Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 21
Understanding Nebulizer Utilization by Patients and Healthcare Providers: A COPD Foundation Nebulizer Consortium Survey Study
Authors Melamed KH, Martinez S ![]() , Cambridge L, Christiani DC, Li J, Ohar J
, Cambridge L, Christiani DC, Li J, Ohar J ![]() , Dhand R
, Dhand R ![]() , Drummond MB
, Drummond MB ![]() , Ari A
, Ari A ![]() , Radonovich LJ Jr, Tashkin D
, Radonovich LJ Jr, Tashkin D ![]() , Dartt M, Perera A, Schloss J, Cochran L, Mannino D, Locantore N, Johnson K, Lacy MK
, Dartt M, Perera A, Schloss J, Cochran L, Mannino D, Locantore N, Johnson K, Lacy MK ![]() , Berlinski A, Gilchrist K, Barjaktarevic I
, Berlinski A, Gilchrist K, Barjaktarevic I ![]()
Received 11 July 2025
Accepted for publication 22 December 2025
Published 19 January 2026 Volume 2026:21 552041
DOI https://doi.org/10.2147/COPD.S552041
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Richard Russell
Kathryn H Melamed,1 Sergio Martinez,2 Lisa Cambridge,3 David C Christiani,4 Jie Li,5 Jill Ohar,6 Rajiv Dhand,7 M Bradley Drummond,8 Arzu Ari,9 Lewis J Radonovich Jr,10 Donald Tashkin,1 Matthew Dartt,1 Arshan Perera,11 Judy Schloss,12 Lauren Cochran,13 David Mannino,2 Nicholas Locantore,2 Karmon Johnson,14 Melinda K Lacy,13 Ariel Berlinski,15 Kim Gilchrist,16 Igor Barjaktarevic,1 Bonnie Truelsen,17 Rosina Ledermueller,18 Jason Suggett PhD, BPharm, MBA,19 Dom Coppolo MBA, RRT, FAARC, AE-C,20 Blake Burnette,21 Candice Clay PhD,22 Pranay P Patel,23 Kim Gilchrist MD,24 Phil Kuehl PhD,25 Donald Mahler MD,26 Akshay Sood MD, MPH,27 Sanjay Sethi MD,28 Brian Carlin MD,29 Isaac Biney MD30 On behalf of the COPD Foundation Nebulizer Consortium
1Division of Pulmonary & Critical Care Medicine, David Geffen School of Medicine at UCLA, Los Angeles, CA, USA; 2Research & Pulmonary Medicine, COPD Foundation Inc., Miami, FL, USA; 3Medical Science, PARI, Inc., Midlothian, VA, USA; 4Department of Environmental Health, Harvard TH Chan School of Public Health, Harvard Medical School, Cambridge, MA, USA; 5Department of Cardiopulmonary Sciences, Division of Respiratory Care, Rush University, Chicago, IL, USA; 6Division of Pulmonary, Critical Care, Allergy and Immunologic Diseases, Wake Forest University School of Medicine, Winston-Salem, NC, USA; 7Division of Pulmonary and Critical Care Medicine, Department of Medicine, The University of Tennessee Graduate School of Medicine, Knoxville, TN, USA; 8Division of Pulmonary Diseases and Critical Care Medicine, University of North Carolina at Chapel Hill, Chapel Hill, NC, USA; 9College of Health Professions, Texas State University, Round Rock, TX, USA; 10Biosecurity Programs, Blueprint Biosecurity, Washington, DC, USA; 11Medical Science, PARI Medical Holding GmbH, Starnberg, Germany; 12Respiratory Care, Monaghan Medical Corporation, Plattsburgh, NY, USA; 13Medical Affairs & Operations, Theravance Biopharma US, LLC, South San Francisco, CA, USA; 14Medical Affairs, Aerogen Ltd., Galway, Ireland; 15Division of Pediatric Pulmonary Disease, University of Arkansas for Medical Sciences, Little Rock, AR, USA; 16Medical Affairs, Viatris Inc., Canonsburg, PA, USA; 17COPD patient; 18PARI, Inc; 19Monaghan Medical Corp.; 20Monaghan Medical Corp.; 21Verona Pharma; 22Verona Pharma; 23Viatris Inc.; 24Viatris Inc.; 25Lovelace Biomedical; 26Geisel School of Medicine at Dartmouth, Hanover, New Hampshire & Valley Regional Hospital in Claremont, New Hampshire, US; 27Division of Pulmonary, Critical Care and Sleep Medicine at University of New Mexico School of Medicine; 28Deputy Director of Clinical and Translational Sciences Institute (CTSI) at University Buffalo, State University of New York; 29UPMC Altoona Regional Medical Center; 30University of Tennessee Medical Center
Correspondence: Igor Barjaktarevic, Division of Pulmonary & Critical Care Medicine, David Geffen School of Medicine at UCLA, Los Angeles, CA, USA, Email [email protected]
Rationale: Inhaled medications are the mainstay of chronic obstructive pulmonary disease (COPD) management. While consensus guidelines for pharmacological management in COPD are well-established, few guidelines exist regarding inhaled medication delivery systems. The COPD Foundation Nebulizer Consortium conducted a cross-sectional survey of patients with COPD and healthcare providers to understand their perceptions and utilization of nebulized medications.
Methods: An online survey was conducted from February 7 through April 9, 2024. Patients completed a 42-question survey, including demographic information, tobacco use, symptoms severity, and the role of nebulizers in their treatment. Healthcare providers responded to a 17-question survey about their clinical experience with nebulized medications.
Results: We analyzed responses from 347 patients and 39 healthcare providers. Among patients, 76.4% (265/347) were ≥ 65 years old, 72.0% (250/347) were female, 93.4% (324/347) were white, 90.5% (314/347) had a current or former smoking history, 77.6% (263/339) reported at least one exacerbation in the past year, and 70.8% (240/339) used some form of supplemental oxygen. Nebulizer use was reported by 84.1% (292/347) of patients. Among nebulizer users, 94.5% (276/292) used short-acting while only 22.3% (65/292) used long-acting nebulized medications. Patients reported that hand-held inhaler devices were easier to use (69.8%, 171/245), but nebulized therapy led to better symptom control (64.9%, 159/245) and had lower copays (67.8%, 166/245). Among prescribers surveyed, most (82.1%, 32/39) believed nebulizers were preferable for patients experiencing exacerbations. Impediments to wider use of nebulizers included difficulties with insurance coverage (69.2%, 27/39), cost (53.8%, 21/39), and lack of combination nebulized drugs (46.2%, 18/39). Two-thirds of providers thought that nebulizers were underused.
Conclusion: We demonstrate that while patients and providers both perceive nebulizers as preferred in clinical management of COPD, there is discordance between patient and provider perception of nebulizer use on the basis of cost and feasibility of use.
Keywords: chronic obstructive pulmonary disease, COPD exacerbation, nebulizer, nebulized medication
Introduction
Inhaled medications are the mainstay of chronic obstructive pulmonary disease (COPD) management.1–3 While consensus guidelines for pharmacological management in COPD are well-established, few guidelines exist regarding inhaled medication delivery systems.1–3 Over time, the number and mode of delivery of inhaled medications have increased, now including short and long acting muscarinic antagonists as well as inhaled corticosteroids, offered alone in inhaler or nebulizer formulation or in a variety of combinations via held-held inhalers.4–9 The four most commonly used delivery devices are metered-dose inhalers (MDI), dry powder inhalers (DPI), soft mist inhalers (SMI), and small volume nebulizers (SVN).4 Together, MDI, DPI, and SMI will herein be referred to as “hand-held inhalers” and are discussed in comparison to all types of SVNs, which include standard jet, vibrating mesh, breath-enhanced, breath-actuated, and ultrasonic nebulizers.
Overall, studies on inhaled medication delivery systems for COPD management have generally been equivocal, showing no consistent data to support the use of one delivery system over another.1,10–13 Prior work has evaluated both patient and provider perspectives on COPD management and inhalation delivery device selection. Patients and providers alike were more knowledgeable about, and paid most attention to, the pharmacologic class of medication, rather than the delivery system.14 Most patients were prescribed hand-held inhaler devices rather than nebulizers for delivery of both rescue and maintenance medication.15,16 Providers generally perceived SVNs to be superior to hand-held inhalers for treatment of a COPD exacerbation, and slightly more than half of patients who had used both types of devices preferred their nebulizer when compared to their hand-held inhalers.15,16
During the COVID-19 pandemic, healthcare institutions and practitioners expressed concerns about infection risk and spread of respiratory viruses with the use of nebulizers, which resulted in further evaluation of nebulization therapy.1 The COPD Foundation Nebulizer Consortium (CNC), a panel of subject matter experts, recently published their findings.17 In summary, the CNC concluded that adherence to recommended safety measures should be emphasized and nebulizer use should not be discouraged when clinically indicated.17 Further work showed that use of a breath-actuated nebulizer with a filtered mouthpiece did not lead to increased dispersion of SARS-CoV-2 RNA compared with an MDI in patients with COVID-19 infection.18
In part due to the COVID-19 pandemic, the CNC has worked to better understand the hesitancy about the use of nebulizers. Medication delivery remains predominantly via MDIs and DPIs with a significant shift away from SVNs as a delivery method.15,16 Meanwhile, new respiratory therapies have been approved via a nebulized delivery method, and updated nebulizer delivery systems, such as vibrating mesh nebulizers, have become commercially available.5,8,19–22
Post-pandemic, we sought to re-evaluate the current state of nebulizer prescribing and utilization patterns. The CNC conducted a cross-sectional survey of patients with COPD and healthcare providers to better understand their perception of nebulizers and their utilization in clinical practice.
Methods
Survey Development
The CNC designed and distributed a survey to patients and healthcare providers regarding nebulizer use for the treatment of COPD. The patient section of this survey was reviewed by patients who were on the CNC. Those questions were written using fifth grade level English, and critical sections like questions about their medications included images of the medicine brand and labeling to facilitate selection. The healthcare provider section was written using college level English and included medical terms.
Survey Format and Administration
The CNC online survey was deemed IRB Exempt under 45 CFR § 46.104(d)(2) by the Western Institutional Review Board (WCG IRB, Puyallup, WA, USA), because this research study only involves a survey and data collection maintained the privacy of its subjects in compliance with the Declaration of Helsinki. Participation was voluntary, and the following language was present on the introduction page of the survey and served as the consent process:
The following short survey is designed to better understand the use of nebulized drugs in COPD. Your responses are completely anonymous and will not be linked back to you. By completing the survey, you acknowledge that the COPD Foundation has your consent to analyze the anonymous responses (data). Your participation in the survey is completely voluntary, and you are not required to share any information that could identify you.
The survey was conducted from February 7 through April 9, 2024.
Participants included adult patients with COPD who resided in the United States and its Territories and healthcare providers recruited through the COPD Foundation’s online patient platform, newsletters, and social media channels, and healthcare providers were recruited via COPD Foundation and the CNC provider network. There was no financial incentive for participation. Patients were included if they confirmed they had a diagnosis of COPD, were 18 years of age or older, and lived in the United States. Healthcare providers, such as pulmonologists, primary care practitioners, nurse practitioners and physician assistants were among the respondents asked whether they prescribed nebulizers. Those who prescribed nebulizers and confirmed that they practiced in the United States were asked to complete the rest of the survey.
Survey Content
Patients completed a 42-question survey (Supplemental Figure 1), including demographic information, smoking status and lifetime cumulative amount in pack-years, and history of lung disease. Specifically, they described their tobacco, marijuana, and vaping use currently and historically. They also described their current level of daily activities, symptoms, and number of COPD exacerbations per year. The final section of the survey included questions about oxygen use, corticosteroid use for exacerbations, and the role of nebulized medication and delivery devices in their treatment regimen.
Healthcare providers were asked 17 questions (Supplemental Figure 2) about their prescribing experience regarding nebulizers, selected nebulized medications, hand-held inhalers, reasons for selection of medications, and patient characteristics considered when selecting nebulizer devices and medications.
Data Analysis
Data was collected via Survey Monkey [SurveyMonkey Inc.; San Mateo, California, USA; www.surveymonkey.com] using the platform’s software. Due to the nature of survey distribution, no formal sample size calculations for this convenience sample were able to be performed. Descriptive analyses of the survey results are provided for both patient and healthcare provider surveys. Comparisons between groups for hand-held inhaler and nebulizer preferences were done using a Chi-square test or Fisher’s Exact Test where appropriate. Analyses were conducted using SAS Version 9.4 (SAS Institute, Cary, NC, USA).
Results
We analyzed 347 responses from patients and 39 responses from healthcare providers who met the inclusion criteria. Response rate is not known given that the survey was distributed to an unknown number of participants via the listed online platforms.
Patient Characteristics
Patient characteristics are shown in Table 1. Notably, 76.4% (265/347) were ≥65 years old, 72.0% (250/347) were female, 93.4% (324/347) were white. Survey participants reported using a variety of health insurances including private insurance (17.3%, 60/347), Medicare (55.0%, 191/347), and Medicaid (10.4%, 36/347), and they spanned socioeconomic groups with 40.3% (140/347) reporting total household incomes of less than $40,000 per year. Most of the patients surveyed (80.7%, 280/347) had a pulmonologist involved in their respiratory-related care.
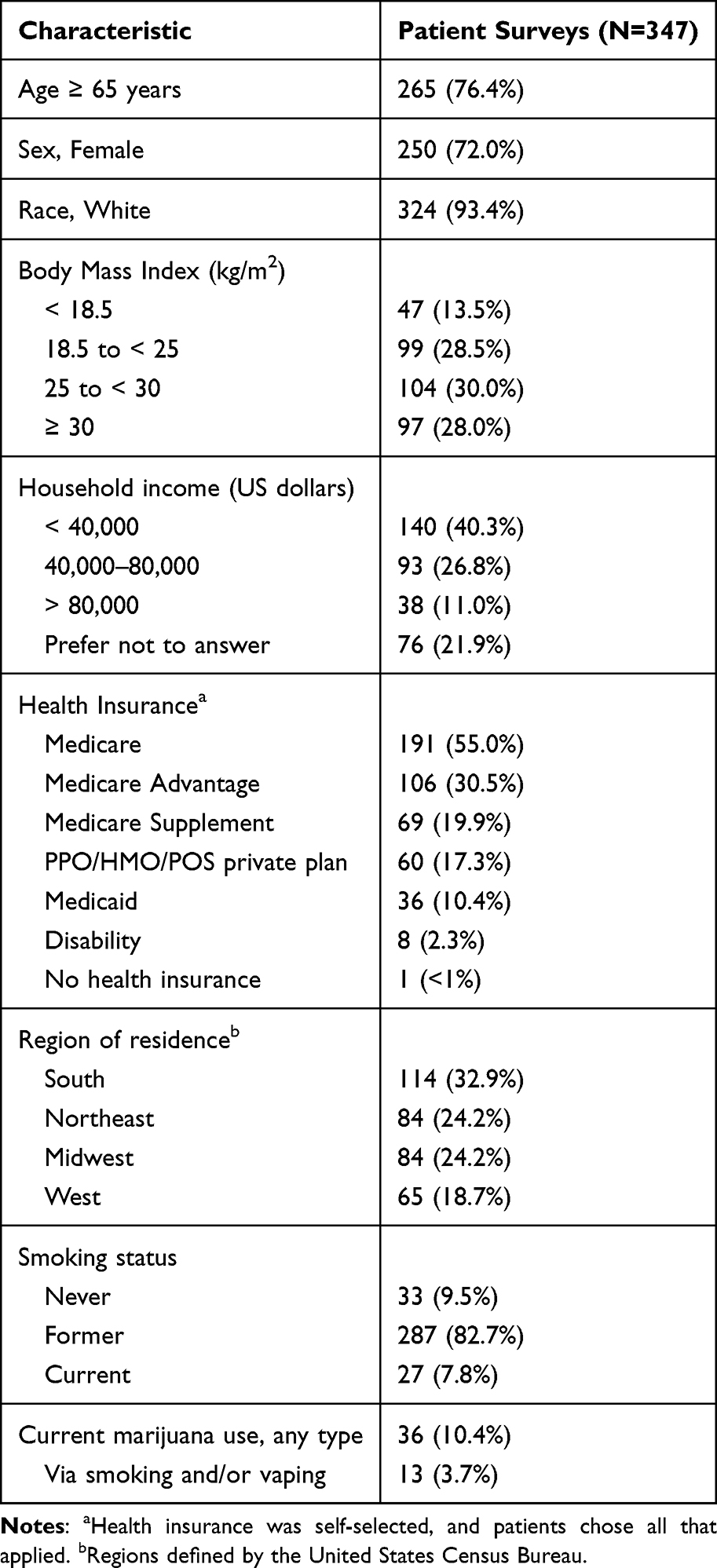 |
Table 1 Patient Characteristics |
Most patients (82.7%, 287/347) were former tobacco smokers, only 7.8% (27/347) were currently smoking, and 9.5% (33/347) were never-smokers (Table 1). Among current and former smokers, median [inter-quartile range (IQR)] pack-year history was 49 [35–80]. Only 10.4% (36/347) of patients reported any marijuana use. Among marijuana users, 31.6% (11/36) used marijuana on a daily basis, with less than half using it in an inhaled form (31.6% or 11/36 smoking and 5.6% or 2/36 vaping).
Patient COPD Disease Severity
Survey participants generally had moderate to severe COPD based on symptoms, exacerbation history, medications, and oxygen use (Table 2). Most patients (96.5%, 327/339) experienced some degree of daily symptoms, indicated by modified Medical Research Council (mMRC) dyspnea score of 1 or more, with 21.5% (73/339) being too short of breath to leave the house (as indicated by a modified Medical Research Council score of 4) and 70.8% (240/339) using supplemental oxygen. The majority (77.6%, 263/339) reported at least one exacerbation that required steroids and/or antibiotics in the past year.
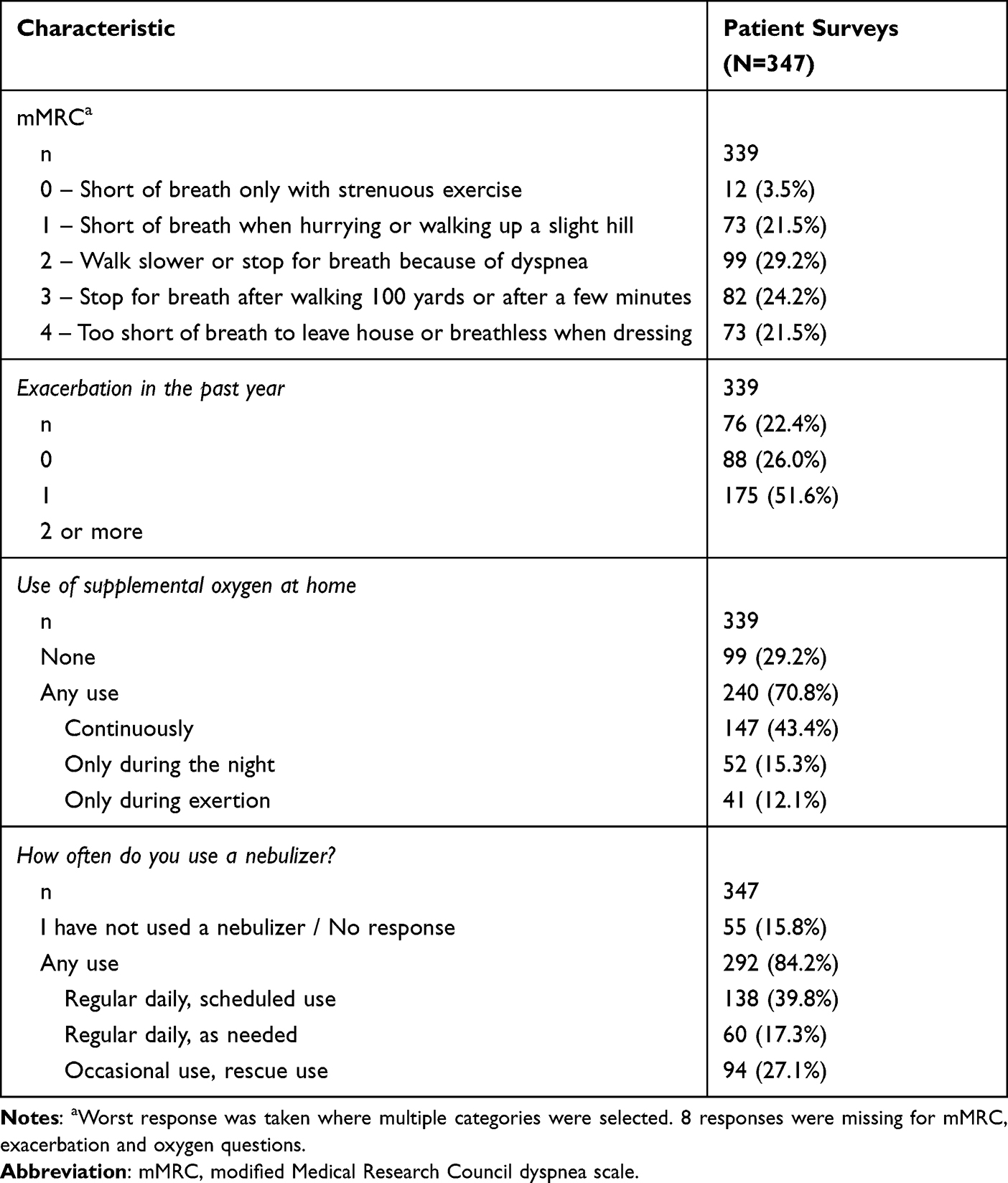 |
Table 2 Patient Clinical Characteristics |
Patient-Reported Nebulizer Use
The majority of surveyed patients (84.2%, 292/347) had used nebulizers in the past, with 57.1% (198/347) reporting daily use (Table 2). Jet nebulizers as a category include standard (or continuously operated) models, as well as more advanced types such as breath-enhanced and breath-actuated jet nebulizers. Among nebulizer users, standard jet (36.6%, 107/292) and breath-enhanced nebulizers (29.8%, 87/292) were used more frequently compared to breath-actuated (16.1%, 47/292), vibrating mesh (13.7%, 40/292), and ultrasonic (13.0%, 38/292) nebulizers. Nebulizers were initially prescribed most often by the patient’s pulmonologist (53.4%, 156/292), followed by the primary care doctors (20.6%, 60/292). The most common reason patients reported for receiving nebulized therapy included worsening symptoms (40.4%, 118/292) or because other inhaler devices did not work well enough (21.9%, 64/292) (Table 3).
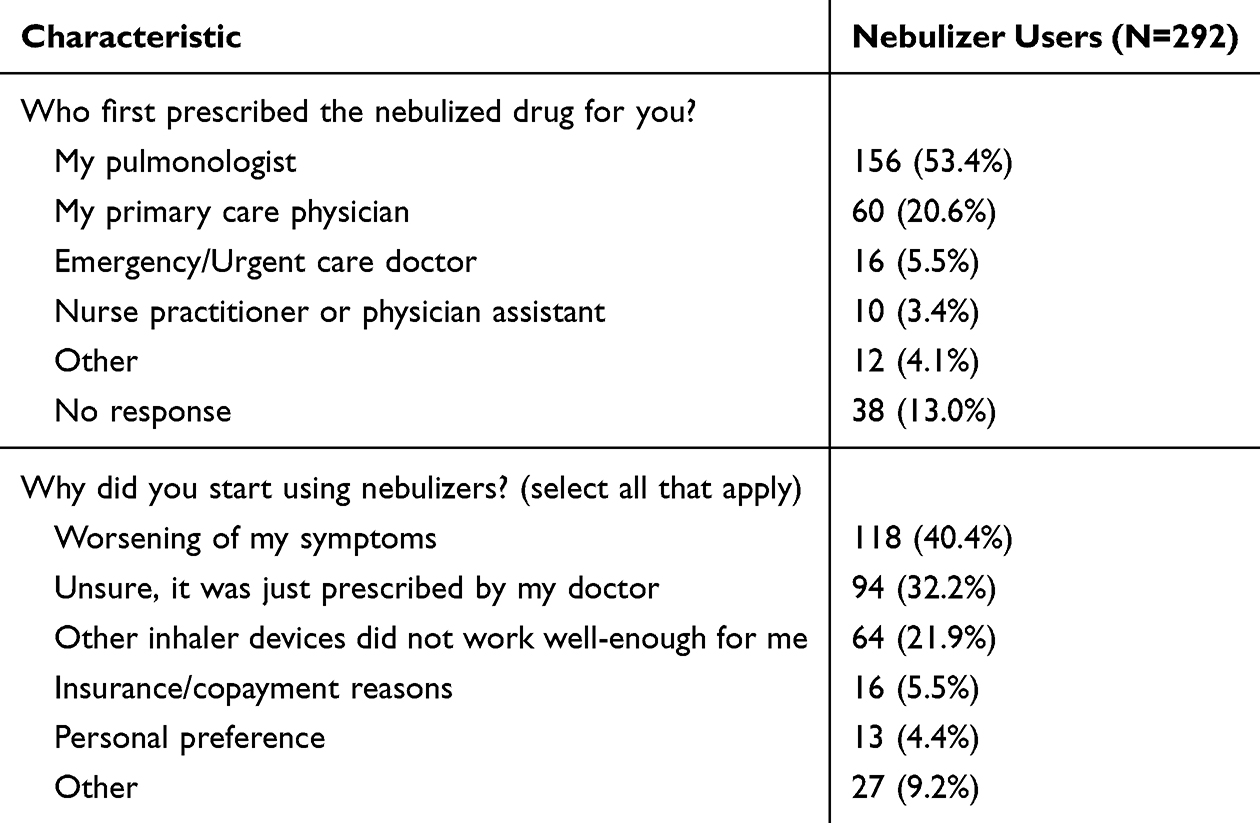 |
Table 3 Nebulizer User Characteristics |
Among patients who reported using nebulizers, most (94.5%, 276/292) used nebulized short-acting bronchodilators, which included beta agonists (63.0%, 184/292), muscarinic antagonists (8.6%, 25/292), or a combination of both (18.2%, 53/292). Only 22.3% (65/292) used one or more long-acting nebulized medications, inhaled corticosteroid most frequently (16.8%, 49/292) followed by long-acting beta agonists (11.0%, 32/292) and long-acting muscarinic antagonists (8.9%, 26/292). Aside from inhaled steroids or bronchodilators, 10.3% (30/292) used other nebulized medications such as hypertonic saline, N-acetylcysteine, or inhaled antibiotics.
Of the 292 patients who use nebulizers, 254 responded to the nebulizer training question, and of those 21.6% (55/254) reported that no teaching about the use of nebulizers was provided by the prescribing team, and another 24.8% (63/254) stated that teaching, when provided, was perceived to be insufficient. In comparison, teaching about the use of hand-held devices was missing or insufficient in 16.1% (41/254) and 22.4% (57/254) of cases, respectively.
245 patients responded to the nebulizer preference questions. Compared to hand-held inhaler devices, surveyed participants reported that nebulized therapy had lower co-pay (67.8%, 166/245) and led to better COPD symptom control (64.9%, 159/245), particularly during an exacerbation (71.0%, 174/245). However, hand-held inhaler devices were perceived as easier to use compared to nebulizers (69.8%, 171/245), and easier to maintain (71.0%, 174/245) (Figure 1). When divided by patient characteristic, patients who were 65 years or older more often found that nebulizers resulted in better daily symptom control compared to younger patients (60% vs 44%, p = 0.0353), whereas those who used oxygen or had one or more exacerbation more often preferred nebulizers during an flare up of symptoms (76% vs 56% p = 0.0017 and 75% vs 54% p = 0.0057 respectively) (Table 4).
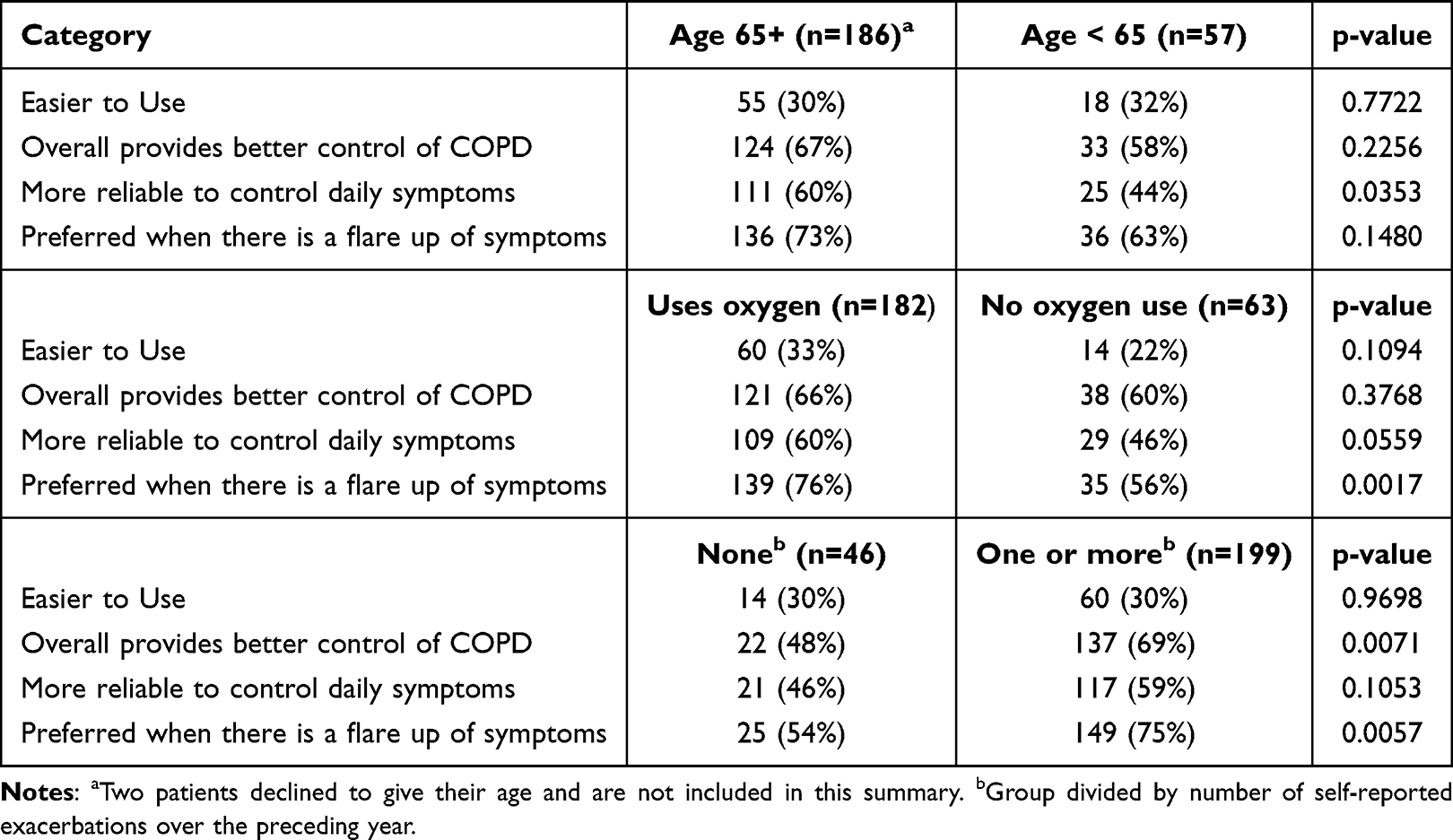 |
Table 4 Summary of Preference for Nebulizer Over Hand-Held Inhaler by Patient Demographic Splits |
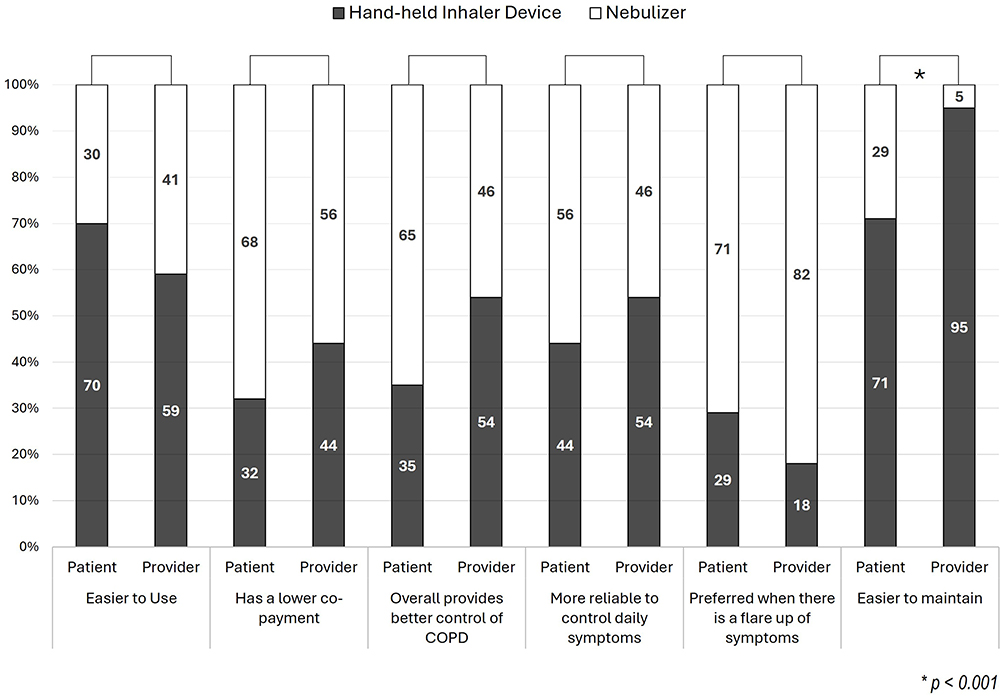 |
Figure 1 Patient and provider perception of hand-held inhaler devices versus nebulizers. |
Regarding the impact of the recent COVID-19 pandemic on the utilization of nebulized drugs, the majority (55.5%, 141/254) reported never having had a COVID-19 infection. Of the 109 patients who reported having COVID-19, 21.1% (23/109) reported being hospitalized, including three who reported being placed on a ventilator for COVID-19 pneumonia during the pandemic. A COVID-19 diagnosis did not change home nebulizer use for most patients (75.2%, 82/109), although 5.5% (6/109) decreased use or changed from using nebulizers.
Provider Responses
Of the 113 healthcare providers who initiated the survey, 55 did not prescribe nebulizers and 19 did not practice in the United States, leaving 39 that met our inclusion criteria. Of these 39 providers, 84.6% (33/39) were pulmonologists. Most providers prescribed jet nebulizers (89.7%, 35/39), followed by ultrasonic (28.2%, 11/39) and vibrating mesh nebulizers (20.5%, 8/39). A majority of prescribers (71.8%, 28/39) indicated that more than 75% of patients for whom they prescribed nebulizers used short-acting bronchodilators, whereas most indicated that long-acting bronchodilators or inhaled corticosteroids were used in less than 20% of their patients (61.5% or 24/39 and 53.8% or 21/39, respectively). The most frequently reported drugs prescribed for nebulization were albuterol and budesonide (each 92.3%, 36/39), followed by albuterol-ipratropium combined formulation (84.6%, 33/39), ipratropium (71.8%, 28/39), and long-acting medications with less frequency (revefenacin at 61.5% or 24/29; arformoterol at 46.2% or 18/46; formoterol at 35.9% or 14/39; glycopyrrolate at 7.7% or 3/39). Other nebulized therapies that were also prescribed by these providers included hypertonic saline (79.5%, 31/39), inhaled antibiotics (41.0%, 16/39), and N-acetylcysteine (25.6%, 10/39).
Prescribing providers were asked to rank the reasons for initiating nebulized drugs on a 5-point scale from 1 (least important) to 5 (most important), with higher scores indicating greater perceived importance. The most important factor for prescribing nebulizers were reported to be the need for better control of symptoms than provided by hand-held inhalers, followed closely by cognitive or dexterity issues (Table 5). Factors such as patient preference, comfort and socio-economic status were rated as less influential, illustrating that prescribers prioritize clinical need and functional limitations over convenience or cost when selecting a delivery device. When asked to compare the benefits of nebulizers versus hand-held inhalers, prescribers reported that nebulizers were preferable to hand-held inhalers for patients experiencing exacerbations (82.1%, 32/39), whereas 53.8% (21/39) believed hand-held inhalers were preferable for routine symptom control (Figure 1).
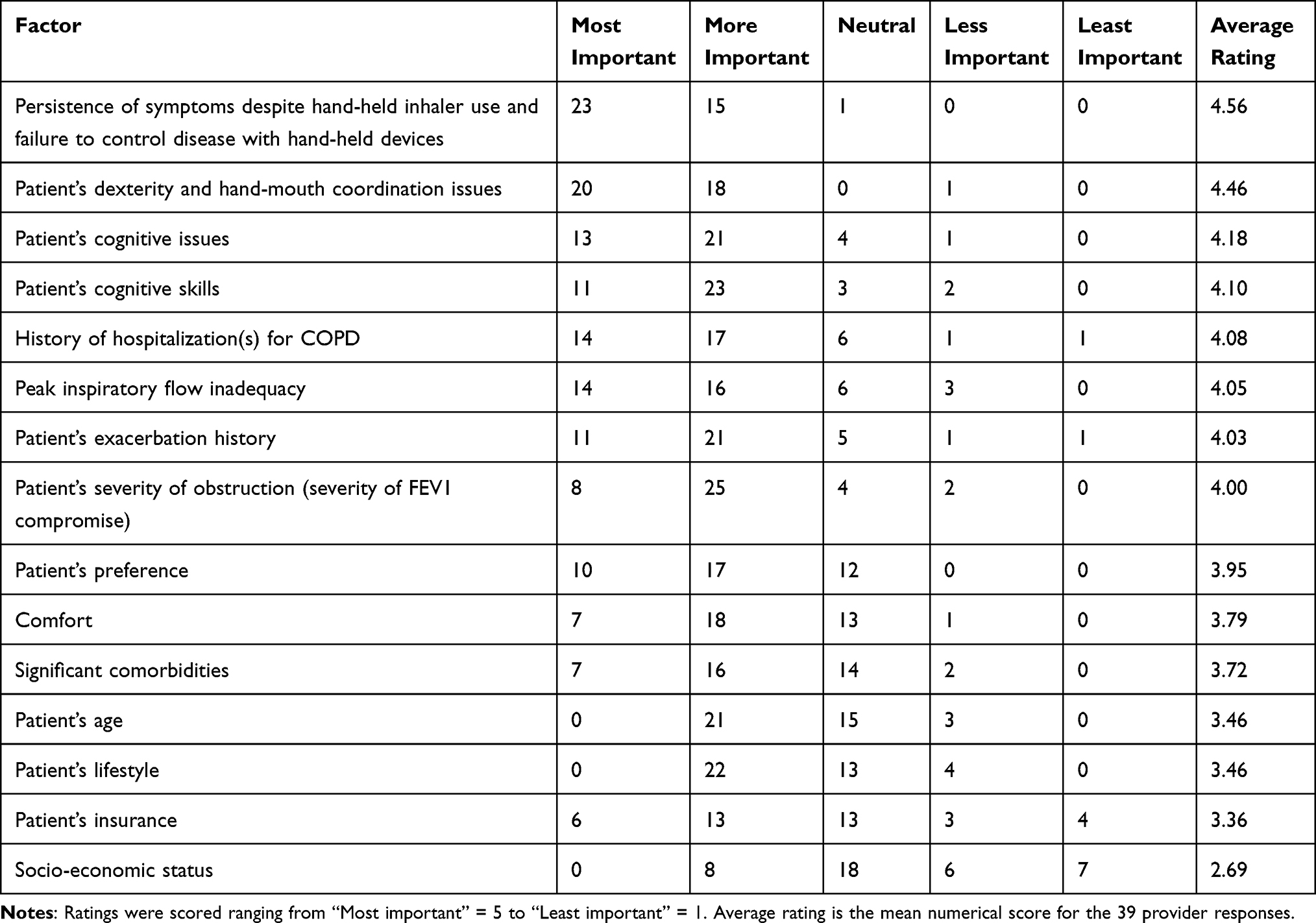 |
Table 5 Factors Considered by Healthcare Providers When Deciding to Prescribe Nebulized Therapy |
For hand-held inhaler device versus nebulizer preference, there were no statistical differences between surveyed providers’ perception of patient preference and surveyed patients’ preference for all surveyed dimensions (p > 0.17), with one the exception that more providers believed that hand-held inhaler devices are easier to maintain (94.9% vs 71.0%, p = 0.0007) (Figure 1).
Common provider-perceived barriers to wider use of nebulizers among their patients were lack of patient insurance coverage or approvals (69.2%, 27/39), patient cost (53.8%, 21/39), and lack of availability of combination drugs for nebulization (46.2%, 18/39). Two-thirds (26/39) of providers thought that nebulizers were underused. Providers’ suggested interventions most likely to increase the use of nebulizers among their patients (in descending order from most to least likely) were availability of combination long-acting drugs (79.5%, 31/39), optimization of insurance coverage and cost (76.9%, 30/39), availability of once-daily drugs (71.8%, 28/39), and improved portability of nebulizers (56.4%, 22/39).
The surveyed prescribers of nebulized pharmacotherapies believed that the COVID-19 pandemic negatively impacted the utilization of nebulizers in hospital settings (48.7%, 19/39) more than in outpatient settings (20.5%, 8/39), but they generally believed that the use of nebulizers has currently returned to the pre-pandemic degree of use in both hospital (69.2%, 27/39) and outpatient settings (74.4%, 29/39).
Discussion
Nebulized medications are widely used by patients to treat COPD. Despite consensus guidelines and numerous clinical trials that have informed pharmacological management of COPD,1–3 as well as the ongoing development of inhaled medications via a variety of delivery systems, there are scant recommendations as to which delivery system to select.1,4–8 Similar to prior data,15,16 our survey found that both patients and providers believed that nebulizers offer superior symptom control compared to hand-held inhaler devices, particularly during an exacerbation. This effect was best seen in older patients, those who use oxygen, and those who have had an exacerbation in the preceding year, suggesting that nebulizers might be particularly beneficial for these high risk groups. This is in contrast to the published literature that does not demonstrate a consistent objective benefit of nebulizers over hand-held inhalers. Some evidence suggests that these findings may have been confounded by the exclusion of patients who did not demonstrate proper technique with hand-held inhalers and the clinically stable setting in which these studies were performed.10–13 With regard to the latter, symptoms or air-trapping during an exacerbation could interfere with the ability of patients to use a hand-held inhaler with proper technique. Interestingly, we found that home nebulizer use and prescribing patterns have not been impacted significantly by the COVID-19 pandemic, despite initial concerns that nebulizers may result in increased infectious risk.
In our study, despite perceived benefits by prescribers and patients, as well as the viewpoint of providers that nebulized medications are underutilized, nearly half of the providers do not prescribe nebulized medications. Also, while 95% of patients in our survey who use nebulizers reported using nebulized short-acting bronchodilators, the use of long-acting nebulized medication, including the long-acting beta-2 agonists, formoterol and aformoterol, the long-acting antimuscarinic bronchodilators, glycopyrrolate and revefenacin, and the inhaled corticosteroid, budesonide, was notably infrequent. With the recent advent of these two nebulized long-acting antimuscarinic bronchodilators,19–22 the number of prescriptions for these drugs as controller medications for select patients may increase. Both glycopyrrolate and revefenacin have been approved for use over the last several years, and more recently after the conclusion of our survey, a novel dual phosphodiesterase 3 and 4 inhibitor, ensifentrine, was approved.23 Moreover, evidence is lacking concerning the efficacy and safety of administering long-acting nebulized controller medications, including long-acting bronchodilators and inhaled corticosteroids, administered in combination, potentially limiting their incorporation into daily practice for the maintenance of moderate to severe COPD.
Our survey explored barriers to nebulizer use by patients and prescription by providers. First, patients consistently reported that nebulizers are considerably more cumbersome to use and maintain compared to hand-held inhalers, although providers seemingly overestimated the degree to which maintenance is prohibitive for patients. Providers also suggested that increased portability and availability of once-daily controller medications would increase nebulizer use. Second, we found that providers perceived that nebulized medications were just as, if not more, expensive than similar drugs available in hand-held inhalers, due to either higher copays or lack of insurance coverage. Interestingly, patients reported the opposite; some nebulized medications were more affordable than hand-held inhalers, often covered through Medicare Part B. Physicians self-reported that the lack of combination long-acting medications as a barrier to more frequent prescribing of nebulized medications. This may help explain why nebulizers are used predominantly for short-acting medications rather than controller medications. Together, this demonstrates discordance between patient and provider perception of nebulizer utility in the clinical management of COPD based on cost and ease of use, but both patient and provider are aligned in the perceived superior symptom control with nebulizer utilization.
There are other possible benefits of nebulizer use as an alternative to hand-held inhalers that exist but are outside the scope of this survey. Several studies have reported the adverse environmental impacts of MDIs.24–27 Recommendations have suggested that use of DPIs and SMIs are preferred to MDIs to minimize the use of hydrofluorocarbons and decrease the carbon footprint. Future work could explore the potential environmental benefit of nebulized medications as well.
Our study has several limitations. First, given the survey distribution methods, which included posting on social media, online platforms, and via newsletters, we are not able to calculate a response rate. Similarly, we acknowledge that our cohort may not accurately reflect all COPD patients, particularly those who do not access to online platforms. Our patients were predominantly female, nearly entirely white, and over half had not been infected by SARS-CoV-2. However, we did have a representative and diverse geographic and socioeconomic sample. Additionally, this is a self-reported patient and provider survey, which carries with it recall bias. Further, patients may not have understood or misremembered details, such as which medications they have been prescribed or which type of nebulizer machine. We did not collect objective patient data to accurately classify their COPD disease severity, although the self-reported questions did give us information to understand that this patient population generally has severe disease. The small sample size limited our ability to perform comparative analysis within the patient or provider cohort. Additionally, not all participants completed the survey in full, leaving some questions with fewer responses than others. Despite these limitations, this is a hypothesis-generating survey to help us understand prescriber and patient utilization practices in the wake of the COVID-19 pandemic.
Conclusions
Our data indicate that nebulized medications are perceived as more affordable and reported to offer better control of chronic disease and acute exacerbation symptoms than hand-held inhalers by both patients and providers alike. However, nebulized therapy is prescribed less often due to several physician-perceived factors, including increased burden to maintain, comparative ease of inhaler maintenance, higher cost of nebulizers, and lack of combination long-acting nebulized therapies. Further work is needed to better understand the relative benefits and drawbacks of nebulized medications, examine the discordance between perceived and objective clinical benefit of nebulized medications, and explore ways of optimizing the identification of patients who will derive the most benefit from their use.
Acknowledgments
The abstract of this paper was presented at the American Thoracic Society Conference as a poster presentation with interim findings. The poster’s abstract was published in American Journal of Respiratory and Critical Care Medicine. 2025 May; Abstract Issue: A7140.
Collaborators
COPD Foundation Nebulizer Consortium
Bonnie Truelsen17, Rosina Ledermueller18, Jason Suggett, PhD, BPharm, MBA19, Dom Coppolo, MBA, RRT, FAARC, AE-C20, Blake Burnette21, Candice Clay, PhD22, Pranay P Patel23, Kim Gilchrist, MD24, Phil Kuehl, PhD25, Donald Mahler, MD26, Akshay Sood, MD, MPH27, Sanjay Sethi, MD28, Brian Carlin, MD29, Isaac Biney, MD30
17COPD patient; 18PARI, Inc; 19Monaghan Medical Corp.; 20Monaghan Medical Corp.; 21Verona Pharma; 22Verona Pharma; 23Viatris Inc.; 24Viatris Inc.; 25Lovelace Biomedical; 26Geisel School of Medicine at Dartmouth, Hanover, New Hampshire & Valley Regional Hospital in Claremont, New Hampshire, US; 27Division of Pulmonary, Critical Care and Sleep Medicine at University of New Mexico School of Medicine; 28Deputy Director of Clinical and Translational Sciences Institute (CTSI) at University Buffalo, State University of New York; 29UPMC Altoona Regional Medical Center; 30University of Tennessee Medical Center
Funding
The COPD Foundation Nebulizer Consortium is funded by Theravance Biopharma, Aerogen Ltd, PARI, Monaghan Medical, Verona Pharma, and Viatris.
Disclosure
Mr Sergio Martinez is an employee of the COPD Foundation. Ms Lisa Cambridge is an employee of PARI. Dr David Christiani served as an paid expert witness for plaintiff’s attorneys on matters of causation involving tobacco, asbestos, silica and other environmental and occupational exposures. He has made every effort to ensure that the current work was conducted with the highest scientific standards. Dr Jie Li reports grants and/or personal fees from COPD foundation, American association for respiratory care, MEKICS Co. Ltd, Vincent Ltd, and Fisher & Paykel Healthcare, outside the submitted work. Dr Jill Ohar reports grants from Mylan, Chiesi, TEVA, COPD Foundation, Spiromics; personal fees from Chiesi, Astra Zeneca, Verona, Genetech, outside the submitted work. Dr Rajiv Dhand reports grants from Theravance, Viatris; personal fees from UptoDate, Genentech, royalties from Taylor and Francis, outside the submitted work. Dr M Drummond reports personal fees from Verona, Chiesi, AstraZeneca, and GlaxoSmithKline, outside the submitted work; and unpaid member of COPD Foundation Medical and Scientific Advisory Committee. Prof. Dr. Arzu Ari reports grants from Aerogen, during the conduct of the study. Dr Arshan Perera was an employee of PARI Medical Holding GmbH during the conduct of the study. Ms Lauren Cochran is an employee and stock holder of Theravance Biopharma LLC. Dr David Mannino reports personal fees from GlaxoSmithKline, AstraZeneca, Chiesi, Lilly, Regeneron, Roche, Amgen, Sanofi, Up to date, and Schlesinger Law Firm, outside the submitted work. Dr Ariel Berlinski is the part of the advisory board for Hollo Medical, outside the submitted work. Dr Kim Gilchrist reports stocks from GSK, Astrazeneca, Pfizer, and Bristol Myers Squibb, outside the submitted work. Dr Igor Barjaktarevic reports grants, personal fees from Astra Zeneca, GSK, CSL, Theravance, Viatris, Verona Pharma, Takeda, Grifols, Sanofi and Regeneron, Genentech, and Aerogen, outside the submitted work. The authors report no other conflicts of interest in this work.
References
1. Venkatesan P. GOLD COPD report: 2024 update. Lancet Respir Med. 2024;12(1):15–12. doi:10.1016/S2213-2600(23)00461-7
2. Nici L, Mammen MJ, Charbek E, et al. Pharmacologic management of chronic obstructive pulmonary disease. An official American Thoracic Society clinical practice guideline. Am J Respir Crit Care Med. 2020;201(9):e56–e69. doi:10.1164/rccm.202003-0625ST
3. Gartman EJ, Mulpuru SS, Mammen MJ, et al. Summary for clinicians: clinical practice guideline on pharmacologic management of chronic obstructive pulmonary disease. Ann Am Thorac Soc. 2021;18(1):11–16. doi:10.1513/AnnalsATS.202007-880CME
4. Laube BL, Janssens HM, de Jongh FH, et al. What the pulmonary specialist should know about the new inhalation therapies. Eur Respir J. 2011;37(6):1308–1331. doi:10.1183/09031936.00166410
5. Barjaktarevic IZ, Milstone AP. Nebulized therapies in COPD: past, present, and the future. Int J Chron Obstruct Pulmon Dis. 2020;15:1665–1677. doi:10.2147/COPD.S252435
6. Pleasants RA, Hess DR. Aerosol delivery devices for obstructive lung diseases. Respir Care. 2018;63(6):708–733. doi:10.4187/respcare.06290
7. Tashkin DP. A review of nebulized drug delivery in COPD. Int J Chron Obstruct Pulmon Dis. 2016;11:2585–2596. doi:10.2147/COPD.S114034
8. Troy M, Van Vleet J, Tashkin D, Barjaktarevic I. Recent advances predict a bright future for nebulizers. Curr Opin Pulm Med. 2023;29(2):123–132. doi:10.1097/MCP.0000000000000941
9. Miravitlles M, Kawayama T, Dreher M. LABA/LAMA as first-line therapy for COPD: a summary of the evidence and guideline recommendations. J Clin Med. 2022;11(22):6623. doi:10.3390/jcm11226623
10. van Geffen WH, Douma WR, Slebos DJ, Kerstjens HAM, van Geffen HA. Bronchodilators delivered by nebuliser versus pMDI with spacer or DPI for exacerbations of COPD. Cochrane Database Syst Rev. 2016;2016(8):CD011826. doi:10.1002/14651858.CD011826.pub2
11. Maltais F, Ostinelli J, Bourbeau J, et al. Comparison of nebulized budesonide and oral prednisolone with placebo in the treatment of acute exacerbations of chronic obstructive pulmonary disease: a randomized controlled trial. Am J Respir Crit Care Med. 2002;165(5):698–703. doi:10.1164/ajrccm.165.5.2109093
12. O’Driscoll BR, Kay EA, Taylor RJ, Weatherby H, Chetty MC, Bernstein A. A long-term prospective assessment of home nebulizer treatment. Respir Med. 1992;86(4):317–325. doi:10.1016/S0954-6111(06)80031-4
13. Dolovich MB, Ahrens RC, Hess DR, et al. Device selection and outcomes of aerosol therapy: evidence-based guidelines: American college of chest Physicians/American college of asthma, allergy, and immunology. Chest. 2005;127(1):335–371. doi:10.1378/chest.127.1.335
14. Hanania NA, Braman S, Adams SG, et al. The role of inhalation delivery devices in COPD: perspectives of patients and health care providers. Chronic Obstr Pulm Dis. 2018;5(2):111–123. doi:10.15326/jcopdf.5.2.2017.0168
15. Braman SS, Carlin BW, Hanania NA, et al. Results of a pulmonologist survey regarding knowledge and practices with inhalation devices for COPD. Respir Care. 2018;63(7):840–848. doi:10.4187/respcare.05717
16. Dhand R, Mahler DA, Carlin BW, et al. Results of a patient survey regarding COPD knowledge, treatment experiences, and practices with inhalation devices. Respir Care. 2018;63(7):833–839. doi:10.4187/respcare.05715
17. Biney IN, Ari A, Barjaktarevic IZ, et al. Guidance on mitigating the risk of transmitting respiratory infections during nebulization by the COPD foundation nebulizer consortium. Chest. 2024;165(3):653–668. doi:10.1016/j.chest.2023.11.013
18. Clemency BM, Clay C, Varughese R, et al. Impact of nebulization versus metered-dose inhaler utilization on viral particle dispersion in patients with COVID-19. J Infect Prev. 2024;26:17571774241266420.
19. Kerwin E, Donohue JF, Goodin T, Tosiello R, Wheeler A, Ferguson GT. Efficacy and safety of glycopyrrolate/eFlow(®) CS (nebulized glycopyrrolate) in moderate-to-very-severe COPD: results from the glycopyrrolate for obstructive lung disease via electronic nebulizer (GOLDEN) 3 and 4 randomized controlled trials. Respir Med. 2017;132:238–250. doi:10.1016/j.rmed.2017.07.011
20. Ferguson GT, Feldman G, Pudi KK, et al. Improvements in lung function with nebulized revefenacin in the treatment of patients with moderate to very severe COPD: results from two replicate phase III clinical trials. Chronic Obstr Pulm Dis. 2019;6(2):154–165. doi:10.15326/jcopdf.6.2.2018.0152
21. Donohue JF, Kerwin E, Sethi S, et al. Revefenacin, a once-daily, lung-selective, long-acting muscarinic antagonist for nebulized therapy: safety and tolerability results of a 52-week Phase 3 trial in moderate to very severe chronic obstructive pulmonary disease. Respir Med. 2019;153:38–43. doi:10.1016/j.rmed.2019.05.010
22. Siler TM, Moran EJ, Barnes CN, Crater GD. Safety and efficacy of revefenacin and formoterol in sequence and combination via a standard jet nebulizer in patients with chronic obstructive pulmonary disease: a phase 3b, randomized, 42-day study. Chronic Obstr Pulm Dis. 2020;7(2):99–106. doi:10.15326/jcopdf.7.2.2019.0154
23. Sciurba FC, Christenson SA, Rheault T, Bengtsson T, Rickard K, Barjaktarevic IZ. Effect of dual phosphodiesterase 3 and 4 inhibitor ensifentrine on exacerbation rate and risk in patients with moderate to severe COPD. Chest. 2025;167(2):425–435. doi:10.1016/j.chest.2024.07.168
24. Janson C, Henderson R, Lofdahl M, Hedberg M, Sharma R, Wilkinson AJK. Carbon footprint impact of the choice of inhalers for asthma and COPD. Thorax. 2020;75(1):82–84. doi:10.1136/thoraxjnl-2019-213744
25. Owens S, Morris K, Hurley E, et al. Estimating the national carbon footprint of inhalers in healthcare. Ir J Med Sci. 2023;192(5):2251–2253. doi:10.1007/s11845-022-03234-0
26. Tirumalasetty J, Miller SA, Prescott HC, et al. Greenhouse gas emissions and costs of inhaler devices in the US. JAMA. 2024;332(12):1017–1019. doi:10.1001/jama.2024.15331
27. Wilkinson A, Woodcock A. The environmental impact of inhalers for asthma: a green challenge and a golden opportunity. Br J Clin Pharmacol. 2022;88(7):3016–3022. doi:10.1111/bcp.15135
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.