Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 18
Umbilical Cord-Derived Mesenchymal Stem Cells Infusion in Type 2 Diabetes Mellitus Patients: A Retrospective Cytopeutics’ Registry Study
Authors Chin SP ![]() , Kee LT
, Kee LT ![]() , Mohd MA, Then KY
, Mohd MA, Then KY
Received 4 December 2024
Accepted for publication 7 May 2025
Published 19 May 2025 Volume 2025:18 Pages 1643—1659
DOI https://doi.org/10.2147/DMSO.S507801
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Halis Akturk
Sze-Piaw Chin,1,2 Li Ting Kee,1 Muzaida Aminah Mohd,1 Kong Yong Then1,3
1Cytopeutics Sdn Bhd, Cyberjaya, Selangor, Malaysia; 2Cardiology Department, CMH Specialist Hospital, Seremban, Negeri Sembilan, Malaysia; 3CryoCord Sdn Bhd, Cyberjaya, Selangor, Malaysia
Correspondence: Sze-Piaw Chin, Cytopeutics Sdn Bhd, Cyberjaya, Selangor, Malaysia, Email [email protected]
Background: Type 2 diabetes mellitus (T2DM) is characterized by insulin resistance, leading to elevated blood glucose levels. Cellular therapies offer promise for improving hyperglycemia in T2DM. This retrospective study aimed to assess the clinical effectiveness of intravenous allogeneic umbilical cord-derived mesenchymal stem cells (UC-MSCs) infusion in T2DM patients through various clinical evaluations, focusing on systemic inflammation, metabolic dysfunction, and insulin resistance.
Methods: The data from a total of 218 T2DM patients who attended for follow-up after 6 months, and 83 patients after 12 months after receiving 50– 100× 10⁶ allogeneic UC-MSCs were analyzed. Blood and urine samples were collected at baseline and follow-up. Key evaluations included changes in anthropometry, diabetes indices, lipids, liver, renal, hormonal, and inflammatory markers.
Results: All patients demonstrated satisfactory outcomes, without adverse effects. Significant reductions in HbA1c levels were observed at 6-months (p< 0.001) and 12-months (p=0.016). Insulin (p=0.048) and HOMA-IR (p=0.007) levels significantly reduced within 6-months, with same trend at 12-months. ALT and GGT levels significantly decreased (p< 0.05), indicating a reduction in liver inflammation. hs-CRP level among patients with higher inflammation were also reduced at 6-months (p=0.073) and significantly at 12-months (p=0.016). Testosterone (p=0.050) and estradiol (p=0.043) levels increased in males and females, respectively, during 12-month follow-up. Additionally, estimated glomerular filtration rate (eGFR) and creatinine levels improved in stage 2 chronic kidney disease (CKD) at 6- and 12-month (p< 0.05), indicating recovered renal function for those in early stage of CKD.
Conclusion: Allogeneic UC-MSCs infusion is safe for patients with T2DM and is associated with overall health outcomes, with sustained benefits up to 12 months. Notably, the treatment significantly improved metabolic indices including glycemic control, liver and renal profile and systemic subclinical inflammation. These findings provide a basis for further exploration of UC-MSCs in managing T2DM in proper randomized control trial, by addressing both metabolic dysregulation and inflammation.
Keywords: human umbilical cord mesenchymal stem cells, type 2 diabetes mellitus, insulin resistance, HbA1c, glucose
Introduction
Diabetes mellitus (DM) is a syndrome resulting from various causes, characterized by metabolic dysfunction and alterations in insulin production, secretion, or its effectiveness to adequately exert its effects on energy sources.1 According to the International Diabetes Federation (IDF), the global prevalence of diabetes among adults was 9.3% in 2019, with projections indicating it will increase to 10.2% by 2030 and 10.9% by 2045 if effective preventive measures are not implemented,2 earning it a place among the foremost causes of elevated mortality and morbidity rates.1
DM is typically classified into two main types: type 1 diabetes (T1DM) and type 2 diabetes (T2DM), with T2DM accounting for approximately 90–95% of all types of diabetes.2,3 T2DM is an adult-onset condition that is characterized by dysfunction in the body’s ability to sense insulin, leading to insulin resistance.4 It can be influenced by various risk factors, including lifestyle changes towards high-calorie diets and reduced physical activity, genetic predisposition, age, smoking, stress, sleep disorders, abdominal obesity, and inflammation.3,5–9 Previous studies have shown that inflammation is the main trigger of T2DM and activated by these risk factors and chronic pro-inflammatory cytokine pathways in insulin-sensitive tissues like adipose tissue, muscle, and liver.8,10,11 Sustained hyperglycemia may lead to complications affecting various organs, such as diabetic nephropathy, retinopathy, neuropathy, cardiovascular diseases, and diabetic foot ulcers.12–14 Moreover, previous studies have highlighted the negative impact of diabetes on patients’ quality of life.15
Consequently, effective treatment is crucial for maintaining healthy blood sugar levels and reducing the risk of diabetes-related complications.16 This chronic condition requires continuous self-management of lifestyle and adaptation.17 Although diet control, physical exercise and oral anti-diabetic drugs are effective in decreasing hyperglycemia, it is difficult for many patients to achieve good glycemic control depending only on these options, and most of these patients will eventually require insulin therapy.1,18 However, none of the current medicines that reduce hyperglycaemia also act directly on inflammation. Therefore, new innovative therapeutic approaches are required for better management of this disease.
Recent advancements in stem cell research have showed the therapeutic potential in a wide array of challenging diseases.19 Stem cells can be sourced from various part within the human body, with selection criteria typically based on logistical, usable, and in vitro characteristics.20 Among the different types of stem cells, mesenchymal stem cells (MSCs) have garnered considerable attention and are the focus of numerous clinical trials, with 1512 trials registered to date (Mesenchymal Stem Cells search at www.clinicaltrials.gov on 08 November 2024). MSCs possess unique properties, including self-renewal capabilities, the capacity to differentiate into diverse cell types, low immunogenicity, and the ability to proliferate ex vivo for extended periods. Additionally, they release trophic factors known to facilitate the regeneration of damaged cells and tissues.21,22 MSCs can be isolated from various adult tissues such as adipose tissue, bone marrow, and peripheral blood, as well as from birth-associated tissues including the placenta, amnion, umbilical cord (UC), and cord blood (CB).23
Human umbilical cord mesenchymal stem cells (UC-MSCs) have emerged as the preferred choice for MSC-based therapies, largely due to their unique attributes. Compared with MSCs derived from more mature tissue sources, UC-MSCs are believed to be more primitive and possess intermediate properties between those of embryonic and adult stem cells. They exhibit a higher proliferation rate, enhanced self-renewal capacity and importantly, they possess paracrine effects that significantly contribute to their therapeutic potential. These paracrine effects include the secretion of various growth factors, anti-inflammatory cytokines, and extracellular vesicles, which play crucial roles in tissue repair, immunomodulation, and regeneration.24,25 Additionally, the umbilical cord, from which UC-MSCs are sourced, is considered medical waste and can be collected through a non-invasive procedure, eliminating any ethical concerns associated with its acquisition.22,26 These favourable properties position UC-MSCs as a promising therapeutic approach for various diseases, including cardiovascular, neurological, orthopaedic, autoimmune, and endocrine disorders.27 We have previously demonstrated Cytopeutics® UC-MSCs to be safe, possess superior immunomodulatory effects even at high doses in both animal and human studies28,29 and exhibit low immunogenicity, enabling their use in allogeneic transplantation without the risk of rejection.30
Several clinical investigations have explored the use of UC-MSCs in treating T2DM.4,31–37 However, some studies have focused solely on assessing the diabetes metabolic profile, while others have examined additional markers, such as immunologic indices, without considering other clinical markers. Clinical markers, including physical measurement and biochemical markers, play a critical role in monitoring disease progression and treatment effectiveness in diabetes.38 We have previously demonstrated that UC-MSCs have an immunomodulatory and anti-inflammatory effect in a dose-dependent manner in healthy volunteers.28 There has been limited clinical research evaluating these beneficial effects of MSCs in T2DM. Therefore, we aimed to explore the effect of intravenous allogeneic UC-MSCs infusion in T2DM patients, specifically focusing on glycemic control, metabolic dysfunction and systemic inflammation. This analysis provides guidance for a proper randomised control clinical trial to be designed and enabling further exploration of the potential of UC-MSCs in diabetes treatment.
Materials and Methods
Study Design
This retrospective registry included diabetes patients who had received UC-MSCs infusion from participating centers between November 2014 and July 2022. A total of 301 patients with diabetes were selected, as they fulfilled the inclusion and exclusion criteria, as detailed in Table 1. The data for this study were retrospectively obtained from the Malaysian Cell Therapy Patient Registry, which has been registered in National Medical Research Register (NMRR-09-925-4820). This registry serves as a centralized database for collecting and analyzing data on adverse events, side effects, and patient outcomes associated with the use of stem cells. Patients were enrolled into this registry following completion of their clinical trial for long term follow up, which is also part of our pharmacovigilance commitment.
 |
Table 1 Inclusion and Exclusion Criteria for the Patients |
Preparation of UC-MSCs
Umbilical cord samples were collected from full-term, healthy newborns, with written consent from both parents. Prior to sample transfer to the laboratory, three generations (newborn, parents, and grandparents) were screened for chronic viral infections, cancers, and inherited diseases. All cell processing procedures were carried out in a certified Good Manufacturing Practice (GMP) laboratory in accordance with Malaysia Guidelines for Stem Cell Research and Therapy as published previously.39,40 Isolation and culturing methodologies have been previously established and documented.41 The umbilical cord tissue was enzymatically digested, and MSCs were isolated based on their adherence to the surface of culture flasks. The cells were then expanded in a proprietary growth medium under controlled conditions (37°C, 5% CO2) in an incubator. Non-adherent cells were discarded after three days and replaced with fresh growth medium until reaching 80% confluence. Subsequently, UC-MSCs were passage to new flasks and cultured further until reaching the desired cell count. Early passages of the cells were cryopreserved to serve as a seed for future use. In this study, cells were thawed and expanded from the seed up to Passage 6. Throughout the process, UC-MSCs underwent quality control testing, including immunophenotyping, differentiation assays, karyotyping, and screening for adventitious agents such as viruses, bacteria, fungi, and mycoplasma contamination.
Intravenous Allogeneic Infusion of UC-MSCs
Administrations of UC-MSCs were performed on the designated day at the medical centers, with eligible subjects registered as outpatients. Prior to the infusion, subjects underwent a routine physical examination, and their vital signs were assessed to ensure their suitability for UC-MSCs administration. Once the patient was confirmed fit for the infusion, a cannula was inserted into the subjects’ vein. Before the infusion, 100 mL of normal saline was administered intravenously over 30 minutes. Following this, 20 mL of UC-MSCs was mixed with another 350 mL of normal saline in the bag and infused over a period of 2 hours, with the saline bottle gently shaken every 15 minutes to ensure the stem cells remained suspended and did not settle at the bottom. All standard precautions for intravenous procedures were strictly adhered to in accordance with routine medical center practices. Subjects were closely monitored for vital signs and adverse events (AEs) every 15 minutes during the infusion and subsequently on an hourly basis for a minimum of 6 hours in the medical center. Adverse events were defined and categorized according to the Good Clinical Practice (GCP) guidelines of the International Council for Harmonization (ICH). These include any unfavorable medical occurrence in the subjects receiving UC-MSCs, irrespective of its potential association with the investigational product (IP). Monitored adverse events encompassed a range of symptoms such as fever, headache, injection site swelling, or pain. Subjects were discharged if no complications were observed after the designated monitoring period. The administration mainly involves the infusion of one or two doses of 50–100 × 106 allogeneic UC-MSCs cells. Most of the patients received just one dose.
Patient Follow-up and Study Outcome Measures
The patients were monitored for one year following the first infusion to evaluate efficacy parameters. The patients who returned to the hospitals between 1–6 months for follow-up were classified as 6-month follow-up, while those who visited between 7–12 months were classified as 12-month follow-up. During the follow-up, 20 mL of blood was drawn from each subject for blood analysis.
Study outcomes were assessed based on baseline data collected prior to UC-MSCs infusion, including demographic information and medical history. This study evaluated separate groups of patients as baselines for the 6-month and 12-month follow-up periods, as patient selection was based on existing data extracted from medical records. Basic demographic data such as gender and age; anthropometry data such as body mass index (BMI), systolic blood pressure (SBP) and diastolic blood pressure (DBP) were collected. Several clinical assessments were conducted at baseline and during follow-up visits 6- and 12-month post-infusion, encompassing routine blood tests.
Efficacy was defined as changes from baseline in parameters related to diabetes metabolic indices (fasting blood sugar (FBS), serum glycated hemoglobin (HbA1c) levels, insulin levels, and Homeostatic Model Assessment of Insulin Resistance (HOMA-IR)), lipid profile (total cholesterol, triglycerides, high-density lipoprotein (HDL), low-density lipoprotein (LDL), and HDL ratio), liver profile (total protein, albumin, globulin, alkaline phosphatase (ALP), gamma-glutamyl transferase (GGT), aspartate transaminase (AST), and alanine transaminase (ALT)), renal profile (creatinine, estimated glomerular filtration rate (eGFR), uric acid and blood urea nitrogen (BUN)), hormonal profile (Testosterone, luteinizing hormone (LH), Estradiol, insulin-like growth factor-1 (IGF-1), dehydroepiandrosterone sulfate (DHEAS), Follicle-stimulating hormone (FSH), and inflammation profile (high-sensitivity C-reactive protein (hs-CRP)) to assess changes in results for each subject.
Regarding hs-CRP measurement, we evaluated all patients and also the sub-group of patients with levels at 1.5 mg/L or higher. This criterion is based on previous studies which reported the median of hs-CRP level of to be approximately 1.5 mg/L for both males and females.42–44 For the assessment of testosterone levels in hormonal profile, only male patients were included in this study, as females do not typically exhibit significant levels of testosterone. In renal profile, metrics including creatinine, eGFR, uric acid, and BUN were analyzed according to Chronic kidney disease (CKD) stages as defined by KDOQI guidelines.45 CKD is categorized into stages based on eGFR thresholds: stage 1 (eGFR ≥ 90 mL/min/1.73 m²), stage 2 (eGFR 60–89 mL/min/1.73 m²), stage 3 (eGFR 30–59 mL/min/1.73 m²), stage 4 (eGFR 15–29 mL/min/1.73 m²), and stage 5 (eGFR < 15 mL/min/1.73 m²). Among 301 patients, 191 had eGFR values recorded for CKD stage identification and subsequently underwent further renal profile assessments. This study focused on CKD stages 2–5 only. The normal range of the parameters were referenced in the medical report.
Statistical Analysis
Statistical analysis was performed using IBM SPSS Statistics v23.0 software. To evaluate the difference between pre- and post-UC-MSCs infusion, paired t-tests were utilized for the 6-month follow-up analysis, while the Wilcoxon signed-rank test was used for the 12-month follow-up analysis due to the smaller patient sample size. For anthropometry and blood test parameters, the result for 6-month follow-up presented as mean ± standard error of the mean (SEM), while 12-month follow-up analysis are presented as median [interquartile range (IQR)].
Statistical significance was defined as p<0.05. Only statistically significant results, parameters related to the diabetes metabolic profile as they considered important markers for diabetes were included in the graphical representation.
Results
Demographic for Diabetes Patients
Between November 2014 and July 2022, a total of 301 diabetes patients that received UC-MSCs were included in the study. Of these, 167 were male and 51 were female patients during the 6-month follow-up period, while 72 were male and 11 were female patients during the 12-month follow-up period. The mean age of the patients at the 6-month follow-up was 61.5 years old, and at the 12-month follow-up, it was 60.8 years old. The baseline demographic characteristics of the patients are presented in Table 2.
 |
Table 2 Demographic for Diabetes Patients |
Anthropometry Measurement
There is no notable contrast observed in BMI and waist and hip ratio between the initial measurement and subsequent follow-ups at 6- and 12-months (Table 3). However, there is a significant decrease in SBP at the 12-month follow-up (Figure 1A) (p<0.05), as well as in DBP at both the 6-month and 12-month follow-ups (Figure 1B) (p<0.05) (Table 3).
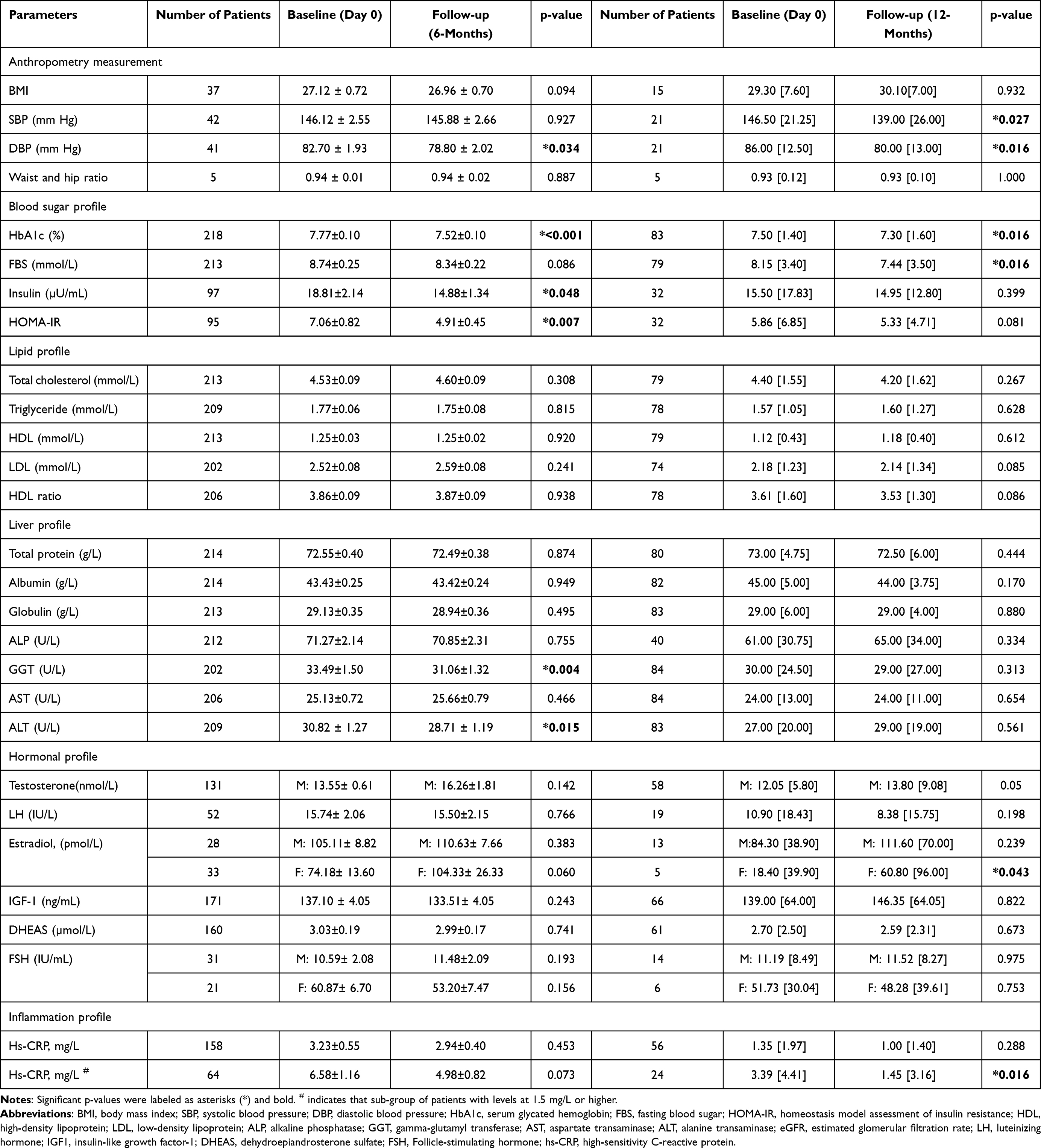 |
Table 3 Parameter Measured at Baseline (Day 0) and the 6-Month Follow-up, as well as Baseline (Day 0) and the 12-Month Follow-up |
 |
Figure 1 Blood pressure level (A) Systolic Blood Pressure (SBP) at the 12-month follow-up (*p=0.027, N=21). (B) Diastolic Blood Pressure (DBP) at both the 6-month and 12-month follow-ups (6-month follow-up: *p=0.034, N=41; 12-month follow-up: *p=0.016, N=21). Paired t-tests were utilized and presented as mean ± SEM for the 6-month follow-up analysis, while the Wilcoxon signed-rank test was used for the 12-month follow-up analysis and presented in median [(IQR)]. |
Efficacy Assessment: Diabetes Metabolic Indices
After treatment, a small but significant decrease in HbA1c levels during the 6-month follow-up period was observed, with the baseline level at 7.77±0.10% reducing to 7.52±0.10% at 6-months (p<0.001), and similarly for the 12-month follow-up period, where the baseline level of 7.50 [1.40]% decreased to 7.30 [1.60]% (p=0.016) (Figure 2A and Table 3). FBS exhibited a decreasing trend over 6-months, although this was not statistically significant (p=0.086) (Figure 2B). However, it showed a significant reduction during the 12-month follow-up period (p=0.016) (Figure 2B). Treatment with UC-MSCs also reduced insulin levels at 6-months post-infusion (p=0.048) (Figure 2C). HOMA-IR, calculated based on insulin and FBS levels before and after the treatment, demonstrated a significant reduction in insulin resistance at 6-months (p=0.007) (Figure 2D) but not at 12 months even though there is a reduction trend in insulin resistance from 5.86 [6.85] at baseline to 5.33 [4.71] (p=0.081).
 |
Figure 2 Metabolic indices level at baseline, 6-month and 12-month follow-ups. (A) Glycated Hemoglobin (HbA1c) levels (6-month follow-up: ***p<0.001, N=218; 12-month follow-up: *p=0.016, N=83). (B) Fasting Blood Sugar (FBS) level (6-month follow-up: p=0.086, N=213; 12-month follow-up: *p=0.016, N=79). (C) Insulin level; 6-month follow-up: *p=0.048, N=97; 12-month follow-up: p=0.399, N=32). (D) Homeostasis Model Assessment of Insulin Resistance (HOMA-IR) (6-month follow-up: **p=0.007, N=95; 12-month follow-up: p=0.081, N=32). Paired t-tests were utilized and presented as mean ± SEM for the 6-month follow-up analysis, while the Wilcoxon signed-rank test was used for the 12-month follow-up analysis and presented in median [Interquartile Range (IQR)]. |
Efficacy Assessment: Lipid Profile
No significant changes were observed between the initial measurement and subsequent follow-up at 6- and 12-months regarding the total cholesterol, triglyceride, HDL, LDL and HDL ratio (Table 3). All these parameters remained within the normal range throughout the study period (normal reference range: total cholesterol (3.40–5.20 mmol/L); triglyceride (0.40–1.70 mmol/L); HDL (>1.04); LDL (<2.60); HDL ratio (3.0–5.0)).
Efficacy Assessment: Liver Profile
The liver transaminases GGT and ALT were significantly decreased at 6-months (GGT: p=0.004, Figure 3A; ALT: p=0.015, Figure 3B). There were no substantial variations observed between the initial measurement and subsequent follow-up at 6- and 12-months for total protein, albumin, globulin, ALP, and AST, all of which were maintained within the normal range throughout the study period (Table 3) (normal reference range: total protein (65–83 g/L); albumin (38–53 g/L); globulin (23–35 g/L); ALP (35–104 U/L); GGT (<50 U/L); AST (10–27 U/L); ALT (5–33 U/L)).
 |
Figure 3 Liver profile at baseline and 6-month follow-up. (A) Gamma-Glutamyl Transferase (GGT) levels (**p=0.004, N=202). (B) Alanine Aminotransferase (ALT) level (*p=0.015, N=209). Paired t-tests were utilized and presented as mean ± SEM for the 6-month follow-up analysis. |
Efficacy Assessment: Renal Profile
CKD is categorized into different stages based on the KDOQI guidelines45 using thresholds of eGFR. Table 4 presents eGFR values for 191 patients, with 140 from the 6-month follow-up and 51 from the 12-month follow-up having their eGFR values recorded for CKD stage identification. These patients with CKD stages 2–5 underwent further renal profile assessments, as shown in Table 5. For CKD stage 2, there was a significant increase in eGFR and a corresponding decrease in creatinine levels at both the 6-month and 12-month follow-ups (Table 5) (eGFR at 6 months: p=0.041, at 12 months: p=0.042; creatinine at 6 months: p=0.041, at 12 months: p=0.030). In contrast, no significant differences in eGFR or creatinine levels were observed between the initial measurement and follow-ups at stages 3 to 5. Uric acid levels showed no significant changes at the 6-month and 12-month follow-ups across all stages. Additionally, in CKD stage 2, BUN levels remained unchanged at both 6-month and 12-month follow-ups (Table 5). Conversely, BUN levels decreased significantly to normal range reference of BUN (2.9–8.2 mmol/L) at the 6-month follow-up in CKD stages 3, 4 and 5 (Table 5; stage 3: p=0.041; stage 4: p=0.032; stage 5: p=0.021).
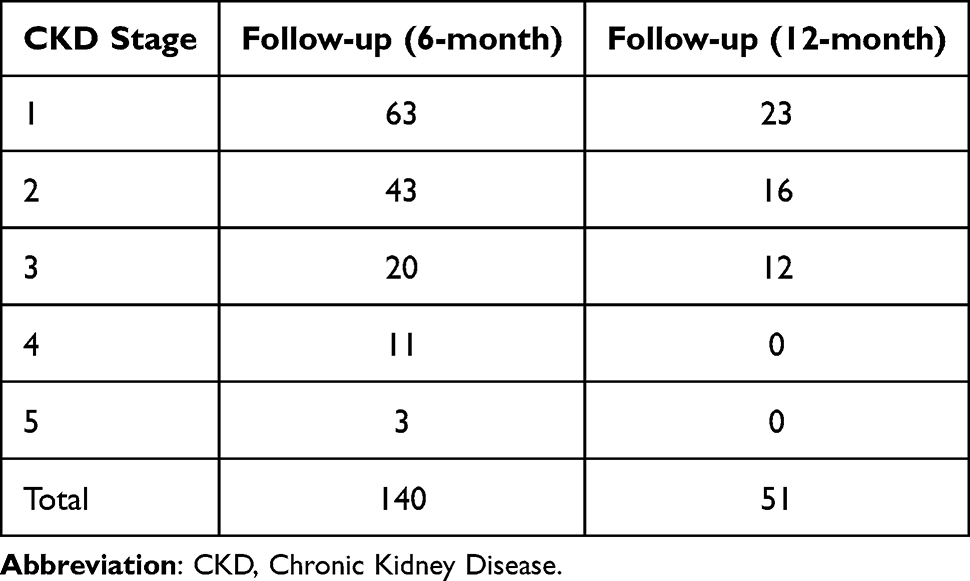 |
Table 4 Number of Diabetes Patients with CKD at Different Stages |
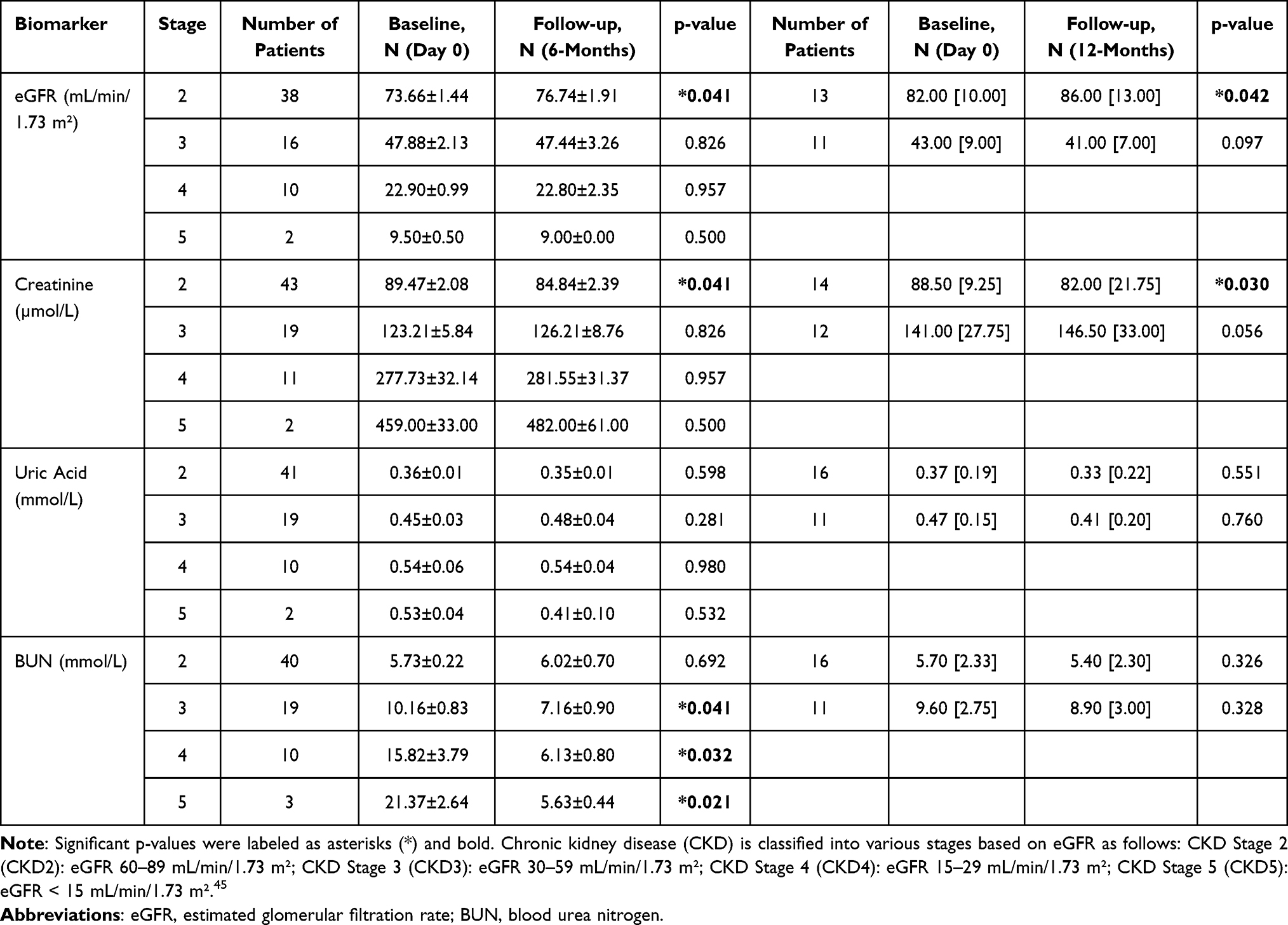 |
Table 5 The Category and Number of Patients for the eGFR at Baseline (Day 0) and the 6-Month Follow-up, as well as Baseline (Day 0) and the 12-Month Follow-up are Summarized |
Efficacy Assessment: Hormonal Profile
Testosterone levels in male patients were observed to increase during the 12-month follow-up period (p=0.050; Figure 4A). Estradiol levels in female patients significantly increased during the 12-month follow-up period (p=0.043; Figure 4B). However, no significant differences were noted between baseline and follow-up (at 6- and 12-months) in estradiol levels for males; LH, IGF-1, DHEAS, as well as FSH levels in both genders (Table 3).
 |
Figure 4 Hormonal profile at baseline and 12-month follow-up. (A) Testosterone levels in male patients (p=0.05, N=58). (B) Estradiol levels in female patients (*p=0.043, N=5). Wilcoxon signed-rank test was used for the 12-month follow-up analysis and presented in median [IQR]. |
Efficacy Assessment: Inflammation Profile
Finally, both 6-month and 12-month follow-up results indicate a numerical reduction in hs-CRP levels, though the decrease was not statistically significant (6-month follow-up: from 3.23±0.55 to 2.94±0.40 mg/L, p=0.45; 12-month follow-up: from 1.35 [1.97] to 1.00 [1.40] mg/L, p=0.29) (Table 3). However, among patients with higher inflammation (hs-CRP ≥1.50 mg/L), hs-CRP showed a trend of decrease, going from 6.58±1.16 mg/L at baseline to 4.98±0.82 mg/L at the 6-month follow-up (p=0.073), while a significant decrease from 3.39 [4.41] mg/L at baseline to 1.45 [3.16] mg/L at the 12-month follow-up (p=0.016), falling within the normal range (reference range: ≤3.00 mg/L) (Table 3 and Figure 5).
 |
Figure 5 High-sensitivity C-Reactive Protein (hs-CRP) value at baseline, 6-month and 12-month follow-up (6-month follow-up: p=0.073, N=64; 12-month follow-up: *p=0.016, N=24). Paired t-tests were utilized and presented as mean ± SEM for the 6-month follow-up analysis, while Wilcoxon signed-rank test was used for the 12-month follow-up analysis and presented in median [IQR]. |
Discussion
Diabetes has become a leading cause of mortality in individuals under the age of 60, with T2DM accounting for over 90% of cases.36 Several studies showed that MSCs may be effective in diabetes management.46 For instance, Zang et al reported that patients receiving UC-MSCs showed significant reductions in insulin levels, HbA1c, and glucose infusion rate (GIR).33 Another study found that UC-MSCs significantly reduced fasting plasma glucose level, improved islet β-cell function, and reduced the need for hypoglycemic agents without serious adverse events.4 Building on these findings, this retrospective analysis aimed to assess the effectiveness of intravenous allogeneic infusion of Cytopeutics® UC-MSCs in T2DM patients in relation to T2DM, systemic inflammation, metabolic dysfunctions, and insulin resistance.
The IDF report in 2021 states that 17.7 million more men than women were living with diabetes in 2021.47 This aligns with our findings, which also showed a higher prevalence of diabetes in men than in women. Another study found that the peak in diabetes prevalence occurs earlier in men (aged 65–69 years) than in women (aged 70–79 years), with male predominance being most evident in middle-aged populations (35–69 years).48 Our study’s average age of approximately 60 years aligns with this trend, which explains the higher diabetes diagnosis rate in men at this age.
To determine the clinical efficacy of MSC therapy for DM, the assessment of HbA1c reduction serves as a pivotal metric as recommended by American Diabetes Association (ADA).49 Unlike blood and urinary glucose measures, HbA1c levels offer a comprehensive insight into long-term glycemic control, spanning over a period of 2 to 3 months.50 Consequently, HbA1c level serve as a reliable indicator of treatment success or failure. In this study, a significant decrease in HbA1c levels was observed during 6-month follow-up, and this reduction was also noted at the 12-month follow-up, indicating that UC-MSCs effectively reduced HbA1c levels in T2DM patients for up to one year, which is consistent with previous findings.51
Insulin, a peptide hormone secreted by pancreatic β cells, plays a crucial role in maintaining blood glucose levels by promoting cellular glucose uptake and regulating the metabolism of carbohydrates, lipids, and proteins.52 In T2DM, insulin resistance resulting in diminished insulin action on target tissues lead to uncontrolled hyperglycemia, which is a hallmark characteristic of the condition.53 In our study, patients with T2DM exhibit elevated insulin levels at baseline, which are associated with higher insulin resistance—a condition where the body fails to respond effectively to insulin, necessitating increased insulin production by the pancreas to overcome resistance.52 The HOMA-IR strongly predicts the development of T2DM, independent of obesity, body fat distribution, and glucose tolerance status. After the infusion of UC-MSCs, a significant decline in the HOMA-IR index was observed. This decrease indicates a reduction in insulin resistance, leading to normal insulin secretion level during the 6-month follow-up period.
Low-grade systemic inflammation is increasingly recognized as a crucial factor in the development and progression of T2DM and its complications, as evidenced in previous studies.9,11,54 Excess nutrients, such as glucose and free fatty acids, stress pancreatic islets and insulin-sensitive tissues including adipose tissue, liver, and muscle, leading to local production of cytokines and chemokines.9,55 This response triggers the recruitment of immune cells, including macrophages, natural killer cells, as well as T- and B-cells, which further contribute to tissue inflammation. The release of reactive oxygen species (ROS), cytokines, and chemokines from adipose tissue into the bloodstream exaggerates inflammation in other regions, including the pancreatic islets, resulting in β-cell death and insulin resistance in peripheral tissues.8,56 Studies have found elevated levels of inflammatory markers such as fibrinogen, C-reactive protein (CRP), interleukin (IL)-6, plasminogen activator inhibitor-1, and white blood cells in adipose tissue, which are linked to obesity-related insulin resistance and islet inflammation.56
Among these markers, CRP is an acute-phase reactant that is synthesized by the liver and regulated by pro-inflammatory cytokines like IL-6 and tumor necrosis factor alpha (TNF-α),57 and serves as a highly sensitive indicator of systemic inflammation.58 Previous studies have established a link between chronic low-grade inflammation, indicated by elevated levels of high-sensitivity CRP (hs-CRP), and T2DM.58 Following UC-MSCs treatment, T2DM patients with higher hs-CRP levels of 1.5 mg/L and above showed a decreasing trend at 6-months, with significant reductions at 12-months. These findings support earlier research suggesting that elevated CRP levels may be linked to hyperglycemia.59 The concurrent reduction in HbA1c over the same period suggests that UC-MSCs may mitigate inflammation and improve glycemic control.
There are also significant albeit small decreases in both SBP and DBP following UC-MSCs infusion. In T2DM, hypertension is commonly associated with insulin resistance, which affects blood vessels and kidneys, leading to increased sodium reabsorption, peripheral artery resistance, and elevated body fluid volume.60–62 The observed reductions in blood pressure suggest that UC-MSCs infusion may improve vascular function, reduce inflammation, and alleviate metabolic dysfunction, potentially offering cardiovascular benefits in this patient population. In this study, we did not observe any reduction in lipid profile. This is possibly because the patients were generally established on lipid-lowering drugs, which rendered their baseline lipid profiles within the recommended range.
Liver function also improved post-UC-MSCs infusion, as reflected by significant reductions in GGT and ALT levels at the 6-month follow-up. T2DM is associated with various liver abnormalities, collectively termed as non-alcoholic fatty liver disease (NAFLD). The development of fatty liver is driven by insulin resistance, which triggers lipolysis and leads to the accumulation of non-esterified fatty acids, ultimately harming hepatocytes.63 Elevated ALT and GGT levels are the indicators of hepatocellular damage and are often observed in diabetic patients.64 Specifically, ALT was found to be elevated in 40.4% of the diabetic population,65 and numerous studies over the past four decades have reported high rates of elevated GGT levels among diabetic patients.66 Elevated GGT levels have been linked to increased oxidative stress, which may lead to β-cell dysfunction and impaired insulin action.66 The improvements in liver function markers following UC-MSCs treatment suggest that addressing inflammation and metabolic dysregulation can significantly benefit liver health in T2DM patients.
Diabetic kidney disease (DKD) is a major cause of chronic kidney disease (CKD),67 affecting 5–7% of the global population, with diabetes and hypertension being primary risk factors.68 People with diabetes are nearly twice as likely to develop CKD, and about 20–50% of those with type 2 diabetes have DKD.68,69 Thus, slowing DKD progression and delaying end-stage kidney disease (ESKD) are crucial. In this study, around 24% of T2DM patients had an eGFR <60 mL/min/1.73 m2 (Stage 3–5), which represent significant loss of kidney function.70 The majority of DKD patients in this cohort are in stage 2 CKD, accounting for around 31%. UC-MSCs infusion significantly improved eGFR and reduced creatinine levels in stage 2 CKD patients, suggesting that MSC therapy may restore kidney tissue function and delay the progression of DKD in line with prior research.71,72 Mechanistically, systemic inflammation plays a critical role in the pathogenesis of DKD.73,74 Hyperglycemia-induced oxidative stress and inflammatory cytokines activate pathways such as NF-κB and JAK/STAT, contributing to kidney tissue damage and fibrosis.74 The reduction in hs-CRP and blood pressure observed in this study may help reduce inflammation in early-stage DKD, thereby promoting kidney repair and improving filtration capacity.
Interestingly, uric acid levels remained unchanged across CKD stages, indicating that MSC treatment may primarily target kidney function and inflammation rather than directly affecting uric acid metabolism. The unchanged BUN level at stage 2 indicates that the kidneys may still process nitrogenous waste similar to before,75 with BUN levels remaining within the normal range. However, the decrease in BUN during advanced stages (stages 3, 4, and 5) from elevated to normal levels suggests improved waste excretion75 and may indicate enhanced kidney function or a positive response to MSC treatment, as elevated BUN is typically associated with kidney dysfunction.76 This decline supports the effectiveness of MSC treatment in improving renal function in more advanced stages of CKD. Overall, these results align with the known benefits of MSCs in promoting renal repair and function, indicating that MSC therapy is advantageous in enhancing kidney function and managing CKD.
Testosterone levels in male patients were significantly increased during the 12-month follow-up. Low serum testosterone levels are commonly observed in men with T2DM77 and are associated with reduced insulin sensitivity and fatty liver infiltration.78 This phenomenon is attributed to the role of testosterone in modulating the expression of crucial genes involved in insulin signalling and glucose uptake, such as glucose transporter-4 (GLUT4). Consequently, diminished testosterone levels can lead to reduced GLUT4 expression in muscle cells and adipocytes, resulting in decreased glucose transport and insulin responsiveness.79 Therefore, the increase in testosterone levels after UC-MSCs therapy may enhance glucose transport and reduce insulin resistance in T2DM patients or may indicate improvement in liver function. Similarly, the significant increase in estradiol levels in female patients at the 12-month follow-up may contribute to improved insulin sensitivity, as estradiol has been shown to exert anti-diabetic effects through various mechanisms, affecting adipose tissue, skeletal muscle, liver, and pancreatic β-cells.80–82
Limitation
This study has several limitations. First, patient selection relied on existing data from medical records, which may be incomplete or contain missing information as we encouraged patients to attend follow-up visits but could not compel them to comply. This limitation constrained our ability to conduct comprehensive analyses using the same patients for both the 6-month and 12-month follow-ups. Consequently, different sets of patients were used as the baseline for the two follow-up periods (6-month and 12-month follow-ups). One notable limitation inherent in this registry was the absence of a control or placebo arm, which would have provided a basis for comparison with the group under investigation. This limitation underscores the importance of prospective designs or randomized controlled trials in future research to address this gap and to enhance the robustness of the findings. Additionally, the retrospective nature of this study presents challenges in controlling confounding variables that could influence the outcomes of interest. Factors such as comorbidities, concurrent medications, lifestyle factors, and changes in clinical practices over time could potentially confound the observed associations with the clinical outcomes of diabetes. Furthermore, the findings of retrospective studies may have limited generalizability to a broader patient population. Our study was specifically conducted among diabetes patients in Selangor, Kuala Lumpur, and Negeri Sembilan, Malaysia. Thus, further investigations are warranted to ascertain whether the observed results can be extrapolated to populations in other states in Malaysia and globally.
Conclusion
In summary, all patients showed satisfactory outcomes without any adverse effects. Our findings support the association of MSC infusion with significant reductions in HbA1c levels and insulin resistance in patient with T2DM. UC-MSCs treatment also resulted in a significant decrease in hs-CRP levels, suggesting a reduction in systemic inflammation with concurrent improved glycemic control. Additionally, improvements in liver and kidney function along with hormonal changes that may enhance insulin sensitivity, further support the multifaceted benefits of this therapy. These findings provide guidance for a well-designed randomized clinical trial to confirm the efficacy of UC-MSCs infusion in T2DM.
Abbreviations
T2DM, Type 2 diabetes mellitus; UC-MSCs, umbilical cord-derived mesenchymal stem cells; DM, Diabetes mellitus; IDF, International Diabetes Federation; T1DM, type 1 diabetes; MSCs, mesenchymal stem cells; UC, umbilical cord; CB, cord blood; GMP, Good Manufacturing Practice; AEs, adverse events; GCP, Good Clinical Practice; ICH, International Council for Harmonization; IP, investigational product; BMI, body mass index; SBP, systolic blood pressure; DBP, diastolic blood pressure; FBS, fasting blood sugar; HbA1c, serum glycated hemoglobin; HOMA-IR, Homeostatic Model Assessment of Insulin Resistance; HDL, high-density lipoprotein; LDL, low-density lipoprotein; ALP, alkaline phosphatase; GGT, gamma-glutamyl transferase; AST, aspartate transaminase; ALT, alanine transaminase; eGFR, estimated glomerular filtration rate; BUN, blood urea nitrogen; LH, luteinizing hormone; IGF-1, insulin-like growth factor-1; DHEAS, dehydroepiandrosterone sulfate; FSH, Follicle-stimulating hormone; hs-CRP, high-sensitivity C-reactive protein; CKD, Chronic kidney disease; SEM, standard error of the mean; IQR, interquartile range; GIR, glucose infusion rate; ADA, American Diabetes Association; DKD, Diabetic kidney disease; ESKD, end-stage kidney disease; GLUT4, glucose transporter-4.
Ethics Approval and Informed Consent
This study adhered to the principles outlined in the Declaration of Helsinki. The data for this study were obtained from the Malaysian Cell Therapy Patient Registry, which is registered in the National Medical Research Register (NMRR-09-925-4820) and approved by Medical Research & Ethics Committee (MREC), Ministry of Health (MOH) National Institutes of Health Malaysia. All participants provided informed consent prior to their inclusion in the registry. Permission to use the data for this research was granted by the dataset owner. As all data were anonymized, patient identifiers were not included, and no further consent for publication was required.
Funding
This study was supported by a publication grant from Cytopeutics Sdn Bhd.
Disclosure
SP Chin serves as Clinical and Research Advisor to Cytopeutics Sdn Bhd, advises on regulatory, clinical, and research activities, and holds a licensed patent (US 11,052,119 B2) with the company. KY Then sits on Cytopeutics medical advisory board. The authors report no other conflicts of interest in this work.
References
1. Tan SY, Mei Wong JL, Sim YJ, et al. Type 1 and 2 diabetes mellitus: a review on current treatment approach and gene therapy as potential intervention. Diabetes Metab Syndr Clin Res Rev. 2019;13(1):364–372. doi:10.1016/j.dsx.2018.10.008
2. Saeedi P, Petersohn I, Salpea P, et al. Global and regional diabetes prevalence estimates for 2019 and projections for 2030 and 2045: results from the International Diabetes Federation Diabetes Atlas, 9th edition. Diabet Res Clin Pract. 2019;157:107843. doi:10.1016/j.diabres.2019.107843
3. American Diabetes Association. Classification and diagnosis of diabetes: standards of medical care in diabetes - 2018. Diabetes Care. 2018;41:S13–S27. doi:10.2337/dc18-S002
4. Lian XF, Lu DH, Liu HL, et al. Effectiveness and safety of human umbilical cord-mesenchymal stem cells for treating type 2 diabetes mellitus. World J Diabetes. 2022;13(10):877–887. doi:10.4239/wjd.v13.i10.877
5. Paprott R, Mensink GBM, Schulze MB, et al. Temporal changes in predicted risk of type 2 diabetes in Germany: findings from the German Health Interview and Examination Surveys 1997–1999 and 2008–2011. BMJ Open. 2017;7(7):1–7. doi:10.1136/bmjopen-2016-013058
6. Park JH, Moon JH, Kim HJ, Kong MH, Oh YH. Sedentary lifestyle: overview of updated evidence of potential health risks. Korean J Fam Med. 2020;41(6):365–373. doi:10.4082/KJFM.20.0165
7. Chen X, Pang Z, Li K. Dietary fat, sedentary behaviors and the prevalence of the metabolic syndrome among Qingdao adults. Nutr Metab Cardiovasc Dis. 2009;19(1):27–34. doi:10.1016/j.numecd.2008.01.010
8. Tsalamandris S, Antonopoulos AS, Oikonomou E, et al. The role of inflammation in diabetes: current concepts and future perspectives. Eur Cardiol Rev. 2019;14(1):50–59. doi:10.15420/ecr.2018.33.1
9. Rohm TV, Meier DT, Olefsky JM, Donath MY. Inflammation in obesity, diabetes, and related disorders. Immunity. 2022;55(1):31–55. doi:10.1016/j.immuni.2021.12.013
10. Marques-Vidal P, Schmid R, Bochud M, et al. Adipocytokines, hepatic and inflammatory biomarkers and incidence of type 2 diabetes. The CoLaus Study. PLoS One. 2012;7(12):1–8. doi:10.1371/journal.pone.0051768
11. Pradhan AD, Manson JE, Rifai N, Buring JE, Ridker PM. C-reactive protein, interleukin 6, and risk of developing type 2 diabetes mellitus. J Am Med Assoc. 2001;286(3):327–334. doi:10.1001/jama.286.3.327
12. Khalil H. Diabetes microvascular complications—A clinical update. Diabetes Metab Syndr Clin Res Rev. 2017;11:S133–S139. doi:10.1016/j.dsx.2016.12.022
13. Ahmad J. The diabetic foot. Diabetes Metab Syndr Clin Res Rev. 2016;10(1):48–60. doi:10.1016/j.dsx.2015.04.002
14. Papatheodorou K, Papanas N, Banach M, Papazoglou D, Edmonds M. Complications of diabetes 2016. J Diabetes Res. 2016;2016:6989453. doi:10.1155/2016/6989453
15. Trikkalinou A, Papazafiropoulou AK, Melidonis A. Diabetes and quality of life. World J Diabetes. 2017;8(4):120–129. doi:10.1016/j.revinf.2015.02.017
16. Garedow AW, Jemaneh TM, Hailemariam AG, Tesfaye GT. Lifestyle modification and medication use among diabetes mellitus patients attending Jimma University Medical Center, Jimma zone, south west Ethiopia. Sci Rep. 2023;13(1):1–10. doi:10.1038/s41598-023-32145-y
17. Adailton da Silva J, Fagundes de Souza EC, Echazú Böschemeier AG, Maia da Costa CC, Souza Bezerra H, Lopes Cavalcante Feitosa EE. Diagnosis of diabetes mellitus and living with a chronic condition: participatory study. BMC Public Health. 2018;18(699):1–8.
18. Marín-Peñalver JJ, Martín-Timón I, Sevillano-Collantes C, Cañizo-Gómez FJD. Update on the treatment of type 2 diabetes mellitus. World J Diabetes. 2016;7(17):354. doi:10.4239/wjd.v7.i17.354
19. Aly RM. Current state of stem cell-based therapies: an overview. Stem Cell Investig. 2020;7:8. doi:10.21037/sci-2020-001
20. Berebichez-Fridman R, Montero-Olvera PR. Sources and clinical applications of mesenchymal stem cells state-of-the-art review. Sultan Qaboos Univ Med J. 2018;18(3):e264–e277. doi:10.18295/squmj.2018.18.03.002
21. Moreira A, Kahlenberg S, Hornsby P. Therapeutic potential of mesenchymal stem cells for diabetes. J Mol Endocrinol. 2017;59(3):R109–R120. doi:10.1530/JME-17-0117.Therapeutic
22. El Omar R, Beroud J, Stoltz JF, Menu P, Velot E, Decot V. Umbilical cord mesenchymal stem cells: the new gold standard for mesenchymal stem cell-based therapies? Tissue Eng Part B Rev. 2014;20(5):523–544. doi:10.1089/ten.teb.2013.0664
23. Hass R, Kasper C, Böhm S, Jacobs R. Different populations and sources of human mesenchymal stem cells (MSC): a comparison of adult and neonatal tissue-derived MSC. Cell Commun Signal. 2011;9(1):12. doi:10.1186/1478-811X-9-12
24. Han Y, Yang J, Fang J, et al. The secretion profile of mesenchymal stem cells and potential applications in treating human diseases. Signal Transduct Target Ther. 2022;7(1). doi:10.1038/s41392-022-00932-0
25. Tai L, Saffery NS, Chin SP, Cheong SK. Secretome profile of TNF-α-induced human umbilical cord mesenchymal stem cells unveils biological processes relevant to skin wound healing. Regener Med. 2023;18:839–856. doi:10.2217/rme-2023-0085
26. Arutyunyan I, Elchaninov A, Makarov A, Fatkhudinov T. Umbilical Cord as Prospective Source for Mesenchymal Stem Cell-Based Therapy. Stem Cells Int. 2016;2016:6901286. doi:10.1155/2016/6901286
27. Baykal B. Mesenchymal stem cells for the treatment of various diseases. J Stem Cell Res Med. 2016;1(2):64–65. doi:10.15761/jscrm.1000110
28. Chin SP, Mohd-Shahrizal MY, Liyana MZ, Then KY, Cheong SK. High dose of intravenous allogeneic umbilical cord-derived mesenchymal stem cells (CLV-100) infusion displays better immunomodulatory effect among healthy volunteers: a Phase 1 clinical study. Stem Cells Int. 2020;2020:4–8. doi:10.1155/2020/8877003
29. Chin SP, Saffery NS, Then KY, Cheong SK. Preclinical assessments of safety and tumorigenicity of very high doses of allogeneic human umbilical cord mesenchymal stem cells. In Vitro Cell Dev Biol Anim. 2024;60(3):307–319. doi:10.1007/s11626-024-00852-z
30. Deuse T, Stubbendorff M, Tang-Quan K, et al. Immunogenicity and immunomodulatory properties of umbilical cord lining mesenchymal stem cells. Cell Transplant. 2011;20(5):655–667. doi:10.3727/096368910X536473
31. Jiang R, Han Z, Zhuo G, et al. Transplantation of placenta-derived mesenchymal stem cells in type 2 diabetes: a pilot study. Front Med China. 2011;5(1):94–100. doi:10.1007/s11684-011-0116-z
32. Izadi M, Sadr Hashemi Nejad A, Moazenchi M, et al. Mesenchymal stem cell transplantation in newly diagnosed type-1 diabetes patients: a Phase I/II randomized placebo-controlled clinical trial. Stem Cell Res Ther. 2022;13(1):1–20. doi:10.1186/s13287-022-02941-w
33. Zang L, Li Y, Hao H, et al. Efficacy and safety of umbilical cord-derived mesenchymal stem cells in Chinese adults with type 2 diabetes: a single-center, double-blinded, randomized, placebo-controlled Phase II trial. Stem Cell Res Ther. 2022;13(1):1–10. doi:10.1186/s13287-022-02848-6
34. Liu X, Zheng P, Wang X, et al. A preliminary evaluation of efficacy and safety of Wharton’s jelly mesenchymal stem cell transplantation in patients with type 2 diabetes mellitus. Stem Cell Res Ther. 2014;5(2):1–9. doi:10.1186/scrt446
35. Zang L, Li Y, Hao H, et al. Efficacy of umbilical cord-derived mesenchymal stem cells in the treatment of type 2 diabetes assessed by retrospective continuous glucose monitoring. Stem Cells Transl Med. 2023;12(12):775–782. doi:10.1093/stcltm/szad060
36. Guan LX, Guan H, Li HB, et al. Therapeutic efficacy of umbilical cord-derived mesenchymal stem cells in patients with type 2 diabetes. Exp Ther Med. 2015;9(5):1623–1630. doi:10.3892/etm.2015.2339
37. Nguyen LT, Hoang DM, Nguyen KT, et al. Type 2 diabetes mellitus duration and obesity alter the efficacy of autologously transplanted bone marrow-derived mesenchymal stem/stromal cells. Stem Cells Transl Med. 2021;10(9):1266–1278. doi:10.1002/sctm.20-0506
38. Wu Y, Ding Y, Tanaka Y, Zhang W. Risk factors contributing to type 2 diabetes and recent advances in the treatment and prevention. Int J Med Sci. 2014;11(11):1185–1200. doi:10.7150/ijms.10001
39. Chin SP, Poey AC, Wong CY, et al. Cryopreserved mesenchymal stromal cell treatment is safe and feasible for severe dilated ischemic cardiomyopathy. Cytotherapy. 2010;12(1):31–37. doi:10.3109/14653240903313966
40. Chin SP, Poey AC, Wong CY, et al. Intramyocardial and intracoronary autologous bone marrow-derived mesenchymal stromal cell treatment in chronic severe dilated cardiomyopathy. Cytotherapy. 2011;13(7):814–821. doi:10.3109/14653249.2011.574118
41. Chin SP, Then KY, Wong CY, Ooi GC, Cheong SK. Allogenic Wharton’s jelly mesenchymal stromal cells intravenous infusion increase serum insulin-like growth factor-1 and dehydroepiandrosterone in healthy volunteers. Cytotherapy. 2013;15(4):S18. doi:10.1016/j.jcyt.2013.01.065
42. Ledue TB, Rifai N. Preanalytic and analytic sources of variations in C-reactive protein measurement: implications for cardiovascular disease risk assessment. Clin Chem. 2003;49(8):1258–1271. doi:10.1373/49.8.1258
43. Albert MA, Ridker PM. C-reactive protein as a risk predictor: do race/ethnicity and gender make a difference? Circulation. 2006;114(5):67–74. doi:10.1161/CIRCULATIONAHA.106.613570
44. Ridker PM. High-sensitivity C-reactive protein: potential adjunct for global risk assessment in the primary prevention of cardiovascular disease. Circulation. 2001;103(13):1813–1818. doi:10.1161/01.CIR.103.13.1813
45. KDOQI. Clinical Practice Guidelines for Chronic Kidney Disease: Evaluation, Classification and Stratification. Vol. 90; 2002.
46. de Klerk E, Hebrok M. Stem cell-based clinical trials for diabetes mellitus. Front Endocrinol. 2021;12:631463. doi:10.3389/fendo.2021.631463
47. International Diabetes Federation. IDF Diabetes Atlas.
48. Cho NH, Shaw JE, Karuranga S, et al. IDF Diabetes Atlas: global estimates of diabetes prevalence for 2017 and projections for 2045. Diabet Res Clin Pract. 2018;138:271–281. doi:10.1016/j.diabres.2018.02.023
49. Classification I. Standards of medical care in diabetes-2014. Diabetes Care. 2014;37(SUPPL.1):14–80. doi:10.2337/dc14-S014
50. Sherwani SI, Khan HA, Ekhzaimy A, Masood A, Sakharkar MK. Significance of HbA1c test in diagnosis and prognosis of diabetic patients. Biomark Insights. 2016;11:95–104. doi:10.4137/Bmi.s38440
51. Mathur A, Taurin S, Alshammary S. The safety and efficacy of mesenchymal stem cells in the treatment of type 2 diabetes-a literature review. Diabetes Metab Syndr Obes. 2023;16:769–777. doi:10.2147/DMSO.S392161
52. Karakas SE. Insulin and insulin resistance. A Case-Based Guid Clin Endocrinol. 2022;26:487–489. doi:10.1007/978-3-030-84367-0_53
53. Li H, Zhu H, Ge T, Wang Z, Zhang C. Mesenchymal stem cell-based therapy for diabetes mellitus: enhancement strategies and future perspectives. Stem Cell Rev Rep. 2021;17(5):1552–1569. doi:10.1007/s12015-021-10139-5
54. Okdahl T, Wegeberg AM, Pociot F, Brock B, Størling J, Brock C. Low-grade inflammation in type 2 diabetes: a cross-sectional study from a Danish diabetes outpatient clinic. BMJ Open. 2022;12(12):1–10. doi:10.1136/bmjopen-2022-062188
55. Stanimirovic J, Radovanovic J, Banjac K, et al. Role of C-reactive protein in diabetic inflammation. Mediators Inflamm. 2022;2022:3706508. doi:10.1155/2022/3706508
56. Velikova TV, Kabakchieva PP, Assyov YS, Georgiev TA. Targeting inflammatory cytokines to improve type 2 diabetes control. Biomed Res Int. 2021;2021:7297419. doi:10.1155/2021/7297419
57. Sproston NR, Ashworth JJ. Role of C-reactive protein at sites of inflammation and infection. Front Immunol. 2018;9. doi:10.3389/fimmu.2018.00754
58. Mahajan A, Tabassum R, Chavali S, et al. High-sensitivity C-reactive protein levels and type 2 diabetes in urban North Indians. J Clin Endocrinol Metab. 2009;94(6):2123–2127. doi:10.1210/jc.2008-2754
59. Pan A, Wang Y, Yuan JM, Koh WP. High-sensitive C-reactive protein and risk of incident type 2 diabetes: a case-control study nested within the Singapore Chinese Health Study. BMC Endocr Disord. 2017;17(1):1–8. doi:10.1186/s12902-017-0159-5
60. Tsimihodimos V, Gonzalez-Villalpando C, Meigs JB, Ferrannini E. Hypertension and diabetes mellitus coprediction and time trajectories. Hypertension. 2018;71(3):422–428. doi:10.1161/HYPERTENSIONAHA.117.10546
61. Petrie JR, Guzik TJ, Touyz RM. Diabetes, hypertension, and cardiovascular disease: clinical insights and vascular mechanisms. Can J Cardiol. 2018;34(5):575–584. doi:10.1016/j.cjca.2017.12.005
62. Ohishi M. Hypertension with diabetes mellitus: physiology and pathology review-article. Hypertens Res. 2018;41(6):389–393. doi:10.1038/s41440-018-0034-4
63. Harris EH. Elevated liver function tests in type 2 diabetes. Clin Diabetes. 2005;23(3):115–119. doi:10.2337/diaclin.23.3.115
64. Noroozi Karimabad M, Khalili P, Ayoobi F, Esmaeili-Nadimi A, La Vecchia C, Jamali Z. Serum liver enzymes and diabetes from the Rafsanjan cohort study. BMC Endocr Disord. 2022;22(1):1–12. doi:10.1186/s12902-022-01042-2
65. Mandal A, Bhattarai B, Kafle P, et al. Elevated liver enzymes in patients with type 2 diabetes mellitus and non-alcoholic fatty liver disease. Cureus. 2018;92(Ci). doi:10.7759/cureus.3626
66. Haghighi S, Amini M, Pournaghshband Z, Amini P, Hovsepian S. Relationship between gamma-glutamyl transferase and glucose intolerance in first degree relatives of type 2 diabetics patients. J Res Med Sci. 2011;16(2):123–129.
67. Bikbov B, Purcell C, Levey AS, et al. Global, regional, and national burden of chronic kidney disease, 1990–2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet. 2020;395(10225):709–733. doi:10.1016/S0140-6736(20)30045-3
68. Jairoun AA, Ping CC, Ibrahim B. Predictors of chronic kidney disease survival in type 2 diabetes: a 12-year retrospective cohort study utilizing estimated glomerular filtration rate. Sci Rep. 2024;14(1):1–13. doi:10.1038/s41598-024-58574-x
69. Reutens AT, Prentice L, Atkins RC. The epidemiology of diabetic kidney disease. Epidemiol Diabetes Mellit. 2008;499–517. doi:10.1002/9780470779750.ch31
70. Evans M, Lewis RD, Morgan AR, et al. A narrative review of chronic kidney disease in clinical practice: current challenges and future perspectives. Adv Ther. 2022;39(1):33–43. doi:10.1007/s12325-021-01927-z
71. Xiang E, Han B, Zhang Q, et al. Human umbilical cord-derived mesenchymal stem cells prevent the progression of early diabetic nephropathy through inhibiting inflammation and fibrosis. Stem Cell Res Ther. 2020;11(1):1–14. doi:10.1186/s13287-020-01852-y
72. Chen L, Xiang E, Li C, et al. Umbilical cord-derived mesenchymal stem cells ameliorate nephrocyte injury and proteinuria in a diabetic nephropathy rat model. J Diabetes Res. 2020;2020:8035853. doi:10.1155/2020/8035853
73. Duran-Salgado MB. Diabetic nephropathy and inflammation. World J Diabetes. 2014;5(3):393. doi:10.4239/wjd.v5.i3.393
74. García-García PM. Inflammation in diabetic kidney disease. World J Diabetes. 2014;5(4):431. doi:10.4239/wjd.v5.i4.431
75. Gounden V, Bhatt H, Jialal I. Renal Function Tests. StatPearls; 2023.
76. Xue Y, Daniels LB, Maisel AS, Iqbal N. Cardiac Biomarkers. In: Reference Module in Biomedical Sciences,
77. Al Hayek AA, Khader YS, Jafal S, Khawaja N, Robert AA, Ajlouni K. Prevalence of low testosterone levels in men with type 2 diabetes mellitus: a cross-sectional study. J Fam Community Med. 2013;20(3):179–186. doi:10.4103/2230-8229.122006
78. Yeap BB, Chubb SAP, Jamrozik K, Hankey GJ, Flicker L, Norman PE. Lower serum testosterone is independently associated with insulin resistance in non-diabetic older men: the Health In Men Study. Eur J Endocrinol. 2009;161:591–599. doi:10.1530/EJE-09-0348
79. Yao QM, Wang B, An XF, Zhang JA, Ding L. Testosterone level and risk of type 2 diabetes in men: a systematic review and meta-analysis. Endocr Connections. 2018;7(4):220–231.
80. Louet JF, LeMay C, Mauvais-Jarvis F. Antidiabetic actions of estrogen: insight from human and genetic mouse models. Curr Atheroscler Rep. 2004;6(3):180–185. doi:10.1007/s11883-004-0030-9
81. Moreno M, Ordoñez P, Alonso A, Díaz F, Tolivia J, González C. Chronic 17β-estradiol treatment improves skeletal muscle insulin signaling pathway components in insulin resistance associated with aging. Age. 2010;32(1):1–13. doi:10.1007/s11357-009-9095-2
82. Gorres BK, Bomhoff GL, Morris JK, Geiger PC. In vivo stimulation of oestrogen receptor α increases insulin-stimulated skeletal muscle glucose uptake. J Physiol. 2011;589(8):2041–2054. doi:10.1113/jphysiol.2010.199018
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.