Back to Journals » Breast Cancer: Targets and Therapy » Volume 17
Ultrasound-Guided Percutaneous Microwave Coagulation Studies on VX2 Rabbit Models for Breast Cancer Treatment and Ultrasound Imaging Assessment
Authors Gao Q, Huang H, Shi JJ, Wang L, Li WM ![]()
Received 12 December 2024
Accepted for publication 19 February 2025
Published 25 February 2025 Volume 2025:17 Pages 241—252
DOI https://doi.org/10.2147/BCTT.S510928
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Robert Clarke
Qi Gao,1,* Hu Huang,2,* Jin-Jun Shi,1 Ling Wang,1 Wei-Min Li3
1Department of Ultrasonography, Zhongda Hospital, Medical School, Southeast University, Nanjing, Jiangsu, People’s Republic of China; 2Department of Thyroid and Breast Surgery, Affiliated Hospital of Jiangnan University, Wuxi, Jiangsu, People’s Republic of China; 3Department of Ultrasonography, Affiliated Hospital of Jiangnan University, Wuxi, Jiangsu, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Wei-Min Li, Department of Ultrasonography, Affiliated Hospital of Jiangnan University, Wuxi, Jiangsu, 214000, People’s Republic of China, Tel +8613912362309, Email [email protected] Ling Wang, Department of Ultrasonography, Zhongda Hospital, Medical School, Southeast University, Nanjing, Jiangsu, 210009, People’s Republic of China, Tel +8613852292915, Email [email protected]
Background: The study aimed to explore the tissue morphology and hemodynamics of rabbit VX2 breast carcinoma by high-frequency ultrasound (US) and the effectiveness and safety of US-guided percutaneous microwave coagulation (PMC) therapy on rabbit VX2 breast tumors.
Methods: Twenty VX2 tumor-bearing rabbits were assessed using color Doppler ultrasound for tumor growth characteristics including echo, size, blood supply and hemodynamic parameters once a week for six weeks. Subsequently, US-guided PMC was performed in randomly assigned ten VX2 tumor-bearing rabbits (the other ten as controls). US images after ablation were obtained and analyzed. Three rabbits with double VX2 tumors were used as pathological observation at weeks 0, 1, and 4 of ablation. The therapeutic efficacy was evaluated by tumor growth, physical examinations, survival time, survival rate and metastasis of tumors and histopathology.
Results: Ultrasound monitoring indicated that the tumor growth rate was 463.09% at the 2nd to 3rd weeks, and PMC was performed during this period under real-time US guidance. After microwave ablation, some tumors were greatly reduced or undetectable at week 8. Moreover, no flow signals were detected by US. The survival rates at 2 and 3 months in the treatment group and control group were 100%, 70% and 10%, 0%, respectively, while the metastatic rates were 10%, 30% and 90%, 100%, respectively (P< 0.05).
Conclusion: The proliferation and metastasis of rabbit VX2 breast carcinoma were monitored by US imaging, and US-guided percutaneous microwave ablation was proven to be a safe, effective and minimally invasive therapeutic option for treating breast cancer in rabbits, showing potential clinical applicability.
Keywords: percutaneous microwave, VX2 rabbit models, breast cancer, ultrasound
Introduction
Breast cancer is the most common cancer worldwide and over 2.3 million new cases and 685,000 deaths from breast cancer occurred in 20201.1 The global incidence continues to rise, affecting approximately 1 in 8 and leading to the greatest number of cancer‐related deaths in women worldwide.2 Although invasive surgery is currently considered the common standard for the treatment of breast tumors, there is an increasing demand for minimally invasive techniques, such as radiofrequency ablation (RFA), cryoablation, laser ablation and microwave ablation and high-intensity focused US (HIFU),3–6 used to treat small breast cancer as an alternative to surgical excision, potentially reducing the complications, improving cosmesis and reducing hospital stay. Among them, percutaneous microwave coagulation (PMC) has gradually been accepted as a promising new modality for the treatment of small breast malignancies and benign breast lesions with many advantages.7–9
As one of the local tumor ablation therapies currently available, PMC is a minimally invasive local thermal ablation procedure that has been reported to be used to destroy tumors and soft tissues by using microwave energy to create coagulation and localized tissue necrosis. Compared with other minimally invasive technologies, including RFA and cryotherapy, PMC shows an improved convection profile, consistently higher intratumor temperatures, larger ablation volumes, and lower ablation times.10 At present, PMC has proven its safety and efficacy in the management of tumor ablation of lung, liver, bone, adrenal gland and kidney.11–13 More recently, there is increasing experimental evidence that image-guided PMC is a promising treatment for solitary breast cancers due to the special anatomical location of the breast, which is between the ectopectoralis and skin.14,15 However, although many studies are available online for evaluating the efficacy and safety of PMC against carcinoma in animals and human, there have been few reports on PMC treatment for breast cancer so far. So the safety and feasibility of PMC therapy are still lacking more evidences and related animal experiments are necessary.
Ideal tumor animal models require as much resemblance as possible in location, histologic type, etiology, and pathogenesis with human tumor biological behavior. The VX2 tumor, a squamous cell cancer model, which was firstly proposed by Shope and Hurst in 1933, has been implanted in many sites of rabbits, including the liver, kidney, lung, breast, and muscle.16 The rabbit breast VX2 tumor implantation model represents an ideal model of breast cancers due to the rapid growth of VX2 tumors and their similarity to human breast cancer. In addition, this large-animal tumor model can be used in evaluating imaging, as well as for the development of minimally invasive therapy. Imaging evaluation, given the wide availability, low‐cost, portability, nonionizing and real-time dynamic nature of US imaging, makes it the most ideal image monitoring method to detect tumor growth morphological changes, tumor size and tumor-perfusing blood vessels. In addition to dynamic monitoring of tumor growth characteristics, US imaging also has the capabilities of real-time dynamic guiding microwave antenna during the PMC and follow-up evaluation of the response to therapy and for surveillance of recurrence and residual tumors.17–19 To ensure complete ablation, it is essential to improve the ablation techniques and refine the imaging guidance.
Here, the the purpose of this study was to establish a rabbit breast VX2 transplantation cancer model and monitor the whole course of VX2 tumor growth and distant metastasis as well as to explore the feasibility and safety of percutaneous US-guided microwave ablation in treating a VX2 rabbit breast solid tumor model by high-frequency US imaging and pathology characteristics, thus laying a certain foundation for subsequent basic and clinical research.
Materials and Methods
Animals and Tumor Model
Healthy adult female New Zealand White rabbits were purchased from the Academy of Military Medical Science (China). All animal experiments were approved by the Animal Care Committee of Jiangsu Province and were performed in accordance with the “Institute Ethical Committee Guidelines” for animal experimentation and care. The inclusion criteria of rabbits were as follows: (1) age range 12–14 weeks, weighing 3.6–4.0 kg; (2) SPF grade; (3) female. The exclusion criteria included the following: (1) There are serious health issues present; (2) abnormal behavior before the experiment. The rabbits were anesthetized using an intravenous injection of pentobarbital (30 mg/mL, 0.8 to 1.2 mL/kg, pentobarbital sodium; Sigma, St., Louis, MO, USA) before VX2 tumor inoculation and other procedures. To establish a rabbit breast VX2 tumor implantation model, the required tumor tissue with fish-meat-like appearance was obtained from one tumor-bearing rabbit with a VX2 tumor in the thigh from the laboratory in the Department of Hepatobiliary Surgery in Xijing Hospital and was first cut into small strips (0.1 cm × 0.1 cm × 0.1 cm), and then 0.2–0.3 mL of the tumor suspension was slowly injected into the mammary fat pad underneath the right second nipple with a 16-gauge needle subcutaneously.20 Experiments were initiated when tumors reached ~3.0 cm in diameter (as determined with ultrasonography) at the 2nd~3rd week after tumor implantation.
US Imaging Observation of VX2 Tumor Growth Characteristics Before PMC
Color Doppler ultrasonography was performed weekly after tumor inoculation using an L739 transducer connected to a GE LOGIQ 500 MR3 PLUS Color Doppler Diagnostic Apparatus. Before acquiring US images of tumors, each of the tumor-bearing rabbits was first fixed on the examination table to perform US scanning. The breast was detected with two-dimensional (2D) ultrasound, which was used to record the lesion echo, diameter, shape and color Doppler flow images inside and outside of the tumor. The maximum diameter of the lesion in 3 axes was measured on the B-mode US images, and their volumes were estimated by the following formula, assuming an ellipsoid shape for the lesions: Volume=length2×width2×heigth2×4π3. Moreover, the pattern of blood flow signals around or inside the tumors detected by CDFI or PDI mode was semiquantified as spotlike, short rod-like and strip blood flow signals according to the criteria proposed by Adler et al.20 Hemodynamic parameters of tumor arteries such as the PSV and RI acquired using Doppler US with spectral analysis were compared.
US-Guided and Monitor PMC
Before PMC, Twenty VX2 tumor-bearing rabbits were also observed by color Doppler ultrasonography as described above. The tumors in the control group (ten) and the experimental group (ten) were also observed by color Doppler ultrasonography as described above. Subsequently, US-guided PMC was performed in randomly assigned ten VX2 tumor-bearing rabbits (the other ten as controls). During the microwave ablation procedure, conventional grayscale US was also used for real-time monitoring. Following multiple US scans, microwave ablation was performed percutaneously under real-time ultrasound guidance using Microwave Ablation System equipment (MTC-3) (Qinghai Microwave Research Institute of Nanjing Qiya Medical Equipment Co., Ltd., Nanjing, China). The same ultrasound system used for tumor US imaging was applied in the ultrasound-guided process of VX2 tumor ablation.
Prior to microwave ablation, the rabbits were anesthetized by the procedure described for tumor implantation and were positioned supine on the examination table Guided with ultrasound imaging, the water-cooled microwave antenna (1.9 mm in diameter) was inserted into the tumor along the long axis until it reached the center of the lesion and penetrated the lesion, and the microwave antenna was fixed. After testing the cold water (4°C) cycling system, the power supply and circulating water pump of the PMC therapeutic apparatus were turned on; the microwave output power was set at 25~40 according to tumor size. The ablation was started under real-time US monitoring. The PMC procedure lasted for one to two minutes to eradicate the entire tumor according to the tumor size and blood supply of the lesion as well as our own experience. Two temperature needles were placed parallel to the surface of the tumor. For larger tumors, two or more microwave antenna ablations were administered to avoid incomplete ablation. Once the temperature reached 60°C, microwave ablation was stopped immediately to avoid skin burns.
After completing US-guided PMC, the antenna was removed, and the incision was closed. US scanning was performed immediately to determine the US signal characteristics of the ablation lesions. After that, lesions were followed at one and four weeks after treatment using ultrasound.
Therapeutic Evaluation by US After PMC
After PMC, all rabbits were monitored for 2–3 months, and tumor sizes were recorded and compared before and after treatment. Likewise, local changes in coagulated tumors and histopathology as well as the severity of scalds on the skin were observed. The tumor size and survival rate of animals in the treatment group and the control group were observed and recorded simultaneously. The relative tumor volume, survival rate and tumor metastasis rate were applied to assess the therapeutic effect between the two groups. For tumor metastasis, after PMC treatment, metastasis in the axillary lymph nodes or one of the viscera was considered tumor metastasis.
Histopathological Examination
The animals were autopsied within six hours after death. The tissue specimens were fixed in 10% formalin solution, embedded in paraffin, sectioned into 4-μm-thick slices, and stained with H&E. The histological slides were evaluated by two experienced pathologist.
Statistical Analysis
Statistical analysis was conducted employing SPSS 26.0 software packages. Numerical data are reported as the mean ± standard deviation. Comparisons between groups were performed using t-test. Differences were considered statistically significant at P < 0.05. All statistical tests were two-tailed.
Results
General Aspects
The rabbit VX2 breast transplantation tumor model was successfully constructed (Figure 1h). Meanwhile, microwave coagulation was successfully performed on the treated group. However, the volume of one tumor was significantly increased one week after PMC treatment, and the value significantly deviated from the data of the whole group, so data related to this tumor were excluded from the group for separate discussion when comparing the mean tumor volume before and after treatment. The volume of the remaining 9 tumors gradually decreased. No other immediate adverse effects occurred in any of the rabbits.
 |
Figure 1 Ultrasound and pathology characteristics of representative rabbit VX2 breast carcinoma. (a) The tumor was unevenly hypoecho with unsharp margin using conventional gray-scale US at one week of transplantation. (b) Calcification lesions was detected at the 2nd to 3rd weeks of transplantation. (c and d) Swollen lymphonodi axillares was found, necrosis or liquefaction appeared and the cavum formed at the 5th ~6th week. (e) The tumor cells were nest-arranged and invaded the normal breast parenchyma in HE staining (×400). (f) Calcification foci within the tumor was found in HE staining (×100). (g) Metastatic lymph nodes under the axilla was found in HE staining (×100). (h) Macroscopic appearances of rabbit VX2 breast carcinoma. |
US Imaging Characteristics of VX2 Tumors
For two-dimensional US imaging, at 1 week, the tumor was approximately 1 cm in size, round-like, with clear boundaries and relatively homogeneous hypoechoic nodules (Figure 1a). At 2~3 weeks, the tumor volume increased significantly (Figure 2), the tumor growth rate was 463.09%, and the echo distribution inside the tumor was not uniform, with calcified lesions seen inside the tumor (Figure 1b). At 3~4 weeks, the tumor continued to grow, with necrosis or liquefaction found. Enlarged lymph nodes could be detected under the axilla of the affected side of two rabbits after 4 weeks (Figure 1c). At 5~6 weeks, large necrotic liquefaction foci with cystic formation could be seen in the center of the transplanted tumor (Figure 1d).
 |
Figure 2 Graph of tumor volume growth of rabbit VX2 breast carcinoma after transplantation. |
For color Doppler US imaging, the tumor blood supply was graded according to the Adler method: 1 week, the blood supply in and around the tumor was grade 0~I; the blood supply in and around the tumor was grade II~III at 2~3 weeks (Figure 3a and b); and the blood supply in and around the tumor was grade I~II at 3~4 weeks. The blood supply of the tumor was mostly from the artery (Figure 3c). The PSV and RI values of artery were 6.02~39.8 cm/s and 0.186~0.622, respectively. Concomitant veins could also be detected inside some tumors (Figure 3d).
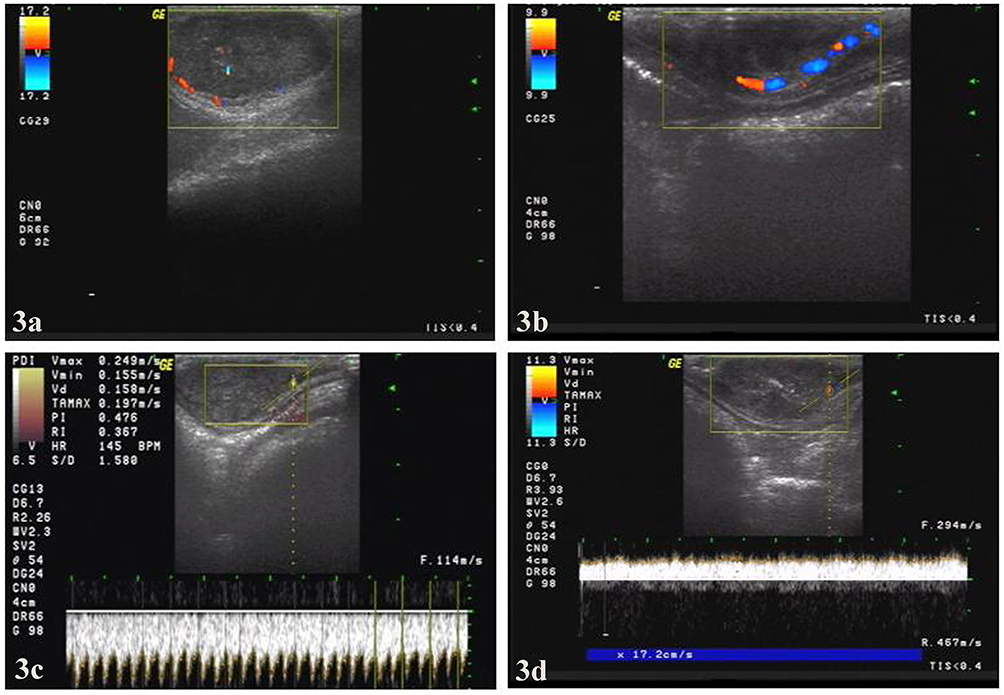 |
Figure 3 Hemodynamic characteristic of representative rabbit VX2 breast carcinoma. (a and b) CDFI indicates short rod-like blood stream signals in the peripheral area of the tumor. (c and d) Doppler US indicates the arterial and venous blood flow spectrum within the tumor. |
US Imaging Evaluation of PMC
Before PMC, the breast lesions presented as hypoechoic masses with little peripheral blood flow (Figure 4a). Intraoperative and postoperative VX2 tumor US images were also simultaneously captured. Under the guidance of real-time US imaging, the microwave antenna was successfully placed in the center of the tumor (Figure 4b). During the ablation procedure, a hyperechoic region appeared around the antenna (Figure 4c and d), visualized by intraprocedural grayscale ultrasound, which was considered to be a result of the inertial cavitation caused by the high energy of microwaves. Immediately following ablation, the strong echo in the coagulation area of the mass gradually dissipated, and only the central punctured strong echo remained, showing heterogeneous hypoecho and scattered punctured strong echo in the center. In 2 cases, there was a small dark area without echo in the center of the coagulation area, which indicated necrosis and liquefaction of the tumor (Figure 4e). For those lesions that required 2 microwave coagulations, the margin between the coagulated area and the unaffected tissue was differentiated and sharp (Figure 4f). In addition, the sonographic findings were also different according to the treatment sequence. When the coagulation area of the first PMC treatment had gradually dissipated (Figure 4g), most of the coagulation area of the second PMC treatment was still covered by a strong echo. Immediately after PMC therapy, ablated regions in 5 rabbits were detected without blood flow signals on CD US and PD US. Moreover, CDFI and PD US demonstrated no residual vessels in periphery ablated areas one week and four weeks after PMC.
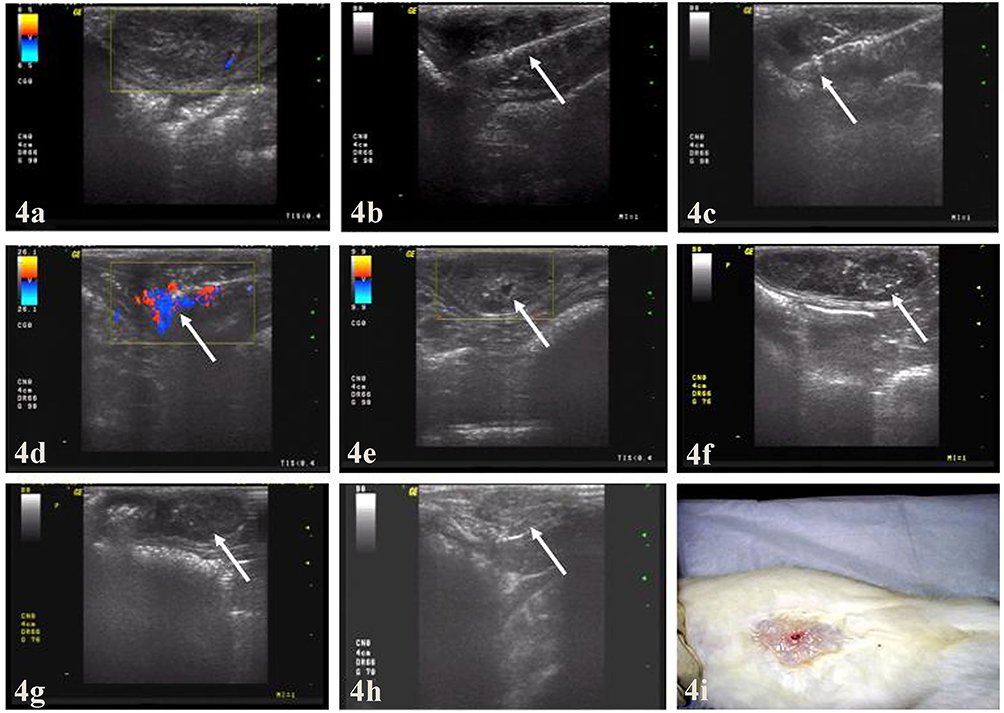 |
Figure 4 Ultrasound images from representative rabbit VX2 breast carcinoma before, during and after PMC therapy. (a)Sonogram shows hypoechoic nodule with clear margin and CDFI showing blood flow signal around nodule before PMC therapy. (b) Longitudinal sonogram shows centrally placed antenna (arrow) in the tumor. (c) Sonogram shows increased echogenicity of the tumor (arrow) near the irradiating segment of the antenna at the beginning of PMC session. (d) CDFI during PMC: heat energy (arrow). (e) Half an hour after PMC, sonogram shows diffusely coarse hyperechogenicity with anechoic dark area (arrow) in the ablated areas and no residual vessels were depicted. (f) Sonogram shows a gradual and diffuse increase in the echogenicity of the tumor from the irradiating segment (arrow) compared with non-PMC session with a clear boundary. (g) Sonogram shows the ablated area still with increased echogenicity covering, while increased echogenicity in the first PMC session (arrow) gradually dissipating in the same tumor. (h) Image obtained four weeks after microwave therapy: most part of the ablated tumor (arrow) was absorbed; (i) Representative photographs from coagulated VX2 tumor eight weeks after microwave therapy: the ablated tumor was absorbed completely to nonpalpable. |
Tumor Growth Inhibition
The in vivo tumor eradication effect was evaluated by measuring and comparing the VX2 xenograft volumes of PMC-treatment and the control group. Before treatment, Tumors in the experimental group had a pretreatment volume of 6.3922±5.7492, with no significant difference in size compared with those in the control group. Except for one case that was not completely inactivated due to oversize, the other nine tumors began to decrease 2 weeks after treatment, while the tumors in the control group increased significantly. As the Figure 5 showed, the average tumor volume of the experimental group was smaller than that of the control group during the same period, with a significant difference (P<0.05) from 2 weeks after treatment. Tumor eradication was achieved in eight rabbits (80%) without any evidence of tumor recurrence and metastasis four weeks after PMC. After 4 weeks of treatment, there was a statistically significant difference in the tumor volume between the PMC group (Figure 4h) and the control group (p<0.05). The tumor volume of 10 rabbits in the control group increased continuously, and the maximum tumor volume reached 869.809 cm3 at the time of death. Interestingly, with efficient microwave ablation, some tumors in the experimental group became completely nonpalpable (Figure 4i) and undetectable by US and histological examinations.
 |
Figure 5 Graph of tumor volume of rabbit VX2 breast carcinoma after treatment showed that the average tumor volume in the PMC-treated group was smaller than that of the control group from 2 weeks after treatment (P<0.05). |
Survival Times of Rabbits With VX2 Breast Solid Tumor Implants
For survival time, all rabbits in the control group died within 3 months, and the 3-month survival rate was 0%. The shortest survival time was 28 days, the longest was 63 days, and the average survival time was 42.400±10.102 days. In contrast, during this period, 7 of the 10 rabbits in the experimental group survived, with a survival rate of 70% at 3 months. The survival time of rabbits in the experimental group after 3 months was assessed until most of them died, ending the experiment. At the end of the experiment, the shortest survival time of animals in the therapy group was 43 days, and the longest was 125 days. Survival analysis showed that rabbits in the PMC group had a significantly higher survival rate than those in the control group (P<0.05) (Figure 6a). Although there was no tumor shrinkage after PMC treatment in one experimental animal, the survival time of rabbits in the experimental group was 64 days longer than the longest survival time of rabbits in the control group. Even the excluded rabbits in the experimental group had a survival time of 64 days, which exceeded the maximum in the control group.
 |
Figure 6 Graph of animal survival and tumor metastasis rate. (a and b) Graph of survival analysis and metastasis rate showed that rabbits in the PMC-treated group had a significantly higher survival and lower rates of tumor metastasis than those in the control group (P<0.05). |
Tumor Metastasis and the Metastasis Rate
After one month of follow-up, the vast majority of tumor metastases were mainly detected in the lung and lymph nodes and occurred in 20% of the rabbits in the non-PMC group, whereas no incidence of lung metastasis or lymph metastasis was found in the PMC group. After two months of follow-up, the rate of tumor metastasis increased to 90% in the control group, while only one of the 10 rabbits in the experimental group showed metastasis. When the experiment ended three months later, a lower metastasis rate was shown in the PMC group than in the control group (30% vs 100%). Obviously, there were significant differences in the tumor metastasis rates between the two groups (P<0.05) (Figure 6b). Moreover, the remaining 7 tumor-bearing rabbits in the treatment group had complete tumor necrosis and exfoliation, and no lymph node metastasis was found in the axilla.
Furthermore, no abnormal behaviors or mortality were observed in rabbits over the course of the experiment, indicating the safety of US-guided PMC in the VX2 rabbit breast cancer model.
Pathological Evidence
The light microscopic appearance with HE staining before ablation in the rabbit breast VX2 tumor is shown in Figure 1e–h. The tumor cells with large hyperchromatic nuclei were nest-arranged and had no distinct boundary with the surrounding breast tissue. In particular, at high magnification, the cytoplasm of cancer cells is abundant, and nuclear division is more common (Figure 1e). In addition, the presence of calcification and axillary lymph nodes during tumor growth is clearly observed (Figure 1f and h).
Half an hour after PMC, the tumor cells in the area along the needle passage developed coagulative necrosis under the microscope, while the tumor cells along the coagulation area around the needle passage showed nuclear shrinkage and no obvious necrosis (Figure 7a). At 1 week, the tumor cells in the coagulation area were necrotic with a small amount of peripheral fibrous tissue hyperplasia (Figure 7b). At 4 weeks, the tumor cells were largely necrotic, and the granulation tissue and fibrous tissue had proliferated (Figure 7c).
 |
Figure 7 Histopathological findings after PMC therapy determined by HE staining. (a) Coagulation necrosis was found in the center of the cancer nest (×200). (b and c) Photomicrographs from coagulated VX2 tumor and viable tumor stained with H & E at week one and week four (×100). (d) Macroscopic appearances of the lungs with metastatic nodules. (e) Metastatic nodules demonstrated by HE staining (×400). |
Autopsy Findings
The autopsy results of rabbits that died of natural causes and rabbits that were euthanized humanely showed that in the experimental group, two rabbits had both axillary lymph node metastasis and pulmonary metastasis, and one rabbit only had axillary lymph node metastasis. In comparison, lymph node metastases were observed in the axilla of all 10 control rabbits, and one or more obvious tumor metastases were observed in the lungs, liver and abdominal cavity, especially in the lungs (Figure 7d). The above results were confirmed by pathology (Figure 7e).
Discussion
At present the commonly used methods in breast cancer treatment and researches have distinct advantages but there are still some disadvantage. As a commonly used thermotherapy, MWA has its own advantages in both research trials and clinical application. Related research has confirmed MWA is relatively effective in treating smaller breast tumours. Y Ji and Zhou W et al found MR-guided PMC of small breast tumors is feasible and could be applied in clinical practice in the future.21,22 In this study, the rabbit breast VX2 transplantation cancer model was successfully constructed using tumor block transplantation, and the whole course of breast tumor growth and lymphatic metastasis was dynamically monitored using US imaging. This was a suitable model used to test the effects of PMC on rabbits exhibiting breast tumors. In view of the characteristics of the thin abdominal wall and subcutaneous growth of VX2-transplanted breast cancer in rabbits, we utilized high-frequency color Doppler ultrasound to dynamically monitor tumor growth and detect tumor blood supply before and after treatment as well as aid in the positioning of microwave delivery systems during operation. Our results demonstrated that US imaging plays a key role in tumor growth monitoring, imaging guidance and treatment evaluation. The blood supply of the tumor is an important condition for the survival of the tumor and an important observation index to evaluate whether the tumor has been completely eliminated.
Studying and characterizing tumor hemodynamic parameters along with monitoring tumor growth prior to microwave ablation are beneficial for subsequent therapy, which provides not only an optimal intervention time reference for US-PMC but also essential data for predicting therapeutic response post‐PMC.23 By continuous observation of tumor growth, we found that the 2nd~3rd week after tumor implantation is suitable for making tumor models, passaging tumors, performing experimental studies on tumor vessels or researching interventional therapy because of the fast tumor growth and rich vasculature in this phase. Based on the above dynamic ultrasonic monitoring data, we chose the 2nd~3rd week after tumor implantation to carry out US-guided PMC and thus achieved relatively satisfactory therapeutic effects. In another study, the volume of tumors measured via US was proven to be more accurate and required ~30% fewer animals to reach statistical significance when compared to standard caliper measurements in preclinical xenograft models.24 As a commonly used image guidance method, real-time US imaging was also applied to accurately guide the microwave antenna to the target area during PMC in this study. It is clear that such visualization of the antenna distribution by US holds great promise in minimizing side effects and maximizing therapeutic efficacy. In addition, the intraoperative ultrasound image vividly demonstrated the whole process of microwave coagulation treatment. Due to the thermal effect of microwaves during the operation, the tumor tissue solidification area showed echogenicity enhancement on the two-dimensional sonogram. The echo enhancement is mainly the result of the acoustic reflection produced by the bubble due to the rising temperature. Combined with the color blood flow diagram, the effective radiation range and location can be further displayed. Therefore, 2D sonograms combined with CDFI and/or PDI can be used to monitor intraoperative changes in real time and to judge the immediate response to treatment.25 The findings of intraoperative imaging are becoming increasingly significant to ensure complete ablation. Furthermore, under the guidance of real-time ultrasound, the water-cooled antenna was precisely placed in the center of the tumor, and percutaneous microwave coagulation therapy was successfully performed, which was proven safe and efficient in increasing tumor necrosis, prolonging animal survival time and reducing tumor metastasis.
In the present study, complete ablation was also assessed according to the results of the postablation US. During the whole process of PMC treatment, the changes in the effective sonogram showed that the echo of the tumor nodules was enhanced and then gradually decreased, with uneven internal echogenicity or liquefaction. The tumor volume was reduced, and CDFI showed decreased or absent color blood flow around or inside the tumor. US was used to monitor tumor growth weekly, and power Doppler US images at 0 min, 24 h and 48 h following PMC were collected, providing evidence of the PMC efficacy. Our results showed that the diameter of PMC-treated tumors was significantly smaller than that in the control group (P<0.05), and no blood supply was detected by high-frequency US, implying that tumor growth in the experimental group was well suppressed. Apart from the above decreases in tumor diameter and the disappearance of tumors in the PMC group, taking the end-point survival time, survival and metastasis rate into account, significant differences in animal end-point survival were identified for the treatment group over the nontreatment group. The PMC group had a significantly longer survival than the control group (P<0.05). The prolonged survival time and lower metastasis rate were relevant to the inhibition of tumor growth, implying complete ablation. Although our results are encouraging, regarding tumor growth inhibition, one VX2 xenograft tumor showed significant growth one week after treatment due to its large volume before treatment, suggesting that larger lesions had a lower chance of disappearance after treatment because of incomplete ablation. One possible explanation could be that in larger lesions, the fiber usually lies within the lesion, which can limit the diffusion of heat, leading to an uneven distribution of energy during the treatment.26 Therefore, even the multineedle combination could not completely inactivate the tumor, and the residual tumor cells caused tumor recurrence. Additionally, the larger the lesion is, the more likely it is to be adjacent to other structures, such as the skin, nipple, chest wall or pectoral fascia; thus, to avoid injury to these normal tissues, the ablation range was set at a low level, which decreases the efficacy of the treatment. Accordingly, a large size should be excluded to attain complete ablation with a relatively low output power. However, even if the tumor was not completely ablated, the rabbit survived for 64 days, exceeding the maximum in the control group. Furthermore, no abnormal behaviors or procedure-related mortality were observed in rabbits over the course of the experiment, indicating the safety of US-mediated microwave coagulation therapy. After PMC, the tumor size was significantly reduced or even disappeared compared with the control group, and the loss of tumor blood supply confirmed the good effect of microwave coagulation. Based on these observations, US imaging displayed feasibility, accuracy and reproducibility in identifying VX2 breast xenografts in rabbits and assessing tumor treatment response after PMC. Similarly, Ramaswamy et al also demonstrated that US imaging has similar accuracies as low‐field magnetic resonance imaging (MRI) in determining tumor volume and growth. Additional pathologic findings of this study also verified efficient tumor coagulation caused by PMC.27
Notably, several limitations still existed in the present study. First, it was limited by the small sample size, the relatively short follow-up period and a single type of breast pathology included. Second, although CDFI and PDI mode were performed to monitor the long-term treatment efficacy of the coagulated tumors by detecting residual vessels after ablation, they were sometimes limited by the conditions of the depth and speed of blood flow, while contrast-enhanced US imaging using a microbubble contrast agent could overcome the above shortcoming and was more sensitive to detecting residual vessels after microwave ablation not found by conventional CD US and PD US.28,29 Therefore, to ensure that the tumor is coagulated more thoroughly, contrast-enhanced US should be introduced as a vital and accurate modality to determine whether the whole tumor is ablated in the future. Third, large animal breast tumor models are limited. Whether there is a similar therapeutic effect in other animal models remains to be determined. Finally, more recent studies have identified that PMC alone is insufficient to defeat breast tumors. Accumulating evidence suggests that combining PMC with adjuvant chemotherapy or other locoregional techniques has the potential to be effective in antitumor therapy over PMC alone.9,30,31 Future studies will be required to validate combination therapy involving PMC, thereby resulting in obvious complementarity and synergistic anticancer benefits.
Our study has several limitations. First, the sample size was small and we cannot avoid bias caused by small sample size. Second, long-term follow-up is lacking and this make it difficult to obtain information on local tumor recurrence. Third, there is still room to improve US guidance and monitoring to better delineate the margin of ablation and to assure complete tumor destruction. If further improvement is made, this advanced technique is hopeful to be universally introduced to actual clinical practice as an alternative treatment for traditional surgical procedures for breast cancer.
Conclusions
US-guided PMC was confirmed to be a safe, effective and feasible nonsurgical minimally invasive method for combating transplanted breast tumors. In this method, microwaves are used to cause coagulative necrosis of the lesion, which leads to shrinkage of the mass or even its disappearance. It has the potential to be considered a feasible alternative option for conventional surgical resection in the future. Nevertheless, larger-scale clinical trials are still needed to validate PMC for adoption into standard clinical practice.
Funding
This work was supported by the Medical Research General Projects of Jiangsu Provincial Health Commission of China (M2021022).
Disclosure
The authors declare that they have no conflicts of interest.
References
1. Arnold M, Morgan E, Rumgay H, et al. Current and future burden of breast cancer: global statistics for 2020 and 2040. Breast. 2022;66:15–23. doi:10.1016/j.breast.2022.08.010
2. Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, Jemal A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2018;68(6):394–424. doi:10.3322/caac.21492
3. Knuttel FM, van den Bosch MA, Young-Afat DA, et al. Patient preferences for minimally invasive and open locoregional treatment for early-stage breast cancer. Value Health. 2017;20(3):474–480. doi:10.1016/j.jval.2016.10.013
4. Peek MC, Ahmed M, Napoli A, et al. Systematic review of high-intensity focused ultrasound ablation in the treatment of breast cancer. Br J Surg. 2015;102(8):873–882. doi:10.1002/bjs.9793
5. Kucharczyk MJ, Parpia S, Walker-Dilks C, Banfield L, Swaminath A. Ablative therapies in metastatic breast cancer: a systematic review. Breast Cancer Res Treat. 2017;164(1):13–25. doi:10.1007/s10549-017-4228-2
6. Ward RC, Lourenco AP, Mainiero MB. Implementing breast cryoablation in practice. J Breast Imaging. 2020;2(1):61–66. doi:10.1093/jbi/wbz077
7. Zhang W, Jin ZQ, Baikpour M, et al. Clinical application of ultrasound-guided percutaneous microwave ablation for benign breast lesions: a prospective study. BMC Cancer. 2019;19(1):345. doi:10.1186/s12885-019-5523-6
8. Yang Q, Li H, Chen BH, et al. Ultrasound-guided percutaneous microwave ablation for 755 benign breast lesions: a prospective multicenter study. Eur Radiol. 2020;30(9):5029–5038. doi:10.1007/s00330-020-06868-9
9. Roknsharifi S, Wattamwar K, Fishman MDC, et al. Image-guided microinvasive percutaneous treatment of breast lesions: where do we stand? Radiographics. 2021;41(4):945–966. doi:10.1148/rg.2021200156
10. Healthcare Engineering JO. Retracted: percutaneous microwave coagulation therapy: a promising therapeutic method for breaking the barrier of the intertumor heterogeneity. J Healthc Eng. 2023;2023(1):9841702. doi:10.1155/2023/9841702
11. Cai H, Tian H, Wei Z, Ye X. Microwave ablation of the lung: comparison of 19G with 14G and 16G microwave antennas in ex vivo porcine lung. J Cancer Res Ther. 2022;18(7):1876–1883. doi:10.4103/jcrt.jcrt_1124_22
12. Li J, Tao HS, Li J, et al. Effect of severity of liver cirrhosis on surgical outcomes of hepatocellular carcinoma after liver resection and microwave coagulation. Front Oncol. 2021;11:745615. doi:10.3389/fonc.2021.745615
13. Li H, Lin Z, Chen J, Guo R. Evaluation of the MR and pathology characteristics immediately following percutaneous MR-guided microwave ablation in a rabbit kidney VX2 tumor implantation model. Int J Hyperthermia. 2019;36(1):1197–1206. doi:10.1080/02656736.2019.1687944
14. Zhou W, Zha X, Liu X, et al. US-guided percutaneous microwave coagulation of small breast cancers: a clinical study. Radiology. 2012;263(2):364–373. doi:10.1148/radiol.12111901
15. Ortega-Palacios R, Trujillo-Romero CJ, Cepeda Rubio MFJ, et al. Feasibility of using a novel 2.45 GHz double short distance slot coaxial antenna for minimally invasive cancer breast microwave ablation therapy: computational model, phantom, and in vivo swine experimentation. J Healthc Eng. 2018;2018:5806753. doi:10.1155/2018/5806753
16. Pascale F, Pelage JP, Wassef M, et al. Rabbit VX2 liver tumor model: a review of clinical, biology, histology, and tumor microenvironment characteristics. Front Oncol. 2022;12:871829. doi:10.3389/fonc.2022.871829
17. Dou Z, Lu F, Ren L, Song X, Li B, Li X. Efficacy and safety of microwave ablation and radiofrequency ablation in the treatment of hepatocellular carcinoma: a systematic review and meta-analysis. Medicine. 2022;101(30):e29321. doi:10.1097/MD.0000000000029321
18. Wang Z, Zuo T, Lin W, Du Z, Zhang X, Liang Y. Clinical efficacy and safety of microwave ablation combined with percutaneous osteoplasty for palliative treatment in pelvic osteolytic metastases. Br J Radiol. 2024;97(1155):553–559. doi:10.1093/bjr/tqad049
19. Zhang HL, Yu SY, Li XL, et al. Efficacy and safety of percutaneous microwave ablation for adenomyosis in the posterior uterine wall. Br J Radiol. 2023;96(1151):20211301. doi:10.1259/bjr.20211301
20. Che D, Yang Z, Wei H, Wang X, Gao J. The Adler grade by Doppler ultrasound is associated with clinical pathology of cervical cancer: implication for clinical management. PLoS One. 2020;15(8):e0236725. doi:10.1371/journal.pone
21. Ji Y, Zhuo Y, Li T, et al. MR-guided percutaneous microwave coagulation of small breast tumors. Insights Imaging. 2024;15(1):76. doi:10.1186/s13244-024-01645-4
22. Zhou W, Ding Q, Liu X, et al. Percutaneous microwave coagulation for eradication of VX2 tumors subcutaneously in rabbits. World J Surg Oncol. 2012;10:97. doi:10.1186/1477-7819-10-97
23. Yi H, Cai B, Ai X, Li K, Song P, Zhang W. Early identification of residual tumors following microwave ablation using contrast-enhanced ultrasonography in a rabbit VX2 liver cancer model. Biomed Res Int. 2020;2020:2462058. doi:10.1155/2020/2462058
24. Ayers GD, McKinley ET, Zhao P, et al. Volume of preclinical xenograft tumors is more accurately assessed by ultrasound imaging than manual caliper measurements. J Ultrasound Med. 2010;29(6):891–901. doi:10.7863/jum.2010.29.6.891
25. Li S, Tsui PH, Song S, Wu W, Zhou Z, Wu S. Detection of microwave ablation coagulation areas using ultrasound Nakagami imaging based on Gaussian pyramid decomposition: a feasibility study. Ultrasonics. 2022;124:106758. doi:10.1016/j.ultras.2022.106758
26. Zhang Z, Hou M, Liu T, et al. Microwave assisted preparation of a hemostatic gauze with mesoporous silica through in-situ synthesis. J Biomater Appl. 2023;37(6):1102–1111. doi:10.1177/08853282221126574
27. Ramasawmy R, Johnson SP, Roberts TA, et al. Monitoring the growth of an orthotopic tumour xenograft model: multi-modal imaging assessment with benchtop MRI (1T), high-field MRI (9.4T), ultrasound and bioluminescence. PLoS One. 2016;11(5):e0156162. doi:10.1371/journal.pone.0156162
28. Ma S, Ding M, Li J, et al. Ultrasound-guided percutaneous microwave ablation for hepatocellular carcinoma: clinical outcomes and prognostic factors. J Cancer Res Clin Oncol. 2017;143(1):131–142. doi:10.1007/s00432-016-2266-5
29. Zhang W, Li JM, He W, et al. Ultrasound-guided percutaneous microwave ablation for benign breast lesions: evaluated by contrast-enhanced ultrasound combined with magnetic resonance imaging. J Thorac Dis. 2017;9(11):4767–4773. doi:10.21037/jtd.2017.09.132
30. Zhu M, Lin XA, Zha XM, Zhou WB, Xia TS, Wang S. Evaluation of the therapeutic efficacy of sequential therapy involving percutaneous microwave ablation in combination with 131I-hypericin using the VX2 rabbit breast solid tumor model. PLoS One. 2015;10(3):e0120303. doi:10.1371/journal.pone.0120303
31. Kong P, Chen L, Shi X, et al. Microwave ablation combined with doxorubicin enhances cell death via promoting reactive oxygen species generation in breast cancer cells. Diagn Interv Imaging. 2018;99(12):783–791. doi:10.1016/j.diii.2018.06.004
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.