Back to Journals » Journal of Pain Research » Volume 19
Ultrasound-Guided Cervical Vagus Nerve Block for Postoperative Opioid Consumption After Thoracoscopic Lung Surgery: Study Protocol for a Randomized Controlled Trial
Authors Liang J, Yan X, Liang C, Chen S, Wei C ![]() , Wu A
, Wu A ![]()
Received 18 April 2026
Accepted for publication 27 June 2026
Published 9 July 2026 Volume 2026:19 617955
DOI https://doi.org/10.2147/JPR.S617955
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Karina Gritsenko
Jinghan Liang,1,* Xiang Yan,1,* Chen Liang,2 Shuo Chen,3 Changwei Wei,1 Anshi Wu1
1Anesthesia & Operation Center, Beijing Chao-Yang Hospital, Capital Medical University, Beijing Key Laboratory of Precision Translational Medicine in Anesthesiology and Pain, Beijing, People’s Republic of China; 2Department of Medical Statistics, Medieco Group Co., Ltd, Beijing, People’s Republic of China; 3Department of Thoracic Surgery, Beijing Chao-Yang Hospital, Capital Medical University, Beijing, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Anshi Wu, Anesthesia & Operation Center, Beijing Chao-Yang Hospital, Capital Medical University, Beijing Key Laboratory of Precision Translational Medicine in Anesthesiology and Pain, No. 8 Gongti Nanlu, Chao-Yang District, Beijing, 100020, People’s Republic of China, Tel +8610 85231330, Email [email protected] Changwei Wei, Anesthesia & Operation Center, Beijing Chao-Yang Hospital, Capital Medical University, Beijing Key Laboratory of Precision Translational Medicine in Anesthesiology and Pain, No. 8 Gongti Nanlu, Chao-Yang District, Beijing, 100020, People’s Republic of China, Tel +8610 85231330, Email [email protected]
Introduction: Effective analgesia after video-assisted thoracoscopic surgery (VATS) remains challenging, as conventional regional techniques mainly target somatic pain but insufficiently address visceral nociception transmitted via the vagus nerve. Cervical vagus nerve block (CVNB) is a novel ultrasound-guided regional technique that may attenuate vagally mediated visceral pain. However, high-quality randomized evidence on its analgesic efficacy and safety after VATS is lacking. This trial aims to evaluate whether adding CVNB to standard thoracic paravertebral block (TPVB) reduces postoperative opioid consumption in patients undergoing VATS lung resection.
Methods and Analysis: This randomized, double-blind, placebo-controlled trial will enroll adult patients scheduled for elective VATS. Participants will be randomly assigned (1:1) to receive either 5 mL of 0.375% ropivacaine for CVNB (intervention group) or an equal volume of normal saline (placebo group), in addition to standardized TPVB. The primary outcome is cumulative opioid consumption within 24 hours postoperatively, expressed as intravenous morphine milligram equivalents (MME). Secondary outcomes include postoperative pain scores, time to first rescue analgesia, incidence of nausea and vomiting, quality of recovery, and sleep quality after surgery. A total of 110 patients are required to detect a clinically meaningful reduction in opioid consumption.
Ethics and Dissemination: The study was approved by the Ethics Committee of Beijing Chaoyang Hospital (2025-ke-16) and has been registered on www.chictr.org.cn. Results will be disseminated through peer-reviewed journals and academic conferences. This study will be conducted in accordance with the principles of the Declaration of Helsinki.
Trial Registration Number: Chinese Clinical Trial Registry: ChiCTR2500096880.
Keywords: cervical vagus nerve block, CVNB, thoracoscopic lung surgery, protocol, nerve block
Introduction
Lung cancer is the leading cause of cancer-related mortality worldwide, and anatomic lung resection remains the standard curative treatment for early-stage disease.1 Video-assisted thoracoscopic surgery (VATS) has largely replaced open thoracotomy due to its reduced surgical trauma and improved postoperative recovery.2,3 Despite these advantages, moderate-to-severe postoperative pain is still frequently reported during the first 24–48 hours after VATS.4,5 Inadequate analgesia may impair deep breathing and coughing, delay early ambulation, increase pulmonary complications, and prolong hospital stay.6,7 Therefore, effective perioperative analgesia remains a critical component of enhanced recovery after thoracic surgery.8,9
Post-thoracoscopic pain has a complex pathophysiology, involving both somatic and visceral components. Somatic pain is primarily related to intercostal nerve injury and incision trauma, whereas visceral pain arises from pleural and pulmonary manipulation.10 While thoracic paravertebral block (TPVB) is widely accepted as a key component of multimodal analgesia for VATS, its sensory coverage predominantly targets somatic pathways and may not sufficiently block visceral nociceptive input.11–13 This may explain the phenomenon observed in our previous study, where although all participants received TPVB, some patients still experienced moderate-to-severe shoulder and back pain within 24 hours after surgery.4 Visceral afferent fibers from the lung, mediastinum, and pleura travel mainly through the vagus nerve, suggesting that regional techniques modulating vagal transmission may enhance analgesia beyond conventional somatic blocks.14
Cervical vagus nerve block (CVNB) is an ultrasound-guided regional technique that temporarily inhibits vagal conduction at the cervical level.15 Preliminary studies and case series have suggested that CVNB may suppress the cough reflex during awake thoracic procedures, reduce visceral discomfort, and potentially decrease postoperative opioid use. Furthermore, the vagus nerve plays an important role in autonomic regulation, raising the possibility that CVNB may influence perioperative physiological responses in addition to pain transmission. However, existing evidence is limited by small sample sizes, non-randomized designs, and inconsistent methodologies. To date, no adequately powered, randomized controlled trials have evaluated the analgesic efficacy and safety of CVNB in patients undergoing VATS lung resection.
Given the significant contribution of vagally mediated visceral pain to the overall postoperative pain burden and the limitations of current regional analgesic strategies, CVNB may offer an important adjunct to enhance postoperative analgesia and reduce opioid requirements. However, with the increasing adoption of opioid-sparing and opioid-free perioperative pathways after VATS, the incremental clinical value of CVNB remains uncertain. Therefore, adequately powered randomized controlled trials are needed to determine whether CVNB provides clinically meaningful benefits beyond current multimodal analgesic strategies.
We hypothesize that, when combined with standard TPVB and general anesthesia, CVNB can provide superior postoperative analgesia and improve recovery after VATS.
To test this hypothesis, we designed a randomized controlled trial to evaluate the efficacy and safety of CVNB in patients undergoing elective VATS wedge resection, segmentectomy, or lobectomy.
Methods
Study Design
This is a randomized, parallel-group, placebo-controlled trial designed to evaluate whether CVNB reduces postoperative pain and opioid consumption in patients undergoing VATS for lung cancer. Eligible participants scheduled for elective VATS wedge resection, segmentectomy, or lobectomy will be recruited from Beijing Chaoyang Hospital, Capital Medical University, between February 2025 and December 2026. The study protocol has been reviewed and approved by the Ethics Committee of Beijing Chaoyang Hospital, Capital Medical University (approval number: 2025-ke-16), and registered at the Chinese Clinical Trial Registry (ChiCTR2500096880) prior to participant enrollment. Preoperative interview and postoperative follow-up will be conducted by specially trained research assistants. They will inform patients about the study objectives, risks and benefits, and obtain written informed consent from participants. Figure 1 shows the flow chart of the study.
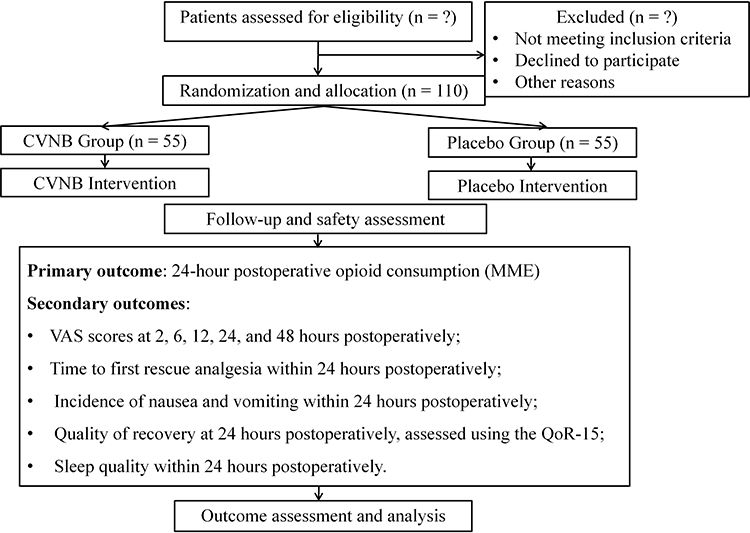 |
Figure 1 Study flow diagram according to the CONSORT 2025 framework. Participants will be screened, randomized, allocated to the CVNB or placebo group, followed for safety and outcome assessment, and included in the planned analyses. Abbreviations: CVNB, cervical vagus nerve block; MME, morphine milligram equivalents; QoR-15, Quality of Recovery-15 questionnaire. |
Population
Inclusion Criteria
On the day before surgery, patients will be screened by a face-to-face visit according to the eligibility criteria. The inclusion criteria include: (1) Adult patients aged 18–65 years with preoperative pulmonary computed tomography diagnosis of lung space-occupying lesions; (2) Patients scheduled to undergo elective thoracoscopic wedge resection, segmentectomy, or lobectomy under general anesthesia.
Exclusion Criteria
Patients will be excluded if they have any of the following exclusion criteria: (1) American Society of Anesthesiologists (ASA) physical status >III; (2) body mass index ≥35 kg/m2; (3) pregnancy and lactation; (4) Known allergy to anesthetic agents; (5) history of opioid abuse; (6) regional block anesthesia contraindicated; (7) Expected duration of postoperative mechanical ventilation >6 hours; (8) Refusal to provide written informed consent.
Randomization and Blinding
Participants will be randomly assigned in a 1:1 ratio using a computer-generated block randomization scheme with randomly varying block sizes of 4 and 6, prepared by an independent statistician who is not involved in patient care. Randomization will be stratified by surgical side (left vs right lung). The randomization sequence will be generated by an independent researcher using SPSS version 29.0 (IBM SPSS, Chicago, IL). Then allocation concealment will be ensured using sequentially numbered, opaque, sealed envelopes. Envelopes will be opened only after patient arrival in the operating room and immediately before block preparation by a designated research assistant not involved in outcome assessment. The study medications will be prepared in identical syringes labeled “CVNB medication”. Patients, surgeons, anesthesiologists responsible for intraoperative management, and outcome assessors will remain blinded to group allocation. The effectiveness of blinding will be assessed by asking patients and outcome assessors to guess the group allocation at 24 hours postoperatively.
Interventions
All subjects will undergo a single session of cervical vagus nerve block and thoracic paravertebral nerve block. CVNB: Patients will be placed in the lateral decubitus position. After standard skin disinfection and sterile draping, a high-frequency linear ultrasound transducer (6–13 MHz) will be positioned transversely at the level of the cricoid cartilage (approximately C6 level). The common carotid artery and internal jugular vein will be identified within the carotid sheath. The vagus nerve, typically located between these two structures, will be visualized as a small, hypoechoic, round structure. Using an in-plane technique, a 25-gauge needle will be advanced under real-time ultrasound guidance toward the vagus nerve. After careful negative aspiration, 5 mL of 0.375% ropivacaine (intervention group) or an equivalent volume of normal saline (control group) will be injected into the perineural space surrounding the vagus nerve. Proper spread of the injectate around the nerve will be confirmed by ultrasound visualization. All procedures will be performed by experienced anesthesiologists who have performed at least 50 ultrasound-guided nerve blocks.15,16 TPVB: A low-frequency convex transducer will be placed in a parasagittal orientation to identify the transverse processes and paravertebral space at the T5 level. The ultrasound probe will then be positioned lateral to the spinous processes to visualize the transverse processes and pleura. The thoracic paravertebral space will be identified as the wedge-shaped area between the parietal pleura and the superior costotransverse ligament. Using an in-plane technique, the needle will be advanced under real-time ultrasound guidance toward the paravertebral space. Correct placement will be confirmed by anterior displacement of the pleura after injection. After negative aspiration, a total of 20 mL of local anesthetic solution (50 mg bupivacaine combined with 133 mg liposomal bupivacaine) will be injected at the T5–6 level. All blocks will be performed before induction of general anesthesia (Figure 2A and B).
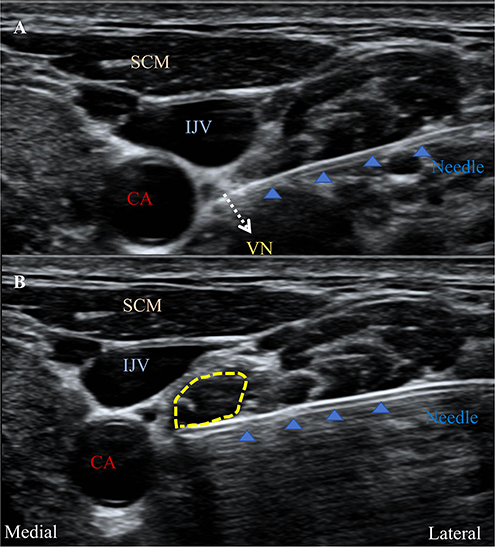 |
Figure 2 Ultrasound-guided cervical vagus nerve block. (A) Identification of the cervical vagus nerve and needle trajectory. The white dotted arrow indicates the location of the vagus nerve. (B) Perineural spread of local anesthetic around the vagus nerve after injection. The yellow dotted line indicates the spread of the local anesthetic. Abbreviations: SCM, sternocleidomastoid muscle; CA, carotid artery; IJV, internal jugular vein; VN, vagus nerve. |
Standard Anesthesia Management
Standard monitoring will include continuous electrocardiography, arterial pressure, heart rate, pulse oxygen saturation, end-tidal carbon dioxide, bispectral index (BIS), and urine output. All patients will be premedicated with intravenous midazolam (0.05 mg/kg) five minutes before anesthesia induction. General anesthesia will be induced with sufentanil (0.3–0.4 µg/kg), propofol (1.5–2.5 mg/kg), and rocuronium (0.6 mg/kg) to facilitate double-lumen tracheal intubation.
After intubation, mechanical ventilation will be performed with a tidal volume of 6–8 mL/kg during two-lung ventilation, and tidal volume is reduced to 4–6 mL/kg during one-lung ventilation, a respiratory rate of 12–20 breaths per minute to maintain normocapnia (PaCO2 35–45 mmHg). Anesthesia will be maintained with total intravenous anesthesia using propofol (3–8 mg/kg/hour) and remifentanil (0.1–0.2 µg/kg/min), targeting a BIS value between 40 and 60. Intraoperative mean arterial pressure will be maintained within ± 20% of the baseline value. Fluid input and urine output will be closely monitored and recorded.
Postoperative analgesia will be provided using a standard PCA containing sufentanil (1.5 µg/kg) and ondansetron (8 mg) diluted to 100 mL with 0.9% saline, with parameters set at a background infusion of 1 mL/hour, a bolus dose of 1 mL, and a lockout interval of 10 minutes. PCA devices are network-connected to automatically record total opioid consumption within 24 hours postoperatively.17 Supplemental tramadol analgesia will be provided when patient-controlled analgesia proves insufficient.
All anesthetic and analgesic procedures will be conducted according to a standardized protocol to ensure consistency across all participants.
Data Collection and Measurement
Table 1 shows data collection at each time point. We will record baseline characteristics including age, gender, weight, medical history, medications, ASA classification, pulmonary function, and sleep quality. All subjects undergo preoperative chest imaging (CT or MRI) to determine lesion location, and extent. During surgery, anesthesiologists will use a standardized case record form to document vital signs, including heart rate, mean arterial pressure, oxygen saturation, end-tidal carbon dioxide pressure, and urine output. Concurrently recorded will be total anesthetic and analgesic drug administration, operative duration, estimated blood loss, fluid replacement volume, transfusion status, and implementation of nerve blocks.
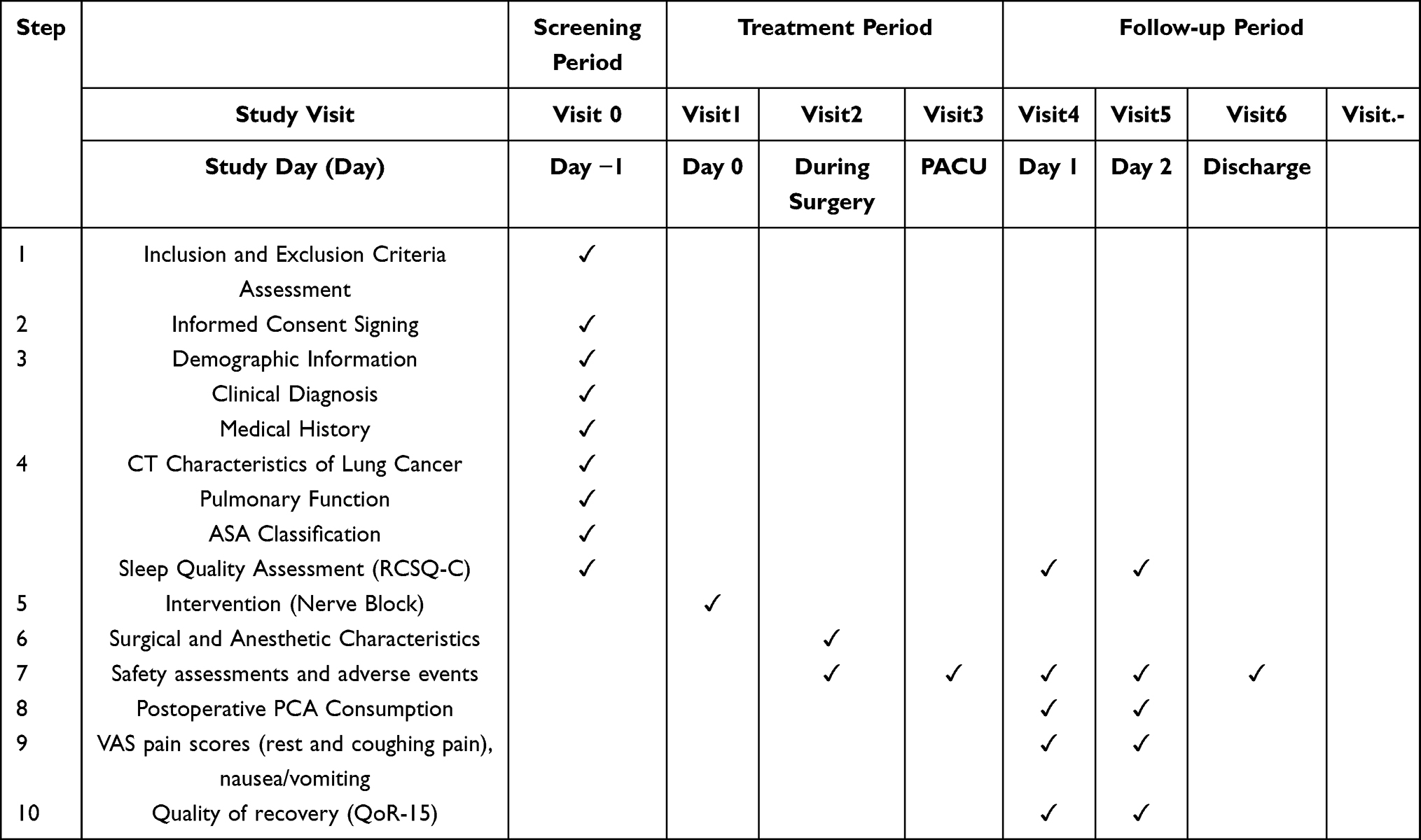 |
Table 1 Data Collection at Each Time Point |
All subjects will be treated with the standardized PCA device stipulated in the protocol until 48 hours after the operation, and the usage of opioid analgesics will be recorded by the electronic analgesic pump. Pain intensity is measured using the VAS at 2, 6, 12, 24, and 48 hours postoperatively. Pain assessments are conducted by uniformly trained investigators while patients are awake and at rest. Additionally, the following will be recorded: time to first rescue analgesia, incidence of postoperative nausea and vomiting, sleep quality (assessed using the Richards-Campbell sleep questionnaire), postoperative recovery quality (assessed using the QoR-15 scale).18,19
To determine the safety of CVNB, we will record the surgery-related complications during and after the operation, and grade the complications, respectively, using the ClassIntra scale and the Clavien-Dindo scale.20 The predefined puncture-related complications include hematoma at the puncture site, allergy to local anesthetics, excessive nerve involvement (Horner’s syndrome or phrenic nerve palsy), and nerve injury. To evaluate the potential effects of vagus nerve blockade on respiratory, digestive, and circulatory systems, we will record intraoperative blood gas analysis, postoperative hypoxemia (oxygen saturation <90% despite supplemental oxygen), and duration of postoperative hoarseness. Time to first flatus and postoperative appetite will also be recorded. Intraoperative and postoperative bradycardia (HR < 60 bpm) within 24 hours, tachycardia (HR > 100 bpm), and new-onset arrhythmias (including atrial fibrillation; ventricular premature beats in couplets or triplets; ventricular fibrillation; atrioventricular block) within 24 hours will be recorded. The postoperative pain and chronic cough of the patients will be followed up on the 30th and 90th days after the operation through the Short-form McGill Pain Questionnaire 2 and the Cough symptom score scale.21,22
Study Objectives
This study aims to investigate the effect of CVNB on postoperative pain in patients undergoing thoracoscopic lung resection. We hypothesize that CVNB can reduce postoperative opioid consumption within 24 hours after surgery.23 In addition, the feasibility and safety of CVNB will be evaluated.
Primary Outcome
Opioid consumption within 24 hours postoperatively, expressed as intravenous morphine milligram equivalents (MME).
Secondary Outcomes
- VAS scores at 2, 6, 12, 24, and 48 hours postoperatively.
- Time to first rescue analgesia within 24 hours postoperatively.
- Incidence of nausea and vomiting within 24 hours postoperatively.
- Quality of recovery at 24 hours postoperatively.
- Sleep quality during 24 hours postoperatively.
Other Pre‑specified Outcomes
- Incidence of intraoperative and postoperative complications.
- Length of post-anesthesia intensive care unit stay.
- Length of hospital stay.
All administered opioids, including sufentanil delivered via the PCA device and rescue tramadol, will be recorded and converted to MME using standard equianalgesic conversion factors. Both background infusion and patient-controlled bolus doses will be included in the total opioid consumption.
Data Monitoring Committee
The study will be overseen by an independent Data Monitoring Committee consisting of experts in anesthesiology, thoracic surgery, medical ethics, biostatistics, and clinical methodology. The Data Monitoring Committee will conduct periodic reviews through on-site assessments or teleconferences, ensuring the integrity and safety of the trial. In the event of any serious adverse event or safety concern, the committee will have the authority to recommend modification or early termination of the study.
Statistical Analysis Plan
All statistical analyses will be performed according to a predefined statistical analysis plan using SPSS software (version 29.0 or later; IBM Corp., Chicago, IL, USA). A two-sided P value <0.05 will be considered statistically significant. The primary analysis will follow the modified intention-to-treat (mITT) principle, including all randomized patients who undergo VATS surgery. A per-protocol analysis will also be conducted as a sensitivity analysis. Continuous variables will be assessed for normality using the Shapiro–Wilk test. Normally distributed data will be presented as mean ± standard deviation and compared using the independent-samples t-test; non-normally distributed data will be presented as median (interquartile range) and compared using the Mann–Whitney U-test. Categorical variables will be expressed as frequencies and percentages and compared using the χ2-test or Fisher’s exact test as appropriate. For the primary outcome, the between-group difference in 24-hour MME will be reported as mean difference with 95% confidence intervals. If the distribution of opioid consumption remains substantially skewed after assessment of normality, non-parametric analyses will be used as the primary comparison method. Repeated measures outcomes, such as VAS, will be analyzed using a linear mixed-effects model with group, time, and group-by-time interaction as fixed effects, and subject as a random effect. Time-to-event outcomes (eg, time to first rescue analgesia) will be analyzed using Kaplan–Meier methods and compared using the Log rank test. Hazard ratios with 95% confidence intervals will be estimated using Cox proportional hazards models. Missing data will be handled using multiple imputation under the assumption of missing at random. Sensitivity analyses will be performed to assess the robustness of the results. Predefined subgroup analyses will be conducted based on sex, surgical side (left vs right), extent of resection (wedge resection, segmentectomy or lobectomy), and duration of anesthesia. Interaction tests will be performed to assess heterogeneity between subgroups.
Sample Size Calculation
The sample size was calculated for a superiority trial using a two-sided alpha of 0.05 and a power of 80%. Based on our preliminary data, the mean postoperative sufentanil consumption within 24 hours was 35 µg with a standard deviation of 10 µg in the control group. We assumed that the addition of CVNB would result in a 12 µg reduction in postoperative sufentanil consumption, corresponding to an approximate 30–35% reduction. This effect size was considered clinically meaningful based on published evidence regarding the minimal clinically important difference for postoperative opioid consumption.24,25 Accordingly, 46 patients were required per group. Considering a potential dropout rate of 20%, the final sample size was set at 55 patients per group.
Reporting of Adverse Events
All adverse events associated with the trial will be recorded and closely monitored until the patient’s condition has stabilized or it has been confirmed that the event is not related to the CVNB. The principal investigator is responsible for the documentation and reporting of all adverse events. Once an adverse event occurs, it should be immediately reported to the research department and the principal investigator to assess its severity and potential relationship to the study intervention. All serious or unexpected adverse events related to this trial will be reported to the Ethics Committee within 24 hours. In the event of a severe adverse event, the study blind may be broken, and the incident will be reported to the principal investigator, the Ethics Committee, and all participating investigators.
Data Management
All data collected during the study will be treated as strictly confidential and used solely for research purposes. Both paper-based case report forms and electronic data capture systems will be utilized simultaneously for data collection. Participant-related documents will be securely stored in locked cabinets within the Department of Anesthesiology, Beijing Chaoyang Hospital. Electronic data will be maintained on a password-protected research computer, with regular backups performed weekly on an external hard drive to ensure data integrity and security.
Protocol Amendment
The principal investigator will hold overall responsibility for any protocol amendments that may affect participant safety, potential benefits, or the scientific integrity of the study. In the event of any modification, such as changes in study population, sample size, procedures, interventions, outcomes, or statistical analyses, the principal investigator will notify all relevant stakeholders and obtain approval from the China Ethics Committee of Registering Clinical Trials prior to implementation.
Ethics and Dissemination
The study protocol was reviewed and approved by the Ethics Committee of Beijing Chaoyang Hospital, Capital Medical University (approval number: 2025-ke-16). The trial was registered at www.chictr.org.cn (ChiCTR2500096880) on 8 February 2025. Participant enrollment began on 21 February 2025, and the trial is expected to be completed by 30 December 2026. The results of this study will be submitted for publication in peer-reviewed scientific journals and presented at academic conferences. This study will be conducted in accordance with the principles of the Declaration of Helsinki.
Discussion
This randomized controlled trial is designed to evaluate the efficacy and safety of CVNB in reducing postoperative pain and opioid consumption in patients undergoing VATS for lung cancer. Although thoracoscopic surgery reduces surgical trauma compared with open thoracotomy, a significant proportion of patients still experience moderate-to-severe pain within the first 24 hours after surgery. This pain often limits early ambulation and pulmonary rehabilitation, thereby delaying postoperative recovery. Previous studies have suggested that this pain is not only somatic but also visceral in nature, and conventional paravertebral or erector spinae plane blocks may not sufficiently cover visceral afferent fibers. Anatomically, the visceral sensation of the lungs and mediastinum is mainly transmitted via the vagus nerve, providing a rationale for exploring the potential analgesic effect of CVNB in thoracic surgery.
Recent case series have reported that ultrasound-guided CVNB can effectively suppress cough reflex and intraoperative visceral discomfort during awake thoracic surgery, with reduced postoperative opioid use. However, these findings were limited by small sample sizes and lacked randomized controlled evidence. The present trial is therefore designed to fill this gap by rigorously evaluating the analgesic efficacy and safety of CVNB in patients undergoing thoracoscopic lung resection under general anesthesia.
Compared with traditional opioid-based analgesic regimens, CVNB may offer several potential advantages. First, by blocking afferent vagal transmission, CVNB could mitigate visceral pain originating from pleural irritation and mediastinal manipulation, which are common sources of postoperative discomfort. Second, the use of a non-opioid regional technique may reduce opioid-related adverse events such as nausea, vomiting, and delayed recovery. Additionally, the combination of CVNB and TPVB could provide a more comprehensive analgesic coverage for both somatic and visceral pain components following VATS.26
The safety of CVNB is another key focus of this study. Although the vagus nerve is located in close proximity to vital vascular and airway structures, ultrasound guidance allows for accurate visualization and precise injection.27,28 Potential adverse events, such as hoarseness, Horner’s syndrome, or transient bradycardia, have been rarely reported and are generally self-limiting.29 In this study, the block is performed under strict aseptic conditions by experienced anesthesiologists, and all participants are closely monitored intraoperatively and postoperatively to ensure safety.
The outcomes of this trial will provide prospective randomized evidence regarding the efficacy and safety of CVNB in thoracic surgery. If proven effective, this technique may provide a novel and opioid-sparing analgesic option for patients undergoing VATS. The findings may also offer insights into the role of the vagus nerve in modulating thoracic visceral pain and perioperative autonomic function.
Patient and Public Involvement
Patients and members of the public were not directly involved in the development of the research question, study design, or selection of outcome measures for this trial. They were also not involved in participant recruitment, conduct of the study, or interpretation of the results.
After completion of the trial, the findings will be summarized in a peer-reviewed manuscript and shared with study participants through their preferred communication channels provided at enrollment (eg, email, telephone, or written summary). The intervention procedures will be performed entirely by anesthesiologists, and no additional burden or self-administration requirements will be imposed on participants during the study.
Patient Consent for Publication
Consent obtained directly from patient(s).
Acknowledgments
The authors would like to express their sincere gratitude to the colleagues of the Department of Anesthesiology and the Department of Thoracic Surgery, Beijing Chaoyang Hospital, Capital Medical University, for their support and cooperation.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agreed to be accountable for all aspects of the work.
Funding
This work was supported by the National Key Research and Development Program of China (Grant No. 2025YFC3607900).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Ceccarelli I, Durand M, Seguin-Givelet A. The evolving role of wedge resection in early-stage non-small cell lung cancer: a literature review. Transl Lung Cancer Res. 2025;14:4078–10. doi:10.21037/tlcr-2025-562
2. Pan H, Chen H, Kong W, et al. Video-assisted thoracoscopic surgery versus thoracotomy following neoadjuvant immunochemotherapy in resectable stage III non-small cell lung cancer among Chinese populations: a multi-center retrospective cohort study. Clin Lung Cancer. 2024;25:395–406.e5. doi:10.1016/j.cllc.2024.03.008
3. Feray S, Lubach J, Joshi GP, et al. PROSPECT guidelines for video-assisted thoracoscopic surgery: a systematic review and procedure-specific postoperative pain management recommendations. Anaesthesia. 2022;77:311–325. doi:10.1111/anae.15609
4. Yan X, Liang C, Jiang J, et al. Effects of balanced opioid-free anesthesia on post-operative nausea and vomiting in patients undergoing video-assisted thoracic surgery: a randomized trial. BMC Anesthesiol. 2025;25:62. doi:10.1186/s12871-025-02938-x
5. Moorthy A, Ní Eochagáin A, Dempsey E, et al. Postoperative recovery with continuous erector spinae plane block or video-assisted paravertebral block after minimally invasive thoracic surgery: a prospective, randomised controlled trial. Br J Anaesth. 2023;130:e137–e147. doi:10.1016/j.bja.2022.07.051
6. Liu Y, Xiao S, Yang H, et al. Postoperative pain-related outcomes and perioperative pain management in China: a population-based study. Lancet Reg Health West Pac. 2023;39:100822. doi:10.1016/j.lanwpc.2023.100822
7. Kulkarni BK. Evaluation of postoperative pain management in surgical patients. J Contemp Clin Pract. 2025;11:845–852.
8. Zhang M, Cai P. Application on perioperative ERAS concept in elderly lung cancer patients undergoing surgery. Medicine. 2024;103:e36929. doi:10.1097/MD.0000000000036929
9. Makkad B, Heinke TL, Sheriffdeen R, et al. Practice advisory for preoperative and intraoperative pain management of thoracic surgical patients: part 1. Anesth Analg. 2023;137:2–25. doi:10.1213/ANE.0000000000006441
10. Boezaart AP, Smith CR, Chembrovich S, et al. Visceral versus somatic pain: an educational review of anatomy and clinical implications. Reg Anesth Pain Med. 2021;46:629–636. doi:10.1136/rapm-2020-102084
11. Batchelor TJP, Rasburn NJ, Abdelnour-Berchtold E, et al. Guidelines for enhanced recovery after lung surgery: recommendations of the Enhanced Recovery After Surgery (ERAS®) Society and the European Society of Thoracic Surgeons (ESTS). Eur J Cardiothorac Surg. 2019;55:91–115. doi:10.1093/ejcts/ezy301
12. Krediet AC, Moayeri N, van Geffen G-J, et al. Different approaches to ultrasound-guided thoracic paravertebral block: an illustrated review. Anesthesiology. 2015;123:459–474. doi:10.1097/ALN.0000000000000747
13. Zhang L, Hu Y, Liu H, et al. Analgesic efficacy of combined thoracic paravertebral block and erector spinae plane block for video-assisted thoracic surgery: a prospective randomized clinical trial. Med Sci Monit. 2023;29:e940247–1–e940247–11. doi:10.12659/MSM.940247
14. Song N, Liu J, Proctor M, Yu J. Right and left vagus nerves regulate breathing by multiplicative interaction. Respir Physiol Neurobiol. 2015;219:25–29. doi:10.1016/j.resp.2015.07.015
15. Gong W-Y, Yue X-F, Cheng C, Peng T, Fan K. The application of cervical vagus nerve block in the awake video-assisted thoracic surgery for bullectomy. Anaesth Crit Care Pain Med. 2021;40:100823. doi:10.1016/j.accpm.2021.100823
16. Gong W-Y, Zhang J-Y, Wang A-Z, Fan K. The combination of paravertebral block and cervical vagus nerve block applied alone for anesthesia of open appendectomy during COVID-19. Anaesth Crit Care Pain Med. 2022;41:101091. doi:10.1016/j.accpm.2022.101091
17. Wu CL, King AB, Geiger TM, et al. American society for enhanced recovery and perioperative quality initiative joint consensus statement on perioperative opioid minimization in opioid-naïve patients. Anesth Analg. 2019;129:567–577. doi:10.1213/ANE.0000000000004194
18. Chen L-X, Ji D-H, Zhang F, et al. Richards-Campbell sleep questionnaire: psychometric properties of Chinese critically ill patients. Nurs Crit Care. 2019;24:362–368. doi:10.1111/nicc.12357
19. Kleif J, Waage J, Christensen KB, Gögenur I. Systematic review of the QoR-15 score, a patient- reported outcome measure measuring quality of recovery after surgery and anesthesia. Br J Anaesth. 2018;120:28–36. doi:10.1016/j.bja.2017.11.013
20. Dindo D, Demartines N, Clavien P-A. Classification of surgical complications: a new proposal with evaluation in a cohort of 6336 patients and results of a survey. Ann Surg. 2004;240:205–213. doi:10.1097/01.sla.0000133083.54934.ae
21. Dworkin RH, Turk DC, Revicki DA, et al. Development and initial validation of an expanded and revised version of the Short-form McGill Pain Questionnaire (SF-MPQ-2). Pain. 2009;144:35–42. doi:10.1016/j.pain.2009.02.007
22. Zhan W, Zhang L, Jiang M, et al. A new simple score of chronic cough: cough evaluation test. BMC Pulm Med. 2020;20:68. doi:10.1186/s12890-020-1106-1
23. Levy N, Quinlan J, El-Boghdadly K, et al. An international multidisciplinary consensus statement on the prevention of opioid-related harm in adult surgical patients. Anaesthesia. 2021;76:520–536. doi:10.1111/anae.15262
24. Laigaard J, Pedersen C, Rønsbo TN, Mathiesen O, Karlsen APH. Minimal clinically important differences in randomised clinical trials on pain management after total Hip and knee arthroplasty: a systematic review. Br J Anaesth. 2021;126:1029–1037. doi:10.1016/j.bja.2021.01.021
25. Beloeil H, Touihri K, El Haddad C, et al. Effect of opioid-free versus opioid-based strategies during multimodal anaesthesia on postoperative morphine consumption after bariatric surgery: a randomised double-blind clinical trial. BJA Open. 2024;9:100263. doi:10.1016/j.bjao.2024.100263
26. Li S, Feng J, Fan K, et al. The effect of ultrasound-guided intercostal nerve block on postoperative analgesia in thoracoscopic surgery: a randomized, double-blinded, clinical trial. J Cardiothorac Surg. 2023;18:128. doi:10.1186/s13019-023-02210-8
27. Goldsmith A, Driver L, Duggan NM, et al. Complication rates after ultrasonography-guided nerve blocks performed in the emergency department. JAMA Network Open. 2024;7:e2444742. doi:10.1001/jamanetworkopen.2024.44742
28. Turhan Ö, Sivrikoz N, Canbolat N, et al. Ultrasound-guided intermediate versus deep cervical plexus block for carotid endarterectomy: a randomized controlled study. BMC Anesthesiol. 2025;25:581. doi:10.1186/s12871-025-03460-w
29. Goel V, Patwardhan AM, Ibrahim M, et al. Complications associated with stellate ganglion nerve block: a systematic review. Reg Anesth Pain Med. 2019;44:669–678. doi:10.1136/rapm-2018-100127
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.