Back to Journals » Journal of Pain Research » Volume 10
Ultrasound-guided bilateral superficial cervical plexus block is more effective than landmark technique for reducing pain from thyroidectomy
Authors Senapathi TGA ![]() , Widnyana IMG, Aribawa IGNM
, Widnyana IMG, Aribawa IGNM ![]() , Wiryana M
, Wiryana M ![]() , Sinardja IK, Nada IKW, Jaya AAGPS
, Sinardja IK, Nada IKW, Jaya AAGPS ![]() , Putra IGKS
, Putra IGKS ![]()
Received 29 March 2017
Accepted for publication 23 June 2017
Published 14 July 2017 Volume 2017:10 Pages 1619—1622
DOI https://doi.org/10.2147/JPR.S138222
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor E Alfonso Romero-Sandoval
Tjokorda Gde Agung Senapathi, I Made Gede Widnyana, I Gusti Ngurah Mahaalit Aribawa, Made Wiryana, I Ketut Sinardja, I Ketut Wibawa Nada, AA Gde Putra Semara Jaya, I Gede Koko Swadharma Putra
Department of Anesthesiology and Intensive Care, Sanglah Hospital, Faculty of Medicine, Udayana University, Denpasar, Bali, Indonesia
Purpose: Thyroidectomy causes postoperative pain and patient discomfort. Bilateral superficial cervical plexus block is a regional anesthesia technique that can provide analgesia during and after surgery. This study aims to compare the effectiveness of ultrasound (US)-guided versus landmark (LM) technique for bilateral superficial cervical plexus block in thyroidectomy.
Patients and methods: Thirty-six patients undergoing thyroidectomy were divided into two groups randomly (n=18); either US-guided (US group) or LM technique (LM group) for bilateral superficial cervical plexus block. Patient-controlled analgesia was used to control postoperative pain. Intraoperative opioid rescue, postoperative visual analog scale (VAS) score and opioid consumption were measured.
Results: The number of patients who required intraoperative opioid rescue was significantly lower in the US group (p≤0.05). There was no significant difference in postoperative VAS score at 3 hours (p>0.05), but postoperative VAS score at 6 and 24 hours was significantly lower in the US group (p≤0.05). Twenty-four hour postoperative opioid consumption was significantly lower in the US group (p≤0.05).
Conclusion: Ultrasound-guided bilateral superficial cervical plexus block is more effective in reducing pain both intra- and postoperatively compared with landmark technique in patients undergoing thyroidectomy.
Keywords: peripheral nerve block, superficial cervical plexus block, ultrasound-guided, pain, thyroidectomy
Introduction
Thyroidectomy causes mild-to-moderate pain, especially within 24 hours after surgery. Patients may experience discomfort in swallowing, burning sensation in the throat, nausea, and vomiting, which are all caused by the surgical procedures or general anesthesia. Various efforts have been made to prevent and treat these problems, such as administration of opioids and nonsteroidal anti-inflammatory drugs, local anesthesia, or regional anesthesia.1
Bilateral superficial cervical plexus block can reduce intra- and postoperative pain. Bilateral superficial cervical plexus block is a popular regional anesthesia used in thyroidectomy, because of its feasibility and efficacy.1 The procedures can be facilitated by ultrasound guidance or the conventional landmark (LM) technique. Ultrasound (US) guidance provides real-time visualization of anatomical structures and needle movement and has decreased the complication rates.2–4
Shih et al,1 in their study, concluded that bilateral superficial cervical plexus block was effective in reducing the amount of general anesthetic required during thyroidectomy, and lowers the severity of postoperative pain during the first 24 hours. Similarly, Gurkan et al’s4 study also concluded that US-guided bilateral superficial cervical plexus block has a significant analgesic effect in patients undergoing thyroid surgery.
In this study, we tried to compare the effectiveness of US-guided and LM technique for bilateral superficial cervical plexus block in thyroidectomy.
Materials and methods
Patients
This is an experimental study with a randomized controlled trial design. A total of 36 patients with American Society of Anesthesiologists (ASA) physical status I–II undergoing thyroidectomy with general anesthesia in the central operating theater at Sanglah Hospital (Joint Commission International – Accredited) from January through March 2017 were admitted to the study. Patients were not admitted to the study if any the following criteria were present: patient refusal, ASA physical status III or more, contraindications using local anesthetics, local infection at the site of injection, and a history of chronic analgesic use.
Procedures
In the preparation room of central operating theater, intravenous access was obtained and ringer lactate 10 mL/kg intravenously (IV) were administered. In the operating room, the subject received oxygen supplementation 2 L/min through a nasal cannula. They either underwent US-guided (US group) or LM technique (LM group) for bilateral superficial cervical plexus block. Bilateral superficial cervical plexus block was done with a 22G needle, using 10 mL of 0.25% plain bupivacaine on each side of the neck.
In the LM group, we used a three-point injection technique, and 10 mL of 0.25% bupivacaine was injected in each side. A 22-Gauge needle was inserted subcutaneously and immediately deep to the sternocleidomastoid muscle (SCM) at the midpoint of the posterior border of the clavicular head of the SCM. After an aspiration test, an injection of 3 mL local anesthetic (LA) was performed in the cephalic direction along the posterior border of SCM. Then, the needle was reoriented in the medial direction and 4 mL of LA was injected. Finally, 3 mL of LA was injected in the caudal direction along the posterior border of SCM. Deep needle insertion (>1–2 cm) was avoided in order to prevent the block of the phrenic or recurrent laryngeal nerve, and subarachnoid or vertebral artery injection. In US group, the transducer was placed over the lateral side of the neck at the midpoint of the posterior border of the clavicular head of the SCM. The transducer is positioned such that the tapering end (posterior border on the ultrasound image) of the SCM is in the center of the screen. The needle is then introduced from the posterior aspect through the skin and platysma, the needle tip is directed to lie in the space between the SCM and the prevertebral fascia, close to the posterior border of the SCM, and 10 mL of 0.25% bupivacaine was deposited just behind this landmark, using a 22-G needle.
General anesthesia was done in both groups after plexus block. Propofol 2–2.5 mg/kg IV was used as an induction agent. Tracheal intubation was facilitated by 0.5 mg/kg atracurium IV and lidocaine 2 mg/kg intratracheally. General anesthesia was maintained with isoflurane and 60% oxygen mixed with compressed air. The concentration of isoflurane was adjusted to maintain a bispectral index between 40 and 60. Fentanyl 1 mcg/kg IV was administered as opioid rescue if variations in systolic blood pressure and heart rate increased to ≥20% basal values.
Postoperatively, patients received patient-controlled analgesia morphine IV as analgesia. Intraoperative opioid rescue, postoperative visual analog scale (VAS) score, and opioid consumption were measured 3, 6, and 24 hours later.
Statistical analysis
All statistical analyses were performed using Statistical Package for Social Sciences (SPSS) for Windows (SPSS Inc., Chicago, IL, USA) software version 20. Numerical variables were expressed as mean ± SD or median (minimum–maximum). Categorical variables were expressed as frequency (%). Test of normality was done using Shapiro–Wilk test, and homogeneity test was done using Levene’s test. Independent t-test was used to compare means if data distribution was normal, or nonparametric test Mann–Whitney U was used if data was not distributed normally. χ2 or Fischer’s exact test was used for assessing categorical variables. The level of significance was set at α 0.05.
Ethics statements
The Research Ethics Committee of Faculty of Medicine Udayana University and Sanglah Hospital approved this study. Prior to participation, all subjects gave written informed consent and were fully informed of the procedures in the studies.
Results
There were no significant differences (p>0.05) in both groups in terms of sex, age, body mass index, and ASA physical status (Table 1). As shown in Table 2, the need for opioid rescue was significantly different (p≤0.05). Patient in LM group needed more intraoperative opioid rescue than US group, 81.2% and 44.4% respectively. Time to the first dose of opioid rescue did not differ significantly (p>0.05).
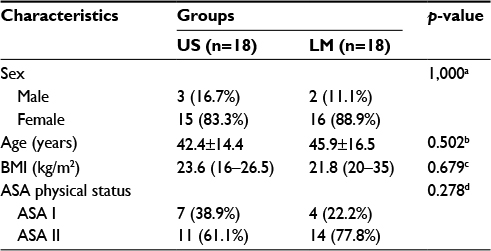 | Table 1 Subject characteristics Notes: Values are expressed as mean ± SD or median (minimum–maximum) for numerical data and frequency (%) for categorical data; n = number of subjects; aFisher’s exact test; bIndependent t-test; cMann–Whitney U-test; dχ2 test. Abbreviations: ASA, American Society of Anesthesiologists; BMI, body mass index; LM, landmark; US, ultrasound. |
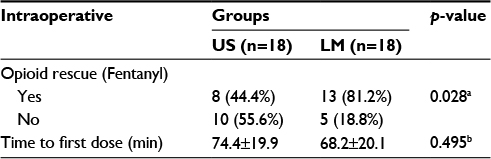 | Table 2 Opioid rescue intraoperative Notes: Values are expressed as mean ± SD for numerical data and frequency (%) for categorical data; n = number of subjects; aχ2 test; bIndependent-t test. Abbreviations: LM, landmark; US, ultrasound. |
Postoperative VAS scores were not significantly different at 3 hours after surgery (p>0.05), but it significantly differed (p≤0.05) at 6 and 24 hours after surgery (Table 3). VAS scores were higher in LM group than US group at 6 hours (mean of 15±8.6 mm and 6.7±8.4 mm, respectively) and 24 hours after surgery (mean of 22.8±8.3 mm and 10±8.4 mm, respectively). The maximum VAS score was 20 mm in US group and 30 mm in LM group.
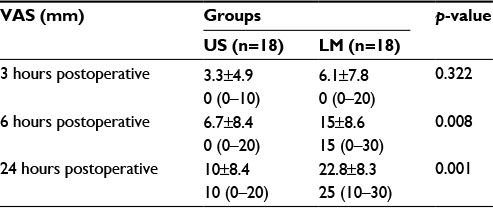 | Table 3 Comparison of postoperative pain score Notes: Values are expressed as mean ± SD and median (minimum–maximum); n = number of subjects; Mann–Whitney U-test. Abbreviations: LM, landmark; US, ultrasound; VAS, visual analog scale. |
As shown in Table 4, postoperative morphine consumption was not significantly different at 3 hours after surgery (p>0.05), but at 6 and 24 hours after surgery, the morphine consumption was significantly lower in US group than LM group (p≤0.05). None of the patients in US group need morphine to control their pain at 3 hours after surgery. Mean of morphine consumption was 0.2±0.5 mg in US group and 1.2±0.7 mg in LM group at 6 hours postoperatively. At 24 hours after surgery, the mean of morphine consumption in US group was 0.5±0.5 mg, while it was 2.4±1.1 mg in LM group.
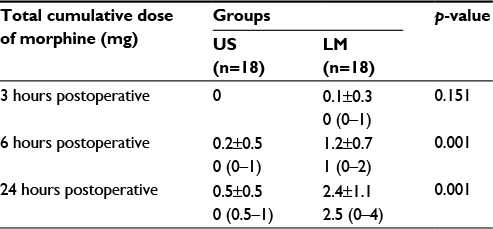 | Table 4 Comparison of postoperative opioid consumption Notes: Value are expressed as mean ± SD and median (minimum–maximum); n = number of subjects; Mann–Whitney U-test. Abbreviations: LM, landmark; US, ultrasound. |
Discussion
Pain after thyroidectomy is regarded as being of mild-to-moderate intensity and short duration. Especially within 24 hours after surgery, most of the patients require opioid and nonopioid analgesics.1,5 Regional anesthesia is one of the modalities to reduce the surgical pain. Aunac et al6 in their study concluded that combined deep and superficial cervical plexus block is an effective technique to alleviate pain during and immediately after thyroidectomy. But in subsequent studies it was shown that superficial cervical plexus block is at least as effective as a combined superficial and deep cervical plexus block.7,8
Several studies have demonstrated the effectiveness of bilateral superficial cervical plexus block. Conventional LM or US-guided technique for bilateral superficial cervical plexus block has been used in thyroidectomy to decrease pain and analgesic requirement both intra- and postoperatively. Conventional LM technique was used in study by Dieudonne et al,9 Andrieu et al,5 and Shih et al,1 and these studies concluded that bilateral superficial cervical plexus blocks improved intraoperative analgesia, reduced the amount of general anesthetic required during thyroidectomy, and lowered the severity of postoperative pain. Another study by Messner et al10 concluded that superficial cervical plexus block was safe, easy to perform, and an effective procedure to reduce morphine consumption and improve pain relief after carotid endarterectomy under general anesthesia. However, the study by Eti et al11 showed that bilateral superficial cervical plexus block did not decrease analgesic requirement after thyroid surgery. Gurkan et al4 in their study concluded that ultrasound-guided bilateral superficial cervical plexus block had a significant analgesic effect in patients undergoing thyroid surgery.
US is the preferred method of nerve localization because of direct visualization of nerves and adjacent anatomical structures. It allows visualization of needle movement and direct spread of LA, thus making the procedure safer and more effective as compared to LM technique. Some case series have demonstrated shortened procedure time and faster block onset compared with conventional techniques. Longer duration of anesthesia and analgesia has also been reported. The effectiveness of US-guided nerve block is achieved because of accurate deposition of LA in close proximity of nerve, resulting in faster and dense block of nerve. In bilateral superficial cervical plexus blocks, deep needle insertion (>1–2 cm) should be avoided in order to prevent the block of the phrenic or recurrent laryngeal nerve, and subarachnoid or vertebral artery injection.2,3,12
Conclusion
US-guided bilateral superficial cervical plexus block more effective in reducing pain both intra- and postoperatively compared with LM technique in patients undergoing thyroidectomy.
Disclosure
The authors report no conflicts of interest in this work.
References
Shih ML, Duh QY, Hsieh CB, et al. Bilateral superficial cervical plexus block combined with general anesthesia administered in thyroid operations. World J Surg. 2010;34(10):2338–2343. | ||
Marhofer P, Chan VW. Ultrasound-guided regional anesthesia: current concepts and future trend. Anesth Analg. 2007;104(5):1265–1269. | ||
Kessler J, Gray AT. Ultrasound guidance for regional anesthesia. In: Miller RD, Cohen NH, Eriksson LI, et al, editors. Miller’s Anesthesia. 8th ed. Philadelphia: Elsevier; 2015:1752–1766. | ||
Gurkan Y, Tas Z, Toker K, Solak M. Ultrasound guided bilateral cervical plexus block reduces postoperative opioid consumption following thyroid surgery. J Clin Monit Comput. 2015;29(5):579–584. | ||
Andrieu G, Amrouni H, Robin E, et al. Analgesic efficacy of bilateral superficial cervical plexus block administered before thyroid surgery under general anaesthesia. Br J Anaesth. 2007;99(4):561–566. | ||
Aunac S, Carlier M, Singelyn F, De Kock M. The analgesic efficacy of bilateral combined superficial and deep cervical plexus block administered before thyroid surgery under general anesthesia. Anesth Analg. 2002;95(3):746–750. | ||
Pintaric TS, Hocevar M, Jereb S, Casati A, Jankovic VN. A prospective, randomized comparison between combined (deep and superficial) and superficial cervical plexus block with levobupivacaine for minimally invasive parathyroidectomy. Anesth Analg. 2007;105(4):1160–1163. | ||
Suh YJ, Kim YS, In JH, Joo JD, Jeon YS, Kim HK. Comparison of analgesic efficacy between bilateral superficial and combined (superficial and deep) cervical plexus block administered before thyroid surgery. Eur J Anaesthesiol. 2009;26(12):1043–1047. | ||
Dieudonne N, Gomola A, Bonnichon P, Ozier YM. Prevention of postoperative pain after thyroid surgery: a double-blind randomized study of bilateral superficial cervical plexus blocks. Anesth Analg. 2001;92(6):1538–1542. | ||
Messner M, Albrecht S, Lang W, Sittl R, Dinkel M. The superficial cervical block for postoperative pain therapy in carotid artery surgery. A prospective randomised controlled trial. Eur J Vasc Endovasc Surg. 2007;33(1):50–54. | ||
Eti Z, Irmak P, Gulluoglu BM, Manukyan MN, Gogus FY. Does bilateral superficial cervical plexus block decrease analgesic requirement after thyroid surgery? Anesth Analg. 2006;102(4):1174–1176. | ||
Madison SJ, Ilfeld BM. Peripheral nerve blocks. In: Butterworth JF, Mackey DC, Wasnick JD, editors. Morgan & Mikhail Clinical Anesthesiology. 5th ed. New York: McGraw-Hill; 2013:975–1022. |
 © 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.