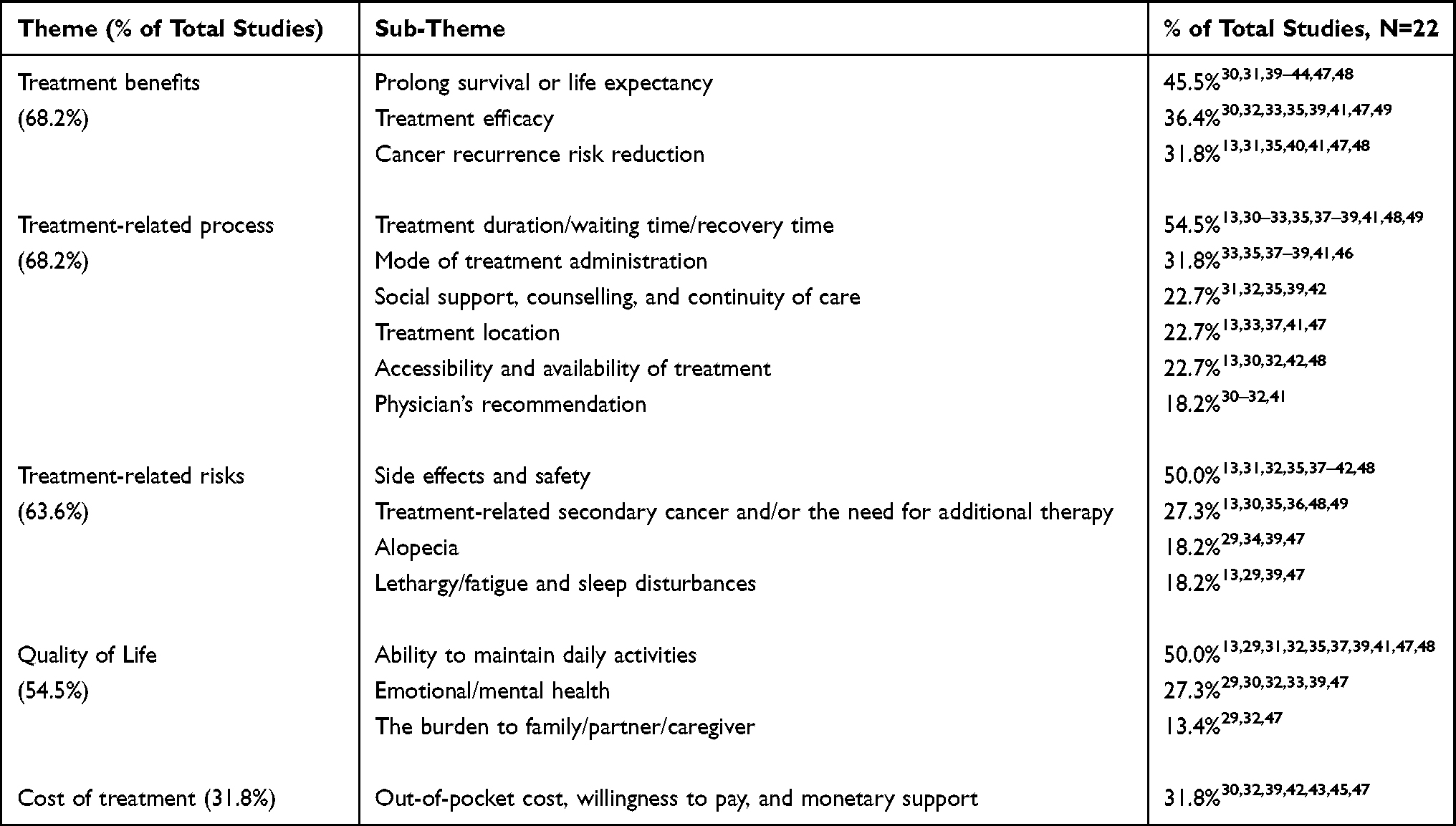 |
Table 3 Conceptual Framework of Important Determinants in Breast Cancer Treatment from Patient’s Perspective, and Percentage of Studies Under Each Sub-Theme |
Treatment Benefits
Prolong Survival or Life Expectancy
The vast majority of patients diagnosed with BC, regardless of the stage of the disease, expressed a strong preference for survival benefits compared to other benefits in treatment decision-making.30,31,39–44,47,48 Women with eBC tend to opt for mastectomy over breast-conserving surgery (BCS) as a means to increase their chance of survival so that they could spend more time with their families, particularly those with young children.30 Furthermore, the decision to undergo chemotherapy was often related to the patient’s desire to be cancer-free, fear of cancer recurrence, and the desire to extend life expectancy.31 Patients with eBC tend to judge small to moderate benefits, in terms of increase in survival rates, as sufficient to consider systemic therapy worthwhile. In contrast, Hamelinck et al reported that approximately one-fifth of women from the study would refuse hormonal therapy even with an absolute survival benefit of 25%.40,41 The individual patient’s attitudes towards the benefits and risks of treatment might vary considerably, with some patients willing to accept treatment for little or no benefit, while others would refuse treatment regardless of the potential benefit.48 On the other hand, Harding et al documented that patients with mBC were more willing to trade off the treatment side effects for a longer life expectancy. Nevertheless, it is worth highlighting that while most patients in the study reported by Harding et al prefer a treatment that can prolong their survival, a minority expressed their desire to live out their time without any medical intervention.42
Treatment Efficacy
Patients with a cancer remission treatment goal prioritized treatment efficacy over other factors.32 However, older women exhibited heightened concerns over the efficacy and likelihood of cures following surgical or hormonal therapy interventions.35 Furthermore, the efficacy of different treatment options for mBC was a prominent concern for patients, with treatment efficacy being rated as the most important attribute, surpassing other attributes related to side effects by almost threefold. Women with mBC revealed a preference towards a treatment that can effectively control the growth of the tumour.39 Similarly, two separate studies have reported a consistent patient preference for a treatment that would effectively reduce the growth of the tumour.30,47 Patients expressed a strong desire to expedite the removal of the tumour, as evidenced by the quote “I just want to get this out of me as soon as possible.”30 Chemotherapy was preferred over hormonal therapy as patients perceived it to have superior efficacy.41 This is supported by evidence from a conjoint analysis study which also identified treatment efficacy as the most important attribute.49
Cancer Recurrence Risk Reduction
BC patients, particularly older patients, often opt for chemotherapy to reduce the risk of cancer recurrence.31 This desire to evade recurrence was also observed in both younger and older patients as a key motivation for undergoing chemotherapy and hormonal therapy.41 In fact, older patients indicated that they wanted to ascertain the likelihood of the treatment they were receiving in preventing cancer recurrence.35 Furthermore, Gandhi et al found that a decrease in recurrence risk of less than 5% was considered worthwhile for continuing hormonal therapy beyond the initial 5 years by women with eBC.40 It is worth noting that the psychological impact of cancer recurrence was a significant concern for BC patients undergoing treatment. Patients undergoing chemotherapy in particular experienced high levels of anxiety and fear, with “fear for metastases and recurrence” being quoted as a major concern.47
Treatment-Related Process
Treatment Duration, Waiting Time, and Recovery Time
For many patients, the long waiting time during treatment was a source of concern, as it can have a profound impact on their daily lives.37 Patients with young children or family members requiring care, in particular, were anxious about the length of time they will be unable to fulfill their familial duties.30,31 On the other hand, the total treatment duration of hormonal therapy was frequently a deterrent, with some patients commending chemotherapy due to its shorter total treatment duration in comparison to hormonal therapy.41,49 Furthermore, it is interesting to note that a conjoint model revealed that the treatment duration was rated as one of the least significant attributes of treatment preference by patients compared to survival, side effects, and QoL.39 Recovery time was also a pertinent deciding factor for patients who have work or personal responsibilities. Patients with significant work or personal responsibilities were more likely to choose BSC and radiation over mastectomy as their preferred surgical treatment, as it allows them to resume their daily activities more quickly.32 Time savings and convenience were reported as the main rationales for preference towards SC administration compared to IV.33,38
Mode of Treatment Administration
BC patients’ preferences for the mode of administration of their cancer treatment vary widely. A multi-center randomized clinical trial revealed a strong patient preference for SC treatment compared to the conventional IV delivery method, particularly for patients with high personal, familial, and occupational commitments.33 The preferences for SC were corroborated by two other studies, citing similar reasons.38,46 Furthermore, in another study, a majority of patients with mBC preferred oral over IV chemotherapy, due to the ease of administration.37 Patients’ opinions on the mode of administration varied, with some preferring oral delivery due to their aversion to needles, while others preferred IV delivery due to their perception that taking a pill every day was burdensome.41
Social Support, Counselling, and Continuity of Care
The lack of social support was identified as a significant factor that can affect patients’ decisions regarding their treatment.31 Specifically, women who lacked social support or were the primary caregiver for their families were more likely to refuse treatments that require them to be away from home.30 Additionally, older women expressed concerns about the availability of support following surgery.35 While not the top priority for some patients, those with mBC expressed a desire for patient support programs offered by drug manufacturers or financial assistance from charities or research organizations.39 Interestingly, patients with mBC expressed a desire for complementary medicines, counselling, out-of-hours support, continuity of care with the same healthcare providers, and involvement in clinical trials in addition to their existing cancer treatment.42
Treatment Location
In general, BC patients preferred a treatment that could be administered as an outpatient, whereas patients with eBC were less likely to prefer chemotherapy due to the burden of frequent hospital visits.41,47 In one study, a significant number of patients expressed a preference for receiving SC chemotherapy in the comfort of their homes, while patients who preferred having treatment at the hospital or clinic enjoyed being in the company of other women and exchanging experiences.33 In another study, however, women with mBC preferred the convenience and privacy of home administration of oral treatment to IV infusion in a clinic setting.37
Accessibility and Availability of Treatment
Research has highlighted the role of travel distance in predicting surgical choice. Women living in rural and remote areas may opt for mastectomy over BSC to avoid subsequent radiation therapy due to the greater distances travelled for radiation treatment.30 Moreover, logistical issues, such as distance to care and transportation, had been identified as significant barriers to treatment access and uptake, particularly for patients residing in rural areas or reliant on others for transportation. Such patients tend to refuse treatment, citing difficulties in accessing care.32 Notably, patients expressed a desire for reduced waiting times for treatment and an improved gap in the delay between diagnosis and treatment commencement. Additionally, they emphasized the importance of having a choice of their preferred physicians, reflecting their desire for greater autonomy in treatment decision-making.42
Physician’s Recommendation
Physicians’ recommendations have been found to play a vital role in shaping patients’ treatment decision-making and preferences. Patients have expressed that a clear and definitive recommendation from their healthcare provider would significantly impact their decision to accept or reject a particular treatment.31,41 Nevertheless, shared decision-making between patients and physicians was also found to be the preferred approach by most patients, where they valued the expertise of physicians and would collaboratively work with their physicians in selecting the treatment that aligns with patient care goals.30–32 This trust is reflected in statements such as, “They’re the experts and I’m not, so their training and everything should be what would lead me to go in a certain direction”.32
Treatment-Related Risks
Treatment-Related Side Effects and Safety
A central theme that emerged from the literature is the paramount importance of considering the treatment-related side effects and safety of the available treatment options. For instance, patients may refuse chemotherapy due to the side effect and its adverse impact on health.31 Patients, irrespective of whether they were in the early or advanced stages of BC, expressed significant concerns about the potential toxicity and long-term safety of a treatment or surgery as major considerations.32,35,39 Notably, younger and older patients had distinct concerns regarding the potential side effects of chemotherapy, highlighting the need for a nuanced approach to treatment decision-making that accounts for the diverse needs and preferences of the patient population.41 Besides, patients’ preference for continuing hormonal therapy appeared to be closely linked to the severity of associated side effects and the flexibility to stop treatment in case of severe side effects.40,41
Treatment-Related Secondary Cancer and/or the Need for Additional Therapy
Among those who underwent radiation therapy, the fear of developing treatment-related secondary cancer was a pervasive concern, compounded by the anxiety associated with the radiation itself. Women who had young children or acted as caregivers to their partners declined radiation or further therapy due to the need to be concomitantly away from home to receive treatment.30 Patients on different anticancer therapy were constantly troubled by the fear and uncertainties of cancer metastases or treatment-related secondary cancer that would expose them to the need for additional therapy.35 Notably, women tend to consider the small risk of developing endometrial cancer (5 out of 1000) to be almost as significant as the substantially higher benefit of hormonal therapy’s efficacy (5 out of 10).49 In contrast, women in the Netherlands assigned less importance on the future risk of a secondary BC compared to the risk of surgery.36
Alopecia
BC patients undergoing chemotherapy often reported alopecia as the most distressing and most desired to be avoided side effects.29,47 Among those receiving taxane-based chemotherapy, madarosis had been shown to significantly impact their daily lives. Interestingly, the severity and timing of regrowth for both eyebrows and eyelashes appeared to vary widely among patients, with several women also experiencing dry and irritated eyes leading to increased tearing as a physiological side effect of madarosis.34 A conjoint analysis revealed that the relative importance of alopecia was ranked second just behind the survival benefit when considering treatment preference.39
Lethargy/Fatigue and Sleep Disturbances
Fatigue and sleep disturbances are common side effects of BC treatment that can significantly impact a patient’s daily life and overall well-being. In fact, lethargy and difficulty sleeping were ranked among the most troublesome concerns reported by women undergoing chemotherapy.29,47 In hypothetical treatment preference analysis, it was observed that women tend to avoid treatments that have the potential to induce fatigue as a side effect.39 Additionally, while sleep disturbances were ranked lower in terms of distress compared to fatigue or weariness, they remained an important consideration among Japanese patients.47
Quality of Life
Ability to Maintain Daily Activities, Work, and Home Duties
BC patients faced a complex decision-making process when considering their treatment options, as their preferences were often influenced by a range of factors related to their quality of life (QoL), ability to maintain daily activities, and fulfil their work and home duties.29,40,47,48 These concerns were often rooted in a desire to maintain independence and continue living life as fully as possible, despite the challenges posed by their illness. For some patients, chemotherapy could be a source of significant anxiety, as they worried about the impact it might have on their QoL and ability to perform activities of daily living, such as grocery shopping and household tasks.31 Others expressed concerns about the impact of treatment on their ability to pursue hobbies, spend time with loved ones, attend life events, social rehabilitation, and travel, all of which were deemed important for maintaining a sense of normalcy and emotional well-being.32,47 Older women with eBC, who may be more vulnerable to the physical and emotional toll of BC and its treatment, may be particularly concerned about the impact of surgery on maintaining their QoL, independence, and ability to perform daily activities.35,41
Emotional/Mental Health
BC patients’ emotional and mental health can be severely impacted by anticancer treatment, causing a range of emotional struggles such as fear, worry, stress, and anxiety.39 Some of these emotions might be related to specific aspects of treatment, such as fear of radiation or surgery, while others described an overall depressed moods and anxiety related to the uncertainty of treatment responses and future outcomes.30,47 It was evident that patients who experienced better well-being during adjuvant systemic therapy were more inclined to accept that particular treatment.33 The effects of BC treatment, such as madarosis, could cause a profound sense of emotional distress, disconnection from one’s appearance, and discomfort in social situations. Patients reported withdrawing from public places and refrain social interactions to avoid being judged by others.34 Patients receiving IV chemotherapy had reported anxiety related to the pain, side effects, and complications associated with the IV line.37,38
Burden to Family/Partner/Caregiver
BC not only takes a toll on the physical health of patients but also exerts a significant psychosocial impact on their relationships with family members, partners, and caregivers.29 The extent of this impact and its influence on treatment preferences has been found to vary among studies. In some cases, patients may opt out of treatment altogether as they do not want to burden their loved ones with the added stress of caring for them.32 Furthermore, BC patients may experience anxieties about the potential ramifications of their illness on their relationships with partners and friends, adding to their already substantial emotional burden.47
Cost of Treatment
BC patients face a significant financial burden associated with the cost of cancer treatment. This burden is particularly pronounced in the context of radiation therapy, which entails a prolonged stay away from home, the hiring of caregivers to tend to family needs and additional transportation costs for those residing in remote areas.30 According to the study conducted by Lawhon et al, older women with eBC exhibited differing levels of concern regarding the cost of treatment, with over a quarter of women stated that cost was not their primary consideration when making decisions about their treatment.32 Willingness to pay (WTP) for treatment varies significantly across patients, with higher household income being associated with greater WTP and patients with higher financial burden elicited a lower WTP, respectively, for a treatment that would restore them to their pre-cancer health status. Notably, patients with brain metastases were willing to pay substantially more for treatment than those with bone metastases.45 However, patients prioritized treatment effectiveness over cost when making treatment decisions, indicating that out-of-pocket costs may not be the sole factor affecting their treatment decisions. The majority of patients, especially those with mBC, voiced a desire for financial support options and less expensive treatments.39,42,47 The financial burdens arising from BC treatment had led to alterations in treatment decisions and even the postponement of treatment for non-cancer-related health issues, mainly due to the high out-of-pocket expenses involved. Nevertheless, despite the high financial burden experienced by some patients, Irwin et al found that the majority of patients did not perceive non-out-of-pocket costs, such as costs to insurance companies or society, as significantly impacting their medical decisions. Most patients indicated a willingness to accept generic drug substitutions in order to mitigate costs.43
Discussion
BC remains a major public health concern, and treatment modalities have evolved considerably in recent years. However, patients’ preferences for BC treatments are not always fully considered in the development and implementation of these treatment advancements. The evidence pooled across studies in this review highlights the important determinants of cancer treatment that matter to BC patients, as well as the existence of significant unmet needs among them.
BC treatment involves a delicate balance between achieving optimal outcomes while minimizing the risks, side effects, and safety concerns that patients may have. In this study, alopecia and madarosis have emerged as profoundly distressing adverse effects of BC treatment. These adverse effects have consistently ranked high on the lists of most challenging concerns from the patient’s perspective for the past four decades.50–52 Considerably varying preferences towards the benefits and risks of treatment were observed among individual patients. Interestingly, our review revealed that some patients demonstrated a willingness to undergo treatments that conferred relatively small survival benefits, but with significant risk or toxicity.39–41 Several factors could account for these inconsistent results. Firstly, inadequate patient awareness regarding the treatment’s benefit-to-risk ratio could be a plausible explanation. Secondly, patients might encounter difficulty comprehending the statistical data presented to them. Lastly, the fear of developing secondary cancer due to the treatment could have influenced their capacity to make well-informed and rational decisions. Even with the observed intra-patient variation, it was evident that patients’ perspectives on BC treatment for all stages of cancer differed significantly from those of healthy individuals or their healthcare providers.30,40,44,47 For instance, patients who were treated with aromatase inhibitors therapy demonstrated a willingness to continue the treatment even for marginal treatment benefits, a threshold lower than what physicians typically prefer for prescribing beyond the 5-year mark.40 In addition, Sakai et al reported that patients, nurses, and physicians exhibited distinct priorities when it came to the severity of treatment-related side effects.47
The QoL of BC patients, especially older women, is notably affected by the treatment they receive. Such treatment has a profound impact on their ability to perform daily activities, fulfil work and home duties, maintain their emotional and mental well-being, and manage their relationships with loved ones and caregivers. The emotional distress stemming from BC treatment may lead to withdrawal from public places and social interactions, particularly in cases where treatment side effects lead to changes in appearance. Likewise, a recent survey of Australian women with BC diagnosis highlighted the significance of body image or sexuality in association with a patient’s emotional and psychosocial well-being.53 BC can also take a toll on patients’ relationships with family members, partners, and caregivers, affecting their psychosocial well-being. The extent of this impact and its influence on treatment preferences varies among studies, with some patients even opting out of treatment entirely to avoid burdening their loved ones. In recent years, there has been a growing awareness of the importance of addressing the mental, emotional, and psychosocial well-being associated with BC treatment, particularly as advancements have made the physical side effects more manageable.54,55 Incorporating a focus on these non-physical mental and emotional health issues into clinical practice is crucial in enhancing the overall QoL of BC patients. By doing so, patients may be more inclined to adhere with their treatment, leading to improved treatment outcomes and an overall health related QoL.
The findings in this review suggest that prolonged treatment duration, especially for chemotherapy or radiotherapy, can have a considerable impact on patient’s daily lives. Nevertheless, it is noteworthy that both conjoint analysis studies in the review identified treatment duration as the least significant factor influencing patients’ treatment preferences.39,49 This implies that while treatment duration and other attributes are relevant, they have a less significant impact on patients’ treatment decisions compared to other treatment attributes. Some patients discussed facing challenges in accessing and availing treatment due to a range of factors, including travel distance, local clinic availability, transportation, and long waiting times for diagnosis and treatment, all of which can significantly impact treatment decision-making. Addressing these challenges may help reduce disparities in BC outcomes, particularly for patients living in rural and remote areas. Moreover, targeted interventions aimed at enhancing the patient experience and reducing waiting times can contribute to improved treatment uptake and better clinical outcomes.56,57
Physicians’ recommendations play a crucial role in shaping patients’ treatment decision-making and preferences, and their guidance and recommendations can have a profound impact on treatment outcomes, as patients value the expertise of physicians and trust that their training and knowledge will guide them toward the right treatment option. However, participants also expressed a desire to be more involved in decision-making, where they collaboratively work with their physicians in selecting the treatment that aligns with their treatment goals. The shared decision-making approach acknowledges patients’ autonomy and their entitlement to participate in the treatment decision-making process.32,58 Although patients prioritize treatment effectiveness over cost when making treatment decisions, the financial toxicity associated with BC treatment remains a substantial concern for many patients.59 A significant proportion of patients reported experiencing financial toxicities as a direct result of their BC treatment, with these financial burdens often causing them to alter their treatment decisions or forgo treatment for non-cancer-related health issues due to the high out-of-pocket expenses. BC was found to impose a greater financial burden than other cancers, as evidenced by substantially higher out-of-pocket costs compared to the combined out-of-pocket costs for colorectal, lung, and prostate cancers.60 Healthcare policy makers shall ensure that necessary measures are taken to implement policies aimed at alleviating the financial burden of both medical and non-medical expenses, thus enhancing the financial well-being of vulnerable patients with BC.
While we came across three systematic review studies61–63 that examined treatment decision-making in patients with BC, they did not meet our inclusion criteria. These studies, however, revealed that patients’ treatment preferences were influenced by various factors, including treatment benefits (such as survival, life expectancy, and probability of cure), treatment risks (including side effects, toxicity, risk of recurrence, and progression), QoL, treatment availability and accessibility, social support, surgeon’s recommendation, treatment cost, and the desire for no additional therapy beyond surgery. Interestingly, these findings align with the results of our own review. In contrast to the systematic review studies mentioned, our review introduces a novel perspective and demonstrates increased comprehensiveness. Our analysis encompasses all stages of BC and the broader landscape of BC treatment, distinguishing it from existing studies that exclusively concentrate on patient preferences in eBC61,62 or on the treatment decision-making of patients with ductal carcinoma in situ.63
This paper employed a narrative review method to examine the important determinants in BC treatment that matter to patients. Narrative reviews have been frequently criticized for their lack of systematicity and explicitness compared to other review methods. However, they offer great flexibility as they can accommodate a vast array of evidence, such as qualitative and quantitative data, research, and non-research sources, without merging findings or creating new theories. Despite the limitations, narrative reviews continue to be useful in policy and management, particularly when time is scarce. Since narrative reviews do not require complex data transformation, they can provide a comprehensive and inclusive analysis.26 Nevertheless, there are several limitations of our review that should be noted. We did not conduct a quality appraisal, which might limit the uptake and relevance of the scoping study.21 However, Arksey and O’Malley20 state that quality assessment is not a standard component of a scoping review. Some articles included in this review had limited details, leaving the review team to exercise their own reflexivity in content extraction, which may lead to incorrect interpretation of the results. Since the purpose of this review was to identify the important determinants of BC treatment from patient’s perspective, formal statistical meta-analysis would have been inappropriate.22,23 Nevertheless, this review provides an overview of the patient’s values and preferences concerning BC treatment, which allows for a detailed exploration of patients’ experiences and perspectives, whilst also providing a rich data source to inform future studies and interventions focused on patient-centered care.
Conclusion
In conclusion, BC patients reported a wide array of preferences regarding the important determinants of cancer treatment. Among 5 overarching themes identified, treatment benefits emerged as the most frequently cited theme, with treatment-related process, treatment-related risk, quality of life, and cost of treatment following in sequence. This literature review emphasizes the importance of considering these key determinants when making treatment decisions for BC patients. Our findings serve as an initial contribution towards developing conceptual frameworks that underpin the important determinants of BC treatment. There is an urgent need for healthcare professionals to engage in effective communication with their patients and involve them in the treatment decision-making process to ensure that their preferences and values are considered. Moreover, the findings highlight the need for personalized medicine, patient decision aids, and tailored financial assistance programs to mitigate the financial toxicity of cancer treatment. To optimize patient outcomes, future research should focus on identifying effective strategies to tailor treatments that align with patients’ preferences.
Data Sharing Statement
The data supporting the findings of this literature review was obtained from the literature. It is available within the article and its Supplementary Information files.
Acknowledgments
We would like to thank the Health Research Council of New Zealand for the study grant.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the Health Research Council of New Zealand Health Delivery Research Activation grant.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Sung H, Ferlay J, Siegel RL., et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2021;71(3):209–249. doi:10.3322/caac.21660
2. Soerjomataram I, Bray F. Planning for tomorrow: global cancer incidence and the role of prevention 2020–2070. Nat Rev Clin Oncol. 2021;18(10):663–672. doi:10.1038/s41571-021-00514-z
3. Cardoso F, Harbeck N, Fallowfield L, Kyriakides S, Senkus E. Locally recurrent or metastatic breast cancer: ESMO clinical practice guidelines for diagnosis, treatment and follow-up. Ann Oncol. 2012;23:vii11–vii19. doi:10.1093/annonc/mds232
4. Riis M. Modern surgical treatment of breast cancer. Ann Med Surg. 2020;56:95–107. doi:10.1016/j.amsu.2020.06.016
5. Waks AG, Winer EP. Breast cancer treatment: a review. JAMA. 2019;321(3):288–300. doi:10.1001/jama.2018.19323
6. Haidinger R, Bauerfeind I. Long-term side effects of adjuvant therapy in primary breast cancer patients: results of a web-based survey. Breast Care. 2019;14(2):111–116. doi:10.1159/000497233
7. Senkus E, Kyriakides S, Ohno S, et al. Primary breast cancer: ESMO clinical practice guidelines for diagnosis, treatment and follow-up. Ann Oncol. 2015;26:v8–v30. doi:10.1093/annonc/mdv298
8. Network NCC. National Comprehensive Cancer Network (NCCN) clinical practice guidelines in oncology.
9. Harrison M, Milbers K, Hudson M, Bansback N. Do patients and health care providers have discordant preferences about which aspects of treatments matter most? Evidence from a systematic review of discrete choice experiments. BMJ open. 2017;7(5):e014719. doi:10.1136/bmjopen-2016-014719
10. Burstein H, Curigliano G, Thürlimann B, et al. Customizing local and systemic therapies for women with early breast cancer: the St. Gallen International Consensus Guidelines for treatment of early breast cancer 2021. Ann Oncol. 2021;32(10):1216–1235. doi:10.1016/j.annonc.2021.06.023
11. Cardoso F, Kyriakides S, Ohno S, et al. Early breast cancer: ESMO clinical practice guidelines for diagnosis, treatment and follow-up. Ann Oncol. 2019;30(8):1194–1220. doi:10.1093/annonc/mdz173
12. Cardoso F, Paluch-Shimon S, Senkus E, et al. 5th ESO-ESMO international consensus guidelines for advanced breast cancer (ABC 5). Ann Oncol. 2020;31(12):1623–1649. doi:10.1016/j.annonc.2020.09.010
13. Raphael D, Ter Stege J, Russell N, Boersma L, van der Weijden T. What do patients and health care professionals view as important attributes in radiotherapy decisions? Input for a breast cancer patient decision aid. Breast. 2020;49:149–156. doi:10.1016/j.breast.2019.11.005
14. Goel V, Sawka CA, Thiel EC, Gort EH, O’Connor AM. Randomized trial of a patient decision aid for choice of surgical treatment for breast cancer. Med Decis Making. 2001;21(1):1–6. doi:10.1177/0272989X0102100101
15. Diekmann A, Heuser C, Ernstmann N, et al. How do breast cancer patients experience multidisciplinary tumor conferences? - A description from the patient perspective. Breast. 2019;44:66–72. doi:10.1016/j.breast.2018.12.012
16. Mohammed K, Nolan MB, Rajjo T, et al. Creating a patient-centered health care delivery system: a systematic review of health care quality from the patient perspective. Am J Med Qual. 2016;31(1):12–21. doi:10.1177/1062860614545124
17. Higgins MJ, Kale N, Homsy C, et al. Patient perspective on post-breast reconstruction exercise and physical therapy. JPRAS Open. 2021;30:160–169. doi:10.1016/j.jpra.2021.09.002
18. Gupta S, Zhang J, Jerusalem G. The association of chemotherapy versus hormonal therapy and health outcomes among patients with hormone receptor-positive, HER2-negative metastatic breast cancer: experience from the patient perspective. Expert Rev Pharmacoecon Outcomes Res. 2014;14(6):929–940. doi:10.1586/14737167.2014.949243
19. García-Foncillas J, Antón-Torres A, Caballero-Martínez F, et al. Patient perspective on the management of cancer pain in Spain. J Patient Exp. 2020;7(6):1417–1424. doi:10.1177/2374373520978872
20. Arksey H, O’Malley L. Scoping studies: towards a methodological framework. Int J Soc Res Methodol. 2005;8(1):19–32. doi:10.1080/1364557032000119616
21. Levac D, Colquhoun H, O’Brien KK. Scoping studies: advancing the methodology. Implement Sci. 2010;5(1):69. doi:10.1186/1748-5908-5-69
22. Peters MD, Godfrey CM, Khalil H, McInerney P, Parker D, Soares CB. Guidance for conducting systematic scoping reviews. JBI Evid Implement. 2015;13(3):141–146.
23. Moher D, Stewart L, Shekelle P. All in the Family: systematic reviews, rapid reviews, scoping reviews, realist reviews, and more. Syst Rev. 2015;4(1):183. doi:10.1186/s13643-015-0163-7
24. Moher D, Liberati A, Tetzlaff J, Altman DG; PRISMA Group* t. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. Ann Intern Med. 2009;151(4):264–269. doi:10.7326/0003-4819-151-4-200908180-00135
25. Tricco AC, Langlois E, Straus SE; World Health Organization. Rapid Reviews to Strengthen Health Policy and Systems: A Practical Guide. World Health Organization; 2017.
26. Mays N, Pope C, Popay J. Systematically reviewing qualitative and quantitative evidence to inform management and policy-making in the health field. J Health Serv Res Policy. 2005;10(1_suppl):6–20. doi:10.1258/1355819054308576
27. Thomas J, Harden A. Methods for the thematic synthesis of qualitative research in systematic reviews. BMC Med Res Methodol. 2008;8(1):1–10. doi:10.1186/1471-2288-8-45
28. Neuendorf KA. The Content Analysis Guidebook. Sage; 2017.
29. Ataseven B, Frindte J, Harter P, et al. Perception of side effects associated with anticancer treatment in women with breast or ovarian cancer (KEM-GO-1): a prospective trial. Support Care Cancer. 2020;28(8):3605–3615. doi:10.1007/s00520-019-05216-y
30. Dicks E, Roome R, Chafe J, et al. Factors influencing surgical treatment decisions for breast cancer: a qualitative exploration of surgeon and patient perspectives. Curr Oncol. 2019;26(2):e216–e225. doi:10.3747/co.26.4305
31. Harder H, Ballinger R, Langridge C, Ring A, Fallowfield LJ. Adjuvant chemotherapy in elderly women with breast cancer: patients’ perspectives on information giving and decision making. Psycho-Oncology. 2013;22(12):2729–2735. doi:10.1002/pon.3338
32. Lawhon VM, England RE, Wallace AS, et al. ”It’s important to me”: a qualitative analysis on shared decision-making and patient preferences in older adults with early-stage breast cancer. Psycho oncology. 2021;30(2):167–175. doi:10.1002/pon.5545
33. Pivot X, Gligorov J, Müller V, et al. Patients’ preferences for subcutaneous trastuzumab versus conventional intravenous infusion for the adjuvant treatment of HER2-positive early breast cancer: final analysis of 488 patients in the international, randomized, two-cohort PrefHer study. Ann Oncol. 2014;25(10):1979–1987. doi:10.1093/annonc/mdu364
34. Smith K, Winstanley J, Boyle F, et al. Madarosis: a qualitative study to assess perceptions and experience of Australian patients with early breast cancer treated with taxane-based chemotherapy. Support Care Cancer. 2018;26(2):483–489. doi:10.1007/s00520-017-3852-z
35. Burton M, Kilner K, Wyld L, et al. Information needs and decision-making preferences of older women offered a choice between surgery and primary endocrine therapy for early breast cancer. Psycho-Oncology. 2017;26(12):2094–2100. doi:10.1002/pon.4429
36. Byng D, Retèl VP, Engelhardt EG, et al. Preferences of treatment strategies among women with low-risk DCIS and oncologists. Cancers. 2021;13(16):3962. doi:10.3390/cancers13163962
37. Ciruelos EM, Díaz MN, Isla MD, et al. Patient preference for oral chemotherapy in the treatment of metastatic breast and lung cancer. Eur J Cancer Care (Engl). 2019;28(6):e13164. doi:10.1111/ecc.13164
38. Ciruelos EM, Montaño A, Rodríguez CA, et al. Phase III study to evaluate patient’s preference of subcutaneous versus intravenous trastuzumab in HER2-positive metastatic breast cancer patients: results from the ChangHER study (GEICAM/2012-07). Eur J Cancer Care (Engl). 2020;29(4):e13253. doi:10.1111/ecc.13253
39. daCosta DiBonaventura M, Copher R, Basurto E, Faria C, Lorenzo R. Patient preferences and treatment adherence among women diagnosed with metastatic breast cancer. Am Health Drug Benefits. 2014;7(7):386–395.
40. Gandhi S, Towns K, Verma S. Patient and physician perceptions on continuing aromatase inhibitors beyond the 5-year mark. Breast J. 2011;17(6):620–629. doi:10.1111/j.1524-4741.2011.01153.x
41. Hamelinck VC, Bastiaannet E, Pieterse AH, et al. A prospective comparison of younger and older patients’ preferences for adjuvant chemotherapy and hormonal therapy in early breast cancer. Clin Breast Cancer. 2016;16(5):379–388. doi:10.1016/j.clbc.2016.04.001
42. Harding V, Afshar M, Krell J, Ramaswami R, Twelves CJ, Stebbing J. ‘Being there’ for women with metastatic breast cancer: a pan-European patient survey. Br J Cancer. 2013;109(6):1543–1548. doi:10.1038/bjc.2013.492
43. Irwin B, Kimmick G, Altomare I, et al. Patient experience and attitudes toward addressing the cost of breast cancer care. Oncologist. 2014;19(11):1135–1140. doi:10.1634/theoncologist.2014-0117
44. Mandelblatt JS, Sheppard VB, Hurria A, et al. Breast cancer adjuvant chemotherapy decisions in older women: the role of patient preference and interactions with physicians. J Clin Oncol. 2010;28(19):3146–3153. doi:10.1200/jco.2009.24.3295
45. Oh DY, Crawford B, Kim SB, et al. Evaluation of the willingness-to-pay for cancer treatment in Korean metastatic breast cancer patients: a multicenter, cross-sectional study. Asia Pac J Clin Oncol. 2012;8(3):282–291. doi:10.1111/j.1743-7563.2012.01546.x
46. Pivot X, Spano JP, Espie M, et al. Patients’ preference of trastuzumab administration (subcutaneous versus intravenous) in HER2-positive metastatic breast cancer: results of the randomised MetaspHer study. Eur J Cancer. 2017;82:230–236. doi:10.1016/j.ejca.2017.05.009
47. Sakai H, Umeda M, Okuyama H, Nakamura S. Differences in perception of breast cancer treatment between patients, physicians, and nurses and unmet information needs in Japan. Support Care Cancer. 2020;28(5):2331–2338. doi:10.1007/s00520-019-05029-z
48. Savard M-F, Alzahrani MJ, Saunders D, et al. Experiences and perceptions of older adults with lower-risk hormone receptor-positive breast cancer about adjuvant radiotherapy and endocrine therapy: a patient survey. Curr Oncol. 2021;28(6):5215–5226. doi:10.3390/curroncol28060436
49. Wouters H, Maatman GA, Van Dijk L, et al. Trade-off preferences regarding adjuvant endocrine therapy among women with estrogen receptor-positive breast cancer. Ann Oncol. 2013;24(9):2324–2329. doi:10.1093/annonc/mdt195
50. Coates A, Abraham S, Kaye SB, et al. On the receiving end—patient perception of the side-effects of cancer chemotherapy. Eur J Cancer Clin Oncol. 1983;19(2):203–208. doi:10.1016/0277-5379(83)90418-2
51. Freedman TG. Social and cultural dimensions of hair loss in women treated for breast cancer. Cancer Nurs. 1994;17(4):334–341. doi:10.1097/00002820-199408000-00006
52. Kocan S, Aktug C, Gursoy A. “Who am I?” A qualitative meta-synthesis of chemotherapy‐induced alopecia and body image perception in breast cancer patients. Support Care Cancer. 2023;31(4):237. doi:10.1007/s00520-023-07704-8
53. Ettridge K, Scharling-Gamba K, Miller C, Roder D, Prichard I. Body image and quality of life in women with breast cancer: appreciating the body and its functionality. Body Image. 2022;40:92–102. doi:10.1016/j.bodyim.2021.11.001
54. Hurtado-de-Mendoza A, Gonzales F, Song M, et al. Association between aspects of social support and health-related quality of life domains among African American and White breast cancer survivors. J Cancer Surviv. 2021:1–11. doi:10.1007/s11764-020-00906-7
55. Masoumi S, Amiri M, Afrashteh MY. Self-compassion: the factor that explains a relationship between perceived social support and emotional self-regulation in psychological well-being of breast cancer survivors. Iran J Psychiatry. 2022;17(3):341. doi:10.18502/ijps.v17i3.9734
56. Zipkin RJ, Schaefer A, Wang C, et al. Rural-urban differences in breast cancer surgical delays in Medicare beneficiaries. Ann Surg Oncol. 2022;29(9):5759–5769. doi:10.1245/s10434-022-11834-4
57. Babatunde OA, Eberth JM, Felder TM, et al. Racial disparities and diagnosis-to-treatment time among patients diagnosed with breast cancer in South Carolina. J Racial Ethn Health Disparities. 2021:1–11. doi:10.1007/s40615-020-00905-5
58. Kugbey N, Oppong Asante K, Meyer-Weitz A. Doctor–patient relationship mediates the effects of shared decision making on health-related quality of life among women living with breast cancer. S Afr J Psychol. 2019;49(3):364–375. doi:10.1177/0081246318801159
59. Ehsan AN, Wu CA, Minasian A, et al. Financial toxicity among patients with breast cancer worldwide: a systematic review and meta-analysis. JAMA Netw Open. 2023;6(2):e2255388–e2255388. doi:10.1001/jamanetworkopen.2022.55388
60. Longo CJ, Bereza BG. A comparative analysis of monthly out-of-pocket costs for patients with breast cancer as compared with other common cancers in Ontario, Canada. Curr Oncol. 2011;18(1):e1–8. doi:10.3747/co.v18i1.681
61. Minami CA, King TA, Mittendorf EA. Patient preferences for locoregional therapy in early-stage breast cancer. Breast Cancer Res Treat. 2020;183(2):291–309. doi:10.1007/s10549-020-05737-9
62. Hamelinck VC, Bastiaannet E, Pieterse AH, et al. Patients’ preferences for surgical and adjuvant systemic treatment in early breast cancer: a systematic review. Cancer Treat Rev. 2014;40(8):1005–1018. doi:10.1016/j.ctrv.2014.06.007
63. Rutherford C, Mercieca-Bebber R, Butow P, Wu JL, King MT. Treatment decision-making in ductal carcinoma in situ: a mixed methods systematic review of women’s experiences and information needs. Patient Educ Couns. 2017;100(9):1654–1666. doi:10.1016/j.pec.2017.04.009
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Exploring the Important Determinants Shaping Treatment Preferences: Qualitative Insights into Breast Cancer Patient Experiences and Perspectives in New Zealand
Yeo HY, Wong JHY, Chan SJ, Latu ATF, Han CH, Anwar M, Marra CA
Patient Preference and Adherence 2023, 17:3525-3537
Published Date: 22 December 2023