Back to Journals » Clinical Ophthalmology » Volume 20
Understanding Capsular Contraction and IOL Decentration in Toric and EDOF Lenses: Clinical and Biomechanical Insights
Received 23 March 2026
Accepted for publication 30 March 2026
Published 2 April 2026 Volume 2026:20 611339
DOI https://doi.org/10.2147/OPTH.S611339
Checked for plagiarism Yes
Editor who approved publication: Dr Sotiria Palioura
Bharat Gurnani,1 Kirandeep Kaur2
1Department of Cataract, Cornea and Refractive Surgery, Gomabai Netralaya and Research Centre, Neemuch, Madhya Pradesh, 458441, India; 2Department of Cataract, Pediatric Ophthalmology and Strabismus, Gomabai Netralaya and Research Centre, Neemuch, Madhya Pradesh, 458441, India
Correspondence: Bharat Gurnani, Department of Cataract, Cornea and Refractive Surgery, Gomabai Netralaya and Research Centre, Neemuch, MP, 458441, India, Tel +919080523059, Email [email protected]
Capsular contraction syndrome (CCS) continues to pose challenges in the era of premium intraocular lenses, where optical precision is crucial for success. Toric and extended depth-of-focus (EDOF) IOLs are particularly sensitive to small positional shifts; even minor decentration or tilt can degrade image quality, induce astigmatism, and cause unwanted visual phenomena.1 While advances in surgical technique, IOL biomaterials, and capsule management have improved consistency, the interplay between the biology of lens epithelial cell (LEC) proliferation and the biomechanics of the capsular bag still determines long-term stability.2 CCS develops when residual LECs on the anterior capsule transform into myofibroblasts that contract circumferentially, causing centripetal shrinkage of the capsule. Ideally, these forces are evenly distributed, maintaining lens centration.3 However, any asymmetry due to zonular laxity, incomplete cortical clean-up, or uneven capsulorhexis overlap can create local variations in tension that distort the IOL’s position. Even a few degrees of tilt or fractions of a millimetre of decentration can meaningfully alter optical performance, particularly in multifocal or toric lenses.4 From a biomechanical perspective, the capsular bag may be conceptualized as an elastic shell under competing forces: radial tension (Tz) from the zonules and circumferential contraction force (Fc) from the anterior capsule. The net force acting across the equator is expressed as:5
When contraction becomes asymmetric such that Fc(θ1)≠Fc(θ2), a torque is generated around the IOL’s center, described by

This torque induces a tilt angle (α) proportional to the rotational stiffness (kr) of the IOL–capsule system:

For single-piece hydrophobic acrylic IOLs, kr averages 2.5 × 10⁻4 N·m/degree. Modeling shows that a 15% asymmetry in the capsular contraction radius (Δr/r) can cause a tilt of approximately 4.5°, enough to reduce modulation transfer function by 20% in an EDOF optic. To visualize this effect geometrically, the capsule equator can be approximated as an ellipse with major and minor axes a and b. The eccentricity of the ellipse determines the optical decentration (δ) according to

where θ represents the axis of maximum contraction. For example, if a=5.0 mm and b=4.7 mm, the resulting decentration (δ) is approximately 0.3 mm equivalent to a 6° rotation in a 2.25 D toric IOL.6 Such small geometric deviations can have meaningful clinical consequences, producing astigmatic residuals, loss of near focus, or asymmetric halos in EDOF designs. Clinically, these biomechanical distortions manifest as predictable optical degradation.7 Every 5° of toric IOL rotation causes about a 17% loss of astigmatic correction; a rotation of 30° effectively nullifies the toric benefit. Similarly, an EDOF lens decentred by more than 0.3 mm or tilted by more than 5° exhibits higher-order aberrations chiefly coma that reduce contrast sensitivity, particularly under mesopic conditions.8 Patients often describe fluctuating vision, ghosting, or localized blur, which can mimic neuroadaptation failure or refractive surprise. Multiple factors influence the degree of capsular contraction. Systemic and ocular conditions such as diabetes, pseudoexfoliation, high myopia, or connective tissue disorders can alter the biomechanical integrity of the zonular apparatus.9 Intraoperative factors such as creating a small (<4.8 mm) capsulorhexis, incomplete overlap of the optic, or inadequate cortical clean-up further predispose to focal fibrosis. Conversely, maintaining a rhexis of 5.0–5.2 mm and ensuring a uniform 360° optic overlap help distribute contraction forces evenly. Anterior capsule polishing reduces the LEC substrate available for fibrotic transformation, and thorough cortical aspiration minimizes postoperative fibrosis.
Mathematical modeling underscores the relevance of these observations. Using a simplified finite-element approach, the relationship between equatorial contraction and optic tilt can be expressed as

where E represents the elastic modulus of the contracting capsule (approximately 0.45 MPa), R the mean equatorial radius (around 5 mm), and Δr the contraction asymmetry. Substituting these values yields tilt angles in the range of 3–6°, which closely align with clinical data from anterior segment OCT studies. In daily practice, several measurable parameters can predict postoperative instability. A capsulorhexis–optic overlap ratio of less than 0.2 suggests uneven tension and correlates with anterior capsule area reduction exceeding 15% within one month postoperatively.10 The anterior capsule area reduction index (ARI) can be calculated as
where A0 and At represent the pre- and postoperative anterior capsule areas. An ARI greater than 15% serves as a reliable early indicator of progressive CCS. Advanced imaging techniques such as Scheimpflug tomography, anterior segment OCT, or Purkinje analysis can quantify IOL tilt (>5° considered significant) and decentration (>0.3 mm considered symptomatic). Prevention begins with surgical mindfulness.11 A well-sized, symmetric rhexis ensures balanced force distribution. Gentle capsule polishing and the use of a capsular tension ring (CTR) in high-risk eyes—such as those with pseudoexfoliation, post-trauma, or long axial length—can mechanically stabilize the equator. CTRs redistribute zonular tension, counteract local contraction, and reduce tilt.12 Pharmacologic adjuncts also play a role. Intraoperative corticosteroid irrigation or postoperative use of nonsteroidal anti-inflammatory agents can attenuate TGF-β–driven fibrosis. Emerging research into anti-TGFβ and anti-EMT (epithelial-mesenchymal transition) agents may offer targeted inhibition of myofibroblast formation in the future. Material choice further influences outcomes.13 Hydrophobic acrylic IOLs with square-edged optics, textured haptics, and stable angulation exhibit better resistance to asymmetric deformation than hydrophilic materials. For toric and EDOF optics, design symmetry and higher torsional rigidity are essential. Some new-generation IOLs incorporate micro-grooved or step-lock haptics that resist rotational drift and limit postoperative decentration. Despite best practices, late contraction can still occur years after surgery.14 Vigilant follow-up with anterior segment imaging helps detect early tilt or capsule phimosis. Nd: YAG anterior capsulotomy can be performed to release focal contraction, while severe cases may require IOL–CTR complex exchange. Early recognition remains the key to preserving optical quality before significant distortion occurs. Ultimately, understanding the mathematical and mechanical underpinnings of capsular contraction bridges the gap between physics and clinical ophthalmology. The equations describing torque, tilt, and decentration quantify what surgeons often observe intuitively: even a small imbalance in capsular behavior can translate into significant optical compromise. Integrating this knowledge into surgical planning, IOL selection, and postoperative care can reduce unpredictable refractive outcomes and improve patient satisfaction in premium cataract surgery (Figures 1 and 2) (Table 1).15
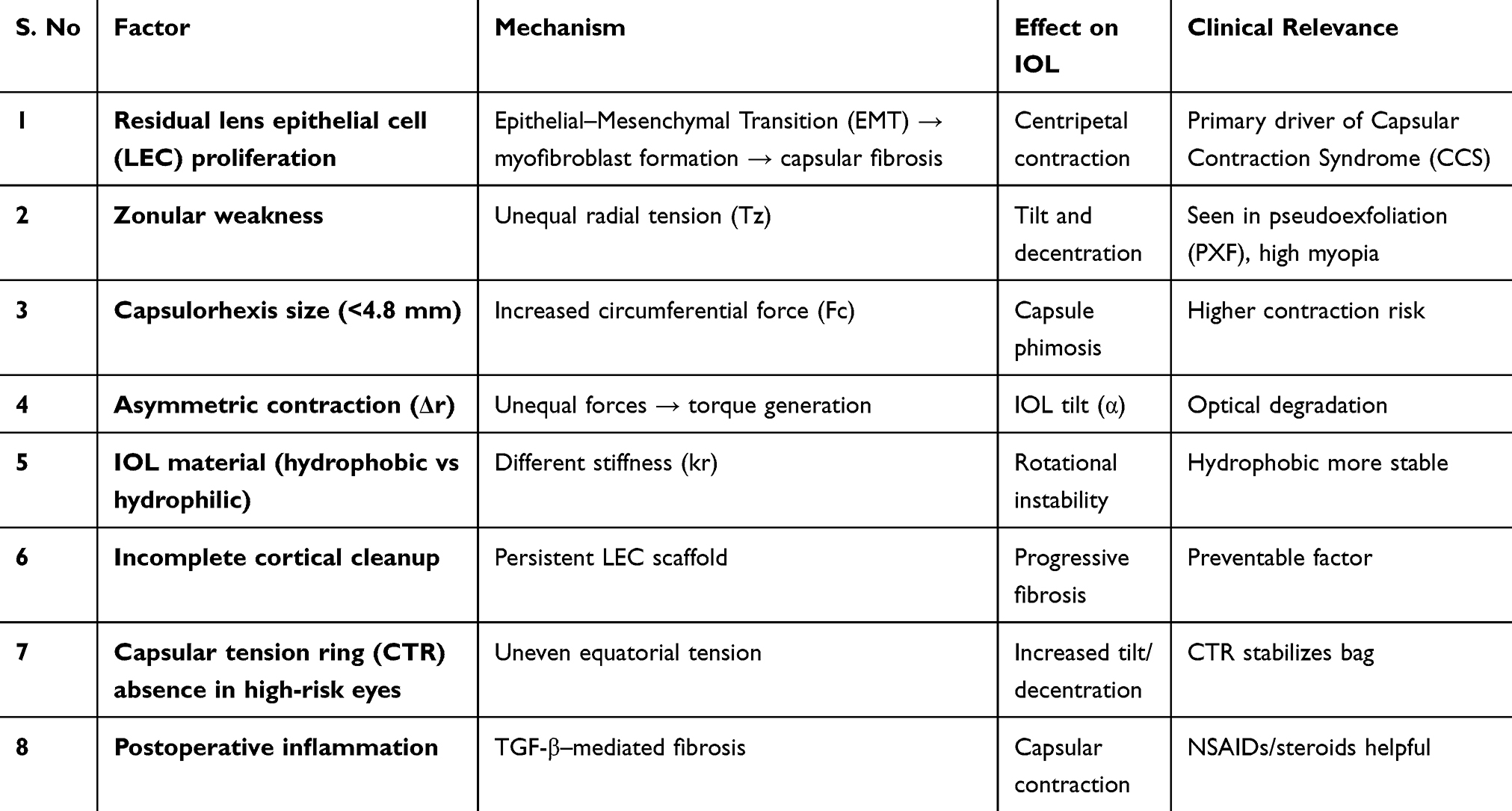 |
Table 1 Depict the Biomechanical Factors Influencing Capsular Contraction and IOL Stability |
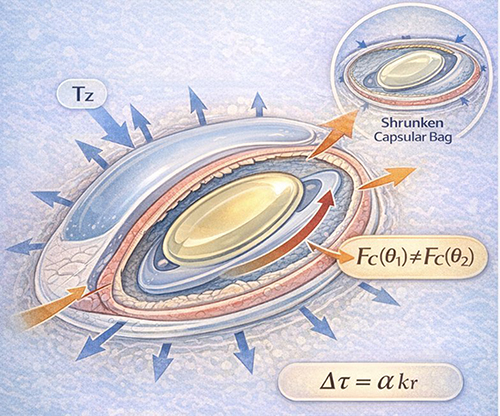 |
Figure 1 Schematic representation of biomechanical forces in capsular contraction syndrome. Radial zonular tension (Tz) and circumferential contraction forces (Fc) act on the capsular bag. Asymmetric contraction generates torque, leading to intraocular lens (IOL) tilt and decentration. |
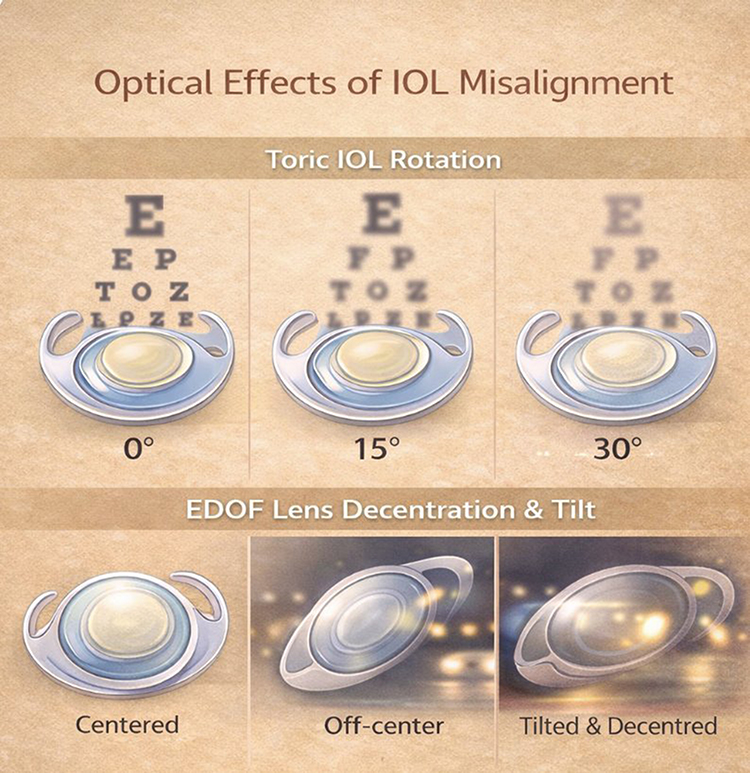 |
Figure 2 Optical consequences of intraocular lens misalignment. Toric IOL rotation results in progressive loss of astigmatic correction, with complete loss at 30°. EDOF lens decentration and tilt induce higher-order aberrations, particularly coma, leading to reduced contrast sensitivity and visual disturbances. |
Funding
There is no funding to report.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Lan P, Nie L, Zhao L. Anterior capsular contraction syndrome in cataract surgery: a review of challenges and solutions. Med Sci Monit. 2025;31:e949046. doi:10.12659/MSM.949046
2. Pérez-Vives C. Biomaterial influence on intraocular lens performance: an overview. J Ophthalmol. 2018;2018:2687385. doi:10.1155/2018/2687385
3. Huang F, Tong W, Wang D, Guan W, Zhang Z, Zhao YE. Impact of anterior capsule polishing on capsule opacification and capsule Bend after age-related cataract surgery. J Cataract Refract Surg. 2024;50(6):599–5. doi:10.1097/j.jcrs.0000000000001407
4. Bisevac J, Anisimova NS, Nagymihály R, et al. Long-term myofibroblast persistence in the capsular bag contributes to the late spontaneous in-the-bag intraocular lens dislocation. Sci Rep. 2020;10(1):20532. doi:10.1038/s41598-020-77207-7
5. Lin X, Ma D, Yang J. Exploring anterion capsular contraction syndrome in cataract surgery: insights into pathogenesis, clinical course, influencing factors, and intervention approaches. Front Med. 2024;11:1366576. doi:10.3389/fmed.2024.1366576
6. Roshdy MM, Riad RF, Morkos FF, Hassouna AK, Wahba SS. Effect of a single-piece aspheric hydrophobic acrylic intraocular lens design on centration and rotation. J Cataract Refract Surg. 2013;39(3):408–413. doi:10.1016/j.jcrs.2012.09.020
7. Álvarez-García MT, Fuente-García C, Muñoz-Puyol C, Piñero DP. Clinical outcomes with extended depth of focus intraocular lenses in cases in which multifocal lenses are not primarily recommended. J Ophthalmol. 2023;2023:8814627. doi:10.1155/2023/8814627
8. Gargallo D, Remón L, Ares J, Castro-Alonso FJ. The influence of rotational error and axial shift of toric intraocular lenses on residual astigmatism. PLoS One. 2024;19(12):e0311566. doi:10.1371/journal.pone.0311566
9. Ljubic A, Trajkovski V, Stankovic B, et al. Systemic and ophthalmic manifestations in different types of refractive errors in patients with down syndrome. Medicina. 2022;58(8):995. doi:10.3390/medicina58080995
10. Li S, Hu Y, Guo R, et al. The effects of different shapes of capsulorrhexis on postoperative refractive outcomes and the effective position of the intraocular lens in cataract surgery. BMC Ophthalmol. 2019;19(1):59. doi:10.1186/s12886-019-1068-3
11. Li L, Wang K, Yan Y, Song X, Liu Z. Research on calculation of the IOL tilt and decentration based on surface fitting. Comput Math Methods Med. 2013;2013:572530. doi:10.1155/2013/572530
12. Feng L, Vidal CC, Weeber H, Koopman B, Sajadi SB, Rozema JJ. Effects of capsulorhexis size and position on post-surgical IOL alignment. Sci Rep. 2024;14(1):31132. doi:10.1038/s41598-024-82377-9
13. Yang HW, Lee SA, Shin JM, Park IH, Lee HM. Glucocorticoids ameliorate TGF-β1-mediated epithelial-to-mesenchymal transition of airway epithelium through MAPK and Snail/Slug signaling pathways. Sci Rep. 2017;7(1):3486. doi:10.1038/s41598-017-02358-z
14. Borkenstein AF, Borkenstein EM. Geometry of acrylic, hydrophobic iols and changes in haptic-capsular bag relationship according to compression and different well diameters: a bench study using computed tomography. Ophthalmol Ther. 2022;11(2):711–727. doi:10.1007/s40123-022-00469-z
15. Öztürk C, Cevher S, Duran M, Üçer MB, Töngüş O. Anterior segment changes following Nd: YAG laser posterior capsulotomy: a quantitative ultrasound biomicroscopy study. Lasers Med Sci. 2025;40(1):302. doi:10.1007/s10103-025-04555-z
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.