Back to Journals » Patient Preference and Adherence » Volume 19
Understanding Medication Self-Management at Home Among Older Adults with Coronary Artery Disease: A Qualitative Study
Authors Xu M ![]() , Lo SHS, Zhu L, Huang X
, Lo SHS, Zhu L, Huang X
Received 27 April 2025
Accepted for publication 21 August 2025
Published 30 September 2025 Volume 2025:19 Pages 3069—3082
DOI https://doi.org/10.2147/PPA.S537115
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Emma Veale
Mengqi Xu,1 Suzanne Hoi Shan Lo,1 Lingyan Zhu,2 Xiaoli Huang2
1The Nethersole School of Nursing, Faculty of Medicine, The Chinese University of Hong Kong, Hong Kong SAR, People’s Republic of China; 2Department of Nursing, Shanghai Sixth People’s Hospital Affiliated to Shanghai Jiao Tong University School of Medicine, Shanghai, People’s Republic of China
Correspondence: Suzanne Hoi Shan Lo, The Nethersole School of Nursing, Faculty of Medicine, The Chinese University of Hong Kong, Hong Kong SAR, People’s Republic of China, Email [email protected]
Background: The medication self-management at home among older adults with coronary artery disease is found suboptimal, leading to discrepancies from the prescriptions. More support is expected to meet their needs in medication self-management. This study aims to understand medication self-management at home of older adults with coronary artery disease.
Methods: From June to August 2024, a descriptive qualitative study was conducted among 28 older adults with coronary artery disease and six healthcare professionals. Older adults participated in interviews before and one month after hospital discharge. The healthcare professionals were interviewed once. The semi-structured interviews were conducted face-to-face or through a virtual platform. Thematic analysis was used in data analysis.
Findings: Two themes with five sub-themes emerged: 1. Dealing with unknown when starting new regimens: seeking support from healthcare professionals when starting medication self-management, self-information seeking is far from satisfactory. 2. Exploring strategies to support adherence to medications: difficulties in integrating medication taking into daily routine, aids as reminders for medication taking, and requesting help from caregivers.
Conclusion: Older adults with coronary artery disease struggled with seeking information to adapt to the new regimens and exploring different strategies to improve their adherence. Future interventions could improve their medication self-efficacy through patient-centred communication and peer education. Offering reliable information resources and improving the capacity to identify the accuracy of online information were important for self-information seeking. Besides, support in medication management aids and involving caregivers in medication management according to their needs were also warranted.
Keywords: coronary artery disease, older, medication, self-management, qualitative study
Background
The fast speed of ageing increases the burden of caring for older adults worldwide. Statistics indicate that there are one billion adults over 60 years old in 2020.1 China has the largest population of adults over 60 years old in the world. Cardiovascular diseases are one of the top reasons for death among older adults. In China, coronary artery disease (CAD) is the second leading cause of death among adults over 60 years old, contributing to 13.895 million Disability-Adjusted Life Years.2
Adhering to medication regimens is the major treatment for CAD. Medication self-management refers to the capacity of self-administering medications as prescribed, which is one of the major self-care activities. It is determined by cognitive and physical capacities.3 Patient education is recommended by the international guidelines and has become a routine in clinical nursing practice to support medication self-management among patients with CAD.4 Nevertheless, the effects were unideal. Discrepancies in medication taking were identified among 55.4% of middle-aged and older adults with CAD in China within one to two months post discharge, such as reducing the type of medications, missing the dosage of medications and replacing the medications.5 About 52.1% discrepancies were related to forgetfulness, feeling unnecessary to take the medications, fearing side effects and distrusting the benefits of medications. Some gaps in current services have been identified by older adults with CAD and nurses, specifically failing to meet the specific needs of older adults with CAD. In a cross-sectional study among 204 Chinese older adults with CAD during hospitalisation, more support was expected in medication self-management, including understanding the consequences of nonadherence (92.6%), identifying and dealing with the side effects (92.2%), and refilling the medication boxes (49.5%).6 Furthermore, 23 nurses from 11 hospitals in China reported having difficulty in understanding the different needs of patients with CAD in disease management to modify the methods of patient education and improve their effectiveness.7 For older adults with CAD, the physical deterioration made them easily develop side effects and forget to take medications,8,9 who may require more support in the management of side effects of CAD medications and medication management skills than the young adults. Existing studies described the experience of medication management among patients with CAD.10,11 Nevertheless, limited information is available about the specific needs of older adults with CAD regarding medication self-management practices. Besides, after transiting from hospital to home, older adults experience the transfer of medication management responsibility, who may meet different challenges in various stages of discharge.12 There was a lack of evidence about the medication self-management practices among older adults with CAD to tailor the interventions to their needs in different stages of hospital discharge.
This study aims to explore medication self-management practices of older adults with CAD at home. It is necessary to deeply understand the medication self-management practices among them to identify the challenges they meet and the support they need to better improve their medication safety.
Methods
Study Design and Setting
This study adopted a descriptive qualitative study design. It was conducted in the cardiology department of a general hospital and a community healthcare centre in Shanghai, China, during June to September 2024. It was part of a longitudinal qualitative study about changes in perceptions of medication management among older adults with CAD. Consolidated Criteria for Reporting Qualitative Research (COREQ) was followed in reporting the study (Supplementary 01).13
We followed the ethical standard of the Declaration of Helsinki. Approval of the study protocol was obtained from the Survey and Behavioural Research Ethics Committee of The Chinese University of Hong Kong (SBRE-23-0688) and the ethics committee of the tertiary hospital (2024–074-(1)). The participants provided consent about the publication of their anonymised responses.
Participants and Recruitment
Older adults with CAD were recruited with purposive sampling. The eligibility criteria for the participants are shown in Table 1. The principal investigator (MQX) and a research assistant approached the potential older adults with CAD at the bedside and introduced the study for recruitment. Those interested in the study were asked to sign the consent forms.
 |
Table 1 Eligibility Criteria |
Data Collection
Semi-structured interviews were adopted in data collection with audio-recording following an interview guide developed through literature review (Supplementary 02). In the interview guide, structured questions were designed based on topics regarding medication nonadherence (for example, forgetfulness, skipping the dosage, adding the dosage and taking the wrong medications), followed by the frequency of their nonadherent behaviours. Researchers also recorded field notes about the nonverbal information during interviews.
Older adults with different lengths of history of CAD were invited to participate in one face-to-face interview one or a half-day before discharge, and the other online or face-to-face interview one month after discharge to get a full picture of their medication self-management practices at home. The healthcare professionals were interviewed once.
The data collection was conducted by MQX or a research assistant. MQX was a PhD student undergoing training in qualitative study and had expereince in conducting qualitative studies. The research assistant was a registered nurse with a bachelor’s degree, who was trained by the PhD student in conducting interviews.
Data Analysis
Thematic analysis was used in data analysis with MAXQDA 2020.14 The interviews were transcribed by MQX and the research assistant and then cross-checked for accuracy. The transcripts were read repeatedly and open-coded by MQX. After becoming familiar with the transcripts, MQX performed the open coding by the “comment” function of Microsoft Word 2018. The codes were grouped to generate potential themes together. MQX checked themes with code extracts and generated a theme map. After reviewing the themes, she defined each theme and illustrated them with selected quotes. The corresponding author (SHSL) reviewed the themes, sub-themes and codes. Through discussion, MQX and SHSL reached a consensus about the results of the data analysis. MQX was a native speaker of Chinese and proficient in English. She translated the themes, sub-themes, and codes and selected verbatim from Chinese to English.
Rigour
We applied the criteria to improve the rigour of the study.15 Credibility is enhanced through member-checking with three participants and the cross-checking of the codes, sub-themes and themes. We selected the participants with maximum variation in the characteristics to improve the transferability of the study. We collected data through audio recordings, photos and field notes for the dependability of the findings. The findings were reviewed by the second reviewer for verification, and the direct quotes were used to enhance the confirmability.
Findings
Participant Characteristics
A total of 28 older adults with CAD were included in this study, among whom 27 participated in the first interviews and 22 participated in the second interviews. The mean age was 69.5 ± 4.9 years old. Eleven (39.3%) of them were newly diagnosed with CAD. Fifteen (53.6%) of them took one to four kinds of medications before discharge and 23 (82.1%) of them took five to eight kinds of medications after discharge. The mean duration of the interview was 25.99 minutes. Six healthcare professionals involved in this study included cardiologists (n = 2), pharmacists (n = 2) and nurses (n = 2), with a mean duration of the interview of 30.8 minutes (Tables 2 and 3: Characteristics of the older adults and the healthcare professionals; Figure 1. Flow of the participants).
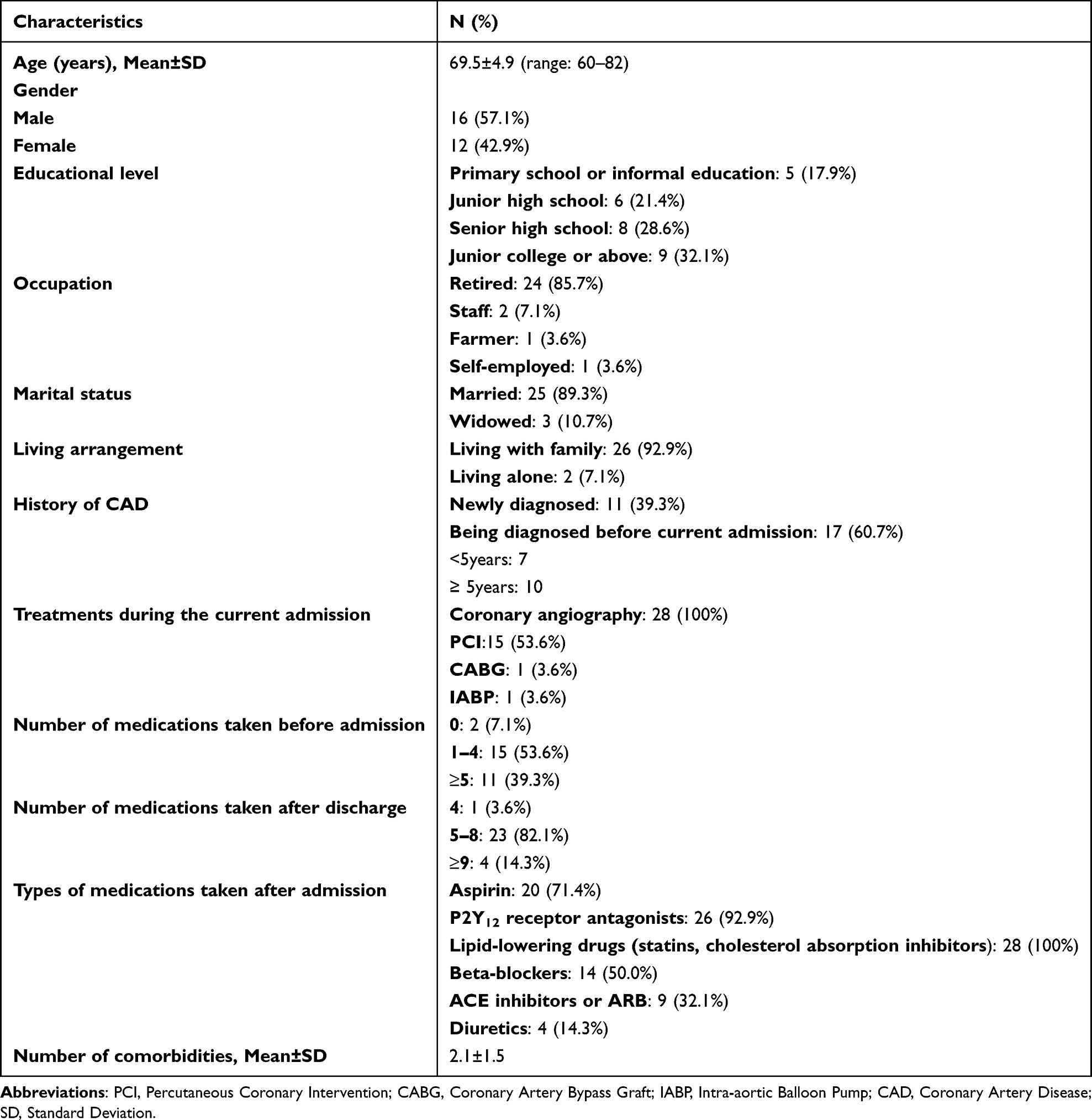 |
Table 2 Demographic and Clinical Information of the Older Adults with CAD (n=28) |
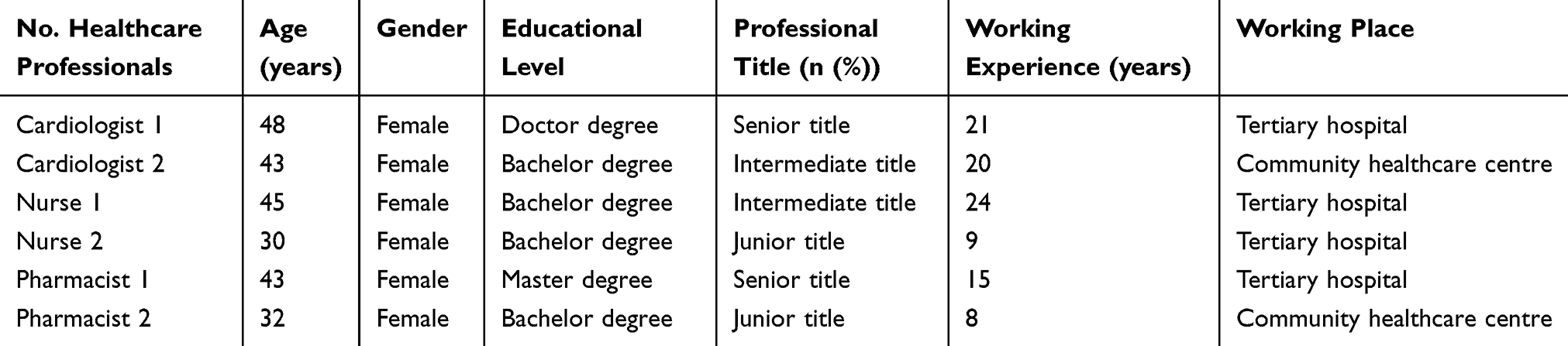 |
Table 3 Socio-Demographic Information of Healthcare Professionals (n=6) |
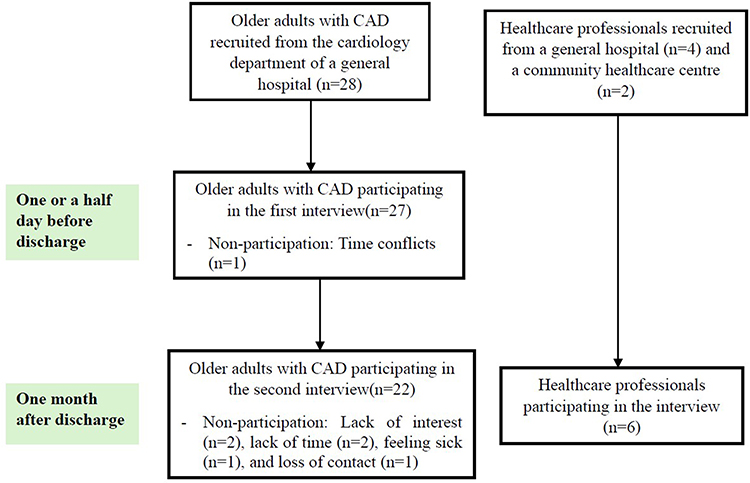 |
Figure 1 Flow of the participants interviewed at different timepoints. Older adults with coronary artery disease (CAD) were recruited from the cardiology department of a general hospital (n=28). Healthcare professionals were recruited from a general hospital (n=4) and a community healthcare centre (n=2). A total of 27 older adults with CAD were interviewed one day or a half day before discharge, and 22 of them were re-interviewed one-month post-discharge. Reasons for non-participation included time conflicts, lack of time, feeling sick and loss of contact. CAD = coronary artery disease. |
Themes and Sub-Themes
Through analysis, two themes with five sub-themes emerged. The themes were as follows: (1) “Dealing with unknowns when starting new regimens”, and (2) “Exploring strategies to support adherence to medications” (Table 4: Summarises the themes, subthemes, and examples of codes).
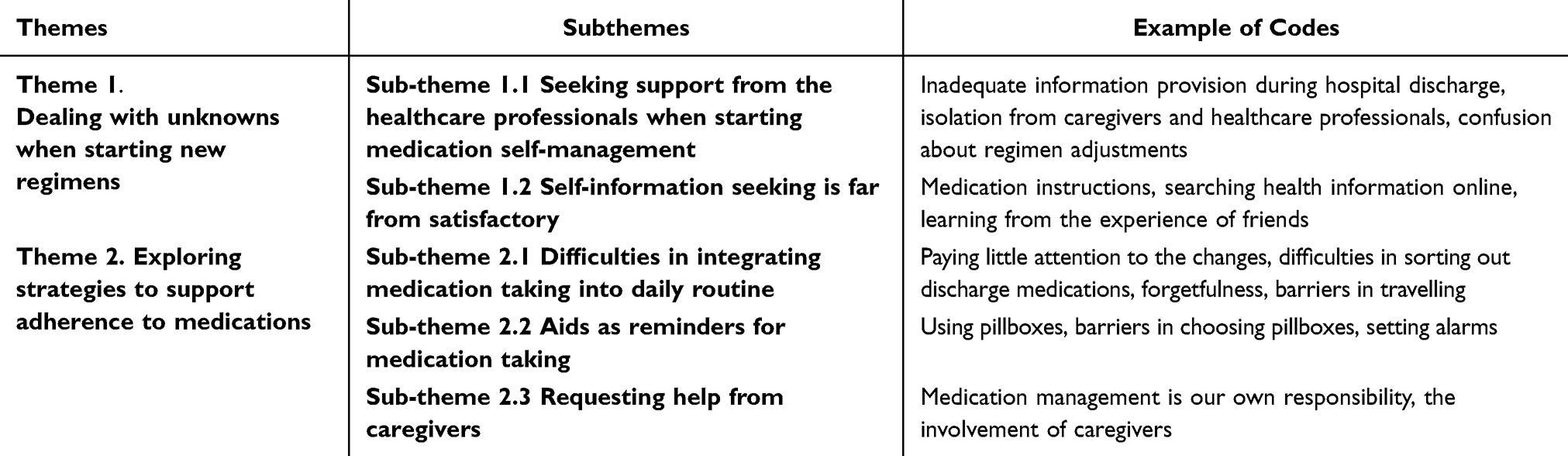 |
Table 4 Theme Map |
Theme 1. Dealing with Unknowns When Starting New Regimens
When starting the medication self-management, older adults with CAD had to adapt to the new regimens. They obtained information about new regimens through medication education and consultations with healthcare professionals. They also sought information from medication instructions, the internet, family and friends.
Sub-Theme 1.1 Seeking Support From Healthcare Professionals When Starting Medication Self-Management
Medication education and consultations with healthcare professionals were the outside support for medication self-management. Adequate information would enhance the confidence in adhering to medications among older adults with CAD, as it strengthened their understanding of the disease and medications. An older adult with CAD highlighted the positive mindsets (for example, confidence) about medications supported him in adhering to medications after hospital discharge.
Confidence is necessary, because belief and mindset play crucial roles. Just like me. I believe that taking this medication will improve my health and clear up clots. These psychological cues are very important. (21. 71y, male, First-time CAD_T2)
In fact, huge gaps were identified between the medication information provided by healthcare professionals and the expectations of older adults with CAD. Older adults reported feeling unconfident and uncertain about medication self-management.
The current discharge medication education was mainly about informing the usage of medications, rather than providing opportunities for consultations. Though highlighting the importance of adhering to medications, nurses found it hard to understand the needs for medication management of older adults with CAD and tailor the information to their needs.
It might be that I don’t fully understand the needs of the patients. We usually inform them about what they need to do regarding the medication treatment for their condition. (Nurse 01. 45y_ female)
Five older adults reported receiving limited verbal explanations about the precautions of medication management at the moment of hospital discharge. Some of them were unsatisfied with discharge education, because of the insufficient information and limited opportunities for consultation. They suggested face-to-face education, and booklets to enhance their understanding in the interviews. Besides, online education with Q&A sessions was regarded as an alternative.
Of course, face-to-face is better, but it’s not easy. On one hand, manpower may not be sufficient. An older adult paired with a doctor for education isn’t very practical. Online (might be practical), typically for dozens or even hundreds of people attending the session. Sometimes they pose questions for the doctors to answer. (3. 82y, male, CAD 3y _T1)
Older adults with CAD were also isolated from the communications between the healthcare professionals and their family members when discharging from the hospital. Due to the difficulties in communicating with the older adults about the regimens, the healthcare professionals often discussed with their family members to improve the working efficiency and expected the family members to elaborate for the older adults. However, some family members underestimated the importance of informing the older adults. Two older adults with CAD were confused about the regimens after hospital discharge because of not being informed by their family members. One of the 22 older adults discontinued the Clopidogrel for not being informed about its benefits to the heart within one month of discharge.
When I was discharged from the hospital, my daughter-in-law took the prescriptions for me. I couldn’t figure out (why I was taking clopidogrel), and they (daughter-in-law and doctors) didn’t tell me. (82y, male, CAD 3y _T2)
Because of the forgetfulness and polypharmacy among older adults with CAD, clear medication lists help them adapt to new regimens at home. Incomplete information about regimens in the discharge summary left older adults with uncertainties in the first few days after discharge. An older adult was not sure whether aspirin needed to be taken, as the doctor told him to take it, but relevant information was lacking in the discharge summary. He consulted his friend who was also a healthcare professional and decided based on his or her advice.
Because he (the doctor) didn’t prescribe aspirin for me. Should I just take my aspirin, or should I stop taking aspirin altogether? But according to their opinion, I should still take it, right? (15. 73y, male, First-time CAD_T2)
Besides, general information about the usage of several common CAD medications was presented in the summaries for the convenience of most patients with CAD, while limited explanations were provided regarding the specific regimens of each participant. An older adult with CAD was confused with the difference between the discharge regimens and the information about CAD medications in the discharge summary because she was prescribed another antiplatelet medication instead of aspirin. She was sceptical about the accuracy of the prescriptions and hesitant to start the self-administration at home. Thus, she consulted the cardiologist again in the clinic for verification.
Because doctor made it very clear in the ward, he said that he would change the regimen. I don’t need to take aspirin and Tegretol after discharge. But after discharge, the discharge summary said that aspirin was to be taken for a lifetime. I consulted the doctor. I knew the change of regimen (stop taking aspirin and Tegretol), but why the discharge summary said again about the importance of aspirin. (11. 63y, female, CAD 1y_ T2)
Another older adult receiving contradicting information about the regimens, who was frustrated and planned to consult with another doctor he trusted more.
This time, doctor L adjusted the dosage of aspirin to 100mg without providing any explanations. I will go back to the clinic of doctor J (who conducted surgery for the older adult) to consult him about the dosage. (19. 68y, male, CAD 9 months_T2)
Though older adults consulted the healthcare professionals in the follow-up visits, three of them did not get the expected guidance. The healthcare professionals also reported the workload and lack of institutional support limited their time spent in consultations with the patients after discharge.
We may give more details about medications in the cardiovascular outpatient. It is generally conducted once every two weeks with other cardiologists in the clinic and only five to ten patients attend…… There are too many patients in the general clinics…… (Cardiologist 02, 32y_ female)
Besides, seven older adults felt unconfident about the right timing for taking medications, when combining medication into their daily routine in self-management. They chose the timing based on their previous medication-taking experience.
I usually take this medication (clopidogrel) after a meal, but I’m not sure if it should be taken before or after a meal. (13. 70y, female, CAD 6y_ T2)
An older adult made mistakes in storing her injectable lipid-lowering drugs at home as she received limited guidance about the medication storage, which resulted in financial losses.
The Evolocumab Injection needs to be used by me. I don’t know and the nurse didn’t tell me that it should be stored in the fridge. When I took it to the hospital, the doctor said, ‘You can’t keep it like this, you should put it in the fridge. It was expired. I had to throw it away and buy a new set. (12.69y, female, CAD 9y _T2)
Sub-Theme 1.2 Self-Information Seeking Is Far From Satisfactory
Because of the lack of guidance in medication self-management from the hospitals, many older adults with CAD sought information in other ways, including reading medication instructions, searching online and consulting family and friends.
Medication instruction was one of their favourite sources of information out of hospitals. However, small fonts and excessive irrelevant information in the medication instructions hindered them from extracting useful information and made them stressed.
I’m not good at reading. There are so many words on the medication instructions. I can’t understand it even reading it. Why bother reading it? The words are too small, I can’t see them clearly anyway. I don’t read (the medication instructions) anyway. Who cares. (12. 69y, male, CAD 9y _T1)
Fifteen out of 28 older adults with CAD reported proactively searching health information online in daily life. Baidu, TikTok, WeChat and Rednote were the main information sources, with encyclopaedia, short videos made by healthcare professionals and experience sharing blogs as major formats. Online information deepened their understanding of the medications and increased their confidence in adhering to the medications. An older adult reported changing from nonadherence to adherence to statins motivated by the information provided by the healthcare professionals online after discharge. During the interview, he also shared the short videos about statins that inspired him.
I would like to tell you why I’m taking statin now. You know, because I search on my phone every day. All people (in the short videos) telling me about it. Then, I start to take it. (27. 69y, male, CAD 18y_T2)
The characteristics of being audio-enabled, large fonts, high interactivity, financial incentives, and being able to replay enhanced the acceptance of online information among older adults with CAD.
Usually, on WeChat, they add you to a group where they offer daily lectures. They keep track of whether you attend these lectures, and if you do, they reward you with a small incentive, like 20 or 30 cents. These lectures aren’t one-time events. They run continuously from 7 or 8 in the morning until 7 or 8 in the evening, playing in a loop. (3. 82y, male, CAD 3y_ T1)
However, vision impairment decreased their access to information from the internet. Technical barriers in using smart devices, especially using search engines, prevented them from obtaining medication information online.
Information about medications online is probably a safe bet. I usually avoid reading other things online because my vision isn’t very good. I have near-sightedness and presbyopia now. (13. 70y, female, CAD 6y_ T1)
I don’t know how to search on the phone. There are so many functions on this phone that I don’t know how to use them. You can find out the benefits of statins online, but I don’t know. I never look it up. (20. 74y, female, CAD 12y_ T1)
Older adults with CAD also sought advice from their family and friends after discharge. In addition to helping them interpret the information about medications on the instructions or provided by the healthcare professionals, their peers (for example, family or friends with CAD) were an important resource in obtaining real experience in using medications and managing medications due to the trust. The experience shared by the peers was regarded as a reference to inform their mediation taking, such as the experience of benefits and dealing with the side effects of CAD medications.
I have a relative who also had CAD came to visit me. He shared a lot with me, and I can tell that he understands CAD medications very well. He is quite knowledgeable in this area. So, I don’t really bother looking things up online or elsewhere. (4. 66y, male, First-time CAD_T2)
An older adult with CAD stated she learnt from the experience of her friends. The adverse events experienced by peers facilitated her to continue to take CAD medications to prevent CAD prognosis and comorbidities.
I have a colleague (had CAD) who didn’t trust what the doctor said. Instead, he drank the heart-care tea (a health supplement). In the end, his condition got worse, and he had to undergo coronary bypass surgery. Another colleague also stopped taking his medication. Later, he had a stroke. From their stories, I learned that I need to listen to the doctor. (25. 68y, female, CAD 9y_T2)
Besides, some of them found the information obtained from the internet and people surrounding them might be unreliable, especially when receiving contradicting information. Some of them were confused about the accuracy of the information of the health product promotion and expected more information disseminated by the healthcare professionals on the internet.
I just listen to the doctors on the phone. The doctors are the ones wearing those surgical gowns, right? I saw a few of them said that (the benefits of adhering to statins), so I take this seriously…….Some of the stuff online is unreliable, like those health supplements. I don’t even bother looking at them and just dismiss them right away. (27. 69y, male, CAD 18y_T2)
Theme 2. Exploring Strategies to Support Adherence to Medications
Medication self-management required effective strategies. Older adults used various aids as reminders and requested help from the caregivers to deal with the barriers in integrating medication taking into daily routine.
Sub-Theme 2.1 Difficulties in Integrating Medication Taking Into the Daily Routine
In the initial days of hospital discharge, most older adults with CAD underwent adjustments in their medication regimens, including changes in the types of medications and dosage. They had difficulties in sorting out their medications, such as the changes in time of medication taking and dosage. An older adult newly diagnosed with CAD explained how he struggled with medication taking during the first few days of discharge due to polypharmacy and forgetfulness, and finally got used to the regimens.
When I just discharged from the hospital and went back home, I was confused looking at these medications…… Later, I just studied myself. After figuring it out, everything became clear. (17. 69y, male, First-time CAD_T2)
Nevertheless, three older adults said they paid little attention to the discharge summary. As all of them had at least one year of CAD history, they decided on the dosage based on their experience. The changes in the dosage might be omitted, which would lead to errors in medication taking.
I had a stent placed before, and this is my second stent. Anyway, I just took the same dosage as before. I’ve been taking these medications for over ten years. Hasn’t it always been taken this way? (26. 70y, female, CAD 9y_T2)
In daily life, five of the 28 older adults reported easily forgetting to take their medications, especially for the medications suggested to be taken at night (for example, statins) and during traveling. Particularly, influenced by the sleeping disorders, two older adults reported going to bed early at night and would not get up to take statins if they forgot to take them. Another two older adults said the social activities at night also made them forgetful in taking statins. Some of them had no idea how to deal with the forgetfulness while just skipping the missed dose. They were also unconfident in modifying the schedule of medication taking to adjust their life routine.
At night, I use the iPad to watch videos. Usually, after that, I take my medication (statin), and then go to bed. When I forgot to take it, I just let it go… For older adults, it’s not easy to fall asleep. If I’m already asleep, there’s no way. Once I wake up, I won’t be able to fall back asleep for two hours. (12. 69y, female, CAD 9y_ T2)
Besides, travelling was perceived as a challenge for medication self-management, including preparing the health insurance card, pillboxes and medication lists. The preparation was perceived as burdensome by older adults with CAD and easily resulted in forgetfulness.
The most troublesome thing is travelling. I have to remember to bring my medication . If I’m going on a three-day trip nearby, I’ll bring five days’ medications…… I also have to bring my health insurance card and prepare things like the name of the medications, prescriptions, or other documents. I even have to take photos of them. When I go to other places, the colour of the medicine or the dosage might be different, and that’s quite troublesome too. (11. 63y, female, CAD 1y_T1)
Older adults with CAD also faced barriers in getting the prescriptions. Because of the comorbidities, polypharmacy and limitations in prescription, they hardly got prescriptions all at once. They had to spend a long time queuing up in the tertiary hospital. They complained about commuting across different settings to get and fill the prescriptions, which was time-consuming and tiring, especially for those without caregivers. The difficulties in getting and filling the prescriptions forbade them from continuing to take medications.
Because I’m getting older, already 68 years old. I feel it’s quite troublesome to go out to get my medications. If the community clinic had these medications, I would just get them there and wouldn’t need to come here (tertiary hospital). (19. 68y, male, CAD 9 months_T1)
Sub-Theme 2.2 Aids as Reminders for Medication Taking
Different aids were adopted by older adults with CAD to remind medication taking. Especially in the early stage of hospital discharge, “trial and error” was common among the older adults in selecting the medication management aids. Choosing an appropriate site to store the medication was the first step to remind medication taking. An older adult altered his original medication storage site by placing medications in more conspicuous locations instead of in the drawer after hospital discharge. He thought the conspicuous location helped him reduce the forgetfulness.
I have it (the medication) placed in front of the TV now. I used to have a dedicated drawer for the medications. If it’s in the drawer, I might forget about it. By keeping it on the table, it’s in my sight, and reminding me not to forget. (15. 73y, male, First-time CAD_T2)
In addition, categorization, labels, and pillboxes were common strategies helpful for adhering to medications. Labels on the packages were regarded as convenient in noting the right dosage. Especially, older adults reported that pillboxes reduced the mistakes when taking medications by reminding them to avoid repetition, compared with not using the pillboxes.
Every day, I put the pill box in the most conspicuous place. When I get up, I see it. At night, the last column is eaten. Then, this empty box is put back, and the full one is taken out, which is for the next day. So, I haven’t made any mistake. (19. 68y, male, CAD 9 months_T1)
However, two older adults with CAD mentioned that they were prone to errors when putting medications in compartmentalized pillboxes. They also found it was hard to choose the appropriate pillboxes, who spent time in searching for information online and trying different types of pillboxes.
I’ve bought those little boxes with compartments for each day of the week, but I found them inconvenient. It’s easier for one big box instead. The compartment box sometimes makes me forgetful. Sometimes, I make mistakes when filling them up. (23. 75y, male, First-time CAD_T2)
A nurse also stated that older adults were less likely to differentiate the medications in the pillbox, which might lead to mistakes during the temporary medication suspension. She also highlighted the difficulties in keeping the medications clean and dry in the pillboxes in the wet weather.
If too many medications are mixed, they might not be able to tell which one to stop if a certain medication needs to be discontinued. During humid weather, some medications can easily absorb moisture, which could reduce their effectiveness. (Nurse 01. 45y_ female)
Besides, three older adults set alarms on their phones to remind them to take their medications. However, single alarm reminding might be unable to improve adherence.
Sub-Theme 2.3 Requesting Help From Caregivers
Older adults with CAD regarded medication management as their own business. They would like to manage medications with their efforts instead of relying on others. Nevertheless, various barriers hindered them in self-administration. Seven of the 28 older adults requested support from caregivers to better adhere to medications.
Older adults with CAD and healthcare professionals agreed that caregivers were helpful in their medication self-management. Caregivers mainly supported medication self-management by monitoring their adherence and the effects after taking medications, filling the pillboxes to ensure the accuracy of medication taking and filling the prescriptions for older adults. Five older adults had reminders from caregivers to take the medications. Two of them received support from caregivers in filling the pillboxes to ensure the accuracy.
Every day, my wife helps me put medications into the pillbox. She supervises me. If I don’t take them, she’ll remind me. (4. 66y, male, First-time CAD_T2)
Especially due to the unstable conditions of older adults with CAD in the first few months of discharge, some of them relied on caregivers. After discharge, an older adult reported becoming adherent to medications under the supervision of her daughter, as she moved to the place of her daughter for recovery.
I take the medications when she (her daughter) gives me. Sometimes, I take them myself when she reminds me. (7. 67y, female, First-time CAD_T2)
Reminding and supervision of the caregivers were perceived as the last guarantee for medication adherence. A nurse highlighted that caregivers could facilitate medication taking among those older adults nonadherent to medications.
Caregivers are very important. We once had a patient who was an older man…… Every day, his son prepares medications for him to take. He told us that if he just put the medications over there and expected his father to take them himself, he would say, ‘What’s going on? Why do I have to take so many medications?’ He won’t take the initiative to do it. He still needs someone by his side. (Nurse 01. 45y_ female)
Discussion
Overall, older adults struggled in medication self-management at home, including information seeking regarding new regimens and finding strategies to support adherence. They dealt with unknowns about new regimens by seeking support from the healthcare professionals, and peers, while they could not receive the expected information and made mistakes in their medication taking. They were unprepared for self-administration, who tried different strategies to get used to the new regimens and improve their abilities in adhering to medications. This study provided new insights in developing interventions addressing these specific needs for improving medication self-management among older adults with CAD.
The findings highlighted improving the understanding of CAD and medications would enhance confidence in medication self-management among older adults with CAD. However, an older adult discontinued clopidogrel wrongly, because of not being informed by the caregivers and healthcare professionals. Existing studies found the healthcare professionals and older adults spent limited time in communicating about medication-related problems.16 Encouraging the older adults to raise queries, collecting their feedback and sending customised educational materials were suggested to promote the older adults’ involvement in medication communication.17 Medication self-efficacy includes the beliefs in accurately understanding the medications and appropriate use of medications.18 Similarly, existing evidence indicated that medication self-efficacy was a mediating factor between medication literacy and medication adherence among older adults with comorbidities.19 Improving medication self-efficacy would help optimize the educational programmes for improving medication adherence. In a systematic review involving 16 studies about enhancing medication self-efficacy and medication adherence among patients with stroke, successful interventions mostly used patient-centred communication, and multi-media formats (for example, video narratives, phone calls and interactive text messages).20 Besides, many older adults with CAD acquired information from peers. Interventions based on peer education, such as storytelling and peer modelling, are potential for improving the understanding of CAD medications and self-efficacy in adhering to CAD medications.21,22 Peer education was also found more cost-effective than other usual education in improving medication adherence among older adults with hypertension.23 Involving peers in the medication management of older adults with CAD may be an acceptable and effective method to optimise their medication management behaviours.
Online health information seeking has become popular among older adults in recent years. Similar with the findings of a systematic review, information about medication and treatment was one of the most popular topics among older adults in their online health information seeking.24 Developing ageing-friendly smart devices, providing training about computer skills and identifying high-quality health information could promote online information-seeking among older adults.24 Besides, the negative online information about CAD medications, for example, aspirin and statins, was associated with medication nonadherence.25,26 More reliable online medication information is expected by the older adults in this study. Optimizing the management of official accounts of government health institutions and enhancing the understanding of compositions of misinformation may be helpful for older adults in identifying useful health information and distinguishing the accuracy of health information online.27
Unique medication management strategies about storing the medications and reminding medication taking were applied by older adults in self-administration.28,29 In this study, though various strategies to adhere to medications were adopted, older adults with CAD encountered challenges in finding the most suitable methods, managing the pillboxes and adhering to medications during traveling and at night. Nurses could provide suggestions about practical strategies to adhere to medication before hospital discharge to reduce the time spent in trial and error among older adults with CAD. Though using pillboxes was suggested as a crucial strategy as an aid for memory and organization in medication self-management,30 an older adult found he often made mistakes when filling in the pillboxes in this study. In clinical nursing practice, evaluating the cognitive functions and capacities in pillboxes management was suggested before recommending the pillboxes to the older adults for self-administration.31 Support from family and healthcare professionals was needed to ensure the accuracy of medication refilling of the pillboxes, especially for older adults with cognitive impairment. Another study found that customized 3D printed pillboxes had large to medium effects on medication adherence, compared with standardised pillboxes, indicating the personalised pillboxes had better potential in optimizing medication self-management.32 This study provided new insights into the difficulties in adhering to specific CAD medications. Statins were easily forgotten to be taken by the older adults with CAD, due to the conflicts of recommended medication taking schedule and daily routine of the older adults. In addition to providing comprehensive guidance about the schedule of different types of statins, special trainings could be provided for the older adults to integrate the statin taking into daily routine to build-up individualised plans.29
The dominance and independence in medication management were highlighted by the older adults with CAD in this study, who regarded themselves as the most reliable people in dealing with occasions without family. Similarly, four of the six successful interventions included caregivers as facilitators to accompany older adults with CAD in medication management.33 Even so, the restrictions on the eligible participants were also acknowledged as one of the limitations in promoting the family-based intervention to improve medication adherence, because those without caregivers were excluded.34 Though caregivers were regarded as a guarantee of medication adherence among older adults with CAD, the burden in medication management of the caregivers should be considered. Due to the limited health education and social support, the caregivers face various challenges in medication management, such as high time consumption, non-cooperation of the patient, and difficulties in adjusting the dosage.35,36 Therefore, they bear a substantial burden in managing medications, even mental health problems.36 In future studies, more assessment of medication management capacity (for example, cognitive capacity in managing pillboxes) of older adults with CAD could be added to tailor the interventions based on the needs of older adults and reduce the burden of caregivers by only involving them in those needing support in medication management.
We acknowledge the following limitations in our study. First, we utilized purposive sampling in the recruitment. Most older adults with CAD had high education levels and were younger than 80 years old. Though the targeted sample size of the qualitative study was achieved, studies with large and diverse samples would be needed to capture a wide range of experiences, given the growing prevalence of CAD among older adults. Second, the study was conducted in Shanghai. The experiences of the participants may not be representative of other places in China.
Conclusion
This study described the medication self-management practices of older adults with CAD. They sought information from various ways to adapt to the new regimens and explored different strategies to improve their adherence. The findings suggested improving medication self-efficacy through patient-centred communication and peer education. Offering reliable information resources and improving the capacity in identifying the accuracy of online information were important for the self-information seeking among older adults with CAD. Besides, supports in finding and using the suitable medication management aids and involving caregivers according to the needs of older adults with CAD were also warranted.
Abbreviation
CAD, Coronary artery disease.
Data Sharing Statement
Data cannot be shared because participants are informed and agree to use their data in the current study.
Ethical Consideration and Consent to Participate
The study protocol has been approved by the Survey and Behavioural Research Ethics Committee of The Chinese University of Hong Kong (SBRE-23-0688) and the study setting (2024-074-(1)). Written consent forms were obtained from the participants before conducting the interviews.
Acknowledgments
We would like to thank all participants involved in this study for sharing their perceptions and experiences. We are also grateful for Miss. Yuan Ding for her contribution to data collection and analysis.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
There is no funding to report.
Disclosure
The authors declare that they have no competing interests in this work.
References
1. World Health Organisation. Ageing and health. 2024. Available from: https://www.who.int/news-room/fact-sheets/detail/ageing-and-health.
2. Wu H, Wang Y, Zhang H, et al. An investigation into the health status of the elderly population in China and the obstacles to achieving healthy aging. Sci Rep. 2024;14(1):31123. doi:10.1038/s41598-024-82443-2
3. Badawoud AM, Salgado TM, Lu J, Parsons P, Peron EP, Slattum PW. Measuring medication self-management capacity: a scoping review of available instruments. Drugs Aging. 2020;37(7):483–501. doi:10.1007/s40266-020-00764-z
4. Byrne RA, Rossello X, Coughlan JJ, et al. 2023 ESC guidelines for the management of acute coronary syndromes: developed by the task force on the management of acute coronary syndromes of the European Society of Cardiology (ESC). Eur Heart J. 2023;44(38):3720–3826. doi:10.1093/eurheartj/ehad191
5. Li Y, Wang X, Lu Y, Li L, Li X. Investigation and study on medication discrepancies and related factors in patients with coronary heart disease. China Pharm. 2015;26(2):273–275.
6. Qi Y. Investigation on polypharmacy health education needs of elderly patients with coronary heart disease and its intervention measures. J Clin Psychosom Dis. 2017;23(5):123–126.
7. Xiong Q, Zhao Q, Tian Y, Xiao M. Nurses’ perceptions of the effectiveness of health education for patients with coronary artery disease: a qualitative study. J Nurses Train. 2014;29(3):216–218.
8. Xia T, Huang F, Li Y, et al. The impact of age on the implementation of evidence-based medications in patients with coronary artery disease and its prognostic significance: a retrospective cohort study. BMC Public Health. 2018;18(1):150. doi:10.1186/s12889-018-5049-x
9. Yu M, Wang L, Guan L, Qian M, Lv J, Deng M. Knowledge, attitudes, and barriers related to medication adherence of older patients with coronary heart disease in China. Geriatr Nurs N Y N. 2022;43:235–241. doi:10.1016/j.gerinurse.2021.12.001
10. Hanna A, Yael EM, Hadassa L, et al. ``It’s up to me with a little support” – adherence after myocardial infarction: a qualitative study. Int J Nurs Stud. 2020;101:103416. doi:10.1016/j.ijnurstu.2019.103416
11. Kimble LP, Momary KM, Adewuyi M. A qualitative study of nuisance bleeding and medication-related beliefs with dual antiplatelet drug therapy. Heart Lung. 2018;47(5):485–488. doi:10.1016/j.hrtlng.2018.05.014
12. Lin X, Xu W, Lin T. Participation in medication safety of older-adult patients with chronic disease during the transition from hospital to home: a descriptive qualitative study. BMC Geriatr. 2024;24(1):877. doi:10.1186/s12877-024-05468-2
13. Tong A, Sainsbury P, Craig J. Consolidated criteria for reporting qualitative research (COREQ): a 32-item checklist for interviews and focus groups. Int J Qual Health Care J Int Soc Qual Health Care. 2007;19(6):349–357. doi:10.1093/intqhc/mzm042
14. Braun V, Clarke V. Using thematic analysis in psychology. Qual Res Psychol. 2006;3(2):77–101. doi:10.1191/1478088706qp063oa
15. Nowell LS, Norris JM, White DE, Moules NJ. Thematic analysis: striving to meet the trustworthiness criteria. Int J Qual Methods. 2017;16(1):1609406917733847. doi:10.1177/1609406917733847
16. Nicosia FM, Spar MJ, Stebbins M, et al. What is a medication-related problem? a qualitative study of older adults and primary care clinicians. J Gen Intern Med. 2020;35(3):724–731. doi:10.1007/s11606-019-05463-z
17. Copley DM, Manias E, Watkins V, Hutchinson AM. Communication processes related to decision-making in medication management between healthcare providers, older people and their carers: a systematic review. Health Expect. 2025;28(2):e70252. doi:10.1111/hex.70252
18. Lamarche L, Tejpal A, Mangin D. Self-efficacy for medication management: a systematic review of instruments. Patient Prefer Adherence. 2018;12:1279–1287. doi:10.2147/PPA.S165749
19. Wang W, Luan W, Zhang Z, Mei Y. Association between medication literacy and medication adherence and the mediating effect of self-efficacy in older people with multimorbidity. BMC Geriatr. 2023;23(1):378. doi:10.1186/s12877-023-04072-0
20. Appalasamy JR, Ramaiah SS, Quek KF, Md Zain AZ, Tha KK. Medication understanding and taking self-efficacy theory-based interventions. J Young Pharm. 2020;12(1):18–24. doi:10.5530/jyp.2020.12.5
21. Bandura A. Reflections on self-efficacy. Adv Behav Res Ther. 1978;1(4):237–269. doi:10.1016/0146-6402(78)90012-7
22. Gucciardi E, Jean-Pierre N, Karam G, Sidani S. Designing and delivering facilitated storytelling interventions for chronic disease self-management: a scoping review. BMC Health Serv Res. 2016;16:249. doi:10.1186/s12913-016-1474-7
23. Ranjbar H, Sadeghi-Vazin K, Bakhshi M. The cost-effectiveness of peer education on medication adherence in the elderly with hypertension: a randomized controlled trial. BMC Public Health. 2024;24:3268. doi:10.1186/s12889-024-20807-z
24. Zhao YC, Zhao M, Song S. Online health information seeking behaviors among older adults: systematic scoping review. J Med Internet Res. 2022;24(2):e34790. doi:10.2196/34790
25. Lim HM, Ng CJ, Abdullah A, Danee M, Raubenheimer J, Dunn AG. Online health information behaviour and its association with statin adherence in patients with high cardiovascular risk: a prospective cohort study. Digit Health. 2024;10:20552076241241250. doi:10.1177/20552076241241250
26. Zhu J, Chen W. Use of aspirin in cardiovascular disease prevention-the role of online information search. Chronic Illn. 2024;20(3):445–453. doi:10.1177/17423953241241761
27. Chang L, Li W, Xin X, Wang J. Strategies for assessing health information credibility among older social media users in china: a qualitative study. Health Commun. 2024;39(12):2767–2778. doi:10.1080/10410236.2023.2288372
28. Gualtieri L, Shaveet E, Estime B, Patel A. The role of home medication storage location in increasing medication adherence for middle-aged and older adults. Front Digit Health. 2022;4:999981. doi:10.3389/fdgth.2022.999981
29. Gualtieri L, Rigby M, Wang D, Mann E. Medication management strategies to support medication adherence: interview study with older adults. Interact J Med Res. 2024;13:e53513. doi:10.2196/53513
30. Schwartz JK. Pillbox use, satisfaction, and effectiveness among persons with chronic health conditions. Assist Technol off J RESNA. 2017;29(4):181–187. doi:10.1080/10400435.2016.1219884
31. Anderson K, Willmore C, Doran E, Oki N, Vonnahme J, Gates BJ. Cognitive and literacy screening as predictors of ability to fill a pillbox using two pillbox assessment scoring methods. Consult Pharm J Am Soc Consult Pharm. 2014;29(5):304–316. doi:10.4140/TCP.n.2014.304
32. Schwartz J, Ballard DH. Feasibility of customized pillboxes to enhance medication adherence: a randomized controlled trial. Arch Phys Med Rehabil. 2022;103(12):2288–2295. doi:10.1016/j.apmr.2022.03.018
33. Xu M, Lo SHS, Miu EYN, Choi KC. Educational programmes for improving medication adherence among older adults with coronary artery disease: a systematic review and meta-analysis. Int J Nurs Stud. 2025;161:104924. doi:10.1016/j.ijnurstu.2024.104924
34. Wu Q, Zhang D, Zhao Q, et al. Effects of transitional health management on adherence and prognosis in elderly patients with acute myocardial infarction in percutaneous coronary intervention: a cluster randomized controlled trial. PLoS One. 2019;14(5):e0217535. doi:10.1371/journal.pone.0217535
35. Look KA, Stone JA. Medication management activities performed by informal caregivers of older adults. Res Soc Adm Pharm. 2018;14(5):418–426. doi:10.1016/j.sapharm.2017.05.005
36. Smith N. Cross-sectional profiling and longitudinal analysis: research notes on analysis in the longitudinal qualitative study, “negotiating transitions to citizenship. Int J Soc Res Methodol. 2003;6(3):273–277. doi:10.1080/1364557032000091888
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Dilemmas of Self-Management in Patients with Pulmonary Arterial Hypertension: A Descriptive Phenomenological Study
Cai J, Zhao N, Gao Y, Pan L, Yang Q
Patient Preference and Adherence 2026, 20:563550
Published Date: 17 January 2026
Roles and Influence of Nursing Assistants in Integrated Medical and Elderly Care Institutions: A Qualitative Study
Song A, Yan X, Yao L, Shao M, Zhou H, Zhou N, Si H, Zhou J, Li X, Li Y
Journal of Multidisciplinary Healthcare 2026, 19:576618
Published Date: 10 February 2026