Back to Journals » Journal of Multidisciplinary Healthcare » Volume 18
Understanding Colorectal Cancer Screening Barriers in Saudi Arabia: Insights From a Cross-Sectional Study
Authors Alhassan NS, Beyari MB ![]() , Aldeligan SH
, Aldeligan SH ![]() , Alqusiyer AA, Almutib SA, Alarfaj MA
, Alqusiyer AA, Almutib SA, Alarfaj MA ![]() , Abdulla MH, Bin Traiki T
, Abdulla MH, Bin Traiki T
Received 19 November 2024
Accepted for publication 28 February 2025
Published 5 March 2025 Volume 2025:18 Pages 1335—1344
DOI https://doi.org/10.2147/JMDH.S507481
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Pavani Rangachari
Noura S Alhassan,1 Mohammed Basem Beyari,2 Saleh Husam Aldeligan,2 Abdulaziz Abdulmuhsin Alqusiyer,2 Shatha Abdulaziz Almutib,2 Mohammed Ahmed Alarfaj,2 Maha Hamadien Abdulla,1 Thamer Bin Traiki1
1Department of Surgery, College of Medicine, King Saud University, Riyadh, Saudi Arabia; 2College of Medicine, King Saud University, Riyadh, Saudi Arabia
Correspondence: Mohammed Basem Beyari, Email [email protected]
Introduction: Colorectal cancer is a significant health concern in Saudi Arabia, ranking among the most common cancers and often presenting at advanced stages due to low early detection rates. Despite available screening tools, many cases are diagnosed late, leading to poor outcomes. The importance of early detection through screening cannot be overstated as it significantly improves prognosis and reduces mortality.
Methods: This study was conducted as a cross-sectional survey in Riyadh from January to July 2024. It aimed to assess awareness and barriers to colorectal cancer screening among the general public. A self-administered questionnaire was distributed, yielding 768 eligible responses after applying exclusion criteria.
Results: The results revealed that, while 88% of respondents were aware of colorectal cancer, only 16% had undergone screening tests primarily via colonoscopy. Significant barriers to screening included a lack of physician recommendation, absence of a comprehensive national screening program and fear of complications from colonoscopy. Females were more likely to experience embarrassment and fair of pain as barriers compared to males. Additionally, residents of rural areas faced challenges related to the avalanche of screening facilities.
Conclusion: These findings underscore the need for targeted public health interventions, including enhanced awareness campaigns and the development of a national CRC screening program to increase early detection rates and reduce the burden of colorectal cancer in Saudi Arabia.
Keywords: colon cancer screening, barriers, awareness
Introduction
Colorectal cancer (CRC) is the most prevalent cancer among Saudi males and ranks third among Saudi females.1 Globally, CRC is the third most common cancer, following lung and breast cancer, with an estimated 1.9 million cases diagnosed in 2022, it is also the second leading cause of cancer-related mortality worldwide,2 accounting for approximately 0.9 million deaths in the same year. In Saudi Arabia, CRC contributed to 3,750 new cases and 1,883 deaths in 2022, with 67% of the fatalities occurring in males.3 Despite the availability of screening tools, the majority of CRC cases in Saudi Arabia are diagnosed through clinical evaluation rather than proactive screening, a 2018 study revealed that only 5.64% of colorectal cancer (CRC) cases in the country were detected via screening modalities.4 Regular screening colonoscopies can significantly reduce the incidence of colorectal polyps.5 Studies indicate that they can increase polyp detection rates by 30–70%, depending on the population and frequency of screening.6 The early detection of CRC through screening methods such as the Fecal Immunochemical Test (FIT) or colonoscopy7 significantly reduces complications and mortality. While the survival rate for CRC is approximately 90% for localized cases, it drops to about 15% for metastatic cases,8 thus underscoring the importance of early detection. A study conducted in Saudi Arabia identified several significant barriers that deter individuals from undergoing CRC screening. The mean age was (39.79 ±12.49 years). The most prevalent obstacle, reported by 41% of participants, is the perception that colorectal cancer does not pose a substantial threat to one’s overall health, leading to a lack of urgency in seeking screening. Other notable barriers include the high cost associated with screening procedures (reported by 30%), the fear of pain or discomfort during the process (22%), and the embarrassment related to the invasive nature of tests like colonoscopies (18%). Additionally, there is a widespread fear of receiving a positive result, which contributes to the reluctance to undergo screening, with 25% of individuals citing this as a concern. A significant portion of the population, approximately 35%, also lacks awareness of where and how to access screening services, further exacerbating the low screening rates.9 Another Study conducted in 2024 in Saudi Arabia Evaluated the awareness and identified another set of barriers that did not share similar results with the previous study, the mean age was (32.9 ± 12.9 years). In this study (16.4%) participants had undergone colonoscopy/sigmoidoscopy, For the rest, the main barrier to undergoing early screening for colorectal cancer is that they had not thought about it (69.9%) had no symptoms (37.3%), lacked medical advice (17.7%), had no screening centers nearby (15.8%), feared colorectal cancer detection (10.9%), thought they were not at risk (7.1%), Said they have no time (6.2%), Said they have no money (5.6%).10 While comparing the results of the two studies, it was noticed the contradicting significance of the role of income between the two studies. To simplify their analysis, they were divided into two groups, those that earn less than 5000 Riyal a month and those who earn more between the first and second study, the percentage that earned less than 5000 were 11.9% and 48.6%, respectively. Interestingly, the study with higher average income thought that the high cost of the procedure was more significant as a barrier.11,12 Our study aims to conduct a comprehensive examination of the current level of awareness regarding colorectal cancer (CRC) within the Saudi Arabian community. Additionally, the study seeks to examine differences in perceived barriers between genders, including factors like feelings of embarrassment and issues with transportation. In addition, it seeks to identify and analyze the barriers that prevent individuals from participating in CRC screening programs. This study involved a larger sample size compared to previous studies and was conducted during a mall-based campaign in different areas of the Riyadh region as well as in the outpatient clinic setting of tertiary care centers. By understanding these obstacles, the study aims to provide insights that can inform targeted interventions and public health strategies to increase CRC screening uptake. Ultimately, the goal is to improve early detection rates and reduce the burden of colorectal cancer in Saudi Arabia.
Methodology
Our study is a cross-sectional study that was done on the general public in Riyadh, Saudi Arabia, on the awareness and barriers of colon cancer screening, the study was done from January 2024 till July 2024. Our study was conducted using a self-administered questionnaire, the questionnaire used was adopted from Alduraywish et al with modification.13 We collected demographic data including gender, age, marital status, education level, residence place then past medical and surgical history. Brief questions about colon cancer screening were asked, and those who had undergone screening were directed to a section to explore the reasons behind their decision. Finally, questions about barriers to colon cancer screening were divided into three parts: an overview of the general barriers preventing patients from screening, followed by sections addressing specific barriers for colonoscopy and fecal occult blood testing. To compare the CRC screening barriers between different groups, we analyzed the questionnaire’s Likert scale responses by specifying the responders’ level of agreement to each barrier and assigned points for each answer. Data collection was done through snowballing technique through social media and posters in different general public areas, and only participants 45 years of age or older were included. Institutional review board (IRB) (E-24-8988) was granted, and patients’ consent were taken at the beginning of the survey. Data were analyzed using JASP software (JASP Team (2024). JASP (Version 0.19.0) [Computer software]). Data were analyzed descriptively, and categorical variables were expressed as frequency by percentages and numbers of respondents.
Results
In a six-month period, we had 934 participants and 768 participants that were eligible after applying our inclusion criteria. Female responders accounted for 52% (n=403) compared to males 48% (n=365), and most of the participants’ age was in the range of 46 to 65 years with the dominance of “46–50 years” range by 33% (n=252). Almost all our participants were living in the city Riyadh 86% (n=660) while only 14% (n=108) was living in the rural areas of Riyadh. Most of the population were “married” 91% (n=698) and 7% (n=57) were “widows or divorced” as only 2% (n=13) were “single”. For education levels, “bachelors” dominated in the population with 49% (n=376) as “higher education studies” have came after it with 23% (n=176) after that “diploma”, “high”, “elementary”, “primary” schools then “illiterate” categories came with 11%, 12%, 3%, 1%,1% of the population, respectively. Monthly income for our population was mostly in the range of “5000–10000 SAR” with 42% (n=322) and 58% (n=446) in the other six categories. For the past medical history, 45% (n=343) have reported medical diseases in which diabetes mellitus type II and hypertension came as the most common two reported diseases with 22% (n=166) and 21% (n=160), respectively, then dyslipidemia, different respiratory conditions, different gastrointestinal (GI) conditions and thyroid dysfunction came at last with 6%, 5%, 3% and 2% respectively.Table 1
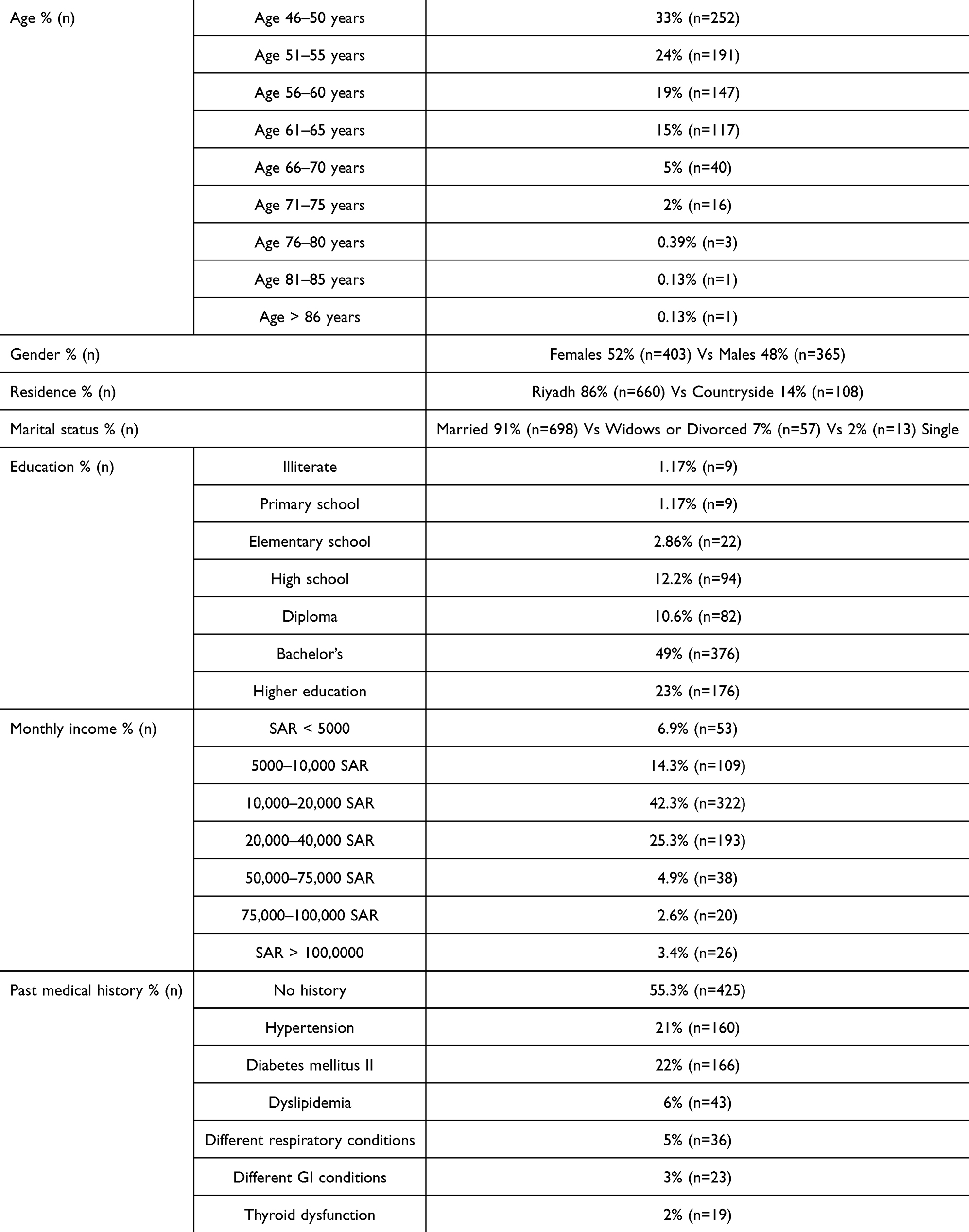 |
Table 1 Demographics and Past Medical History |
The second part of the survey assessed the participants’ knowledge about CRC. Family history of CRC was present in 21% (n=165) of our population, 77% of those were directed for CRC screening by their treating physicians, and 21% were directed to screening by awareness campaigns. About 44% (n=335) of our population are thinking of getting CRC screening when asked in our survey. Furthermore, only 16% (n=124) of our population have underwent CRC screening and most of them have got screened due to multiple causes, most commonly reported was “routine testing” 59% (n=73) then “blood per rectum”, “chronic constipation”, “pain while defecating”, “IBS”, “colonic mucosal inflammation”, “chronic diarrhea with mucus” came next with 16%, 13%, 8%, 8%, 7% and 5% respectively. Then, when asked about the number of times you have got screened for CRC, most of the participants were screened v Dr. Thamer Alturaikionly once 65% (n=80) while only 16% (n=20) were screened twice and the rest of the participants were either screened 3 times or 4 times and more, which were frequent in 10% and 8%, respectively. Colonoscopy was the most prevalent way of screening by 52% (n=65) and fecal blood sampling was 21% (n=26) but both combined were more frequent 24% (n=30) than fecal blood alone. Most participants underwent the screening in the age range of “41 to 50 years” 40% (n=50) then “51 to 60 years” age range was less common with 39% (n=48) and the rest of participants were screened in the age range of “less than 40 years”, “less than 60 years” and “41 till 60 years” with frequencies of 1%, 15% and 4% respectively.Table 2
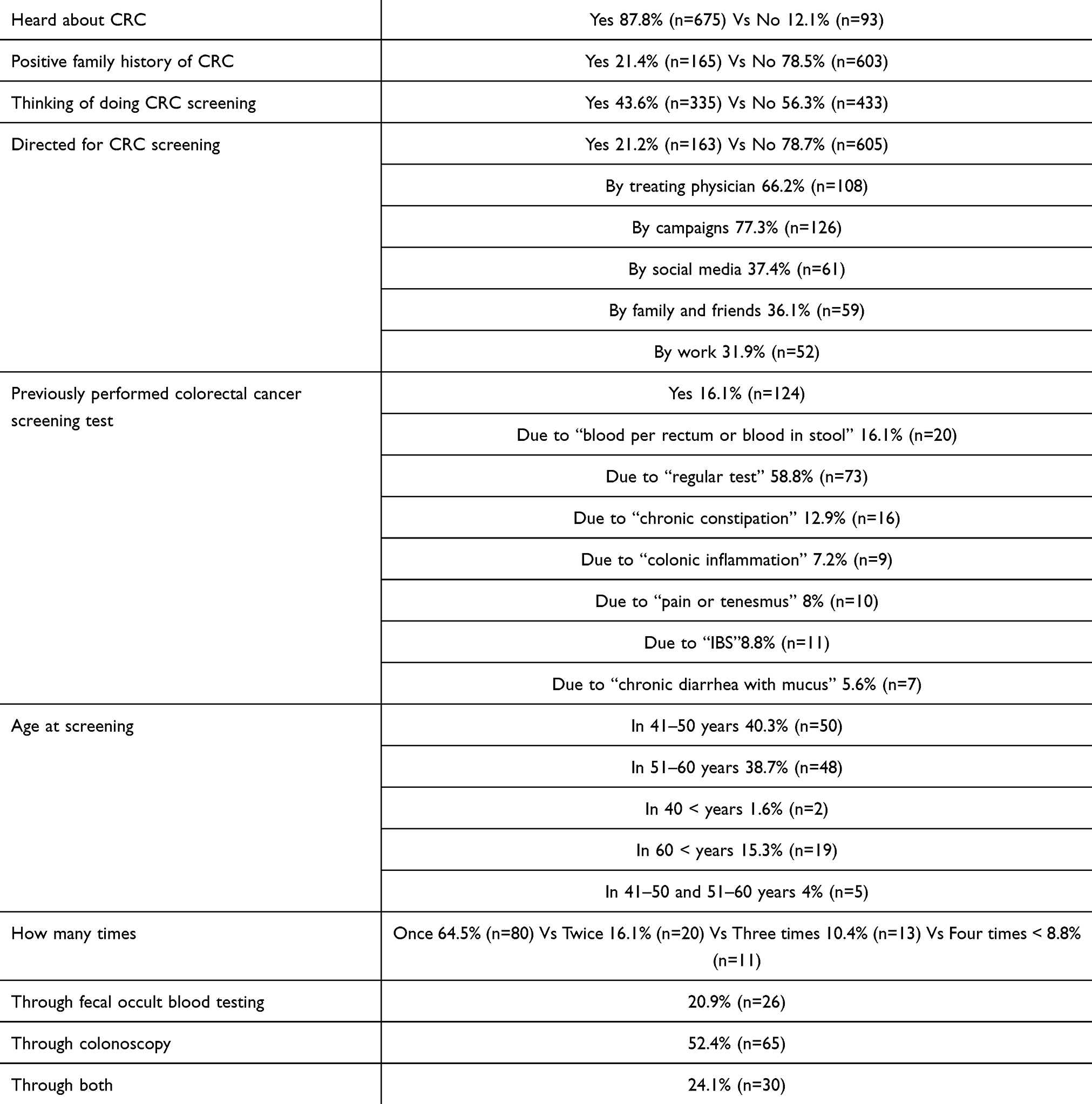 |
Table 2 Knowledge About CRC, CRC Screening and Previous CRC Screened Participants |
When asked about general barriers for CRC screening, 28% (n=213) have disagreed that their knowledge about CRC was a barrier. Then, participants’ responses showed that symptoms of CRC and spotting the signs of developing CRC were one of the highest reported barriers with 53% (n=408) and 64% (n=493) percentages of approval, respectively. Nonetheless, a very small percentage showed approval when asked about their beliefs in screening and if they believe in the importance of general screening 18% (n=141) which also was accompanied with a very low percentage of distrust in physicians 13% (n=105). In contrast, high percentages of approval were noticed when participants were asked about the “Absence of medical advice for CRC screening” as 31% (n=241) answered “strongly agree” and 27% (n=210) answered “agree”. When participants were asked about the lack of family and friends support as a barrier for screening, results were conflicting as 31% (n=235) answered “neutrall”, and 18% agreed compared to 29% disagreed. Similarly, participants did not agree on transportation as a barrier for screening with 36% (n=275) and 31% (n=238) answering “disagree” and “strongly disagree”, respectively. For the fear from general medical examinations and CRC screening results, our population showed a near to equal distribution in agreeing and disagreeing with a slight tendency toward disapproval, with the rest being on the neutral side. As for the fear from medical examination in general, only 37% (n=283) confirmed that barrier. Similarly, the fear from CRC results was confirmed by 35% (n=270) compared to the disapproval of 42% (n=322) with the rest of the population on the neutral side (22% (n=168) and 23% (n=176), respectively). In contrast, 51% of the population have agreed on the deficiency of a screening program for CRC screening, while 25% (n=195) were on the neutral side. 31% disagreed that CRC is a mean fate. Furthermore, most of our population did not know about fecal occult blood as a way for CRC screening when compared to colonoscopy (59% Vs 32%, respectively), most of the population answered on being shy or gross from giving fecal samples by disagreement 68% and 70%, respectively. Then, to determine the population’s barriers for screening, we have calculated the grand mean for general barriers, which was 2.0575, but for screening barriers through FOBT, the grand mean was 2.41, and for colonoscopy, it was 2.237, then each statement mean’s answers were calculated and compared by the grand means for making the decisions for these statements.Table 3
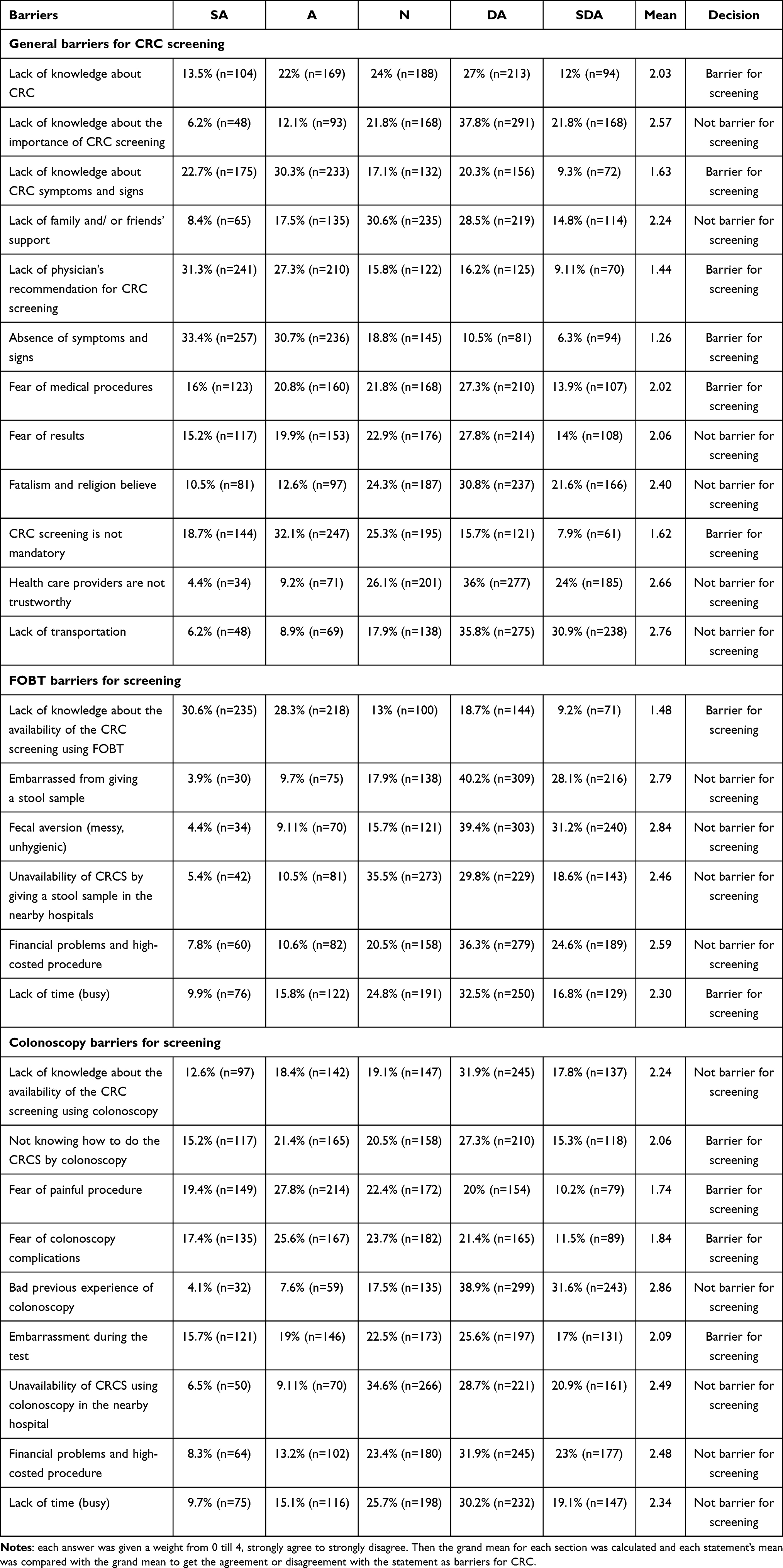 |
Table 3 Barriers for General Screening, CRC Colonoscopy Screening and CRC Fecal Blood Screening |
Nonetheless, we have found statistical significance when we compared barriers between genders, females had transportation, embarrassment in both FOBT and colonoscopy as a barrier when compared to males (p<0.001). Also, females were found to have fear from painful colonoscopy or the complications of it compared to males with statistical significance (p<0.001). Then, when comparing urban area residents compared to Riyadh residents, transportation, availability of scopes and FOBT kits were of statistically significant associations as barriers for screening (p<0.05). Surprisingly, family history of CRC was not associated with fear from screening or was counted as a barrier for screening (p=0.5). An association was also found in participant who have heard about CRC compared to those who did not have as lack of knowledge about CRC, lack of knowledge about the importance of CRC screening, lack of knowledge about the availability of CRC screening using FOBT and using colonoscopy were all a statistical significance barriers for screening (p<0.01). Moreover, participants who do not want to get screened for CRC reported having fear from complications and pain of colonoscopy as barriers for screening (p<0.001). In addition, they have reported the lack of medical advice for CRC screening as a significant barrier (p<0.05). Furthermore, the lack of a formal CRC screening program was also a significant barrier for participants who did not want to undergo CRC screening (p<0.001).
Discussion
In our study we have excluded participants who are less than 45 years old as they are not the targeted population with CRC screening. The American Cancer Society recommends that people at average risk of colorectal cancer (people with no personal or family history of colorectal cancer or IBD) start regular screening at age 45.14 Most of our participants were below 65 years old. That could be attributed to the nature of the questionnaire using google forms as paper-based surveys could have resulted in more participants from high age groups. As expected, due to the nature of our community as most of the population get married before 45 years old most of our population have been married with a very small percentage of singles over 45 years old. Moreover, our population was well educated as mostly bachelor’s and post graduate degrees were reported by over half of the population in addition to our population being mostly middle class as 42% of the population had a monthly income of 10000 SAR. Due to the nature of CRC and the prevalence of cancer especially CRC in Saudi Arabia almost all of the population have heard about it and family history of CRC was prevalent by 21% which could be due the familial types that are present in Saudi Arabia and the high prevalence of it.1,15 However, only 21% of the population were directed to CRC screening although all of them were eligible for screening and the most common way of direction surprisingly was not the treating physician but awareness campaigns. Although 21% were directed only 16% have undergone screening and colonoscopy was the most common way of testing. Half of the participants have undergone CRC screening as a regular test which proves the rise of CRC in Saudi Arabia for early detection of CRC.1 The percentage of population undergoing screening is almost exactly similar to the study done in Al-qunfudah (16.4%), assuring the accuracy of this number among the Saudi population.12 Also more than 40% are thinking of undergoing CRC screening but have not yet. This could be attributed to the barriers that were found in our study. Although CRC is prevalent and on the rise in the Middle East and Saudi Arabia still the lack of knowledge about CRC and the lack of its symptoms were found to be a huge barrier against the screening and early detection of CRC.11,13 The lack of physician’s recommendation for CRC screening was also found to be a huge barrier for screening that was accompanied with the lack of a formal national CRC screening program. In contrast to the trust in healthcare professionals, the fear of medical procedures was found to be a barrier which could be overcome by the rise of CRC screening awareness campaigns and explanations about the ways of screening and the details of these procedures. Despite the conservative nature of our Saudi population, embarrassment of FOBT and fecal aversion was not found to be a barrier for screening in the general population in contrast to embarrassment from colonoscopy. However, statistical significance was found when comparing between genders as females had the embarrassment of both FOBT and colonoscopy as barriers that prevent them from CRC screening. Also, fear of pain during colonoscopy and its complications were found as general barriers that prevent the population from screening in both males and females as this matches up with the lack of knowledge in the way that colonoscopy is used for CRC screening and could explain these two as barriers. But the difference between males and females in fear from pain during colonoscopy and its complications as barriers were found to be statistically significant as females have that as barriers more than males. As expected the residents of rural areas had the lack of FOBT kits and scopes as a huge and main barrier for CRC screening. We could get over that issue with the development of a national CRC screening program in which centers could be found country-wide. Despite our Saudi community being a religious and conservative community, believing in fate and having a family history of CRC was not found to be a barrier for screening as this tells us that our population is favoring CRC screening rather than fearing such procedures. In contrast, colon capsule video endoscopy (CCVE) is not widely used in Saudi Arabia as a screening tool for colon cancer primarily due to its limited sensitivity and specificity, which may result in missed lesions, particularly smaller polyps. The capsule can sometimes fail to visualize the entire colon, leading to incomplete examinations, and it cannot perform therapeutic interventions like polyp removal or biopsies, necessitating follow-up colonoscopy if abnormalities are detected. Additionally, CCVE can be more expensive than traditional methods, and established guidelines from major health organizations do not currently recommend CCVE as a primary screening method. Many patients may prefer the familiarity and immediate options available through traditional colonoscopy. The study identified several critical barriers to CRC screening. Actions can be taken to eliminate or reduce these barriers. Among these barriers, the lack of physician recommendation was the most notable one; by implementing mandatory CRC screening, counselling in primary care clinics for the targeted population could improve CRC screening rates. On a broader scale, implementing a nationwide screening program and deploying mobile screening units in rural areas could enhance accessibility and substantially increase participation rates.
Limitations
This study has several limitations that should be considered when interpreting the results. First, the cross-sectional design limits the ability to establish causality between identified barriers and low screening rates for CRC. Second, the study population was primarily composed of residents from Riyadh, which may not fully represent the broader Saudi Arabian population, especially those in rural areas or other regions with different socio-economic and cultural backgrounds. Additionally, data collection was conducted via an online self-administered questionnaire, which may have introduced selection bias, as it likely excluded individuals without internet access or those less familiar with digital platforms. The reliance on self-reported data could also lead to recall bias or social desirability bias, where participants might underreport or overreport their behaviors and barriers to screening. Furthermore, the exclusion of participants under the age of 45, though consistent with current CRC screening guidelines, limits the study’s ability to capture perspectives from younger individuals who might be at risk due to family history or other factors. Finally, while the study identified significant barriers to CRC screening, it did not explore the potential influence of cultural factors in depth, which could be a critical aspect in understanding screening behaviors in Saudi Arabia. These limitations suggest that further research, including longitudinal studies and qualitative assessments, is necessary to provide a more comprehensive understanding of the barriers to CRC screening in the Saudi population.
Conclusion
This study highlights the significant gaps in awareness and participation in CRC screening within the Saudi Arabian population, particularly among females and residents of rural areas. While knowledge of CRC is widespread, screening uptake remains low due to barriers such as the lack of physician recommendation, absence of a formal screening program, and fear of colonoscopy-related pain and complications. Addressing these barriers through targeted public health strategies, including the implementation of a national screening program and increased awareness campaigns, is essential for improving early detection rates and reducing the burden of CRC in Saudi Arabia. Our recommendations include making CRC screening discussions a standard part of primary care visits, encouraging doctors to routinely discuss screening with patients over 45 to increase awareness and rates. Additionally, expanding accessibility through a national program by establishing a government-supported initiative with well-equipped centers and mobile clinics can ensure availability, especially in rural areas. Developing female-focused educational programs that address unique concerns, such as embarrassment and fear, through culturally sensitive and female-led initiatives can improve participation. Finally, leveraging digital platforms to boost awareness by engaging the public through social media, online health resources, and virtual consultations can encourage more individuals to undergo screening.
Data Sharing Statement
The data sets generated and/or analyzed during the current study are not publicly available but are available from the corresponding author on reasonable request.
Ethics Approval and Consent to Participate
The study was approved by the Institutional Review Board at the College of Medicine, King Saud University, Ref. No. (E-24-8988). This study was conducted in accordance with the declaration of Helsinki. All participants provided written informed consent prior to the commencement of the study.
Funding
The authors extend their appreciation to the deanship of scientific research, King Saud University for funding through the Vice Deanship of Scientific Research; Research Chair of Colorectal cancer.
Disclosure
The authors declare that they have no competing interest in this work.
References
1. Almatroudi A. The incidence rate of colorectal cancer in Saudi Arabia: an observational descriptive epi- demiological analysis. Int J Gen Med. 2020;13:977. PMID: 33149661. doi:10.2147/IJGM.S277272
2. Roshandel G, Ghasemi-Kebria F, Malekzadeh R. Colorectal cancer: epidemiology, risk factors, and prevention. Cancers. 2024;16(8):1530. PMID: 38672612; PMCID: PMC11049480. doi:10.3390/cancers16081530
3. Sung H, Ferlay J, Siegel RL, et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2021;71(3):209–249. PMID: 33538338. doi:10.3322/caac.21660
4. Al-Hajeili M, Abdulwassi H, Alshadadi F, Alqurashi L, Idriss M, Halawani L. Assessing knowledge on preventive colorectal cancer screening in Saudi Arabia: a cross-sectional study. J Fam Med Primary Care. 2019;8:3140. doi:10.4103/jfmpc.jfmpc_508_19
5. Ferlay J, Ervik M, Lam F, et al. Global cancer observatory: cancer today. Lyon, France: International Agency for Research on Cancer. Available from: https://gco.iarc.fr/today.
6. Khoja A, Aljawadi M, Al-Shammari SA, et al. Utilization of colorectal cancer screening among Saudi elderly population: a study from the Saudi National Survey for elderly health. Asian Pac J Cancer Prev APJCP. 2018;19:3401–3407. doi:10.31557/APJCP.2018.19.12.3401
7. Triantafillidis JK, Vagianos C, Malgarinos G. Colonoscopy in colorectal cancer screening: current aspects. Indian J Surg Oncol. 2015;6(3):237–250. Epub 2015 Apr 12. PMID: 27217671; PMCID: PMC4856683. doi:10.1007/s13193-015-0410-3
8. Zhang J, Chen G, Li Z, et al. Colonoscopic screening is associated with reduced colorectal cancer incidence and mortality: a systematic review and meta-analysis. J Cancer. 2020;11(20):5953–5970. PMID: 32922537; PMCID: PMC7477408. doi:10.7150/jca.46661
9. Almadi MA, Barkun AN. Initial guidelines for colorectal cancer screening in Saudi Arabia: a beginning. Ann Saudi Med. 2015;35(5):341–342. doi:10.5144/0256-4947.2015.341
10. Fayadh MH. Colorectal cancer in Abu Dhabi, UAE - initial data 2014–2016. Colorectal Cancer. 2016;2(3). doi:10.21767/2471-9943.100024
11. Imran M, Baig M, Alshuaibi RO, Almohammadi TA, Albeladi SA, Zaafarani FTM. Knowledge and awareness about colorectal cancer and barriers to its screening among a sample of general public in Saudi Arabia. PLoS One. 2023;18(8):e0290269. PMID: 37611015; PMCID: PMC10446202. doi:10.1371/journal.pone.0290269
12. Aldabali F, Alotibi B, Alkhaldi A, et al. Evaluation of public awareness, knowledge, and attitudes about colorectal cancer screening among the general population in Al-qunfudah. Am J Cancer Res. 2024;14(4):1926–1934. PMID: 38726260; PMCID: PMC11076243. doi:10.62347/XKUW3822
13. Alduraywish SA, Altamimi LA, Almajed AA, et al. Barriers of colorectal cancer screening test among adults in the Saudi population: a cross-sectional study. Preventive Med Rep. 2020;20:101235. doi:10.1016/j.pmedr.2020.101235
14. Colorectal Cancer Guideline |how Often to Have Screening Tests. American CancerSociety. https://www.cancer.org/cancer/types/colon-rectal-cancer/detection-diagnosis-staging/acs-recommendations.html.
15. Jasperson KW, Tuohy TM, Neklason DW, Burt RW. Hereditary and familial colon cancer. Gastroenterology. 2010;138(6):2044–2058. PMID: 20420945; PMCID: PMC3057468. doi:10.1053/j.gastro.2010.01.054
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.