Back to Journals » Pediatric Health, Medicine and Therapeutics » Volume 13
Umbilical Cord Care Practices and Associated Factor Among Mothers of Neonates Visiting Mizan-Tepi University Teaching Hospital Southwest Ethiopia 2021
Authors Dessalegn N ![]() , Dagnaw Y, Seid K
, Dagnaw Y, Seid K ![]() , Wolde A
, Wolde A ![]()
Received 28 February 2022
Accepted for publication 30 May 2022
Published 7 June 2022 Volume 2022:13 Pages 227—234
DOI https://doi.org/10.2147/PHMT.S363252
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Roosy Aulakh
Nigatu Dessalegn,1 Yalemtsehay Dagnaw,1 Kalid Seid,1 Asrat Wolde2
1Department of Nursing, College of Medicine and Health Science, Mizan-Tepi University, Mizan, Southwest Ethiopia People Regional State, Ethiopia; 2Department of Psychiatry, College of Medicine and Health Science, Mizan-Tepi University, Mizan, Southwest Ethiopia People Regional State, Ethiopia
Correspondence: Nigatu Dessalegn, Department of Nursing, College of Medicine and Health Sciences, Mizan-Tepi University, PO Box 260, Mizan, Southwest Ethiopia People Regional State, Ethiopia, Tel +251-92-845-5726, Email [email protected]
Background: Due to unsanitary cord care practices, cord infections are more common and prevalent in developing countries. In settings where mortality is low, dry and clean cord care is recommended for newborns delivered in health facilities or at home. Cord care practices would directly contribute to infection in newborns, accounting for a large proportion of millions of annual neonatal deaths. This study aimed to assess the cord care practices of mothers and to identify areas for intervention.
Methods: An institution-based cross-sectional study was conducted among mothers of neonates who gave birth in the last six months. Systematic random sampling technique was employed to include women who visited pediatric OPD and immunization clinics. Epi data version 3.1 was used to enter the data and then exported to SPSS version 26 for analysis. The association between the outcome and independent variables was examined using binary logistic regression. The strength of the association was measured using odds ratio (OR), 95% confidence intervals (CI) and p-value. Statistical significance was declared at a p-value < 0.05.
Results: Four hundred twenty-two mothers were participated in the study. More than half (59.2%) of the respondents had good cord care practices, while nearly half (45.3%) mothers added nothing to the cord. Factors significantly associated with good cord care practices were educational status (AOR = 4.7; 95% CI = 1.34, 7.59), ANC follow-up (AOR = 3.58; 95% CI = 1.24, 10.32), initiation of breastfeeding (AOR = 1.74; 95% CI = 1.10, 2.77), and apply anything to the cord (AOR = 3.08; 95% CI = 1.92, 4.95).
Conclusion: The proportion of mothers with good cord care practices was inadequate. For such a high cause of neonatal death, prevention should be the priority intervention, and improving its implementation requires further effort.
Keywords: newborn, cord care, Mizan, sepsis
Introduction
The current WHO recommendation for developing countries has prioritized hygienic cord care, which includes cutting the cord with a new or sterilized instrument, using a clean delivery kit, and appropriate cord care.1 Hygienic cord care is recommended to reduce the risk of sepsis, a major cause of newborn mortality specifically, infection that enters the body at the cord stump site in the newborn. Due to unsanitary cord care practices, cord infections are more common and prevalent in developing countries.2,3 In settings where mortality is low, dry and clean cord care is recommended for newborns delivered in a health facility or at home.4,5
Nearly 7.5 million neonates die in the first month of life worldwide, with developing countries accounting for 98% of these deaths.6,7 A significant proportion of deaths of neonate from infection are traceable to initial cord infections.8,9 Contamination of the umbilical cord can lead to omphalitis, which may have an incidence as high as 77 per 1000 hospital-born infants.10
During the neonatal period, proper care of the neonate’s umbilical cord is critical, and improper umbilical cord practices have been linked to infections.5 Infections are responsible for 30% of the 2.5 million newborn deaths that occur each year around the world. Infections are responsible for 30% of the 2.5 million newborn fatalities that occur each year worldwide.11 Bacteria can enter the susceptible neonate through a newly cut umbilical cord, causing neonatal sepsis. Most of the infections can be prevented using evidence-based cord care.2
Neonatal sepsis is the third leading cause of neonatal mortality in the first month of life, accounting for more than 15% of all neonatal deaths worldwide.12 Harmful traditional cord-care practices are often cited as an important public health concern. In order to address the high rates of newborn sepsis, it is important to have a clear knowledge of the behavioral intention behind traditional cord care practice in low- and middle-income nations.13,14
Despite efforts to enhance cord care practices, recommendations for umbilical cord care are rarely followed in many developing countries where deliveries are performed by unskilled professionals. Numerous studies carried out in developing countries reported that mothers apply substances such as mustard oil, turmeric, cow dung, and antiseptic lotion to the cord stump.5,11,19 Even though there are some studies which are conducted in developing countries, there was no study conducted in Ethiopia assessing umbilical cord care practice of mothers. Therefore, this study was conducted to determine the umbilical cord care practices of mothers visiting Mizan-Tepi University teaching hospital.
Methods and Materials
Study Area, Setting and Period
Mizan Tepi Teaching Hospital [MTUTH] is located in southwest people region, southwest Ethiopia. The hospital is located in Mizan Aman Town, and provides various health services for the population from its catchment area. The hospital provides various services such as outpatient treatment, ANC, maternal and child health and inpatient services. This study was conducted from August to October 29, 2021.
Study Design and Population
A facility-based cross-sectional study was conducted among mothers who had given birth in the last six months. All mothers who had an infant age less than six months and visited MTUTH were the source population. Randomly selected women who have an infant age less than six months and visited MTUTH during the study period were the study population. All women who gave birth, who were within six-month postpartum and who came to the immunization clinic and Pediatrics OPD of MTUTH during the data collection period, and mothers who were willing to participate were included in the study. Mothers who were unable to respond to the questionnaire because of severe illness or mental problems were excluded from the study.
Sample Size Determination and Sampling Techniques
The required sample size was determined using a single-population proportion formula. The prevalence of cord care practices in the study area is unknown, so we took 50% since there is no previous study and the minimum adequate sample size will be achieved by taking 50%. Therefore, taking this (p = 0.50) and 5% margin of error, the sample size was calculated as follows: (zα/2).(1−p) d2 = (1.96) 2* 0.50*0.40 = 384. By adding 10% non-response rate, the final sample size was 422. A systematic random sampling technique was used to include women attending Pediatric OPD and MCH clinics during the data collection period. We took the total number of mothers who previously came to immunization and OPD clinics, and after taking that report, we calculated the K-value. The total number of mothers who came to immunization and under five OPD was 845; by dividing the total flow to our sample size, it gives 2.00; every 2 mothers were selected for an interview.
Data Collection Techniques and Data Quality Control
A pretested interviewer-administered structured questionnaire adapted from a previously similar study was used to collect data. The tool includes socio-demographic characteristics of the study participants (age, residence, marital status, occupational status, and educational status), obstetric related factors (ANC visit, colostrum feeding, initiation of breastfeeding, and place of delivery) and cord care-related questions (substance applied to cord, cord care). The questionnaire was prepared in English and translated into the local language (Amharic) by a language expert. It was also back-translated into English to ensure consistency. The Amharic version of the questionnaire was used to collect the data. To ensure the quality of the data, two days of training were given before data collection for data collectors and supervisors regarding the objective of the study and techniques of data collection. Data were collected by 3 BSc nurses, and daily supervision was performed by the principal investigator. The supervisors checked each filled questionnaire for completeness during the data collection.
Data Processing and Analysis
Data were entered into Epi data version 3.1 and exported to SPSS version 26 for analysis. Data were presented as tables and proportions (percentages). Binary logistic regression was used to assess the association between the outcome and independent variables. The outcome variable (cord care practice) was categorized as good practice (coded as 1) and poor practice (coded as 0). Odds ratio (OR) with 95% confidence intervals (CI) and a p-value were used to measure the strength of the association. In the bivariate analysis, variables with p-values <0.25 were considered as candidates for a multivariable analysis. Statistical significance was declared at a p-value <0.05.
Ethical Consideration
Ethical clearance was obtained from the ethical review Committee of Mizan-Tepi University, College of Medicine and Health Sciences with a protocol number of Nurs/375/01/14. Then, official letter was submitted to MTUTH administrative bodies. A necessary explanation was given for the participant about the purpose and their right to participate or not to participate in the study. Confidentiality of the response was declared to the respondents by the anonymity of the interviewer-administered questionnaire. Participant’s oral informed consent was taken before recruitment to participate in the study. Participant’s oral informed consent was taken before recruitment to participate in the study, and it was approved by the ethics committee. Name and other personal information that can violate the confidentiality of the respondents were not taken. The study was approved by Mizan-Tepi University ethical review committee, and it was conducted in accordance with the Declaration of Helsinki.
Results
Socio-Demographic Characteristics of the Study Participants
A total of 422 mothers participated in this study, yielding a response rate of 100%. Most of the respondents 228 (54%) were between 25 and 34 years, with a median age 32 years. The Majority of the respondents 289 (94.8%) were married. Nearly one-fourth 100 (23.7%) of the respondents had not attended formal education. Regarding their occupation, 177 (41.9%) were merchants. Majority, 349 (82.7%) of study participants were urban dwellers (Table 1).
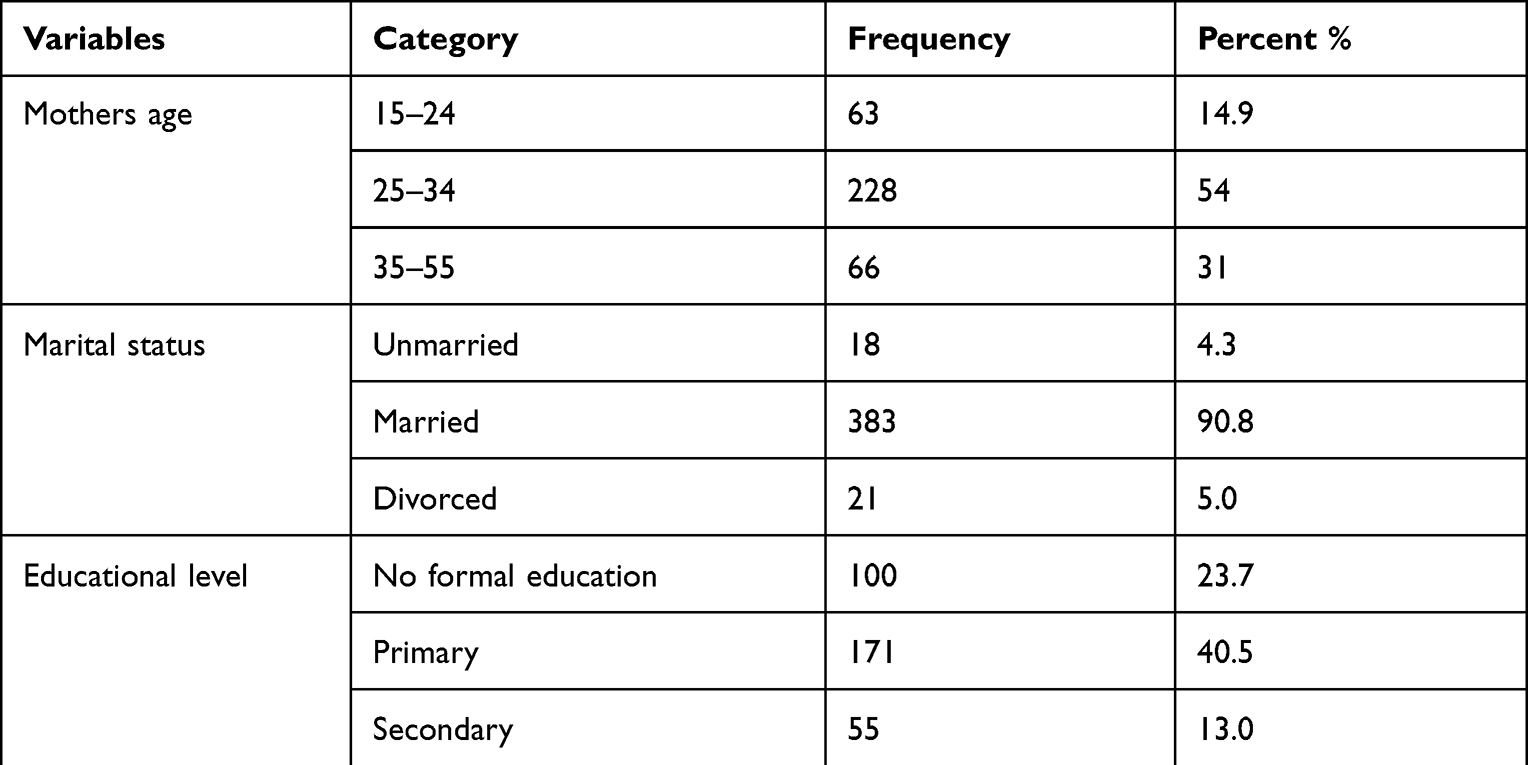 |
Table 1 Socio-Demographic Characteristics of Mothers Who Delivered Their Babies in the Last Six Months in Mizan-Tepi University Teaching Hospital South-West Ethiopia, 2021 |
Obstetric-Related Factors and Cord Care Practice
The majority, 403 (95.5%) of participants, had ANC visits for their current pregnancy of which 162 (38.4%) had ANC visits at a government hospital, 132 (31.3%) at health centers, and the rest had ANC visits at private health facilities. With regard to place of delivery, the vast majority of mothers 400 (94.8%) gave birth in health care facilities. More than half 231 (54.7%) of the respondents were reported as applied substance on the cord, of these 82 (35.5%) and 123 (53.0%) of the women had applied butter and Vaseline, respectively (Table 2). The proportion of mothers who had good cord care practice in this study was 59.2% CI (54.3–63.3%).
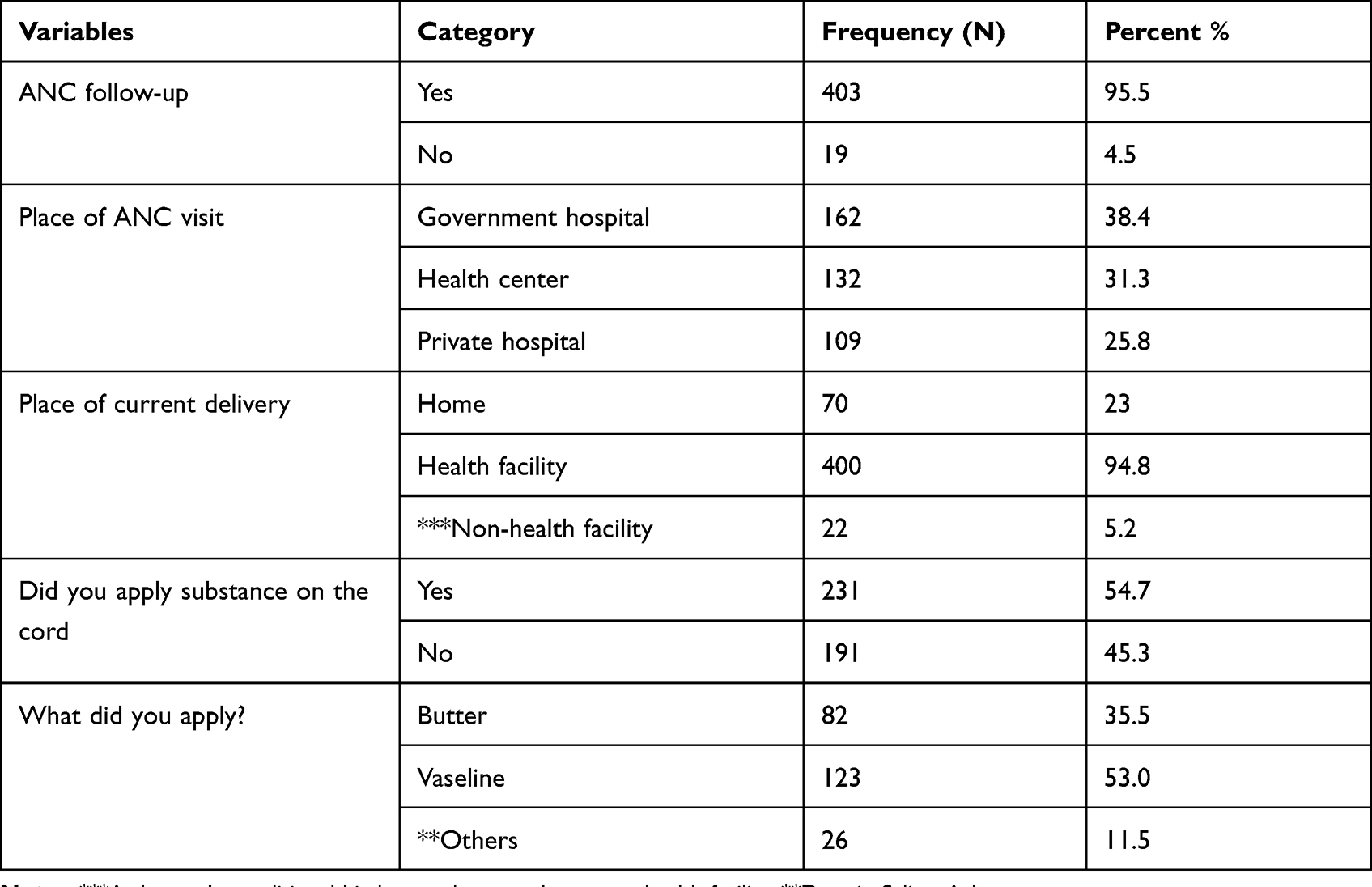 |
Table 2 Obstetrics-Related Factors and Cord Care Practice Among Mothers Who Delivered Her Babies in the Last Six Months in Mizan-Tepi University Teaching Hospital South-West Ethiopia, 2021 |
Factors Associated with Maternal Cord Care Practice
In bivariate logistic regression analysis, factors with a p-value of ≤0.25 were educational status of the mother, occupation, place of delivery, initiation of breastfeeding, colostrum feeding, ANC follow-up, and application of anything on the cord.
To control for possible confounders, all independent variables with a p-value ≤0.25 on the bivariate logistic regression analysis were included in the multivariable analysis, and p-value less than 0.05 in the multivariable logistic regression was considered as significant. Multivariable analysis showed that maternal educational status, application of substance on the cord, initiation of breastfeeding and ANC follow-up were significantly associated with good cord care practice.
Mothers who attended college and the above educational attainment were 5 times more likely to have good cord practice than those who had no formal education (AOR = 4.71; 95% CI = 2.19–10.14). Mothers who initiated breastfeeding within one hour of delivery were 2 times more likely to have good cord practice than those who initiated breastfeeding after one hour (AOR = 1.69; 95% CI = 1.07–2.68). Mothers who had ANC follow-up during their current pregnancy were 3 times more likely to have good cord care practice than those mothers who had no ANC follow-up in their current pregnancy (AOR = 3.58; 95% CI = 1.24–10.32) (Table 3).
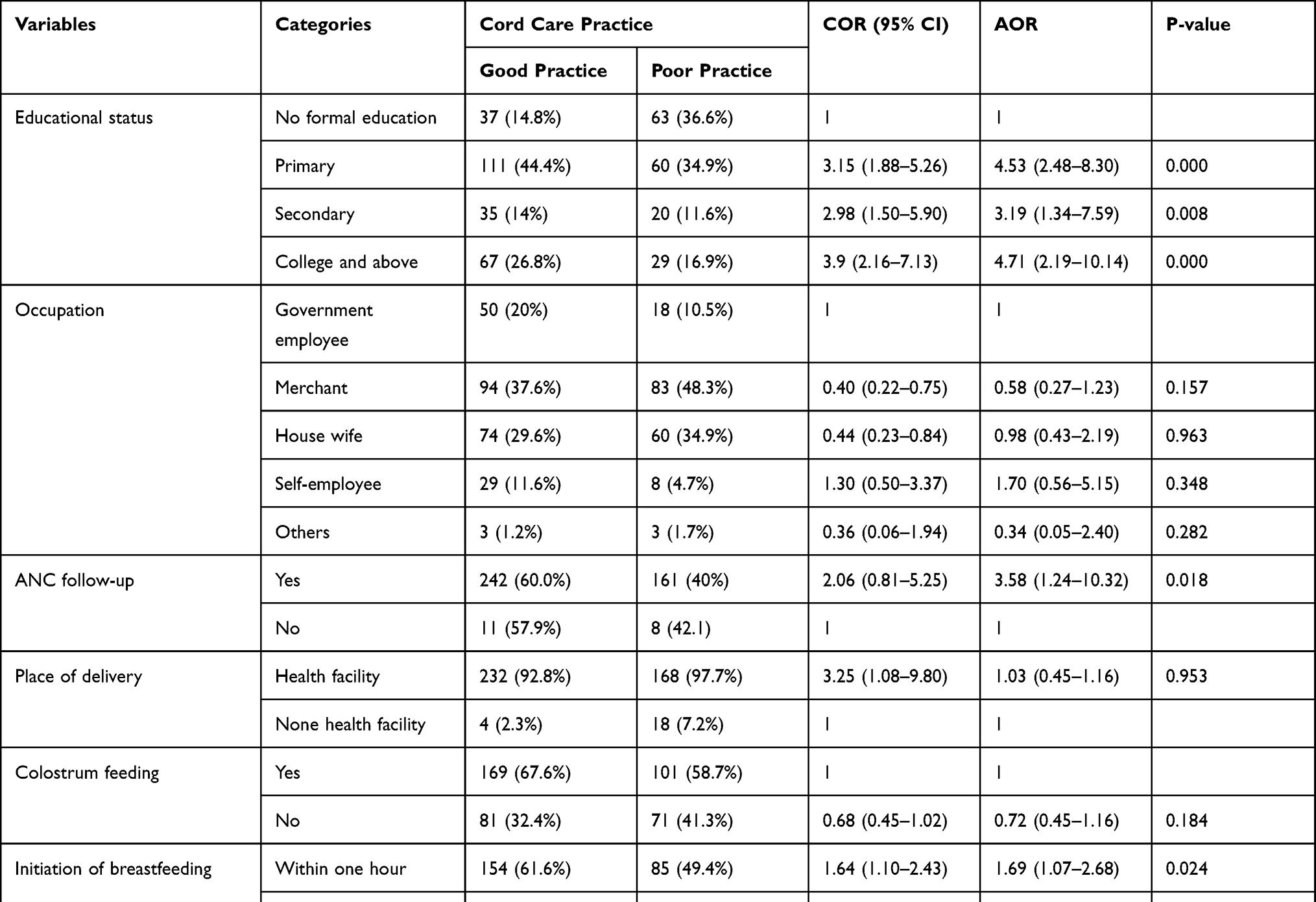 |
Table 3 Bivariate and Multivariable Logistic Regression Analysis of Factors Associated with Maternal Cord Care Practice Among Mothers Who Delivered Her Babies in the Last Six Months in Mizan-Tepi University Teaching Hospital South-West Ethiopia, 2021 |
Discussion
In this study, the overall cord care practice of mothers was 59.2% CI (54.3–63.3%). More than half (54.7%) of the respondents reported having applied unnecessary substances to the cord; among these, 24.2% and 21.2% of the women had applied butter and Vaseline, respectively.
This is higher than a study conducted in India on cord care (49%),15 and the discrepancy between these findings might be attributed to the difference in methods used, study settings, and sample size used. Furthermore, the variation might be due to expanding health care coverage, increased awareness and information, and maternal health services. The findings of this study were consistent with a study conducted in Nigeria (61.4%)5 and Rwanda (54%).11 However, the findings of this study were lower than those of studies conducted in Chit wan district (95%),16 East Gojjam (94.6%),17 Nepal (73%),18 and Nigeria (82.0%).19 This variation might be due to the study setting and multi-cultural variation among countries and regions. This may be due to study setting and multi-cultural variation among countries and regions.
A study conducted in Ghana20 found that mothers’ educational status was significantly associated with cord care practices. The use of beneficial cord care practices increased as maternal education increased.2 The practice of cord care grew in tandem with mother’s education. Highly educated mothers are more likely to practice good cord care because they might have learned what should be done for cord care. Differences in educational status may be caused by the health extension program of the country which provides adequate service for all mothers regardless of educational status. These findings are consistent with studies that show that the higher the level of maternal education, the better the health-seeking behavior and thus exposure to better knowledge of cord care practice. The umbilical cord is an important portal of entry for pathogenic agents. Thus, parents, especially mothers, need to understand the necessity of appropriate cord care practices.5
In our study, mothers who had ANC follow-up in a health facility were more likely to have effective cord care practices than those who had no ANC follow-up. This finding is consistent with studies conducted in Cameroon.21 The possible reason could be that mothers who visited ANC would receive counseling on the advantages of delivery by skilled birth attendants and institutional delivery, which is believed to increase their knowledge and practice about good cord care.22
Mothers who did not add anything to the cord must have practiced good cord care, indicating that the use of harmful agents was more common among mothers of babies delivered at traditional birth attendant’s location. The majority of mothers who used nothing in the cord had better cord care practices than those who used something in the cord.23 The use of substances in cord care has long been linked to umbilical cord infection in studies conducted in various settings.24,25 This has highlighted the significance of culture as a driver of cord care practice, as well as its underappreciated subtle contributions to neonatal morbidity and mortality, particularly in resource-poor countries. The World Health Organization has stated that dry and cord care practices are critical for reducing neonatal and under-five mortality in developing countries.1
Conclusion and Recommendations
The proportion of mothers with good cord care practices was inadequate. For such a high cause of neonatal death, prevention should be the priority intervention, and improving its implementation requires further effort. Umbilical cord infection is preventable through affordable and straightforward strategies, including evidence-based cord care and avoiding unnecessary applications.
Acknowledgments
We are grateful to the mothers who participated in this study. We are thankful to those who allowed us to conduct this study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation or in all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; agreed on the journal to which the article has been submitted; and agreed to be accountable for all aspects of the work.
Funding
The authors received no specific fund for this work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Opara PI, Jaja T, Dotimi DA, Alex-Hart BA Newborn cord care practices amongst mothers in Yenagoa local government area, Bayelsa State, Nigeria; 2012.
2. Mohammad AU, Omeneke IK, Kehinde IP, Omoshalewa UM, Fatima JB. Determinants of Umbilical Cord Care Practices among Mothers of Neonates Admitted into Special Care Baby Unit of Usmanu Dan Fodiyo University Teaching Hospital, Sokoto, Nigeria; 2021.
3. Perry DS. The umbilical cord: transcultural care and customs. J Nurse Midwifery. 1982;27(4):25–30. doi:10.1016/0091-2182(82)90166-5
4. World Health Organization. WHO recommendations on newborn health: guidelines approved by the WHO Guidelines Review Committee. World Health Organization; 2017.
5. Chizoma MN, Fisayo Oluwatosin M, Abimbola OO. Umbilical cord care knowledge and practices of mothers attending selected Primary Health Care Centres in Ibadan, Nigeria. Int J Caring Sci. 2020;13(1):143–151.
6. Clark H, Coll-Seck AM, Banerjee A, et al. A future for the world’s children? A WHO–UNICEF–Lancet Commission. Lancet. 2020;395(10224):605–658. doi:10.1016/S0140-6736(19)32540-1
7. Lawn JE, Cousens S, Zupan J; Team LNSS. 4 million neonatal deaths: when? Where? Why? lancet. 2005;365(9462):891–900. doi:10.1016/S0140-6736(05)71048-5
8. Mullany LC, Darmstadt GL, Khatry SK, et al. Topical applications of chlorhexidine to the umbilical cord for prevention of omphalitis and neonatal mortality in southern Nepal: a community-based, cluster-randomised trial. Lancet. 2006;367(9514):910–918. doi:10.1016/S0140-6736(06)68381-5
9. Antia-Obong O, Ekanem E, Udo J, Utsalo S. Septicaemia among neonates with tetanus. J Trop Pediatr. 1992;38(4):173–175. doi:10.1093/tropej/38.4.173
10. Güvenç H, Güvenç M, Yenioglu H, Ayata A, Kocabay K, Bektasl S. Neonatal omphalitis is still common in eastern Turkey. Scand J Infect Dis. 1991;23(5):613–616. doi:10.3109/00365549109105186
11. Uwingabire E, Tengera O, Batamuriza M, Mukamana D. Umbilical cord care among postnatal mothers in Kibungo Hospital catchment area, Rwanda. Rwanda J Med Health Sci. 2020;3(2):167–180. doi:10.4314/rjmhs.v3i2.7
12. Liu L, Oza S, Hogan D, et al. Global, regional, and national causes of child mortality in 2000–13, with projections to inform post-2015 priorities: an updated systematic analysis. Lancet. 2015;385(9966):430–440. doi:10.1016/S0140-6736(14)61698-6
13. Traverso H, Kahn A, Rahim H, et al. Ghee applications to the umbilical cord: a risk factor for neonatal tetanus. lancet. 1989;333(8636):486–488. doi:10.1016/S0140-6736(89)91378-0
14. Mull DS, Anderson JW, Mull JD. Cow dung, rock salt, and medical innovation in The Hindu Kush of Pakistan: the cultural transformation of neonatal tetanus and iodine deficiency. Soc Sci Med. 1990;30(6):675–691. doi:10.1016/0277-9536(88)90253-5
15. Sinha LN, Kaur P, Gupta R, Dalpath S, Goyal V, Murhekar M. Newborn care practices and home-based postnatal newborn care programme – Mewat, Haryana, India, 2013. WPSAR. 2014;5(3):22. doi:10.5365/wpsar.2014.5.1.006
16. Chaudhary J, Dhungana G, Ghimire HC. Factors affecting newborn care practices among Tharu mothers in selected village development committees of Chitwan district. J Chitwan Med Coll. 2013;3(1):42–45. doi:10.3126/jcmc.v3i1.8465
17. Kokebie T, Aychiluhm M, Degu G. Community based essential newborn care practices and associated factors among women in the rural community of Awabel district. Int J Adv Sci Res. 2015;1(1):17–27. doi:10.7439/ijasr.v1i1.1637
18. Tuladhar S The Determinants of Good Newborn Care Practices in the Rural Areas of Nepal; 2010.
19. Abegunde D, Orobaton N, Beal K, et al. Trends in newborn umbilical cord care practices in Sokoto and Bauchi States of Nigeria: the where, who, how, what and the ubiquitous role of traditional birth attendants: a lot quality assurance sampling survey. BMC Pregnancy Childbirth. 2017;17(1):1–11. doi:10.1186/s12884-017-1551-x
20. Asiedu SSO, Apatu NAA, Tetteh R, Hodgson A. Neonatal cord care practices among mothers and caregivers in the Volta region of Ghana. Int J Matern Child Health AIDS. 2019;8(1):63. doi:10.21106/ijma.272
21. Saaka M, Iddrisu M. Patterns and determinants of essential newborn care practices in rural areas of northern Ghana. Int J Popul Res. 2014;2014:1–10. doi:10.1155/2014/404387
22. Ababa A. Federal Democratic Republic of Ethiopia Ministry of Health. Ethiopia: Postnatal Care; 2003.
23. Ambe J, Bello M, Yahaya S, Omotara B. Umbilical cord care practices in Konduga local government area of Borno State, North-eastern Nigeria. Internet J Trop Med. 2009;5(2):34–41.
24. Mullany LC, Darmstadt GL, Katz J, et al. Risk of mortality subsequent to umbilical cord infection among newborns of southern Nepal: cord infection and mortality. Pediatr Infect Dis J. 2009;28(1):17. doi:10.1097/INF.0b013e318181fb4c
25. Petwa V, Callender-Carter ST Factors influencing the prevalence of umbilical cord sepsis among newborn babies at the China-Uganda Friendship Hospital Naguru. GRIN Verlag; 2015.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Harmful Traditional Practices of Umbilical Cord in Edaga Hamus Community, Asmara, Eritrea

Negash FB, Simel LL, Tekle LR, Berhane BB
Pediatric Health, Medicine and Therapeutics 2024, 15:181-188
Published Date: 14 May 2024