Back to Journals » Patient Preference and Adherence » Volume 19
Uncertainty Dilemma and Service Demands During the Discharge Transition Period for Elderly Patients with Comorbidities: A Qualitative Study
Authors Wu X ![]() , Lv J, Feng Y, Qiu T
, Lv J, Feng Y, Qiu T ![]() , Liang T, Yan P
, Liang T, Yan P
Received 20 August 2025
Accepted for publication 11 November 2025
Published 17 November 2025 Volume 2025:19 Pages 3657—3671
DOI https://doi.org/10.2147/PPA.S561781
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Xing Wu,1,2 Jiahui Lv,3 Yajuan Feng,3 Tian Qiu,4 Tingting Liang,5 Ping Yan3
1Administrative Management Department, The Seventh Affiliated Hospital of Xinjiang Medical University, Urumqi, Xinjiang, People’s Republic of China; 2Health Care Research Center for Xinjiang Regional Population, Urumqi, Xinjiang, People’s Republic of China; 3School of Nursing, Xinjiang Medical University, Urumqi, Xinjiang, People’s Republic of China; 4General Practice Department, The Seventh Affiliated Hospital of Xinjiang Medical University, Urumqi, Xinjiang, People’s Republic of China; 5Department of Cardiology, The Seventh Affiliated Hospital of Xinjiang Medical University, Urumqi, Xinjiang, People’s Republic of China
Correspondence: Xing Wu, Administrative Management Department, The Seventh Affiliated Hospital of Xinjiang Medical University, Urumqi, Xinjiang, People’s Republic of China, Email [email protected]
Purpose: This study aims to explore the challenges and service needs faced by elderly patients with comorbidities during the transition from hospital discharge, and the study is proposing a way forward for transitioning the elderly patients with multimorbidity.
Patients and Methods: A purposive sampling approach was employed to select 12 elderly patients with comorbidities from the geriatric departments of two tertiary hospitals in the Xinjiang region between November 2024 and March 2025. A phenomenological research design was utilized to conduct semi-structured interviews with participants. Data were analyzed using the seven-step Colaizzi method for phenomenological analysis, supported by Nvivo 15.0 software.
Results: Three main themes and twelve subthemes were identified: (1) Support System Dilemma, (2) Guidance Needs for Discharge Information, (3) Demand for Continuous Services and Safeguards in Medical Institutions.
Conclusion: Elderly patients with comorbidities experience multiple challenges and unmet needs during the discharge transition period. Clinically, it is essential to establish a multidisciplinary transitional care team, conduct comprehensive pre-discharge assessments, enhance system support and polypharmacy management, develop tailored discharge guidance plans to improve the quality of life during the post-discharge transition period.
Keywords: elderly, comorbidity, discharge transition period, uncertain predicament, service needs, qualitative research
Introduction
With the intensification of global aging, multimorbidity among older adults has become increasingly prevalent, emerging as a critical factor threatening their health and quality of life.1 Multimorbidity is defined as the coexistence of two or more chronic diseases or health conditions in an individual.2 Evidence indicates that the prevalence of multimorbidity among older adults in China reaches 65.14%, with affected individuals facing a 44% higher mortality risk compared to those without multimorbidity. Furthermore, each additional chronic condition increases the risk of death by approximately 20%.3,4 Older patients with multimorbidity often require long-term and continuous medical care and rehabilitation support due to age-related physiological decline, complex treatment regimens, and the interplay among multiple concurrent conditions.5,6 China’s healthcare system is centered on a three-tiered service framework, which has established a tiered care model characterized by “primary-level initial diagnosis, bidirectional referrals, differentiation between acute and chronic disease management, and coordinated interactions across different levels”.7 Within this structure, primary healthcare institutions—including community hospitals—serve fundamental roles such as first-contact care and chronic disease management. Patients can purchase medications at these facilities out-of-pocket, with reimbursement available for drugs listed in the national medical insurance directory according to policy provisions. As a foundational component of the three-tiered system, community hospitals differ significantly from tertiary general hospitals. The former primarily focus on managing common illnesses, health monitoring, and rehabilitative nursing, offering localized services with high accessibility. In contrast, tertiary hospitals specialize in treating complex and critical cases, advancing medical research, and providing clinical education, supported by more comprehensive medical resources. Functional complementarity between these two tiers is facilitated through an established bidirectional referral mechanism.8
Within the context of this healthcare system, elderly patients with comorbidities frequently require coordinated care between tertiary general hospitals and community healthcare facilities throughout their diagnostic and treatment processes. The discharge transition period—serving as a critical juncture linking in-hospital treatment and outpatient rehabilitation—represents the most vulnerable segment of the care continuum and a pivotal point for inter-institutional coordination. During this phase, patients with complex multimorbidity face significant challenges, including adjustments to new models of medical care and lifestyle changes.9,10 They are also susceptible to medication discrepancies, dependency on nursing support, fragmented continuity of care, and inadequate discharge planning.11–14 Consequently, their service needs become increasingly diverse and nuanced. These issues may compromise the quality of post-discharge transitions, increase the risk of hospital readmission, and substantially impair patients’ quality of life.
Currently, research on the challenges faced by elderly patients during the discharge transition period in China has primarily focused on single diseases or specific patient populations,15,16 with relatively limited attention given to elderly patients with comorbidities. Donghui H et al17 investigated the collection of medical and nursing records for hospitalized patients with comorbidities and conducted a statistical analysis of their post-discharge continuing care needs. However, the assessment framework employed was narrow in scope, increasing the risk of overlooking critical information and failing to capture patients’ latent or unexpressed needs. Bian Jiahong et al18 conducted interviews with elderly patients with comorbidities to evaluate their home care requirements but did not sufficiently address broader challenges encountered during the discharge transition, such as psychological and social difficulties. To date, there remains a significant gap in understanding the subjective experiences, perceived challenges, and service needs of elderly patients with comorbidities during this transitional phase, indicating a lack of comprehensive research in this area. Meleis’ Transition Theory19 provides a conceptual framework for understanding how individuals move from one life state to another. Its core components—perception of transition, preparedness, and coping ability—offer valuable insights for interpreting and predicting individual transition experiences.Therefore, guided by Meleis’ Transition Theory, this study conceptualizes the process of elderly patients with comorbidities returning home after hospitalization as a transitional period. Using qualitative research methods, semi-structured interviews were conducted with patients during this phase to explore the manifestations of uncertainty they experience and their core service needs. The findings aim to inform the optimization of continuity mechanisms within the healthcare system and provide evidence for the development of personalized intervention strategies.
Materials and Methods
Participants
We employed the Meleis’ transition theory framework to guide both participant selection and data interpretation.Eligible participants were elderly patients with comorbidities recruited from the geriatrics departments of two tertiary general hospitals in the Xinjiang region between November 2024 and March 2025.Research participants were selected using purposeful sampling. To achieve maximum sample differentiation, subjects with varying marital statuses, educational levels, and comorbidities were included. The sample size was determined with reference to the recommendations for qualitative research proposed by Hennink20 et al, and the principle of data saturation was followed. Specifically, data collection was terminated when no new thematic information emerged.
Inclusion criteria were as follows: (1) aged 60 years or older; (2) meeting the diagnostic criteria for comorbidities as specified in the Chinese Expert Consensus on the Management of Comorbidities in the Elderly;21 (3) having stable clinical conditions with the ability to communicate effectively and respond appropriately; (4) providing informed consent and voluntarily participating in the study.
Exclusion criteria included: (1) presence of severe mental or psychological disorders precluding cooperation; (2) severe organ dysfunction or terminal-stage disease; (3) transfer to another hospital during the study period.
Study Design and Data Collection
This study used semi-structured interviews for data collection.Pre-interview steps:After obtaining the consent of the nursing department, the researchers first consulted the nurse in charge of the department to understand the condition of each patient and establish a harmonious relationship.Participants were fully informed about the study and signed a written informed consent form before the interview began.Interview execution: One-on-one in-depth interviews were held in quiet environments (eg, wards, meeting rooms) for 20–30 minutes.With consent, interviews were recorded, and researchers took notes.They remained non-directive (no guidance/hints), observed non-verbal cues (facial expressions, body language), and asked follow-ups as appropriate. As all participants are elderly, their educational backgrounds and physical frailty levels may directly affect question comprehension, expressive ability, and communication style.For those with low education: turning abstract questions into concrete scenarios (eg, replacing “How do you manage medication adherence after discharge?” with “What would you do if you had trouble taking your medication after discharge?”), slowing the interview pace, and reducing professional jargon.For those with physical frailty: minimizing patient movement and obtaining extra informed consent from legal guardians, rather than relying solely on the patients themselves.
Guided by Meleis’ Transition Theory,19 an interview outline was developed based on the research objectives, a comprehensive literature review, and internal discussions within the research team. A pilot interview was conducted with two participants, and the outline was revised and refined based on the pilot results to finalize the interview guide. The key questions included: Transition perception: (1) As you prepare to be discharged and return home, how would you describe your current physical condition? (2) What difficulties or challenges do you anticipate facing during the transition from hospital to home? Preparation level: (3) Will you have access to adequate assistance with personal care after discharge? (4) What types of support or guidance do you believe would best address the challenges encountered during the discharge transition? Coping capacity: (5) If you encounter difficulties related to physical health, psychological well-being, illness management, or daily life after discharge, how would you handle them? (6) How has living with comorbidities impacted your life or your family’s life, and what adjustments have you made? (7) Are you satisfied with the services provided by medical staff or community resources? Do you have any additional needs or suggestions? (8) Is there anything else you would like to share?
Date Analysis
Within 24 hours of each interview, audio recordings were transcribed verbatim into text. Data were managed and analyzed using Colaizzi’s seven-step phenomenological approach,22 supported by NVivo 15.0 software. This study strictly adhered to the ethical principles of confidentiality and non-maleficence. We followed the Uniform Standard for Reporting Qualitative Research (COREQ).23
Quality Control Methods
To enhance research rigor in line with the characteristics proposed by CyPress, the following measures were implemented:All researchers completed systematic training in qualitative research methods, covering basic theories, interview techniques, data coding, and analytical procedures. This training ensured proficiency in interview skills and laid a theoretical foundation for conducting qualitative research. The research team comprised two master’s students majoring in nursing, two full-time senior nurses, one associate professor, and one professor. T.Q. and T.L. maintained regular contact with the head nurses of various departments in daily work,Prior to the investigation, they were responsible for liaising with the head nurses of the departments involved in the study and ensuring smooth communication throughout the research period. Given that the participants were generally of advanced age, and to address potential safety risks for the patients, each interview was conducted by two researchers: one conducted the interview with the patient, while the other provided on-site assistance. J.L. and Y.F.analyzed and transcribed the data by integrating audio recordings and on-site notes,Subsequently, NVivo 15 software was used to conduct independent data analysis and coding, so as to guarantee the reliability of the research results. In case of any divergences, team members carried out further analysis and discussion, and finally reached a consensus to enhance the credibility of the findings. X.W. and Y.P. reviewed and validated these topics. As the principal investigator of the entire project, X.W. oversees its overall execution. All research team members are acquainted with one another and maintain regular communication and feedback exchanges through telephone calls and in-person meetings.
Ethical Considerations
The study was conducted in accordance with the ethical principles outlined in the Declaration of Helsinki. The research protocol was approved by the Ethics Committee of the Seventh Affiliated Hospital of Xinjiang Medical University (Approval No. 20240621–003). Written informed consent was obtained from all participants, including the publication of anonymous responses/direct quotes.
Results
No participants withdrew from this study. Based on the principle of data saturation, the final sample size was determined to be 12 cases. The demographic characteristics of the participants are presented in Table 1.
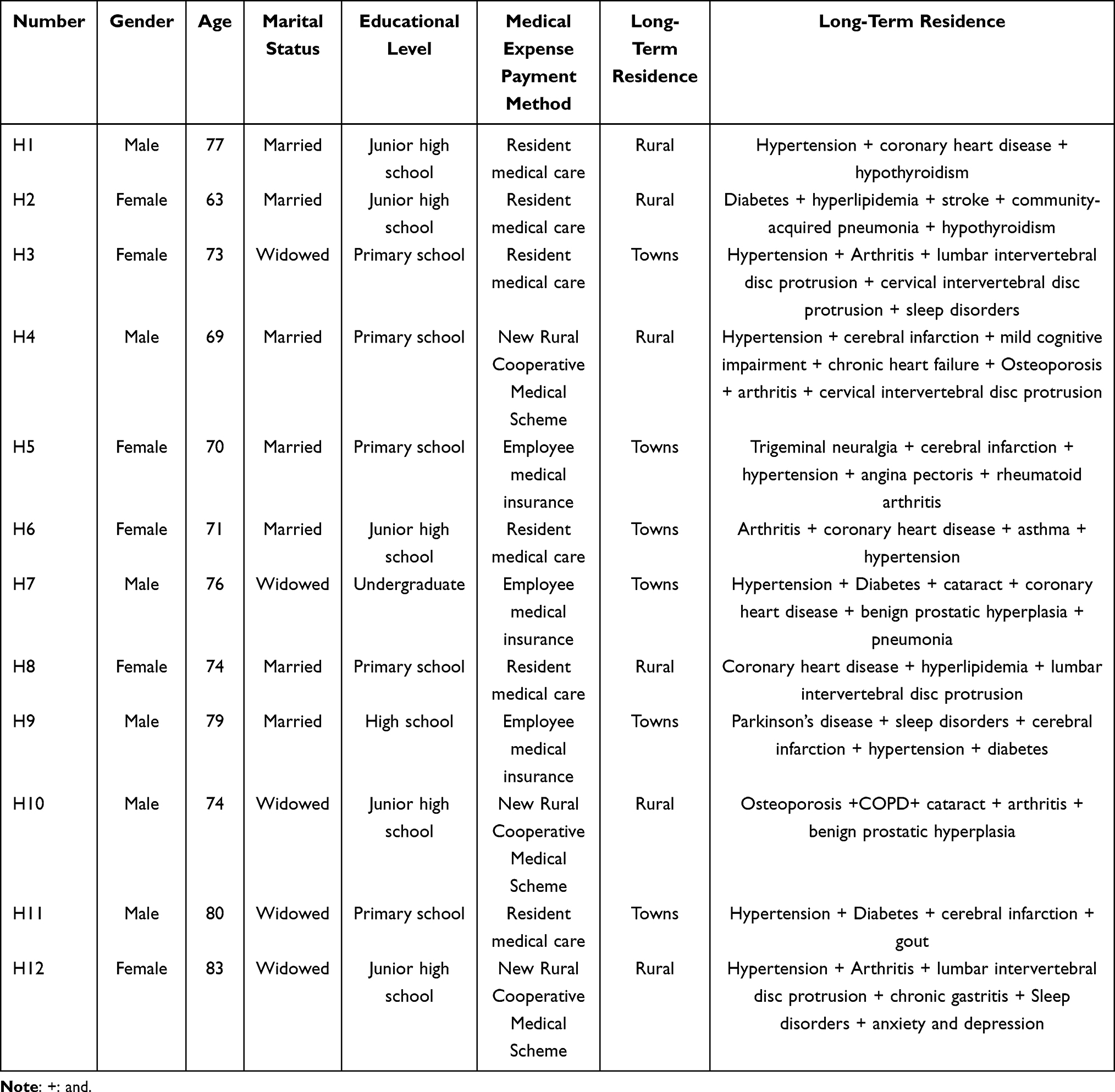 |
Table 1 General Information of Respondents (n=12) |
Three core themes were identified from the analysis. Themes and Subtopics are shown in Table 2. The themes, sub-themes and representative statements are presented in Supplementary Table 1.
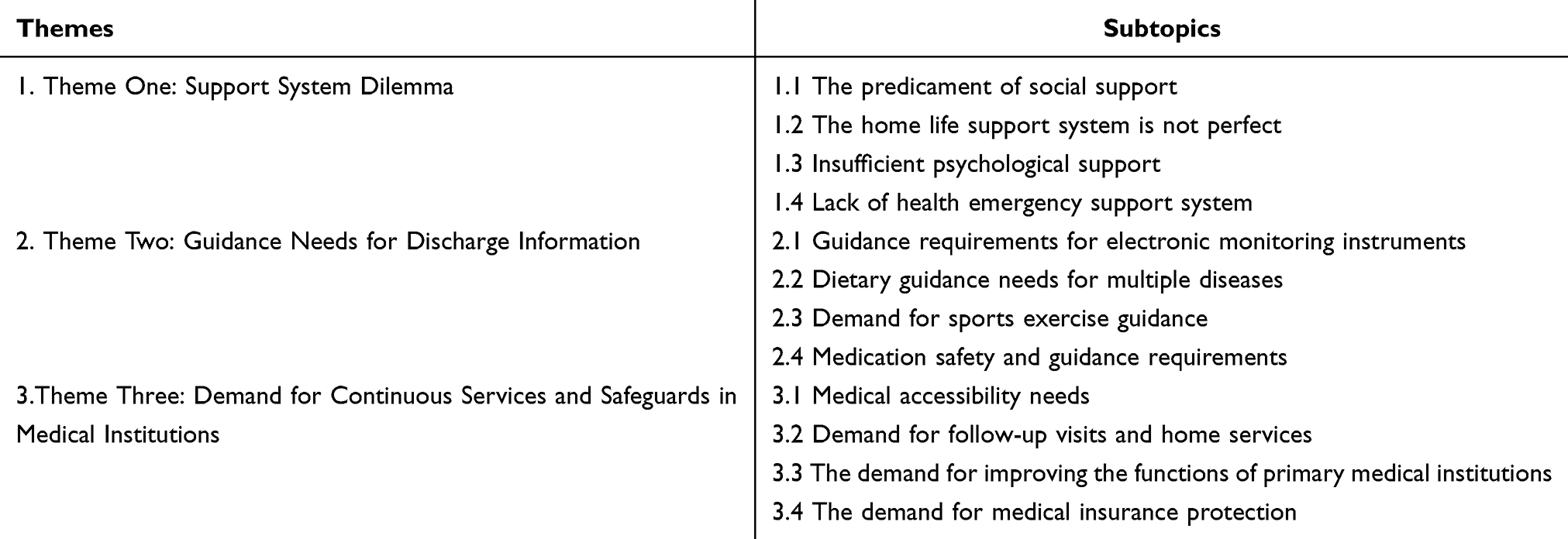 |
Table 2 Themes and Subtopics |
Theme One: Support System Dilemma
Subtopic 1 The Predicament of Social Support
One-third of the respondents noted that, plagued by illness, their social circles had narrowed, their daily activities had grown monotonous, and their social interactions had passively decreased.
H1: “There aren’t many people in the village anymore. Apart from staying at home, I just take a stroll around the door every day.” H5: “I’m getting older, I don’t talk much, I can’t play poker or chess, I just stay at home and do things (with a wry smile).” H7: “A few years ago, I often sat at the bottom of the community and watched them (the neighbors) play cards. Now, I seldom visit them.” H11: “I used to play chess with my old friends in the community activity room, but now that my legs are not as agile as before, I can’t go there anymore.”
Subtopic 2 The Home Life Support System is Not Perfect
Participants struggle to independently perform basic living activities due to their illnesses or complications, and the current care capacity is significantly insufficient. Additionally, participants’ home environments have not been adapted to their physical conditions, and the lack of assistive devices has further heightened the risks to their mobility and safety. This means that participants cannot obtain adequate, safe care support from their families, nor can they move independently in a home environment tailored to their physical needs.
H6: “I can’t go out in winter. I’m afraid I might lose my balance and slip. I have to be careful to walk.” H7: “My knees are not in good condition.It’s hard for me to go up and down stairs or cook.” H8: “There’s a squat toilet at home. I can’t bend down like this.” H10: “I can’t lift my arms high when getting dressed (arthritis), and it’s hard to put on a pullover.” “There’s a small step at the bathroom door. Every time I step over it, I have to hold onto the wall.” “I have to stand on tiptoes to dry clothes, I have osteoporosis and I’m afraid of falling, so I don’t dare to exert force.” H11: “The most dreaded thing when taking a bath is slipping and being unable to stand steadily.” H12: “When bending over to wash rice or cut vegetables, my back can’t straighten up, arthritis follows suit, and my hands feel weak.”
Subtopic 3 Insufficient Psychological Support
During the post-discharge transitional period, patients often experience emotional distress and loneliness. Uncertainty about their post-discharge recovery gives rise to various complex psychological issues, which significantly impact their quality of life.
H3: “My spouse passed away this year. Every night, I’m still thinking about things to some extent. I’ve been hospitalized three times this year and can’t sleep well every day. I still have no appetite for food. (worried and nervous)”. H4: “After being discharged from the hospital, I’m afraid I won’t be able to take good care of myself and I’m afraid I’ll be hospitalized again”. H5: “I’m the youngest among my siblings. One of my elder sisters passed away long ago, and so did my elder brother. Only my nephews and nieces have time to come and visit. (Feeling down)”. H7: “When I was first admitted to the hospital, I was extremely anxious. I was always thinking about family matters and also worried about whether my health would get better”. “Blood sugar and blood pressure also need to be closely monitored every day, without the slightest carelessness (anxiety).” “Especially during the epidemic, a friend who often went out for walks together had lung problems and passed away (choking up).” H11: “Being discharged from the hospital is a good thing. It’s just going home alone.” H12: “It’s been three years since my husband left. The room is so quiet. My own health has broken down, and my son will be under even more pressure. I don’t want to hold him back”.
Subtopic 4 Lack of Health Emergency Support System
The coexistence of multiple diseases among participants complicates their conditions, making it difficult to accurately identify sudden symptoms. Combined with physical deterioration, living alone, or lack of caregivers, their ability to handle unexpected situations is further diminished.
H7: “I also want to know who to turn to for help when I feel unwell at home. I can’t just rush to the hospital for a minor matter.” H9: “Hospital nurses can help measure blood pressure and blood sugar. But if our blood pressure suddenly rises when we get home, we don’t know what to do first”. H10: “My illness keeps recurring. If I suddenly have severe shortness of breath at night or my joints hurt so much that I can’t bear it, and there’s no medicine at home, who should I turn to?” H11: “Before, when my wife was around, she would call 120. Now I’m alone. When I suddenly fall ill, no one takes care of me. Sometimes I can’t even reach my phone”. H12: “I live alone. If I suddenly faint at night, there won’t even be someone to call out to.”
Theme Two: Guidance Needs for Discharge Information
Subtopic 1 Guidance Requirements for Electronic Monitoring Instruments
Elderly patients with comorbidities often suffer from chronic conditions such as hypertension and diabetes. Given the need for regular disease monitoring and their limited ability to operate devices, these patients hope to receive guidance on using home monitoring tools—such as blood pressure monitors and blood glucose meters—when discharged from the hospital.
H2: “The small card of the blood glucose meter is too small for my eyes to see clearly. I just muddle it up every time.” H3: “I’m not sure if the electronic blood pressure monitor at home measures correctly. When I was in the hospital, it was always the nurses who took the measurements. It seems a bit different from when I did it at home. When the nurses were taking the measurements, their hands were both touching and stuffed. (helpless)”. H7: “Could you teach my family how to measure my blood pressure and blood sugar? We have all kinds of devices at home. My eyesight is too blurry. If they learn, I’ll feel more at ease”. H8: “(I took out an elderly mobile phone from under the pillow). My son bought it for me. It said that pressing ‘1’ would make a call to him. Last time, I was so flustered and my hands were shaking that I pressed the wrong number. I have no idea where the call went”.
Subtopic 2 Dietary Guidance Needs for Multiple Diseases
Patients with chronic diseases have distinct, even conflicting, dietary requirements. In this study, some respondents noted that they need professional dietary guidance from medical staff to balance the dietary restrictions of their various conditions.
H9: “People with diabetes can’t eat sweet food, those with hypertension need to consume less salt, and it seems that Parkinson’s disease requires some high-protein food? With all these ingredients together, I don’t even know what to ask my wife to cook”.
Subtopic 3 Demand for Sports Exercise Guidance
Due to their conditions, elderly patients with comorbidities often experience issues like reduced limb function and diminished activity endurance. The interaction between multiple diseases may further worsen such functional impairments. In this study, some respondents noted that they urgently need medical staff to provide specific, safe guidance on home-based exercise before discharge.
H4: “Does our hospital have any rehabilitation exercises or anything like that? I saw them doing Tai Chi in the park before and it was quite good. But I don’t know how to do it either. I really want to practice these. (joking tone)”. H6: “The doctor asked me to do some exercise, but it’s winter now and I can’t go out. I can only walk around at home.” H7: “A few years ago, I often followed the people in the community to do exercises. But now that I’m ill and can’t do it anymore, if there’s a doctor or a nurse who can tell me exactly how to exercise, like how many steps to take each day and when to walk, that would be great”. H8: “My back hurts so much that I dare not move much. But my heart is not in good condition. The doctor said I should move more.” H9: “The doctor said I need to practice walking at home, but I’m always afraid of falling when I walk by holding onto the wall. So I wonder if there’s any simple way to practice safely at home”. H12: “Could a doctor teach me some exercises that I can do at home to stretch my waist and joints, the kind that won’t be too tiring?”
Subtopic 4 Medication Safety and Guidance Requirements
Elderly patients with comorbidities typically suffer from multiple chronic conditions and require concurrent use of multiple medications. With advancing age, their physiological functions decline, leading to a significant increase in medication-related risks and growing concerns about medication safety. Additionally, due to memory impairment, the complexity of polypharmacy, and individualized needs, these patients often require repeated medication guidance and management from healthcare providers. In this study, some patients—who took a large number of medications and feared medication confusion post-discharge—expressed a desire to receive support and guidance on their prescribed medications before leaving the hospital.
H4: “The doctor prescribed over ten kinds of medicine. There are so many that I can’t remember them all. I’m afraid I’ll forget to take them.” “I found that every time I was hospitalized and changed to another hospital, each doctor said something different.” “I’d like to ask if, for my situation, it’s possible to add traditional Chinese medicine and combine traditional Chinese and Western medicine. I’m not sure if it would be beneficial for this illness”. H7: “How should I take the medicine after I get home? I have a poor memory and I am afraid I might take the wrong one”. “I don’t know the side effects of the medicine, I just take it as the doctor says”. H8: “(I helplessly patted my pocket). The note I wrote last time (the note about the medicine), I had no idea where it had gone while I was carrying it.” H9: “I have to take several kinds of medicine every day, and the dosage of each medicine is different. When I get home, I’m afraid of missing or taking the wrong medicine”. H10: “The calcium tablets I used to take were too big. They always got stuck in my throat when I swallowed them. Are there any smaller ones?” H11: “Could you write me a list before I’m discharged from the hospital, whether on an empty stomach or after a meal, and teach me how to dispense the medicine by myself?” “Check my medicine box before I leave the hospital to see which medicines are about to expire and which ones need to be replenished.” H12: “This medicine comes in red and tablet forms. It’s for high blood pressure, for the stomach, for relieving joint pain, and for controlling sleep. With my memory, I’m afraid I might forget the number of meals or take the wrong amount”.
Theme Three: Demand for Continuous Services and Safeguards in Medical Institutions
Subtopic 1 Medical Accessibility Needs
In this study, some respondents noted that their homes were far from the hospital and expressed a desire to obtain their doctors’ contact information before discharge—reflecting a strong demand for accessible medical care.
H1: “During my hospitalization, most of my time was spent on check-ups. It was rare to see a doctor, and when I wanted to contact him, there was no phone number.” H2: “. If something happens at home, just call and ask. It would be even better if you could leave your phone number.” H3: “Sometimes my child drives me to the hospital for an injection. The traditional Chinese medicine hospital is quite far away, and each round trip takes a long time. So I try to go there as little as possible”. H4: “Our home is too far from the big hospital. Every week, my younger brother drives us here. We have always been in the countryside and there are no good hospitals here. The distance is a problem for us”. H12: “Every time I have a follow-up checkup, I definitely have to go. But it’s ten miles from the village to the town hospital. There’s no shuttle bus and taking a taxi is very expensive”.
Subtopic 2 Demand for Follow-Up Visits and Home Services
Most respondents noted that they faced difficulties accessing medical care due to factors like their health conditions, severe weather, and long distances to hospitals—and expressed a desire to receive home visits or regular follow-up services.
H1: “I heard from fellow patients that their community offers home visits (referring to medical staff). I wonder if our small community will have such services in the future”. H6: “Does the hospital or clinic deliver medicine to your door? Paying some money is not a big deal. The main thing is that we can’t go out in winter and we don’t want to trouble our daughter”. H8: “If someone could come to our home often to listen to our heartbeats and measure our blood pressure, we wouldn’t have to travel long distances with our old arms and legs”. H9: “If things like medication, exercise, and diet are all made clear, and there’s someone who can check in on me anytime, I think I could score an 8.” H11: “My legs are not very mobile due to stroke sequelae, so it’s difficult for me to go to the community hospital for re-examinations and to get medicine. Could doctors come to my home to check my blood pressure and blood sugar?. Or is it possible to have medicine delivered to my home on a fixed day every month?”
Subtopic 3 the Demand for Improving the Functions of Primary Medical Institutions
Some respondents rarely seek medical care in communities and have a low opinion of primary medical institutions. Consequently, patients demand improvements in the functions of primary medical institutions to address the inadequacies in continuity of care at these facilities.In addition, some patients have noted that primary medical institutions often face issues such as drug shortages and flawed drug procurement mechanisms, and they are eager for the inclusion of traditional Chinese medicine.
H1: “In community hospitals, it’s just injections and intravenous infusions. Serious illnesses can’t be treated at all.” H2: “Oh dear, our community hospital seems to be on the verge of going out of business. The blood pressure measuring machine in the community is so intimidating that it shows over 200 every time! I wonder if it could be replaced with a new one?. When I went there to buy medicine before, there was no medicine I wanted to buy”. H3: “When we fall ill, we actually also want to receive treatment at community hospitals. They are closer, but there is still a difference compared to big hospitals”. H4: “.If there were people practicing traditional Chinese medicine in the community hospital, we wouldn’t have to go back and forth and run around.” H6: “The community hospital only prescribes medicine for one week. Since we can’t go out in winter, can we prescribe medicine for one or two months?”
Subtopic 4 the Demand for Medical Insurance Protection
A few patients noted that due to the heavy use of medications and frequent hospitalizations, they faced high expenses, while medical insurance reimbursement was inadequate.
H2: “The reimbursement from medical insurance is not very generous either. Just this medicine costs a huge sum of money each time. Last time I was hospitalized for surgery, I stayed for many days and spent tens of thousands of yuan”. H4: “The family is borrowing money everywhere. The medical insurance doesn’t cover much either. It’s basically all out of pocket. The medicine is not reimbursed either. This expense is really huge”. H8: “My family is from the countryside. The most worrying thing is the money for buying medicine! The expensive pills for my waist, I cannot bear to take them every day. Only when the pain is unbearable do I break off half a tablet and swallow it. The money I save has to be used to buy medicine for my heart, so it cannot be covered by medical insurance.”
Discussion
Accurately Assessing Post-Discharge Transitional Difficulties and Systematically Enhancing the Support System
The results of this study indicate that elderly patients with comorbidities face predicaments related to support systems when transitioning from hospital to home during the post-discharge period. This is mainly reflected in the patient’s reduced social circle, potential safety hazards in the home environment, and multiple negative psychological emotions, etc. Notably, approximately 21.4% of elderly individuals in urban China live in a state of social isolation.24 Having withdrawn from the labor market, the elderly lose their work-related roles and access to various social resources,25 which in turn leads to insufficient daily social interaction. Additionally, the inherent characteristics of comorbidities mean these patients are highly dependent on family care—a situation that significantly increases their risk of feeling self-reproach and guilt toward caregivers.26 Fan Yingzhu et al27 further confirmed that 218 elderly patients with comorbidities exhibited relatively high psychological vulnerability, linked to factors such as marital status and social support. Moreover, life-related concerns can exacerbate this psychological burden. Liu Linfeng’s research also demonstrated a positive correlation between social isolation and fear of falling among elderly patients.28 Collectively, inadequate social and psychological support leaves patients anxious about their daily activities post-discharge, undermining their confidence in the transition and ultimately impairing their quality of life during this period. Connie et al29 conducted a review of transitional care model applications in hospital-to-home transitions for elderly patients with multiple chronic conditions. Their findings indicated that such models enhanced patients’ discharge satisfaction and improved their quality of life during the transitional period. In terms of psychological interventions, approaches like mindfulness techniques30 entail dynamic monitoring of patients’ psychological state changes during the transition by nursing teams. This practice not only enhances patients’ psychological flexibility and fosters an optimistic mindset but also alleviates negative emotions at discharge. Therefore, clinically, it is recommended that a multidimensional assessment of patients’ transitional challenges—encompassing comorbidities, psychological status, social support, and home environment—be performed prior to discharge. Subsequently, personalized guidance should be provided targeting patients’ identified weaknesses to deliver comprehensive support and care.
Currently, home-based care remains the primary form of elderly care in China. However, in most regions, there exists a prominent contradiction characterized by a mismatch between supply and demand, coupled with insufficient provision of elderly care facilities. Specifically, elderly patients with comorbidities have a strong demand for home-based care, while simultaneously facing high safety risks in the home setting18—these risks manifest as potential hazards during their daily activities. Furthermore, home environments often lack essential safety protection measures, such as anti-slip modifications and handrail installations. Concurrently, inadequate support for household chores (eg, grocery shopping and cooking) not only impedes the elderly’s ability to maintain or improve their daily living skills but also poses latent threats to their safety and health. Against this backdrop, formulating tailored discharge plans and implementing refined home-based care post-discharge can effectively enhance patients’ post-discharge quality of life and strengthen their self-care capabilities. Therefore, it is recommended that the government conduct regular assessments of rural patients’ home living conditions. For patient families with poor home environments and high safety risks, targeted age-friendly modifications should be implemented to facilitate their smooth transition from hospital to home.
In this study, when elderly patients experienced sudden discomfort at home, they were unable to quickly assess their condition and were unsure whether to prioritize contacting community doctors, emergency centers, or their children. This “helplessness when seeking assistance” directly revealed a critical flaw in the post-discharge emergency support system for elderly patients. Studies have confirmed that wearable smart devices, underpinned by big data,31 hold significant application value. These devices can monitor the physical health of elderly patients in real time; when abnormalities are detected, health data is automatically synchronized to family emergency assistance apps and the community medical and health service platform. This not only effectively addresses gaps in home care but also helps reduce medical costs and improve patients’ quality of life. However, the current application of wearable smart devices still has notable limitations, such as inadequate design adaptability for the elderly, insufficient accuracy of health data monitoring technologies, and weak ecological integration between devices, community medical services, and family terminals.31 These issues prevent such devices from fully exerting their intended effects. Therefore, future research should focus on further optimizing device design and related technologies, as well as improving the ecological collaboration mechanism. This will enable more effective application of wearable smart devices in the context of elderly patient care in China, fundamentally addressing the predicament of the post-discharge emergency support system and enhancing patients’ discharge readiness.
Establish a Multidisciplinary Medical Team and Develop a “Comorbidity-Oriented” Transitional Discharge Guidance System
This study found that the pre-discharge needs of elderly patients with comorbidities remain insufficiently addressed, primarily in four areas: electronic monitoring equipment, diet for multiple conditions, exercise guidance, and medication guidance. This result not only reflects the unique needs of the elderly comorbid population but also reveals weaknesses in current discharge information and guidance services. Elderly patients with comorbidities require long-term, continuous condition monitoring. With advancing age, they often experience declines in physiological functions and cognitive abilities, making it difficult to retain complex treatment and care information. They thus need repeated emphasis and guidance from medical staff, and have high demands for the operational accuracy of electronic monitoring devices (such as blood glucose meters and blood pressure monitors) as well as clear interpretation of their data. Furthermore, studies have shown that dietary or exercise recommendations tailored to a single disease are unsuitable for their “multi-morbidity” characteristic, often leading to issues such as conflicting dietary plans and unclear exercise intensity.32,33 A multidisciplinary medical team—comprising professionals such as physicians, nurses, dietitians, and rehabilitation therapists—can meet patients’ needs through a multidimensional approach.34 During hospitalization, medical staff can provide specialized instruction and training on the home use of electronic devices. Dietitians can develop personalized meal plans based on patients’ specific conditions (with clear dietary requirements and contraindications), while physicians evaluate the plans’ impact on disease management. Nurses are responsible for educating patients and their families. Based on patients’ comorbidities and physical limitations, rehabilitation therapists design safe and effective home exercise regimens, with physicians monitoring the exercises’ effects on their conditions to ensure safety.
It is worth noting that patients with comorbidities are affected by the interactions between multiple systemic diseases and take a wide range of medications with complex dosing frequencies, making them vulnerable to the risks of missed doses or incorrect administration. After discharge, the lack of medication supervision and guidance from medical staff increases their medication burden and impairs their ability to self-manage medications.35 This leads to a heightened demand for pre-discharge medication management, which aligns with the findings of Zhao Linbo et al.36 Currently, most guidance primarily relies on written and verbal education, lacking personalized explanations regarding drug interactions and the identification of adverse reactions.37 The 2024 Expert Consensus clearly states that establishing multidisciplinary medication clinics for the elderly is a key measure to ensure rational drug use, and it plays a significant role in developing and optimizing the full-process management pathway for elderly patients on multiple medications. The core concept of such clinics is to adopt a “holistic approach” and conduct comprehensive assessments of elderly patients with comorbidities.38 As an emerging form of medical service, it is still in its early stages of development in China, and most patients remain unfamiliar with it.
Therefore, in future clinical practice, efforts should be made to strengthen the training of medical professionals such as clinical pharmacists and physicians, and establish geriatric polypharmacy clinics. Medical staff can jointly participate in the management and guidance of polypharmacy for elderly patients with comorbidities, thereby improving the quality and safety of medication management during the patients’ transitional period after discharge. Building on this, a multidisciplinary team should be further established to provide comprehensive, continuous, and personalized discharge guidance tailored to patients’ comorbidities. Through diverse methods such as illustrated manuals, video demonstrations, and on-site drills, patients’ retention of information can be enhanced. Meanwhile, the guidance plan should be dynamically adjusted in response to changes in patients’ conditions, ultimately facilitating a smooth transition for patients from hospital to home.
Give Full Play to the “Medical Consortium” Model and Improve Continuous Care Services
In this study, some respondents expressed a strong demand for accessible medical services, eager to receive continuous care such as follow-up visits and home check-ups. For various reasons—including the significant urban-rural disparity in healthcare, particularly for patients residing in rural areas—many develop a reliance on medical staff during hospitalization. Combined with functional impairments caused by their conditions, they often worry about post-discharge accidents like falls, which increases the risk of readmission.39 Currently, community hospitals face limitations such as a narrow service radius, scarce medical resources, and weak diagnostic capabilities. Meanwhile, tertiary general hospitals may be less accessible to rural patients due to long distances and complex consultation procedures. This imbalance in the distribution and allocation of medical resources hinders patients from accessing comprehensive, continuous care. As a key model for integrating regional medical resources, the “county-level medical consortium” can facilitate seamless transitions for patients with comorbidities from hospital to home by uniting tertiary hospitals, secondary hospitals, community health service centers, and other institutions.40 Before discharge, tertiary hospitals should take the lead in clarifying the core care responsibilities that communities need to undertake. After discharge, community hospitals within the consortium provide seamless follow-up, extending standardized in-hospital care to the home setting through home visits and other means, thereby eliminating the “post-discharge care gap.” Thus, moving forward, it is advisable for the government to refine healthcare policies and strengthen the foundational role of primary medical institutions. Clinically, leveraging the “medical consortium”, a “hospital-community-family” linkage model should be established, along with an information management platform and telephone consultation system for transitional care of elderly patients with comorbidities. This would form a closed-loop service, ensuring the continuity and targeting of transitional care, supporting patients in safely transitioning from hospitalization to home, and enhancing the efficiency of continuous care services. Additionally, this study found that some elderly patients with comorbidities face significant medical and economic burdens. Hospitals should pay greater attention to patients’ financial challenges—for instance, by establishing special funds for patients from low-income families and providing financial subsidies—to alleviate their economic pressure.
Relevance for Clinical Practice
Medical institutions should enhance the personalization of discharge planning, strengthen post-discharge communication, and provide guidance on the transfer of care responsibilities to alleviate patients’ sense of uncertainty. Community health service institutions need to engage in transitional management proactively, establish a seamless follow-up system from hospital discharge to community integration. Furthermore, leveraging Xinjiang’s regional characteristics, pilot programs for integrated transitional care combining medical and elderly care services could be developed, integrating medical, rehabilitation, and social support resources to effectively mitigate transitional risks for patients.
Study Limitations
First, this study exclusively incorporated the perspectives of patients and did not include insights from other key stakeholders. This decision was based on the core analytical focus of the research—“Discharge Transition Challenges and Service Needs from the Patient’s Perspective”—which aims to thoroughly examine patients’ subjective experiences and perceptions. Although nursing staff, community healthcare providers, and hospital transition teams are relevant to the topic, their viewpoints constitute an “external observational dimension” that diverges from the primary objective of this study. Including these perspectives concurrently could dilute the analytical focus and hinder an in-depth exploration of patient-centered experiences. Therefore, future studies may benefit from a multi-stakeholder approach, incorporating input from family members and healthcare professionals, thereby enabling a more comprehensive understanding of discharge transition dynamics.
Second, The sample size of this study was 12 patients, drawn solely from two general hospitals in Xinjiang, this restricts the generalizability of the findings, as they cannot account for variations across medical institutions of different tiers in Xinjiang (eg, primary care facilities and specialized hospitals) or between urban and rural settings.Therefore, future studies should aim to expand the sample size and recruit participants from diverse regions and hospitals.This approach will strengthen the representativeness of the sample and thereby improve the generalizability of the research findings.Future research can also explore different core transitional stages, such as patients’ adaptation period upon admission and long-term rehabilitation period.
Thirdly, the predicaments and needs of patients with comorbidities may undergo complex changes across different transitional stages.The present study only included interviews with patients during the post-discharge transition period, and the fact that interviews were conducted in winter may introduce certain potential confounding effects on the research findings.Future research could employ longitudinal qualitative designs to conduct in-depth analyses of dynamically evolving challenges and service needs.
Finally, elderly patients often exhibit characteristics such as memory impairment and reduced logical thinking speed. During interviews, this may lead to difficulties in clearly recalling details related to disease diagnosis and treatment, as well as logical inconsistencies when responding to questions—ultimately resulting in the loss of key information. Therefore, there is a potential risk of memory bias in the data collected.
Conclusions
This study, through interviews with elderly patients with comorbidities, identified that they face multiple challenges during the post-discharge transition period and have numerous unmet needs. Clinically, a transitional multidisciplinary medical team should be established to accurately assess the transitional predicament of patients before their discharge, improve the support system, strengthen the management of polypharmacy, formulate a transitional discharge guidance plan, and construct a “hospital-community-family” tripartite linkage model, in order to improve the quality of life of patients during the transitional period after discharge.
Data Sharing Statement
The datasets analyzed during the current study are not publicly available due to ethical and privacy reasons.
Ethics Statement
This study has been approved by the Ethics Committee of the Seventh Affiliated Hospital of Xinjiang Medical University (Approval Number: 20240621-003).
Acknowledgments
We sincerely thank the medical staff and patients of the hospital for their valuable support and assistance.
Funding
The Health Commission of the Xinjiang Uygur Autonomous Region, “Tianshan Talents” Program for High-Level Talent Development in Medical and Healthcare. [No.TSYC202301A054].
Disclosure
The authors declare that they have no competing interests in this work.
References
1. Alemayehu GE, Gebresillassie BM, Mulugeta F, et al. Treatment burden and health-related quality of life of patients with multimorbidity: a cross-sectional study. Qual Life Res. 2023;32(11):3269–3277. doi:10.1007/s11136-023-03473-3
2. Zijun W, Ganling S, Enying G, et al. Comorbidity guidelines: current situation, challenges and opportunities. Chin J Evidence-Based Med. 2024;24(6):621–625. doi:10.7507/1672-2531.202401171
3. Nunes BP, Flores TR, Mielke GI, et al. Multimorbidity and mortality in older adults: a systematic review and meta-analysis. Arch Gerontol Geriatr. 2016;67:130–138. doi:10.1016/j.archger.2016.07.008
4. Yanna L, Yiqiao W. Research on the current situation and pattern of comorbidity of chronic diseases among the elderly in China. Chin General Pract. 2021;24(31):3955–3962,3978. doi:10.12114/j.issn.1007-9572.2021.00.295
5. Glenn S, Kamoto I, Morrison L, et al. Exploring patient, informal carer and care professional perspectives to understand the key clinical and non-clinical care needs of those living with multiple long-term conditions (MLTC). Br J General Pract. 2023;73(suppl 1).
6. Health TLG. Joined up care is needed to address multimorbidity. Lancet Glob Health. 2023;11(9):e1314–e1314. doi:10.1016/S2214-109X(23)00277-2
7. R ZS, X WH, L LX, et al. Problems and reflections on hierarchical medical system from the perspective of guiding opinions on promoting the construction of hierarchical medical system. Med Debates. 2017;8(5):53–55,61. doi:10.13276/j.issn.1674-8913.2017.05.015
8. Women’s Health Care Department, Keqiao District Maternal and Child Health Care Institute, Shaoxing City, Zhejiang Province. Guiding opinions of the general office of the state council on promoting the construction of the hierarchical medical treatment system. Chin Rural Med. 2015;(20):86–88. doi:10.3969/j.issn.1006-5180.2015.20.045
9. Lucy D, Bradley E, Rushton CA, et al. Heart failure and chronic obstructive pulmonary disease multimorbidity at hospital discharge transition: a study of patient and carer experience. Health Expectations. 2015;18(6):2401–2412. doi:10.1111/hex.12208
10. Sharifuddin A, Cox A, Rickard F, et al. Discharge transition programme to reduce readmission to hospital among older people: a feasibility study. Eur Geriatric Med. 2025;16(prepublish):1–8. doi:10.1007/s41999-024-01121-8
11. Park J, Kim AJ, Cho E-J, et al. Unintentional medication discrepancies at care transitions: prevalence and their impact on post-discharge emergency visits in critically ill older adults. BMC Geriatr. 2024;24(1):1000. doi:10.1186/s12877-024-05517-w
12. Lin QE. Research on the Current Situation and Development Trajectory of Nursing Dependence in Elderly Patients with Comorbidities of Ischemic Stroke. Guangdong: Southern Medical University; 2024.
13. Hong P, Shen H. Research progress of medication deviation between hospital and family in elderly patients. Nurs Rehabil. 2022;21(03):p.75–78.
14. Cui M, Hua J, Shi X, et al. Factors associated with instrumental support in transitional care among older people with chronic disease: a cross-sectional study. BMC Nurs. 2022;21(1):230. doi:10.1186/s12912-022-01014-w
15. Jing Q, Lang W. A qualitative study on the dilemma of discharge preparation in elderly patients with urostomy. J Nurs. 2024;39(11):46–49. doi:10.3870/j.issn.1001-4152.2024.11.046
16. Yuting L, Yuanyuan S, Wenjing D, et al. A qualitative study on the discharge preparation experience and nursing needs of elderly patients undergoing radical resection of esophageal cancer. Geriatric Res. 2025;6(1):44–48. doi:10.3969/j.issn.2096-9058.2025.01.009
17. Donghui H, Haihong X, Yan X, Lijun W. Analysis of continuous nursing needs and coping strategies for elderly hospitalized patients with comorbidities after discharge. Med Inf. 2021;34(11):187–190. doi:10.3969/j.issn.1006-1959.2021.11.054
18. Bian J, Lu XE, Huang Y, et al. A qualitative study on the home care needs of elderly comorbidities. Evidence-Based Nurs. 2022;8(18):2483–2488.
19. Meleis AI, Sawyer LM, Im E-O, et al. Experiencing transitions: an emerging middle-range theory. ANS Adv Nurs Sci. 2000;23(1):12–28. doi:10.1097/00012272-200009000-00006
20. Hennink MM, Kaiser BN, Marconi VC. Code saturation versus meaning saturation: how many interviews are enough? Qual Health Res. 2017;27(4):591–608. doi:10.1177/1049732316665344
21. Zhu ML, Liu XH, Dong BR, et al. Chinese Expert Consensus on the Management of Comorbidity in the Elderly. Chin J Clin Health Care. 2023;26(05):577–584.
22. Liu M. Colaizzi’s Seven Steps Application in the Analysis of Phenomenological Research Data. J Nurs. 2019;34(11):90–92. doi:10.3870/j.issn.1001-4152.2019.11.090
23. Dossett LA, Kaji AH, Cochran A. SRQR and COREQ reporting guidelines for qualitative studies. JAMA Surg. 2021;156(9):875–876. doi:10.1001/jamasurg.2021.0525
24. Shuo Z, Gong C. Research on the current situation and influencing factors of social isolation among the elderly in Chinese cities. J Population Sci. 2015;37(4):66–76. doi:10.16405/j.cnki.1004-129X.2015.04.007
25. Jing RZ, Li L. The relationship between intergenerational living distance, intergenerational support and cognitive function in the elderly. Population Develop. 2025;31(1):12–22.
26. McPherson CJ, Wilson KG, Chyurlia L, et al. The balance of give and take in caregiver-partner relationships: an examination of self-perceived burden, relationship equity, and quality of life from the perspective of care recipients following stroke. Rehabil Psychol. 2010;55(2):194–203. doi:10.1037/a0019359
27. Fan YZ, Yang Y. Current status and influencing factors of psychological vulnerability in elderly patients with chronic diseases. Jilin Med Sci. 2024;45(9):2277–2282. doi:10.3969/j.issn.1004-0412.2024.09.075
28. Liu LF, Zhang W, Ma WL, et al. A study on the correlation between social isolation, social support and fear of falling in elderly patients with type 2 diabetes. Chin J Convalescent Med. 2025;34(8):16–19. doi:10.13517/j.cnki.ccm.2025.08.004
29. Connie B, Nicoline M, Gitte B. Transitional care model for older adults with multiple chronic conditions: an evaluation of benefits utilising an umbrella review. J Clin Nurs. 2023;33(2):481–496. doi:10.1111/jocn.16913
30. Baimei S, Xiaohong C, Ruijuan L. Observation on the effect of mindfulness-based stress reduction therapy combined with narrative therapy on improving the psychological state of patients with post-stroke depression. Electronic J Pract Clin Nurs. 2022;7(25):72–75.
31. Bingfei W, Rui J, Siyuan H. A brief discussion on the demand of the elderly in the community for portable wearable devices - taking smart bracelets as an example. Chin J Geriatric Health Care. 2020;18(4):21–26. doi:10.3969/j.issn.1672-2671.2020.04.007
32. Gomez DA, Carballo-Casla A, Beridze G, et al. Dietary patterns and accelerated multimorbidity in older adults. Nature Aging. 2025;5(8):1–10. doi:10.1038/s43587-025-00929-8
33. Alessio B, Tang LH, Thomssen JL, et al. Physical activity and exercise therapy for people with multimorbidity. Ugeskrift for Laeger. 2023;185(42).
34. Wilkinson I, Harper A. Comprehensive geriatric assessment, rehabilitation and discharge planning. Medicine. 2024;52(11):656–661. doi:10.1016/j.mpmed.2024.08.005
35. Wanyu P, Chunhui Z, Zhenxiang Z, et al. Analysis of self-management level of medication and influencing factors in hospitalized middle-aged and elderly patients with chronic comorbidities. Nurs Res. 2022;36(19):3534–3539. doi:10.12102/j.issn.1009-6493.2022.19.030
36. Linbo Z, Qinghua Z, Huanhuan H, et al. A qualitative study on the medication experience of elderly patients with multiple medications during the hospital-home transition period. Chin Nurs Educ. 2024;21(7):866–872. doi:10.3761/j.issn.1672-9234.2024.07.016
37. Huiyan M, Zhigang Z, Chunfeng Q, et al. Investigation on the current situation of safe home medication for elderly patients with chronic diseases in chinese urban areas and analysis of influencing factors: a National Multi-Center Study. Zhongnan J Pharm. 2024;22(10):2696–2701. doi:10.7539/j.issn.1672-2981.2024.10.023
38. Yuanchao Z, Pengfei J, National Center for Geriatrics. et al. Expert consensus on standard operating procedures for multidrug use in elderly outpatient clinics (2024 Edition). Chinese J Geriatrics. 2024;43(11):1382–1391. doi:10.3760/cma.j.issn.0254-9026.2024.11.002
39. Yinghong Y, Shanshan S, Xingkun Z, et al. The impact of intrinsic capacity decline on falls and readmission in elderly patients. Chinese J Geriatrics. 2023;42(2):165–168. doi:10.3760/cma.j.issn.0254-9026.2023.02.005
40. Yixin T, Yu J. Reform of county medical communities: a Chinese solution for building an integrated medical and health service system. Governance Res. 2025;(1):81–90. doi:10.3969/j.issn.1007-9092.2025.01.007
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Perspectives of People with Type 2 Diabetes Mellitus Towards a Decision Aid Assessing Preferences of Glucose-Lowering Drugs: The Dilemma of Choosing
Roldan Munoz S, Mol PGM, de Vries F, van Dijk PR, Hillege H, Postmus D, de Vries ST
Patient Preference and Adherence 2025, 19:215-234
Published Date: 25 January 2025
Polypharmacy Experience of Middle-Aged and Elderly Patients with Type 2 Diabetes Comorbidity: A Qualitative Study
Han Z, Wang L
Patient Preference and Adherence 2026, 20:605584
Published Date: 9 July 2026