Back to Journals » ClinicoEconomics and Outcomes Research » Volume 13
Ultrasound-Guided Pudendal Nerve Block in Patients Undergoing Open Hemorrhoidectomy: A Post-Hoc Cost-Effectiveness Analysis from a Double-Blind Randomized Controlled Trial
Authors Mongelli F ![]() , Lucchelli M, La Regina D, Christoforidis D
, Lucchelli M, La Regina D, Christoforidis D ![]() , Saporito A, Vannelli A, Di Giuseppe M
, Saporito A, Vannelli A, Di Giuseppe M
Received 16 February 2021
Accepted for publication 19 April 2021
Published 28 April 2021 Volume 2021:13 Pages 299—306
DOI https://doi.org/10.2147/CEOR.S306138
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Xing Lin Feng
Francesco Mongelli,1 Massimo Lucchelli,2 Davide La Regina,3 Dimitri Christoforidis,1 Andrea Saporito,4 Alberto Vannelli,5 Matteo Di Giuseppe3
1Department of Surgery, Ospedale Regionale di Lugano, Lugano, Switzerland; 2Financial Department, Ospedale Regionale di Bellinzona e Valli, Bellinzona, Switzerland; 3Department of Surgery, Ospedale Regionale di Bellinzona e Valli, Bellinzona, Switzerland; 4Department of Anesthesia, Ospedale Regionale di Bellinzona e Valli, Bellinzona, Switzerland; 5Department of Surgery, Ospedale Valduce, Como, Italy
Correspondence: Francesco Mongelli
Ospedale Regionale di Lugano, via Tesserete 46, Lugano, 6900, Switzerland
Tel +41764706297
Fax +41918119066
Email [email protected]
Background: Pudendal nerve block (PNB) has been demonstrated to reduce postoperative pain and re-admission rates after open hemorrhoidectomy and may reduce costs but, to date, no study has reported data on this aspect. The aim of our study was to perform a cost analysis on PNB use in in- and outpatients undergoing open hemorrhoidectomy.
Methods: From January 2018 to December 2019, patients undergoing open hemorrhoidectomy were included and randomized to undergo spinal anesthesia either with or without the PNB. Clinical data, direct and indirect costs for in- and outpatients, operating time and operating theatre occupancy were recorded. A cost-effectiveness analysis based on the diagnosis-related groups (DRG) and TARMED reimbursement systems was performed.
Results: Patients who underwent PNB in addition to spinal anesthesia had significantly less pain and a shorter length of hospital stay after open hemorrhoidectomy. The cost analysis included all 49 patients, 23 of whom, in addition to spinal anesthesia, received a PNB. There were no significant differences in operating theatre occupancy (p=0.662), mean operative time (p=0.610) or time required for anesthesia (p=0.124). Direct costs were comparable (482± 386 vs 613± 543 EUR, p=0.108), while indirect costs were significantly lower in the PNB group (2606± 816 vs 2769± 1506 EUR, p=0.005). We estimated an incremental cost-effectiveness ratio (ICER) of − 243 ± 881 EUR/pain unit on the VAS.
Conclusion: Despite limitations, the ultrasound-guided PNB seems to reduce costs in patient undergoing open hemorrhoidectomy under spinal anesthesia. It was shown to be clinically beneficial and cost-effective, and therefore recommendable in patients undergoing open hemorrhoidectomy.
Keywords: pudendal nerve, nerve block, cost-benefit analysis, postoperative pain, hospital costs
Introduction
Hemorrhoidectomy is a common surgical procedure, often associated with significant postoperative pain1 and a remarkable economic burden, estimated at $800 million annually in the United States.2 Driven by a global need to reduce health care costs, hemorrhoid surgery is increasingly performed in a day surgery setting, and many studies have demonstrated its feasibility from a clinical and organizational point of view. An optimal post-operative pain management is the key to reducing the rate of primary admission and re-hospitalization which still remains a relevant issue.3–7 Pudendal nerve block (PNB) has been demonstrated to reduce postoperative pain and re-admission rates after open hemorrhoidectomy.8–10
In our previous article,11 we already described results of a double-blind randomized trial addressing the use of PNB in patients undergoing open hemorrhoidectomy. In short, we demonstrated that patients undergoing PNB in addition to spinal anesthesia had significantly less pain and shorter length of hospital stay after open hemorrhoidectomy. In particular, at 6, 12, 24 and 48 hours the pain on the VAS resulted to be 2.8 vs 4.6 (p=0.046), 3.4 vs 4.7 (p=0.697), 1.4 vs 3.1 (p=0.016) and 1.0 vs 2.1 (p=0.288) in the PNB and control groups, respectively. Opioid consumption was comparable between groups (21.7% vs 38.5% in the PNB and control groups, p=0.356). Length of hospital stay was 1.2 vs 1.8 days, respectively (p=0.046). Nine patients in the PNB group and ten in the control group were planned as day-case surgery, of whom, two patients in the control group required to be hospitalized because of a case of minor bleeding and a case of severe pain. One case of urinary retention in the PNB groups and two cases of postoperative bleeding in the control arm were noted. The two groups were similar in terms of number of planned in- and outpatient management, unplanned hospital admission rates, comorbidities and complications.
As shorter hospital stay and unplanned re-admissions have been demonstrated already,10,11 we can assume that the PNB use may also play a role in reducing costs related to hemorrhoid surgery but, to date, no study has addressed this aspect.
The aim of our study was to perform a cost analysis on PNB use in in- and outpatients undergoing open hemorrhoidectomy.
Methods
Study Design
This study was a double-blind randomized controlled trial, performed at the Department of Surgery, Ente Ospedaliero Cantonale, Regional Hospital of Bellinzona e Valli, and approved by the local ethic committee (2017–00769 CE TI 3222, ClinicalTrials.gov Identifier NCT04251884).
Patients undergoing Milligan-Morgan hemorrhoidectomy from January 2018 to December 2019 were included and randomized to undergo spinal anesthesia either with or without the PNB. Details on patient selection and analyses methods have been reported in the previous publication by Di Giuseppe et al.11 Among its secondary endpoints, a post-hoc cost-effectiveness analysis based on the code and TARMED reimbursement system in Switzerland was planned and represents the topic of this study.
Along with the already published demographic and clinical data, in-hospital direct and indirect costs for in- and outpatients, operating time and operating theatre occupancy were prospectively collected. All patients operated until December 31st, 2018 were planned to stay overnight. Thereafter, following a change in Swiss federal health insurance coverage policy, it became mandatory to manage all patients as outpatients, unless contraindicated because of significant comorbidities or logistical reasons, that had to be documented.12 One additional visit was planned in the outpatient group a week after surgery and such costs were also included.
Cost Calculation and Modeling
The types of costs to consider included direct, indirect, and total costs. Direct costs were defined as those directly charged to patients (medications, medical products, partial physicians fees) and correspond to the actual resource consumption. Indirect costs were those not directly accountable to patients but that had to be estimated and they were either variable or fixed. Such variable costs are calculated according to diagnostic (ICD-10)13 and intervention codes (CHOP; Swiss operation classification)14 for operating theatre, anesthesia, radiology, laboratory, physician salaries and hospital stay. The CHOP and ICD-10 codes are registered during the hospital stay according to diagnostics, interventions and procedures that patients undergo. Other indirect costs that are fixed (ie, administration) are charged independently for the interventions and diagnostics the patients undergo.
Since January 1st 2012, all hospitals in Switzerland have adopted diagnosis-related group (DRG) as reimbursement system (Swiss-DRG) for inpatient treatment.15,16 The DRG-based reimbursement for a given patient accounts for a severity score (cost-weight) and a fixed reimbursement according to the length of stay.17 Unlike outpatient treatments, the hospital reimbursement is regulated by the tariff system for outpatient medical services (TARMED),18 a nationwide, uniform tariff structure with respect to fee-for-service tariffs. TARMED defines a code for every medical procedure carried out in the outpatient setting. A specific number of points are assigned to each code according to the medical and technical efforts of the respective procedure. DRG- and TARMED-based reimbursements should cover the costs that hospital incurs in providing healthcare services.
All financial data are expressed in EURO (EUR): Swiss Franc to EUR exchange rate = 0.92291 (updated on 19th August 2020).
Statistical Methods
Quantitative data on direct, indirect and total costs were presented as mean with standard deviation (SD) and compared with the variance ratio test (F-test). Qualitative data are presented as absolute number with percentage and were compared with the Chi-Square test. Incremental cost-effectiveness ratio (ICER) was defined as (cost1-cost0)/(effect1-effect0). A probabilistic sensitivity analysis was conducted to test the robustness of the model results in changes in costs and health outcome (ie, pain on the VAS). A log-normal probability distribution, parameterized by the observed measures of centrality (sample means) and dispersion (standard errors) was used to generate a thousand pair values of costs and effects differences, thus representing uncertainty around the mean estimates of the two variables of interests. Univariate and multivariate analyses with odds ratio (OR) and 95% confidence interval (CI) were performed to test association between costs and variables of interest. A p-value < 0.05 was considered statistically significant. MedCalc Statistical Software version 19.3.1 (MedCalc Software Ltd, Ostend, Belgium; https://www.medcalc.org; 2020).
Results
The cost analysis included all 49 patients, 23 of whom, in addition to spinal anesthesia, received a PNB, whereas 26 did not. There were no statistically significant differences in mean overall occupation time of the operating theatre (80.6 ± 17.3 vs 73.2 ± 15.8 minutes, p=0.662), mean operative time (PNB group: 31.3 ± 11.0 vs control group: 29.2 ± 9.9 minutes, p=0.610) or time required for anesthesia (PNB group: 49.3 ± 15.9 vs control group: 44.0 ± 11.6, p=0.124).
Direct costs were comparable between groups (PNB group: 482 ± 386 vs control group: 613 ± 543 EUR, p=0.108), while indirect costs were significantly lower in the PNB group (2606 ± 816 vs 2769 ± 1506 EUR, p=0.005). Total costs were lower in the PNB group (PNB group: 3088 ± 979 vs control group: 3497 ± 1697, p=0.007). Hospital earnings resulted comparable in PNB and control groups (729 ± 1904 vs 442 ± 1339 EUR, p=0.101) as the hospital reimbursement did not change due to the PNB performing. Details are reported in Figure 1 and Table 1.
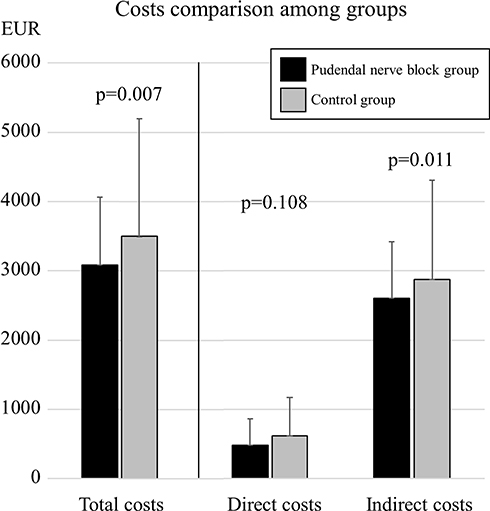 |
Figure 1 Total, direct and indirect costs comparison between groups. |
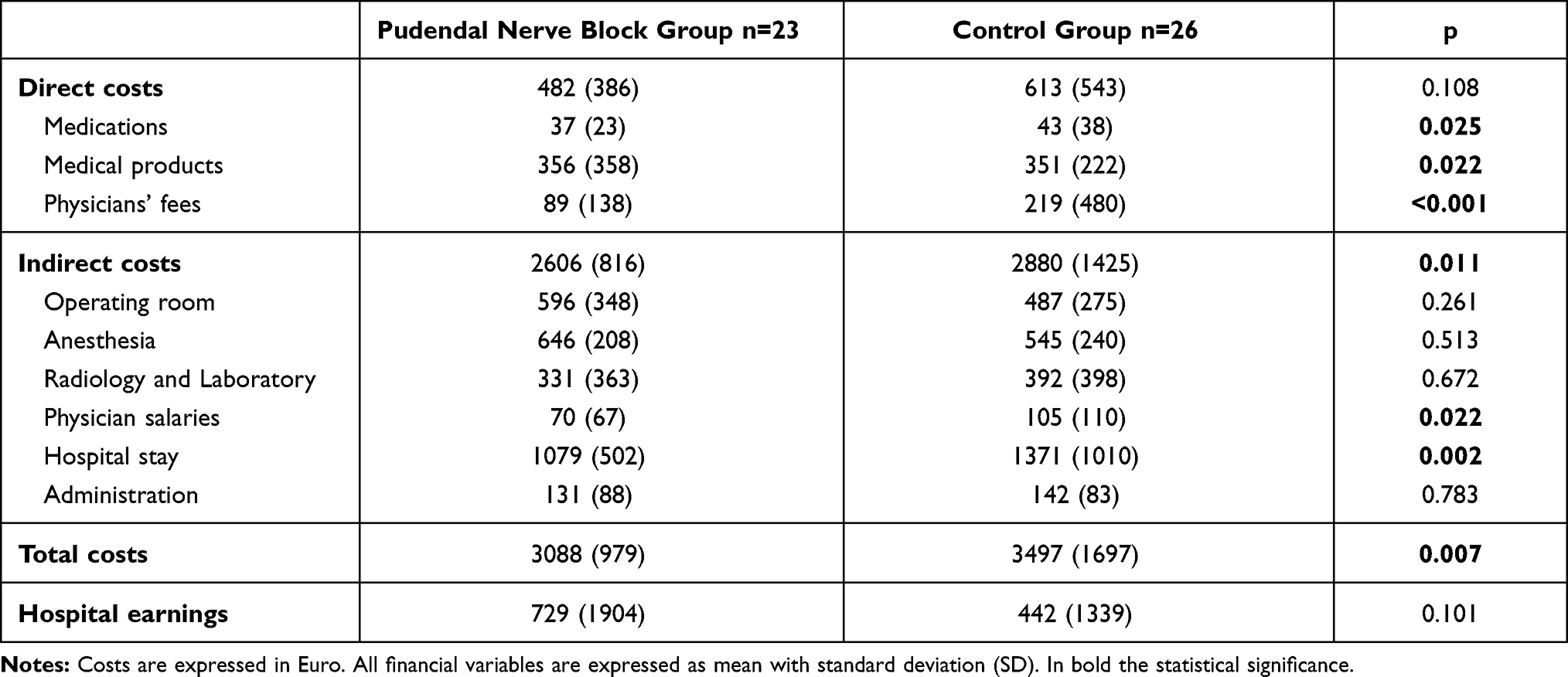 |
Table 1 Costs Analysis Among Groups |
The overall cost saving in PNB group was estimated in 409 ± 1401 EUR. Based on our finding of 1.68 ± 2.00 units pain difference on the VAS at 24 hours between PNB and control group, the ICER resulted −243 ± 881 EUR/pain unit on the VAS. Sensitivity analyses showed that the results ranged from quite robust to uncertain. PNB was 50% likely to result the dominant approach – with a negative ICER – while chances are that its cost-effectiveness does not overcome the threshold of 500 EUR (950 EUR) per pain unit on the VAS in 70% (80%) of the cases (Figure 2).
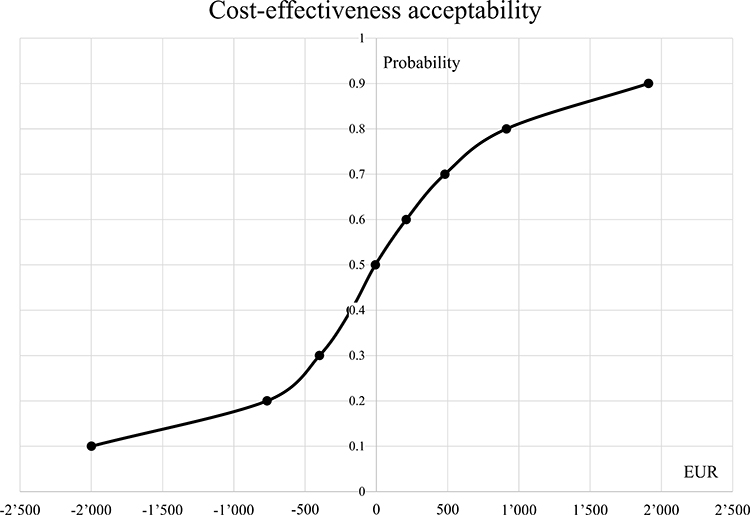 |
Figure 2 Cost-effectiveness acceptability of the pudendal nerve block use. |
In the uni- and multivariate analyses, the only retained factor which showed to be independently correlated to total costs was the length of hospital stay (OR 3.026, 95% CI 1.017–9.007, p=0.047). Table 2. Sub-analyses for direct and indirect costs did not show any noteworthy difference as compared to the total cost analysis.
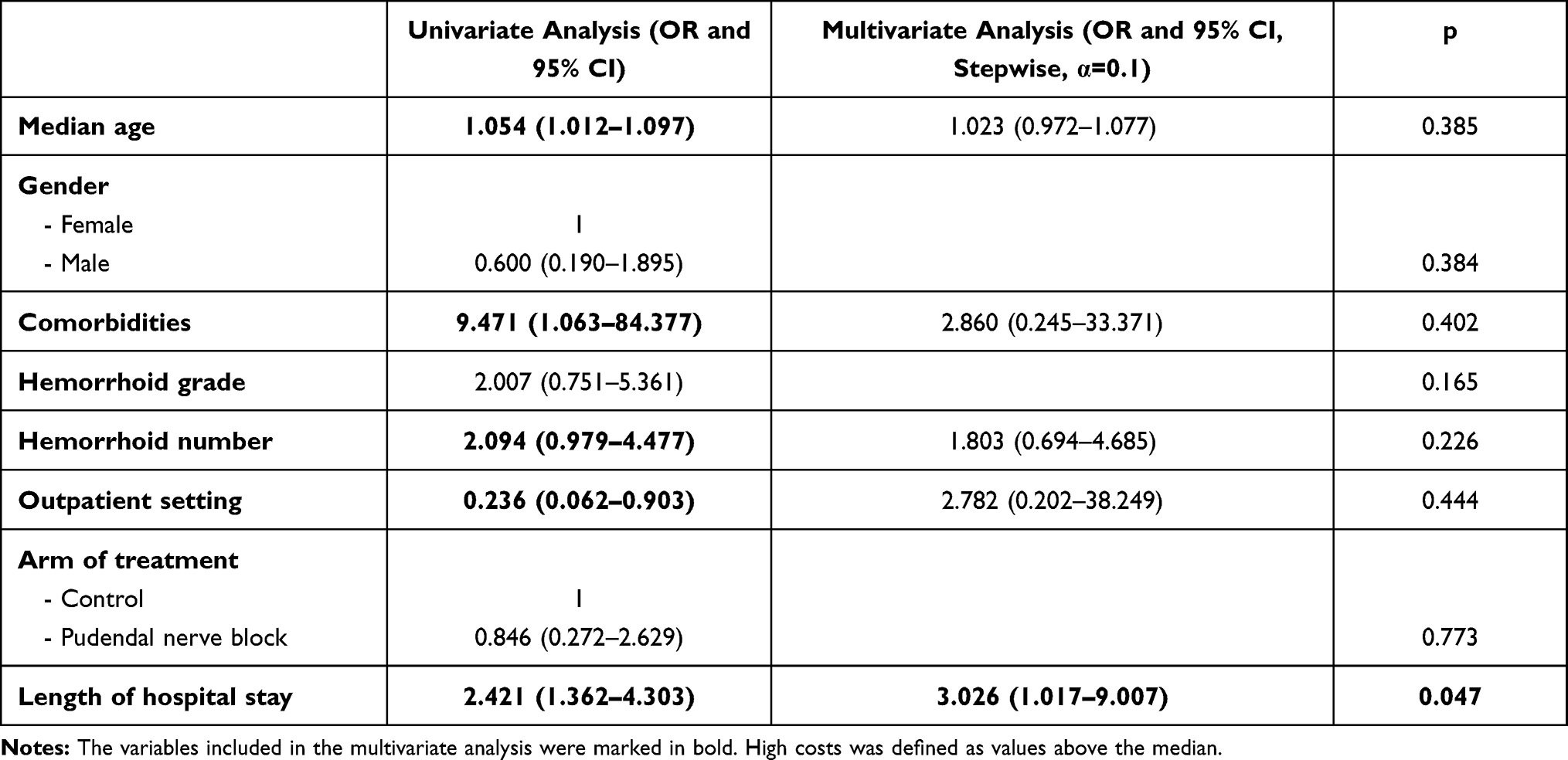 |
Table 2 Uni- and Multivariate Analyses of Factors Associated with High Total Costs |
The sub-group analysis on in- and outpatients showed that in the inpatient group, direct costs (PNB group: 544 ± 462 vs control group: 664 ± 687 EUR, p=0.159), indirect costs (PNB group: 2833 ± 895 vs control group: 3048 ± 1322 EUR, p=0.165) and total costs (PNB group: 3377 ± 1121 vs control group: 3712 ± 1699 EUR, p=0.140) were similar. In the outpatient group, direct costs were similar among groups (PNB group: 385 ± 213 vs control group: 533 ± 158 EUR, p=0.416), but indirect costs (2253 ± 545 vs 2582 ± 1628 EUR, p=0.006) and total costs (2638 ± 469 vs 3115 ± 1723 EUR, p=0.001) were lower in the PNB group.
Discussion
Analytical accounting data from our double-blind randomized trial demonstrated a significant reduction in indirect and total costs in patients treated with open hemorrhoidectomy with PNB in addition to spinal anesthesia, compared to those with spinal anesthesia only.
This important finding suggests that PNB could be a solution to two problems related to hemorrhoid surgery: post-operative pain and cost. Several trials have demonstrated that PNB is safe, feasible, effective and does not prolong the overall operative time.8,9,11,19,20 Indeed, the PROSPECT group guidelines suggest the use of perianal anesthesia or PNB in the management of pain after excisional hemorrhoidectomy.21
Pain and cost related to hemorrhoid surgery have been the subject of several studies, comparing different surgical techniques. It is well accepted that, compared to other less invasive techniques, excisional hemorrhoidectomy is the most efficient technique in terms of recurrence rates but at the price of higher post-operative pain.1,22,23 Studies have shown excisional hemorrhoidectomy to be less costly than stapled hemorrhoidectomy.24,25 Watson et al.,24 in a large multicenter National Health Service based randomized trial, found that the traditional excisional surgery was more cost-effective than stapled hemorrhoidopexy. Authors reported a mean cost per patient for traditional excisional surgery of £602 ± 507 compared with £941 ± 415 for stapled hemorrhoidopexy. The Quality Adjusted Life Years (QALY) for excisional surgery group was 1.69 ± 0.38 vs 1.62 ± 0.43 for hemorrhoidopexy group, thus concluding that stapled hemorrhoidopexy cost more and had a lower QALYs than excisional surgery. Open and stapled hemorrhoidectomy have been also evaluated in 2012 by Manfredelli et al,26 who reported that conventional procedures were more invasive and slightly more painful in the early postoperative period than stapled hemorrhoidectomy, which showed more complications and, therefore, was associated with higher costs. Brown et al27 reported a mean total cost of £1750 vs £723 per patient in the hemorrhoidal artery ligation and rubber band ligation groups, respectively. Kim28 reported higher overall costs in patients undergoing complete excisional hemorrhoidectomy and repair using flaps as compared to primary excisional hemorrhoidectomy and secondary suture-ligation in patients with circumferentially protruding hemorrhoids.
Our study did not aim at comparing the costs of different surgical techniques but rather the costs related to different anesthesia techniques. The finding that PNB not only reduces pain but also decreases costs, may be a further argument for open hemorrhoidectomy. That being said, to date, no studies have analyzed the financial impact of peripheral anesthetic blocks in patients undergoing open hemorrhoidectomy.
In our study, costs associated with the pudendal nerve block procedure (performed by an expert anesthetist) were adequately compensated by the reduced need for pain medications, decreased demand for care and rapid discharge. In particular, the shorter hospital stay led to cost savings in medications, physicians’ fees and salaries and hospital stay costs. Altogether, savings ended up being greater than the increased costs to perform the PNB, so that, 409 EUR per patient was saved. Interestingly, the DRG- and TARMED-based reimbursements did not change when PNB was performed, so that with the PNB use, hospital has earned more consensually. Although the PNB in patients undergoing open hemorrhoidectomy requires investment in resources, the better pain control and the shorter hospital stay led to an overall cost saving, making it cost-effective. The sensitivity analysis seems to confirm such findings, even strong evidence cannot be drawn.
The subgroup analyses showed for outpatients lower indirect and total costs in the PNB group, while for inpatients it did not show any significant difference. As effect of the hospitalization, patients incur in higher charges that may mitigate the PNB impact on costs. The absence of a significant difference can also be explained with the smaller sample size (30 patients), though, a trend of cost saving in the PNB group was noted. For outpatients, the cost difference was even more pronounced than in the whole group analysis. Specifically, the outpatient group benefits most from PNB, as the improved pain control allowed early discharge and showed to be more cost-effective.
This study has some limitations. The first and most important encompasses the replicability and generalizability of our results. In particular, the present financial analysis may not be directly applicable worldwide since costs and reimbursement widely vary among countries. Differences between DRG- and non-DRG-based systems are present, and even between national DRGs.29 However, many healthcare systems have adopted the DRG-based reimbursements, ie the Swiss-DRG is similar to German-DRG, which shares similarities with other European countries and is even comparable with the US-DRG.13,29–31 In the outpatient setting, TARMED is similar to other nationwide used fee-for-service tariff systems. Nevertheless, generalizing our results would be admittedly hazardous.
Another limitation is represented by the small number of patients included that restricts the strength of evidence and probably limited the sensitivity analysis and likelihood of the multivariate analysis to detect factors associated to the higher costs. A further limitation is the lack of a precise disposable material count and time needed to perform the PNB. However, the randomization of patients and the precise data collection within a clinical trial are key points which minimized the risk of biases in the present study.
Conclusions
Despite limitations, the ultrasound-guided PNB seems to reduce indirect and total costs in patient undergoing open hemorrhoidectomy under spinal anesthesia. It was showed to be clinically beneficial and cost-effective, and therefore recommendable in patients undergoing open hemorrhoidectomy.
Abbreviations
CHOP, Swiss operation classification; DRG, diagnosis-related groups; EUR, euro; ICD-10, diagnostic codes; ICER, incremental cost-effectiveness ratio; LoS, length of stay; PNB, Pudendal nerve block; QALY, quality adjusted life years; SD, standard deviation; Swiss-DRG, Swiss diagnosis related groups; TARMED, tariff system for outpatient medical services; VAS, visual analogue scale.
Data Sharing Statement
The dataset analyzed during the current study is available from the corresponding author on reasonable request.
Ethics Approval and Consent to Participate
The study was approved by the local ethics committee (Comitato Etico Cantonale 2017-00769 CE TI 3222) and conducted in accordance with the Declaration of Helsinki. Registered on ClinicalTrials.gov (Identifier NCT04251884). Written informed consent was obtained before the inclusion in the study.
Author Contributions
Protocol/project development: Francesco Mongelli, Matteo Di Giuseppe, Davide La Regina, Andrea Saporito. Data acquisition and interpretation: Alberto Vannelli, Dimitri Christoforidis, Massimo Lucchelli. Statistical analysis. Francesco Mongelli, Matteo Di Giuseppe, Dimitri Christoforidis. Manuscript drafting. Andrea Saporito, Massimo Lucchelli, Alberto Vannelli. Manuscript revision and accountable for all aspects of the work: Francesco Mongelli, Davide La Regina, Matteo Di Giuseppe, Dimitri Christoforidis. All authors approved the final version of the manuscript. All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
No funding was received for this article.
Disclosure
All authors have no conflicts of interest or financial ties to disclose.
References
1. Simillis C, Thoukididou SN, Slesser AA, Rasheed S, Tan E, Tekkis PP. Systematic review and network meta-analysis comparing clinical outcomes and effectiveness of surgical treatments for haemorrhoids. Br J Surg. 2015;102(13):1603–1618. doi:10.1002/bjs.9913
2. Yang JY, Peery AF, Lund JL, Pate V, Sandler RS. Burden and cost of outpatient hemorrhoids in the United States employer-insured population, 2014. Am J Gastroenterol. 2019;114(5):798–803. doi:10.14309/ajg.0000000000000143
3. Asteria CR, Lauretta A, Martellucci J, et al. Does anaesthesia change severity of haemorrhoidal disease? A prospective and multicentre case-control study on haemorrhoidal disease assessment in two different settings: outpatient and operating theatre. Int J Colorectal Dis. 2016;31(8):1529–1531. doi:10.1007/s00384-016-2553-2
4. Yin X, Xu Y, Man X, et al. Direct costs of both inpatient and outpatient care for all type cancers: the evidence from Beijing, China. Cancer Med. 2019;8(6):3250–3260. doi:10.1002/cam4.2184
5. Ferrari D, Lopes TJ, França PF, Azevedo FM, Pappas E. Outpatient versus inpatient anterior cruciate ligament reconstruction: a systematic review with meta-analysis. Knee. 2017;24(2):197–206. doi:10.1016/j.knee.2017.01.002
6. Diurni M, Di Giuseppe M. Hemorrhoidectomy in day surgery. Int J Surg. 2008;6(Suppl 1):S53–5. doi:10.1016/j.ijsu.2008.12.018
7. Esser S, Khubchandani I, Rakhmanine M. Stapled hemorrhoidectomy with local anesthesia can be performed safely and cost-efficiently. Dis Colon Rectum. 2004;47(7):1164–1169. doi:10.1007/s10350-004-0550-y
8. Naja Z, Ziade MF, Lönnqvist PA. Nerve stimulator guided pudendal nerve block decreases posthemorrhoidectomy pain. Can J Anaesth. 2005;52(1):62–68. doi:10.1007/BF03018582
9. Naja Z, El-Rajab M, Al-Tannir M, et al. Nerve stimulator guided pudendal nerve block versus general anesthesia for hemorrhoidectomy. Can J Anaesth. 2006;53(6):579–585. doi:10.1007/BF03021848
10. Mongelli F, Treglia G, La Regina D, et al. Pudendal nerve block in hemorrhoid surgery: a systematic review and meta-analysis. Dis Colon Rectum. 2021;64(5):617–631. doi:10.1097/DCR.0000000000001985
11. Di Giuseppe M, Saporito A, La Regina D, et al. Ultrasound-guided pudendal nerve block in patients undergoing open hemorrhoidectomy: a double-blind randomized controlled trial. Int J Colorectal Dis. 2020;35(9):1741–1747. doi:10.1007/s00384-020-03630-x
12. The portal of the Swiss government. Ambulant vor stationär – liste mit Eingriffen verabschiedet. Available from: https://www.admin.ch/gov/de/start/dokumentation/medienmitteilungen.msg-id-69835.html.
13. La Regina D, Di Giuseppe M, Lucchelli M, et al. Financial impact of anastomotic leakage in colorectal surgery. J Gastrointest Surg. 2019;23(3):580–586. doi:10.1007/s11605-018-3954-z
14. Prozeduren (CHOP 2020). Available from: https://medcode.ch/ch/de/chops/CHOP%202020.
15. Mongelli F, Ferrario Di Tor Vajana A, FitzGerald M, et al. Open and laparoscopic inguinal hernia surgery: a cost analysis. J Laparoendosc Adv Surg Tech A. 2019;29(5):608–613. doi:10.1089/lap.2018.0805
16. Swiss DRG. Available from: https://www.swissdrg.org/.
17. Chok L, Bachli EB, Steiger P, et al. Effect of diagnosis related groups implementation on the intensive care unit of a Swiss tertiary hospital: a cohort study. BMC Health Serv Res. 2018;18(1):84. doi:10.1186/s12913-018-2869-4
18. Health systems in transition: Switzerland Vol 17 No 4. Available from: https://www.bag.admin.ch/dam/bag/fr/dokumente/int/switzerland-hit-rapport-complet.download/switzerland-hit-rapport-complet.switzerland-hit-rapport-complet.
19. Brunat G, Pouzeratte Y, Mann C, Didelot JM, Rochon JC, Eledjam JJ. Posterior perineal block with ropivacaine 0.75% for pain control during and after hemorrhoidectomy. Reg Anesth Pain Med. 2003;28(3):228–232. doi:10.1053/rapm.2003.50132
20. Tepetes K, Symeonidis D, Christodoulidis G, Spyridakis M, Hatzitheofilou K. Pudendal nerve block versus local anesthesia for harmonic scalpel hemorrhoidectomy: a prospective randomized study. Tech Coloproctol. 2010;14(Suppl 1):S1–3. doi:10.1007/s10151-010-0614-z
21. Sammour T, Barazanchi AW, Hill AG. Evidence-based management of pain after excisional haemorrhoidectomy surgery: a PROSPECT review update. World J Surg. 2017;41(2):603–614. doi:10.1007/s00268-016-3737-1
22. Panarese A, Pironi D, Vendettuoli M, et al. Stapled and conventional Milligan-Morgan haemorrhoidectomy: different solutions for different targets. Int J Colorectal Dis. 2012;27(4):483–487. doi:10.1007/s00384-011-1342-1
23. Laughlan K, Jayne DG, Jackson D, Rupprecht F, Ribaric G. Stapled haemorrhoidopexy compared to Milligan-Morgan and Ferguson haemorrhoidectomy: a systematic review. Int J Colorectal Dis. 2009;24(3):335–344. doi:10.1007/s00384-008-0611-0
24. Watson AJ, Hudson J, Wood J, et al. Comparison of stapled haemorrhoidopexy with traditional excisional surgery for haemorrhoidal disease (eTHoS): a pragmatic, multicentre, randomised controlled trial. Lancet. 2016;388(10058):2375–2385. doi:10.1016/S0140-6736(16)31803-7
25. Ho YH, Cheong WK, Tsang C, et al. Stapled hemorrhoidectomy–cost and effectiveness. Randomized, controlled trial including incontinence scoring, anorectal manometry, and endoanal ultrasound assessments at up to three months. Dis Colon Rectum. 2000;43(12):1666–1675. doi:10.1007/BF02236847
26. Manfredelli S, Montalto G, Leonetti G, et al. Conventional (CH) vs. stapled hemorrhoidectomy (SH) in surgical treatment of hemorrhoids. Ten years experience. Ann Ital Chir. 2012;83(2):129–134.
27. Brown SR, Tiernan JP, Watson AJM, et al. Haemorrhoidal artery ligation versus rubber band ligation for the management of symptomatic second-degree and third-degree haemorrhoids (HubBLe): a multicentre, open-label, randomised controlled trial. Lancet. 2016;388(10042):356–364. doi:10.1016/S0140-6736(16)30584-0
28. Kim JC. Analysis of surgical treatments for circumferentially protruding haemorrhoids: complete excision with repair using flaps versus primary excision with secondary suture-ligation. Asian J Surg. 2006;29(3):128–134. doi:10.1016/S1015-9584(09)60071-3
29. Quentin W, Scheller-Kreinsen D, Blümel M, Geissler A, Busse R. Hospital payment based on diagnosis-related groups differs in Europe and holds lessons for the United States. Health Aff (Millwood). 2013;32(4):713–723. doi:10.1377/hlthaff.2012.0876
30. Eurostat. Handbook on prices and volume measures in national accounts. Available from: https://ec.europa.eu/eurostat/documents/3859598/7152852/KS-GQ-14-005-EN-N.pdf.
31. Busse R, Geissler A, Aaviksoo A, et al. Diagnosis related groups in Europe: moving towards transparency, efficiency, and quality in hospitals? BMJ. 2013;346(jun07 3):f3197. doi:10.1136/bmj.f3197
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.