")
Back to Journals » International Medical Case Reports Journal » Volume 15
Ultrasound-Guided Placement of a Hemodialysis Catheter into the Distal Femoral Vein in a Patient with Multiple Catheters: A Case Report
Authors Morishige S, Yamaguchi Y , Nakajima K, Tsuboi S, Sugawara Y, Hayami H, Tobias JD , Inagawa G
Received 20 January 2022
Accepted for publication 8 April 2022
Published 19 April 2022 Volume 2022:15 Pages 209—212
DOI https://doi.org/10.2147/IMCRJ.S359258
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 5
Editor who approved publication: Professor Ronald Prineas
Shuta Morishige,1 Yoshikazu Yamaguchi,1 Kei Nakajima,1 Sayaka Tsuboi,1 Yoh Sugawara,2 Hajime Hayami,1 Joseph D Tobias,3 Gaku Inagawa1
1Department of Anesthesiology, Yokohama Municipal Citizen’s Hospital, Yokohama, Japan; 2Department of Anesthesiology, Critical Care and Pain Medicine, Massachusetts General Hospital, Boston, MA, USA; 3Department of Anesthesiology and Pain Medicine, Nationwide Children’s Hospital and The Ohio State University, Columbus, OH, USA
Correspondence: Yoshikazu Yamaguchi, Department of Anesthesiology, Yokohama Municipal Citizen’s Hospital, 1-1 Mitsuzawanishimachi, Kanagawa-ku, Yokohama-shi, Kanagawa, 221-0855, Japan, Tel +81-45-316-4580, Fax +81-45-316-6580, Email [email protected]
Abstract: Cardiac surgery-associated acute kidney injury may require postoperative renal replacement therapy. Although the right internal jugular vein and femoral veins are generally the preferred insertion sites for the hemodialysis catheter for continuous renal replacement therapy, the presence of other indwelling catheters or prior thrombotic events from previous catheters may preclude use of these sites. We present a case in which the hemodialysis catheter was inserted into the distal femoral vein using point-of-care ultrasound in a patient with multiple catheter insertions after coronary artery bypass grafting. Although the tip of the dialysis catheter was more distal than the classic femoral approach, renal replacement therapy was performed without problems. Moreover, it was easier for the nurses to keep the insertion site clean and to change the patient’s position.
Keywords: central venous catheter, renal replacement therapy, femoral vein
Introduction
The incidence of cardiac surgery-associated acute kidney injury (AKI) is 22% with 2.3% of patients requiring renal replacement therapy (RRT).1 Although the right internal jugular vein (IJV) and femoral vein are generally the preferred choices for hemodialysis catheter insertion, those veins may not be readily available after cardiac surgery because of the presence of other indwelling catheters or previous catheter insertions and venous thrombotic complications.2 In the classical approach to the femoral vein, the vein is punctured approximately 2–3 cm below the inguinal ligament. In the low femoral vein approach, the femoral vein is accessed 10–15 cm below the inguinal ligament.3 We present a 71-year-old man with end-stage kidney disease (ESKD) requiring hemodialysis who presented for coronary artery bypass grafting (CABG). The patient had a central venous line and pulmonary artery catheter in his right IJV, an intra-aortic balloon pump (IABP) in his right femoral artery, and extra-corporeal membranous oxygenation (ECMO) cannulas in his left femoral artery and vein after surgery. Due to limited venous access to other sites, point-of-care ultrasound (POCUS) was used to guide the cannulation of the distal femoral vein for placement of the hemodialysis catheter. Written informed consent for publication of this case was obtained from the patient. The presentation follows the guidelines of the Institutional Review Board of Yokohama Municipal Citizen’s Hospital.
Case Presentation
A 71-year-old 75.9-kg man presented for on-pump coronary CABG for the treatment of coronary ischemia. His past medical history was significant for atrial fibrillation, type-2 diabetes mellitus, hypertension, and ESKD requiring hemodialysis, three times a week through an arteriovenous fistula in the left forearm. Preoperative transthoracic echocardiography (TTE) demonstrated an ejection fraction of 41% and mild-moderate mitral regurgitation. Coronary artery angiography revealed stenosis in the left anterior descending branch, the left circumflex branch, and the right coronary artery. After tracheal intubation, a central venous catheter and a pulmonary artery catheter were inserted in the right IJV. The surgical duration was 8 hours and 10 minutes. The duration of cardiopulmonary bypass was 5 hours and 15 minutes with an aortic cross-clamp time of 3 hours 6 minutes. The total blood loss was estimated at 1000 mL. Total fluids and transfusions included 1090 mL of isotonic crystalloid, 4 units of fresh frozen plasma, and 1000 mL of intraoperative blood salvage. As he was tilted to move from the operating table to the intensive care unit (ICU) bed, his blood pressure suddenly decreased. Massive bleeding and cardiac tamponade were ruled out by TEE. Despite the epinephrine infusion, hemodynamic instability and shock persisted. Therefore, an IABP was placed in the right femoral artery and venous-arterial ECMO was initiated through cannulation of the left femoral artery and vein. Postoperatively, due to fluid overload with an increase in body weight of more than 10 kg, the decision was made to initiate continuous renal replacement therapy (CRRT) with hemofiltration. Due to inability to access other venous sites due to the presence of other cannulas, a hemodialysis catheter was placed in the distal right femoral vein using POCUS. Bedside ultrasonography demonstrated that the catheter to the distal aspect of the femoral vein ratio was less than 45% and that the distal femoral vein was parallel to the femoral artery. The 12 French, 25 cm hemodialysis catheter (Blood access UK catheter kit, NIPRO, Japan) was placed using an out-of-plane ultrasound guided technique (Figure 1). Although the tip of the catheter was within the femoral vein, it was easy to maintain a blood flow of 100 mL/min. Anticoagulation was maintained by the infusion of nafamostat at 10–20 mg/hour.
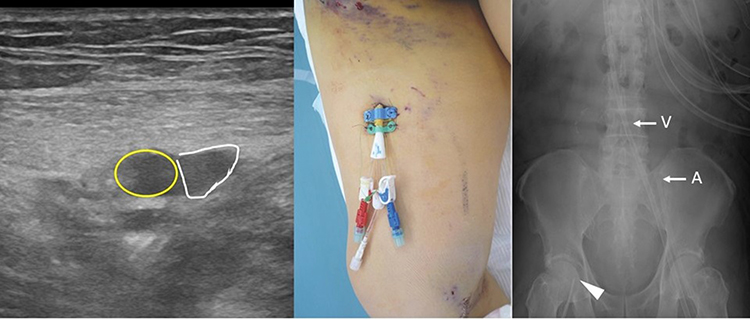 |
Figure 1 Out of plane, point-of-care ultrasound demonstrating the femoral artery (yellow circle) and femoral vein (white triangle). The femoral vein was located 1.8 cm from the skin (left). Hemodialysis catheter secured at the mid-point of the femoral vein (center), and plain radiograph demonstrating the position of the hemodialysis catheter in the femoral vein (arrow head), arterial ECMO cannula (arrow A), and venous ECMO cannula (arrow V) (right). |
After three thoracic explorations to achieve hemostasis, VA-ECMO was discontinued on the third postoperative day (POD). The IABP was removed on POD 7. When the IABP introducer sheath was removed, CRRT was paused as compression of the femoral artery disrupted CRRT flow. After the pressure was released, CRRT was resumed without problems. The patient’s trachea was extubated on POD 7. CRRT was performed until POD 14. Ultrasonography using B-mode and color Doppler demonstrated that there was no deep venous thrombosis in the femoral vein after removal of the hemodialysis catheter. The patient was discharged from the ICU on POD 16.
Discussion
The need for RRT after cardiac surgery has been estimated to be 2.3% in adults.4 CRRT is generally preferred over intermittent hemodialysis in hemodynamically unstable patients.5 A double lumen percutaneous hemodialysis catheter is the preferred access to establish CRRT. The preferred site for cannulation is the right IJV followed by the right or left femoral vein.2 Using an arteriovenous fistula for CRRT is generally contraindicated due to the high incidence of complications. Al Rifai et al reported that 21% of patients with ESKD who underwent CRRT using an arteriovenous fistula or graft had access complications including bleeding, infiltration, and thrombus.6 Although the left internal jugular vein is generally considered the third option for percutaneous placement of a hemodialysis catheter, there have been anecdotal reports of brachiocephalic vein perforation due to the length of the catheter and the angle of the venous confluence.7 These concerns may be further complicated following cardiac surgery in critically ill patients due to indwelling catheters, cannulas, and mechanical devices. This was the case in our patient as a pulmonary artery catheter had been placed through the right IJV, ECMO cannulas had been placed in the left femoral artery and vein, an IABP had been placed in the right femoral artery, and bedside ultrasound revealed that femoral artery and vein were in a vertical position at the typical femoral vein cannulation site. The left and right subclavian veins were not considered optimal because of their depth and the patient’s full anticoagulation status during ECMO. Due to these concerns, a distal femoral vein approach was chosen.
The distal femoral vein approach was first reported in 1998.8 To date, the majority of reports have been anecdotal, published as letters or brief correspondence without ultrasound images to demonstrate the technique.3,8,9 The quality of ultrasound machines have dramatically improved over the past 10 years, and most practicing anesthesiologists are facile with bedside point-of-care ultrasound for placement of central venous and arterial access. Given the deeper nature of the femoral vessels at their midpoint, palpation of the femoral artery impulse may not be feasible, thereby making ultrasound identification of the vessels mandatory for successful cannulation. POCUS can be used to demonstrate both the anatomical relationship of the vessels and accompanying structures as well as the needle tip, which may limit the incidence of puncture of the posterior wall of the vessel thereby limiting bleeding risk. Additionally, measurement of the vein is feasible to guide selection of the appropriate size of the hemodialysis catheter. There are some limitations to the clinical use of POCUS that should be recognized. Orientation of the probe must be maintained to correctly demonstrate the positioning of the vessels to avoid arterial puncture. Identification of the needle tip may be difficult in the patient with obesity. Significant education and clinical training is needed to initially master and maintain familiarity with the use of ultrasound.
The procedure for ultrasound-guided distal femoral vein approach resembles that of ultrasound-guided adductor canal block or saphenous nerve block. The patient’s leg is slightly abducted. The landmark for the needle insertion point is the midpoint between the anterior superior iliac spine and the base of patella.10 After a high frequency linear probe is placed at this landmark point, the probe needs to move cephalad and caudad until a point is identified where the femoral artery and vein lie side-by-side. In addition to offering another access point to the femoral vein away from other mechanical devices and cannulas, the distal femoral approach may lead to improved flows with less kinking of the catheter as the angle into the vein is less acute and there may be a decreased incidence of fecal soiling of the site when compared to the classic approach to the femoral vessels.
However, Karakitosos et al reported that there is a higher risk of thrombotic complications with the distal femoral vein approach over the classic femoral vein approach. Despite prophylactic low-molecular weight heparin therapy, they reported that DVT occurred in 32.5% of patients with the distal femoral approach compared to 10% of patients with the classic femoral approach.9 DVT was detected an average of 9 days after catheter insertion. The use of titrated regional anticoagulation for CRRT in our patient and systemic anticoagulation during ECMO may have decreased the risk of DVT in our patient. Additionally, to ensure adequate flows for CRRT, the distal tip of the catheter should ideally be located at the lower edge of the inferior vena cava. This may be difficult to achieve given the length of the hemodialysis catheter and the distal site of insertion. In our patient, although the distal catheter tip was located in the femoral vein, CRRT flows were adequate.
In summary, we present the use of the distal femoral vein for the placement of a hemodialysis catheter for CRRT. The distal femoral vein should be considered when other access sites are limited due to the presence of catheters, mechanical devices, or thrombotic disease. Point-of-care ultrasound can be used to facilitate placement and select the appropriate size of the hemodialysis catheter.
Abbreviations
AKI, acute kidney injury; CRRT, continuous renal replacement therapy; DLC, double lumen catheter; ECMO, extra-corporeal membranous oxygenation; ESKD, end-stage kidney disease; IJV, internal jugular vein; RRT, renal replacement therapy; TEE, transesophageal echocardiography; CABG, coronary artery bypass grafting; POD, postoperative day.
Disclosure
The authors do not have conflicts of interest in this work.
References
1. Parida S, Badhe AS. Cardiac surgery-associated acute kidney injury. J Anesth. 2013;27:433–446. doi:10.1007/s00540-012-1523-2
2. Huriaux L, Costille P, Quintard H, Journois D, Kellum JA, Rimmele T. Haemodialysis catheters in the intensive care unit. Anaesth Crit Care Pain Med. 2017;36:313–319. doi:10.1016/j.accpm.2016.10.003
3. Wilson E, Hillier J, Farrimond J. Ultrasound guided ‘low approach’ femoral vein cannulation. Anaesthesia. 2004;59:725. doi:10.1111/j.1365-2044.2004.03850.x
4. Hu J, Chen R, Liu S, Yu X, Zou J, Ding X. Global incidence and outcomes of adult patients with acute idney injury after cardiac surgery: a systematic review and meta-analysis. J Cardiothorac Vasc Anesth. 2016;30:82–89. doi:10.1053/j.jvca.2015.06.017
5. Borisov AS, Malov AA, Kolesnikov SV, Lomivorotov VV. Renal replacement therapy in adult patients after cardiac surgery. J Cardiothorac Vasc Anesth. 2019;33:2273–2286. doi:10.1053/j.jvca.2019.02.023
6. Al Rifai A, Sukul N, Wonnacott R, Heung M. Safety of arteriovenous fistulae and grafts for continuous renal replacement therapy: the Michigan experience. Hemodial Int. 2018;22:50–55. doi:10.1111/hdi.12550
7. Winkes MB, Loos MJ, Scheltinga MR, Teijink JA. Dialysis catheter placement via the left internal jugular vein: risk of brachiocephalic vein perforation. J Vasc Access. 2016;17:e75–e78. doi:10.5301/jva.5000566
8. Sato S, Ueno E, Toyooka H. Central venous access via the distal femoral vein using ultrasound guidance. Anesthesiology. 1998;88:838–839. doi:10.1097/00000542-199803000-00047
9. Karakitsos D, Saranteas T, Patrianakos AP, Labropoulos N, Karabinis A. Ultrasound-guided “low approach” femoral vein catheterization in critical care patients results in high incidence of deep vein thrombosis. Anesthesiology. 2007;107:181–182. doi:10.1097/01.anes.0000268280.02529.88
10. Wong WY, Bjorn S, Strid JM, Borglum J, Bendtsen TF. Defining the location of the adductor canal using ultrasound. Reg Anesth Pain Med. 2017;42:241–245. doi:10.1097/AAP.0000000000000539
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.