Back to Journals » Journal of Pain Research » Volume 19
Ultrasound-Guided Transversus Abdominis Plane Block Using 0.125% versus 0.25% Bupivacaine for Postoperative Opioid Consumption in Kidney Transplant Recipients: A Prospective, Randomized, Double-Blind Clinical Trial
Authors Nonphiaraj S ![]() , Siwakul P, Sangsungnern P
, Siwakul P, Sangsungnern P ![]() , Intrapongpan J
, Intrapongpan J ![]() , Theeragul S, Nuwatkrisin K
, Theeragul S, Nuwatkrisin K ![]() , Somdee W, Wanphon K
, Somdee W, Wanphon K ![]()
Received 31 October 2025
Accepted for publication 16 February 2026
Published 21 February 2026 Volume 2026:19 578126
DOI https://doi.org/10.2147/JPR.S578126
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Karina Gritsenko
Saranyoo Nonphiaraj,1 Patipharn Siwakul,1 Peerapong Sangsungnern,1 Jedniphat Intrapongpan,1 Suapa Theeragul,2 Kanrapee Nuwatkrisin,2 Wilawan Somdee,1 Krittiya Wanphon1
1Department of Anesthesiology, Faculty of Medicine, Khon Kaen University, Khon Kaen, Thailand; 2Department of Surgery, Faculty of Medicine, Khon Kaen University, Khon Kaen, Thailand
Correspondence: Peerapong Sangsungnern, Department of Anesthesiology, Faculty of Medicine, Khon Kaen University, Khon Kaen, 40002, Thailand, Tel +66-43-363060, Email [email protected]
Purpose: Transversus abdominis plane (TAP) block is a widely accepted technique for postoperative pain management in kidney transplant (KT) patients, typically with 0.25– 0.5% bupivacaine. Lower concentrations, such as 0.125%, may reduce systemic toxicity while remaining effective. This study aimed to compare the efficacy and safety of 0.125% versus 0.25% bupivacaine for TAP block in KT patients.
Patients and Methods: In this prospective, double-blind, randomized trial, KT patients received either 0.125% or 0.25% bupivacaine for ultrasound-guided TAP block prior to surgery, followed by intravenous fentanyl patient-controlled analgesia postoperatively. The primary outcome was 24-hour fentanyl consumption. Secondary outcomes included intraoperative fentanyl use, time to first analgesic request, pain scores, TAP block complications, opioid-related side effects, and patient satisfaction.
Results: Seventy-six patients were enrolled, with 74 completing the study (37 per group). Baseline characteristics were comparable between groups. Intraoperative fentanyl use was significantly lower in the 0.25% bupivacaine group (140.5 ± 39.7 mcg) compared to the 0.125% group (166.8 ± 44.7 mcg; P = 0.009). However, 24-hour postoperative fentanyl consumption did not differ significantly, with the 0.125% group using 201.5 ± 110.4 mcg and the 0.25% group using 177.3 ± 104.1 mcg (mean difference: − 24.2; 95% CI: − 73.9 to 25.5; P = 0.335). The 0.25% group had a longer median time to first analgesic request (15 vs 10 minutes; P = 0.020). Postoperative pain scores, TAP block complications, and patient satisfaction were similar between groups.
Conclusion: TAP block with 0.125% bupivacaine provided comparable postoperative opioid consumption and pain scores to 0.25%, without associated complications.
Keywords: transversus abdominis plane block, TAP block, bupivacaine, kidney transplant, renal transplant, postoperative pain, opioid consumption
Introduction
Postoperative pain is a widely recognized issue after kidney transplant (KT), with some patients experiencing intense discomfort that can be difficult to manage.1 Effective postoperative pain management after KT is crucial, as it facilitates early oral intake, early mobilization, and improved respiratory function—key factors in optimizing graft outcomes and patient recovery.2,3
Guidelines from the Enhanced Recovery After Surgery (ERAS) society and other expert consensus recommend multimodal analgesia—including the use of opioids, non-opioid analgesics, and regional anesthesia such as the transversus abdominis plane (TAP) block—to optimize pain control and minimize opioid use in this high-risk population.2,4 However, analgesic options in patients with reduced kidney function are limited. Accumulation of renally excreted opioids and their toxic metabolites may lead to oversedation, myoclonus, seizures, and respiratory depression.5 Non-steroidal anti-inflammatory drugs (NSAIDs) should be avoided due to their potential nephrotoxicity.6,7 Epidural block may be controversial because of the risk of epidural hematoma from platelet dysfunction or reduced graft perfusion caused by hypotension.8
TAP block has emerged as a valuable component of multimodal analgesia for abdominal surgeries, including KT, by targeting the T10–L1 spinal nerves located between the internal oblique (IO) and transversus abdominis (TA) muscles.4,9,10 It covers the typical KT incision area without the side effects or risks associated with neuraxial techniques.11 Recent meta-analyses have shown that TAP blocks significantly reduce postoperative opioid consumption and pain scores in KT recipients, with bupivacaine concentrations commonly ranging from 0.25% to 0.5%.9,12 TAP block with a lower concentration, such as 0.125% bupivacaine, has also been effective for pain control in various types of surgery, including laparoscopic appendectomy, laparoscopic hysterectomy, lower abdominal surgery, and inguinal hernia repair.13–16 Furthermore, in inguinal hernia repair, TAP block using 0.125% bupivacaine has been shown to be as effective as 0.25% in reducing opioid consumption and postoperative pain scores.17,18
Renal failure increases the risk of local anesthetic systemic toxicity (LAST), largely due to reduced drug clearance. Additionally, conditions common in renal failure, such as uremia and acidosis, can lead to higher concentrations of free local anesthetics in the body.19 As a result, careful selection of local anesthetic concentration is essential to balance analgesic efficacy and minimize toxicity. However, despite its widespread use, current evidence—summarized in systematic reviews—shows that the optimal bupivacaine concentration to maximize efficacy while minimizing toxicity in the KT population remains unclear.12
We hypothesized that ultrasound-guided TAP block using 0.125% bupivacaine would provide postoperative analgesia that is not clinically inferior to that achieved with 0.25% bupivacaine, as measured by 24-hour fentanyl consumption, while potentially offering a better safety profile with respect to LAST. To test this, we conducted a randomized, double-blind clinical trial comparing these two concentrations in KT recipients.
Materials and Methods
Design and Ethics
This prospective, double-blind, randomized controlled trial was conducted at Srinagarind Hospital, Khon Kaen University, Thailand, from October 2023 to December 2024. All kidneys were donated voluntarily with written informed consent, in accordance with the principles of the Declaration of Istanbul on Organ Trafficking and Transplant Tourism. All procedures followed the ethical standards laid down in the Declaration of Helsinki. The study protocol was approved by the Khon Kaen University Ethics Committee for Human Research (HE661296) and registered with the Thai Clinical Trials Registry (TCTR20230919004). Written informed consent was obtained from all participants prior to enrollment. The trial was designed, conducted, and reported in accordance with the Consolidated Standards of Reporting Trials (CONSORT) guidelines for randomized clinical trials.
Participants
Adults aged 18 years or older with end-stage renal disease (ESRD) scheduled for KT and classified as American Society of Anesthesiologists Physical Status (ASA PS) Class III or IV were eligible for inclusion in this study. Patients were excluded if they had a history of chronic pain, had used analgesic medication within 24 hours prior to surgery, or had been on long-term treatment (at least 3 months) with antidepressants, antipsychotics, anticonvulsants, or clonidine. Additional exclusion criteria were a known allergy to any of the study medications, current pregnancy or lactation, contraindications to performing a TAP block such as coagulopathy or localized skin infection, and either inability or refusal to use intravenous patient-controlled analgesia (IV PCA). Patients were withdrawn from the study if they required re-operation within 24 hours postoperatively, exhibited symptoms of LAST, or experienced intraperitoneal injection during the TAP block procedure.
Randomization and Blinding
Participants were randomly assigned in a 1:1 ratio to either the 0.125% or 0.25% bupivacaine group using a computer-generated block-of-four randomization list. The randomization sequence was generated by an independent statistician from the Clinical Epidemiology Unit who was not involved in patient recruitment, intraoperative management, or outcome assessment. Allocation concealment was ensured with sequentially numbered, sealed opaque envelopes, opened only after the patient arrived in the operating room. In the 0.25% group, patients received 50 mg of bupivacaine (10 mL) and 100 mcg of adrenaline (0.1 mL), diluted with normal saline to a total volume of 20 mL. In the 0.125% group, patients received 25 mg of bupivacaine (5 mL) and 100 mcg of adrenaline (0.1 mL), also diluted to 20 mL. Both solutions were prepared in identical syringes, matched for volume and appearance, by a research team member not involved in patient care or outcome assessment. As a result, the anesthesiologists performing the TAP block, the attending anesthesiologist, and the outcome assessors were all blinded to group allocation.
Study Protocol
Preoperative
After KT scheduling, patients received study information and provided written informed consent. They were then instructed on how to use the IV PCA device and the numerical rating scale (NRS) for pain assessment. Baseline characteristics—including sex, age, weight, height, body mass index (BMI), underlying diseases, ASA PS classification, and laboratory values—were recorded.
Intraoperative
Standard monitoring and preoxygenation were performed. Baseline vital signs were recorded 5 minutes after the patient was positioned on the operating table. General anesthesia was induced with fentanyl (1 mcg/kg IV), propofol (1.5–2.5 mg/kg IV), and either succinylcholine (1–1.5 mg/kg IV) or rocuronium (1–1.2 mg/kg IV), followed by endotracheal intubation. Paracetamol 1000 mg IV was administered after intubation.
An ultrasound-guided unilateral TAP block was performed on the surgical side after intubation using an in-plane technique, targeting the posterior end of the TAP (posterior approach). The block was performed by one of three experienced anesthesiologists from the research team, all proficient in the technique. A linear ultrasound probe was placed at the midaxillary line between the subcostal margin and iliac crest. The three muscle layers—external oblique (EO), internal oblique (IO), and transversus abdominis (TA)—were identified, and the probe was moved posteriorly to the most posterior limit of the TAP between the IO and TA muscles (Figure 1). Once the needle tip was properly positioned, the assigned concentration of bupivacaine (0.25% or 0.125%) was administered. Correct TAP placement was confirmed by visualizing the needle tip between the IO and posterior end of TA muscles with fascial plane separation during injectate spread. As the block was performed under general anesthesia, sensory testing was not feasible; block effectiveness was therefore assessed indirectly by hemodynamic responses to surgical stimulation, with more than 20% increases in blood pressure or heart rate prompting supplemental fentanyl. TAP block-related complications—such as hematoma, LAST, and intraperitoneal injection—were monitored.
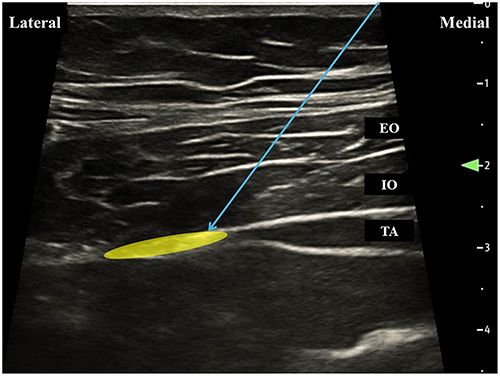 |
Figure 1 Ultrasonographic image of the posterior transversus abdominis plane (TAP) block. The needle is inserted at the midaxillary line from medial to lateral using an in-plane technique, targeting the posterior end of the TAP. Blue arrow, needle patch; yellow area, target plane for local anesthetic deposition. Abbreviations: EO, external oblique muscle; IO, internal oblique muscle; TA, transversus abdominis muscle. |
General anesthesia was maintained with sevoflurane in oxygen and air, targeting a minimum alveolar concentration of 1. Intraoperative fentanyl was administered at the attending anesthesiologist’s discretion in response to hemodynamic changes (increase of >20% from baseline), with 25 mcg IV doses titrated every 5 minutes as needed. No other analgesics were used intraoperatively. Intraoperative data were recorded, including total fentanyl consumption, incision site, operative time, and estimated blood loss.
At the end of surgery, patients received ondansetron 8 mg IV for postoperative nausea and vomiting (PONV) prophylaxis. Anesthesia was then discontinued, and neuromuscular blockade was reversed. No additional local anesthetic was administered via wound infiltration by the surgeon.
Postoperative
After extubation, patients were connected to IV PCA (fentanyl 10 mcg/mL; PCA-only mode, 1 mL bolus, 5-minute lockout, maximum 8 mL/hour) for at least 24 hours. Standard postoperative care was provided, and patients were transferred to the ward or ICU as clinically indicated. All patients also received 1000 mg of IV paracetamol every 6 hours for 24 hours. Postoperative pain scores using the NRS (at rest and during activity) and opioid-related complications (PONV, drowsiness, and pruritus) were assessed every 6 hours for 24 hours by ward nurses blinded to group allocation. Cumulative fentanyl consumption and time to first analgesic request were retrieved from the IV PCA machine records. Patient satisfaction with pain management was assessed at 24 hours postoperatively using a 5-point Likert scale (1 = strongly disagree, 2 = disagree, 3 = neither agree nor disagree, 4 = agree, 5 = strongly agree).
Outcomes Measurement
The primary outcome was cumulative fentanyl consumption during the first 24 hours after surgery. Secondary outcomes included intraoperative fentanyl use, time to first analgesic request, NRS pain scores at rest and with movement at 0, 6, 12, 18, and 24 hours postoperatively, and complications related to the TAP block or opioid use—such as hematoma, LAST, intraperitoneal injection, PONV, drowsiness, and pruritus. Patient satisfaction with pain management was also assessed.
Sample Size Calculation
Our data from KT recipients who received a TAP block with 0.25% bupivacaine showed a mean 24-hour postoperative fentanyl consumption of 221.25 ± 62.45 mcg. Using this value, a sample size calculation was performed with 90% power, a significance level of 0.05, and margin of 20% (44.25 mcg). The calculation indicated that at least 34 patients were required per group. To allow for a potential 10% dropout rate, the final sample size was set at 38 patients per group.
Statistical Analysis
Analyses were performed on a per-protocol basis, including all randomized patients who received the allocated TAP block and completed 24-hour postoperative follow-up (n = 74). There were no missing data among the 74 analyzed patients; therefore, no imputation methods were required. Categorical variables were reported as frequencies and percentages and analyzed using either the Chi-square test or Fisher’s exact test, as appropriate. Continuous variables were presented as mean ± standard deviation (SD) or median with interquartile range (IQR) and compared using the independent t-test or Mann–Whitney U-test, as appropriate. Mean or median differences and their 95% confidence intervals (CI) were calculated. Repeated NRS pain scores were analyzed using generalized estimating equations (GEE) with Bonferroni correction. All statistical analyses were conducted using STATA version 18 (StataCorp LP, College Station, TX, USA). A p-value of less than 0.05 was considered statistically significant.
Results
Eighty-one patients scheduled for KT were screened for eligibility. Five were excluded due to the unavailability of an anesthesiologist to perform the TAP block. Seventy-six patients were enrolled and randomized to receive either 0.125% or 0.25% bupivacaine in the TAP block, with 38 patients in each group. One patient in the 0.25% group was withdrawn due to postoperative delirium that prevented IV PCA use, and one in the 0.125% group was withdrawn after requiring reoperation, leaving 74 patients who completed the study (Figure 2).
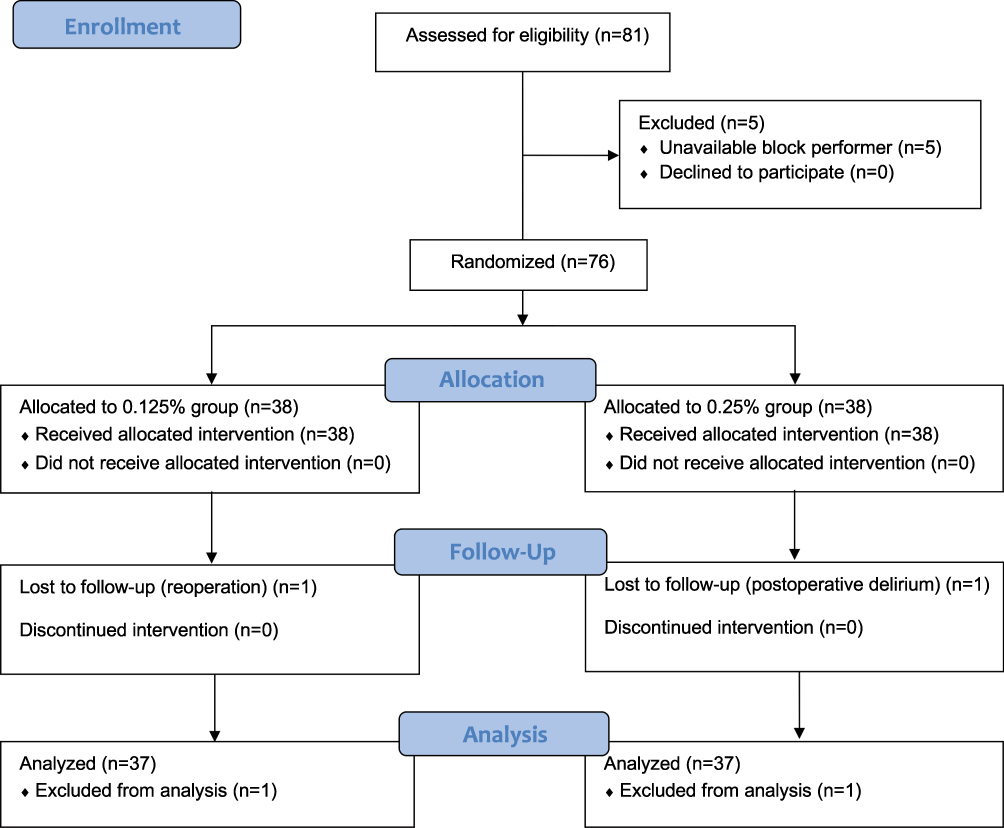 |
Figure 2 Consolidated Standards of Reporting Trials (CONSORT) flow diagram of the study population. Abbreviation: IV PCA, intravenous patient-controlled analgesia. |
Baseline characteristics and intraoperative data were similar between the groups (Table 1). Although baseline serum creatinine and estimated glomerular filtration rate (GFR) were slightly different between groups (with numerically higher serum creatinine and lower GFR in the 0.125% group), these differences were not statistically significant, and all patients had end-stage renal disease requiring transplantation. Most participants were male (53.9%) with a mean age of 43 years. All patients were classified as ASA PS class 3. The most common comorbidity was hypertension (79.7%). Regarding intraoperative data, 93.2% had a right-sided incision, the average operative time was 138 minutes, and estimated blood loss ranged from 150 to 200 mL.
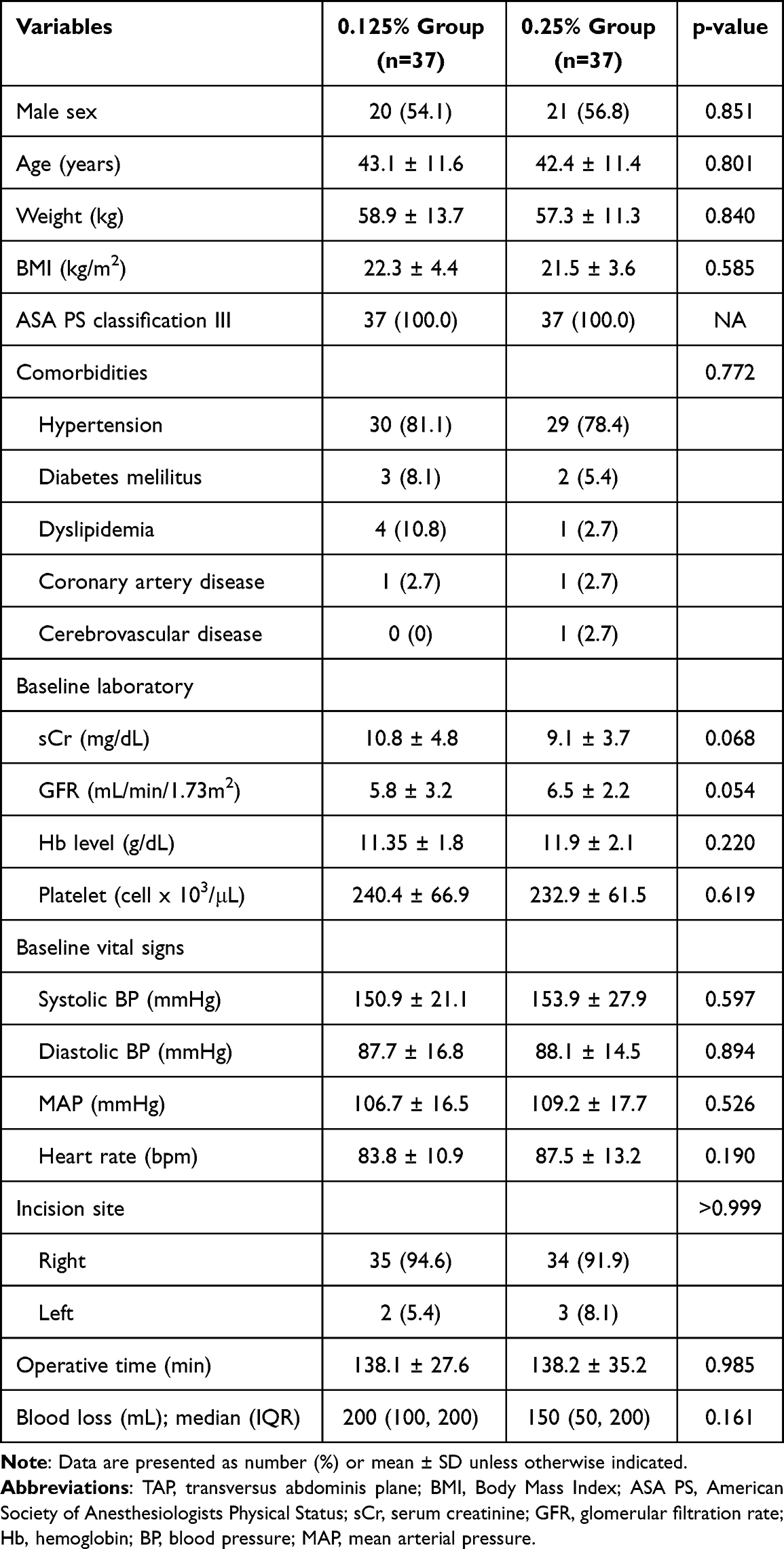 |
Table 1 Baseline Characteristics and Intraoperative Data of Kidney Transplant Recipients Categorized by Bupivacaine Concentration Used for TAP Block |
Fentanyl consumption and time to first analgesic request are shown in Table 2. Intraoperative fentanyl consumption was significantly lower in the 0.25% group compared to the 0.125% group (140.5 ± 39.7 mcg vs 166.8 ± 44.7 mcg; mean difference: −26.2 mcg, 95% CI: −45.8 to −6.6, P = 0.009). However, total fentanyl consumption within the first 24 hours postoperatively did not differ significantly between the groups (177.3 ± 104.1 mcg in the 0.25% group vs 201.5 ± 110.4 mcg in the 0.125% group; mean difference: −24.2 mcg, 95% CI: −73.9 to 25.5, P = 0.335). The median time to first analgesic dose was significantly shorter in the 0.125% group at 10 (0, 15) minutes compared to 15 (10, 30) minutes in the 0.25% group (P = 0.020).
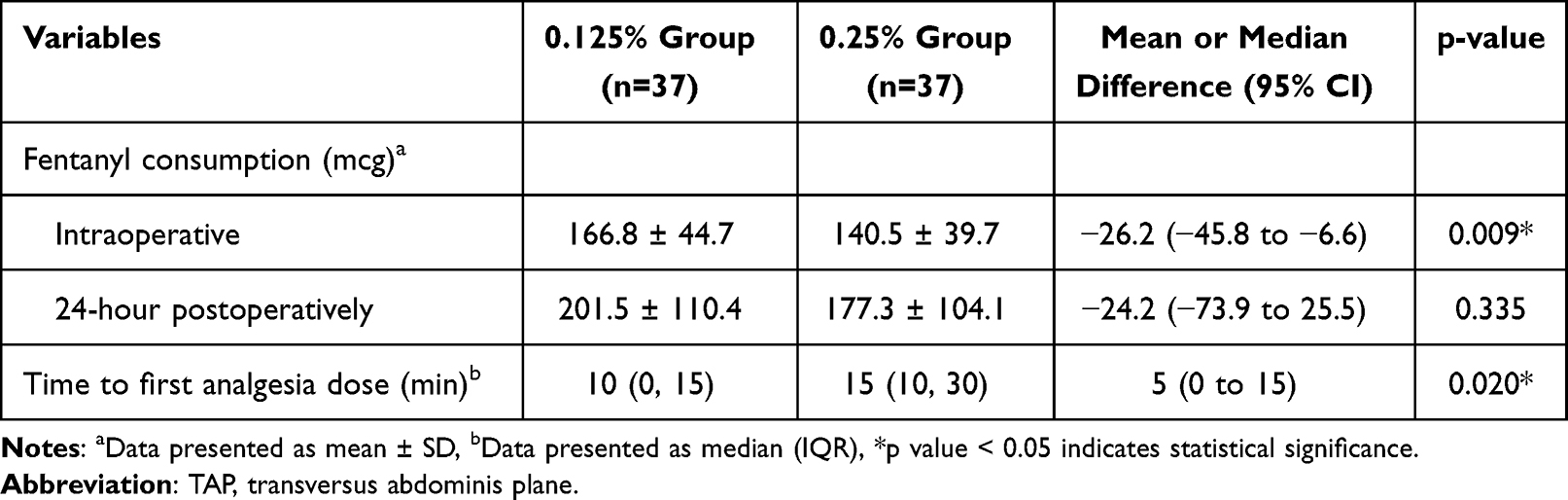 |
Table 2 Comparison of Fentanyl Consumption and Time to First Analgesic Dose Between 0.125% and 0.25% Bupivacaine Groups for TAP Block in Kidney Transplant Recipients |
Pain scores assessed by the NRS (Table 3) did not differ significantly between the two groups at any time point, either at rest or during activity. The overall difference in pain NRS over the 24-hour postoperative period, analyzed using GEE, was 0.1 (95% CI: −1.0 to 1.1, P = 0.889) at rest and 0.2 (95% CI: −0.9 to 0.6, P = 0.620) during activity.
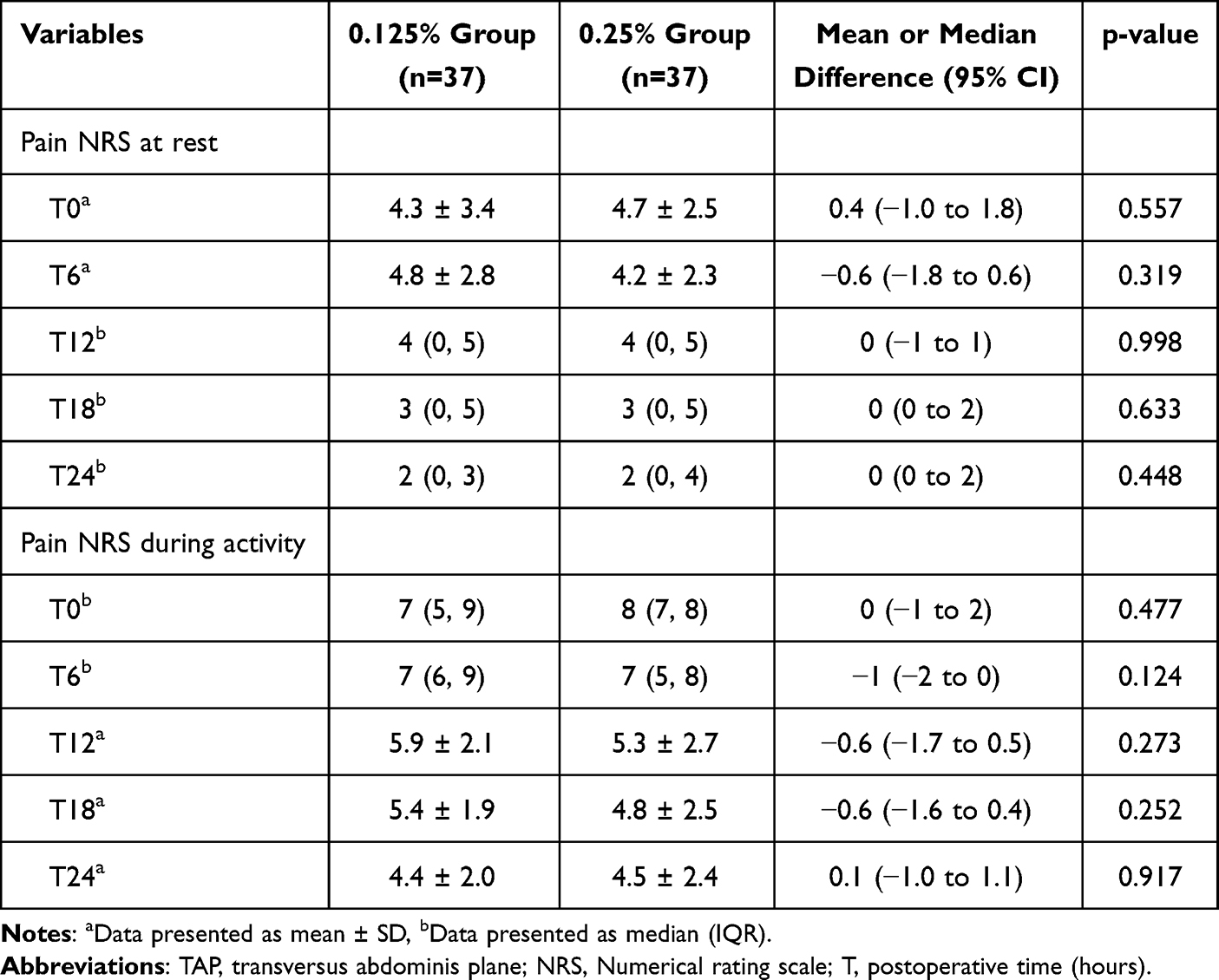 |
Table 3 Comparison of Postoperative Pain Score (NRS 0-10) at Rest and During Activity Between 0.125% and 0.25% Bupivacaine Groups for TAP Block in Kidney Transplant Recipients |
Incidence of adverse events is shown in Table 4. No complications related to the TAP block—such as hematoma, LAST, or intraperitoneal injection—were observed in either group. Among opioid-related complications, the most common was PONV, which occurred in 7 patients (9.5%): 4 in the 0.25% group and 3 in the 0.125% group, with no significant difference. One patient in the 0.25% group experienced drowsiness. Regarding patient satisfaction, most participants (75%) strongly agreed with the postoperative pain control method, and mean satisfaction scores were high in both groups.
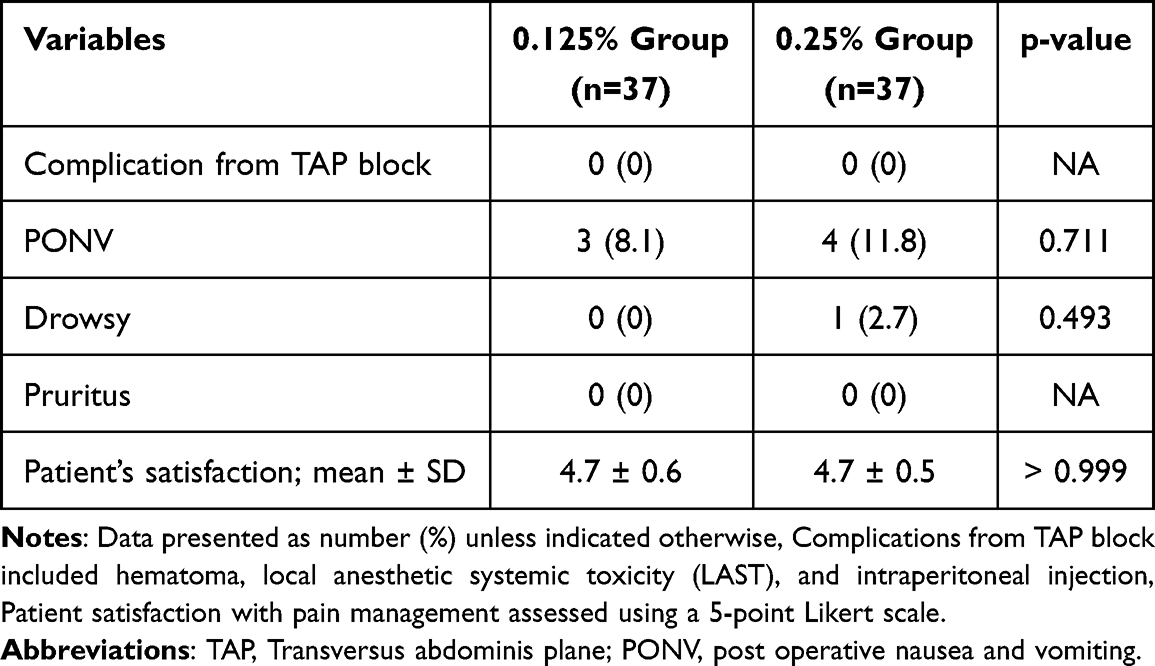 |
Table 4 Incidence of Adverse Events and Patient Satisfaction with Pain Management Within 24 hours Between 0.125% and 0.25% Bupivacaine Groups for TAP Block in Kidney Transplant Recipients |
Discussion
This randomized controlled trial evaluated the efficacy and safety of two bupivacaine concentrations (0.125% vs 0.25%) for ultrasound-guided TAP block in KT recipients. The 0.25% concentration, more commonly used, has been shown in several studies to significantly reduce opioid consumption and postoperative pain compared to placebo in this population.20–22 Our findings demonstrate that TAP block with 0.125% bupivacaine offers a comparable level of postoperative opioid sparing and pain control to 0.25%. This is consistent with previous reports, such as Erdoğan Arı et al18 who found no significant difference in opioid use or pain scores between 0.125% and 0.25% bupivacaine for TAP block in inguinal hernia surgery. Similarly, Prabhu et al17 reported comparable analgesic efficacy between these concentrations in unilateral inguinal hernia repair.
Additional supportive evidence comes from a recent pediatric trial that compared these two concentrations of bupivacaine in children undergoing unilateral inguinal hernia repair, demonstrating that both concentrations provided equally effective postoperative pain control.23 Moreover, a recent meta-analysis supports the use of low-dose TAP blocks for cesarean section, indicating that lower concentrations of local anesthetic can provide analgesia and opioid-sparing effects comparable to higher-dose regimens.24
Patients in the 0.25% bupivacaine group required significantly less intraoperative fentanyl and had a longer median time to first postoperative analgesic request. The reduced intraoperative fentanyl use in this group may reflect a faster onset or denser neural blockade achieved with the higher local anesthetic concentration.25 In contrast, the 0.125% concentration may have produced a less dense block, resulting in more frequent breakthrough pain early in the postoperative period and prompting earlier requests for rescue analgesia.26 Although the difference in median time to first analgesic request between groups was statistically significant (10 minutes vs 15 minutes; P = 0.020), this 5-minute gap is unlikely to be clinically meaningful. To our knowledge, no formal minimal clinically important difference (MCID) has been defined for time to first rescue analgesia after regional anesthesia. However, previous TAP block studies in lower abdominal or hernia surgery have reported between‑group differences in the range of tens of minutes to several hours (eg, Erdoğan Arı et al18 reported a time to first morphine request of 182 minutes in the 0.25% group and 143 minutes in the 0.125% group), which are substantially larger than the difference observed here. In addition, our IV PCA regimen used a 5‑minute lockout interval, and all patients had immediate access to rescue analgesia. Under these conditions, a 5‑minute difference is unlikely to alter the quality of postoperative pain control or overall recovery. Therefore, while statistically detectable, the longer time to first analgesic request in the 0.25% group should be interpreted as a small effect of limited clinical relevance.
The observed NRS scores indicated moderate pain at rest and moderate-to-severe pain during activity early postoperatively (T0 and T6). This pattern reflects inherent limitations, including the somatic focus of the single-shot unilateral TAP block which poorly addresses visceral pain from graft manipulation or peritoneal irritation. Furthermore, given the patients’ severe renal impairment, the fentanyl PCA regimen was conservatively dosed to prioritize safety over aggressive analgesia, and NSAIDs were contraindicated. Despite these factors, pain scores progressively improved over 24 hours, and high mean patient satisfaction scores (4.7/5 in both groups) suggest an acceptable balance between analgesia and safety was achieved. This reinforces that TAP block functions as one component of multimodal management, rather than a complete solution for all pain sources in this high-risk cohort.
No significant differences in pain scores were observed at any postoperative time point, either at rest or during activity. This similarity may be due to patients’ ability to self-administer opioids via IV-PCA until adequate pain relief was achieved.27 Despite this, the total opioid consumption was comparable between groups.
Although the 0.25% bupivacaine group showed an early analgesic advantage, it did not lead to reduced overall opioid use or improved pain scores during the first 24 hours postoperatively. This suggests that the effectiveness of the TAP block may depend more on the volume of injectate and accurate anatomical placement than on anesthetic concentration.28 Regarding safety, no TAP block–related complications—such as hematoma, LAST, or intraperitoneal injection—were observed in either group.
The use of ultrasound guidance, the addition of adrenaline, and the posterior approach for the TAP block likely enhanced the block’s efficacy and minimized complications in this study. Previous research has shown that ultrasound guidance improves both the effectiveness and safety of nerve blocks and allows for a lower minimum effective volume of local anesthetic.29 A prior study using the landmark technique for TAP block in KT patients found no reduction in postoperative morphine requirements and suggested that ultrasound guidance could improve block success.30 The addition of epinephrine to bupivacaine can prolong block duration by slowing systemic absorption.31 We also employed the posterior approach, which has been associated with reduced postoperative opioid use and longer analgesia duration compared to the lateral approach.32 Additionally, all TAP blocks were performed by experienced anesthesiologists, which likely contributed to the consistent success of the procedure. This contrasts with earlier studies that did not control for operator experience and found no significant improvement in block efficacy over controls.33
The incidence of opioid-related adverse events was low and comparable between groups. Patient satisfaction was also high in both groups, supporting the clinical acceptability of 0.125% bupivacaine.
Our findings indicate that both concentrations provide effective analgesia, reinforcing the use of lower bupivacaine concentrations to reduce the risk of LAST while maintaining adequate pain control. This study builds on previous meta-analytic evidence,9,12 confirming that a 0.125% bupivacaine TAP block is as safe and effective as the standard 0.25% in reducing perioperative opioid use. These results align with ERAS recommendations, which emphasize optimizing both safety and efficacy—especially in KT patients who are at increased risk for analgesic-related complications.2,4
This study’s strengths include its randomized, double-blind design, use of standardized protocols, and comprehensive evaluation of both efficacy and safety. Our findings help address existing evidence gaps by supporting the use of low-dose local anesthetic regimens for TAP block in KT surgery.
However, several limitations should be considered. First, plasma bupivacaine levels were not measured. Given that our patient population had impaired renal function, evaluating systemic bupivacaine exposure would have provided important safety data. Without these measurements, our conclusions about toxicity are inferred rather than confirmed. Second, because TAP blocks were performed under general anesthesia, we did not perform systematic postoperative sensory mapping to document dermatomal coverage, and silent block failures cannot be completely excluded. Third, the trial was powered only for the primary outcome; secondary endpoints were exploratory and may have been underpowered. Accordingly, nonsignificant findings for these outcomes should be interpreted with caution. In addition, the follow-up period was limited to 24 hours, preventing evaluation of long-term outcomes such as persistent postoperative pain or delayed complications. Lastly, these results may not be generalizable to techniques involving continuous TAP block or the use of adjuvant medications. Future studies should include plasma local anesthetic monitoring and longer follow-up to assess long-term efficacy and safety, which are especially important in KT patients due to their heightened risk of analgesic-related complications and chronic pain.
Conclusion
Ultrasound-guided TAP block using 0.125% bupivacaine provides comparable postoperative opioid consumption, analgesic efficacy, and patient satisfaction to the standard 0.25% concentration in KT recipients, without an increase in adverse events. Although the 0.25% group demonstrated a statistically longer time to first rescue analgesia, the 5-minutes difference is unlikely to be clinically relevant in the context of immediate IV PCA availability. These findings support the use of the lower bupivacaine concentration for single-shot unilateral TAP blocks in KT recipients.
Data Sharing Statement
The datasets generated and/or analyzed during the current study are available from the corresponding author upon reasonable request.
Consent for Publication
No published individual participant data were reported that would require consent from the participants.
Acknowledgments
The authors gratefully acknowledge Dr. Dylan Southard for his professional assistance in editing the manuscript through the Khon Kaen University Publication Clinic, Thailand. We also wish to thank Ms. Piyanan Suparattanagool, statistician at the Clinical Epidemiology Unit, Faculty of Medicine, Khon Kaen University, for her support with data analysis.
Funding
This work was financially supported by the Faculty of Medicine, Khon Kaen University, Thailand (Grant number IN67056). The authors also acknowledge the Thai Transplantation Society for partial support of the publication fees.
Disclosure
The authors declare that they have no conflicts of interest relevant to this work.
References
1. Kim H, Jung H. Considerations regarding anesthesia for renal transplantation. Anesth Pain Med. 2024;19(1):5–11. doi:10.17085/apm.23153
2. Elsabbagh AM, Ghoneim I, Moiz A, Welch K, Brown JS. Enhanced recovery after surgery pathway in kidney transplantation: the road less traveled. Transplant Direct. 2022;8:e1333.
3. Zhu Q, Yang J, Zhang Y, Ni X, Wang P. Early mobilization intervention for patient rehabilitation after renal transplantation. Am J Transl Res. 2021;13(6):7300–7305.
4. Jaszczuk S, Natarajan S, Papalois V. Anaesthetic approach to enhanced recovery after surgery for kidney transplantation: a narrative review. J Clin Med. 2022;11(12):3435. doi:10.3390/jcm11123435
5. Pham PC, Khaing K, Sievers TM, et al. 2017 update on pain management in patients with chronic kidney disease. Clin Kidney J. 2017;10(5):688–697. doi:10.1093/ckj/sfx080
6. Sridharan K, Shah S. Use of non-steroidal anti-inflammatory drugs in renal transplant patients: a retrospective study. Int J Risk Saf Med. 2023;34(4):379–386. doi:10.3233/JRS-220065
7. Jeong R, Lentine KL, Quinn RR, et al. NSAID prescriptions in kidney transplant recipients. Clin Transplant. 2021;35:e14405.
8. Williams M, Milner QJW. Postoperative analgesia following renal transplantation—current practice in the UK. Anaesthesia. 2003;58(7):712–713. doi:10.1046/j.1365-2044.2003.32661.x
9. Singh P, Borle A, Makkar J, Trisha A, Sinha A. Evaluation of transversus abdominis plane block for renal transplant recipients—a meta-analysis and trial sequential analysis of published studies. Saudi J Anaesth. 2018;12(2):261–266. doi:10.4103/sja.SJA_598_17
10. Tsai HC, Yoshida T, Chuang TY, et al. Transversus abdominis plane block: an updated review of anatomy and techniques. Biomed Res Int. 2017;2017:8284363. doi:10.1155/2017/8284363
11. Ojha H, Bhukal I, Jayant A, Singh S, Mulla R, Padhi PP. Comparison of analgesic efficacy of continuous transversus abdominis plane (TAP) block with continuous epidural analgesia in renal transplant recipients. Saudi J Anaesth. 2025;19(1):45–51. doi:10.4103/sja.sja_444_24
12. Viderman D, Aubakirova M, Nabidollayeva F, et al. The effect of transversus abdominis plane block on pain-related outcomes in kidney transplantation: a systematic review with meta-analysis and trial sequential analysis. J Clin Med. 2025;14(6):1879. doi:10.3390/jcm14061879
13. Talebi G, Moayeri H, Rahmani K, Nasseri K. Comparison of three different doses of dexmedetomidine added to bupivacaine in ultrasound-guided transversus abdominis plane block: a randomized clinical trial. Anesth Pain Med. 2021;11:e113778.
14. Warner M, Yeap YL, Rigueiro G, Zhang P, Kasper K. Erector spinae plane block versus transversus abdominis plane block in laparoscopic hysterectomy. Pain Manag. 2022;12(8):907–916. doi:10.2217/pmt-2022-0037
15. Neethirajan SGR, Kurada S, Parameswari A. Efficacy of dexmedetomidine as an adjuvant to bupivacaine in ultrasound-guided transverse abdominis plane block for laparoscopic appendicectomy: a randomised controlled study. Turk J Anaesthesiol Reanim. 2020;48(5):364–370. doi:10.5152/TJAR.2019.67689
16. Iyer S, Bavishi H, Mohan C, Kaur N. Comparison of epidural analgesia with transversus abdominis plane analgesia for postoperative pain relief in patients undergoing lower abdominal surgery: a prospective randomized study. Anesth Essays Res. 2017;11(3):670–674. doi:10.4103/0259-1162.206856
17. Prabhu R, Singh D, Krishnaveni N. A comparative study of postoperative analgesia provided by ultrasound-guided transversus abdominis plane block using two concentrations of bupivacaine in patients undergoing inguinal hernia repair. Anesth Essays Res. 2017;11(4):934–939. doi:10.4103/aer.AER_84_17
18. Erdoğan Arı D, Yıldırım Ar A, Karadoğan F, et al. Ultrasound-guided transversus abdominis plane block in patients undergoing open inguinal hernia repair: 0.125% bupivacaine provides similar analgesic effect compared to 0.25% bupivacaine. J Clin Anesth. 2016;28:41–46. doi:10.1016/j.jclinane.2015.07.020
19. Macfarlane AJR, Gitman M, Bornstein KJ, El-Boghdadly K, Weinberg G. Updates in our understanding of local anaesthetic systemic toxicity: a narrative review. Anaesthesia. 2021;76(S1):27–39. doi:10.1111/anae.15282
20. Ibrahim TH, Abdellatif MK, Osama FM. Efficacy of the transversus abdominis plane block using 30 mL bupivacaine 0.25% in reducing postoperative fentanyl requirements in renal transplant recipients. Ain Shams J Anaesthesiol. 2017;10:258–263.
21. Parikh B, Waghmare V, Shah V, et al. The analgesic efficacy of continuous transversus abdominis plane block in renal transplant recipients. J Anaesthesiol Clin Pharmacol. 2015;31(4):531–535. doi:10.4103/0970-9185.169084
22. Soltani Mohammadi S, Dabir A, Shoeibi G. Efficacy of transversus abdominis plane block for acute postoperative pain relief in kidney recipients: a double-blinded clinical trial. Pain Med. 2014;15(3):460–464. doi:10.1111/pme.12311
23. Karadeniz MS, Atasever AG, Salviz EA, et al. Transversus abdominis plane block with different bupivacaine concentrations in children undergoing unilateral inguinal hernia repair: a single-blind randomized clinical trial. BMC Anesthesiol. 2022;22(1):355. doi:10.1186/s12871-022-01907-y
24. Ng SC, Habib AS, Sodha S, Carvalho B, Sultan P. High-dose versus low-dose local anaesthetic for transversus abdominis plane block post-Caesarean delivery analgesia: a meta-analysis. Br J Anaesth. 2018;120(2):252–263. doi:10.1016/j.bja.2017.11.084
25. Kim HJ, Lee S, Chin KJ, et al. Comparison of the onset time between 0.375% ropivacaine and 0.25% levobupivacaine for ultrasound-guided infraclavicular brachial plexus block: a randomized-controlled trial. Sci Rep. 2021;11:4416. doi:10.1038/s41598-021-83679-y
26. Sakura S, Sumi M, Kushizaki H, Saito Y, Kosaka Y. Concentration of lidocaine affects intensity of sensory block during lumbar epidural anesthesia. Anesth Analg. 1999;88(1):123–127. doi:10.1213/00000539-199901000-00023
27. Ratanasuwan P, Nonphiaraj S, Pongjanyakul S, et al. Efficacy of a combination of ketamine and morphine for intravenous patient controlled-analgesia in upper abdominal surgery: a prospective, double-blind, randomized controlled trial. J Med Assoc Thai. 2021;104:1528–1534.
28. Tammam TF. Transversus abdominis plane block: the analgesic efficacy of a new block catheter insertion method. Egypt J Anaesth. 2014;30(1):39–45. doi:10.1016/j.egja.2013.07.008
29. McNaught A, Shastri U, Carmichael N, et al. Ultrasound reduces the minimum effective local anaesthetic volume compared with peripheral nerve stimulation for interscalene block. Br J Anaesth. 2011;106(1):124–130. doi:10.1093/bja/aeq306
30. Freir NM, Murphy C, Mugawar M, Linnane A, Cunningham AJ. Transversus abdominis plane block for analgesia in renal transplantation: a randomized controlled trial. Anesth Analg. 2012;115(4):953–957. doi:10.1213/ANE.0b013e3182642117
31. Rozier R, Le Guennec Y, Capdevila X, et al. Impact of epinephrine on ropivacaine pharmacokinetics in TAP blocks: a randomized controlled trial. Reg Anesth Pain Med. 2025:rapm–2025–106500. doi:10.1136/rapm-2025-106500
32. Abdallah FW, Laffey JG, Halpern SH, Brull R. Duration of analgesic effectiveness after the posterior and lateral transversus abdominis plane block techniques for transverse lower abdominal incisions: a meta-analysis. Br J Anaesth. 2013;111(5):721–735. doi:10.1093/bja/aet214
33. Gharaei H, Imani F, Almasi F, Solimani M. The effect of ultrasound-guided TAPB on pain management after total abdominal hysterectomy. Korean J Pain. 2013;26(4):374–378. doi:10.3344/kjp.2013.26.4.374
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Real-World Pharmacovigilance Analysis of Adverse Events Associated with Liposomal Bupivacaine and Bupivacaine

Chen DX, Chen XM, Chen SM, Wang YD
Journal of Pain Research 2025, 18:1805-1816
Published Date: 3 April 2025