Back to Journals » International Journal of General Medicine » Volume 19
Ultrasound-Guided Small-Caliber Catheter Drainage for Complex Septated Pleural Effusions: Discrimination of Septal Characteristics for Outcomes
Received 9 October 2025
Accepted for publication 20 January 2026
Published 24 January 2026 Volume 2026:19 571764
DOI https://doi.org/10.2147/IJGM.S571764
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Reynold Panettieri Jr
Wenqiang Lin,1 Peifen Chen2
1Department of Ultrasound, The First Affiliated Hospital of Shantou University Medical College, Shantou, Guangdong Province, People’s Republic of China; 2Department of Radiology, The First Affiliated Hospital of Shantou University Medical College, Shantou, Guangdong Province, People’s Republic of China
Correspondence: Peifen Chen, Department of Radiology, The First Affiliated Hospital of Shantou University Medical College, 57 Changping Road, Shantou, Guangdong Province, 515041, People’s Republic of China, Tel +8613822869774, Email [email protected]
Purpose: The objective of this study was to identify the sonographic and clinical predictors of drainage procedure failure using small-caliber catheters under ultrasound guidance for complex septated pleural effusions.
Materials and Methods: In this retrospective cohort study, we analyzed 145 consecutive patients who underwent ultrasound-guided small-caliber (6- or 8-Fr) catheter drainage for complex septated pleural effusion at a single tertiary center. Demographic, clinical, and pleural fluid data were collected. Sonographic images were reviewed to classify septation complexity (widespread vs few) and to quantitatively measure septal thickness. Multivariable logistic regression was used to identify independent predictors of drainage failure.
Results: Unsuccessful drainage occurred in 79 patients (54.5%). Widespread septations (72.2% vs 36.4%, P< 0.001) and greater septal thickness (3.3 vs 2.1 mm, P< 0.001) were more common in the unsuccessful group. Multivariable analysis identified widespread septations (adjusted odds ratio [aOR]=2.94, P=0.033) and septal thickness (aOR=3.39 per mm, P< 0.001) as independent predictors of failure. The optimal cut-off for septal thickness was > 2.4 mm (sensitivity 82.3%, specificity 69.7%). An alternative cut-off of > 1.8 mm provided high sensitivity (93.7%) and a negative likelihood ratio (LR−) of 0.1 for ruling out failure.
Conclusion: Quantitative sonographic assessment of septation complexity and thickness independently predicts small-caliber catheter drainage failure in complex septated pleural effusions. Incorporating these parameters into pre-procedural evaluation can aid in risk stratification and guide individualized management, potentially facilitating timely escalation to advanced therapies when indicated.
Keywords: pleural effusion, septation, ultrasonography, drainage, catheterization
Introduction
The accumulation of pleural effusion is a frequent clinical manifestation of various underlying pathologies, capable of severely compromising respiratory function by impairing ventilation and gas exchange.1–3 Prompt and effective drainage is essential in cases requiring intervention, including those with significant respiratory compromise, a need for diagnostic sampling, or complications from infection or malignancy. Timely drainage relieves respiratory distress, improves pulmonary mechanics, and decreases the need for invasive surgery.4
Over the past decades, the therapeutic paradigm has shifted decisively from traditional open drainage using large-bore catheters to minimally invasive techniques employing small-caliber drains.5–7 This evolution is driven by the clear benefits of smaller catheters, including enhanced patient tolerance, reduced procedural pain, and superior cosmetic outcomes.8 The concurrent integration of bedside ultrasound has further refined this approach, providing real-time guidance that improves targeting accuracy, significantly lowers the risk of iatrogenic complications such as pneumothorax, and facilitates rapid intervention in critically ill or non-ambulatory patients.9–11
Notwithstanding these significant procedural advancements, the management of complex septated pleural effusions continues to pose a considerable clinical challenge. Pathophysiologically, these pleural effusions are characterized by the intrapleural deposition of fibrin and cellular debris, which subsequently organizes into septa and result in the formation of multiple, isolated fluid loculations.12 The process of compartmentalization has the potential to impede the flow of fluid, thus rendering the efficacy of single-catheter drainage ineffective. Consequently, a pertinent clinical controversy exists regarding the utility of small-caliber catheters for these complex effusions, with concerns that their narrow lumens are susceptible to occlusion by viscous fluid or fibrinous material, leading to premature drainage failure.13 Despite the postulation of an association between the sonographic presence of septations and adverse drainage outcomes, this relationship remains unproven. Furthermore, the specific risk factors predictive of catheter occlusion are not well-established.14
Current clinical guidelines for the management of complex loculated pleural effusions advocate for early escalation to intrapleural fibrinolytic therapy or surgical intervention if initial drainage fails.5,15 However, the decision to progress to these more invasive strategies is frequently made retrospectively, following the failure of a standard drainage attempt. Pre-procedural sonographic markers that could reliably predict drainage outcomes remain poorly defined, leading to potential delays in optimal therapy.
Therefore, a more profound comprehension of sonographic predictors is essential to refine patient selection, guide initial procedural planning, and facilitate timely escalation of care when indicated. The primary objective of this retrospective study was to identify specific ultrasound-derived and clinical variables associated with failure of ultrasound-guided small-caliber catheter drainage in patients with complex septated pleural effusions.
Materials and Methods
Study Design and Patient Selection
This retrospective cohort study was conducted at a single tertiary university hospital. Electronic medical records of consecutive patients who underwent ultrasound-guided small-caliber catheter drainage for complex septated pleural effusion between January 2022 and June 2024 were reviewed. A total of 185 patients were initially identified.
Eligibility was determined by a thoracic ultrasound–confirmed diagnosis of complex septated pleural effusion. Exclusion criteria included: (1) insufficient data to ascertain the definitive outcome of the drainage procedure, such as patients discharged with the catheter in situ, transferred to another facility, or who died from causes unrelated to pleural effusion before outcome assessment; and (2) absence of pleural fluid biochemical analysis in the medical records, which precluded comprehensive characterization of the effusion.
The patient selection process is illustrated in Figure 1. The Institutional Review Board at the First Affiliated Hospital of Shantou University Medical College provided review and approval for the study’s protocol (Approval No. B-2024-169). Patient consent was waived by the ethics committee, as the study utilized anonymized ultrasound data and biological samples obtained from prior routine clinical examinations. All procedures were conducted in accordance with the ethical guidelines established by the Declaration of Helsinki. Patient data were anonymized prior to analysis in accordance with the protocol to ensure confidentiality.
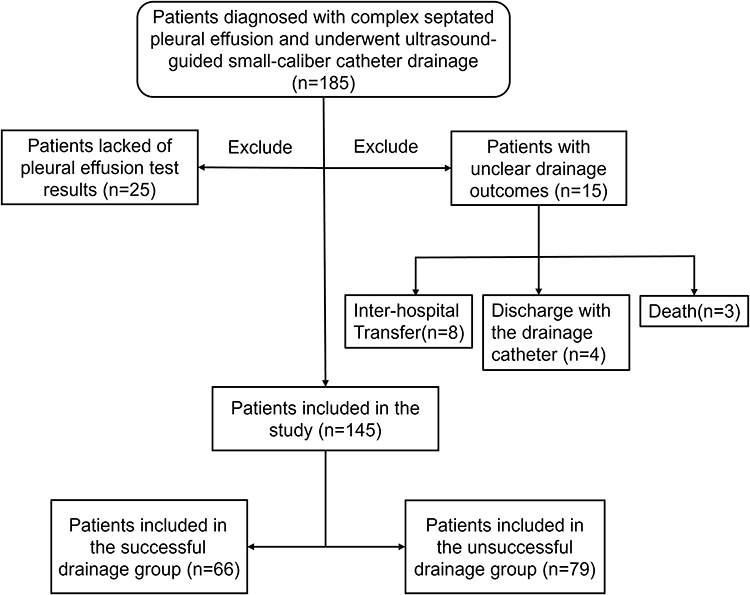 |
Figure 1 Flowchart of the study. Patients diagnosed with complex septated pleural effusion and underwent ultrasound-guided small-caliber catheter drainage were identified. Inclusion and exclusion criteria are applied to reach the final analytic cohort, which is then divided by drainage outcome (successful vs unsuccessful). |
Ultrasonic Examination and Drainage Procedure
The decision to perform diagnostic and therapeutic drainage was made by the managing physician based on clinical indications, including significant respiratory compromise, the need for diagnostic sampling, or suspicion of infected or complicated pleural effusion. All drainage procedures were performed by an interventional radiologist with at least 5 years of clinical experience.
Prior to the procedure, thoracic ultrasound was performed using an EPIQ 7 ultrasound system (Philips Medical Systems, Bothell, WA, USA) equipped with a C5-1 convex-array transducer (1–5 MHz) to evaluate effusion complexity, septation characteristics, and to determine the optimal puncture site. With the patient in a seated position, a 6- or 8-French multi–side-hole catheter was inserted under real-time ultrasound guidance using the Seldinger technique and connected to a closed drainage system.
Following the procedure, catheter management adhered to standard ward protocols, including flushing with 10 mL of normal saline every 24 hours to maintain catheter patency. Catheters were removed once the criteria for successful drainage were met or in cases of persistent catheter occlusion.
Successful drainage was defined by fulfillment of all post-procedural criteria: (1) complete resolution of the effusion using a single catheter; (2) drainage volume <50 mL over 24 hours; and (3) residual pleural fluid thickness <20 mm on follow-up ultrasound. Failure to meet any of these criteria was classified as unsuccessful drainage.
Data Collection and Image Analysis
Demographic, clinical, and laboratory data were extracted from electronic medical records. Pleural effusions were classified as exudative or transudative according to Light’s criteria. Etiology was independently adjudicated by two physicians based on clinical, microbiological, and pathological data.
All baseline ultrasound images were analyzed by a physician with more than 5 years of experience who was blinded to clinical outcomes. Septation complexity was categorized as either few septations (countable septa with simple loculations) or widespread septations (uncountable, mesh-like septa) (Figure 2).
 |
Figure 2 Representative ultrasound images and septal measurements. (A) Ultrasound imaging of a 69-year-old female with pneumonia and pleural effusion, showing a small number of septations (fewer-septation pattern). A 6-Fr catheter was placed, yielding successful drainage. (B) ImageJ measurement of the thickest septum in (A) (2.33 mm) using the local magnification. (C) Ultrasound imaging of a 66-year-old male with tuberculous pleurisy, showing extensive, fine fibrin septa (widespread-septation pattern). An 8-Fr catheter was placed, resulting in unsuccessful drainage. (D) ImageJ measurement of the thickest septum in (C) (3.43 mm) using the local magnification. The yellow line indicates the measured thickness of the septum. |
Quantitative assessment of septal thickness was performed using ImageJ software (version 1.54f; National Institutes of Health, Bethesda, MD, USA). The thickest septum within the most highly septated region was measured five times under magnification, and the mean value (mm) was recorded. Interobserver agreement was assessed in 30 randomly selected images analyzed by two blinded physicians. The intraclass correlation coefficient for septal thickness was 0.92 (95% CI, 0.84–0.96).
Statistical Analysis
Statistical analyses were performed using SPSS Statistics software (version 22.0; IBM Corp., Armonk, NY, USA). The Shapiro–Wilk test was used to assess the normality of continuous variables. Normally distributed data are presented as the mean ± standard deviation (SD) and were compared using the independent Student’s t test, whereas non-normally distributed data are expressed as the median with interquartile range (IQR) and were analyzed using the Mann–Whitney U-test. Categorical variables are summarized as counts and percentages and were compared using the chi-square test or Fisher’s exact test, as appropriate.
Univariable logistic regression analyses were conducted to evaluate associations with drainage failure. Variables with a P value < 0.20 in univariable analyses were entered into a stepwise forward multivariable logistic regression model to identify independent predictors. Results are reported as odds ratios (ORs) or adjusted odds ratios (aORs) with 95% confidence intervals (CIs). The optimal cutoff value for septal thickness was determined using receiver operating characteristic (ROC) curve analysis by maximizing the Youden index. A two-tailed P value < 0.05 was considered statistically significant.
Results
A total of 145 patients met inclusion criteria and were analyzed, stratified into successful (n = 66, 45.5%) and unsuccessful drainage groups (n = 79, 54.5%) (Figure 1). Baseline age, sex, and smoking history were comparable between groups (Table 1). Parapneumonic effusion (48.3%) and empyema (18.6%) were the most common etiologies, and 92.4% of effusions were exudative, with no between-group differences.
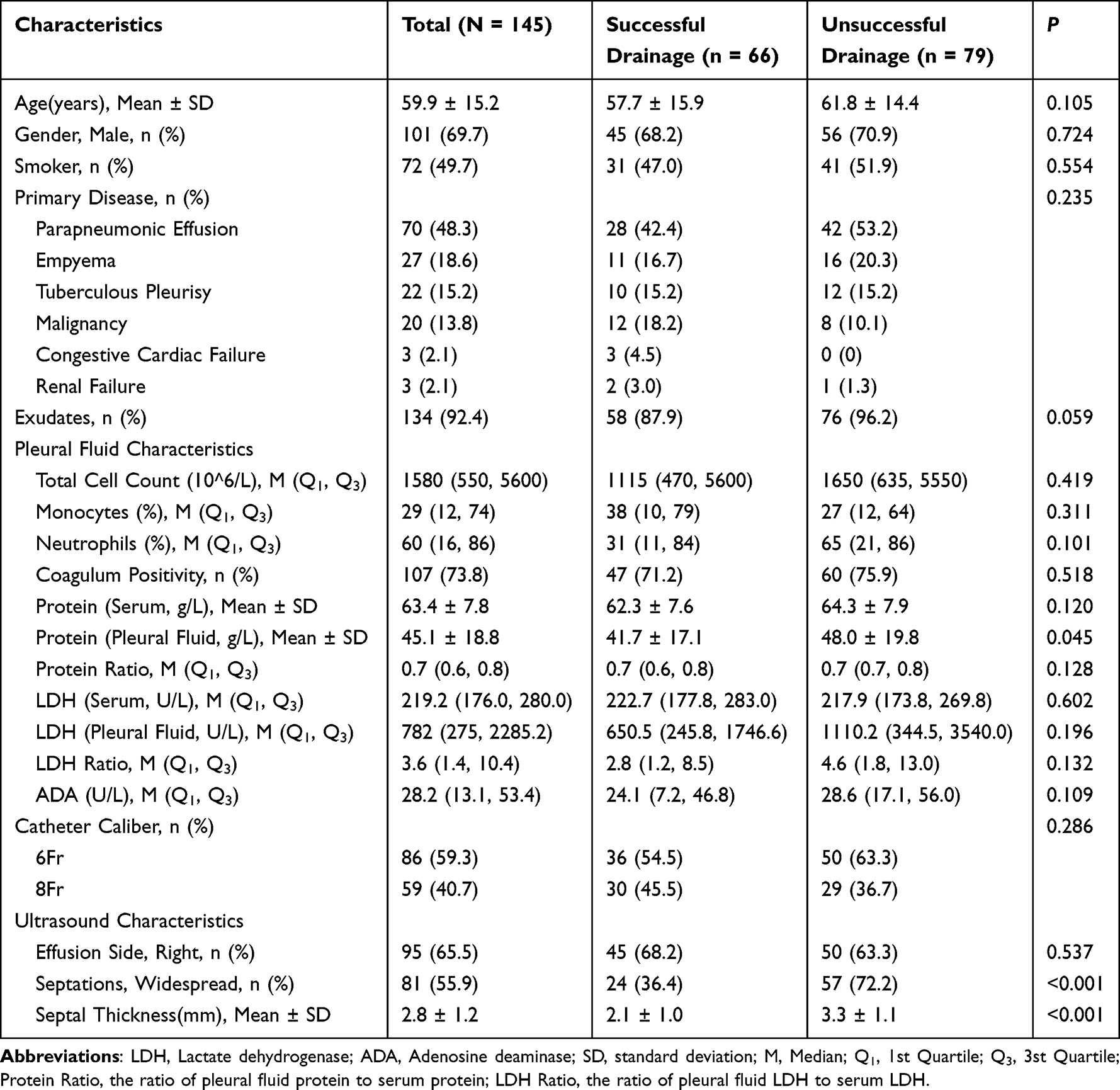 |
Table 1 Baseline Characteristics of 145 Patients with Complex Septated Pleural Effusions |
Pleural fluid biochemical analysis revealed a statistically significant difference in total protein concentration, which was higher in the unsuccessful drainage group than in the successful group (48.0 ± 19.8 g/L vs 41.7 ± 17.1 g/L, P = 0.045). In contrast, no significant between-group differences were observed in the pleural fluid–to–serum protein ratio (P = 0.128), pleural fluid lactate dehydrogenase (LDH) levels (P = 0.196), or the LDH ratio (P = 0.132) (Table 1).
Markers of inflammation and cellularity, including total cell count (P = 0.419), neutrophil percentage (P = 0.101), monocyte percentage (P = 0.311), and adenosine deaminase (ADA) levels (P = 0.109), were comparable between the two groups. Notably, coagulum positivity, a macroscopic indicator of coagulation factor activity, was observed in 73.8% of the overall cohort but did not differ significantly between the successful and unsuccessful drainage groups (71.2% vs 75.9%, P = 0.518). With respect to procedural variables, neither catheter caliber (6 Fr vs 8 Fr, P = 0.286) nor effusion laterality (P = 0.537) was significantly associated with drainage success (Table 1).
Ultrasound evaluation demonstrated marked morphological differences between groups. Patients with unsuccessful drainage had a significantly higher prevalence of widespread septations than those with successful drainage (72.2% vs 36.4%, P < 0.001). Moreover, quantitative analysis revealed that mean septal thickness was significantly greater in the unsuccessful drainage group (3.3 ± 1.1 mm) compared with the successful group (2.1 ± 1.0 mm, P < 0.001) (Table 1).
In univariable logistic regression analysis, widespread septations (odds ratio [OR] = 4.53, 95% confidence interval [CI], 2.25–9.15; P < 0.001) and increased septal thickness (OR = 3.11 per mm, 95% CI, 2.06–4.70; P < 0.001) were significantly associated with unsuccessful drainage, whereas pleural fluid protein level showed a borderline association (OR = 1.02 per g/L, 95% CI, 1.00–1.05; P = 0.053) (Table 2).
 |
Table 2 Results of Univariable and Multivariable Logistic Regression |
Variables with P < 0.20 were entered into a forward stepwise multivariable logistic regression model. Widespread septations (adjusted OR [aOR], 2.94; 95% CI, 1.09–7.94; P = 0.033) and septal thickness (aOR, 3.39 per mm; 95% CI, 2.10–5.47; P < 0.001) remained independently associated with drainage failure. Age was retained in the model (aOR, 1.03; 95% CI, 1.01–1.07; P = 0.031) but demonstrated a small effect size. Pleural fluid protein level and other clinical or biochemical variables were not independently associated with outcome (all P > 0.05) (Table 2).
Receiver operating characteristic (ROC) curve analysis demonstrated good discriminatory performance of septal thickness for predicting drainage failure, with an area under the curve (AUC) of 0.81. The optimal cutoff value was >2.4 mm, yielding a sensitivity of 82.3% and a specificity of 69.7% (Figure 3). To support clinical risk stratification, alternative cutoff values were evaluated (Table 3). A threshold of >1.8 mm achieved high sensitivity (93.7%) with a negative likelihood ratio (LR−) of 0.10, whereas the >2.4 mm cutoff provided a positive likelihood ratio (LR+) of 2.7.
 |
Table 3 Diagnostic Performance of Various Septal Thickness Cut-Offs for Predicting Small-Caliber Catheter Drainage Failure |
 |
Figure 3 ROC curve for septal thickness. The optimal cut-off of 2.4 mm (Youden index) is marked as a red dot, with the corresponding sensitivity and specificity values of 82.3% and 69.7%, respectively. Abbreviation: AUC, Area Under Curve. |
Discussion
In this investigation, it was found that both the complexity and thickness of intrapleural septations were potent, independent predictors of small-caliber catheter drainage failure in patients with complex septated pleural effusions. These findings contribute to the advancement of current understanding, which has been largely confined to differentiating outcomes between septated and non-septated effusions,14,16,17 by establishing a quantitative, dose-dependent relationship between the sonographic burden of septation and the likelihood of procedural failure. Furthermore, we identified septal thickness as a novel and quantifiable prognostic factor. Collectively, these findings indicate that a comprehensive ultrasonographic evaluation of septal morphology prior to intervention is imperative for risk stratification and therapeutic planning.
The observed association between an increasing septation grade and a higher failure rate is consistent with the established pathophysiology of pleural inflammation, which progresses through exudative, fibrinopurulent, and organizational stages.18 The formation and proliferation of septa signify a transition into the fibrinopurulent phase, a state characterized by upregulated pro-coagulant activity and attenuated local fibrinolysis due to reduced plasminogen activator levels.19 We postulate that a lower septation grade reflects an earlier point in this pathological continuum, where septa are fewer, more fragile, and communication between fluid locules is at least partially preserved. Consequently, mechanical forces from catheter manipulation, respiratory motion, or changes in patient positioning may be sufficient to disrupt these fibrinous bands, leading to cavity coalescence and improved drainage. Conversely, a high septation grade likely represents an advanced disease state characterized by extensive, organized fibrin deposition that creates multiple, discrete, and non-communicating microcompartments, thereby presenting an insurmountable physical barrier to effective fluid evacuation via a single catheter. Clinically, this implies that patients with widespread septations face a substantially higher risk of failure, a fact that necessitates candid pre-procedural counseling and proactive consideration of alternative management strategies, such as intrapleural enzyme therapy or surgical intervention.
Of note, to our knowledge, this is the first study to demonstrate that septal thickness is an independent predictor of drainage outcome; however, this novel finding should be interpreted with caution pending external validation. The underlying mechanism may be twofold. Firstly, thicker septa (>2.4 mm in our cohort) likely exert greater mechanical resistance against the pressure gradients generated by drainage and may also represent a more advanced state of fibrous organization with greater collagen deposition and fibroblast infiltration, making them less susceptible to spontaneous or mechanically induced rupture. This interpretation is supported by our observation that increasing drainage catheter diameter did not improve success rates, suggesting that the structural integrity of the septa, rather than the catheter orifice size, is the rate-limiting factor. Secondly, increased thickness may correlate with a more profound impairment of local fibrinolytic pathways, rendering the septa less susceptible to endogenous or exogenous enzymatic degradation. This finding strongly suggests that sonographic evaluation should extend beyond merely identifying the presence of septa to quantifying their thickness.
The evaluation of multiple diagnostic thresholds for septal thickness provides a nuanced framework for clinical decision-making. A cutoff of >1.8 mm demonstrated high sensitivity (93.7%) and a low negative likelihood ratio (LR− = 0.1), indicating that values below this threshold effectively rule out a high risk of drainage failure and support initial attempts with standard small-caliber catheter drainage. The >2.4 mm threshold, identified by the Youden index as optimal, offered balanced performance (sensitivity 82.3%, specificity 69.7%) and a positive likelihood ratio (LR+ = 2.7). Values above this threshold indicate a moderately increased risk of failure, warranting heightened clinical vigilance and preparedness for adjunctive interventions. Integrating these thresholds into pre-procedural assessment enables a stratified approach: patients with septal thickness <1.8 mm can undergo standard drainage (low risk), those with 1.8–2.4 mm require close monitoring and contingency planning (intermediate risk), and patients with >2.4 mm may be considered for upfront advanced interventions (elevated risk). Incorporating septal thickness into risk stratification refines prognostication, identifying patients unlikely to benefit from standard small-caliber drainage who may benefit from earlier escalation of care, including intrapleural fibrinolytic therapy.20,21
In contrast, our multivariable analysis confirmed that pleural fluid biochemical markers, specifically total protein and adenosine deaminase (ADA) levels, did not predict drainage success. This finding aligns with the understanding that these parameters reflect distinct pathophysiological pathways unrelated to the mechanical determinants of fluid removal. Total protein levels indicate the degree of vascular permeability,22 while ADA levels serve as a marker of lymphocyte activation,23 both of which are central to establishing an etiological diagnosis.2,24,25 Nevertheless, drainage efficacy is governed by the physical architecture of the pleural space. The presence of robust, organized fibrin septa creates an anatomical barrier that is indifferent to the underlying biochemical milieu of the fluid. Taken together, these results reinforce that while pleural fluid analysis remains indispensable for determining etiology, it holds little value in predicting the technical success of a drainage procedure. Instead, therapeutic decisions should be guided primarily by the morphological characteristics revealed by imaging.
While our study offers a more granular understanding of drainage failure predictors, several limitations warrant consideration. First, the single-center, retrospective design inherently risks selection bias and may limit the external validity of our findings to populations with different demographic or etiological profiles. Second, our relatively modest cohort size (n=137) precluded adequately powered subgroup analyses, particularly regarding different underlying etiologies, and likely contributed to the wide confidence intervals observed for some estimates. Third, although we used a standardized protocol for measuring septal thickness, the lack of a formal interobserver variability analysis means we cannot exclude the possibility of measurement bias. Future research should prioritize a large-scale, multicenter prospective study to validate our proposed predictors using a protocolized ultrasound assessment with blinded analysis. Such a study would also allow for stratification by etiology and could incorporate longer-term follow-up to assess outcomes like the development of fibrothorax. Therefore, our data suggest that a pre-procedural ultrasonographic assessment focused on quantifying both septation complexity and septal thickness is essential for stratifying patients with complex septated effusions and guiding decisions between standard drainage and more aggressive interventions.
Conclusions
In conclusion, this study establishes that the quantitative sonographic assessment of septal architecture is a critical determinant of drainage efficacy, providing an evidence-based framework to refine therapeutic strategies for patients with complex septated pleural effusions. These findings suggest that pre-procedural sonographic assessment of septal architecture can aid in risk stratification. However, these results should be considered preliminary and require validation in larger, prospective multicenter studies before being incorporated into routine clinical practice.
Acknowledgments
No financial support was provided for this study by public, commercial, or non-profit funding organizations. There are no conflicts of interest related to financial, material, or social relationships in this research. Furthermore, the authors have not revealed any connections that might be seen as impacting the research shared in this paper.
Disclosure
The authors disclose an absence of any personal conflicts or financial interests that could affect this study.
References
1. Ferreiro L, Toubes ME, San José ME, Suárez-Antelo J, Golpe A, Valdés L. Advances in pleural effusion diagnostics. Expert Rev Resp Med. 2020;14:51–10. doi:10.1080/17476348.2020.1684266
2. Valdés L, San José ME, Pose A, et al. Diagnosing tuberculous pleural effusion using clinical data and pleural fluid analysis A study of patients less than 40 years-old in an area with a high incidence of tuberculosis. Resp Med. 2010;104:1211–1217. doi:10.1016/j.rmed.2010.02.025
3. Zaki HA, Albaroudi B, Shaban EE, et al. Advancement in pleura effusion diagnosis: a systematic review and meta-analysis of point-of-care ultrasound versus radiographic thoracic imaging. Ultrasound J. 2024;16:3. doi:10.1186/s13089-023-00356-z
4. Chung C-L, Chen C-H, Yeh C-Y, Sheu J-R, Chang S-C. Early effective drainage in the treatment of loculated tuberculous pleurisy. Eur Respir J. 2008;31:1261–1267. doi:10.1183/09031936.00122207
5. Roberts ME, Rahman NM, Maskell NA, et al. British Thoracic Society Guideline for pleural disease. Thorax. 2023;78:1143–1156. doi:10.1136/thorax-2023-220304
6. Hooper C, Lee YCG, Maskell N; BTS Pleural Guideline Group. Investigation of a unilateral pleural effusion in adults: British thoracic society pleural disease guideline 2010. Thorax. 2010;65 Suppl 2:ii4–17. doi:10.1136/thx.2010.136978
7. Porcel JM. Chest tube drainage of the pleural space: a concise review for pulmonologists. Tuberc Respir Dis. 2018;81:106–115. doi:10.4046/trd.2017.0107
8. Cao G-Q, Li L, Wang Y-B, Shi -Z-Z, Fan D-Y, Chen H-Y. Treatment of free-flowing tuberculous pleurisy with intrapleural urokinase. Int J Tuberc Lung Dis. 2015;19:1395–1400. doi:10.5588/ijtld.15.0128
9. Havelock T, Teoh R, Laws D, Gleeson F; BTS Pleural Disease Guideline Group. Pleural procedures and thoracic ultrasound: British thoracic society pleural disease guideline 2010. Thorax. 2010;65 Suppl 2:ii61–76. doi:10.1136/thx.2010.137026
10. Romero Romero B, Vollmer Torrubiano I, Martín Juan J, et al. Ultrasound in the study of thoracic diseases: innovative aspects. Arch Bronconeumol. 2024;60:33–43. doi:10.1016/j.arbres.2023.10.009
11. Hansell L, Milross M, Delaney A, Tian DH, Ntoumenopoulos G. Lung ultrasound has greater accuracy than conventional respiratory assessment tools for the diagnosis of pleural effusion, lung consolidation and collapse: a systematic review. J Physiother. 2021;67:41–48. doi:10.1016/j.jphys.2020.12.002
12. Jing W, Weng R, Lin P, Luo M. Urokinase in the treatment of tuberculous pleurisy: a systematic review and meta-analysis. BMC Infect Dis. 2024;24:258. doi:10.1186/s12879-024-08975-0
13. Shen KR, Bribriesco A, Crabtree T, et al. The American Association for Thoracic Surgery consensus guidelines for the management of empyema. J Thorac Cardiovasc Surg. 2017;153:e129–e146. doi:10.1016/j.jtcvs.2017.01.030
14. Chen C-H, Chen W, Chen H-J, et al. Transthoracic ultrasonography in predicting the outcome of small-bore catheter drainage in empyemas or complicated parapneumonic effusions. Ultrasound Med Biol. 2009;35:1468–1474. doi:10.1016/j.ultrasmedbio.2009.04.021
15. Sedhai YR, Bhat P, Acharya R, et al. Intrapleural tissue plasminogen activator and deoxyribonuclease in complex pleural effusion and empyema, clinical outcomes, and predictors. Ther Adv Respir Dis. 2025;19:17534666251343711. doi:10.1177/17534666251343711
16. Shankar S, Gulati M, Kang M, Gupta S, Suri S. Image-guided percutaneous drainage of thoracic empyema: can sonography predict the outcome? Eur Radiol. 2000;10:495–499. doi:10.1007/s003300050083
17. Keeling AN, Leong S, Logan PM, Lee MJ. Empyema and effusion: outcome of image-guided small-bore catheter drainage. Cardiovasc Inter Rad. 2008;31:135–141.
18. Rahman NM, Chapman SJ, Davies RJO. The approach to the patient with a parapneumonic effusion. Clin Chest Med. 2006;27:253–266. doi:10.1016/j.ccm.2005.12.005
19. Tucker TA, Idell S. The contribution of the urokinase plasminogen activator and the urokinase receptor to pleural and parenchymal lung injury and repair: a narrative review. Int J Mol Sci. 2021;22(3):1437. doi:10.3390/ijms22031437
20. Botana Rial M, Pérez Pallarés J, Cases Viedma E, et al. Diagnosis and treatment of pleural effusion. recommendations of the spanish society of pulmonology and thoracic surgery. Update 2022. Arch Bronconeumol. 2023;59:27–35. doi:10.1016/j.arbres.2022.09.017
21. Taniguchi J, Matsui H, Nagai T, et al. Association between intrapleural urokinase monotherapy and treatment failure in patients with pleural infection: a retrospective cohort study. BMC Pulm Med. 2023;23:273. doi:10.1186/s12890-023-02559-5
22. Tyan Y-C, Wu H-Y, Su W-C, Chen P-W, Liao P-C. Proteomic analysis of human pleural effusion. Proteomics. 2005;5:1062–1074. doi:10.1002/pmic.200401041
23. Liang Q-L, Shi H-Z, Wang K, Qin S-M, Qin X-J. Diagnostic accuracy of adenosine deaminase in tuberculous pleurisy: a meta-analysis. Resp Med. 2008;102:744–754. doi:10.1016/j.rmed.2007.12.007
24. Shimoda M, Hirata A, Tanaka Y, et al. Characteristics of pleural effusion with a high adenosine deaminase level: a case-control study. BMC Pulm Med. 2022;22:359. doi:10.1186/s12890-022-02150-4
25. Rabbi MF, Ahmed MN, Patowary M, et al. Pleural fluid adenosine deaminase to serum C-reactive protein ratio for diagnosing tuberculous pleural effusion. Bmc Pulm Med. 2023;23:349. doi:10.1186/s12890-023-02644-9
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.