")
Back to Journals » Therapeutics and Clinical Risk Management » Volume 11
Umeclidinium bromide/vilanterol combination in the treatment of chronic obstructive pulmonary disease: a review
Authors Spyratos D, Sichletidis L
Received 17 January 2015
Accepted for publication 20 February 2015
Published 25 March 2015 Volume 2015:11 Pages 481—487
DOI https://doi.org/10.2147/TCRM.S67491
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Garry Walsh
Dionisios Spyratos, Lazaros Sichletidis
Pulmonary Department, “G Papanikolaou” Hospital, Aristotle University of Thessaloniki, Exohi, Thessaloniki, Greece
Abstract: Chronic obstructive pulmonary disease (COPD) is a common disease among the elderly that could be prevented by smoking cessation. As it is characterized by airflow limitation that is not fully reversible, bronchodilator therapy is the first choice of treatment. Symptomatic COPD patients with or without risk for future exacerbations have a strong indication for the permanent use of long- and ultralong-acting ß2-agonists and/or long-acting muscarinic antagonists. Combining bronchodilators is an effective approach, as they demonstrate synergic action at a cellular level and have additive clinical benefits and fewer adverse events compared with increased doses of the monocomponents. Novel fixed-dose combinations of long-acting ß2-agonists/long-acting muscarinic antagonists in one inhaler have been approved for clinical use by the US Food and Drug Administration and the European Medicines Agency. This review focuses on published clinical trials about the fixed-dose combination of umeclidinium/vilanterol trifenatate in patients with COPD. Results from six studies (five of them of 12 weeks’ duration and one that lasted 1 year, including more than 6,000 patients in total) showed that umeclidinium/vilanterol trifenatate improved lung function, dyspnea, and health-related quality of life and decreased the exacerbation rate with no serious adverse events. More longstanding trials are needed to evaluate the effect of the drug on disease progression and compare it directly with other fixed-dose combinations.
Keywords: COPD treatment, bronchodilators, lung function, long-acting ß2-agonists, long-acting muscarinic receptor antagonist combination, umeclidinium/vilanterol
Introduction
Chronic obstructive pulmonary disease (COPD) is a common, preventable, and treatable disease characterized by airflow limitation that is not fully reversible and is usually progressive during follow-up.1,2 It is estimated that the prevalence of the disease that is clinically significant is 10.1% in adults aged 40 years and older,3 and males, current or former smokers, and the elderly are more commonly affected.4 By 2030, COPD is expected to become the fourth leading cause of death worldwide and the third leading cause in middle-income countries.5
Patients usually present with dyspnea,6 reduced physical activity,7 worsening of health-related quality of life, and exacerbations of the disease. The latter contribute to COPD severity, as they are related to more rapid decline in lung function8 and worse prognosis.9 In addition, the systemic manifestations of the disease and comorbidities have been proven to act as prognostic factors.10,11
Although COPD is a chronic, incurable disease, its treatment can be divided into three different components: prevention (smoking cessation, avoidance of occupational and environmental exposure, vaccinations), pharmacotherapy (bronchodilators, inhaled corticosteroids [ICS], roflumilast), and nonpharmacological strategies (pulmonary rehabilitation, long-term oxygen therapy, lung volume reduction surgery).1
Maintenance treatment with long-term bronchodilators (long-acting muscarinic antagonists [LAMAs] and long-acting β2-agonists [LABAs]) are considered the basis of pharmacotherapy for COPD, as they improve lung function, reduce dyspnea, increase exercise capacity, and prevent future exacerbations.12,13 Moreover, a subgroup analysis of the Understanding Potential Long-Term Impacts on Function with Tiotropium (UPLIFT) study showed that tiotropium reduced the rate of decline of lung function in the early stage of COPD.14
Using LAMAs and LABAs in a fixed-dose combination inhalation device is a new treatment option for COPD patients and is recommended by the Global Initiative for Chronic Obstructive Lung Disease (GOLD) as the first or alternative choice for groups B–D.1 Combining bronchodilators of different classes leads to an improvement in efficacy with fewer adverse events in comparison with increased doses of the monocomponents.15
In this review, we mainly evaluate clinical trials of the fixed-dose combination umeclidinium/vilanterol trifenatate (UMEC/VI) in COPD patients. This combination of UMEC/VI at a dose of 62.5/25 μg, delivered by the dry powder device Ellipta® has been licensed (1 year ago in the United States and 6 months ago in the European Union)16,17 for once-daily maintenance treatment in COPD patients.
The role of LAMA/LABA combinations in COPD treatment
Short-acting β2-agonists and muscarinic antagonists are recommended as a first choice for COPD patients in GOLD group A (few symptoms, forced expiratory volume in 1 second [FEV1]>50% predicted, and 0–1 moderate exacerbations in the previous year). These drugs could be used as relievers of symptoms or on a regular basis, but they are less convenient (low adherence) than long-term bronchodilators.1 In addition, their short action leads to lower trough FEV1 compared with LAMAs and LABAs.18
In group B (more symptoms, FEV1>50% predicted, and 0–1 moderate exacerbations in the previous year), the recommendation of GOLD is LAMA or LABA, and their combination is an alternative choice.1 Patients in group C (fewer symptoms, FEV1<50% predicted, or 2 moderate/1 severe exacerbation in the previous year) are generally suggested to use two drugs (LAMA/LABA combination and LAMA or LABA plus ICS or phosphodiesterase 4 inhibitor) or LAMA monotherapy.1 In group D (more symptoms, FEV1<50% predicted, or 2 moderate/1 severe exacerbation in the previous year), the recommendation is for the use of two or three drugs with all regimens including LAMA and/or LABA.1
Studies that used the GOLD 2011 classification for major COPD cohorts concluded that the majority of patients (63%–79%) in groups C and D were categorized there because of lung function (FEV1<50% predicted, groups C1 and D1) and history of frequent or severe exacerbations.19,20 All these patients should be probably treated with a LAMA/LABA combination.
ICS are recommended for patients in group C or D, with frequent exacerbations that do not respond to treatment with long-term bronchodilators. The stable finding of increased risk for pneumonia among studies21–23 should be possibly taken into account in patients with a history of severe lower respiratory infections. However, in everyday clinical practice, there is overtreatment of COPD with ICS,24 and recent studies showed that discontinuation of ICS in patients who were not frequent exacerbators did not increase exacerbation rate.25,26 Roflumilast (a phosphodiesterase 4 inhibitor) is recommended for patients with severe obstruction, clinical phenotype of chronic bronchitis, and frequent exacerbations. All studies used roflumilast as add-on therapy with long-acting bronchodilators.27,28
Combining LAMAs with LABAs is currently proposed by GOLD as a separate treatment option, even though their clinical effectiveness over monocomponents was proved almost 10 years ago.1,29 There are several proposed mechanisms that justify the combination therapy: they demonstrate different ways of action (LAMAs inhibit the action of acetylcholine at M1 and M3 receptors; LABAs promote stimulation of β2-adrenoreceptor, leading to an increase in cyclic adenosine monophosphate) that both result in smooth muscle relaxation and possibly interact at intracellular level;30,31 sympathetic activity is increased during the day, whereas the parasympathetic system is more active at night, so an intervention for both systems might produce additive effects;30,32 there are some data about the anti-inflammatory properties of long-acting bronchodilators,33,34 as well as an cooperative in vitro effect;35 and adverse events related to a LAMA/LABA combination are less than giving monocomponents in increased doses,1 whereas fixed-dose combinations possibly increase adherence to treatment as a result of less-complicated dosing schemes.36
The fixed-dose combination of UMEC/VI
UMEC is a novel LAMA with strong M3 affinity. It has fast onset of action (time to maximal plasma concentration [Tmax], 5–15 minutes) and slow functional reversibility at the M3 receptor, whereas in short-term administration, there were no adverse events related to electrocardiogram, blood pressure, and clinical laboratory tests.37 In addition, in a 12-week clinical study among COPD patients with moderate to very severe disease, UMEC in doses of 62.5 and 125 μg showed improvement from baseline in trough FEV1 at the end of the study (127 and 152 mL, respectively, compared with placebo; P<0.001).38 There was also clinically significant improvement both in dyspnea score and health status, as evaluated by the St George’s Respiratory Questionnaire. In a 24-week clinical study of UMEC/VI in two different doses, the subgroup of patients who received the monocomponent UMEC at 125 μg had a numerical difference in trough FEV1 (186 vs 149 mL), 0–6 hours weighted mean FEV1 (206 vs 180 mL), and peak FEV1 (282 vs 256 mL) from baseline on day 169 compared with those who were treated with tiotropium 18 μg.39
VI is a selective (greater selectivity for β2-adrenoreceptor than formoterol, indacaterol, and albuterol)40 ultra-LABA with rapid onset (5 minutes) and prolonged action that is administered once daily.41 In a dose–response study of VI administered to 602 patients with moderate-severe COPD over the course of a 4-week period, the doses of 25 and 50 μg showed an increase in trough FEV1 of 137 and 165 mL, respectively, over placebo (both P<0.001).42 There were no adverse events with regard to blood pressure, electrocardiogram, and blood glucose and potassium levels.
The fixed-dose combination of UMEC/VI is delivered once daily via the Ellipta® multidose dry powder inhaler and has been recently approved for clinical use in the United States and European Union. Many studies concerning safety, dose response, and bronchodilatory and clinical effects (improvement in dyspnea, quality of life, and exercise capacity) of the drug proved its usefulness in COPD patients.
A safety, randomized, placebo- and moxifloxacin-controlled, 10-day study among 103 healthy subjects43 concluded there were no clinically significant changes from baseline in QT interval corrected using Fridericia’s correction with UMEC 500 μg and UMEC/VI 125/25 μg. On day 10, the mean change from baseline in heart rate was +8.4 beats per minute with UMEC/VI 125/25 μg and +20.3 beats per minute with UMEC 500/100 μg compared with placebo at 10 minutes postdose, whereas after this point, heart rate rapidly returned to normal levels. Another safety, placebo-controlled study of 4 weeks among 42 patients with moderate to very severe COPD showed that a supratherapeutic dose of UMEC/VI (500/25 μg) was well tolerated.44 There was no difference in weighted mean pulse rate over 0–6 hours at the end of the study, as well as in blood pressure, minimum/maximum pulse rate, and QT interval corrected using Fridericia’s correction assessments. Both agents showed rapid absorption (median Tmax ~6 minutes for both drugs) with no evidence of accumulation (area under the curve or Cmax on day 28).
The largest and most recent study about safety and tolerability included 562 patients (342 completed the study) over the course of a 1-year period who were randomized to receive UMEC/VI (125/25 μg), UMEC (125 μg), and placebo.45 Any serious on-treatment adverse events, adverse events that lead to withdrawal from the study, cardiovascular adverse events, and abnormal, clinically significant Holter electrocardiogram interpretations were similar across all treatment groups.
In Table 1, we present five published clinical trials39,46–48 of 24 weeks’ duration that evaluated the effect of the fixed-dose combination UMEC/VI (62.5/25 and 125/25 μg) compared with its monocomponents, tiotropium and placebo, on trough FEV1 as the primary endpoint. Another trial with a longer duration (52 weeks) was a safety and tolerability study that evaluated trough FEV1 as a secondary endpoint. In the only study that used both doses of UMEC/VI (62.5/25 and 125/25 μg),39 there was no difference between the doses in lung function as well as symptomatic improvement. For UMEC/VI (62.5/25 μg, which is the approved dose for clinical use), the differences in trough FEV1 were 167, 52, 22, 90–95, and 60–112 mL compared with placebo, UMEC 62.5 μg, UMEC 125 μg, VI 25 μg, and tiotropium 18 μg, respectively. All these differences were statistically significant with the exception of UMEC 125 μg. The percentage of patients who achieved clinical significant bronchodilation (increase in FEV1≥12% and 200 mL) during the initial 6 hours on the 1st day after drug administration was 61%–69%.39,46,48
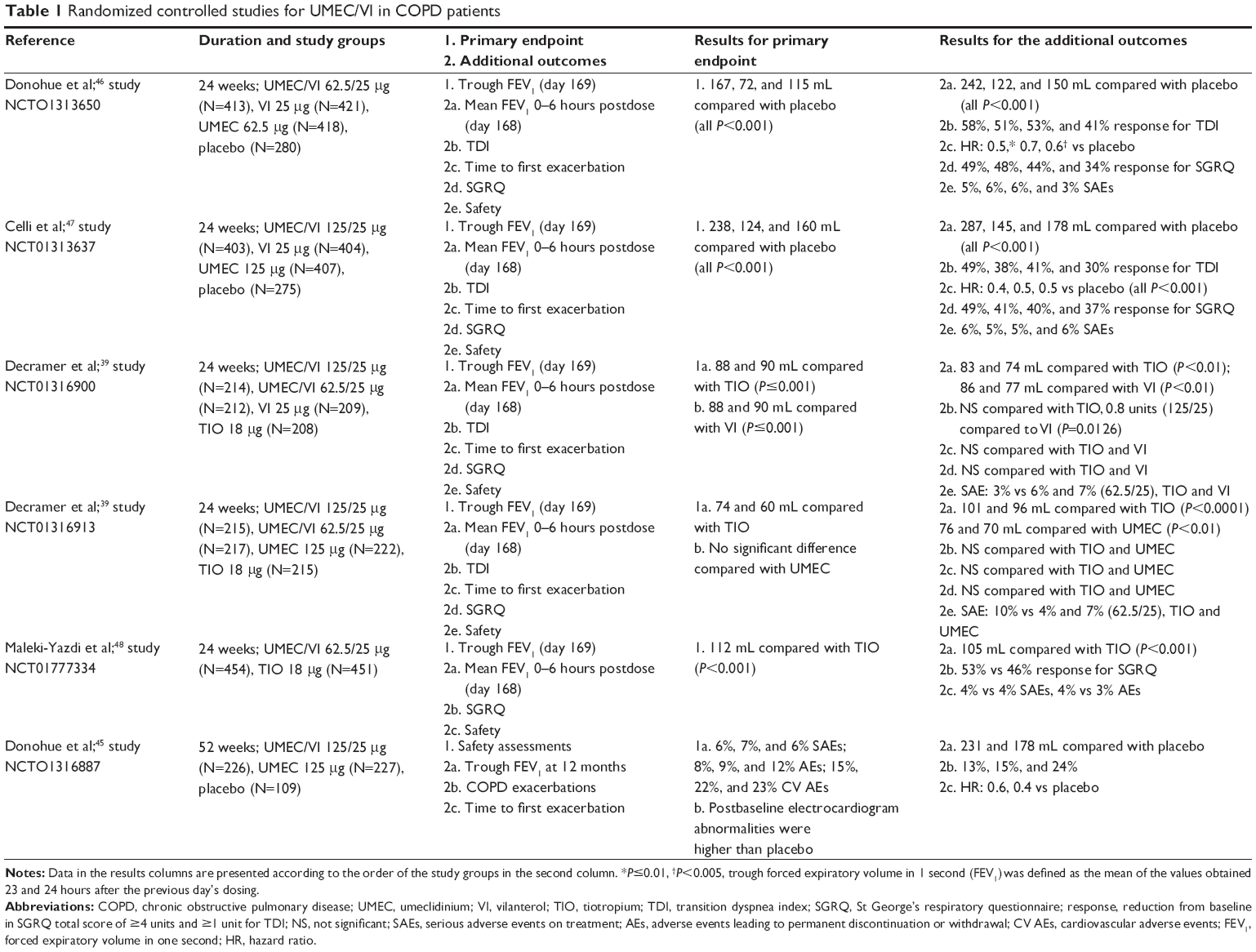 | Table 1 Randomized controlled studies for UMEC/VI in COPD patients |
There were also significant effects on patient-centered outcomes of UMEC/VI (62.5/25 μg). The percentage of patients who achieved the minimally clinical important improvement in TDI (≥1 unit) was 58%,46 in St George’s Respiratory Questionnaire (≥4 units achieved) it was 49%–53%,46,48 and the mean reduction in rescue medication (puffs of albuterol/day) was 1.3–2.7.39,46 In the 52-week study,45 fewer patients experienced COPD exacerbations with UMEC/VI 125/25 μg (13%) compared with placebo (24%). COPD exacerbations that led to hospital admission were also fewer with UMEC/VI 125/25 μg compared with placebo (6% vs 12%).
In two identical 12-week, crossover studies that included 655 patients in total, exercise time as measured by the endurance shuttle walking test 3 hours after drug administration was the primary endpoint.49 One study showed significant increase in exercise time compared with placebo (+69.5 seconds for UMEC/VI 62.5/25 μg; P=0.003), as well as the post hoc integrated analysis (+43.7 seconds for UMEC/VI 62.5/25 μg; P=0.001). Improvements in exercise endurance and trough FEV1 were similar for both doses of UMEC/VI.
In a more recent IIIb, randomized, 12-week clinical trial among 716 moderate/severe COPD patients, with no moderate/severe exacerbations during the last year, UMEC/VI (62.5/25 μg) was compared with fluticasone propionate/salmeterol (500/50 μg twice a day).50 All lung function indices were improved significantly with UMEC/VI, and there was no difference in dyspnea score or health-related quality of life.
In Table 2, we present the main fixed-dose combinations of LAMA/LABA that either have been approved for clinical use, such as indacaterol/glycopyrronium, which is delivered via the Breezhaler® dry powder device, or are in the development phase (eg, tiotropium/olodaterol via the Respimat® device, aclidinium bromide/formoterol via the Genuair®, and glycopyrrolate/formoterol via metered dosed inhaler). All combinations seem promising, as they fulfill important characteristics of an ideal bronchodilator: early onset of action, significant effect during the initial 4–6 hours, longstanding action, and favorable safety profile in a disease that is mainly characterized by irreversible airway obstruction.
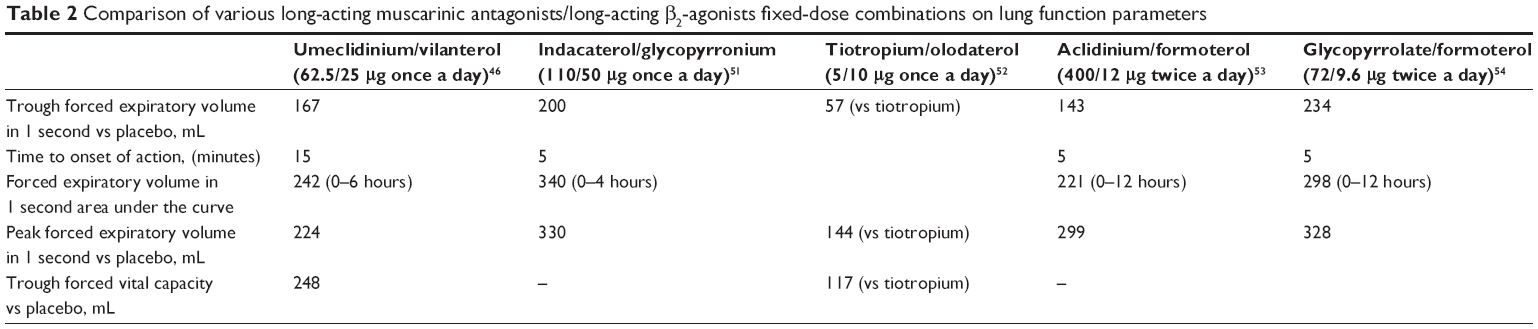 | Table 2 Comparison of various long-acting muscarinic antagonists/long-acting β2-agonists fixed-dose combinations on lung function parameters |
Conclusion
The UMEC/VI combination is an effective and safe bronchodilator delivered via an innovative and easy-to-use device that significantly improved clinical status compared with placebo. More longstanding studies are needed to investigate its role on exacerbations, hospitalizations, disease progression (annual FEV1 decline), and mortality, as well as head-to-head comparisons with other fixed-dose combinations. Patients in group B and those with diminished lung function (FEV1<50% predicted) and infrequent exacerbations (groups C1 and D1) should be the target population for these combinations, and ICS could be the next step, based on a personalized medical approach.
Disclosure
DS has received honoraria for speaking from Astra Zeneca, Menarini, Chiesi, Novartis, and Boehringer-Ingelheim and financial support to attend advisory board meetings and congresses from Novartis, Boehringer-Ingelheim, and Menarini. LS has received honoraria for speaking from Astra Zeneca, Menarini, and Chiesi and financial support to attend advisory board meetings and congresses from Novartis, Boehringer-Ingelheim, and Menarini.
References
Global Initiative for Chronic Obstructive Lung Disease. Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease. Global Initiative for Chronic Obstructive Lung Disease; 2014 [updated 2015]. Available from: http://www.goldcopd.org/uploads/users/files/GOLD_Report_2015.pdf. Accessed Jan 17, 2015. | ||
Vestbo J, Edwards LD, Scanlon PD, et al; ECLIPSE Investigators. Changes in forced expiratory volume in 1 second over time in COPD. N Engl J Med. 2011;365(13):1184–1192. | ||
Buist AS, McBurnie MA, Vollmer WM, et al; BOLD Collaborative Research Group. International variation in the prevalence of COPD (the BOLD Study): a population-based prevalence study. Lancet. 2007;370(9589):741–750. | ||
Menezes AM, Perez-Padilla R, Jardim JR, et al; PLATINO Team. Chronic obstructive pulmonary disease in five Latin American cities (the PLATINO study): a prevalence study. Lancet. 2005;366(9500):1875–1881. | ||
Mathers CD, Loncar D. Projections of global mortality and burden of disease from 2002 to 2030. PLoS Med. 2006;3(11):e442. | ||
Nishimura K, Izumi T, Tsukino M, Oga T. Dyspnea is a better predictor of 5-year survival than airway obstruction in patients with COPD. Chest. 2002;121(5):1434–1440. | ||
Pitta F, Troosters T, Spruit MA, Probst VS, Decramer M, Gosselink R. Characteristics of physical activities in daily life in chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2005;171(9):972–977. | ||
Soler-Cataluña JJ, Martínez-García MA, Román Sánchez P, Salcedo E, Navarro M, Ochando R. Severe acute exacerbations and mortality in patients with chronic obstructive pulmonary disease. Thorax. 2005;60(11):925–931. | ||
Donaldson GC, Seemungal TA, Bhowmik A, Wedzicha JA. Relationship between exacerbation frequency and lung function decline in chronic obstructive pulmonary disease. Thorax. 2002;57(10):847–852. | ||
Mannino DM, Thorn D, Swensen A, Holguin F. Prevalence and outcomes of diabetes, hypertension and cardiovascular disease in COPD. Eur Respir J. 2008;32(4):962–969. | ||
Barnes PJ, Celli BR. Systemic manifestations and comorbidities of COPD. Eur Respir J. 2009;33(5):1165–1185. | ||
Cope S, Donohue JF, Jansen JP, et al. Comparative efficacy of long-acting bronchodilators for COPD: a network meta-analysis. Respir Res. 2013;14(1):100. | ||
Wedzicha JA, Decramer M, Seemungal TA. The role of bronchodilator treatment in the prevention of exacerbations of COPD. Eur Respir J. 2012;40(6):1545–1554. | ||
Decramer M, Celli B, Kesten S, Lystig T, Mehra S, Tashkin DP; UPLIFT investigators. Effect of tiotropium on outcomes in patients with moderate chronic obstructive pulmonary disease (UPLIFT): a prespecified subgroup analysis of a randomised controlled trial. Lancet. 2009;374(9696):1171–1178. | ||
Sethi S, Cote C. Bronchodilator combination therapy for the treatment of chronic obstructive pulmonary disease. Curr Clin Pharmacol. 2011;6(1):48–61. | ||
US Food and Drug Administration. FDA approves Anoro Ellipta to treat chronic obstructive pulmonary disease. Silver Spring, MD: US Food and Drug Administration; 2013. Available from: http://www.fda.gov/newsevents/newsroom/pressannouncements/ucm379057.htm. Accessed Jan 17, 2015. | ||
European Medicines Agency. Anoro. London: European Medicines Agency; 2014. Available from: http://www.ema.europa.eu/ema/index.jsp?curl=pages/medicines/human/medicines/002751/human_med_001754.jsp&mid=WC0b01ac058001d124. Accessed. | ||
Beeh KM, Beier J. The short, the long and the “ultra-long”: why duration of bronchodilator action matters in chronic obstructive pulmonary disease. Adv Ther. 2010;27(3):150–159. | ||
Lange P, Marott JL, Vestbo J, et al. Prediction of the clinical course of chronic obstructive pulmonary disease, using the new GOLD classification: a study of the general population. Am J Respir Crit Care Med. 2012;186(10):975–981. | ||
Agusti A, Hurd S, Jones P, et al. FAQs about the GOLD 2011 assessment proposal of COPD: a comparative analysis of four different cohorts. Eur Respir J. 2013;42(5):1391–1401. | ||
Calverley PM, Anderson JA, Celli B, et al; TORCH investigators. Salmeterol and fluticasone propionate and survival in chronic obstructive pulmonary disease. N Engl J Med. 2007;356(8):775–789. | ||
Suissa S, Patenaude V, Lapi F, Ernst P. Inhaled corticosteroids in COPD and the risk of serious pneumonia. Thorax. 2013;68(11):1029–1036. | ||
Kew KM, Seniukovich A. Inhaled steroids and risk of pneumonia for chronic obstructive pulmonary disease. Cochrane Database Syst Rev. 2014;3:CD010115. | ||
Corrado A, Rossi A. How far is real life from COPD therapy guidelines? An Italian observational study. Respir Med. 2012;106(7):989–997. | ||
Rossi A, Guerriero M, Corrado A; OPTIMO/AIPO Study Group. Withdrawal of inhaled corticosteroids can be safe in COPD patients at low risk of exacerbation: a real-life study on the appropriateness of treatment in moderate COPD patients (OPTIMO). Respir Res. 2014;15:77. | ||
Magnussen H, Disse B, Rodriguez-Roisin R, et al; WISDOM Investigators. Withdrawal of inhaled glucocorticoids and exacerbations of COPD. N Engl J Med. 2014;371(14):1285–1294. | ||
Fabbri LM, Calverley PM, Izquierdo-Alonso JL, et al; M2-127 and M2-128 study groups. Roflumilast in moderate-to-severe chronic obstructive pulmonary disease treated with longacting bronchodilators: two randomised clinical trials. Lancet. 2009;374(9691):695–703. | ||
Calverley PM, Rabe KF, Goehring UM, Kristiansen S, Fabbri LM, Martinez FJ; M2-124 and M2-125 study groups. Roflumilast in symptomatic chronic obstructive pulmonary disease: two randomised clinical trials. Lancet. 2009;374(9691):685–694. | ||
van Noord JA, Aumann JL, Janssens E, et al. Comparison of tiotropium once daily, formoterol twice daily and both combined once daily in patients with COPD. Eur Respir J. 2005;26(2):214–222. | ||
Cazzola M, Molimard M. The scientific rationale for combining long-acting β2-agonists and muscarinic antagonists in COPD. Pulm Pharmacol Ther. 2010;23(4):257–267. | ||
Meurs H, Dekkers BG, Maarsingh H, Halayko AJ, Zaagsma J, Gosens R. Muscarinic receptors on airway mesenchymal cells: novel findings for an ancient target. Pulm Pharmacol Ther. 2013;26(1):145–155. | ||
Undem BJ, Kollarik M. The role of vagal afferent nerves in chronic obstructive pulmonary disease. Proc Am Thorac Soc. 2005;2(4):355–360. | ||
Powrie DJ, Wilkinson TM, Donaldson GC, et al. Effect of tiotropium on sputum and serum inflammatory markers and exacerbations in COPD. Eur Respir J. 2007;30(3):472–478. | ||
Pera T, Zuidhof A, Valadas J, et al. Tiotropium inhibits pulmonary inflammation and remodelling in a guinea pig model of COPD. Eur Respir J. 2011;38(4):789–796. | ||
Costa L, Roth M, Miglino N, et al. Tiotropium sustains the anti-inflammatory action of olodaterol via the cyclic AMP pathway. Pulm Pharmacol Ther. 2014;27(1):29–37. | ||
Price D, Lee AJ, Sims EJ, et al. Characteristics of patients preferring once-daily controller therapy for asthma and COPD: a retrospective cohort study. Prim Care Respir J. 2013;22(2):161–168. | ||
Tal-Singer R, Cahn A, Mehta R, et al. Initial assessment of single and repeat doses of inhaled umeclidinium in patients with chronic obstructive pulmonary disease: two randomised studies. Eur J Pharmacol. 2013;701(1–3):40–48. | ||
Trivedi R, Richard N, Mehta R, Church A. Umeclidinium in patients with COPD: a randomised, placebo-controlled study. Eur Respir J. 2014;43(1):72–81. | ||
Decramer M, Anzueto A, Kerwin E, et al. Efficacy and safety of umeclidinium plus vilanterol versus tiotropium, vilanterol, or umeclidinium monotherapies over 24 weeks in patients with chronic obstructive pulmonary disease: results from two multicentre, blinded, randomised controlled trials. Lancet Respir Med. 2014;2(6):472–486. | ||
Procopiou PA, Barrett VJ, Bevan NJ, et al. Synthesis and structure-activity relationships of long-acting beta2 adrenergic receptor agonists incorporating metabolic inactivation: an antedrug approach. J Med Chem. 2010;53(11):4522–4530. | ||
Kempsford R, Norris V, Siederer S. Vilanterol trifenatate, a novel inhaled long-acting beta2 adrenoceptor agonist, is well tolerated in healthy subjects and demonstrates prolonged bronchodilation in subjects with asthma and COPD. Pulm Pharmacol Ther. 2013;26(2):256–264. | ||
Hanania NA, Feldman G, Zachgo W, et al. The efficacy and safety of the novel long-acting β2 agonist vilanterol in patients with COPD: a randomized placebo-controlled trial. Chest. 2012;142(1):119–127. | ||
Kelleher D, Tombs L, Preece A, Brealey N, Mehta R. A randomized, placebo- and moxifloxacin-controlled thorough QT study of umeclidinium monotherapy and umeclidinium/vilanterol combination in healthy subjects. Pulm Pharmacol Ther. 2014;29(1):49–57. | ||
Feldman G, Walker RR, Brooks J, Mehta R, Crater G. 28-Day safety and tolerability of umeclidinium in combination with vilanterol in COPD: a randomized placebo-controlled trial. Pulm Pharmacol Ther. 2012;25(6):465–471. | ||
Donohue JF, Niewoehner D, Brooks J, O’Dell D, Church A. Safety and tolerability of once-daily umeclidinium/vilanterol 125/25 mcg and umeclidinium 125 mcg in patients with chronic obstructive pulmonary disease: results from a 52-week, randomized, double-blind, placebo-controlled study. Respir Res. 2014;15:78. | ||
Donohue JF, Maleki-Yazdi MR, Kilbride S, Mehta R, Kalberg C, Church A. Efficacy and safety of once-daily umeclidinium/vilanterol 62.5/25 mcg in COPD. Respir Med. 2013;107(10):1538–1546. | ||
Celli B, Crater G, Kilbride S, et al. Once – Daily Umeclidinium/Vilanterol 125/25 μg Therapy in COPD. A Randomized, Controlled Study. Chest. 2014;145(5):981–991. | ||
Maleki-Yazdi MR, Kaelin T, Richard N, Zvarich M, Church A. Efficacy and safety of umeclidinium/vilanterol 62.5/25 mcg and tiotropium 18 mcg in chronic obstructive pulmonary disease: results of a 24-week, randomized, controlled trial. Respir Med. 2014;108(12):1752–1760. | ||
Maltais F, Singh S, Donald AC, et al. Effects of a combination of umeclidinium/vilanterol on exercise endurance in patients with chronic obstructive pulmonary disease: two randomized, double-blind clinical trials. Ther Adv Respir Dis. 2014;8(6):169–181. | ||
Singh D, Worsley S, Zhu CQ, et al. Umeclidinium/vilanterol (UMEC/VIL) once daily (OD) vs fluticasone/salmeterol combination (FSC) twice daily (BD) in patients with moderate-to-severe COPD and infrequent COPD exacerbations. Eur Respir J. 2014;44:Suppl 58 (P290). | ||
Bateman ED, Ferguson GT, Barnes N, et al. Dual bronchodilation with QVA149 versus single bronchodilator therapy: the SHINE study. Eur Respir J. 2013;42(6):1484–1494. | ||
Maltais F, Beck E, Webster D, et al. Four weeks once daily treatment with tiotropium olodaterol (BI 1744) fixed dose combination compared with tiotropium in COPD patients (abstract no. P5557). Eur Respir J. 2010;36(suppl 54):1014s. | ||
Singh D, Jones PW, Bateman ED, et al. Efficacy and safety of aclidinium bromide/formoterol fumarate fixed-dose combinations compared with individual components and placebo in patients with COPD (ACLIFORM-COPD): a multicentre, randomised study. BMC Pulm Med. 2014;14(1):178. | ||
Reisner C, Fogarty C, Spangenthal S, et al. Novel combination of glycopyrrolate and formoterol Mdi (GFF-MDI) provides superior bronchodilation compared to its components administered alone, tiotropium DPI, and formoterol DPI in a randomized, double-blind, placebo-controlled Phase 2b study in patients with COPD [abstract]. Am J Respir Crit Care Med. 2011;183(1):A6435. |
 © 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.